The Dissertation on
INCIDENCE OF ACUTE KIDNEY INJURY IN PATIENTS WITH
ACUTE MYOCARDIAL INFARCTION
submitted to
THE TAMILNADU DR.M.G.R.MEDICAL UNIVERSITY
CHENNAI- 600 032
in partial fulfilment of the regulations for the award of the degree of
MD GENERAL MEDICINE
BRANCH – I
DEPARTMENT OF GENERAL MEDICINE GOVERNMENT KILPAUK MEDICAL COLLEGE
CHENNAI – 600 010 TAMIL NADU, INDIA
CERTIFICATE
This is to certify that this dissertation titled “INCIDENCE OF ACUTE KIDNEY INJURY IN PATIENTS WITH ACUTE MYOCARDIAL INFARCTION” has been done by Dr.M.SUBASHRI under the supervision and guidance of Prof.Dr.A.SHAIK SULAIMAN MEERAN MD., at the Department of General Medicine, Government Kilpauk Medical College, Chennai, during the Academic year 2015-2018, and is being submitted to The TamilNadu Dr.M.G.R.Medical University, Chennai in partial fulfilment of the University regulations for the award of the M.D. (GENERAL MEDICINE) Degree Examination to be held in May 2018.
Prof. Dr.A.Shaik Sulaiman Meeran MD., Prof. Dr.K.V.Rajalakshmi MD., Guide and Professor of Medicine HOD & Professor of Medicine Department of General Medicine Department of General Medicine Govt. Kilpauk Medical College Govt. Kilpauk Medical College
Chennai – 10 Chennai - 10
Prof. Dr.Ashok Victor M.D., D.M., Co-guide & Professor of Cardiology Department of Cardiology,
Govt. Kilpauk Medical College/ GRH, Chennai.
Prof.Dr.P.VASANTHAMANI MD, DGO, MNAMS,DCPSY,MBA THE DEAN
DECLARATION
I, Dr.M.SUBASHRI, solemnly declare that this dissertation “INCIDENCE OF ACUTE KIDNEY INJURY IN PATIENTS WITH ACUTE MYOCARDIAL INFARCTION ” is the bonafide work done by me at the Department of General Medicine, Government Kilpauk Medical College and Hospital, Chennai, during the period of April 2017 to September 2017, under the guidance and supervision of Prof.Dr.A.SHAIK SULAIMAN MEERAN M.D., Professor of General Medicine, Government Kilpauk Medical College, Chennai - 600 010. This dissertation is submitted to The Tamil Nadu Dr.M.G.R. Medical University, Chennai in partial fulfilment of the University regulations for the award of degree of MD GENERAL MEDICINE examinations to be held in MAY 2018.
Place: Chennai. Date:
ACKNOWLEDGEMENT
My sincere thanks to Prof.Dr.P.VASANTHAMANI MD, DGO, MNAMS,DCPSY,MBA., the Dean, Government Kilpauk Medical College and Hospital for giving me permission to commence this dissertation and use the resources of this institution.
I wish to express my profound thanks to my esteemed professor and teacher, Prof.Dr.K.V.RAJALAKSHMI M.D., Professor and HOD of Medicine, Department of General Medicine for encouraging and extending invaluable guidance to perform and complete this dissertation.
I owe my sincere gratitude to Prof.Dr.A.SHAIK SULAIMAN MEERAN M.D., Department of General Medicine, Government Kilpauk Medical College, Chennai for his constant encouragement & guidance, for the liberty given to me throughout & for his resolute personality that helped me prepare and complete this study.
I wish to express my grateful thanks to Prof. Dr.ASHOK VICTOR M.D. D.M, Department of Cardiology, Government Kilpauk Medical College, Chennai for his invaluable guidance and for all his inestimable suggestions he gave me at every stage of this study.
I wish to express my grateful thanks to my previous chief Prof.Dr.R. MUTHUSELVAN MD., Department of General Medicine, for his masterly guidance in helping me choose this topic and for his valuable suggestions during every phase of this study.
I also extend my sincere thanks to my Assistant Professors DR.RANJANI MD., Dr.S.GEETHA M.D, DR.AGILA SARAVANAN M.D, DR. SANGEETHA M.D, and Dr. RAJA M.D, for their support.
I thank my colleagues, my seniors and juniors for their timely help, co-operation and support. I also extend my gratitude to my parents for all the support they gave during each stage of this study.
I also would like to thank the Institutional Ethics Committee, Kilpauk Medical College for approving my study.
CONTENTS
S.NO. TITLE PAGE
NO.
1. INTRODUCTION 3
2. REVIEW OF LITERATURE 6
3. AIM 32
4. METHODOLOGY 34
5. RESULTS 46
6. DISCUSSION 68
7. CONCLUSION 73
8. ANNEXURES
a) BIBLIOGRAPHY 75
b) PROFORMA 82
c) CONSENT FORM 84
d) PLAGIARISM CERTIFICATE 90
e) ETHICS COMMITTEE APPROVAL 91
1
ABBREVIATIONS
AKI - Acute Kidney Injury
AMI - Acute Myocardial Infarction
CAD - Coronary artery disease
SCr - Serum Creatinine
KDIGO - Kidney Disease: Improving Global Outcomes
eGFR - estimated Glomerular Filtration Rate MDRD - Modification of Diet in Renal Disease
CKD-EPI - Chronic Kidney Disease Epidemiology Collaboration
HbA1c - Glycated Hemoglobin
SBP - Systolic Blood Pressure
DBP - Diastolic Blood Pressure
TGL - Triglycerides
2
INCIDENCE OF ACUTE KIDNEY
INJURY IN PATIENTS WITH ACUTE
3
4
INTRODUCTION
Acute Kidney Injury (AKI) is a complex syndrome occurring due to various etiological factors, such as decreased intravascular fluid volume, decreased cardiac output, infections, drugs, etc. The spectrum of AKI ranges from mild elevation of serum creatinine to anuric renal failure leading on to a dialysis requiring stage.
