This is a repository copy of Including patient choice in cost-effectiveness decision rules.
White Rose Research Online URL for this paper:
http://eprints.whiterose.ac.uk/10913/
Monograph:
Dixon, S. (2007) Including patient choice in cost-effectiveness decision rules. Discussion
Paper. (Unpublished)
HEDS Discussion Paper 07/06
eprints@whiterose.ac.uk https://eprints.whiterose.ac.uk/ Reuse
Unless indicated otherwise, fulltext items are protected by copyright with all rights reserved. The copyright exception in section 29 of the Copyright, Designs and Patents Act 1988 allows the making of a single copy solely for the purpose of non-commercial research or private study within the limits of fair dealing. The publisher or other rights-holder may allow further reproduction and re-use of this version - refer to the White Rose Research Online record for this item. Where records identify the publisher as the copyright holder, users can verify any specific terms of use on the publisher’s website.
Takedown
If you consider content in White Rose Research Online to be in breach of UK law, please notify us by
- 1 -
HEDS Discussion Paper 07/06
Disclaimer:
This is a Discussion Paper produced and published by the Health Economics
and Decision Science (HEDS) Section at the School of Health and Related
Research (ScHARR), University of Sheffield. HEDS Discussion Papers are
intended to provide information and encourage discussion on a topic in
advance of formal publication. They represent only the views of the authors,
and do not necessarily reflect the views or approval of the sponsors.
White Rose Repository URL for this paper:
Once a version of Discussion Paper content is published in a peer-reviewed
journal, this typically supersedes the Discussion Paper and readers are invited
to cite the published version in preference to the original version.
Published paper
None.
H
H
e
e
a
a
l
l
t
t
h
h
E
E
c
c
o
o
n
n
o
o
m
m
i
i
c
c
s
s
a
a
n
n
d
d
D
D
e
e
c
c
i
i
s
s
i
i
o
o
n
n
S
S
c
c
i
i
e
e
n
n
c
c
e
e
D
D
i
i
s
s
c
c
u
u
s
s
s
s
i
i
o
o
n
n
P
P
a
a
p
p
e
e
r
r
S
S
e
e
r
r
i
i
e
e
s
s
No. 07/06
INCLUDING PATIENT CHOICE IN
COST-EFFECTIVENESS DECISION RULES
Simon Dixon
11.
Health Economics and Decision Science, School of Health and Related
Research, University of Sheffield.
Corresponding author:
Dr Simon Dixon
HEDS, ScHARR, University of Sheffield
Regent Court, 30 Regent Street, Sheffield, UK, S1 4DA
Tel: +44 (0) 114 2220724
Fax: +44 (0) 114 2224095
email : s.dixon@sheffield.ac.uk
Abst r act
There has been incr easing discussion in t he econom ic lit er at ur e, about t he appr opr iat eness of using gener al populat ion values wit hin t echnology appr aisal. This paper pr oposes an alt ernat ive appr oach t o incor por at ing pat ient values int o t he cost - effect iveness decision rule t hat lies at t he heart of funding decisions. Whilst t he cur r ent decision r ule is const ruct ed around a t echnical quest ion, nam ely, ‘which t reat m ent is t he m ost cost - effect ive?’, t he key policy quest ion is ‘w hich t r eat m ent s should be offer ed t o t he pat ient ?’. A t w o- part decision rule is explor ed w hich gives t he pat ient t he choice of t he m ost cost - effect ive t r eat m ent plus all cheaper opt ions. Whilst t he adopt ion of t his pat ient based cost
-effect iveness rule m ay not alt er m any decisions com par ed t o t he cur r ent
appr oach, it w ould r epr esent a pr ofound shift in t he w ay t hat pat ient values and pat ient choice ar e incor por at ed int o econom ic evaluat ion.
Ba ck grou n d
Pur chasers of healt h car e acr oss t he w orld incr easingly m ake decisions about w hich t r eat m ent s can be used by pat ient s using cost - effect iveness consider at ions. Wit hin t his fr am ew or k, effect iveness is m ost fr equent ly m easur ed using qualit y-adj ust ed life year s ( QALYs) . QALYs ar e calculat ed by sum m ing m or bidit y w eight ed life- expect ancy, wit h t he w eight s t ypically based ar ound m ean values gener at ed fr om a sam ple of t he gener al populat ion. The w eight s r epr esent valuat ions of healt h- r elat ed w ell- being ( or ut ilit y) , and are anchor ed on 1 ( r epr esent ing full- healt h) and 0 ( r epr esent ing deat h or healt h st at es consider ed t o be equivalent t o deat h) .
