1
Assessing the impact of
the Mayhew “TheraPaws”
dog-assisted therapy
programme on older
people in care homes
Research report
July 2019
Dr Briony Jain, Prof Trish Hafford-Letchfield, Dr Carl Chandra, Sioban O’Farrell-Pearce,
Barbara Billings, Ruth Teacher, Shabeer Syed, Toby Ellmers, & Prof Carmel Clancy
2
Contents
Acknowledgements ... 3
1. Background ... 4
1.1. Mayhew and TheraPaws ... 4
1.2. Rationale for the research ... 5
2. Systematic Review of the Literature ... 7
2.1. Aims and method ... 7
2.2. Key findings ... 9
2.3. Implications ... 15
3. The Research Project ... 16
3.1. Aims ... 16
3.2. Methods ... 16
3.2.1. Setting and recruitment of research sites ... 16
3.2.2. Co-production ... 17
3.2.3. Study design and participants ... 17
3.2.4. Data analysis ... 20
3.3. Ethical considerations ... 22
4. Key Findings ... 23
4.1. Participants ... 23
4.2. Researcher observation of TheraPaws sessions ... 23
4.3. Stakeholder perspectives ... 32
4.3.1. Resident questionnaire ... 32
4.3.2. Staff focus groups ... 32
4.3.3. Volunteer focus group ... 35
4.4. Quality of life assessment ... 41
5. Implications and Conclusion ... 43
5.1. Strengths and limitations of the research ... 43
5.2. Implications for Mayhew ... 44
5.3. Implications for care homes ... 45
5.4. Implications for research ... 46
3
Acknowledgements
This work has been a research collaboration between Mayhew and Middlesex University London, Department of Mental Health and Social Work. It was made possible by funding from the University Department’s small grant funding scheme (2018/19 round) which is designed to provide support to academic staff who wish to conduct research projects and to generate and sustain research activity across the department. We hope that this is the first of many successful collaborations between Mayhew and Middlesex, and will potentially lead to further externally funded research projects and inform future partnerships.
This research was led by Dr Briony Jain, Research Fellow in Social Care and Social Policy with the Department of Mental Health and Social Work. Members of the research team included Middlesex University staff Professor Trish Hafford-Letchfield, Professor Carmel Clancy, Dr Carl Chandra, and Ms Sioban O’Farrell-Pearce, and two external research assistants Mr Shabeer Syed and Mr Toby Ellmers. The research was also supported and enhanced by the involvement of two peer-researchers sourced from the Middlesex Centre for Co-production, Ms Barbara Billings and Mrs Ruth Teacher, whom we would like to thank sincerely for their time and enthusiasm.
As the TheraPaws Programme Coordinator at Mayhew, Ms Niamh Carwood was instrumental in facilitating and co-designing this research. In saying this however, we would like to re-iterate that neither Ms Carwood or the Mayhew organisation has influenced the research findings in any way.
4
1. Background
1.1.
Mayhew and TheraPaws
Mayhew is an animal welfare organization operating predominantly in London. In addition to rescuing and rehoming animals in need, Mayhew also delivers a broad range of community-based animal care, education, and welfare programs that aim to benefit animals, their owners, and the broader community. One aspect of Mayhew’s work is the TheraPaws dog-assisted therapy programme which involves volunteers and their dogs visiting older adults in care homes. The programme promotes the potential and perceived benefits of taking animals into care settings to encourage social interaction and improve emotional and physical wellbeing among older people. The TheraPaws programme relies on volunteers, and their dogs making regular weekly or fortnightly visits usually lasting between 60 – 90 minutes (depending on the energy of the dog).
5
1.2.
Rationale for the research
In addition to Mayhew’s organisational motivations for conducting this research, the findings of such research have potentially far-reaching benefits for a range of stakeholders locally, nationally and internationally.
The world’s population is ageing rapidly, and it is anticipated that by the year 2050, older adults aged 60 years and over will make up approximately 25% of the national population in many countries around the world (World Health Organization, 2015). This is likely to place a greater demand on aged care services in the future, not just in terms of aged care places and care staff, but importantly in the quality of care provided and the quality of life for residents.
In the UK, it is estimated that more than 400,000 older people currently live in care homes and this is
set to increase with an ageing population (Office of National Statistics [ONS], 2014). Older adults living in care homes are a potentially vulnerable population who can be at increased risk of social isolation, loneliness, and depression (Victor, 2012, Stewart et al., 2014). They are often experiencing major life changes including personal loss (i.e. loss of spouse or loss of independence), and may be impacted by multiple comorbidities, including physical and cognitive decline (Gordon et al., 2014). For many residents in care homes, there are a range of issues that impact on their quality of life;
specifically, the need for meaningful activities which facilitate engagement, interaction and a sense
of wellbeing through person-centred care (Help the Aged, 2007). Increased activity and engagement
has been shown to have a positive effect on quality of life and contribute to other important
outcomes including mortality rates (Bath and Deeg, 2005). Given some of the challenges in funding long-term care (Davies, 2018), creativity in how older people are engaged is often required to make the best of available resources. As such, there is significant value in finding community-based interventions that are low cost and compliment traditional care relationships and settings.
6 2013, Allen et al., 2002). AAT has been reported to exert a wide range of benefits on wellbeing (Bernabei et al., 2013) including improving psychosocial functioning (Allen et al., 2002). Some studies have also highlighted the benefits of AAT for carers in that it can help to reduce stress, depression, and compassion fatigue commonly experienced by carers of people with dementia (Coleman, 2016, Islam et al., 2017, Zimmerman et al., 2005).
Dog-assisted therapy (DAT) is one of the most common forms of AAT, mainly due to dogs’ well-established emotional connections with human beings and receptiveness to behavioural training
(Wells, 2009). Despite its popularity and widespread use, the empirical evidence-base on the impact
of DAT for older people in care homes is relatively limited, as will be further discussed in the next
7
2. Systematic Review of the Literature
2.1.
Aims and method
Before conducting our study of the Mayhew TheraPaws program, it was important to establish what is currently known about other DAT programmes around the world. The purpose of this in the context of the broader research project was twofold: 1.) to inform the design of the current study; and 2.) to be able to then situate the findings of this research and the TheraPaws programme in the context of the existing international literature. Between May 2018 and May 2019, the research team conducted a systematic search of academic literature databases to identify original research articles that had been published on the topic of DAT for older people in care homes (Jain et al., 2019) (in review). A summary of the methods and results of the review is presented here.
In particular, we aimed to (1) describe the study methods and outcome measures that have been used to measure the impact of DAT among older people in care homes; (2) synthesize the reported benefits of DAT among older people in care homes; and (3) assess the quality of existing empirical evidence on DAT for older people in care homes.
8
9
2.2.
Key findings
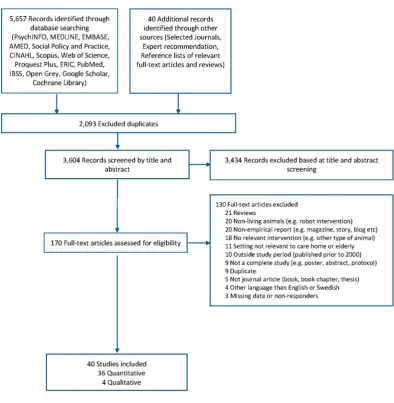
The search identified 36 studies using quantitative methods of data collection and analysis and just four qualitative research studies. The majority of quantitative studies (n=25, 69.4%) were assessed as low-quality according to the MMAT criteria (Table 1). Hence, this review identified a lack of high-quality empirical research on DAT in care homes internationally, and very few qualitative studies that explored the experiences of older people themselves.
