Children’s Social Care Innovation Programme Evaluation Report 56
Safe Families for
Children
Evaluation report
July 2017
Michael Little, Georgina Warner and
Vicky Baker – Dartington Social
2
Contents
List of figures 4
List of tables 5
Acknowledgements 6
Executive Summary 7
Findings 9
Lessons learned for stakeholders 10
Learning for Safe Families 11
Learning for Local Authorities 11
Learning for Government 11
Learning for Research 12
Recommendations 12
Aims 15
Background 16
Legal, Administrative and Fiscal Context 17
The Innovation Process 19
Five Innovations 20
Methodology 23
Findings 26
Local Authority Take Up of Safe Families 26
The Five Innovations 28
Scale 28
Just in Time 29
Reaching Category 2 Cases 30
PSP 32
The System Dynamics Seminars 32
The Trial 32
Does Safe Families divert the flow of children into foster and residential care by
3
Is there any evidence of increased stress on carers whose children are supported
by Safe Families? 37
Is there any evidence of impairment to the well-being of children supported by
Safe Families? 39
Conclusions and Recommendations 41
Lessons Learned 42
Challenges 44
Conclusions 45
Recommendations 46
Appendices 49
Appendix 1: The Legal Status of Children Supported by Safe Families 49
Appendix 2: Statistics on Section 20 Cases 52
4
List of figures
Figure 1: Randomisation Arrangements 24
Figure 2: Consolidated Standards of Reporting Trials (CONSORT) Flow Diagram 34
Figure 3: Randomisation dates by regional hub (single case in June 2015 excluded
5
List of tables
Table 1: Referrals, Families Supported And Children Supported In The 2015/16
Financial Year 26
Table 2: The Number Of Bed Nights Provided To Children By Safe Families 27
Table 3: New Volunteers Recruited By Safe Families In 4 New Hubs In The 2015/16
Financial Year 28
Table 4: Reach And Potential Market Penetration In The 5 Hub 29
Table 5: Referrals To Safe Families In The 2015/16 Financial Year 30
Table 6: Reach And Potential Market Penetration In The 5 Hubs 31
Table 7: The Number Of Category 2 Cases Included In The RCT 31
Table 8: The Situation And Outputs For The 13 Families In The Control Group 36
Table 9: Primary Carer Anxiety And Depression 37
Table 10: Levels Of Social Support For Primary Carer 38
Table 11: Carer Satisfaction With Different Aspects Of Safe Families Provision 39
6
Acknowledgements
7
Executive Summary
Safe Families for Children originated in Chicago, Illinois, in 2003, an innovation of the Christian charity: Lydia Homes. It provides vulnerable families with 3 types of family support: respite for the children to live away from home for short periods; friendship for the main carer, usually the birth mother; and resources to help make the family home a healthy environment for children. All 3 family supports are provided by volunteers recruited from the Christian church. The programme has spread to several U.S. states.
In 2013, businessman and philanthropist Peter Vardy, and the CEO of the Vardy
Foundation, Keith Danby, started a charity with the aim of bringing Safe Families to the majority of English local authorities, starting in the North-East of England.
Safe Families was introduced to Dartington Social Research Unit (DSRU) in 2014, leading to rapid analysis of its potential. It was claimed that the U.S. model of Safe Families diverted children away from state sponsored foster and residential care. The previous evidence for this claim is mixed and difficult to verify, given the differences between U.S. and English child welfare systems. Early evidence from the programme in England suggested that it had the potential to support many vulnerable families at low cost, including a significant proportion of those children that were on the edge of the care system. This early evidence also found that:
the programme did not evangelise on behalf of the Christian church
the initial transfer of the programme from the U.S. to the North-East of England had realised a steady stream of volunteers
the programme fitted well with local government’s need to forge new relationships between public services and civil society
the real benefit to local authorities would be in the potential to reduce the flow of children into foster and residential care
the programme was scalable.
Using the support from the Department for Education’s Innovation Fund, DSRU and Safe Families collaborated to develop and scale the programme. Five innovations emerged from this work. First, the programme would focus on 2 categories of children: those in need of what local authorities call ‘early help’ (Category 1) and those on the edge of care (Category 2). The goals were to reach 15% of the children aged 0-10 years of age
8
authorities within 12 months, using evidence and user recommendation to pull in the other 84% of authorities. Fourth, in line with DSRU’s traditions, it was decided to subject the intervention to rigorous evaluation, to estimate impact on flows of children into care; birth parent outcomes; child outcomes; volunteer and user satisfaction. Armed with rigorous evaluation, we were able to trial a new financial model for introducing innovation at scale, called a Public Social Partnership (PSP). Fifth, we introduced seminars on the management of system dynamics to help participating local authorities reap the full benefits of children diverted from the care system.
This report, which covers the period January 2015 to March 2016 seeks to answer 3 primary and 2 secondary research questions:
does Safe Families divert the flow of children into foster and residential care by 10%?
is there any evidence of increased stress on birth parents or other primary carers whose children are supported by Safe Families?
is there any evidence of impairment to the well-being of children supported by Safe Families?
does Safe Families reach needy families in a timely manner?
is the programme scaling in line with the Rogers’ strategy described above?
Methodology
9
Findings
Safe Families provided support to 192 families, comprising 480 children in families designated as Category 1: early help or family support cases. Although these children were not deemed to be ‘on the edge of care’, Safe Families support nevertheless included the provision of 218 nights of respite care across this group of children
There were fewer children in Category 2 (edge of care) referred than initally anticipated. In total during the period of the evaluation, 83 families with such children were referred. Of these, 40 families comprising 91 children received support from Safe Families
When the evaluation team looked at a cohort of children entering care under Section 20 of the Children Act 1989, 15% had a profile that was suitable for the type of help that Safe Families provided. The legal grounds for using Safe Families as an alternative to Section 20 was established during the evaluation period. However, the potential to divert children from care is not being realised evenly across all user local authorities. Many children identified by Safe Families as ‘edge of care’ were not those likely to have gone into care had they not been involved in the project. Rather, they were those needing early help. The uneven, and slower than anticipated, application of Safe Families to children on the edge of care can likely be attributed to 3 causes:
the time it takes local authorities and practitioners to build up confidence in an untested innovation
the difficulty of matching the innovation to the right families, and in a timely way
a nervousness on the part of some Safe Families staff in managing more serious cases. The time taken to match families meeting eligibility criteria to Safe Families volunteers reduced markedly in the evaluation phase but, in most cases, remains too long to effectively respond to the stress experienced by the primary carer
DSRU offered advice to all user local authorities on managing system dynamics, so they could fully reap the benefits of any children diverted from foster or residential care by Safe Families. This advice was taken up by less than half of the local authorities and, as far as can be gauged, not yet applied in any.
The RCT has not been able to provide strong evidence on the impact of the innovation due to the low numbers of families with children on the edge of care who received support from Safe Families during the evaluation period. Of the 83 families referred for such support, only 26 met the criteria for entry into the RCT and were willing to
10
However, whilst acknowledging the above limitation, the evaluation found that , no children in the intervention group entered care in the 6 month follow up period, (2 from the control group entered care and one was placed under a Special Guardianship Order). This suggests that Safe Families can divert cases away from the social care system. Data from the parental stress rating scales, SDQs, and inerviews suggest that Safe Families volunteers can provide suitable support; that no harm had resulted to children, and the stress levels of carers had not increased as a result of the innovation. The focus on child protection was strong, and continued to improve. Carers and children supported by Safe Families as an alternative to coming into care appeared to be satisfied, although numbers were too low to draw any reliable findings.
Safe Families has been successful at scaling the innovation, and in getting it embedded in 20 (14%) of the 150 English local authorities within a 12 month period. All 20 local authorities committed funds for Safe Families before evaluation results for the Public Social Partnership were available. As predicted by the initial scale strategy, consumer satisfaction among the 20 users is creating pull from other groups of local authorities, and Safe Families is extending the programme to 3 new local authorities on the South Coast and is exploring 2 new regions to start in the 2017/18 financial year.1
As welcome as this expansion may be, there is much unsupported need within the 3 regions covered by Safe Families meaning that local authorities not yet signed up in those regions could benefit from the innovation, and more children within existing user authorities could be diverted from care, justifying expanding the use of the innovation by those authorities.