The lack of a uniform definition led to conflicting epidemiological data on Acute Kidney Injury in various parts of the world, until 21st century.
The latest definition of AKI, as per Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group, 2012[1] is : AKI is defined as any of the following (Not Graded): Increase in Serum creatinine (SCr) by 0.3 mg/dl (X26.5 µmol/l) within 48 hours; or increase in SCr to X1.5 times baseline, which is known or presumed to have occurred within the prior 7 days; or urine volume 0.5 ml/kg/h for 6 hours.
5
infarction (AMI), the development of which is associated with unfavourable outcomes and higher mortality after an Acute myocardial infarction.
The mechanisms causing AKI in the first few days after an AMI are multifactorial, including systemic and renal hemodynamic changes secondary to an impaired cardiac output and an imbalance of vasodilators and vasoconstrictors, the use of contrast media, and immunological and inflammatory kidney damage resulting from crosstalk between the heart and the kidney [3].
Therefore, Acute Kidney Injury, if not identified & intervened at the earliest, may become partly irreversible or even progress to chronic kidney disease, which has a profound impact on cardiovascular outcomes in patients with acute coronary syndromes as well as in the general population.[2]. Worsening of renal function during admission for myocardial infarction is a powerful and independent predictor of in-hospital and 1-year mortality[4]
6
7
REVIEW OF LITERATURE
[image:13.612.237.403.434.672.2]Located in the retro-peritoneum, the pair of kidneys has a wide range of functions that are essential for life. Morphologically, each kidney contains approximately 1 million functional units, which are called nephrons. Each of these nephrons is made up of a renal corpuscle, also called glomerulus and a complex tubular portion which unifies to form collecting duct system. These nephrons are present in both outer cortex and inner medullary portion of the kidneys. The segmentation of a single nephron is such that, it comprises of renal corpuscle (with bowman’s capsule and glomerular tuft), proximal tubule, loop of Henle, distal tubule and collecting tubules. (Figure 1)
8
Physiologically, kidneys maintain water and electrolyte balance, excrete waste products such as urea, uric acid, creatinine, end-products of haemoglobin metabolism, drugs etc. It plays a vital role in maintaining acid-base balance in the body. The kidneys produce erythropoietin, a peptide hormone that stimulates red blood cell production in the bone marrow. Kidneys also are a source of gluconeogenesis, and are the actual site for production of the active form of Vitamin D (1,25-dihydroxyvitamin D3). The kidneys maintain sodium
and water balance in the body, which help in maintaining the blood volume, on which depends the blood pressure. Hence the kidneys play a crucial role in maintaining the arterial blood pressure, as well.
ACUTE KIDNEY INJURY:
The latest definition of AKI, as per Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group, 2012[1] is :
9
PATHOPHYSIOLOGY OF ACUTE KIDNEY INJURY :
Following ischemia, the sub-lethally injured renal cells release a number of cytokines, or Danger-Associated Molecular Pattern molecules (DAMPs) which include chromatin- associated protein high-mobility group box1, Adenosine triphosphate, uric acid, etc. These molecules activate immune effector cells, such as dendritic cells, which are responsible for activating immune mechanisms through Toll-like receptors and the nuclear factor- kappa B system. The DAMPs also activate complement cascades. (Figure 2)
10
Another type of de-differentiation involves conversion of renal cells into other cell types like phagocytes, which characteristically expresses Kidney injury Molecule – 1 (KIM-1). And these cells after de-differentiation have the ability of internalizing apoptotic bodies and necrotic cells. They also can remove irreversibly damaged cells when there is no infiltration of the actual macrophages.
Subsequently during the process of kidney injury and later recovery, there is deposition of cellular matrix components in the extracellular compartment. When the normal dynamic balance between cellular matrix production and degradation is hampered (which is otherwise maintained in normal kidneys), there is abnormal deposition of interstitial collagen I and III.
11
[image:17.612.137.433.309.670.2]and extracellular matrix deposition. Whereas, Hepatocyte Growth Factor antagonizes TGF- β1 and inhibits protein synthesis, and also directs cell regeneration and tissue repair against Transforming Growth Factor -β1 . Thus, recovery from injury occurs as a result of complex interplay of soluble mediators. Any disturbance in these mechanisms can cause intrinsic cell losses, glomerulosclerosis, and progressive interstitial fibrosis which are indications that there is incomplete renal recovery and the renal cells ultimately die.
12
ACUTE KIDNEY INJURY IN ACUTE MYOCARDIAL INFARCTION:
Acute kidney injury (AKI) is a common complication occurring in patients with acute myocardial infarction (AMI) and other critical illness. In recent times, there has been an increased interest in studying the association between worsening renal function during hospitalization and the risk of short- and long-term mortality in various cardiac conditions. [5] [6]
A considerable proportion of patients admitted to the hospital,
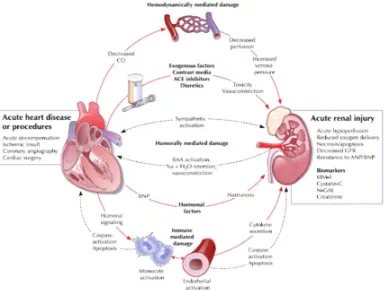
especially to the critical care setting, have cardiac or renal dysfunction. And the disease of one of the two organs affects adversely by causing injury or dysfunction secondarily in the other organ, through complex neuro-humoral feedback mechanisms (Figure 3). Hence an acute & rapidly worsening heart can cause acute renal injury. This process can occurs in the setting of hypertensive pulmonary oedema with preserved left ventricular systolic function , cardiogenic shock, right heart failure or in acutely decompensated cardiac failure, acute myocardial infarction.