In terms of the design and delivery of DAT programs, interventions typically involved weekly 30-90-minute visits from a small-to medium-sized dog led by a handler for a period of 13 weeks.
Almost half (47%) of the quantitative studies did not find any significant changes over time, or differences between groups of care home residents who had or had not been exposed to DAT.
The other nineteen quantitative studies (53%) produced statistically significant findings on a range of benefits of DAT for care home residents. The most salient intervention effects included improved social functioning (n=9), reduced depressive symptoms (n=5), and reduced loneliness (n=5).
10
Table 1: Quality assessment of included articles
First Author Study design Sampling Representativeness Comparisons
Data
Completeness Total score
Quality Assessment (Low=<3; good=3+)
Bernstein 2000 1. Descriptive 0 0 1 0 1 Low
Hall 2000 1. Descriptive 1 0 1 1 3 Good
Karefjard 2018 1. Descriptive 0 1 1 1 3 Good
Kawamura, 2007 1. Descriptive 0 0 1 1 2 Low
Marx 2010 1. Descriptive 0 0 1 0 1 Low
McCabe 2002 1. Descriptive 0 0 1 1 2 Low
Mossello 2011 1. Descriptive 0 0 1 1 2 Low
Motomura 2004 1. Descriptive 0 0 0 0 0 Low
Nordgren 2014a 1. Descriptive 0 0 1 1 2 Low
Nordgren 2014c 1. Descriptive 1 1 1 0 3 Good
Phelps 2008 1. Descriptive 0 0 1 1 2 Low
Prosser 2008 1. Descriptive 0 0 1 1 2 Low
Richeson 2003a 1. Descriptive 0 0 1 1 2 Low
Sellers 2006 1. Descriptive 0 0 1 1 2 Low
Tournier 2017 1. Descriptive 0 0 1 0 1 Low
Vrbanac 2013 1. Descriptive 0 0 1 1 2 Low
First Author Study design Sampling Representativeness Comparisons
Data
Completeness Total score
Quality Assessment (Low=<3; good=3+)
Berry 2012 2. Non-randomised 0 1 1 0 2 Low
Kanamori 2001 2. Non-randomised 0 1 1 0 2 Low
Kramer 2009 2. Non-randomised 0 0 1 1 2 Low
Majic 2013 2. Non-randomised 0 1 1 1 3 Good
Moretti 2011 2. Non-randomised 0 1 1 1 3 Good
11 First Author Study design Randomisation
Allocation Concealment
Blinding Participant
Blinding Researcher
Data
Completeness Drop-Out Total score
Quality Assessment (Low=<3; good=3+)
Banks 2002 3. RCT 0 0 0 0 0 0 0 Low
Banks 2005 3. RCT 0 0 0 0 1 1 2 Low
Banks 2008 3. RCT 0 0 0 0 1 1 2 Low
Barak 2001 3. RCT 0 0 0 0 1 1 2 Low
Bono 2015 3. RCT 1 1 0 0 0 0 2 Low
Friedmann 2015 3. RCT 1 0 0 0 1 1 3 Good
LeRoux 2009 3. RCT 0 0 0 0 1 1 2 Low
Lutwack-Bloom 2005 3. RCT 0 0 1 1 1 1 4 Good
Olsen 2016b 3. RCT 1 0 0 0 1 1 3 Good
Olsen 2016c 3. RCT 0 0 0 0 0 0 0 Low
Sollami 2017 3. RCT 0 0 0 0 1 1 2 Low
Thodberg 2016a 3. RCT 1 0 0 0 1 1 3 Good
Thodberg 2016b 3. RCT 1 0 0 0 1 1 3 Good
Travers 2013 3. RCT 1 0 0 0 1 0 2 Low
12
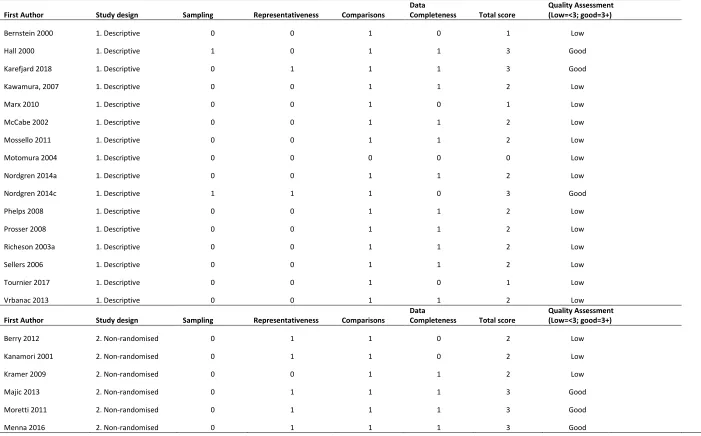
Table 2: Selected characteristics of studies on DAT in care homes
Source Design Country Main Health Problem N
Mean age, years (SD) No. Females (%) DAT Intervention, duration No. of weekly visits/No. weeks Comparator intervention Primary outcome
(Ascertainment type)c Main Findings
Travers, 2013 RCT Australia Dementia 55 84.9 (6.1) 43 (78.2)
GDAT, 40-50
min 2-3/11
Psychosocial group
Mood, quality of life & psychosocial functioning (CI)
No significant differences between groups across outcomes
Thodberg,
2016a RCT Denmark
Dementia/physical
health issues 100 85.5 (NR) 69 (69.0) IDAT, 10 min
1 (bi-weekly)/6
Toy cat & Robot seal
Behavioural/social engagement (AVR)
Significantly improved interaction during intervention compared to controls Thodberg,
2016bb RCT Denmark
Dementia/physical
health issues 101 85.5 (NR) 69 (68.3) IDAT, 10 min 2/6
Toy cat & Robot seal
Sleep, depression & cognitive capacity (CI)
No significant differences between groups across outcomes
Bono, 2015 RCT Italy Minor/mild AD 24 82.1 (6.2) 8 (33.3) IDAT, 60 min 1/32 TAU Cognitive function (CI)
Significantly improved ADAS, Cornell and Barthel index scores post-intervention compared to controls
Sollami, 2017 RCT Italy
Mild cognitive
impairment 28 NR NR IDAT, 60 min 2/16 TAU
Depression, anxiety & loneliness (SR)
Significantly improved depression and cognitive scores post-intervention compared to controls
Olsen, 2016b RCT Norway Dementia 58 84.2 (NR) 32 (55.2) GDAT, 30 min 2/12 TAU
Depression & agitation (RI)
Significantly improved CSDD scores post-intervention compared to controls
Olsen, 2016cb RCT Norway
Dementia/physical
health issues 49 84.8 (NR) 26 (53.1) GDAT, 30 min 2/12
GDAT at day centre
Social engagement (AVR)
Significantly improved POMS post-intervention compared to controls
LeRoux, 2009 RCT
South
Africa Physical health issues 16 NR 8 (50) GDAT, 30 min 3/6 TAU
Depression & anxiety
(SR) No significant differences across outcomes.