Remarkably, and unusually for volunteer-based innovations, Safe Families has stimulated a steady flow of people from the community willing to give their time to do what others have been paid for, and satisfaction levels among volunteers remains strong.
Lessons learned for stakeholders
Although limited in scope, this evaluation indicates important learning for several stakeholders in the fight to improve the lives of children in need in the U.K.
11
Learning for Safe Families
The future of Safe Families depends on its ability to continue to support more children who otherwise would have been drawn into the foster care system.
Priority should be given to expanding existing hubs of Safe Families activity over developing new hubs.
The success of Safe Families, like any innovation for children on the edge of care, will depend on effective matching between support offered to families and the needs of those families.
Momentum behind existing efforts to apply learning about volunteer recruitment to non-Christian and non-faith groups should increase.
Learning for Local Authorities
It is tempting to treat children in the different sub-systems of children’s services as homogenous, by virtue of their label, such as child in care or child in need of protection. Services can be much better differentiated if these groups are disaggregated by pattern of need.
There is an alarming loss of knowledge about system dynamics; the management of numbers of children in care, and the consequences of effective innovation on those numbers. Knowledge accumulated in the last decades of the last century will aid progress.
Civil society contains huge tapped and untapped resrouces for families in need. Many children who are exposed to risks that may impair their health or
development are not known to the public system. Evidence suggests that those formally designated as ‘children in need’ are likely only a small proportion of this total (DSRU, forthcoming). The experience of Safe Families suggests that there are many people in civil society ready to volunteer for unpaid roles that have traditionally been paid for by public systems.
Learning for Government
12
Much evidence regarding children in care is alarmingly out of date, and there is limited evidence about impact on outcomes. As an intrusive and costly intervention in family life, there is an ethical imperative to determine its effect.
There is a loss of knowledge about the origins and aspirations of the Children Act, 1989, which represents the primary legal statement about the relationship
between state and family. There is a danger of narrow concerns about child protection crowding out broader legal and ethical questions about child and family rights.
Learning for Research
Despite low numbers, this evaluation shows that it is possible to mount a
randomised control trial of children coming into state care. Highly disadvantaged children deserve high quality evidence about the impact of interventions supported by the state.
There is a continued need for innovation in data collection, in the context of high family stress. The apps developed for this evaluation were largely unsuccessful but this should not deter future innovation.
There is a balance to be found between aspiring to the highest standards of scientific excellence and finding practical solutions to the complex processes of public systems.
While priority should be given to understanding the impact of alternatives to
interventions like foster and residential care, there is much to learn about effective practice for families in need of what is called ‘early help’ or ‘family support’.
Recommendations
The initial scale up of Safe Families between January 2015 and March 2016
demonstrates from the feedback from families, the potential to alter the way in which local authorities respond to children on the edge of care, forging a new relationship between public systems and civil society, and providing a model for other reforms. However, as with all start-ups, there remains much to learn, and challenges to be overcome before the potential of the innovation can be fully realised. Based on the evaluation results, DSRU recommends:
13
authorities call ‘early help’, according to the feedback from the families involved, the primary benefit of Safe Families comes from its provision of an alternative for about 15% of children who each year come into foster or residential care. The promise lies in the potential benefits to children and families by exposing them to greater community support and less system involvement, and to the easing pressure on hard-pressed local authority budgets.
if the first recommendation is accepted, we estimate that each year there would be as many as 708 children on the edge of care in the 3 regions covered by Safe Families and within the 20 early adopter local authorities. Two-thirds of these 708 children could be successfully diverted from foster or residential care. Extending Safe Families to 90% of local authorities in the existing 3 hub areas (meaning the innovation would serve 47 local authorities in total) could see it divert 1,533 children from care annually. We therefore recommend that Safe Families favour consolidation in existing local authorities, and extending into new local authorities within existing regions, over the development of new regions. These 2 options need not be mutually exclusive, it is a matter of balance.
however, none of this potential can be realised unless Safe Families and user local authorities collaborate to ensure a good and timely match between the innovation and the families that can benefit from the innovation (those whose reaction to a crisis means that their younger children are at risk of a short period of accommodation in care). We recommend finding a lasting solution to this
challenge.
the potential for local authorities to translate reductions in the flow of children into care into reduced numbers in care at any one time (or a reduction in overall bed nights) cannot be realised without them paying more attention to the management of system dynamics (engaging local people and experts to choose a number that is right for local conditions; managing stock and flow; analysing the consequences of decisions at one point in the system for another). Through the contact between the evaluation team and local authority project participants, DSRU staff have been struck by the loss of knowledge about system dynamics within local authorities. We recommend that local authorities using Safe Families are given more access to training and tools to manage foster and residential care numbers to a level that is comfortable for elected members, the executive and senior practitioners.
14
possible. Mistakes were made by DSRU in the initial trial, and these need to be rectified in any future evaluation.
15
Aims
The evaluation sought to answer 3 primary and 2 secondary questions. The primary questions were of most interest to local authorities, and formed part of all the PSP agreements:
1. Does Safe Families divert the flow of children into foster and residential care by 10%?
2. Is there any evidence of increased stress on carers whose children are supported by Safe Families?
3. Is there any evidence of impairment to the well-being of children supported by Safe Families?
The secondary research questions concerned the conditions to be satisfied if Safe Families was to achieve impact at scale:
1. Does Safe Families reach needy families in a timely manner?
16
Background
Safe Families for Children originated in Chicago, Illinois, the brainchild of David
Anderson, the Chief Executive of Lydia Homes, a major provider of child welfare services in the city. A lot of claims have been made for Safe Families in the United States,
primarily focusing on its ability to support at home children who otherwise would have gone into state care. These claims, which may or may not be true, are being rigorously evaluated in the U.S. as well as England.
The idea is that Safe Families offers 3 types of volunteers. There are host families who will take the children into their homes to stay for short periods; family friends who offer support (they are friends not therapists), and resource friends, who will offer or find goods or support that disadvantaged families need, such as a stair-gate or help clearing the garden. Many programmes - Homestart for example - offer one of these inputs. Safe Families is unique in offering all 3.
Lydia Homes is a Christian based Non-Governmental Organisation. Anderson finds volunteers from the Christian Church. As they like to say in Safe Families, ‘finding the volunteers is straightforward because we know where they are on a Sunday morning’.
Established in 2003, Safe Families is now operating in over 40 sites across the United States. However, just as there have been few reliable studies of the efficacy of placement of children in foster or residential care, there is no well-founded research about the
impact of Safe Families on child outcomes. The Juvenile Protection Association in Chicago, Illinois undertook a good descriptive study in 2009. They found that children stayed with host families for extensive periods (an average of 53 days). There was some indication that the rate of children removed into what is called ‘protective custody’ - state care in England - was lower than for families getting support from child protection
services - what we would think of as early help in England (8% for Safe Families, 16% for child protection services). However, these differences, and potential implied cost benefits and savings to public systems, cannot be reliably attributed to the intervention. A low cost, randomised control trial, facing many of the same challenges encountered in the DSRU evaluation, is being undertaken by a team led by Mark Testa at the University of North Carolina: Chapel Hill.
17
Legal, Administrative and Fiscal Context
Public perceptions of children in care have progressed since Dickensian times, when they were thought of as orphaned children rescued from the street. In fact there are hardly any orphans. In 1968 and again in 1986, Jean Packman provided a helpful
typology of children in care comprising victims - of neglect and abuse; volunteers - whose parents find they are temporarily unable to cope and have no back up; and villains - whose behaviour is beyond what parents, and sometimes schools, can deal with. Unfortunately, this has never been replicated. In this context, it is the children who are volunteered into care who are the one’s best suited to an innovation like Safe Families.