13
Figure 3: Pathophysiology of Cardio-renal syndrome- Type 1
14
In the setting of myocardial infarction, acute kidney injury occurs as a result of decreased renal perfusion, unless proved otherwise. This occurs due to decreased cardiac output in myocardial infarction and venous congestion in the renal system. There is also a state of decreased responsiveness to diuretics in congestive state, as a result of diminished effectiveness of the diuretic drug that occurs secondary to sodium retention following diuretic use. Hence diuretics, which are preferred in a setting of volume overload, and is given as continuous low-dose infusion so as to achieve gradual diuresis. Large bolus doses of diuretics cause more of extracellular volume loss, thereby decreasing effective arterial blood volume, which in turn decreases renal perfusion and aggravates renal injury.
15
urine output, a parameter that is used to assess renal function in state of acute kidney injury.
Yet another group of drugs of concern, is the beta-blockers if used in the setting where the stroke volume cannot be increased and the resultant tachycardia, either absolute or relative, helps to maintain adequate cardiac output, these beta-blockers abolish the compensatory tachycardia and inotropic compensation, mediated by the sympathetic system, and can hence precipitate or further worsen cardiogenic shock, thus leading to higher rates of mortality. [10] However, beta blockers, in particular atenolol or sotalol, which are excreted through the kidneys, can be administrated slowly and carefully once hemodynamic stability is achieved.
16
that an acute kidney injury accelerates cardiovascular pathological mechanisms by activating inflammatory pathways. [9]
If patients with acute myocardial infarction, who develop acute kidney injury, the changes in renal hemodynamics leads to under-treatment in such patients, as it precludes the use of beta- blockers and Angiotensin-converting enzyme inhibitors and Angiotensin receptor blockers, during the critical period of illness, if not all together in later stages. Raising renal parameters which signify worsening kidney function, per se, is an independent risk factor for both immediate and 1-year mortality in patients with Myocardial infarction.
It is very important to monitor the renal functions in these patients, because the use of radio-contrast dyes in therapeutic or diagnostic cardiac imaging, further precipitates renal failure in acutely injured kidneys. [11]
17
CHARACTERISTICS OF AN IDEAL BIOMARKER:
The characteristics feature of an ideal biomarker depends on the disease under investigation. However, the following characteristics are important any biomarker, in general: it should be
· Non-invasive, should be easily measurable, cost-effective, offer rapid
results.
· From readily available sources such as urine or blood.
· Highly sensitive, allowing early detection, and should not have
overlapping values between diseased patients and healthy controls.
· Highly specific, either greatly upregulated or downregulated specifically
in diseased patients and not affected by other comorbid conditions.
· The levels of biomarkers should vary rapidly in response to treatment
· Aid in risk stratification and possess prognostic value in terms of
outcomes.
· Biologically plausible and offer insight into the underlying
18
AN IDEAL BIOMARKER FOR ASSESSMENT OF RENAL DISEASE: For a biomarker to be considered ideal in assessment of renal disease, the following features should be fulfilled. It should,
· Pinpoint the location of primary injury ( proximal tubule, distal tubule, interstitium or vasculature)
· Determine the duration of kidney failure (Acute or chronic or ‘acute on chronic’ kidney failure)
· discerning subtypes of Acute Kidney Injury (prerenal, intrinsic renal or postrenal)
· Identify the cause of Acute Kidney Injury (ischemia, toxin, sepsis or a combination of all these)
· Differentiate Acute Kidney Injury from other forms of acute kidney disease conditions such as urinary tract infection, glomerulonephritis, or interstitial nephritis, etc.
· Help in risk stratification and prognostication (duration and severity of AKI, need for renal replacement therapy, length of hospital stay and mortality)
· Define the course of Acute Kidney Injury
· Monitor the response to therapeutic interventions of AKI
19
Hence numerous attempts have been in vogue to find an ideal biomarker, which led to the discovery of a number of novel biomarkers which can identify Acute Kidney Injury. (Box: 1)
BOX:1 List of novel biomarkers which can identify AKI
BIOMARKER ASSOCIATED INJURY
Cystatin C Proximal Tubule Injury
KIM-1 Ischemia and nephrotoxins
NGAL(Lipocalin) Ischemia and nephrotoxins
NHE3 Ischemia, pre-renal, post-renal AKI Cytokines (6,
IL-8, IL-18)
Toxic, delayed graft function
Actin-actin
depolymerizing F
Ischemia and delayed graft function
α- GST Proximal tubular injury, acute rejection
π-GST Distal tubular injury, acute rejection L-FABP Ischemia and nephrotoxins, sepsis
Netrin-1 Ischemia and nephrotoxins
Keratin-derived chemokine
Ischemia and delayed graft function
20
Neutrophil gelatinase- associated lipocalin (NGAL):
Neutrophil gelatinase- associated lipocalin (NGAL) is detected in blood and serum in patients with AKI. It is an early predictor in both children & adults who undergo cardiac surgery or those who are admitted in Intensive Care setting, delayed graft function.[12]
Cystatin C :
Cystatin C in blood, does not appear to be affected by age, gender, race or muscle mass [13] . Studies say that it is a better predictor of glomerular function, predicts AKI and the need for renal replacement therapy. Both NGAL and Cystatin C together helps in assessing structural and functional derangement in acute kidney injury.
Kidney injury molecule- 1 (KIM-1):
21
However these biomarkers are not widely available for clinical use and are quite expensive. Studies are being conducted to prove their efficacy, so that these molecules become available for use on a day-to-day basis while monitoring renal functions in acutely ill patients. Hence, currently we rely on serum creatinine so as to diagnose acute kidney injury.
Creatinine:
22
Figure 4: Pathways of creatinine metabolism. (From Heyms eld SB, Arteaga
C, McManus C, et al. Measurement of muscle mass in humans: validity of
23
The generation of creatinine is dependent on age, gender and body weight, which in turn is affected by both diet and muscle mass. Hence in conditions involving muscle wasting, where there is decreased creatine pool, there is associated decreased creatinine generation and excretion.
Likewise a reduction in dietary protein again , reduces the availability of creatine precursors- such as, Arginine and Glycine by 5-15%. Therefore elimination of dietary creatine decreases urinary creatinine excretion by as much as 30% . During cooking, as much as 18- 65% of the creatine in meat is converted into creatinine, which get absorbed from the gastrointestinal tract, which causes a sudden increase in the serum creatinine concentration and urinary creatinine excretion transiently.
