STUDIES ON THE INHIBITORY EFFECT OF VARIOUS
PHYTOCHEMICAL COMPONENTS ON 3- HYDROXY 3- METHYL GLUTARYL (HMG) CoA REDUCTASE IN CHOLESTEROL
BIOSYNTHESIS
Thesis submitted to
THE TAMIL NADU Dr. M.G.R. MEDICAL UNIVERSITY CHENNAI – 600 032.
In partial fulfillment of the requirements for the award of
Ph.D. degree under Basic Medical Sciences
Submitted by
J. MERCY JASMINE M.Sc. INSTITUTE OF BIOCHEMISTRY
MADRAS MEDICAL COLLEGE CHENNAI – 600 003
SUPERVISOR & GUIDE DR. R.VANAJA, M.Sc., Ph.D
CERTIFICATE
Certified this thesis titled “STUDIES ON THE INHIBITORY EFFECT OF VARIOUS PHYTOCHEMICAL COMPONENTS ON 3-HYDROXY-3-METHYL GLUTARYL (HMG) CoA REDUCTASE IN CHOLESTEROL BIOSYNTHESIS” submitted by J. Mercy Jasmine, is a bonafide record of work done by her in the Institute of Biochemistry, Madras Medical College, in partial fulfillment of the regulations of The Tamilnadu Dr.M.G.R Medical University, Chennai.
DEAN,
Madras Medical College &
CERTIFICATE
This is to certify
(i) That the thesis entitled “STUDIES ON THE INHIBITORY EFFECT OF VARIOUS PHYTOCHEMICAL COMPONENTS ON 3-HYDROXY-3-METHYL GLUTARYL (HMG) CoA REDUCTASE IN CHOLESTEROL BIOSYNTHESIS” is a bonafide record of research work done by the candidate Ms. J. MERCY JASMINE, during the period of study (2010-2014) under my supervision and guidance and that the thesis has not formed the basis for the award to the candidate of any other Degree, Diploma, associateship, fellowship or other similar titles and
(ii) That the thesis submitted by Ms. J. MERCY JASMINE represents independent and original work on the part of the candidate.
Chennai 600 003 Supervisor & Guide
Date:
CERTIFICATE
This is to certify
(i) That the thesis entitled “STUDIES ON THE INHIBITORY EFFECT OF VARIOUS PHYTOCHEMICAL COMPONENTS ON 3-HYDROXY-3-METHYL GLUTARYL (HMG) CoA REDUCTASE IN CHOLESTEROL BIOSYNTHESIS” is a bonafide record of research work done by the candidate Ms. J. MERCY JASMINE, during the period of study (2010-2014) under my guidance and that the thesis has not formed the basis for the award to the candidate of any other Degree, Diploma, associateship, fellowship or other similar titles and
(ii) That the thesis submitted by Ms. J. MERCY JASMINE represents independent and original work on the part of the candidate.
Chennai 600 003 Co-Guide
Date:
DECLARATION
ACAD-1(2)/09059/2009, dated 13.08.2010
EXII(1)/09059/2009, dated 07.09.2011
I, J. Mercy Jasmine, hereby declare that the thesis titled “STUDIES ON THE INHIBITORY EFFECT OF VARIOUS PHYTOCHEMICAL COMPONENTS ON 3-HYDROXY-3-METHYL GLUTARYL (HMG) CoA REDUCTASE IN CHOLESTEROL BIOSYNTHESIS” submitted to The Tamilnadu Dr. M.G.R. Medical University, Chennai-32 for the award of Doctor of Philosophy, under basic medical science is a record of work entirely done by me and that it has not previously formed the basis for the award of any Degree, Diploma, associateship, fellowship or other similar titles of any other university.
Chennai 600003
ACKNOWLEDGEMENT
I thank and praise Lord Jesus, EL Shaddai, for providing me with this His spirit,
wisdom, strength and endurance to complete this research work. I am sincerely
grateful for His guidance and for reasons too numerous to mention.
I would like to express my greatest gratitude to my guide and supervisor Dr. R.
Vanaja M.Sc., Ph.D, Associate Professor, Department of Biochemistry, A.C.S.
Medical College and Guide and Supervisor, The Tamilnadu Dr. M.G.R Medical
University, for her unceasing guidance that enabled me to complete this work
successfully.
I wish to acknowledge the guidance provided by Dr. D. Nandhini, M.Sc.,M.Phil,
Ph.D, Associate Professor of Biochemistry, Ragas Dental College, as co-guide
and member of doctoral advisory committee throughout the work.
My profound gratitude to Dr. K. Ramadevi M.D, Director and Head of the
Department, Institute of Biochemistry, Madras Medical College for her
perpetual advice as member of doctoral advisory committee and for providing
me the facilities to carry out this research work.
My special thanks to the Dean, Madras Medical College and to the Director of
It is my privilege to thank the Vice Chancellor of The Tamilnadu Dr.M.G.R.
Medical University for permitting me to accomplish the research work.
My deepest regards are due to Dr. G. Gaddam Aadhinaath Reddy, M.Pharm,
Ph.D, Research Officer, Pharmacology, Siddha Central Reasearch Institute for
his constant guidance in animal experimentation and valuable suggestions
whenever required.
I would like to express my very great appreciation to Dr. K. Latha, Vice
President, Research & Development, T.Stanes Company Pvt. Ltd., Coimbatore,
for her valuable and constructive suggestions during the planning and
development of this research work.
I am immensely grateful to Dr. Shantha Ravishankar, Professor of Pathology,
Madras Medical College, for lending her expertise in helping me with the
histological studies.
I wish to express my gratitude to Mr. R. Ganesan, Research Officer,
Biochemistry, Siddha Central Research Institute for permitting me to use his lab
to carry out a part of my biochemical analysis.
My earnest regards to Mr. S. Kumaravel, Assistant Professor, Department of
Chemistry, Indian Institute of Crop Processing Technology, Thanjavur, for his
My special thanks are extended to the lab technicians of the department of
pharmacology and biochemistry, Siddha Central Research Institute for their
technical assistance and cooperation in completing this work successfully.
I owe a special thanks to Mrs. R. K. Jananie, Ms. V. Priya and Mrs. Regina
Prem, my fellow research workers for helping me with the animal
experimentation and sharing their valuable insights throughout the period of
work.
I am much obliged to thank Mr. M. Santhosh for helping me with the molecular
docking studies and for helping me to understand the basics of bioinformatics.
I am truly grateful to Ms. Divya Sekar, Ms. Divya Kodi and Ms. S. Sobhana for
their assistance in formatting the thesis.
I am incredibly thankful to Ms. Archana Krishnan, for being my friend, moral
support and helping me with the flow charts and proof reading even though
she does not consider this as English.
My heartfelt gratitude to my father Dr. S. John Gurupatham, my rock of
strength, for being the most understanding dad and for providing me with
everything that I could ever ask for. My profound gratitude is due to my family
for being my support system especially my brother Mr. J. Sam Charles and my
CONTENTS
Chapter Title Page No.
1. Introduction 1
2. Aims and Objectives 7
3. Review of Literature 9
4. Scope and Plan of work 41
5. Materials and Methods 43
6. Results and Analysis 82
7. Discussion 115
8. Summary and Conclusion 133
Bibliography
1
1. INTRODUCTION
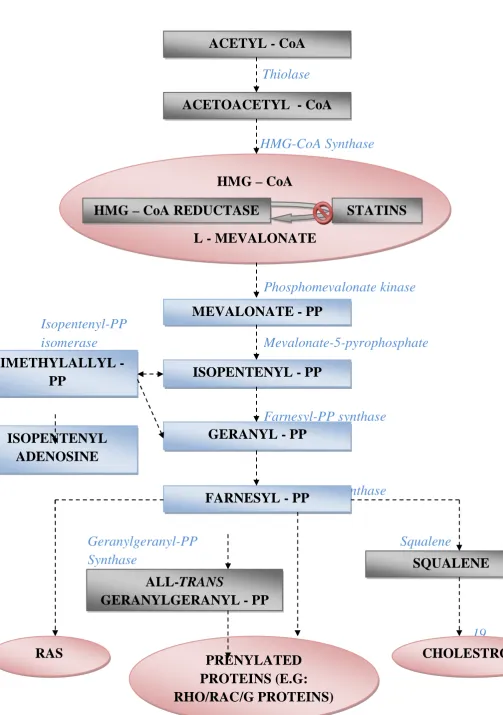
Hyperlipidemia is a condition which is characterized by abnormal elevation of lipids (triglyceride and cholesterol) and lipoproteins (LDL, VLDL) levels in the blood. [1] It is also the major risk factor in the initiation and progression of the atherosclerotic lesions. Evidence suggests that the progression can be slowed if elevated serum concentration of the atherogenic lipoprotein and triglycerides are reduced, thereby preventing coronary heart disease. [2] Statins, a class of cholesterol lowering drugs that inhibits cholesterol synthesis, have been most widely prescribed for treating hypercholesterolemia and reducing cholesterol levels through therapeutic drugs as statins have significantly reduced the risk of the development of atherosclerosis and associated cardiovascular diseases [3].