Banks, 2002 RCT USA Physical health issues 45 NR 36 (80) IDAT, 30 min 1-3/6
Intensive IDAT
& TAU Loneliness (SR)
Significantly reduced loneliness scores post-intervention compared to TAU
Banks, 2005 RCT USA Cognitive dysfunctions 33 80 (NR) 19 (57.6) IDAT, 30 min 1/6 GDAT Loneliness (SR)
No significant differences between groups across outcomes
Banks, 2008 RCT USA
No history of
dementia 38 NR NR
IDAT & IDAT + Robot dog, 30
min 1/8 TAU Loneliness (SR)
Significantly reduced loneliness scores post-intervention compared to TAU
Barak, 2001 RCT USA Chronic schizophrenia 20 79.1 (7.4) 14 (70) GDAT, 180 min 1/52
Psychosocial
group Social adaptiveness (CI)
Significantly improved SAFE Scores (i.e. social functioning) post-intervention compared to controls Friedmann,
2015 RCT USA
Dementia/physical
health issues 40 80.7 (9.1) 29 (72.5) IDAT, 60-90 min 2/12
Psychosocial group
Biopsychosocial functioning (O)
Significantly improved depression scores post-intervention relative to the controls.
Lutwack-Bloom, 2005 RCT USA NR 68 69.9 (NR) 40 (58.8)
GDAT, 15-20
min 3/24 TAU Depression & anxiety No significant differences across outcomes.
Majic, 2013 QE Germany Dementia 54 81.7 (9.4) 38 (70.4) IDAT, 45 min 1/10 TAU
Depression &
agitation/aggression (RI)
No significant differences between groups across outcomes
Berry, 2012 QE Italy
Dementia/physical
health issues 19 85.0 (NR) 13 (68.4)
IDAT + Physical
therapy, 60 min 2/20 TAU Quality of life (AVR)
No significant differences between groups across outcomes
Menna, 2016 QE Italy Mild/moderate AD 50 75.0 (6.0) 37 (74)
IDAT+ ROT
therapy, 45 min 1/36 TAU
Depression & cognitive function (RI)
Significantly improved GDS and MMSE scores post-intervention compared to controls
Moretti, 2011 QE Italy Dementia/depression 21 84.7 (9.9) 20 (95.2) IDAT, 90 min 4/6 TAU
Cognitive function, mood & quality of life
(RI) No significant differences across outcomes Kanamori,
2001 QE Japan Dementia 27 79.4 (6.1) NR IDAT
1
(bi-weekly)/6 TAU
Cognitive function &
13
Hall, 2000 QE USA
Multiple psychiatric
conditions 10 NR NR GDAT, 90 min 7/2 TAU Social interaction (O) Between-group differences not compared
Kramer, 2009 QE USA Dementia 8 NR 8 (100) IDAT 1/3
Dog handler only & Robot
dog Social interaction (AVR) No significant differences across outcomes
Marx, 2010 QE USA Dementia 56 87.0 (NR) 44 (78.6) IDAT, 3-15min 1/1
Different dog-related activities
Intervention engagement
Significantly less time spent engaging with a small dog and the colouring activity relative to the puppy video and medium/large sized dogs
Prosser, 2008 PP Australia Physical health issues 18 85.1 (10.1) 16 (88.9) GDAT, 90 min 1/6 N/A Depression (SR)
No significant differences between groups across outcomes
Vrbanac,
2013 PP Croatia NR 21 80.5 (6.6) 17 (80.9) GDAT, 90 min 3/24 N/A Loneliness (SR)
Significantly improved loneliness scores compared to baseline
Mossello,
2011 PP Italy
Severe cognitive
impairments 10 79 (6.0) 4 (40.0) GDAT, 100 min 3/3 Plush dog
Depression, anxiety &
cognitive function (O) Significantly reduced anxiety compared to baseline Kawamura,
2007 PP Japan Dementia 10 Range: 75-95 9 (90) IDAT, 120 min 1-2/52 N/A
Cognitive & social functioning (O)
No significant differences across outcomes at 12-month follow-up
Motomura,
2004 PP Japan AD 8 84.8 (7.0) 8 (100) GDAT, 60 min 4/1 N/A
Depression & cognitive function (RI)
No significant differences between groups across outcomes
Karefjard,
2018 PP Sweden
Alcohol
related-dementia 59 Range: 61-82 34 (57.6) IDAT 1-2/10 N/A Quality of life (CI)
Significantly improved quality of life scores compared to baseline
Nordgren,
2014a PP Sweden Dementia 20 Range: 58-88 12 (60.0) IDAT, 45-60 min 1/10 N/A Quality of life (CI)
Significantly improved quality of life compared to baseline
Nordgren,
2014b PP Sweden Dementia 33 81 (NR) 12 (36.4) IDAT, 45-60 min 1-2/26 TAU Cognitive function (NR)
No significant differences between groups across outcomes
Tournier,
2017 PP Switzerland Dementia 11 82.9 (NR) 10 (90.9) IDAT, 60 min 1/20 N/A Cognitive function (O)
No significant differences between groups across outcomes
Bernstein,
2000 PP USA Socially isolated 33 Range: 70-80 29 (87.9)
IDAT + activities,
60-120 min 1/10 N/A Social stimulation (O)
Significantly improved social interaction during visits compared to controls
McCabe,
2002 PP USA Dementia 22 83.7 (NR) 15 (68.2) FDAT, 24 hours 7/4 N/A Problem behaviours (O)
Significantly reduced problem behaviours during day time compared to baseline
Phelps, 2008 PP USA Elderly residents 5 84.2 (NR) 3 (60.0) IDAT, 5-10 1/6 N/A
Depression & social interaction (SR)
No significant differences between groups across outcomes
Richeson,
2003 PP USA Dementia 15 86.8 (NR) 14 (93.3) GDAT 5/9 TAU
Cognitive function, agitation & social interaction (O)
Significantly reduced agitation scores and improved social interaction compared to baseline
Sellers, 2006 PP USA Dementia 4 87.0 (NR) 3 (75.0) IDAT, 15 min 5/5 N/A
Social interaction & agitation (AVR)
Significantly reduced agitation scores and improved social interaction compared to baseline
Abbreviations: AD=Alzheimer's Disease, PP=Pre-Post design, QE=Quasi-Experimental design, RCT= Randomised Controlled Trial, IDAT= Individual Dog Assisted Intervention, GDAT=Group sessions of Dog Assisted Intervention, TAU=Treatment as Usual (care home only), NR= Not Reported, SR=Self-Report, CI=Clinical Interview, RI=Researcher interview, O=Observation, AVR=Audio Visual Recordings, N/A=Not applicable.
a=Studies are sorted by study design and alphabetically by country. b= Study linked to Thodberg, 2016a and Olsen, 2016b, respectively.
15
2.3.
Implications
The results of this review indicate there is potential for older adults to benefit from the provision of DAT in care homes, yet the full extent of such benefits remains to be determined. The findings support the development of a standardized format for designing, implementing, and evaluating DAT in care homes, which would promote stakeholder inclusion and consistent methodology to
determine its benefits.
16
3. The Research Project
3.1.
Aims
This research aimed to systematically assess the TheraPaws dog-assisted therapy programme with respect to its impact on key stakeholders including care home residents, the care home organization, TheraPaws volunteers and their dogs. The specific research questions to be addressed included:
What are the immediate and short-term impacts of the Therapaws programme on care home residents overall wellbeing and quality of life?
What are the experiences of residents, volunteers, and their dogs of participating in the programme, and what are the perceived benefits and adverse effects of the TheraPaws programme from an individual perspective?