RENAL HANDLING OF CREATININE:
Creatinine is the most commonly used as an endogenous filtration marker ever since it was introduced by Jaffe more than 125 years ago[17] . Though the normal value of serum creatinine in healthy young individuals is 0.7 to 0.9 mg per dl, which is maintained by sufficiently functioning kidneys with normal GFR, the reference ranges varies among laboratories based on variation in serum creatinine assays.
24
Modification of Diet in Renal Disease (MDRD) formula :
For serum creatinine (Scr) in mg/dL:
eGFR= 186 x SCr -1-154 x Age-0.203 x [1.210 if Black] x [0.742 if female]
Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula:
eGFR = 141 x min 9Scr/k,1)a x max Scr/k,1)-1.209
x 0.993Age x [1.018 if female] x [1.159 if Black],
where SCr is serum creatinine (mg/dL), k is 0.7 for females and 0.9 for
males, a is −0.329 for females and −0.411 for males, min indicates the
minimum of SCr/k or 1, and max indicates the maximum of SCr/k or 1.
25
ROLE OF SERUM CREATININE IN DIAGNOSIS OF ACUTE KIDNEY
INJURY:
26
Figure 5: Relationship between serum creatinine and glomerular filtration
rate (GFR). Changes in serum creatinine represent smaller changes in
GFR as renal functions decreases. Creatinine increase from A to B
corresponds to a GFR decrease of GFR of 130 to 70 mL per minute,
whereas from B to C the same delta creatinine corresponds to a decrease in
GFR from 70 to 50 mL per minute. (Modified from Finn WF. The clinical
and renal consequences of contrast-induced nephropathy. Nephrol Dial
Transplant. 2006, 21(6):i2-i10.)
27
fluctuate. Hoste et al. showed that in a group of recently admitted intensive care unit patients with normal serum creatinine the 1-hour urinary creatinine clearance revealed values lower than 80 mL/min/1.73 m2 in 46.2% of the patients.[18] These data suggest that serum creatinine is not a reliable tool as it tends to raise only after acute insult to kidneys have already occurred.
Clinical Situations in Which Estimating Equations for Creatinine
Clearance or Glomerular Filtration Rate Measurements May Not be
Accurate and Clearance Measurements May be Recommended
Extremes of age & body size
Malnutrition or obesity Skeletal muscle disorders
Vegetarian diet
Rapidly changing kidney function
Pregnancy
28
MEASUREMENT OF CREATININE:
Creatinine can be measured easily in serum, plasma, and urine and a variety of methods are used by clinical laboratories. The National Kidney Disease Education Program (NKDEP) and the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) has helped in more accurate reporting of estimated GFR by standardizing serum creatinine assays to minimize differences in clinical laboratories. The reference standard for creatinine assay is isotope dilution mass spectrometry (IDMS) using either gas or liquid chromatography. All instruments can now be calibrated to standardized serum creatinine using secondary reference materials and testing programs. However, calibration does not eliminate the problem of interference by specific substances in serum with specific assays.
29
measurement can be greater, however, in diabetic ketoacidosis due to the increased concentration of acetoacetate, and in patients taking certain cephalosporins which can contribute to the colorimetric reaction. Very high serum bilirubin levels can cause falsely lower creatinine levels. (refer box below)
Medications and other Conditions That Affect Serum Creatinine without Actually Affecting Renal Function
Mechanism and Medication
Increased serum creatinine by the inhibition of creatinine secretion Trimethoprim
Cimetidine
Increased serum creatinine due to interference with creatinine measurement
Ascorbic acid Cephalosporins Flucytosine Plasma ketosis
Falsely low serum creatinine due to interference with creatinine measurement
Very high serum bilirubin levels (usually 5.85 mg/dL) Enhanced creatinine production
Cooked meat (creatine is converted to creatinine by cooking)
30
concentration in urine to interfere with creatinine measurement. Hence, measurement of creatinine clearance in normal individuals using the Jaffé reaction results in values that are approximately 20% lower than the true value. The kinetic alkaline picrate method takes advantage of the differential rate of color development for non-creatinine chromogens compared to creatinine. It significantly reduces, but does not eliminate, both types of positive interferences described earlier.
A survey by the College of American Pathologists (CAP) in 2004 found that assays based on the alkaline picrate method were the most widely used in clinical laboratories in the United States.
To circumvent interferences in the alkaline picrate reaction, other methods have been developed which are increasingly used by clinical laboratories. Enzymatic methods include the creatinine iminohydrolase and creatininase-creatinase- sarcosine oxidase methods. The antifungal agent, flucytosine, interferes with the creatinine iminohydrolase method, whereas bilirubin, dopamine, dobutamine, ascorbic acid, and sarcosine may interfere with the creatinase creatininase methods.
31
Utility Of Serum Creatinine As Marker Of AKI (From Previous Studies):
When serum creatinine was used as a marker of acute kidney injury, the results were such that the hazard ratio for developing End Stage Renal Disease was 41.2 (95% confidence interval [CI] 34.6 to 49.1) in patients who presented with Acute on Chronic kidney disease, 13.0 (95% CI 10.6 to 16.0) for patients with AKI and without previous CKD , and 8.4 (95% CI 7.4 to 9.6) for patients with CKD and without episodes of acute kidney injury, after adjusting for age, sex, race and co-morbidities like diabetes, hypertension, as per previous studies [16]
32
33 AIM OF THE STUDY
· To study the incidence of Acute Kidney Injury (AKI) in patients
admitted with Acute Myocardial Infarction
· To study the co-morbidities associated with development of AKI
34
35
SUBJECTS AND METHODS
This cohort study was done at Institute of Non-Communicable Diseases, Government Royapettah Hospital, Kilpauk Medical College, Chennai. Individuals who got admitted with Acute Myocardial Infarction in the Intensive Coronary Care Unit of Government Royapettah Hospital were included in the study. The period of study is 6 months. The Institutional Ethics Committee of Government Kilpauk Medical College, approved the study (Protocol ID. No.19/2017) and written informed consent of all participants was obtained.