2
catalyzing the NADPH-dependent, two-step reduction of HMG CoA to mevalonate. The inhibition of this enzyme results in the significant decrease in cholesterol levels. [6],[7] This is a highly regulated process within the cholesterol biosynthetic pathway and as a result an attractive target for intervention in the treatment of hypercholesterolemia.
Sterols regulate the transcription of HMGR and the non-sterols regulate the translation of mRNA. Both sterols and non-sterols are essential for the regulation of HMGR protein degradation.[6]
The rate of synthesis of reductase mRNA is controlled by the sterol regulatory element binding protein (SREBP). This transcription factor binds to a short DNA sequence called the sterol regulatory element (SRE) on the 5 side of the reductase gene. When cholesterol levels fall, the amino-terminal domain of SREBP from the nuclear membrane is released and migrates to the nucleus and binds the SRE of the HMGR gene, to enhance transcription. When cholesterol levels rise, the proteolytic release of the SREBP is blocked, and the SREBP in the nucleus is rapidly degraded. These two events halt the transcription of the genes of the cholesterol biosynthetic pathway.
3
Mevalonate reduces the HMG-CoA mRNA translation by 80% with no change in the mRNA levels.
In response to increasing concentrations of cholesterol, the membrane domain of HMGR undergoes a change in its oligomerization state making the enzyme more susceptible to proteolysis. Homologous sterol-sensing regions are present in the protease that activates SREBP. The enzyme is further degraded by ubiquitination.
Phosphorylation decreases the activity of the HMGR by inactivating the AMP-activated protein kinase. Thus, cholesterol synthesis ceases when the ATP level is low.
The synthesis of LDL receptor is subjected to feedback regulation. When cholesterol is abundant inside the cell, new LDL receptors are not synthesized, and so the uptake of additional cholesterol from plasma LDL is blocked. When cholesterol is required, the amount of mRNA for the LDL receptor rises and more receptor is found on the cell surface. This state can be induced by a two mechanisms. First, the intestinal reabsorption of bile salts, that promote the dietary cholesterol, is inhibited. Second, de novo synthesis of cholesterol is blocked.
4
Reductase blockers known as statins prevent the synthesis of cholesterol at the mevalonate and provide significant protection against coronary artery disease,[9],[10] stroke[11] and ischemic injury.[12] In addition to their pleiotropic effect, these drugs were proven to have adverse side effects such as autoimmune diseases, polyneuropathy and myopathy.[13],[14],[15]
Medicinal plants are regarded as potential sources of new compounds of therapeutic value and as sources of lead compounds in drug development. In developing countries, it is estimated that 80% of the population really depends on traditional medicine for their healthcare. Thereby it is essential to screen medicinal plants for bioactive compounds as a basis for further pharmacological studies.[16] Decholestrate is a polyherbal formulation that comprises of the extracts of the plant constituents from Zingiber officinale (Ginger), Tinospora cordifolia (Guduchi), Piper longum (long pepper), Phyllanthus emblica (Amla), Embellia ribes (False black pepper), Vigna unguiculata (Cow pea), Garcinia cambogia (Gambooge), Commiphora mukul (Guggul), and Camellia sinensis (Tea leaves). Phytoformulation-1 is a polyherbal formulation that contains the extracts of the plant constituents from Terminalia arjuna (Arjun tree), Emblica officianalis (Indian gooseberry), Plectranthus barbatus (Coleus forskohlii), Curcuma longa (Turmeric),
5
cambogia (Gambooge). In the present study, the aqueous extract of the polyherbal formulations, Decholestrate and Phytoformulation 1 were investigated for antihyperlipidemic activity in hyperlipidemic rats.
6
availability of the structural information aids in proper selection of target for inhibitor discovery as the binding sites of the molecules are identified.[17] This in silico analysis was applied in the current study to optimize the phytochemicals that bind with the target protein of the enzyme, HMGR.
7
2. AIMS AND OBJECTIVES
Aim:
To study the inhibitory action of phytochemical components in the polyherbal formulation Decholestrate and Phytoformulation 1, towards 3- Hydroxy 3- Methyl Glutaryl (HMG) CoA reductase in cholesterol biosynthesis.
Objectives:
1. To collect, identify and to prepare the aqueous extract of the plant/plant parts.
2. To conduct the in vivo study by inducing the lipid levels of the animals by feeding them with the hyperlipidemic diet and treating with the drugs.
3. To monitor the body weight and food intake of the animals throughout the study.
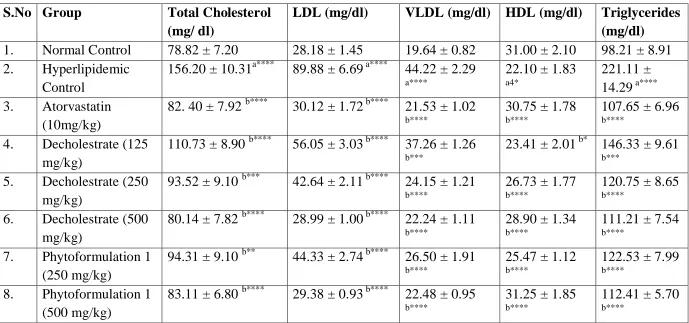
4. To estimate the level of Total Cholesterol, Triglycerides, HDL, VLDL and LDL in serum and hepatic tissue.
8
6. To assay the level of Lipid Peroxidation, Catalase (CAT), Superoxide Dismutase (SOD), Vitamin E and Vitamin C in plasma, hemolysate and hepatic tissue.
7. To assay the level of Aspartate Transaminase (AST), Lactate Dehydrogenase (LDH), Creatinine Kinase (CK-MB) to monitor the tissue damage and to estimate the level of Glucose in blood.
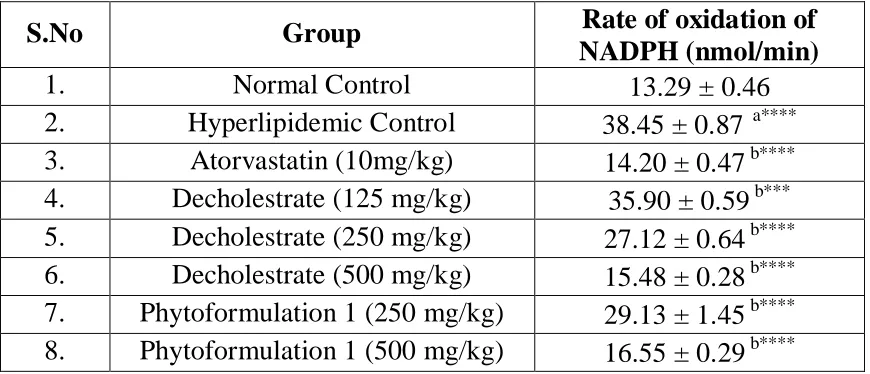
8. To assess the activity of HMG CoA reductase by determining the rate of oxidation of NADPH in the hepatocytes.
9. To screen the histopathological changes in the tissues.
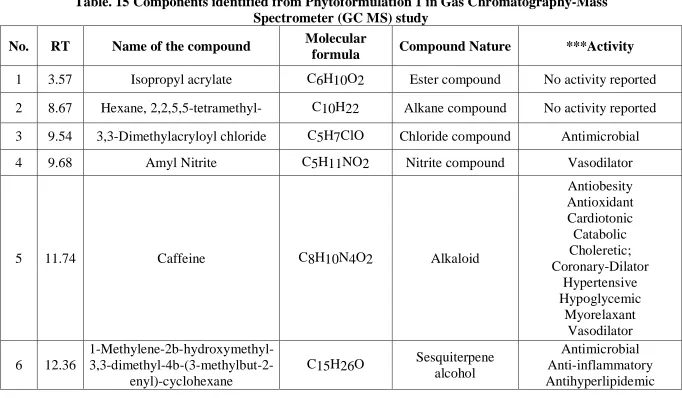
10.To identify the major secondary metabolites present in the test drug by analyzing the plant extract in Gas Chromatography-Mass Spectrometer (GCMS).