The majority of children coming into care (or being looked after) are separated under a voluntary arrangement between the primary carer and the local authority. The children are not separated by compulsion: they are accommodated with foster parents or, in a minority of cases, in a residential home. The primary carer can ask for their children to come back to the family home at any time, and a social worker can only object by going to court and asking magistrate or judge to intervene with an order.
These voluntary arrangements have long been a part of the English and Welsh system of supporting children away from home (they are less common abroad, and do not apply in the U.S. context). Arrangements were clarified in the ground-breaking framework
legislation of the Children Act, 1989, which re-defined the relationship between the state and family. Section 20 of the 1989 Act covers these voluntary arrangements. Three-fifths of looked after children in England are under Section 20, and three-fifths of them are 10 years of age or less. Most stay for short-periods of time, with most back at home within a matter of weeks2.
Prior to legislation in 1963, it was not possible for local authorities to take actions designed to prevent children coming into foster or residential care. Gradually, this
changed and the 1989 legislation enshrined much higher levels of family support for what were called ‘children in need’. Most of this provision was covered under Section 17 of the Act and, consistent with the rest of the legislation, this extended to all needs, including disability for example. At the beginning of this century, government began to take a census of the number of children who local authorities considered to be in need, a list that soon mushroomed to about a third of a million at any one time. In the last decade, this family support aimed at helping children to remain at home with their primary carers is often referred to as ‘early help’.
18
The good intentions of the 1989 Act have, to some extent, been undermined by a failure to protect a small number of children from gross maltreatment, resulting in greater government scrutiny, a more stringent inspection and regulatory approach and much higher levels of bureaucracy, as picked up in the Munro Review of 2011. Many
researchers (e.g. Brown, 2010 ) have noted the risk averse climate in which children’s services leaders and practitioners are working which might have been expected to lead to cautious responses to the innovation involved in this project.
The idea, then, that an unpaid, untrained volunteer, albeit one who has been vetted using procedures modelled on those used by local authorities to assess foster parents, could support children who otherwise would come into care under Section 20 of the Children Act 1989 is unsurprisingly challenging for some. Indeed, officials in 4 local authorities raised questions about the legal status of children diverted from care. One local authority involved in the evaluation took the view that, although supported by Safe Families, the cases should still be captured under Section 20 and, as such, counted under local authority statistical returns, which stood against one of the primary aims of the innovation.
The matter was considered by legal experts supporting DSRU, legal experts brought in by Safe Families for Children, and also by officials and lawyers at the Department for Education, which appointed 2 Directors of Children’s Services to look into the matter in more depth.
It was concluded that, once hosting was agreed by the parent and Safe Families for Category 2: Edge of Care, support would be sanctioned under Section 17 of the Children Act, 1989, with the designation ‘children in need’. Where a parent seeks, of their own volition, to place their child in foster care under Section 20 of the legislation, they may be persuaded of the merits of Safe Families - including the host family option. In such an instance, the support is covered under Section 17 of the 1989 legislation. Most of the 20 local authorities use this interpretation, but a handful take the view that, if a family meets the Section 20 threshold, then Safe Families cannot be considered as an option. Given the complexities and extensive scrutiny, Safe Families appointed national expert Wendy Rose to oversee a panel to continually improve already strong child protection
procedures. DSRU’s view is summarised in Appendix 1.
Safe Families finds itself at the fulcrum of competing forces in children’s services. On the one hand, government and the inspectorate, hold local authorities and individual
19
context, the idea of testing the efficacy of the help available within civil society has become pressing.
The Innovation Process
In 2014, Sir Peter Vardy and Keith Danby, Chair and CEO of the Vardy Foundation, approached DSRU for help in evaluating the U.K. version of the programme. Our initial due diligence highlighted:
the potential of the programme to help public systems forge a better relationship with civil society
the possible benefits to child outcomes and local authority finances of using the programme to divert children away from foster care.
DSRU scrutinised the religious component of the programme and found it to be restricted to volunteer and staff recruitment, and not in any way evangelical in the sense of
proselytising Christianity to birth parents or children. We also found appropriate child protection processes in place.
The due diligence also drew attention to:
the potential benefits of shifting the emphasis from early help to edge of care. It was clear that the U.S. version of Safe Families was aimed at families with greater levels of need, a higher proportion of whom were in danger of having their children placed in foster care. The child welfare systems in the U.S. and England are different, but there was clearly an opportunity for Safe Families to divert many more children away from the care system in England
the need to get help to families at the moment of crisis, not several weeks later. Our initial analysis showed that it could take local authorities between 3 and 6 weeks to refer families to Safe Families, which in some cases could then take another 3 weeks to decide whether their intervention was appropriate. We knew from the earlier evidence that proximity of intervention to the moment of crisis would bear heavily on outcomes for parents and children
the value of a strategy to scale the innovation across the England. Sir Peter Vardy and Keith Danby both had huge expertise in scaling business propositions, but not in scaling interventions for children within public systems. They could see the opportunity to build an army of volunteers ready to help children across the England, but not the means to achieve the end
20
both the innovation and the orthodoxy, and to establish the basic ethic that public interventions first do no harm.
In the summer of 2014, an opportunity to take the work of Safe Families forward was presented in the form of the Department for Education Innovation Fund. Safe Families and DSRU collaborated in producing a bid to the Fund to scale and evaluate the programme. DSRU methods were used to bring together stakeholders - Safe Families staff, potential public system commissioners, volunteers and users - to examine available data, understand barriers to impact at scale, and then devise innovations to get around those barriers. We were aided in the process by the support of the Spring Consortium, which had been appointed by the Department for Education to assist applicants, with help on business planning proving particularly useful.
A revised model of Safe Families emerged, as it is set out in the application to the Department for Education in the autumn of 2014 (available on request). The Innovation Fund awarded Safe Families £2.4m, sufficient to implement the innovations, scale and evaluate the programme. A significant limitation of the funding was that money had to be spent in the 2015-16 financial year.
Five Innovations
The process of innovation just described meant that the Safe Families programme delivered after support from the Department for Education Innovation Fund award differed from that being operated in the North-East of England in 5 important respects. First, after modelling flows of children into local authority care across England, we
estimated that around 15% of children being placed in foster care each year could safely be supported by Safe Families volunteers, and that two-thirds of those children would not subsequently require support from children’s services, with a net reduction of in-flow into foster care of 10% a year in each participating local authority at steady state. This was consistent with the Department for Education Innovation Fund’s goals to ease pressure on social workers and reduce the flow of children into care.
It was therefore planned to encourage local authorities to use Safe Families for 2 types of case: Category 1: early help or family support cases (in other words continuing the model delivered in the North-East of England); and Category 2: Edge of Care’ cases.
21
the Children Act, 1989; and where there were no serious child protection concerns or obvious threats to the host family or other volunteers3.
At steady state, it was estimated that Safe Families would support 75 families (and approximately 160 children) in each local authority each year, covering both Category 1 and Category 2. In order to ensure good implementation quality, it was agreed to support 25 families in year 1, 40 families in year 2, arriving at steady state of 75 families in year 3.
Second, analysis of Safe Families work in the North-East showed that getting the intervention to families as quickly as possible after the precipitating crisis would be a critical contributor to a successful outcome. This included being responsive to families who sought help from children’s services departments out of office hours.
This innovation is referred to as ‘just in time’. It avoids the typical pattern whereby children’s services assess cases for several days before referring on to a voluntary organisation, who prolongs the assessment process further. An app was built to sit on social workers’ desktop computers, or on their phones or tablets, which the social worker used for 2 or 3 minutes per case. It ascertained whether there was a match between the referral and the threshold criteria (both Category 1 and Category 2) for Safe Families. If there was a match, and the mother or other primary carer agreed, the app sent an email directly to the Safe Families social worker who visited within 2 working days.
Third, to have significant impact on the lives of children in the England, Safe Families required a scale strategy. The approach taken was based on Rogers’ (1962) diffusion theory . If Safe Families could successfully implement its programme in 16% (N=24) of the 150 English local authorities, a natural pull would be generated among successive groupings for the 84% of later adopters.