INCLUSION CRITERIA:
Patients admitted with Acute Myocardial Infarction in Intensive Coronary Care Unit at Govt. Royapettah hospital were included in this study.
EXCLUSION CRITERIA:
· Age less than 18 years
36 SAMPLE SIZE:
With prevalence of Acute Kidney Injury In hospitalised Acute Myocardial Infarction patients of 14%, confidence level of 95%, non-response rate of 15% and accuracy level at 6%, the estimated sample size that is required for the study is 150.
37 CASE DEFINITIONS:
MYOCARDIAL INFARCTION:
According to the classic World Health Organization criteria, diagnosis of acute
myocardial infarction requires two of the following three criteria:
· A history suggestive of coronary ischemia for a prolonged period of time
(>30 minutes)
· Positive cardiac biomarkers or
· Electrocardiographic evidence of acute myocardial infarction.
38
ELECTROCARDIOGRAPHIC MANIFESTATIONS OF ACUTE MYOCARDIAL ISCHEMIA (IN THE ABSENCE OF LEFT BUNDLE BRANCH BLOCK):
ST Elevation :
New ST elevation at the J point in two contiguous leads with the following cut points:
• ≥0.1 mV in all leads (except V2-V3)
• In leads V2-V3 the following cut points apply:
• ≥0.2 mV in men ≥40 years
• ≥0.25 mV in men <40 years
• ≥0.15 mV in women
ST Depression and T Wave Changes:
• New horizontal or downsloping ST depression ≥0.05 mV in two contiguous leads
39
ELECTROCARDIOGRAPHIC CHANGES ASSOCIATED WITH
PREVIOUS MYOCARDIAL INFARCTION (IN THE ABSENCE OF LEFT VENTRICULAR HYPERTROPHY AND LEFT BUNDLE BLOCK)
· Any Q wave in leads V2-V3 ≥0.02 sec or a QS complex in leads V2 and
V3
· Q wave ≥0.03 sec and ≥0.1-mV deep or QS complex in leads I, II, aVL,
aVF, or V4-V6 in any 2 leads of a contiguous lead grouping (I, aVL; V1-V6; II, III, aVF)
· R wave ≥0.04 sec in V1-V2 and R/S ≥1 with a concordant positive T
40
ELECTROCARDIOGRAPHIC MANIFESTATIONS OF ISCHEMIA IN THE SETTING OF LEFT BUNDLE BRANCH BLOCK :
Electrocardiographic Criterion POINTS
ST-segment elevation ≥1 mm and concordant with the QRS complex
5
ST-segment depression ≥1 mm in lead V1, V2, or V3 3
ST-segment elevation ≥5 mm and discordant with the QRS complex
2
A score of ≥3 had a specificity of 98% for acute MI.
CARDIAC BIOMARKERS:
Cardiac Enzymes Normal reference values (ng/mL)
Troponin I <0.5
Creatine Kinase-MB <5.0
41 ACUTE KIDNEY INJURY:
AKI, as per Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group, 2012[1] is :
AKI is defined as any of the following (Not Graded): Increase in SCr by 0.3 mg/dl (X26.5 µmol/l) within 48 hours; or increase in SCr to X1.5 times baseline, which is known or presumed to have occurred within the prior 7 days; or urine volume 0.5 ml/kg/h for 6 hours.
Staging of Acute Kidney Injury (AKI) (according to KDIGO guidelines)
Stage Serum Creatinine Urine Output
1 1.5-1.9 times baseline (or)
≥0.3 mg/dl (≥26.5 µmol/l) increase
<0.5 ml/kg/h for 6–12 hours
2 2.0-2.9 times baseline <0.5 ml/kg/h for ≥12 hours 3 3.0 times baseline (or)
Increase in serum creatinine to ≥4.0 mg/dl (≥353.6 µmol/l) (or)
Initiation of renal replacement therapy (or) In patients <18 years, decrease in estimated Glomerular Filtration Rate (eGFR) to <35 ml/min per 1.73 m2
<0.3 ml/kg/h for ≥ 24hours (or)
42 HYPERTENSION:
As defined by Eighth Joint National Committee (JNC 8)
Blood Pressure Classification
SBP (mm Hg) DBP (mm Hg)
Normal <120 and <80
Pre-hypertension 120-139 or 80-89
Stage 1 Hypertension 140-159 or 90-99
Stage 2 Hypertension ≥ 160 or ≥ 100
SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure
DIABETES MELLITUS:
As defined by American Diabetes Association (ADA)
Random Blood Sugar- 200 mg/dL (or) Fasting Blood Sugar- 126 mg/dL (or)
HbA1c- >6.5%
43
METHODOLOGY
BASIC DEMOGRAPHICS:
After obtaining informed written consent, all individuals who meet the inclusion and exclusion criteria were included in the study. A basic demographic details, detailed clinical history, physical examination, and basic investigations were done and entered in the prescribed pro-forma on individuals admitted with acute Myocardial infarction. For the history of diabetes, hypertension and prior coronary artery disease, appropriate medical documents will be taken into account.
MEASUREMENT OF BLOOD PRESSURE:
Blood pressure was recorded in the supine position in the right arm to the nearest 2 mmHg with mercury sphygmomanometer (Diamond Deluxe BP apparatus; Pune, India). Two readings were taken 5 min apart, and the mean of the two was used.
BIOCHEMICAL PARAMETERS:
44
biomarkers estimation. Blood glucose levels, serum triglycerides and serum triglycerides levels and hemoglobin levels were estimated as well.
The plasma glucose (glucose oxidase-peroxidase method), serum total cholesterol (cholesterol oxidase-peroxidase amidopyrine method) serum triglycerides (glycerol phosphate oxidase-peroxidase amidopyrine method), serum creatinine (Jaffe’ method) were measured using a Roche Autoanalyzer. And haemoglobin levels were measured by spectrophotometry in autoanalyzer.