9
3. REVIEW OF LITERATURE
3.1 HYPERLIPIDEMIA
Hyperlipidemia is a powerful risk factor for coronary heart disease (CHD).[18] An increased risk of morbidity and mortality in atherosclerotic diseases (angina, heart attack, peripheral vascular diseases etc.,) is a result of elevated plasma cholesterol, particularly low-density lipoprotein (LDL) cholesterol. In humans, most of the cholesterol biosynthesis occurs in hepatocytes. So regulating the production of cholesterol or inhibiting its overproduction is crucial to maintain the homeostasis, ensuing the adverse effects of hyperlipidemic conditions are prevented.
3.2 HMG-COA REDUCTASE INHIBITORS
10
complexes cause disorder in the several catalytically relevant residues near the carboxy terminus of HMGR. In addition to competing with HMG-CoA for the active site of the enzyme [20], statins also change the enzyme confirmation on binding, preventing HMG-CoA reductase from attaining a functional structure. [21] As a result the concentration of the hepatic cholesterol is reduced. This leads to the homeostatic response, involving up-regulation of cell-surface receptors that bind LDL and very-low-density lipoprotein (VLDL). These lipoproteins are taken up into cells and degraded. Statins may inhibit hepatic synthesis of apolipoprotein B-100, causing reduced synthesis and secretion of triglyceride-rich lipoproteins [22] (Grundy SM, 1988). The primary mechanism of action for LDL lowering is enhanced clearance of LDL via LDL receptors. Atorvastatin and Simvastatin are capable of lowering LDL in patients with homozygous familial hypercholesterolemia, who have no functional LDL receptors. [23]
3.3 TYPES OF STATINS
11
inhibitor than Mevastatin with a Ki of 0.6nM without causing hepatocellular toxicity. Thus it became the first approved cholesterol lowering agent of this class. Since then, several new natural and chemically modified statins have become commercially available such as pravastatin, simvastatin, fluvastatin, atorvastatin, cerivastatin, pitavastatin and rosuvastatin. [24]
12
Lipophilicity may not predict the ability of statins to exert extra hepatic effects in animal and human studies. There may be specific mechanisms for hydrophilic statins to enter extra hepatic cells, such as endothelial cells. Hepatocytes possess such a mechanism, where the organic anion transporter (OATP-C) enables the hydrophilic statins to enter the cell.[28] Lovastatin, simvastatin, atorvastatin and cerivastatin undergo the cytochrome P 450 (CYP) 3A4 pathway for metabolism or biotransformation. The metabolism of fluvastatin occurs via CYP2C9 pathway. [29]
3.4 EFFECTS OF STATIN TREATMENT
13
atorvastatin 80 mg and rapid impairment on statin withdrawal after 30 days. [32] These findings support the view that statins may exert beneficial effects on endothelial dysfunction that are independent of the degree of plasma cholesterol lowering.
3.5 BENEFICIAL PLEIOTROPIC EFFECTS OF STATINS
Many drugs, even when they modulate one single metabolic step, have multiple effects due to the different functions that the affected pathway in different organs or tissues. In recent years, major clinical trials and supplementary mechanistic studies have provided growing evidence that some of the impressive effects of statins, which are the most widely prescribed lipid-lowering drugs, on the occurrence or recurrence of vascular events could be credited to their pleotropism.
3.5.1 Effects on endothelium
14
endothelial nitric oxide synthase eNOS, in endothelial cells. [34] Statins also directly enhance constitutive eNOS activity, thereby increasing the bioavailability of NO. [35] Statins also interfere with the prenylation of Rho GTPase by geranylgeranyl pyrophosphate (GGPP), preventing its translocation to the cell membrane where it negatively regulates eNOS activity.[36] A study with atorvastatin in type 2 diabetes demonstrated a significant improvement in endothelium-dependent vasodilation. [37] A similar finding was reported with atorvastatin in young patients with type 1diabetes and normal cholesterol levels. [38]
3.5.2 Effects on smooth muscle cell
Statins can decrease smooth muscle cell growth in vitro at pharmacological doses. Additionally, both simvastatin and pravastatin reduce the proliferation of macrophages exposed to oxidized LDL. [39] It is well established that statins inhibit the growth of lymphocytes and other blood mononuclear cells via multiple pathways unrelated to cholesterol metabolism.[40]
3.5.3 Statins and platelet function
15
plaque rupture and vascular injury. [41] Hypercholesterolemia is associated with increased platelet reactivity. These abnormalities are linked to increases in the cholesterol/phospholipid ratio in platelets. Other potential mechanisms include increase in thromboxane A2 (TXA2) biosynthesis, platelet 2-adrenergic receptor density and platelet cytosolic calcium. One of the well characterized effects of endothelial NO is the inhibition of platelet aggregation. [42] Potential additional mechanisms include a reduction in the production of Thromboxane A2 (TXA2) and modifications in the cholesterol content of platelet membranes. [43] The cholesterol content of platelet and erythrocyte membranes is reduced in patients taking statin therapy. This may lead to a decrease in the thrombogenic potential of these cells. Indeed, animal studies suggest statin therapy inhibits platelet deposition on damaged vessels and reduces platelet thrombus formation. [44]
3.5.4 Statins and inflammation
16
17
complement activation and thereby increasing the expression of cellular adhesion molecules, and decreasing eNOS expression, which leads to the propensity for thrombosis, inflammation, and endothelial dysfunction. Studies also show that the transgenic over expression of human CRP in transgenic mice leads to arterial injury. [51] In the Cholesterol and Recurring Events (CARE) trial, statins significantly decreased plasma hs-CRP levels over a five-year period in patients who did not experience recurrent coronary events. [52] Furthermore, preliminary data from the Pravastatin Inflammation/CRP Evaluation (PRINCE) study confirm that statin therapy can significantly reduce serum hs-CRP levels in primary and secondary prevention populations. [53] These studies thereby indicate that statins effectively decrease systemic and vascular inflammation.
3.5.5 Effect of statin on hypertrophy
18
also inhibited by simvastatin (2 mg/kg/d for 4 weeks). [55] These results suggest that statins in addition to the vascular wall and the heart exert.[56] 3.5.6 Statins and cancer therapy
Among the Rho family members, RhoA protein is overexpressed in tumor cells from different tissues. [57] Inhibiting RhoA prenylation was shown to prevent apoptosis by Bcl-2 and the treating with statin particularly lipophilic statins (fluvastatin and lovastatin) reduced the rate of prenylation inhibition since the mevalonate addition was able to reverse the effect. [58] Competitive inhibitors of HMGR induce cell cycle arrest in G1 phase. [59] Also HMGR activity has been shown to be related to cell transformation [60] and to mediate the growth-inhibitory effects of retinoic acid in neuroblastoma cells. [61] These findings HMGR inhibitors can be a potential target for cancer treatment.
3.5.7 Effects on stroke, hypertension and Alzheimer’s disease
Experimental and clinical evidence suggest that chronic statin treatment may also decrease stroke severity and improve outcome when given after ischemia onset. Evidence also suggest that in patients with acute vascular syndrome or those undergoing cardiovascular surgery discontinuation of statin medication may be associated with impaired vascular function. [62]
19
arterial pressure in hypertensive rats. [63] HMGR inhibitors may cause vasodilation and decrease the blood pressure by resorting endothelial dysfunction that frequently accompanies hypertension and hypercholesterolemia. The beneficial effects of pravastatin on blood pressure can be mediated not only by a decrease in LDL cholesterol but also by the upregulation of nitric oxide synthase [36]
Observational studies reveal that an elevated serum cholesterol level is a risk factor for Alzheimer’s disease. [64] Statins, regardless of their brain availability have been suggested to induce alterations in cellular cholesterol distribution in brain. Wolozin and colleagues suggested that the prevalence of Alzheimer’s disease in patients taking statins is 60% lower in comparison to patients taking other medications used in the treatment of cardiovascular diseases. [65] The systemic vascular protective effects of statin treatment are likely to contribute to their beneficial effects, especially on vascular forms of dementia syndrome.
3.6 ADVERSE EFFECTS OF STATINS 3.6.1 Liver and muscle toxicity
20
than the upper limit of normal. Myopathy, which is dose related, occurs in approximately1 in 1000 patients. Symptoms may include fever and malaise, and cases have been associated with elevated serum statin drug levels. Rhabdomyolysis and acute renal failure may result if myopathy is not recognized with the continuous use of the drug.[15] If recognized promptly, the myopathy is reversible, and acute renal failure is unlikely to ensue.