Because volunteer recruitment crossed local authority boundaries, it was decided to operate in hubs comprising 4 to 10 local authorities. In addition to the North-East (potentially 12 local authorities), it was proposed to establish Safe Families hubs in Merseyside (potentially 7 local authorities); Greater Manchester (10); East Midlands (9); and West Midlands (14).
Fourth, because the evidence for the effectiveness of Safe Families had fallen short of the standard used by DSRU’s Investing in Children what works repository, widely used by English and Scottish local authorities, it was necessary to find a way of getting local authorities to test the programme before making a longer term commitment.
22
The solution adopted was a Public Social Partnership between Safe Families, each participating local authority, an independent investor and DSRU, operating as the independent arbiter. Sometimes known as ‘try before you buy’, the PSP allowed local authorities to try Safe Families for a period of up to 12 months without payment. Costs were covered by an independent investor. During the trial period, a rigorous evaluation established whether the programme achieved what each of the parties to the PSP wanted it to achieve. If the results were positive, the local authority bought the programme for a subsequent 2-year period.
The regular commissioning rules are suspended during the period of the PSP to allow for the innovation to be tested, but resume at the end of the PSP contract.
Fifth, while it was anticipated that Safe Families had the potential to reduce the flow of children into care by 10%, it was known that the resultant empty foster beds would only be filled by other needy children. In other DSRU studies (forthcoming), we estimate that for every child in care, there are another 6 with exactly the same profile not in care. Much of the variance in the numbers of children in care from one local authority to another is not explained by need. Most of the differences are explained by system factors; some by the explicit decisions of system leaders and practitioners; some by the dynamics that occur as a result of complex processes, like connecting needy children with a range of high-end supports.
DSRU has long experience of helping local authorities to manage system dynamics, usually with the objective of reducing numbers: the same process can be used to increase numbers.
23
Methodology
A mixed method approach was used. This included scrutiny of administrative records on 569 children in need or on the edge of care held by 20 local authorities and Safe
Families, and regular checking in with the Safe Families project management system covering volunteer and family recruitment, matching of families and volunteers. We also undertook qualitative interviews with 15 birth parents and volunteers and 10 local
authority staff, in order to understand their satisfaction with the programme, and also to get suggestions for improvement. We held 5 seminars of Safe Families staff and
interviewed local authority staff to get feedback on DSRU-led innovations such as the PSP. Some additional bespoke data was assembled on behalf of some of the
participating local authorities. Ethical approval for the study was given by the DSRU Ethics Committee run by Centre for Social Policy fellows4, and additional scrutiny was
given by a handful of the participating local authorities.
At the core of the evaluation was a randomised control trial of 26 Category 2 cases. Families referred to the programme by local authority teams were screened using the app described above, or by a paper-based approach applying the same criteria. This identified whether the family matched the criteria for Category 2: Edge of Care provision; asked the main carer for permission for a Safe Families caseworker to visit the family home, and sent an email to the local Safe Families office to begin the referral process. Safe Families committed to conducting a home visit to all families entered by the app within 2 working days of receiving the email. A separate procedure was operated for emergency cases allowing for eligibility to be assessed outside of the home.
On visiting the family, in addition to undertaking their own assessment, it was planned for the Safe Families caseworker to hand parents a tablet that contained a second app. This comprised a procedure for giving consent to participation, and a series of questions relating to 3 scales: the Strengths and Difficulties Questionnaire (SDQ),5 focused on
children’s well-being, including mental health; the Hospital Anxiety and Depression Scale (HADS), focused on parents’ stress and depression; and the Interpersonal Support Evaluation List (ISEL), focused on the amount of support available to carers.
If the case was considered a match by the Safe Families caseworker, the app sent a message to the DSRU team that conducted a statistical procedure which randomly assigned each case to either an intervention group, to receive Safe Families support; or a control group to receive services as usual from the local authority.
4 http://centreforsocialpolicy.org
24
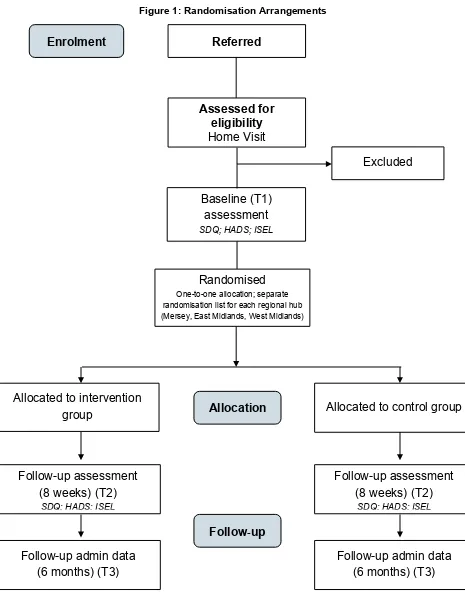
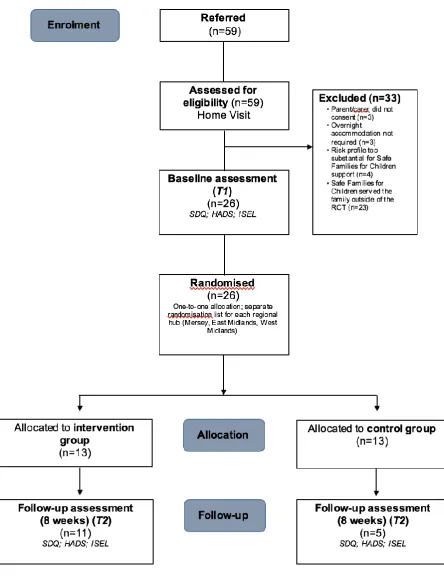
[image:24.595.61.526.130.742.2]The statistical procedure involved a computer-generated randomisation sequence designed to provide user local authorities with a balance of cases in intervention and control groups over a 12 month period. Figure 1 summarises the randomisation arrangements.
Figure 1: Randomisation Arrangements
Enrolment Referred
Assessed for eligibility Home Visit
Excluded
Baseline (T1) assessment SDQ; HADS; ISEL
Randomised
One-to-one allocation; separate randomisation list for each regional hub (Mersey, East Midlands, West Midlands)
Allocated to intervention
group Allocation Allocated to control group
Follow-up assessment (8 weeks) (T2)
SDQ; HADS; ISEL
Follow-
up
Follow-up assessment (8 weeks) (T2)
SDQ; HADS; ISEL
Follow-up admin data (6 months) (T3)
25
In addition, data were collected from administrative records at referral 6 months later, and directly from primary care givers, using the same app used by Safe Families caseworkers on a phone or tablet (these data were collected at referral and 8 weeks later).
The randomised control trial addressed the 3 primary research questions. We hypothesised a successful outcome, and a reason for local authorities to continue commissioning Safe Families, against the 3 questions:
1. Does Safe Families divert the flow of children into foster and residential care by 10%? Success would mean: (i) Safe Families supported sufficient children from Category 2 in each user local authority; (ii) the majority of children in the control group went into care under Section 20, indicating that Safe Families was targeting and reaching the right children; (iii) less than a third of the children supported by Safe Families under Category 2 later came into foster or residential care.
2. Is there any evidence of increased stress on carers whose children are supported by Safe Families? Success would mean the stress levels of mothers receiving Safe Families not deteriorating (that is, no harm) and, ideally, improving compared to the control group. We selected parental stress as an indicator because
continued high levels of anxiety would likely lead to repeated calls on children’s services for support.
3. Is there any evidence of impairment to the well-being of children supported by Safe Families? Success would mean no deterioration (that is, no harm) to children from families receiving the intervention, and ideally an improvement in well-being and mental health.
26
Findings
The results are reported in 3 sections. The first deals with a description of the take-up of Safe Families across 20 local authorities during the 15 month evaluation period. We move on to consider the effectiveness of the 5 innovations, and the secondary research questions. This is followed with a summary of results from the randomised controlled trial covering the primary research questions.