What are the experiences of care home staff of having TheraPaws visits in their places of work, and what are the perceived benefits and adverse effects of the TheraPaws programme on care home staff and management from an organizational perspective?
3.2.
Methods
3.2.1.
Setting and recruitment of research sites
This research involved the assessment of a single dog-assisted therapy programme (TheraPaws) operated by a mid-sized animal welfare organisation (Mayhew) at four participating care home sites in inner London (one of which was a mixed provider with a supported housing unit).
Selected care homes that were either already receiving regular TheraPaws visits (x2) or were interested in starting the programme in their homes (x2) were approached by the Mayhew
17
3.2.2.
Co-production
This research was co-designed with Mayhew and the participating care homes. Between June and August 2018, several meetings were held between the lead researcher, the TheraPaws Programme Coordinator, and a representative from the care home that was being invited to participate in the research. The purpose of this was to design a study that could feasibly be conducted in each of the care homes, taking into account the difference in resident cohorts and physical design of the buildings, which would enable the TheraPaws visits to operate as normally as possible while researcher observation took place, and to be as minimally disruptive and burdensome to the care home management and staff as possible. Several options for recruitment and data collection procedures were proposed and discussed with each of the care homes, and an approach that met the needs of all stakeholders was agreed upon and written up as part of the ethics application for this project.
3.2.3.
Study design and participants
This research employed a mixed-method study design comprising four different methods of data collection described in detail below. All residents at each care home were invited to participate in the research regardless of their physical or cognitive abilities, or desire to participate in the DAT sessions.
1. Overt, naturalistic researcher observation during TheraPaws sessions with residents
18 based on the Social Behaviour Observation Checklist developed by Sellers (2006), and the Animal Assisted Therapy Flow Sheet developed by Richeson (2003). Observations included watching residents reactions during the session, listening to their conversations about the dogs, and behaviours towards dog and volunteer (Sellers, 2006). This included notes on whether the resident looked at dog, touched dog, spoke to dog, remembered and used dog’s name, engaged in activity with dog, reminisced about own dog, looked at dog handler, spoke to handler, and remembered handler’s name (Richeson, 2003).
2. Brief questionnaire of residents experience and satisfaction with dog-assisted therapy
visits
At the end of the 12 week observation period, all residents were administered with a brief questionnaire (adapted from Phelps et al. (2008)) to assess their level of participation and satisfaction with the weekly DAT sessions. The one-page questionnaire was completed by residents themselves (if possible/preferred) or with the assistance of care staff, family members or research staff where the questions were read out to residents and their spoken answers recorded.
3. Focus groups conducted with TheraPaws volunteers and care home staff.
Focus groups were conducted separately for volunteers and care home staff as each
discussion had a slightly different focus. Each focus group was conducted in a central London location, at a time and date deemed most convenient for each participant group, and lasted anywhere between 20 and 90 minutes with refreshments provided. Each session was facilitated by members of the research team, and discussions were audio-recorded and transcribed for data analysis.
a. Volunteers were initially approached by the Mayhew TheraPaws manager and invited to participate in a focus group as part of the TheraPaws research project. If they expressed interest in participating, a formal invitation was sent with a
19 and location of the focus group (27th Nov 2018, 4pm-5:30pm at the Mayhew office). During the focus group, volunteers were asked to discuss the benefits and potential adverse impacts of the programme on themselves, their dogs, and the care home residents.
b. Care home staff members were asked to participate in a focus group after liaising with the care home manager to find a suitable date and time which will be least disruptive to their work (between Dec 2018 and March 2019). The focus group included specific questions for staff about the perceived impact of the DAT
programme on each residents overall wellbeing and quality of life; and the perceived benefits and adverse effects of the TheraPaws programme on residents more generally and care home staff and management from an organizational perspective. 4. Quality of life assessments completed by the care home activities co-ordinator for each
participating resident at baseline and follow-up.
In October 2018, the activities co-ordinator of each of the four participating care homes was interviewed by the lead researcher to collect basic information about each of the
20 also taken at the time of interview. At the end of the interview, the researcher provided the activities co-ordinator with a relevant quality of life assessment form to complete using either the Older Peoples Quality of Life (OPQOL) assessment or Quality of Life in Dementia (QUALIDEM) assessment questionnaire scale depending on whether the resident had a diagnosis of dementia or not. The same form was completed again for each resident
following the conclusion of the observation period (Dec 2018) and up to 3 months follow up (March 2019).
3.2.4.
Data analysis
All researcher field notes and audio recording transcriptions from each phase of the research were collated and imported into an Excel spreadsheet or relevant data analysis software package NVIVO or SPSS. Basic descriptive analysis was conducted on pre-study interview data to measure
frequencies and proportions in resident profiles. Data from focus groups were analysed thematically to identify major and minor themes in participants responses, and researcher observation data were analysed thematically and using basic descriptive statistics to provide context to the results. Full details on the analysis techniques for each phase of the research are provided below.
Analysis of observation data
Qualitative observation data was collected in a structured way using a proforma to ensure
consistency across the different researchers conducting observations. In the analysis stage, the
analysis was guided by an inductive approach by being open to what emerged from reading it such
as recurring phenomena and any connections across the observational data set. We also tracked
key individuals through the analysis (minimum of 1 per care setting) in order to consider any case
studies where a narrative approach could be used to describe how individuals consistently observed
were impacted by the intervention. There were in total 238pages of observational data and these were analysed by 6 members of the research team manually. The process involved two people
21
any common themes about the environment in which the intervention took place; who was there,
the process of the intervention and main actions that took place. They were asked to make
immediate notes about the overall themes from the data recorded and also importantly noting any
differences or contradictions between them. This was followed by a second process of individual
labelling and coding of data that appeared to have significance or meaning. The individuals then
compared their notes and began to group and collate the coded data and interpretation in order to
identify and represent a broader theme or emerging idea. The final stage involved working together
to agree summative codes and ensuring that these were tracked through direct examples from the
text. Finally, the data was then collated across the 36 observations and discussed in a team meeting.
Analysis of focus group data
The five focus group transcripts were subject to content analysis to describe, interpret or make
sense of what the key stakeholders said about DAT interventions and in response to the topic guide
used. A similar process was followed as described in the observational data analysis through a
process of coding and developing categories and broad thematic analysis.
Quantitative analysis of Quality of Life assessment data and resident questionnaires
22 used instead. Effect sizes (an assessment of the magnitude of any differences observed between baseline and follow-up) are reported as Cohen’s d, unless the assumption of normality is violated, where effect sizes are instead reported as r (Fritz et al., 2012). According to Rosenthal and Rosnow (1984), a small effect for Cohen’s d is 0.20, where a small effect for r is 0.10; a medium effect for Cohen’s d is 0.50, where a medium effect for r is 0.30; and a large effect for Cohen’s d is 0.80, where a large effect for r is 0.50.
3.3.
Ethical considerations
23
4. Key Findings
4.1.
Participants
A total of 54 residents from four care homes participated in this study, ranging from 11 to 15 residents from each home. The majority of participants were female (n=40, 74%) and participant ages ranged from 57 to 103 years, with a mean and median of 82 years. The majority of residents had a diagnosis of dementia (n=38, 70.4%). Where severity of dementia was known (n=18), this was fairly evenly distributed across mild, moderate, and severe. The duration of residence in the care home ranged from 0.1 to 24.9 months, with a mean of 3.8 months. A total of six residents (11%) withdrew from the study before data collection was completed due to death (n=4) or moving out of the care home (n=2).