3.6.2 Statins and combination therapy
21 3.6.2 Statin therapy and myositis
According to WHO (World Health Organisation) criteria, the relationship between statin therapy and diplopia (double vision), ptosis (drooping eyelid) or ophthalmoplegia (extraocular muscle palsy) is possible. This is based on the time of the drug administration and adverse drug reaction (ADR) development. The plausible mechanism for the above conditions may be due to the myositis of the extracellular muscles and the levator palpebrae superiosis muscles or both. [70]
3.6.3 Statins and risk of polyneuropathy
22 3.6.4 Statins and autoimmune disease
More than 20 cases taking statins have been reported to have developed autoimmune disease. Most patients had systemic lupus erythematosus (SLE) but dermatomytosis, autoimmune hepatitis and pemphigoides are also reported.[13] Several pathogemic mechanisms have been postulated in statin induced SLE. Cellular apoptosis, which has an important role in SLE might be exacerbated or triggered by second generation statins, which are pro-apoptotic agents. Release of nuclear antigens into the circulation could cause production of pathogenic autoantibodies. Also the direct immunomodulator effect of statins on T cells may possibly be involved. SLE is characterised by a shifting of T helper 1 to T helper 2 immune responses, causing B-cell reactivity and production of pathogenic autoantibodies. Statins and selenoprotein inhibition can aggravate this event. [73]
3.6.5 Effect of Statin on Coenzyme Q 10
23
on the cholesterol lowering or anti-inflammatory properties of the statin drugs. [74]
3.7 ROLE OF OXIDATIVE STRESS IN HYPERLIPIDEMIA
Consumption of high-cholesterol diet (HCD) and reduced physical activity to dissipate the energy leads to hyperlipidemia.[75] Oxidative stress in hyperlipidemia is thought to be an important factor in the development of atherosclerotic plaques.[76]Accumulation of lipid peroxides generated by free
24
the development of functional foods and nutraceuticals to prevent oxidative stress [88] and the oxidation of lipids.[89]
3.8 PLANT BASED COMPOUNDS AS HMG-COA REDUCTASE INHIBITORS
Many plant-derived products have shown to have potent inhibitory properties towards HMG CoA Reductase enzyme. Policosanol safely down-regulates HMG-CoA Reductase – potential as a component of the Esselstyn regimen. [90] The tocotrienols derived from barley are widely distributed in the plant kingdom and differ from tocopherols (Vitamin E) only in three double bonds in the isoprenoid chain which appear to be essential for the inhibition of cholesterogenesis.[91] It is currently accepted that the consumption of fruit-derived antioxidants such as Vitamin C, Carotenoids, and Flavonoids provides a preventive effect against cardiovascular disease. Kiwifruit have potential cardiovascular protective properties in vitro. [92] The tetralin derivatives and salts were proved to inhibit HMG-CoA Reductase and so inhibit cholesterol biosynthesis.
3.9 POLYHERBAL FORMULATIONS
25
rats. The LD50 values of the plant extracts that constitutes the formulations were above 2.5g/kg body weight
3.9.1 Decholestrate
Zingiber officinale
Ginger or ginger root is the rhizome of the plant Zingiber officinale, consumed as a delicacy, medicine, or spice and it belongs to the family, Zingiberaceae . It was reported to possess anti-inflammatory, anti thrombic and anti hyperlipidemic properties. [93],[94] It also acts as a protective agent against acetaminophen induced hepatotoxicity.[95] It was also shown to prove prevent platelet aggregation. [96] Ginger has also been shown to be potent antipyretic, analgesic, antimicrobial activity. [97]
Phyllanthus emblica
26
Tinospora cordifolia
Tinospora cordifolia, family Menispermaceae (Common names: Guduchi, Amrita, Giloya, Shinddil kodi) is a widely used shrub in folk and ayurvedic systems of medicine. The chemical constituents reported from its shrub belong to different classes such as alkaloids, diterpenoid lactones, glycosides, steroids, sesquiterpenoid, phenolics, aliphatic compounds and polysaccharides. The notable medicinal properties reported are anti- diabetic, anti-periodic, anti-spasmodic, anti-inflammatory, anti- arthritic, anti- oxidant, anti-allergic, anti-stress, anti-leprotic, anti-malarial, hepatoprotective, immunomodulatory and anti- neoplastic activities. [103]
Commiphora mukul
Guggulsterones, family Burseraceae (Common names: Kukkil, Maishakshi, Gukkal, Kiluvai, Gugglu. It was proven to have antibacterial activity. [104] and anti-inflammatory activity. [105] Two antihyperlipidemic compounds, Z-, and E-Guggulsterone from the tree Commiphora mukul, has been traditionally used for mitigating lipid disorders. [106]
Garcinia combogia (Hydroxy Citric Acid)
27
Laboratory and animal studies of HCA have produced results that indicate a potential for modulation of lipid metabolism [108] consequently HCA is an ingredient in some weight loss products and dietary supplements. One isomer of HCA, known as (2S, 3R)-HCA, inhibits pancreatic alpha-amylase and intestinal alpha-glucosidase, leading to a reduction in carbohydrate metabolism in vitro.[107]
Piper longum
Piper longum Linn. is a native of Indo-Malaya region, sometimes called Indian long pepper, belongs to family Piperaceae. Piper longum Linn. has been used as a therapeutic agent in the treatment of various pathological conditions. Traditionally it is used for cardiovascular activities and anti-inflammatory activity. Extracts of Piper longum fruits have been reported to be bio-availability enhancer, immunomodulatory effect, antiasthamatic and hepatoprotective activity. [109]
Camellia sinensis
28
(UV) damage (which can damage the skin cells and cause skin cancer) and other types of cancers including breast cancer and skin cancer. [110]
Embelia ribes
Embelia ribes, commonly known as False Black Pepper, is a species in the Myrsinaceae. The ethanolic extract of Embelia ribes showed antioxidant effects on sterptozotocin induced diabetes in rats. [111] Embelin was proven to possess anticonvulsant activity against both grand mal and petit mal epilepsy. [112] E. ribes extract enhances the antioxidant defense against MCAO- induced focal cerebral ischemia in rats and exhibits neuroprotective activity. [113]
Vigna unguiculata
29 Phytoformulation 1
Terminalia arjuna
Terminalia arjuna, commonly known as arjuna or arjun tree in English, is a tree of the genus Terminalia. Terminalia Arjuna therapy in our patients with refractory congestive heart failure, mostly related to idiopathic dilated cardiomyopathy, appeared safe and caused long lasting improvement in symptoms and signs of heart failure along with improvement in left ventricular ejection phase indices with definite improvement in quality of life. [115] Terminalia arjuna tree bark powder has significant antioxidant action that is comparable to vitamin E. In addition, it also has a significant hypocholesterolaemic effect.[116] Aqueous extract of Terminalia arjuna prevents carbon tetrachloride induced hepatic and renal disorders against CCl4 induced oxidative stress. [117] Butanolic fraction of Terminalia arjuna bark has protective effects against Dox-induced cardiotoxicity and may have potential as a cardioprotective agent. [118]
T. arjuna acts as an gastroprotective agent probably due to its free radical scavenging activity and cytoprotective nature. [119] Emblica officianalis
30
responsible for anti-pyretic and analgesic activities. [120] The lipid lowering and antiatherosclerotic effects of Emblica officinalis was evaluated in cholesterol-fed rabbits. Aortic plaques were regressed suggesting that the E. officinalis juice is an effective hypolipidaemic agent. [121] Flavonoids from Emblica officinalis and Mangifera indica effectively reduce lipid levels in serum and tissues of rats induced hyperlipidemia. [122]
Plectranthus barbatus
Plectranthus barbatus is a tropical perennial plant related to the typical coleus species belongs to Lamiaceae. have been used to treat heart disease, convulsions, spasmodic pain and painful urination. [123] The chemical constituents of Plectranthus barbatus showed interesting activities in vitro, such as antioxidant activity [124] and acetylcholinesterase inhibition. [125]
Curcuma longa
31
collagenase, elastase, hyaluronidase, monocyte chemoattractant protein-1 (MCP-1), interferon-inducible protein, tumor necrosis factor (TNF), and interleukin-12 (IL-12). [127]The turmeric anti-oxidant protein (TAP) had been isolated from the aqueous extract of turmeric. The protein showed a concentration-dependent inhibitory effect on the promoter induced lipid peroxidation. [128] Dietary turmeric lowers lipid peroxidation by enhancing the activities of antioxidant enzymes. [129] Dietary curcumin also showed significant reduction in the lipid profile and phospholipids in the diabetic rats. [130]
Piper nigrum
Black pepper (Piper nigrum) is a flowering vine in the family Piperaceae, cultivated for its fruit, which is usually dried and used as a spice and seasoning. Supplementation of the black pepper or its active form piperine can reduce high fat diet induced oxidative stress to the cells. [131]
Piperine, an active alkaloidal constituent of the extract obtained from Piper longum and Piper nigrum, was reported to possess antihepatotoxic potential even more than siymarin. [132]
Allium sativum
32
including S-allylcysteine, have been found to retard the growth of chemically induced and transplantable tumors in several animal models. Therefore, the consumption of garlic may provide some kind of protection from cancer development. [133] Garlic was proven to possess a wide spectrum of actions such as antibacterial, antiviral, antifungal and antiprotozoal. [134] The ethanolic extract of garlic was reported to have a potent antidiabetic activity in the streptozotocin induced diabetic rats. [135]
The phytochemicals present in the plant extracts contribute to the protective effect of the plants towards a broad spectrum of clinical conditions. Thus the development of novel and sophisticated screening processes can be used to recognize the numerous applications of natural products and the introduction of natural product chemicals for treating disease could result in life saving drugs.