Local Authority Take Up of Safe Families
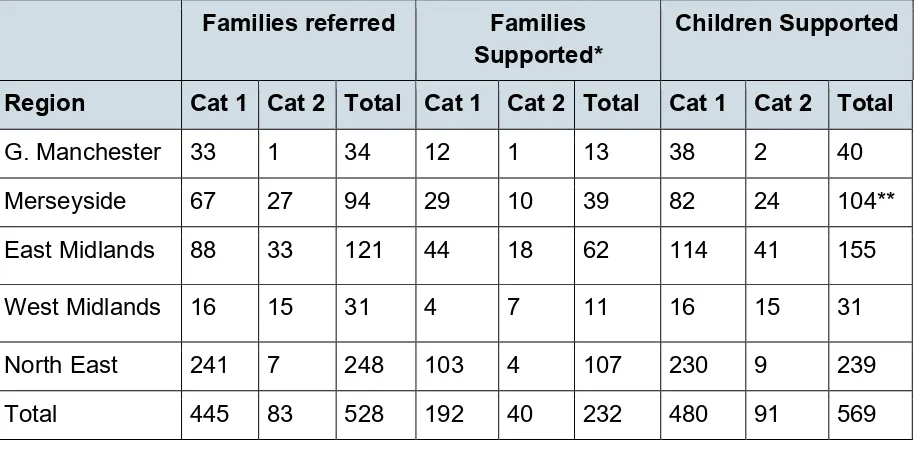
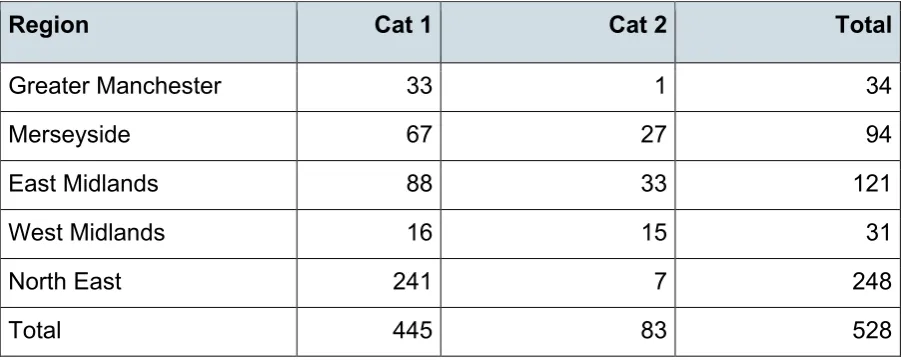
As might be expected, while the take up of Safe Families provision has been extensive it was still slower than anticipated at the planning stage, particularly with respect to families with children on the edge of care. Just over 15% of referrals of families (83) came under Category 2: Edge of Care in the financial year 2015/16, whilst for Category 1 (support for familes with children in need) there were 445 families referred. The conversion rate of referrals to support ran at 44% for Category 1 (192 families comprising 480 children), and 48% for Category 2. As Table 1 illustrates, 40 of the 83 families seeking Category 2 help were supported by Safe Families, comprising 91 children6. Once again, East Midlands
[image:26.595.60.517.424.649.2]and Merseyside hubs were responsible for the majority (70%) of families supported under Category 2.
Table 1: Referrals, Families Supported and Children Supported in the 2015/16 Financial Year
Families referred Families Supported*
Children Supported
Region Cat 1 Cat 2 Total Cat 1 Cat 2 Total Cat 1 Cat 2 Total
G. Manchester 33 1 34 12 1 13 38 2 40
Merseyside 67 27 94 29 10 39 82 24 104**
East Midlands 88 33 121 44 18 62 114 41 155
West Midlands 16 15 31 4 7 11 16 15 31
North East 241 7 248 103 4 107 230 9 239
Total 445 83 528 192 40 232 480 91 569
*Families referred and supported in 2015/16 financial year. The table does not count those referred in
27
2015/16 financial year and supported in the 2016/17 financial year.
**2 children were re-referred under a different category within the same year.
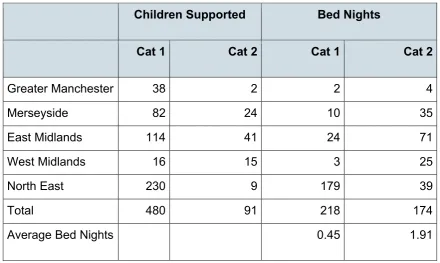
[image:27.595.55.496.209.472.2]Table 2 reveals 2 important findings from the Safe Families offer. First, unique among providers of early help and family support services, Safe Families is providing 218 nights of respite away from the family home for the 480 children supported under Category 1. Second, stays for those children placed with host families under Category 2 are relatively short, about 1.9 bed nights on average.
Table 2: The Number of Bed Nights Provided to Children by Safe Families
Children Supported Bed Nights
Cat 1 Cat 2 Cat 1 Cat 2
Greater Manchester 38 2 2 4
Merseyside 82 24 10 35
East Midlands 114 41 24 71
West Midlands 16 15 3 25
North East 230 9 179 39
Total 480 91 218 174
Average Bed Nights 0.45 1.91
28
The Five Innovations
Scale
Arguably the greatest success of the Safe Families programme post award of the
Department for Education Innovation Fund grant was to scale the programme to 20 local authorities: just short of the goal to be active in 16% (n=24) of the 150 English local authorities. In addition to the existing North-East hub, a further 4 hubs were established in Merseyside, Greater Manchester, East Midlands and West Midlands.
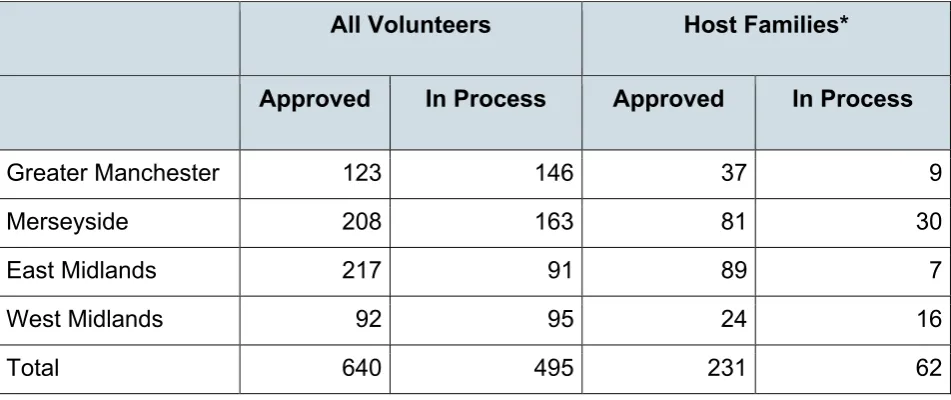
[image:28.595.59.535.330.530.2]As mentioned above, the primary failing of volunteer-based innovations is the difficulty in recruiting volunteers. Safe Families has clearly overcome this challenge. Table 3 counts new volunteers recruited in the 4 new hubs up to the end of March 2016. As can be seen, 640 new volunteers were recruited, of whom over two-fifths (46%) had capability to offer respite for children from referred families in their own home.
Table 3: New Volunteers Recruited by Safe Families in 4 New Hubs in the 2015/16 Financial Year
All Volunteers Host Families*
Approved In Process Approved In Process
Greater Manchester 123 146 37 9
Merseyside 208 163 81 30
East Midlands 217 91 89 7
West Midlands 92 95 24 16
Total 640 495 231 62
*Includes family friends also acting as hosts
As of October 1st 2016, Safe Families had 1,969 volunteers approved, of which 634 had the capability to serve as a host family7. Consistent with other results, the spread of
volunteers was not even, clustering in the East Midlands, Merseyside and the North-East, and within hubs, clustering in Wirral, Liverpool and Nottingham. It is unsurprising,
therefore, that Safe Families consolidated its operations at the end of the first year into 3 hubs, serving the North-East, North-West and Midlands.