4.2.
Researcher observation of TheraPaws sessions
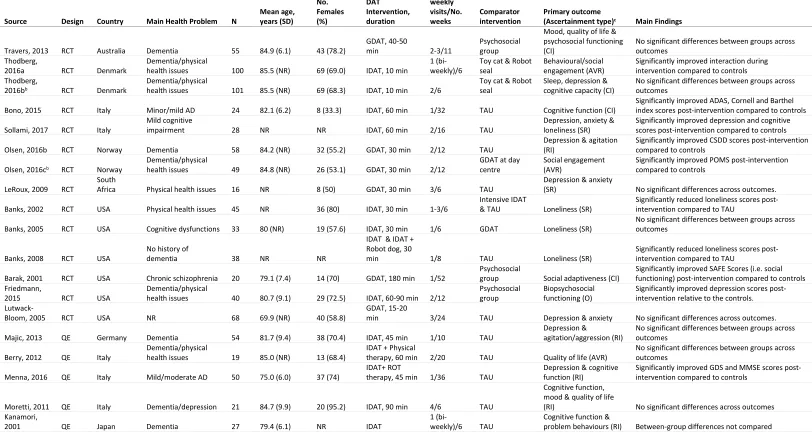
The researcher observation allowed for the collection of very rich, detailed data on what actually occurs during a typical TheraPaws visit. The analysis of this data revealed several themes relating to each of the key players in the session and the nature of interactions between them. This is illustrated in Figure 3a and 3b and explained in detail below.
Themes about impact on the resident
24 In regards to the emotional stimulation, a change in resident’s demeanour from the start of the session to the end was often observed. Some residents were noted to be in a bit of a bad mood at beginning of session, but as the session went on, they began smiling and interacting with others.
“F said once that she didn’t like the dog and threw a bag of sweets towards it. She then took
5 biscuits and fed them to the dog. She made a lot of references to her past in the session
but not addressing anyone in particular. She talked about how she liked custard creams
herself but she never had any as a child. Her stepfather hadn’t let her have any because ‘he
was a selfish bastard’. She also talked to the volunteer and the manager about how she lived
in the area and had bought a paintbrush in the local B&Q. F appeared to be in a bad mood
at times and appeared unhappy and at other times she did laugh and smile.”
Another common occurrence was resident’s recalling memories from their past lives, either about previous pets they had owned or known, places they had lived, or people they had known.
Depending on the resident’s cognitive status, the memories evoked by seeing the dog could sometimes be clear and repeated in the same way on several different occasions or were mixed in together with other memories from different time points in their lives or stories about someone else’s life.
Themes about the dog
25 their best work”. The needs of the dog included things like adjusting the room temperature, the provision of drinking water, adjusting to the number of people present, and monitoring the dog’s mood and wellbeing for the duration of the session.
Themes about the volunteer
Each of the volunteers observed in this study exhibited a clearly compassionate nature and
personality. In addition to this, the volunteers demonstrated a high level of professionalism and skill in being able to engage with the resident and enhance the experience for them while simultaneously being attuned to the needs of the dog. Examples of this include being purposefully inclusive, making several efforts to engage people who may not be consistent in their response and using light touch to communicate with people or to place the dog near enough to them to enable physical and sensory stimulus. Volunteers also demonstrated attentive listening and this was evident as the sessions cumulated in the way the volunteer recalled what a resident had told them previously which acknowledged and conveyed value in what had been shared between them. This helped to build relationships over time and gain trust and in some instances increased the opportunities for small talk and sharing more equally information about each other. There was also some light banter and humour used as the relationships developed which had a positive effect on the group as a whole.
Themes about the care staff
26 inviting them to interact rather than allowing a more naturalist evolvement of contact. This may not offer the best environment to allow residents to find their own way with how they interact and the extent to which they wish to interact with the dog. It was also unclear about how much choice is given in relation to residents participation and there were significant contrasts in some settings. For example, in one setting, residents were able to make their own way to the lounge where the visit took place and leave or move away if they wished whereas in another, more dependent residents were taken to a fairly small room, positioned in a circle until the intervention was completed and it was in this latter setting where more tensions were noted including irritability and frustration on behalf of some residents. On some occasions, residents were asleep during the session and did not interact at all.
Themes about other residents and care home environment
There were different group dynamics in each home and with each resident cohort which impacted on the TheraPaws sessions. For example, there were some situations where residents with dominant personalities or a particular affection for the dog could potentially overshadow the enjoyment of other residents through either their mood or over-involvement. There was also frequent
competition for the volunteer’s attention noted in one home which contributed to a sense of irritability/ frustration as well as mixed emotions among the residents.
“F spoke constantly during the session but usually to herself as the lounge was very noisy and
there was a lot of competition to be heard.”
27 that fewer people were able to interact with the dog on that day. It was often observed that the space used for the group sessions with dogs was not set up or prepared well for a therapeutic intervention to take place but rather more for an ad-hoc activity.
Relationship between resident and dog
The relationship between residents and the dog blossomed over the 12-week period, with some residents making closer connections than others. One of the first things that the researchers observed during the TheraPaws visits were the varying levels of interaction between residents and the dog. This ranged from no participation in the session at all, to expressions of hesitation or reservations in interacting with the dog, to residents being content to simply sit and watch the dog, to patting and feeding the dog (the most common forms of interaction), and finally to kissing and cuddling the dog. Although the latter was not the most common form of interaction, it did occur more frequently than expected.
The TheraPaws visits held different meaning for different groups of residents. While some residents didn’t really mind either way if the dog came or not, the meaning of the dog and the TheraPaws visits each week were extremely important to many of the residents in the study. These were manifest in strong emotional expressions of love and warmth directed towards the dog:
‘Lovely dog – I love her: I’m going to take her away to Jamaica’
‘Ahh doggy, I’m only talking to your girl but you’re my best friend’
There was much value in the opportunities for physical contact and showing unconditional love and attachment.
“B was in a wheelchair and flailed her head and arms about a bit during the session. When her
attention was drawn to Jessie, she really focused on touching her. She cupped her hands under
his chin to try and make eye contact with Jessie and stroked his back constantly. When she
28 in the room except Jessie. N (the volunteer) tried to speak to her but she does not have speech
and she looked at him and laughed and smiled. She appeared to really enjoy the interaction.”
For the most part however, the dog’s presence appeared to simply offer something outside normal routine and this had benefits albeit for some, these were literally in the moment.
Social interaction between resident and volunteer
The observation gave a detailed insight into how DAT can and does increase social interaction for residents. Social interaction occurred mostly between residents and volunteers, but occasionally between residents and staff, and between the residents themselves (although this was less
common). The nature of conversations between residents and volunteers covered a range of topics including but not limited to: the dog and its behaviour/care; reminiscing about the resident’s life and experiences; shared interest such as music, books, and travelling; the local community; and current affairs. Through these conversations the residents appeared to benefit from reciprocity and
exchange – where instead of simply having something done to or provided for them, they were able to give something back by passing on knowledge and giving advice – and having a regular connection to the outside world, as volunteers were often from the same local community as the home and the area where residents had lived previously.
Social interaction between resident and care staff
29 care-to-carer relationship where the resident is having something done or provided to them by the carer.