3.10 IN SILICO CHEMICO BIOLOGICAL APPROACH
33
excretion and toxicity profile and avoid safety issues. Commonly used computational approaches include ligand-based drug design (pharmacophore, a 3D spatial arrangement of chemical features essential for biological activity), structure-based drug design (drug-target docking), and quantitative structure–activity and quantitative structure–property relationships. Regulatory agencies as well as pharmaceutical industry are actively involved in development of computational tools that will improve effectiveness and efficiency of drug discovery and development process, decrease use of animals, and increase predictability.
3.10.1 Phytochemicals as lead compounds
34
mechanisms of action. In particular, in silico tools, combined with classical research methods, are expected to be more frequently applied by natural product scientists in an effort to maximize efficacy in drug discovery. These multidisciplinary studies are expected to bring novel molecules of great biomedical relevance.
3.10.2 Lead Compounds within Plant Extracts
35
PAO1. [138] This finding might be relevant for treatment of the inflammatory process of cystic fibrosis (CF). [139]
3.10.2 Identification of lead compounds
36
3.10.3 Identifying molecular targets and structurally related compounds
Collaboration between chemists, molecular and cellular biologists is of great added value. The identification of putative molecular targets is important for at least two reasons: (i) development of advanced biological assays and (ii) screening of sets of structurally related compounds. Several research groups have hypothesized specific cellular targets for lead compounds identified in medicinal plant extracts. They enhanced the simple docking procedure by means of a sort of combined target- and ligand based drug design approach. The results sustain the concept that docking performance is predictive of a biochemical activity.
37
like binding energy, inhibition constant and intermolecular energy were determined. The results showed that all the selected flavonoids showed lesser binding energy ranging between -8.40 kcal/mol to -6.03kcal/mol when compared with that of the standard(-4.47 kcal/mol).Intermolecular energy (-10.78kcal/mol to -6.63kcal/mol) and inhibition constant (698.45 nM to 37.98 M)of the compounds also coincide with the binding energy. Usually, presence of benzopyran ring in the basic nucleus contributes to the anti gout activity.All the selected flavonoids consist of benzopyran ring in its structure, which may attribute to its xanthine oxidase inhibitory activity. [142]
38
Enumerated based on the GOLD Scoring function to pick out the best Marine inhibitor based on GOLD score. Thus from the entire 122 Marine compounds which were Docked, we got best 4 of them with optimal GOLD Score. [143]
Aromatase (cytochrome P450 (CYP) 19) is a validated target for breast cancer. A ligand-based pharmacophore (abstract description of molecular features which are necessary for molecular recognition of a ligand by a biological macromolecule) was generated with three non-steroidal inhibitors. Two out of the three compounds were ultimately found to be micromolar inhibitors. [144] A structure-based catalyst pharmacophore was developed for acetylcholine esterase, which was subsequently used to search a natural product database. The same database was also screened against cyclooxygenase (COX)-1 and COX-2 structure-based pharmacophores, leading to the identification of known COX inhibitors.[145]
3.10.5 In silico analysis in antihyperlipidemic studies
39
inhibition, predicted in term of binding energy, for the first time implied that quinic acid ( G: -8.14 Kcal/mol) and paravastatin ( G: -8.22 Kcal/mol) exhibited almost same binding energy while other compounds also showed good binding energy, which in turn suggest that quinic acid alone or in combination with other major bioactive compounds were might be responsible for the HMGR inhibitory property of this extract. [146]
Cholesteryl esterase is the key enzyme involved in the hydrolysis of lipids and transport of free cholesterol. The reduction of cholesterol absorption by inhibiting cholesteryl esterase is a target site of intervention for the treatment of hyperlipidaemia. Molecular docking of pancreatic cholesteryl esterase (1F6W) and 28 phytochemicals reported from Terminalia cuneata Roth. with an automated docking software AutoDock 4.2, GOLD Suite of Programs 5.2 and iGEMDOCK. Of the 28 molecules, five showed best ligand binding energy which are Ellagic acid, Gallic acid, Leucocyanidin, Luteolin and Pyrocatechol. The autodock results were also compared with the GOLD and iGEMDOCK results. By using Dempster-Shafer theory (DST), luteolin identified as best lead compound from the plant T. Cuneata and the luteolin compound from the plant T. cuneata has the potential to regulate the cholesterol level in the blood by limiting the activity of the enzyme, pancreatic cholesteryl esterase [147]
40
41
4. SCOPE AND PLAN OF WORK
Scope:
The present study is carried out to
• Determine inhibitory potency of the polyherbal formulations, Decholestrate & Phytoformulation 1 on HMG CoA Reductase which is as effective as statin as well as devoid of any of its side effects.
• Screen the secondary metabolites in the formulations and study their chemical nature which is responsible for the inhibition of HMG CoA Reductase.
• Dock the phytochemicals obtained from the GC-MS study and further identify the compounds responsible for the inhibition and to exploit its potential as a possible lead for treating the hyperlipidemic clinical conditions.
Plan of work:
Phase I
• Collection of plant materials
• Confirmation of taxonomical identification
42
• Preparation of test drugs Decholestrate and Phytoformulation 1
Phase II
• Preparation of Atherogenic Diet
• Animal experimentation
• Estimation of lipid profile and glucose (serum and hepatic tissue) and determination of body weight
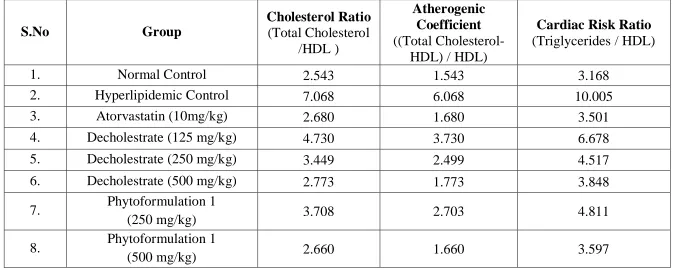
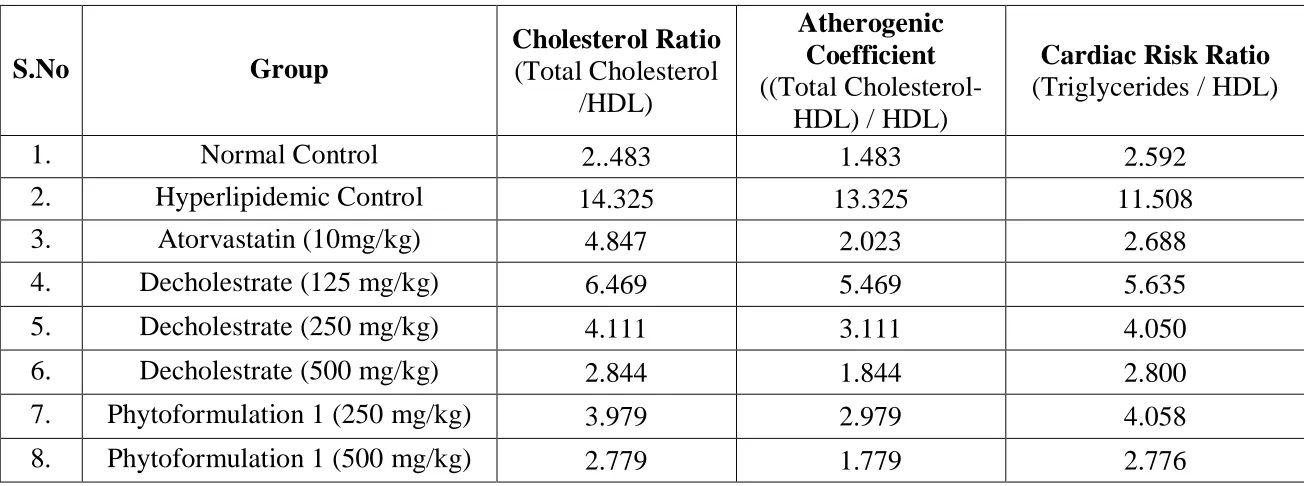
• Determination of atherogenic indices, Coefficient, Cardiac risk ratio, Cholesterol ratio and percentage of protection
• Estimation of antioxidants (plasma, hemolysate and hepatic tissue) and Enzymatic assay (AST, LDH, CK-MB)
• Determination of HMG CoA Reductase activity
• Histopathological studies
Phase III
• Identification of major secondary metabolites by GCMS
43
5. MATERIALS AND METHODS
5.1 Plant material
Fresh plant/plant parts were purchased, taxonomic identities were confirmed and the voucher specimen numbers of the plants were deposited at Phytopharma testing lab, T.Stanes Company Ltd. Coimbatore. Fresh plant material was washed under running tap water, air dried and then homogenized to fine powder and stored in airtight bottles.