There has been incr easing discussion in t he econom ic lit er at ur e, about t he appr opr iat eness of using t hese gener al populat ion values wit hin t echnology appr aisal ( Br azier et al., 2005) . I t is ar gued, by som e, t hat pat ient values ar e bet t er est im at es of healt h- r elat ed w ell- being as pat ient s have fir st hand
experience of t he healt h st at e. Describing a part icular healt h st at e, t hen asking a m em ber of t he gener al public t o place a value on it , is pot ent ially flaw ed by t he lim it at ions of t he descript ive syst em used t o descr ibe t he healt h st at e and t he abilit y of a m em ber of public t o im agine what it is like t o be in t hat healt h st at e. Given t hese pr oblem s, it is lit t le w onder t hat large differ ences bet w een pat ient and public values ar e obser ved.
Despit e t hese pr oblem s, t he use of gener al populat ion values cont inue t o dom inat e t echnology appr aisals, alt hough t he r easons for t his t end t o focus on t he pot ent ial disadvant ages of using pat ient values. One gr oup of influent ial econom ist s ar gued t hat societ y should adopt a ‘veil of ignor ance’ w hen choosing healt h st at e values t o pur posely avoid t he influence of self int er est ( Gold et al., 1996) . Such self int er est , it has been ar gued, can lead t o st r at egic behaviour w hen collect ing healt h values. Anot her pr oblem avoided by t he use of populat ion values is t hat som e aspect s of pat ient values m ay w ant t o be excluded fr om our valuat ion of healt h out com es. Adapt at ion, it is ar gued can lead t o pat ient s being sat isfied wit h t heir dim inished funct ioning, t hus leading t o higher t han expect ed values, and conver sely, low er t han expect ed gains fr om t r eat m ent .
2
pr oblem s associat ed wit h t heir lack of exper ient ial know ledge. Whilst t her e is an incr easing am ount of w or k ar ound pat ient values, and t heir r ole wit hin t echnology appr aisal, t he cost - effect iveness decision rule t hat lies at t he hear t of funding decisions has rem ained unquest ioned.
Th e cu r re n t cost - effe ct iv e ne ss ru le
The cost - effect iveness r ule used r out inely in t echnology appr aisal is t hat for any given m onet ar y value placed on healt h ( or a QALY) , t he recom m ended t r eat m ent for funding is ident ified as t hat w it h t he highest incr em ent al cost - effect iveness r at io ( I CER) t hat falls beneat h t his t hr eshold value1.
This cost - effect iveness rule can be illust r at ed using Table 1. ‘Do not hing’
r epr esent s a sit uat ion where no act ive t her apy is given t o t he pat ient , t r eat m ent s ‘A’, ‘B’ and ‘C’ ar e new , m or e expensive t her apies. Using t he cur rent decision r ule, and a t hr eshold value of £30 000 per QALY, w e see t hat t r eat m ent A is deem ed t he m ost cost - effect ive, and is t her efore r ecom m ended for pat ient s wit h t he condit ion.
Ta ble 1 : Cost - e ffe ct iv en e ss of fou r h y pot he t ica l t r e a t m en t choices
Tr eat m ent Cost QALYs I ncr em ent al cost
-effect iveness r at io r elat ive t o DN
I ncr em ent al cost -effect iveness r at io
r elat ive t o next best opt ion
C 100 000 5.5 39 600 100 000
A 50 000 5.0 24 500 20 000
B 20 000 3.5 38 000 38 000
Do not hing ( DN) 1 000 3.0
How ever , t he curr ent decision rule is const ruct ed ar ound a t echnical quest ion, nam ely, ‘which is t he m ost cost - effect ive t r eat m ent ?’, w hen t he quest ion t hat should be asked is ‘which t r eat m ent s should be offer ed t o t he pat ient ?’. Under t he cur r ent rule, som e pat ient choice r em ains as a pat ient can not be for ced t o accept t he t her apy deem ed m ost - cost - effect ive; t hey act ually have t he choice of ‘Do not hing’ and ‘A’. How ever , som e pat ient s m ay pr efer t r eat m ent ‘B’ over t r eat m ent ‘A’, but ar e not allow ed t his under t he decision rule, even t hough it is expect ed t o cost less t han A.2
This sit uat ion is pr oduced because m ean ex post gener al populat ion values and
ex ant e individual pat ient values r ank t he t reat m ent s differ ent ly; populat ion
values suggest t hat t r eat m ent ‘A’ is pr efer r ed, whilst pat ient values suggest t hat t r eat m ent ‘B’ is pr efer r ed. I t also pr oduces an inconsist ency w it h r espect t o t he im plied pat ient choice w it hin t he cur r ent decision rule; pat ient s are able t o choose one t r eat m ent w hich cost s less but is deem ed less effect ive based on m ean
gener al populat ion values ( i.e. ‘Do not hing’) , but not anot her ( i.e. ‘B’) .