29
Consistent with the Rogers’ (1962) hypothesis, there was now a strong interest from other local authorities across England in buying Safe Families provision. However, therein lies a dilemma for the organisation. Table 4 goes back to the 5 original hubs. It shows that, in total, they had the potential to reach 52 local authorities (a third of those in England). At the end of the first 12 months, 20 of the 52 had signed PSPs and
subsequently made commitments to fund Safe Families into a second year. If the programme reached its potential to support 15% of children coming into care under Section 20 of the Children Act, 1989, over 1,500 would be supported, and over 1,000 would be diverted from the care system. As the final column of Table 4 indicates, the restricted reach within existing regions to 20 of the 52 possible local authorities means that between a third and half of children, and 91% in the West Midlands, would miss out.
Table 4: Reach and potential market penetration in the 5 hub
Possible in 5 Hubs Potential in 20 LAs Served
Number of LAs
15% of Entrants
LAs Served
15% of Entrants
Potential Market Penetration
Greater Manchester
10 286 4 143 50%
Merseyside 7 206 3 114 55%
East Midlands 9 366 5 236 64%
West Midlands 14 561 2 50 9%
North East 12 284 6 165 58%
Total 52 1703 20 708 42%
The challenge for Safe Families is to know whether expanding into new regions will bring greater gains than consolidating and growing within existing geography.
Just in Time
30
Reaching Category 2 Cases
As described above and in Appendix 2, local authorities’ enthusiasm to embrace Safe Families as an alternative to voluntary accommodation of children in care varied, but over the 15 months of evaluation referrals of edge of care cases grew and, as shown later, has continued to grow after the evaluation was closed. Overall, during the evaluation period, just over 15% of referrals came under Category 2: Edge of Care in the financial year 2015/16. As can be seen in Table 5, over two-thirds (72%) of the Category 2 referrals came from the East Midlands and Merseyside, and 2 local authorities -
[image:30.595.58.509.265.445.2]Nottingham and Liverpool - were responsible for the majority of the referrals in these 2 hubs.
Table 5: Referrals to Safe Families in the 2015/16 Financial Year
Region Cat 1 Cat 2 Total
Greater Manchester 33 1 34
Merseyside 67 27 94
East Midlands 88 33 121
West Midlands 16 15 31
North East 241 7 248
Total 445 83 528
31
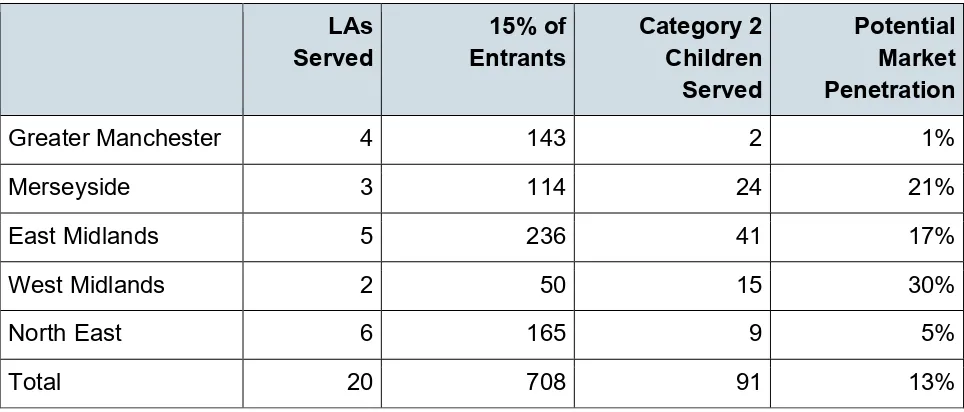
Table 6: Reach and potential market penetration in the 5 hubs
LAs Served
15% of Entrants
Category 2 Children Served
Potential Market Penetration
Greater Manchester 4 143 2 1%
Merseyside 3 114 24 21%
East Midlands 5 236 41 17%
West Midlands 2 50 15 30%
North East 6 165 9 5%
Total 20 708 91 13%
Unfortunately, the low level of connection between need and service meant that there were fewer than anticipated cases for the randomised control trial. As Table 7 shows, only 13 of the 40 families supported by Safe Families under Category 2: Edge of Care were also included in the evaluation trial, and all but one of these cases came from either the East Midlands or Merseyside hubs. These 13 cases are matched with another 13 drawn from the 43 families not supported by Safe Families.
Table 7: The Number of Category 2 Cases Included in the RCT
Category 2 Cases Category 2 Trial
Referred Supported Control Intervention
Greater Manchester 1 1 0 0
Merseyside 27 10 7 6
East Midlands 33 18 6 6
West Midlands 15 7 0 1
North East 7 4 0 0
[image:31.595.57.540.457.683.2]32
By any standard, 26 families is too low a number from which to draw reliable findings and falls far short of the 360 anticipated.
Public Social Partnership (PSP)
A review of the PSP was undertaken by DSRU one year after the beginning of the evaluation. It shows mixed results. The PSP had clear attractions for the senior
leadership of local authorities, in that it allowed them to try Safe Families to see whether it worked, without having to pay until the innovation was shown to work. If it did work, it would clearly be cost-beneficial to the local authority. The level below senior leadership were less enthusiastic, and many commissioning staff responsible for agreeing the individual PSP contracts viewed it with suspicion, particularly since it bypassed many of the ordinary checks and balances that makes a public system work efficiently and fairly. This meant that senior staff in Safe Families had to do much more work than they had anticipated, trying to convince commissioners to adopt the PSP model, some of whom only signed up several months into the free period. We cannot tell whether the use of conventional contractual arrangements would have been easier or quicker.
The basic idea of a PSP is to try before buying, with the decision to buy being guided by the results of evaluation. As it turned out, 20 local authorities decided to buy without having seen the evaluation results and, as far as we know, no local authority declined to buy Safe Families because of the evaluation. In this sense, we failed to implement the basic PSP idea.
DSRU has used the results from Safe Families to develop the PSP concept as part of a broader investment portfolio for innovation in children’s services, but we accept that its utility on a deal by deal basis such as Safe Families is as yet unproven.
The System Dynamics Seminars
Only half of the local authorities took up the offer of a seminar on management of system dynamics, and we could not see any evidence of any actions resulting from the seminars except in 2 local authorities that have engaged with DSRU to take a more robust and rigorous approach to the challenge.
The Trial
In this section we report the findings, however as has been indicated, the number of children recruited into the randomised control trial is too low from which to draw reliable results.
33
selected by DSRU was counter-productive. While it was sufficient to satisfy the most sceptical scientist, it also meant that one local authority experienced 4 consecutive referrals being randomised to control in a short period. This naturally upset both hard pressed social workers and Safe Families caseworkers, and undermined the confidence of local authority leadership in the programme. Using the best evaluation method
34
Figure 2: Consolidated Standards of Reporting Trials (CONSORT) Flow Diagram
35
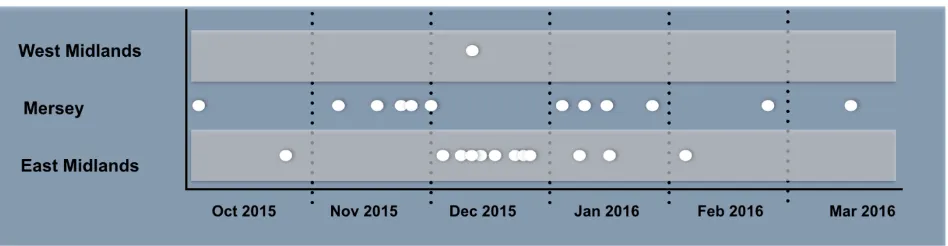
[image:35.595.58.532.120.243.2]delayed. Figure 3 illustrates the pattern of recruitment of cases across the 3 consolidated regions.
Figure 3: Randomisation dates by regional hub (single case in June 2016 excluded from figure)
Bearing in mind all of the caveats about the data, we explore, below, what they say about the primary research questions.
Does Safe Families divert the flow of children into foster and
residential care by 10%?
Success would mean: (i) Safe Families supported sufficient children from Category 2 in each user local authority; (ii) the majority of children in the control group went into care under Section 20, indicating that Safe Families was targeting and reaching the right children; (iii) less than a third of the children supported by Safe Families under Category 2 later came into foster or residential care.