5.1.1 Plant extraction procedure
10 g of air-dried powder of the plant constituents was added to distilled water [1:10] and boiled on slow heat for 2 h and centrifuged at 5000rpm for 10 mins. The supernatant was collected and the above procedure was repeated thrice. After 6 hours, the supernatant collected at an interval of every 2 hours were pooled together and concentrated to make the final volume one-fourth of the original volume [149]. It was then autoclaved at 121o C and at 15 lbs pressure and stored at 4o C. The resulted powder was collected for every individual plant. These powders in equal proportions were mixed, homogenised in distilled water [1:20] at 60 o C to form a concoction and used for the experiment.
5.2 Animals
44
with filter tops under controlled conditions of a 12 h light/12 h dark cycle, 50% humidity and 28o C. The animals were fed standard rats chow and water ad libitum. The experiment was conducted after obtaining the approval of the institutional animal ethical committee clearance (IAEC approval No: 110/PHARMA/SCRI, 2011). The composition of atherogenic diet used during the study was given in the Table 1.
Table 1: Composition of Atherogenic Diet Constituents Normal Diet
(%)
High Fat Diet (%)
Carbohydrates 67.3 57.3
Protein 22 22
Fat 5 15
Minerals 4.5 4.5
Vitamin mix 1 1
Cholesterol - 1
5.3 Experimental design
In order to induce hyperlipidemia, the method reported by Bopanna et al., was followed [2].
45
Group I (Normal Control) Normal diet
Group II (Hyperlipidemic Control) Atherogenic diet containing 1% cholesterol
Group III (Atorvastatin 10mg/kg) Atherogenic diet was given for 8 weeks to induce hyperlipidemia and treated with Atorvastatin (10mg/kg)
for 4 weeks Group IV (Decholestrate
125mg/kg)
Atherogenic diet was given for 8 weeks to induce hyperlipidemia and
treated with Decholestrate (125mg/kg) for 4 weeks
Group V (Decholestrate 250mg/kg) Atherogenic diet was given for 8 weeks to induce hyperlipidemia and
treated with Decholestrate (250mg/kg) for 4 weeks
Group VI (Decholestrate 500mg/kg)
Atherogenic diet was given for 8 weeks to induce hyperlipidemia and
treated with Decholestrate (500mg/kg) for 4 weeks
Group VII (Phytoformulation 1 250mg/kg)
Atherogenic diet was given for 8 weeks to induce hyperlipidemia and
treated with Phytoformulation 1 (250mg/kg) for 4 weeks
Group VIII (Phytoformulation 1 500mg/kg)
Atherogenic diet was given for 8 weeks to induce hyperlipidemia and
46
Bodyweight and the food intake of the animals were monitored once a week throughout the experiment. At the end of the 12th week the rats were fasted overnight and blood was drawn from retro orbital plexus and the animals were sacrificed by cervical decapitation. Serum and plasma were prepared for biochemical analysis.
Preparation of Hemolysate:
5.0 ml of anticoagulant blood was centrifuged at 3000rpm for 10 minutes to remove the plasma and the buffy coat. To the pack cells, added equal volume of 0.9% sodium chloride and washed thrice at 3000 rpm. The upper layer was discarded. To the lower layer, 2.5 ml ice cold ethanol-chloroform mixture [6.25:3.75] was added and stirred continuously in ice cold condition for 15 minutes. 0.5 ml of cold double distilled water was added and centrifuged at 3000 rpm for 10 minutes. The supernatant obtained was hemolysate.
Preparation of Liver homogenate:
47
again centrifuged at 8000 rpm for 15 minutes. The resultant supernatant was used to analyze the antioxidant levels in the liver.
Lipid Extraction:
Liver was cleared of adhering fat, weighed accurately and used for lipid extraction. Lipids were extracted from tissues as described previously by Folch et al. [150].
5.4 METHODS
5.4.1 ESTIMATION LIPID PROFILE AND BLOOD GLUCOSE
ESTIMATION OF TRIGLYCERIDES
Triglyceride was estimated by Colorimetric enzymatic method[151], [152],[153]
Principle:
Lipoprotein Lipase
Triglycerides + H2O ---> Glycerol + Fatty Acid Glycerol Kinase, Mg2+
Glycerol + ATP ---> Glycerol-3-Phosphate + ADP
GPO
Glycerol-3-Phosphate + O2 ---> Dihydroxyacetone Phosphate + H2O2
Peroxidase
48 Reagents:
Reagent 1 (Enzymes/Chromogen):
Lipoprotein lipase
Glycerol Kinase
Glycerol-3-Phosphate Oxidase
Peroxidase
4-Aminoantipyrine
ATP
1100 U/L
450 U/L
5000 U/L
350 U/L
0.7 mmol/L
0.3 mmol/L
Reagent 1A (Buffer):
Pipes buffer, pH 7.00
ADPS
Magnesium salt
50 mmol/L
0.9 mmol/L
17.8 mmol/L
Standard (Triglycerides 200mg/dL):
Glycerol (Triglycerides equivalent) 200 mg/dL
2 g/L
49 Reagent Reconstitution:
Allow the reagents to attain room temperature. Dissolve the contents of reagent 1 with reagent 1A and mix by gentle swirling. Let it stand for 5 minutes.
Procedure:
The samples and the reconstituted reagent were brought to the room temperature prior to use. 10 µL of standard and sample were taken in separate tubes and 1mL of reconstituted reagent was added. The contents of the tubes were mixed, incubated at 370C for 5 minutes and read at 546 nm against the reagent blank.
ESTIMATION OF TOTAL CHOLESTEROL
Cholesterol was estimated by enzymatic method. [154]
Principle:
Cholesterol Esterase
Cholesterol Ester + H2O ---> Cholesterol + Fatty Acids Cholesterol Oxidase
Cholesterol + O2 ---> Cholest-4-en-3-one + H2O2 Peroxidase
50
The concentration of cholesterol in the sample is directly proportional to the intensity of the red complex (Red Quinone) which is measured at 500 nm.
Reagents:
Reagent 1 (Enzymes/Chromogen):
Cholesterol Esterase
Cholesterol Oxidase
Peroxidase
4-Aminoantipyrine
30 U/L
250 U/L
1000 U/L
0.5 mmol/L
Reagent 1A (Buffer):
Pipes buffer, pH 6.95
Phenol
Sodium Cholate
50 mmol/L
24 mmol/L
0.5 mmol/L
Standard (Cholesterol 200 mg/dL):
51 Reagent Reconstitution:
Allow the reagents to attain room temperature. Dissolve the contents of reagent 1 with reagent 1A and mix by gentle swirling. Let it stand for 5 minutes.
Procedure:
The samples and the reconstituted reagent were brought to the room temperature prior to use. 10 µL of standard and sample were taken in separate tubes and 1mL of reconstituted reagent was added. The contents of the tubes were mixed, incubated at 370C for 5 minutes and read at 500 nm against the reagent blank.