Cardiac biomarkers were measured by immuno-chromatography by Nanochecker 710 analyzer for the rapid qualitative and quantitative determination of three key cardiac enzymes (Myoglobin, CK-MB, Troponin I), which requires a very little quantity of as much as 80µL of whole blood or plasma.
These patients were followed up during a period of next 48 hours, and 3 ml of venous blood was again sent for serum creatinine estimation after 48 hours, to detect Acute Kidney Injury (urine output is not included as a criterion in our study) & the factors associated with the development of AKI were studied, while the treatment of Acute myocardial infarction were not compromised during the study.
45 STATISTICS:
The collected data were analysed with IBM.SPSS statistics software 23.0 Version. To describe about the data descriptive statistics frequency analysis, percentage analysis were used for categorical variables and the mean & S.D were used for continuous variables. To find the significant difference between the bivariate samples in Paired groups the Paired sample t-test was used & for Independent groups the Unpaired sample t-test was used. To find the significance in categorical data Chi-Square test and Fisher's exact test was used. In all the above statistical tools the probability value .05 is considered as significant level.
.
P-Value ** Highly Significant at P ≤ .01
P
-Value * Significant at 0.01 < P ≤ .05
P
46
47
RESULTS
BASELINE CHARACTERISTICS:
Table 1 illustrates the baseline characteristics of the entire study population. Out of the total 150 patients, the mean ± S.D. age of the patients was 60±9 years (Range: 36-85 yrs). The mean ± S.D. Systolic BP was 134±32 mm Hg (Range: 60-220 mm Hg) , and the mean ± S.D. Diastolic Blood pressure was 84±10 mm Hg (Range: 50-120 mm Hg).
The mean ± S.D of blood sugar on admission was 164±59 mg/dL. The mean ± S.D of serum creatinine at the time of admission was 0.9±0.3 mg/dL and at the end of 48 hours was 1.1±0.5 mg/dL. The mean ± S.D serum cholesterol value was 184±42 mg/dL and that of serum triglycerides was 131±61 mg/dL. The mean duration of chest pain in these patients was 6 hours (Range: 0-72 hours). And the mean ± S.D haemoglobin value was 12±1.5 gm/dl.
Out of 150 patients who were admitted with acute myocardial infarction 70 were female (46.7%) and 80 were male (53.3%).
48
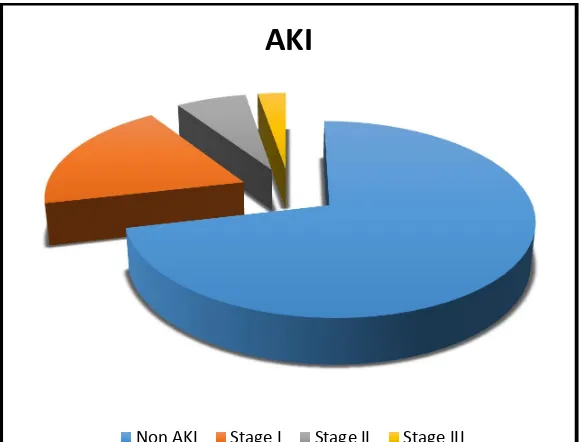
Table 3 represents, out of the total 150 patients, 107 patients did not develop Acute Kidney Injury (Non-AKI group) and 43 patients developed Acute Kidney Injury (AKI group). Of the 43 patients (28.6%) who developed AKI, 29 patient (19.3%) had Stage I AKI , 10 patients (6.7%) had stage II AKI, and 4 patients(2.7%) had stage III AKI. However in Fox C S et al study, the percentage of AKI in patients with acute myocardial infarction was only 16%
[23]
.
Table 4 indicates the total number of deaths during the hospital stay among 150 patients were 23 (15.3%).
From Table 5, the mean±S.D. age of 43 patients who presented with AKI was 63±10 years , which was higher compared to the mean age of patients in Non-AKI group and has p value= 0.027, significant at 0.01 < P ≤ .05. The mean±S.D systolic and diastolic BP of these AKI patients were 130±42 mm Hg and 84±12 mm Hg. The mean random blood sugar of the AKI patients was 154±52 mg/dL, which was however less than that of non-AKI patients.
Also, the mean±S.D of serum creatinine value at the time of admission of AKI patients was 0.9±0.3 mg/dL, which was same as that of non-AKI patients. And the mean±S.D. of serum creatinine value after 48 hours in AKI patients was 1.6±0.5 mg/dL, which was higher than that of non-AKI group, which was 0.9±0.2 mg/dL.
49
and that of serum triglycerides was 122±28 gm/dL and the mean hemoglobin value of patients who developed AKI was 11.8±1.7 gm/dL.
The mean duration of chest pain in patients who developed AKI was 10 hours, which was higher than that of non-AKI patients , and with a statistically significant p=0.009, which meant longer the duration of chest pain, more is the tendency to develop AKI in MI patients (Table 14).
COMPARISON OF ASSOCIATED RISK FACTORS AND COMORBIDITIES IN ACUTE MI AND DEVELOPMENT OF AKI
Table 6 shows, the percentage of female with Non-AKI was 48.6% and with AKI was 41.9%. But the comparison between sex and AKI shows no statistical significance ( p=0.454) which reveals there is no gender predilection for the development of AKI in MI patients.
Table 7 represents, the percentage of patients with history of hypertension with Non-AKI was 54.2% and percentage of patients with history of hypertension with AKI was 51.2%. By Chi-square test, the comparison between history of hypertension and AKI shows no statistical significance (p=0.736), which reveals the presence of history of hypertension is not associated with development of AKI in MI patients.