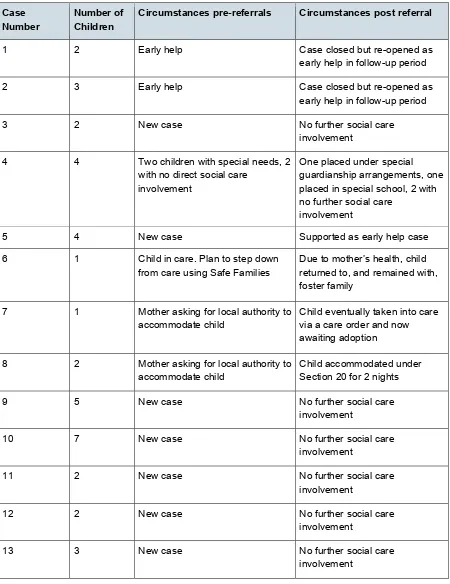
Safe Families did not support sufficient children from Category 2 in most of the local authorities to meet the first criterion for success. As has been seen, the flow of Category 2 cases was uneven, and only got near to target in 2 local authorities: Nottingham and Liverpool. Moreover, analysis of children allocated to the control group, summarised in Table 8, indicates that few of the children in the trial met the criteria for Section 20 of the Children Act 1989. Once the Safe Families option was stopped, as a result of allocation of the case to the control group, 6 of the 13 families received no further support from children’s services, and only 3 got more early help support. In 2 cases the threshold was met, and in one case the situation bordered on being beyond what Safe Families could responsibly manage. In addition to the trial cases, Safe Families also supported 78 families under Category 2 outside of the evaluation, several of which were counted as an emergency. These cases were much more likely to meet the Section 20 threshold.
36
[image:36.595.60.510.119.703.2]under a Special Guardianship Order) suggesting that Safe Families was diverting cases away from the social care system, and, in some cases, from foster and residential care.
Table 8: The situation and outputs for the 13 families in the control group
Case
Number Number of Children Circumstances pre-referrals Circumstances post referral
1 2 Early help Case closed but re-opened as
early help in follow-up period
2 3 Early help Case closed but re-opened as
early help in follow-up period
3 2 New case No further social care
involvement
4 4 Two children with special needs, 2 with no direct social care
involvement
One placed under special guardianship arrangements, one placed in special school, 2 with no further social care
involvement
5 4 New case Supported as early help case
6 1 Child in care. Plan to step down from care using Safe Families
Due to mother’s health, child returned to, and remained with, foster family
7 1 Mother asking for local authority to accommodate child
Child eventually taken into care via a care order and now awaiting adoption
8 2 Mother asking for local authority to accommodate child
Child accommodated under Section 20 for 2 nights
9 5 New case No further social care
involvement
10 7 New case No further social care
involvement
11 2 New case No further social care
involvement
12 2 New case No further social care
involvement
13 3 New case No further social care
37
Is there any evidence of increased stress on carers whose children are
supported by Safe Families?
Success would mean the stress levels of mother’s receiving Safe Families did not
deteriorate (that is, no harm was done) and improved compared to the control group. We selected parental stress as an indicator because continued high levels of anxiety would likely lead to repeated calls on children’s services for support.
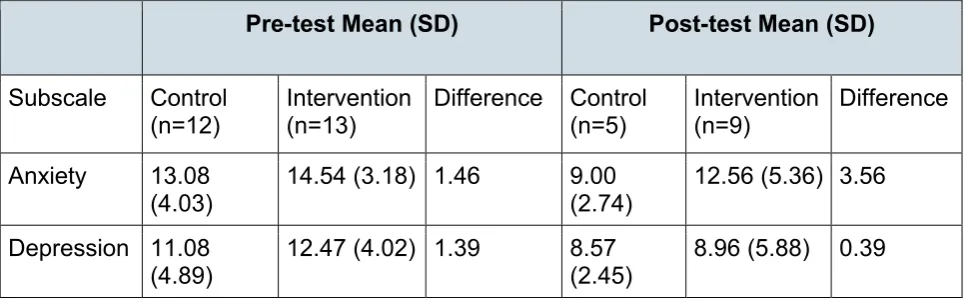
[image:37.595.58.541.277.428.2]As Table 9 shows, parental anxiety reduced over time for the primary carer in both intervention and control group, with slightly greater gains for those in the control group. Similarly, depression decreased for the primary carer in both groups, this time with more gains for the Safe Families participants.
Table 9: Primary Carer Anxiety and Depression
Pre-test Mean (SD) Post-test Mean (SD)
Subscale Control
(n=12) Intervention (n=13) Difference Control (n=5) Intervention (n=9) Difference
Anxiety 13.08
(4.03)
14.54 (3.18) 1.46 9.00
(2.74)
12.56 (5.36) 3.56
Depression 11.08 (4.89)
12.47 (4.02) 1.39 8.57
(2.45)
8.96 (5.88) 0.39
(Note: a mean change score of below zero indicates average reductions in scores, with positive figures indicating increases in scores)
We also assessed the perceived availability of 4 separate forms of social support in the control and intervention group using a measure called the ISEL: "tangible" support
measures the perceived availability of material aid; the "appraisal" subscale captures the perceived availability of someone to talk to about one's problems; the "self-esteem" subscale, the perceived availability of a positive comparison when comparing one's self to others; and the "belonging" subscale, the perceived availability of people with whom to share life’s pleasures. Table 10 summarises the results, with lower scores indicating lower levels of perceived support.
Despite the control group having higher levels of perceived support at pre-test (on all scales), by post-test, those families receiving Safe Families reported much higher levels of perceived support, more than they had reported at pre-test and more compared to the control group at pre and post-test. This may reflect the availability of a range of
38
In summary, there is no evidence of the Safe Families intervention harming the carers of children in supported families, and there is some indication that there could be benefits, particularly with respect to reduced stress and depression, and increased perceived social support. However, further evidence is needed to support this finding..
As Table 11 illustrates, levels of satisfaction with Safe Families among primary carers, usually the mothers of children supported, is extremely high, whereas levels of
[image:38.595.56.549.293.581.2]satisfaction decreased among control parents, though the small sample size should be acknowledged. Carers were asked to rate each of the components of the Safe Families service, not just the 3 core elements of host family, family friend, and resource friend. Again, the number of cases in the sample is small, and variation in results is low, but nonetheless, satisfaction levels are about as high as could be achieved for this kind of innovation operating in the context of high levels of family stress.
Table 10: Levels of Social Support for Primary Carer
Pre-test Mean (SD) Post-test Mean (SD)
Subscale Control (n=10) Intervention (n=11) Difference Control (n=5) Intervention (n=10) Difference Overall score 52.94 (28.06) 33.69 (12.44) 19.25 47.93 (19.33) 59.70 (27.02) 11.77 Tangible support
10.83 (8.83) 5.33 (5.26) 5.50 7.24
(5.50) 12.80 (7.07) 5.56 Belonging support
11.91 (8.34) 6.27 (4.58) 5.64 11.93
(5.89) 13.78 (8.63) 1.85 Self-esteem support
15.40 (4.84) 10.86 (4.66) 4.54 16.75 (2.22) 15.81 (6.49) 0.94 Appraisal support
14.80 (8.29) 11.07 (6.45) 3.73 12.00 (7.97)
17.31 (7.56)
39
Table 11: Carer Satisfaction with Different Aspects of Safe Families Provision
Average Rating (0=Low,
10=High)
N
Host Family 9.50 10
Family Friend 9.20 5
Resource Friends 9.33 3
Family Support Manager 9.27 11
Family Coach 9.56 9
Overall 9.82 11
Recommend to a friend 9.73 11
Is there any evidence of impairment to the well-being of children
supported by Safe Families?
Success would mean no deterioration (that is, no harm) to children from families
receiving the intervention, and ideally an improvement in well-being and mental health.