ESTIMATION OF HDL – CHOLESTEROL
HDL – Cholesterol was estimated by phosphotungstate method.[155] Principle:
52 Reagents
Reagent 1 (Enzymes/Chromogen):
Cholesterol Esterase
Cholesterol Oxidase
Peroxidase
4-Aminoantipyrine
30 U/L
250 U/L
1000 U/L
0.5 mmol/L
Reagent 1A (Buffer):
Pipes buffer, pH 6.95
Phenol
Sodium Cholate
50 mmol/L
24 mmol/L
0.5 mmol/L
Reagent 2 (Precipitating Reagent):
Phosphotungstic Acid
Magnesium Chloride
2.4 mmol/L
39 mmol/L
Standard (HDL Cholesterol 50 mg/dL):
53 Reagent Reconstitution:
Allow the reagents to attain room temperature. Dissolve the contents of reagent 1 into reagent 1A and mix by gentle swirling till completely dissolved. Let it stand for 5 minutes.
Procedure:
The samples, the precipitating reagent 2 and the reconstituted reagent were brought to the room temperature prior to use.
I. Precipitation
0.20 mL (200 µL) of the sample and 0.20 mL (200 µL) of the precipitating reagent 2 were dispensed into a centrifuge tube and mixed well. Centrifuge for 3500-4000 rpm for 10 minutes. The clear supernatant is separated immediately and the cholesterol content was determined.
II. HDL – Cholesterol Assay:
54
Low density lipoprotein (LDL-C) was calculated using Friedwald formula[156]:
LDL = Total Cholesterol - HDL - Triglycerides/5.0 (mg/dL)
Very low density lipoprotein (VLDL-C) was calculated as:
VLDL = TG/5.0 (mg/dL).
The atherogenic index of serum and the percentage of protection were calculated as follows:
Atherogenic index (AI) = log (TG/HDL-C)
AI of Hyperlipidemic control-AI of treated group
Protection (%) = --- x 100
AI of Hyperlipidemic control
The cholesterol ratio is determined as: Total Cholesterol/HDL
The atherogenic coefficient and cardiac risk ratio were calculated as follows:
Atherogenic coefficient (AC) = (Total Cholesterol- HDL) / HDL
55 ESTIMATION OF GLUCOSE
Estimation of blood glucose was done by Glucose oxidase/peroxidase (GOD/POD) method. [157]
Principle:
Glucose is oxidized by glucose oxidase (GOD) into gluconic acid and hydrogen peroxide. Hydrogen peroxide in presence of peroxidase (POD) oxidizes the chromogen 4-aminoantipyrine to a red coloured compound; the intensity of the red coloured compound is proportional to the glucose concentration and is measured at 505 nm.
Reagent 1 (buffer/enzymes/chromogen):
Phosphate buffer 95 mmol/L
4-aminoantipyrine 0.2 mmol/L
p-hydroxy benzoic acid 5.9 mmol/L
Glucose oxidase 5000 U/L
Peroxidase 5000 U/L
Standard (Glucose 100 mg/dL):
56 Procedure
The samples and the reagent were brought to the room temperature prior to use. 10 µL of standard and sample were taken in separate tubes and 1mL of reagent was added. The contents of the tubes were mixed, incubated at 370C for 15 minutes and read at 505 nm against the reagent blank.
5.4.2 ESTIMATION OF ANTIOXIDANTS
ASSAY OF SUPEROXIDE DISMUTASE
The assay of superoxide dismutase is devised on the method followed by Mustafa et al., 2007[158].
Principle
Pyrogallol autooxidises rapidly in aqueous or alkaline medium solution and this has been employed for the estimation of superoxide dismutase. SOD inhibits the auto oxidation of pyrogallol. This principle was employed in a rapid and convenient method for the determination of the enzyme concentration
Reagents
1. Absolute ethanol 2. Chloroform
57
To 1 ml of the sample, 0.25 ml of absolute ethanol and 0.15 ml of chloroform were added. After 15 min of shaking in a mechanical shaker, the suspension was centrifuged and the supernatant obtained constituted the enzyme extract. The reaction mixture (control) for auto-oxidation
consisted of 2ml of 0.1M Tris-HCl buffer, 0.5ml of 2mM pyrogallol and 1.5ml of water. Initially the rate of auto-oxidation of pyrogallol was noted
at an interval of 1 min for 3 mins. The assay mixture for the enzyme contained 2ml of 0.1M Tris-HCl buffer, 0.5ml of pyrogallol, aliquots of the
enzyme preparation and water to make up 4 ml. The rate of inhibition for pyrogallol auto-oxidation after the addition of the enzyme was noted at an
interval of 1 min for 3 mins at 420 nm. The enzyme activity was expressed in terms of units/min/mg protein or units/min/ml of serum.
Calculations
Absorbance reading of control - A Absorbance reading of sample - B
Units of SOD/4 ml of assay mixture = [(A-B) / (A×50)] ×100. Unit x 10 = Units/ml of serum.
ASSAY OF LIPID PEROXIDATION
58 Principle
Malondialdehyde (MDA) formed from the breakdown of polyunsaturated fatty acids serves as a convenient index for the determination of the extent of peroxidation reaction. MDA, a product of lipid peroxidation reacts with TBA (thiobarbituric acid) to give a pink coloured product having absorption maxima at 532nm.
Reagents
1. 20% Tricholoro acetic acid 2. Sodiun dodecyl sulphate 3. Thiobarbituric acid 0.1 M
4. N- butanol – pyridine mixture (15:1)
Lipid peroxidation in the liver homogenate was determined by measuring the amounts of malondialdehyde produced. To 0.2 ml of tissue homogenate, 1.5 ml of 20% acetic acid, 0.2 ml of sodium dodecyl sulphate and 1.5 ml of thiobarbituric acid were added. The volume of the mixture was made up to 4.0 ml with distilled water and then heated at 950C in a water bath for 60 minutes. After incubation the tubes were cooled to room temperature and final volume was made to 5.0 ml. 5.0 ml n-butanol-pyridine (15:1) mixture was added and the contents were mixed
59
sample. The MDA equivalent of the samples were calculated using the extinction coefficient 1.56x105M-1cm-1.The level of lipid peroxidation was expressed as n moles of malondialdehyde (MDA)/mg protein in liver homogenate.
ASSAY OF CATALASE
Catalase activity was assayed following the method of Kaur et al., 2006[161].
Principle
The UV absorption of hydrogen peroxide can be measured at 240nm, whose absorbance decreases when degraded by the enzyme catalase. From the decrease in absorbance, the enzyme activity can be calculated.
Reagents
1. Phosphate buffer: 0.067 M (pH 7.0)
2. Hydrogen peroxide (2mM) in phosphate buffer Procedure
The tissue is homogenized with phosphate buffer at 1 to 4ºC and centrifuged at 3000 rpm for 10 minutes. Stirred the sediment with cold phosphate buffer and allowed to stand in the cold condition with occasional shaking. Repeat the extraction once or twice. The supernatants were combined and used for assay. 3ml of H2O2 phosphate buffer was taken in one cuvette, to that 0.01-0.04 ml of sample were added and read
60
phosphate buffer at 240 nm. It was noted for a decrease in the optical density from 0.450 to 0.400. From the decrease in the absorbance, the enzyme activity can be calculated. One enzyme unit was calculated as the amount of enzyme required to decrease the absorbance at 240 nm by 0.05 units.
VITAMIN C (ASCORBIC ACID)
Vitamin C was analysed by the spectrophotometric method described by Omaye et al., 1979[162]
Principle
Ascorbate is converted into dehydroascorbate on treatment with activated charcoal, which reacts with 2,4-dinitrophenyl hydrazine to form osazones. These osazones produce an orange coloured solution when dissolved in sulphuric acid, whose absorbance can be measured spectrophotometrically at 540nm.
Reagents 1. TCA (4%)
2. 2,4-dinitrophenyl hydrazine (DNPH) reagent (2%) in 9N H2SO4 3. Thiourea (10%)
4. Sulphuric acid (85%)
61 Procedure
0.5ml of plasma (or) tissue homogenate was mixed thoroughly with 1.5ml of 6% TCA and centrifuged for 10 minutes at 3500 rpm. The supernatant was treated with a pinch of activated charcoal, shaken vigorously using a cyclomixer and kept for 5 minutes. The charcoal particles were removed by centrifugation and aliquots were used for the estimation.
0.5ml of the supernatant was mixed with 0.5ml of DNPH reagent and 2 drops of 10% thiourea and allowed to stand at room temperature for 3 hrs resulting in the formation of osazone crystals. The crystals were dissolved by adding 2.5ml of 85% sulphuric acid and allowed to stand for 30 min. The absorbance was read at 530 nm. A set of standards containing 10-50 g of ascorbic acid were taken and processed similarly along with a blank to which DNPH reagent and thiourea were added after the addition of sulphuric acid. Ascorbic acid values were expressed as mg/dl in plasma and M/mg in tissue.