50
was 41.9%, which appears to be higher. But by Chi-square test, the comparison between history of diabetes and AKI shows no statistical significance (p=0.537) which again, reveals the presence of history of diabetes is not associated with development of AKI in MI patients
From Table 9, it is evident that the percentage of patients with history of Coronary Artery Disease (CAD) with Non-AKI was 23.4% and the percentage of patients with history of CAD with AKI was 34.9% , which appears higher compared to that of non- AKI patients. However, the comparison between history of CAD and AKI shows no statistical significance with p=0.149, which reveals the presence of past history of CAD is not associated with development of AKI in MI patients, during the present episode.
The results from Table 10 shows, the Percentage of patients with history smoking with Non-AKI group was 27.1% and those with AKI was 32.6%. Yet again, the comparison between history of smoking and AKI shows the no statistical significance with p=0.504 reveals the presence of history of smoking is not a risk factor for the development of AKI in MI patients.
51
p=0.525 reveals the presence of history of alcohol consumption is not a risk factor for the development of AKI in MI patients.
And the percentage of patients who underwent thrombolysis with Non-AKI group was 59.% and that of Non-AKI group was 86.0% (Table 12). The comparison between thrombolysis and AKI shows the highly statistical significance with p value=0.002 , which reveals that patients with acute myocardial infarction who are treated with thrombolysis are more prone for development of AKI, which however needs further studies which would compare different modalities of treatment of acute MI- such as thrombolysis, Percutaneous Coronary Intervention.
52
53
[image:59.612.96.523.127.650.2]Descriptive statistics
TABLE 1: Baseline Characteristics of the study population (n=150)
Parameters Mean±S.D. Minimum Maximum
Age
(years) 60±9 36 85
Systolic Blood Pressure
(mm Hg) 134±32 60 220
Diastolic Blood Pressure
(mm Hg) 84±10 50 120
Blood Sugar on admission
164±59 78 347
(mg/dL)
Serum Creatinine-on admission
(mg/dL) 0.9±0.3 0.6 2.4
Serum Creatinine –after 48 hours
(mg/dL) 1.1±0.5 0.6 4.1
Serum Cholesterol
(mg/dL) 184±42 81 320
Serum Triglycerides
(mg/dL) 131±61 54 500
Chest pain duration
(in hours) 6±8 0 72
Hemoglobin
(gm/dL) 12±1.5 8 15
54
TABLE 2: Distribution of gender among the total study population (n=150)
Sex n Percentage
Total Female Male
150 70 80
46.7% 53.3%
Figure 6: Pie chart showing distribution of gender among the total study population
Gender
[image:60.612.155.453.370.632.2]55
[image:61.612.88.538.156.323.2]ACUTE KIDNEY INJURY:
TABLE 3: Distribution of Non-AKI and various stages of AKI among the total study population (n=150)
Parameters Non-AKI AKI
Stage I
Stage II
Stage III
n 107 29 10 4
Percentage(%) 71.3 19.3 6.7 2.7
AKI, Acute Kidney Injury ; Non-AKI ,Non- Acute Kidney Injury
Figure 7: Pie chart showing distribution of Non-AKI and various stages of AKI among the total study population
AKI
[image:61.612.160.450.453.674.2]56
TABLE 4: Distribution of 5-day in-hospital mortality among the total study population
5-day in-hospital mortality
n(150) Percentage (%)
Died 23 15.3
Survived 127 84.7
Figure 8: Pie chart showing distribution of 5 day in-hospital mortality among the total study population
In-Hospital Mortality
[image:62.612.139.471.433.643.2]57
TABLE 5: Group statistics of study population in AKI (n=43) and Non-AKI-(n=107) groups ( T-test)
Parameters Non-AKI n(107) AKI n(43)
p value Mean
Std. Deviation
Std. Error
Mean Mean
Std. Deviation
Std. Error Mean
Age(years) 59 8 0.8 63 10 1.6 0.027
Systolic
BP(mm Hg) 136 26 2.5 130 42 6.4 0.492*
Diastolic
BP(mm Hg) 84 11 1.0 84 12 1.8 0.677*
Blood sugar on admission (mg/dL)
168 62 5.9 154 52 7.8 0.217*
Serum Creatinine – On admission (mg/dL)
0.9 0.3 .03 0.9 0.3 .04 0.846*
Serum Creatinine – after 48 hours (mg/dL)
0.9 0.2 .02 1.6 0.5 .08 <0.001
Serum Cholesterol (mg/dL)
180 38 3.7 192 51 7.8 0.206*
Serum
Triglycerides (mg/dL)
134 70 6.8 122 28 4.3 0.123*
Chest pain duration (in hours)
4 4 0.3 10 13 1.9 0.009
Hemoglobin (gm/dL)
12.0 1.5 0.1 11.8 1.7 0.3 0.354*
AKI, Acute Kidney Injury ;Non-AKI,Non Acute Kidney Injury;
58
[image:64.612.128.485.160.268.2]GENDER & AKI
TABLE 6: Distribution of sex between patients among Non- AKI (n=107) and AKI (n=43) patients
Gender Non-AKI AKI
Female, n (%) 52 (48.6) 18 (41.9)
Male, n (%) 55 (51.4) 25 (58.1)
AKI, Acute Kidney Injury ; Non-AKI ,Non- Acute Kidney Injury
Figure 9: Bar diagram showing distribution of sex between patients with Non-AKI and AKI
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Non AKI AKI
Gender
[image:64.612.160.454.412.639.2]59
[image:65.612.72.516.217.389.2]HISTORY OF HYPERTENSION & AKI
TABLE 7: Distribution of History of hypertension among Non-AKI(n=107) and AKI (n=43) patients.
History of Hypertension Non- AKI AKI
Hypertensive, n (%) 49 (45.8) 21 (48.8)
Non-hypertensive, n (%) 58 (54.2) 22 (51.2)
AKI, Acute Kidney Injury ; Non-AKI ,Non- Acute Kidney Injury
HISTORY OF DIABETES & AKI
TABLE 8: Distribution of History of diabetes among Non-AKI (n=107) and AKI (n=43) patients.