1
Although the decision rule should relate to the increment relative to the next best option, the rule is frequently operationalised with the increment relating to ‘do nothing’ or ‘current treatment’. 2
[image:6.595.86.510.351.451.2]Whilst t his is an int er est ing hypot het ical exam ple, is it likely t o happen in t he r eal w or ld?
Th e ca se of ost e opor osis
Nat ional I nst it ut e for Clinical Excellence ( NI CE) Technology Appr aisal 87 ( NI CE 2005) set s out r ecom m endat ions for t he use of bisphosphonat es, select ive oest r ogen r ecept or m odulat or s and par at hyr oid hor m one for t he secondar y pr event ion of ost eopor ot ic fr agilit y in post m enopausal w om en. The cost -effect iveness analysis for t his appr aisal is com plex w it h alt ernat ive figur es pr oduced for alt er nat ive evidence bases, and pat ient populat ions described in t er m s of age and bone m iner al densit y. A sum m ar y of t he r esult s ar e given in Table 2, which includes a single bisphosphonat e ( as opposed t o t he t hr ee w hich w er e assessed) , r aloxifene, oest r ogen, and t eripar at ide.
I n sum m ar y, t he guidance r ecom m ended bisphosphonat es as t he preferr ed t r eat m ent , w it h t he opt ion for using r aloxifene if bisphosphonat es w er e cont r aindicat ed, pr oduced an unsat isfact ory r esponse or if pat ient s w ere
physically unable t o com ply w it h t he st r ict direct ions for t aking bisphosphonat e m edicat ions ( NI CE 2005) . The use of bisphosphonat es ent ails fast ing and
ingest ion of m edicat ion at least 30 m inut es befor e br eakfast and rem ain st anding for 30 m inut es aft er t aking t he t ablet .
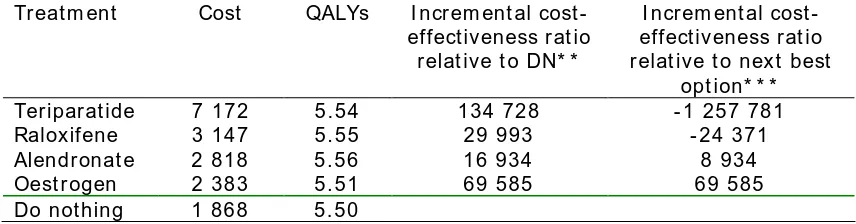
Ta ble 2 : Cost - e ffe ct iv en e ss of t r ea t m e n t s for t h e se con da r y pr e v en t ion of ost e opor ot ic fr a gilit y in post m e n opa usa l w om e n a t 7 0 y ea r s of a ge *
Tr eat m ent Cost QALYs I ncr em ent al cost
-effect iveness r at io r elat ive t o DN* *
I ncr em ent al cost -effect iveness r at io r elat ive t o next best
opt ion* * *
Ter ipar at ide 7 172 5.54 134 728 - 1 257 781
Raloxifene 3 147 5.55 29 993 - 24 371
Alendr onat e 2 818 5.56 16 934 8 934
Oest r ogen 2 383 5.51 69 585 69 585
Do not hing 1 868 5.50
* Som e t r eatm ent s and analyt ic scenar ios have been excluded fr om t he full t able pr esented by Stevenson and colleagues ( 2005) for sim plicit y.
* * Figures taken fr om report . I CERs based on m odel estim ates, w hilst costs and QALYs ar e r ounded.
* * * Figures calculated fr om t able, as they are not available fr om t he report . I CER for Oest r ogen kept t he sam e as in previous colum n for consistency.
The NI CE guidance did not allow pat ient s t he choice of t aking oest r ogen, even t hough it is possible t hat t hey w ould consider t he lifest yle r est rict ions associat ed w it h alendr onat e as being disr upt ive t o t he ext ent t hat oest r ogen w as consider ed pr efer able. I n such a sit uat ion, t he pat ient w ould be offer ed a t r eat m ent t hat t hey consider ed t o be w or se and m or e expensive ( alendr onat e) . Only if t hey w er e “ physically unable” t o follow t he t reat m ent dir ect ions w ould t hey be allow ed t o even consider anot her t r eat m ent choice ( r aloxifene) , and t hen not oest r ogen.