Social interaction between residents
The dog visit provoked both positive and negative interactions between the residents often related to the way in which the intervention was set up and the environmental conditions. For example, in one home the arrangement of the TheraPaws visits was modified over time, progressing from a single large group visit in the first few weeks to a series of smaller group and one-to-one sessions each week. In the first few sessions, two residents with particularly dominant personalities frequently overshadowed the session as one resident wanted to continually talk to the volunteer which caused another resident to get frustrated, telling her to ‘shut up’. However, these negative social interactions occurred less frequently in the smaller group sessions of 3-4 residents, even when these included the two dominant personalities as there was less overall competition for the
volunteers time and attention.
It was rare that residents interacted with each other one-on-one during the sessions as the focus was primarily on interacting with the dog and volunteer who were external to the home and thus a novelty. If they did, however, this was often as part of a group conversation, or an unrelated
30
Care staff
Other residents
Volunteer
[image:30.842.138.737.56.515.2]
31
+/-Themes about impact on the resident
- Sensory and emotional stimulation
- Changes in demeanor
- Reminiscence Themes about the dog
- Dog as vehicle/catalyst
- Intuitive nature
- Needs of dog
Themes about the volunteer
- Compassionate nature
- Professionalism and skill
Themes about the care staff
- Expectations of programme
- Role of staff
- Allowing residents space to find their way
Themes about other residents and care home environment
- Group dynamics
- Distractions
Relationship between resident and dog
- Levels of interaction
- Meaning for residents
Social interaction between resident and volunteer
- Nature of conversations
- Reciprocity and exchange
- Links to community
Social interactions between resident and care staff
- Opportunity to expand care relationship
- Personhood
Social interactions between residents
- Positive
[image:31.842.85.632.33.526.2]- Negative
32
4.3.
Stakeholder perspectives
4.3.1.
Resident questionnaire
Of the 54 residents across four care homes, 41 (75.9%) completed a self-report questionnaire at the end of the observation period. Almost half of the residents (n=19, 46.3%) self-reported attending 10-12 TheraPaws sessions over the 10-12-week observation period.
Overall the vast majority of residents viewed the TheraPaws sessions positively according to how much they enjoyed the sessions, how much they look forward to them, and how the sessions made them feel. On a scale from 1 to 5 regarding how much they enjoyed the session, the majority of residents (n=26, 63.4%) selected “5 - Very much”. Similarly, when asked whether they looked forward to the weekly sessions, 26 (63.4%) residents selected “5 - Very much”. Finally, when asked how the DAT sessions made them feel, most residents (n=24, 58.5%) responded with “5 – Very happy”.
In the comments section of the questionnaire, residents expressed how much they enjoy the
sessions and love the dog (n=12, 29.3%); requested more frequent sessions or for sessions to be held on a different day of the week or time of day so they could attend more often (n=7, 17%); and a few expressed their indifference as to whether the dog comes or not (n=3, 7.3%).
4.3.2.
Staff focus groups
Four small focus groups consisting of 3-4 people each were conducted at two of the participating care homes to accommodate the working schedules of participants. In total, 12 care home staff members participated in the focus groups. Qualitative analysis of transcripts from the staff focus groups identified the following three key themes.
33 One of the most frequent themes noted by the care workers was the potential offered by the visit of the dog and the volunteer to trigger and forge more diverse relationships. These were related to residents anticipation and recall of visits which served to initiate new conversations between residents and workers, relatives and workers. Residents also came to the sessions willing to share their personal experiences, history and interests which carers found were enlivened by engaging with the dog and handler. The dog also became a focal point for eliciting discussion between the residents. Residents showed curiosity about the dog in relation to details about its habits, likes and welfare. The personality of the volunteer appeared to be central to these more detailed discussions and the dynamics that followed:
“And people got to know her [volunteer] really well, you know? …and they're interested in
her holidays, and they want to know where she went, and how long she went. But what
happened to [the dog]? They're more concerned with what happened to [the dog] on their
holidays, you know? But I mean it is lovely that they actually ask them questions”. (Care
Worker FG 1b).
Carers found that the residents spoke to them more after the dog had left and also remembered the TheraPaws visit appointment in comparison to other appointments which could be forgotten.
Without exception, the carers described a positive effect on the environment overall which was important as they described challenges for residents who were resistant to the idea of group living. The visits generated a more positive atmosphere in this respect bringing residents together with a purpose that had both a group and individual effect. This lifting of mood could last hours after the dog had left. This could sometimes make it easier to carry out care tasks.
“An experience very dear to them and they want again which is why they cannot stop talking
about it.” (Care worker, FG 1b)
34 Many descriptions were given of the residents physical and emotional interactions with the dog during the visits such as holding, stroking, kissing, and holding the lead. These were particularly noted for those with sensory loss where isolation can be a factor without assertive interaction. The physicality of the dogs presence was seen to provide an opportunity to stimulate those senses that remain. Again the role of the volunteer was valuable in providing a description of the activities going on such as nuanced description of its colour.
“They like the comfort of stroking”. (Carer FG 1b)
This also included those residents who may not be overtly interested in dogs – declared themselves to be more of a cat person. These would observe from the side-lines:
“yeah they're looking every time [the dog] is moving around. You can see them following you
know, what [the dog] is doing. So it's really interrupting everyone. Because they are
following, even though the ones that might not be stroking him” (Care worker FG 1b)
Carers felt that residents were given an opportunity to express feeling of love, care, joy and to contribute physically, verbally and emotionally through words and tactile interactions.
Theme 3: Environmental influences
Some staff expressed conflict with being trained in strict hygiene policies with witnessing the
interactions between dogs and residents without intervening. They referred to people being ‘fragile’ in relation to their current health.
“Some residents, they'll come and then they'll start to kiss the dog. And then put biscuits
in their mouth and try to feed the dog like that. I don't think it's right. People might consider
it as nothing, the people can kiss their dogs but I'm thinking, yeah dog would be treated
obviously and wouldn't have any infections or diseases but-“ (Care home worker, FG A.1)
35 Carers noted that not every member of staff was comfortable around dogs and did not have to participate but this was worked around. This could be the same for residents and so to agreeing a controlled environment was important before the intervention took place. Further carers noted that older people come with a unique background which is not always tapped into in the day to day care practices and therefore this activity enabled a greater understanding of the needs of older people.
4.3.3.
Volunteer focus group
There were seven participants in the focus group conducted with volunteers (n=5 females, 2 males). All participants had been volunteering with Mayhew for at least 12 months, and all were dog owners with the exception of one participant who worked with another dog owner.
Throughout the focus group, participants were friendly, engaging and facilitative. Focus group participants acknowledged that they rarely meet up so this offered them an opportunity to describe their experiences, which they found interesting and allowed for common elements to emerge. There was a general consensus that the descriptions of the key themes presented below were ‘shared’ by the group.
Some of the themes identified throughout the focus group discussion with volunteers are reflective of the themes identified through the researcher observation. In the following sections, any common themes are presented first followed by the new or unique themes emerging from the volunteer perspective.
Themes about older people
36 sensory deficits such as blindness or deafness, or cognitive impairments (dementia) who are at increased risk of ‘isolation’. The introduction of the dogs offers ‘tactile contact’, licking, kisses, stroking of soft fur etc. It was felt that the impact of this was to increase residents sense of control and ‘engagement with the world’, and ‘feeling human’ again. Similarly, to the observation data, volunteers discussed that the dog visits offer a point of reflection and reminiscence for residents, evoking past (usually positive) memories and creating a renewed connection to their past.