We measured child well-being using a widely applied measure known as the Strengths and Difficulties Questionnaire that captures 4 domains of mental health - emotional difficulties, conduct problems, hyperactivity and peer relationships - as well as children’s capacity to act in pro-social ways; for example, helping others. The results are
40
Table 12: Children’s Mental Health and Pro-social Behaviour
Pre-test Mean (SD) Post-test Mean (SD)
Subscale Control
(n=27) Intervention (n=22) Differ Control (n=12) Intervention (n=18) Differ
Total Difficulties 15.70 (6.09)
20.82 (6.33) 5.12 17.25
(4.33)
17.50 (7.97)
0.25
Emotional
symptoms 3.63 (2.53) 5.00 (2.71) 1.37 4.17 (2.86) 3.89 (2.85) 0.28
Conduct problems
4.30 (2.18) 5.18 (2.17) 0.88 5.00 (1.48)
4.61 (2.43) 0.39
Hyperactivity/att
ention 4.33 (3.10) 6.41 (3.03) 2.08 4.75 (2.26) 4.83 (3.09) 0.08
Peer
relationships problems
3.44 (1.40) 4.23 (1.82) 0.79 3.33 (1.61)
4.17 (2.12) 0.84
Pro-social behaviour
8.22 (1.78) 7.09 (2.67) 1.13 7.50 (1.73)
7.83 (1.76) 0.33
(Notes: higher scores indicate poor outcomes on all scales apart from pro-social scale, and a mean change score of below zero indicates average reductions in scores, with positive figures indicating increases in scores.)
As can be seen, prior to the intervention beginning, the Safe Families group had poorer scores than the control group on all the domains, but had improved to the level of the control group by the time of follow-up. The deteriorating situation of the children in the control group - that is, not receiving Safe Families’ support - would signal concern were it evident in many more cases.
41
Conclusions and Recommendations
The previous pages have mostly reported what Safe Families does, how the programme developed and what the evaluation discovered. In this section, we set out our reflections on those findings, offering opinions on how the innovation is performing and how it could do better.
For the most part, Safe Families should be regarded as a successful innovation, one that has the potential to transform children’s services in England and pave the way for others to follow and build upon. It offers pointers to how to respond differently to children, who have consistently been shown, in research studies over the last 3 decades, to benefit little from - and occasionally be harmed by - traditional admission to care practice. Future evaluations should explore the impact on groups such as older adolescents, for whom innovation has been scant and untested.
Among the indicators of success, we point to going from a start up charity to delivering services supporting several hundred children in 20 local authorities within a 2 year period.
We can only speculate on why it has scaled, but our experience leads us to stress the following:
there was a good scale strategy rooted in evidence relevant to public systems
the innovation is simple and well explained
it is right for the political and social context, effectively linking public systems with civil society
there is a clear pull from the primary purchaser, local authority children’s services
Safe Families’ leadership invested a lot of what we came to call ‘sweat equity’, spending much more time than anticipated with local authority managers on
working through routine problems - as did Safe Families staff - learning to respond to local demand such as the Friday afternoon crisis that causes major headaches for local authority social workers.
42
Safe Families identified people in society who want to help families, and it matched volunteers’ capability and capacity to the different roles of supporting needy families. Safe Families is drawing out those who want to befriend, provide resources or take in other people’s children for short periods. These people appear to be in plentiful supply: they do not seek financial remuneration and are not over burdened by unreasonable requests - for example, to take in children for longer periods than they can comfortably manage.
This finding-and-matching process has resulted in high levels of consumer satisfaction among volunteers and families in need. Foster carers are known for their ability to forge close bonds with their foster children, but perhaps they are less known for their work with the birth parents. Safe Families’ volunteers appear to be doing both, and it is noteworthy that, in some cases, the bond results in a relationship that outlasts the involvement of both local authority and Safe Families. As one social worker commented to us about one of his cases:
“Safe Families was a really positive experience for this family, and their support through hosting prevented the family from being in crisis, and potentially could have led to the children having to be placed outside of the immediate family without this support. The family have continued the hosting arrangement despite Safe Families officially withdrawing due to the friendship between children in both families.”
Public system satisfaction with Safe Families is also high, as evidenced by the 20 local authorities that were prepared to buy the intervention at the end of the one year trial period, despite the evaluation data not being available. This attraction, essential to the effective scaling of interventions, has extended beyond the 20 early adopter local authorities to another 10 potential users in different parts of the country. Such buy-in is remarkable, given the restrictions on local authority finances.
Safe Families should also be commended for undertaking evaluation that gives tentative evidence for the principle of ‘first do no harm’. It is worth reflecting that if Safe Families is at least as good as foster and residential care in terms of birth parent and child
outcomes, it represents a better proposition to local authorities because it keeps children in their home environment, supports the family for longer periods of time and engages civil society.
Lessons Learned
43
funding within the 2015/16 financial year greatly reduced leverage on local authority funds and resulted in many getting a much foreshortened free period. In addition, without the PSP, Safe Families would have taken their chances with orthodox commissioning arrangements, and it is doubtful they would have scaled to 20 local authorities under those conditions. Nonetheless, there are important lessons to be drawn from the trial.
In DSRU, the apps we produced to help local authorities match eligible cases to Safe Families provision in a timely way, and to collect well-being data from family members in a non-intrusive manner, were largely unsuccessful. Many local authorities could not make the referral app work on the desktop technology available, and social workers were
restricted in how they can use personal phones and tablets. Much of the outcome data was collected using old fashioned paper and pencil techniques. DSRU innovations were conceptually sophisticated but the technological follow-through was lacking. These failures may have fed into the less-than-hoped-for progress in reducing the amount of time between family crises and Safe Families response, where more needs to be done to make the average experience more like the best.
The randomised control trial, while important, is limited by lack of numbers. To some extent, the low numbers reflect the low number of children on the edge of care referred by local authorities and signed up by Safe Families. In addition, DSRU’s over zealous methodological approach caused discomfort for local authorities, and, in one case, severe irritation. There will need to be rigorous evaluation of the Safe Families
intervention in the future, not only for what it can tell us about the intervention, but also for what it will reveal about the experience of children coming into orthodox foster care. We have learned of the need for a practical balance between scientific rigour on the one hand, and the practicalities of supporting vulnerable children on the other. We did not achieve the right balance in this evaluation.
As has been noted, the impact of the system dynamic seminars was limited. The seminar leader drew on ideas based on research from the 1980s and 1990s, dealing with
knowledge that, 3 decades ago would have been well understood by leaders and middle managers in local authorities. The seminar leader observed that much of this wisdom - for example about the difference between the numbers of children in care and the flow of children into and out of care – appears to have diminished. Nonetheless, we were left with the impression that, in the majority of the 20 LAs studied, system dynamics were influencing the decisions of system leaders more than system leaders were successfully managing system dynamics.
44
Christian church to other faith and non-faith groups. As the evaluation came to an end, such experimentation was underway.
Challenges
Any start-up faces multiple challenges. Safe Families is no different. Here we focus mainly on 2: the difficulty of making the intervention a true alternative to local authority care, and of how to maintain continuity in scaling.
DSRU has put a lot of stress on the potential for Safe Families to act as a viable alternative for about 15% of children separated into local authority care, the 4,500 children aged 10 years or less entering under Section 20 of the Children Act 1989 in England each year. Some local authorities fail to see this potential. Maybe Safe Families is better used as part of a range of early help interventions.
We suggest, though, that there is a need that can be met by Safe Families. The legal basis for using Safe Families as an alternative to care has been established. We have found a steady flow of 15% of children coming into care that meet the Safe Families’ eligibility criteria in all 20 local authorities. Safe Families has shown that it can support such families, without causing harm, and while producing high levels of satisfaction among primary carers.
Second, many local authorities are under immense strain coping with budget cuts. By focusing on the populations that cause concern to elected members and senior staff, Safe Families can build its reputation. It can release pressure on local authorities, not least in the willingness it has shown to respond, in a timely way, to the Friday evening crisis when social workers have little time to think and few alternatives at hand.
Third, in 3 years’ time, when local authority budgets are likely to be further reduced, it is likely that many will turn to the array of early help services when looking for cuts. A service aimed at children and families that the local authority must support has much greater chance of surviving an economic downturn.
Fourth, innovat