[image:7.595.83.511.412.524.2]4
highlight t he pot ent ial for cheaper , pat ient - pr efer r ed t r eat m ent opt ions t o exist in r eal life and t o be om it t ed fr om t r eat m ent opt ions by r eim bursem ent aut hor it ies.
A pa t ie n t - ba se d cost - e ffe ct iv en e ss r u le
Clear ly, t he cur r ent decision r ule is capable of producing uncom fort able scenar ios t hat are gener at ed by differ ences bet w een m ean gener al populat ion values and individual pat ient values. Som e w or k has been under t aken t o assess t he feasibilit y of calculat ing pat ient specific I CERs ( Sculpher 1998) . How ever , t his appr oach requir es t he elicit at ion of ex ant e healt h st at es fr om all pat ient s r equir ing t r eat m ent so as t o calculat e individual expect ed QALYs, w hich is a daunt ing pr ospect .
A part ial resolut ion of t he pr oblem is t o r efor m ulat e t he cur r ent decision rule so t hat it bet t er r eflect s t he key quest ion of ‘which t r eat m ent s should be offer ed t o t he pat ient ?’. The pr oposal r aised her e, is t o allow pat ient s t o have a choice over t he m ost cost - effect ive t her apy ( as adj udged by m ean gener al populat ion
values) , t hose t r eat m ent s t hat are less cost ly t han t he cost - effect ive t her apy, and ‘do not hing’. Pat ient s w ould not be given t he choice of t her apies t hat ar e m or e expensive and m or e cost ly t han t he m ost cost - effect ive t her apy ( for exam ple, ‘C’ in Table 1) .
This reflect s a t w o part decision pr ocess; t he ident ificat ion of t he m ost cost -effect ive t her apy using m ean gener al populat ion values ( i.e. t he cur r ent r ule) , t hen r elat ive t o t hat , t he ident ificat ion of t hose t r eat m ent s t hat ar e cheaper t han t he m ost cost - effect ive t her apy.
Under t his pat ient - based cost - effect iveness rule, if a pat ient pr efer s a t r eat m ent such as ‘B’ in Table 1 ( or oest r ogen in Table 2) , t hey should be able t o choose it . I n effect t hey have adjudged t hat t heir w ell- being w ill be gr eat er under ‘B’ t han for ‘A’ and t he m ean cost s ar e low er . I n ot her wor ds, w hen assessing t he
pat ient - pr efer ence I CER, ‘B’ dom inat es. Tr eat m ent ‘C’ w ould not be offer ed even if t he pat ient chose it , as t he incr eased w ell- being needs t o be t r aded- off wit h incr eased cost s.
One fur t her issue is w ort h consider at ion. I t is possible t hat a for m of adver se select ion could exist , wher eby t hose w ho choose B are expect ed t o have cost s m uch gr eat er t han t he m ean populat ion values ( i.e. £20 000) . This w ould r esult in higher pat ient w ell being but pot ent ially ver y high cost s. This can be guar ded against by using sub- gr oup analyses t o see if t hey belong t o a pat ient gr oup who ar e expect ed t o have higher cost s t hat A.
Pot en t ia l pr oble m s
Tw o issues ar e w or t h furt her consider at ion. Fir st ly, t he nat ur e of t he cost savings pr oduced by t he pr oposed rule, as t hese ar e not cert ain. Secondly, t he ‘validit y’ of a rule w hich offer s a pr agm at ic solut ion w it h no t heor et ical base.
Nat ur e of t he cost savings
The pat ient - based cost - effect iveness rule offer s t he possibilit y of pat ient s choosing a cheaper t r eat m ent ( ‘B’) t han t hat recom m ended using t he cur r ent appr oach ( ‘A’) . How ever , it is possible t hat w it hout t his choice, som e pat ient s w ould have chosen ‘do not hing’. I n such cir cum st ances, t he offer of an
alt er nat ive t r eat m ent ( ‘B’) r aises t he possibilit y of incr eased cost s. Consequent ly, w het her t he pr oposed rule is cost - saving or cost - incr easing at t he populat ion level, is an em pir ical quest ion.
Theor et ical validit y of t he rule
Whilst t he pr oposed rule has been descr ibed in t he cont ext of cost - effect iveness decisions, and t aps int o not ions of a pat ient - pr efer ence I CER, it does not have t he t heoret ical base of cost - effect iveness analysis. I t is a pr agm at ic solut ion, t hat m ixes t oget her societ al and pat ient per spect ives. I t could also be ar gued t hat t he w ider choice it pr ovides m oves aw ay fr om t he not ion of t he public pr ovision of healt h care, t o a social insur ance m odel w her e pat ient s have a right t o choose fr om a m enu of appr oved t r eat m ent s.