Volunteers also speculated on the meaning of the dog visits for residents and suggested that it offers engagement outside of ‘self’. That is, it creates an opportunity for residents to develop relationships with the dog and the volunteer and care about something bigger than their ‘world’, providing something to look forward to each week or fortnight.
Themes about the dog
Volunteers also recognised the dog’s ability to engage with residents with significant impairments including those who were non-verbal, visually impaired, or experienced limited mobility. The volunteers were able to elaborate on this further offering the explanation that it is the dogs non-judgmental nature which allows this to happen - they do not get caught up in the ‘emotions’ attached with the circumstance of the person.
“Just for a few minutes maybe, it was a bit longer with those two occasions and the Chinese
chap didn't say a word, but he was just so full on for a while. Tess was on the bed, which
she's not normally- that was unfamiliar for her, but she really embraced- well they
embraced- she embraced the moment and they embraced her”.
37 and respond to. So that the positive rewards for the dog can be indirect and not necessarily all about the treats they receive during the session.
A second insight about the dog’s experience gained from the volunteers is the notion of love overload. The sessions can be tiring for dogs both in terms of the duration of the visit and the number of people wanting to interact with the dog. Dogs are only able to be authentic to their nature, so this work is not suitable for all dogs. The dog needs to like to receive touch, praise, and attention. The volunteer must work within the limits of the dog, be mindful of dogs state of mind (in terms of insecurities) and recognise when they have had enough. In the same vain, the dogs are very ‘tuned into emotions’ of owners and can sense when something is off if the owner is having a bad day, feeling rushed, etc. They will take cues from owners emotions rather than those of the people they are visiting.
Themes about the volunteer
Volunteers self-identified that their personal characteristics and social skills were an important factor in the sessions. Specifically, this included the ability to be compassionate; self-aware; assertive (to care for wellbeing of dog); flexible; and responsive. Volunteers discussed having a dual outlook in that they wanted to (1) be compassionate to the person they were visiting, by putting them first and not drawing attention to their own contributions; and (2) being mindful of the dog’s needs.
A major new theme emerging from the focus group was the meaning of the dogs to their owners, and the notion of family with the dog in it. Volunteers described their dogs as family members, not as an analogy but as their reality.
“Dogs are my children”
38 “Sometime people will not handle your dog in a way that is acceptable or appropriate.”
Volunteering with TheraPaws offers them an outing, and experience, and the opportunity for emotional development.
A second key theme was the impact that participating in the TheraPaws programme has for volunteers. When asked why they decided to join the programme and what motivated them to do so, many couldn’t think of a definitive reason other than it seemed like a good idea, but once they had started, they didn’t want to leave. They felt the programme enabled them to “give back” by making a difference to someone’s day, and in turn it made them feel good too. This could act as a sort of self-therapy for volunteers where the dog offers a bridge to connectivity with other human beings. The emotional experience of this could be quite powerful for volunteers, where one
participant reported that she was so overwhelmed with emotion that she cried after her first visit to a care home, but that it was a positive thing because the resident had reminded her of her late father and she was able to do something positive for that person.
“Yeah I agree with all of that completely. Because you are- you've been seeing somebody for
a year or two and they pass away, it's not easy. But the positive side is that you know you've
made a little bit of a difference in those last year or two. You can smile at the fact that, yes,
that was a friend.”
Themes about care staff
Volunteers noted that care home staff often engage with the dog and seem to enjoy the dog visits as well. It was proffered that the dogs offer ‘comfort’ and an opportunity for ‘stress reduction’ for staff who may be over worked and is a good release for them. However, this can often distract from main purpose of visit if staff are ‘too engaged’ and it disrupts the flow of the visit with residents.
39 includes patients in hospital settings, family members visiting the person in care setting, and the dog can even offer a distraction from the ‘trauma’ for children who are visiting, providing ‘carers relief’ for their parents. It is clear that the benefits of a TheraPaws visit is not only limited to older people in care homes and this provides opportunities to explore further applications of the TheraPaws program.
Themes about the nature of relationships during the intervention
Overwhelming themes relating to the nature of the relationship between the residents and the dog include: ‘bridging’; ‘connections’; ‘non-judgemental’; ‘easy/relaxed distraction from self,
circumstance, trauma, pain’. It was felt that the dog acts as a ‘bridge’ or a conduit between the inner world of the patient and the external world the dog is operating within. This provided a trigger and anchor for communication exchange or enabling connections that might otherwise be difficult.
"Oh, I should just pull back" in the moment? Because there's something intimate happening
between the dog and the person”
The participants used florid and expressive language to describe the nature of the interactions between dogs and residents and the impact this had on residents. This centred on words such as ‘lights up’; ‘joy’; the patient/client ‘blossoms’; and ‘giving back’. Finally, the dog can offer a sense of fun and light relief in the face of some very serious personal circumstances for residents.
Challenges experienced by volunteers
40 1. ‘Overheating’ due to the nature of the venues the room temperature is kept purposely high
– this can lead to the dog becoming dehydrated, listless, owners off set this by taking water with them;
2. Food – in general dogs are food orientated so would scavenge; seek out ‘treats’; this can pose handling challenges in situ – particularly when patients/residents seek to reward the dogs with treats – biscuits, chocolate etc – this requires handlers to have a keen eye – to ensure the welfare of the dog is protected;
3. Food smells – similar to previous point – particularly if the visiting rooms are adjacent to kitchens etc;
4. Accessibility – dependent on mobility of residents/patients – some are in beds –(dogs can’t climb onto beds either not permitted or dog is too heavy to jump up);
5. Hospital equipment can get in the way – tubes; machines etc – need to navigate or ensure dog welfare;
6. Patients/clients/their carers or visitors sensitive to allergies – hence dog cannot or prevented from engaging
7. Background noises – particularly TVs
8. Smoking cigarettes – making environment unpleasant for both dog and handler
9. Transporting dog to venue – if the dog ‘walks’ this can result in dog arriving tired and limiting interactions due to the dog being tired.
41
4.4.
Quality of life assessment
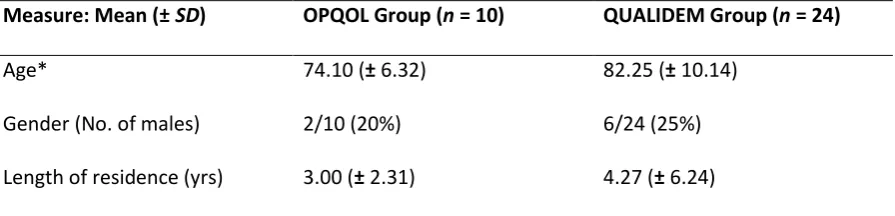
Of the 34 participants for whom both baseline and follow-up quality of life assessments were completed, 24 were diagnosed with dementia and were thus assessed via the QUALIDEM. The remaining 10 participants completed the OPQOL-Brief. Gender ratios for the two groups were largely comparable (males =25% for QUALIDEM and 20% for OPQOL), and the duration of residence
[image:41.595.76.524.350.458.2]between the two groups was statistically comparable (U = 96, Z = -0.38, p = .703, r = 0.07). A key difference is that the OPQOL group (those without a diagnosis of dementia) were significantly younger than the QUALIDEM group (t(32) = 2.35, p = .025, d = 0.97). Demographic data for the two participant groups are reported in Table 3.