ESTIMATION OF VITAMIN E ( -TOCOPHEROL) Tocopherol was estimated as reported by Baker et al., 1951[163] Principle
62 Reagents
1. Standard solution: (D,L- -tocopherol, 10mg/L in absolute alcohol) 2. Ethanol
3. Petroleum ether
4. 2,2-1-dipyridylsolution 5. Ferric chloride
6. Butanol Procedure
To 0.1 ml of plasma (or) lipid extract, 0.1 ml of standard and 0.1 ml of distilled water, 1.5 ml of ethanol and 2 ml of petroleum ether were added, mixed and centrifuged at 3000 rpm for 10 minutes. The supernatant was evaporated to dryness at 80 °C. To the supernatant add 0.2 ml of 2, 1-dipyridyl solution and 0.2 ml of ferric chloride solution and mixed well. This was kept in dark for 5 mins and 2 ml of butanol was added. Then the absorbance was read at 520 nm.
Sample A520nm
63 5.4.3 ENZYMATIC ASSAYS
ASSAY OF LACTATE DEHYDROGENASE (LDH)
Level of Lactate dehydrogenase (LDH) in the serum was determined by Optimized test according to German Society of Clin Chem. [164]
Principle
Lactate dehydrogenase (LDH) is an enzyme that catalyzes the interconversion of L-lactate to pyruvate and NADH to NAD. LDH activity in the serum/plasma is directly proportional to the rate of decrease in the absorbance of NADH at 340 nm. Increased LDH activities are found in a variety of pathological conditions.
LDH
Pyruvate + NADH + H+ --- Lactate + NAD+ Reagents
Reagent 1
Phosphate buffer pH 7.5
Pyruvate
50 mmol/L
0.60 mmol/L
Reagent 2
64 NADH
Reagent reconstitution
Reagent was prepared by mixing by 4 parts of reagent 1 and 1 part of reagent 2
Procedure
20 µL (25 0C / 30 0C) of the sample was mixed with 1000 µL of reconstituted reagent, mixed well and after one minute absorbance was read at 340 nm against air (A1) and again read after 3 minutes (A2). The difference in the absorbance was calculated as A = A1- A2
Calculation:
A/min x 8095 = LDH [U/I]
QUANTITATIVE DETERMINATION OF CREATINE KINASE – MB (CK-MB)
The serum creatine kinase (CK-MB) was determined by optimized UV test[165].
65
CK-MB consists of the subunits CK-M and CK-B. Specific antibodies against CK-M inhibit the complete CK-MM activity (main part of total CK activity) and CK-M – subunit of CK-MB. Only CK-B activity is measured, which is half of the CK-MB activity.
Reagents
Reagent 1 (Buffer)
Imidazol pH 6.7
Glucose
Magnesium acetate
EDTA
100 mmol/L
20 mmol/L
10 mmol/L
2 mmol/L
Reagent 2 (Anti CK-MB) *
Anti CK-M
ADP
AMP
di-Adenosine-5-pentaphosphate
NADP
Hexokinase (HK)
2000 U/L
2 mmol/L
5 mmol/L
10 mmol/L
2 mmol/L
66 Glucose-6-phosphate dehydrogenase
N-acetylcysteine
Creatinine phosphate
1500 U/L
20 mmol/L
30 mmol/L
*
Anti CK-M sufficient to inhibit up to 2000 U/L of CK-MM.
Reagent reconstitution
One tablet of Reagent 2 was dissolved in 2.5 ml of Reagent 1. The contents were mixed gently to dissolve the contents.
Procedure
1.0 mL of the reconstituted reagent added to 40 µL of the sample, mixed well and incubated for 10 minutes at 300C. The initial absorbance of the sample (A1) was read and again read after 5 minutes (A2). The difference in the absorbance was calculated as A = A1- A2.
Calculation:
A/min x 1651 = CK-MB [U/L]
QUANTITATIVE DETERMINATION OF ASPARTATE TRANSAMINASE (AST)
67 Principle
AST
L- Aspartate + – Ketoglutarate ---> Oxaloacetate + L- Glutamate MDH
Oxaloacetate + NADH + H+ ---> L-Malate + NAD+ AST = Aspartate transaminase
MDH = Malate dehydrogenase
There is a decrease in absorption at 340 nm as NADH is converted to NAD. The rate of decrease in absorbance is measured and is proportional to AST activity in the sample.
Reagents
Reagent 1 (Enzymes)
MDH (Malate Dehydrogenase)
LDH (Lactate Dehydrogenase)
NADH
-Ketoglutarate
800 U/L
4000 U/L
> 0.20 mmol/L
> 13 mmol/L
Tris buffer, pH 7.80
L – Aspartate
88 mmol/L
68 Reagent Reconstitution
The reagents were brought to room temperature. Reagent 1 was dissolved with equal part of reagent 2 and mixed gently.
Procedure
The samples and the reconstituted reagent should be brought to room temperature prior to use. 1 mL of the reconstituted reagent was mixed with 100 µL and read immediately.
5.4.4 ASSAY OF THE ACTIVITY OF HMG COA REDUCTASE
Liver microsome preparation [167]
69 Principle [168]
HMG Co A Reductase
HMGCoA+2NADPH+2H+ Mevalonate +2NADP+ +CoASH
HMG CoA and NADPH are converted to Mevalonate and NADP respectively catalyzed by HMG CoA Reductase. Rate of oxidation of NADPH to NADP is measured at 340 nm continuously at 30 sec intervals for 5 min. Inhibition of HMGCoA Reductase decreases the rate of oxidation of NADPH.
Reagents:
1. 0.1 M Tris HCL buffer 2. HMG CoA
3. 10 mM Dithiothreitol 4. 1 mM Disodium EDTA 5. 75 mM Nacl
Procedure: [169],[170]
70
NADPH was immediately recorded at 340 nm continuously at 30 sec intervals for 5 min. Control reading was taken by omitting drug. To determine the relative oxidation of NADPH by other enzymes present in homogenate whole system excluding HMG CoA was measured. Rate of oxidation of NADPH was calculated using 6200M-1 cm-1 as an extinction coefficient.
5.5 HISTOPATHALOGICAL EXAMINATION
Liver tissue and artery were fixed in 10% neutral-buffered formalin, embedded in paraffin, and sectioned at a 5µm thickness. The sections were stained with haematoxylin-eosin for microscopic assessment.
5.6 STATISTICAL ANALYSIS
One way analysis of variance (ANOVA) followed by Dunnett’s multiple comparison test was performed using GraphPad Prism version 6.00. The limit statistical significance was set at P 0.05.
5.7 IDENTIFICATION OF THE SECONDARY METABOLITES BY GC-MS
71
compared with the spectrum of the known components stored in the NIST library. The Name, Molecular weight, Structure of the components in the test material was ascertained.
5.7.1 IDENTIFICATION OF COMPONENTS
Interpretation of mass spectrum GC-MS was conducted using the database of National Institute Standard and Technique (NIST) having more than 62,000 patterns. The spectrum of the unknown component was compared with the spectrum of the known components stored in the NIST library. The Name, Molecular weight, Structure of the components in the test material was ascertained.
5.8 IN SILICO ANALYSIS OF THE SECONDARY METABOLITES BY MOLECULAR DOCKING STUDIES
5.8.1 PROTEIN DATA BANK
72
The PDB was a key resource in areas of structural biology, such as structural genomics. Most major scientific journals, and some funding agencies, such as the NIH in the USA, now require scientists to submit their structure data to the PDB. If the contents of the PDB were thought of as primary data, then there were hundreds of derived (i.e., secondary) databases that categorize the data differently. For example, both SCOP and CATH categorize structures according to type of structure and assumed evolutionary relations.
The structure files may be viewed using one of several open source computer programs. Some other free, but not open source programs include VMD, MDL Chime, Swiss-PDB Viewer, StarBiochem (a Java-based interactive molecular viewer with integrated search of protein databank) and Sirius. The RCBS PDB website had contained an extensive list of both free and commercial molecule visualization programs and web browser plugins. The protein 1HWK was used for studying the protein ligand interactions in the present study.
5.8.2 DRUGBANK
73
nearly 4800 drug entries including >1,350 FDA-approved small molecule drugs, 123 FDA-approved biotech (protein/peptide) drugs, 71 nutraceuticals and >3,243 experimental drugs. Additionally, more than 2,500 non-redundant protein (i.e. drug target) sequences are linked to these FDA approved drug entries. Each DrugCard entry contains more than 100 data fields with half of the information being devoted to drug/chemical data and the other half devoted to drug target or protein data.
5.8.3 PUBCHEM COMPOUND