So, does t he lack of a t heoret ical foundat ion and t he m ixing up differ ent per spect ives w it hin a decision rule invalidat e t he r ule? I t is clear t hat t he NHS does not oper at e a single all- encom passing evaluat ive fr am ew or k. Whilst ext r a-w elfarism is used by m any healt h econom ist s t o j ust ify t he pr edom inant
evaluat ive fr am ew or k used by t hem selves, t he NHS uses a r ange of decision m aking cr it eria fr om a m ixt ur e of sources; t heoret ical, pr agm at ic and polit ical.
These differ ent view s ar e r ecognised by Drum m ond and colleagues ( Dr um m ond et al, 2005) who cont r ast t he pr agm at ic ‘decision- m aking appr oach’ wit h t he t heoret ical appr oaches of w elfarism and ext r a- welfarism . The rule for w ar ded in t his paper is clear ly pr agm at ic, and fr om a decision- m aking per spect ive, I w ould ar gue t hat it s desir abilit y can be evaluat ed. The decision m aker needs t o
evaluat e w het her t he benefit s t he rule confer s in t er m s of gr eat er choice and gr eat er healt h benefit s as evaluat ed by t he pat ient , ar e w ort h t he pot ent ial ext r a cost and reduced healt h benefit s as evaluat ed by a populat ion t ar iff.
Su m m a r y
Cost - effect iveness r ules have developed t o answer a t echnical quest ion, wit hout due regar d for pat ient choice. Am ending t his rule allow s gr eat er choice for t he pat ient w it hout necessarily incr easing t he pr ogram m e cost . How ever , using t he m et ric of gener al populat ion values t his alt ernat ive decision r ule r educes healt h gains. This loss of ex post societ y- valued healt h gain m ust be balanced against t he increase in pat ient choice and ex ant e pat ient - valued healt h gain. Whet her societ y is w illing t o bear t he pot ent ial ext r a cost for t hese gains becom es t he cent r al quest ion.
6
possible t hat such cir cum st ances ar e r ar e, and m ade r arer st ill by t he use of non-cost effect iveness infor m at ion in t he decision process t o account for pat ient
Re fer e nces
Br azier J, Akehur st R, Br ennan A, Dolan P, Claxt on K, McCabe C, Sculpher M, Tsuchiya A. Should pat ient s have a gr eat er r ole in valuing healt h st at es? Applied
Healt h Econom ics and Healt h Policy 2005; 4: 210- 208.
Dr um m ond MF, Sculpher MJ, Tor r ance GW, O’Brien BJ, St oddar t GL. Met hods for t he econom ic evaluat ion of healt h care pr ogr am m es. Thir d edit ion. Oxfor d: Oxfor d Univer sit y Pr ess, 2005.
Gold M, Siegel J, Russell L, Weinst ein M. Cost - effect iveness in healt h and m edicine. New Yor k: Oxfor d Univer sit y Pr ess, 1996.
Nat ional I nst it ut e for Clinical Excellence. Bisphosphonat es ( alendr onat e,
et idr onat e, risedr onat e) , select ive oest ogen r ecept or m odulat or s ( r aloxifene) and par at hyr oid horm one ( t er ipar at ide) for t he secondar y pr event ion of ost eopor ot ic fagilit y fr act ur es in post m enopausal w om en. London: Nat ional I nst it ut e for Clinical Excellence, 2005.
Sculpher M. The cost - effect iveness of pr efer ence- based t r eat m ent allocat ion: t he case of hyst er ect om y ver sus endom et rial r esect ion in t he t r eat m ent of
m enor rhagia. Healt h Econom ics 1998; 7: 129- 142.
St ephenson, Lloyd Jones M, De Nigris E, Br ew er N, Davis S, Oakley J. A syst em at ic r eview and econom ic evaluat ion of alendr onat e, et idr onat e, r isedr onat e, r aloxifene and t eripar at ide for t he pr event ion and t r eat m ent of post m enopausal ost eopor osis. Healt h Technology Assessm ent 2005 ; 9( 22) .
Weinst ein MC. Principles of cost - effect ive r esour ce allocat ion in healt h car e or ganizat ions. I nt er nat ional Journal of Technology Assessm ent in Healt h Car e 1990; 6: 93- 105.
Ackn ow le dge m e n t s
The aut hor w ould like t o t hank Pr ofessor John Br azier , Pr ofessor Ron Akehur st and Dr Colin Gr een for helpful com m ent s, and Dr Mat t St evenson for com ing up t he ost eopor osis exam ple. How ever , t he paper m ay not r epr esent t heir view s on t his issue.