Table 3: Demographic data for the OPQOL and QUALIDEM participant groups
Measure: Mean (± SD) OPQOL Group (n = 10) QUALIDEM Group (n = 24)
Age* 74.10 (± 6.32) 82.25 (± 10.14)
Gender (No. of males) 2/10 (20%) 6/24 (25%)
Length of residence (yrs) 3.00 (± 2.31) 4.27 (± 6.24)
Note: Mean refers to the average value for that variable across the group as a whole; whereas standard
deviation, or SD, refers to the level of variance (i.e., the degree to which the individual values within that group deviate from the mean score).
* p < .05 when the two groups were significantly compared for this particular variable.
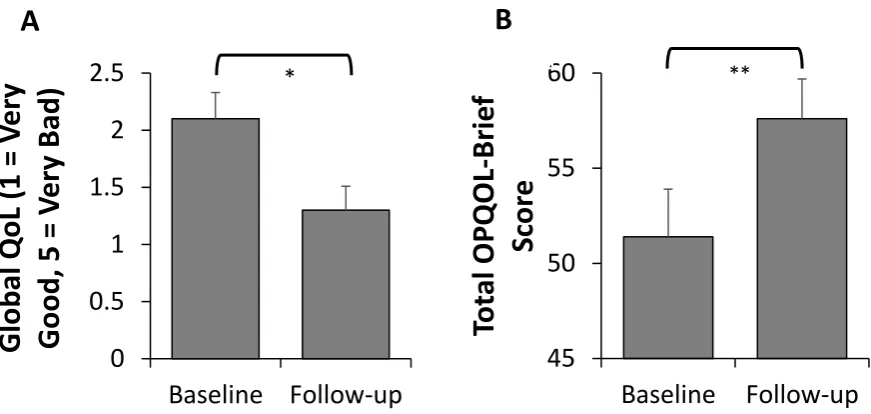
OPQOL Group
As illustrated in Figure 4A, there was a significant improvement in Global QoL scores at follow-up (M = 1.30, SD = 0.68), compared to baseline (M = 2.10, SD = 0.74), Z = -2.53, p = .011, r = 0.80).
42 Figure 4A: Change in Global QoL scores from Baseline to Follow-up (mean ± standard error), *p<0.05. Note: Lower scores reflect better quality of life.
Figure 4B: Change in Total OPQOL-Brief scores from Baseline to Follow-up (mean ± standard error), *p<0.01. Note: Higher scores reflect better overall quality of life.
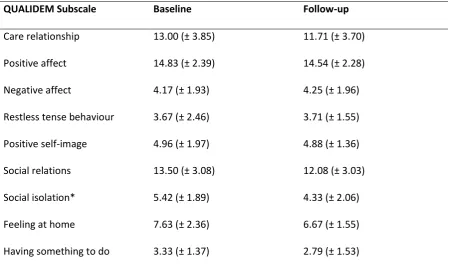
QUALIDEM Group
There was a lack of significant change from baseline to follow-up for the majority of subscales assessed in the QUALIDEM, including: care relationship (t(23) = 1.63, p = .118, d = 0.34); positive affect (Z = -0.85, p = .397, r = 0.17); negative affect (Z = -0.51, p = .612, r = 0.10); restless tense behavior (Z = -0.15, p = .878, r = 0.30); positive self-image (t(23) = 0.19, p = .849, d = 0.05); social relations (Z = -1.91, p = .056, r = 0.39); and feeling at home (t(23) = 1.70, p = .102, d = 0.48). There was, however, a significant worsening in the social isolation subscale at follow-up compared to Baseline (t(23) = 2.39, p = .026, d = 0.48). However, with the absence of a matched control-group (e.g., a group diagnosed with dementia who did not participate in the TheraPaws programme), it is difficult to accurately assess the impact of the TheraPaws Programme on quality of life in those diagnosed with dementia. For example, Hoe et al. (2009) reported declines in QoL over a 5-month period for people with dementia living in care homes. Consequently, it is entirely plausible that a general absence of significant negative change observed at follow-up in the present research represents a positive outcome. These data are reported in Table 4.
0
0.5
1
1.5
2
2.5
Baseline Follow-up
Glo
b
al
Q
oL (
1
=
V
er
y
Go
o
d
, 5
=
V
er
y Ba
d
)
*
45
50
55
60
Baseline
Follow-up
To
tal
OPQOL
-Bri
ef
Sc
o
re
*
**43 Table 4: Mean (± SD) values for the QUALIDEM subscales
QUALIDEM Subscale Baseline Follow-up
Care relationship 13.00 (± 3.85) 11.71 (± 3.70)
Positive affect 14.83 (± 2.39) 14.54 (± 2.28)
Negative affect 4.17 (± 1.93) 4.25 (± 1.96)
Restless tense behaviour 3.67 (± 2.46) 3.71 (± 1.55)
Positive self-image 4.96 (± 1.97) 4.88 (± 1.36)
Social relations 13.50 (± 3.08) 12.08 (± 3.03)
Social isolation* 5.42 (± 1.89) 4.33 (± 2.06)
Feeling at home 7.63 (± 2.36) 6.67 (± 1.55)
Having something to do 3.33 (± 1.37) 2.79 (± 1.53)
Note: Higher scores indicate higher quality of life (even for “negative subscales”, e.g., social isolation”). * indicates significant finding of p < .05
5. Implications and Conclusion
5.1.
Strengths and limitations of the research
One of the major strengths of this research is its comprehensiveness in using objective measures to assess the impact of DAT and the inclusion of the resident, volunteer, and care home staff
perspectives. The qualitative methods employed in this study addressed an identified gap in the literature (Jain et al, in review). Further strengths of the research include the multiple research sites, and the double up of researcher observers at each of the sites throughout the study period.
Limitations arose from the need to be flexible with the care homes, and the volunteers, in that the researchers had less control of dates and times of visits, who was present at each session, and where the sessions were held. However, this did allow for a truly naturalistic observation study.
44 dementia diagnosis (OPQOL). The data collection for this was reliant on care home staff reading the user guides carefully and completing the assessments in an accurate, timely, and consistent manner, which could not necessarily be guaranteed by the research team. A more reliable method may have been for the researchers to seek permission to access to the residents’ care files for the previous two-week period and complete the assessment forms based on this. However, this approach would have been subject to incomplete data.
5.2.
Implications for Mayhew
This research provides the empirical evidence to support the long-held beliefs and anecdotal evidence of the benefits of the TheraPaws programme. Specifically, the research has shown that TheraPaws visits in care homes do indeed contribute to:
- Increased social interaction; - Companionship with the dog; - Unlocking memories;
- Building relationships between resident and volunteer;
- Improved communication between resident and care home staff; and
- Improved overall quality of life among people without a diagnosis of dementia
The research findings also indicate that the TheraPaws programme is highly valued not only by the residents, but also by the volunteers, and care home staff and management.
45 the programme as any changes and improvements would need to be consulted on through different voices and expectations.
5.3.
Implications for care homes
46
5.4.
Implications for research
The findings of this research support previous findings regarding the impact of dog assisted therapy on increasing social interaction (Bernstein et al., 2000, Berry et al., 2012, Thodberg et al., 2016a, Thodberg et al., 2016b) and improving social functioning among care home residents (Sellers, 2006). The research evidence on the impact of dog assisted therapy on overall quality of life remains mixed, in that an increase in quality of life was only detected among residents without a diagnosis of
dementia, despite the researchers observations that residents with dementia were among those to benefit most from the dog visits “in the moment”. Further methodological research on how to best measure quality of life in care home residents may be warranted.