History of Diabetes Non AKI AKI
Diabetics, n (%) 39 (36.4%) 18 (41.9%)
Non- diabetics, n (%) 68 (63.6%) 25 (58.1%)
[image:65.612.73.483.559.687.2]60
[image:66.612.88.468.266.441.2]HISTORY OF CORONARY ARTERY DISEASE & AKI
TABLE 9: Distribution of History of Coronary Artery Disease among Non-AKI (n=107) and Non-AKI (n=43) patients
History of CAD Non AKI AKI
Present, n (%) 25 (23.4%) 15 (34.9%)
Absent, n (%) 82 (76.6%) 28 (65.1%)
61
[image:67.612.140.438.203.335.2]HISTORY OF SMOKING & AKI
TABLE 10: Distribution of history of smoking among Non-AKI (n=107) and AKI (n=43) patients
History of Smoking
Non-AKI AKI
Present 29 (27.1%) 14 (32.6%)
Absent 78 (72.9%) 29 (67.4%)
AKI, Acute Kidney Injury ; Non-AKI, Non- Acute Kidney Injury
HISTORY OF ALCOHOL INTAKE & AKI
TABLE 11 : Distribution of history of alcohol intake among Non-AKI (n=107) and AKI (n=43) patients
History of alcohol intake
Non-AKI AKI
Present 25 (23.4%) 8 (18.6%)
Absent 82 (76.6%) 35 (81.4%)
[image:67.612.140.469.494.626.2]62
[image:68.612.139.469.206.267.2]THROMBOLYSIS & AKI
TABLE 12: Distribution of thrombolysis among Non-AKI (n=107) and AKI (n=43) patients
Thrombolysis Non-AKI AKI
Lysed 64 (59.8%) 37 (86.0%)
AKI, Acute Kidney Injury ; Non-AKI, Non- Acute Kidney Injury
Figure 10: Bar diagram showing distribution of sex between patients with Non-AKI and AKI
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Non AKI AKI
Thrombolysis
[image:68.612.129.479.396.652.2]63
[image:69.612.119.496.213.423.2]5-day IN-HOSPITAL MORTALITY & AKI TABLE 13: Distribution of thrombolysis among
Non-AKI (n=107) and AKI (n=43) patients
AKI, Acute Kidney Injury ; Non-AKI, Non- Acute Kidney Injury 5-day
In-Hospital mortality
Non-AKI AKI Total
Died 10 (9.3%) 13 (30.2%) 23(15.3%)
64
Figure 11: Bar Diagram showing In-hospital mortality among AKI and Non-AKI patients
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Non AKI AKI
In-hospital mortality
65
TABLE 14: Age-wise distribution of male and
female population within AKI group (n=43)
Age-wise distribution within AKI
Number of male
Number of female
19-20 yrs - -
21-30 yrs - --
31-40 yrs - -
41-50 yrs 4 3
51-60 yrs 7 4
61-70 yrs 9 6
71-80 yrs 5 4
81-90 yrs - 1
Total 25 18
66
TABLE 15: Gender-wise distribution of associated co-morbities in MI patietnts who developed AKI
AKI, Acute Kidney Injury Within AKI
n(43)
Male n(25) Female, n(18)
History of Hypertension 15 6
History of Diabetes 12 6
History of CAD 7 8
67
TABLE 16: Gender-wise distribution of MI patients across various stages of Acute Kidney Injury
AKI Male, n(25) Female, n(18)
Stage I 17 12
Stage II 6 4
Stage III 2 2
68
69
DISCUSSION
The main findings of the study are as follows:
1. The incidence of Acute Kidney Injury in hospitalized patients presenting with Acute myocardial Infarction is 28.6%
2. History of hypertension, diabetes, prior CAD, and personal habits such as smoking and alcohol consumption were not significantly associated with development of AKI in acute MI patients in this study.
3. Development of AKI is associated with poor outcome in terms of in-hospital mortality of acute MI patients, with p= 0.001.
70
AKI in hospitalised acute MI patients [23] and Bruetto RG et al study that documented 14.6% of AKI in acute MI patients[24].
From Table 14, we infer, most number of MI patients who developed AKI fall within the elderly age group of 61-70 yrs. Previous studies have revealed that development of renal insufficiency in elderly MI patients adversely affects outcome in terms of mortality which continues until 6 months after myocardial infarction[25].
From Table 15, among 43 patients who developed AKI, 25 were male (58.2%) and 18 female (41.8%). Here, though the percentage of male who developed AKI is higher, by statistical analysis, gender does not prove to be an individual risk factor for developing AKI in hospitalized acute MI patients. Of the 18 female who developed AKI, 6 female (33.3%) had co-existing hypertension, 6 female (33.3%) were diabetics and history of coronary artery disease was present in 8 (44.4%) of them.
71
From Table 16, we infer that both male and female population who developed AKI, fall into stage I, accounting for 19.3%, Stage II with 6.7% and stage II with 2.7%, thus adding upto a cumulative percentage of 28.6%, the distribution of which was similar to the results from CS Fox et al study across various stages [23].
Of the total 150 study population, 23 patients had died during their 5-day in-hospital stay. Of the 23 patients who died, 13 patients (5 female) had developed Acute kidney Injury, thus proving that patients with Acute Myocardial Infarction who had developed Acute Kidney Injury had poor outcome in terms of 5-day in-hospital mortality, which is very much similar to the results obtained from the previous studies .(see the table)[26-30]
72 LIMITATIONS:
Even though, Kidney Disease: Improving Global Outcomes (KDIGO) and Acute Kidney Injury Network (AKIN) guidelines still use serum creatinine to define the criteria for diagnosing Acute Kidney Injury, its usage does come with a few drawbacks, as mild decrease in kidney function may not reflect changes in serum creatinine, and circumstances during which creatinine values prior to admission are not known. Furthermore, if the new biomarkers which detect even mild decrease in kidney function much earlier, such as cystatin-C, Kidney Injury Molecule- 1,etc, are made available at lower cost, it would help us study the actual disease burden in a better way.
STRENGTH:
73
74
CONCLUSION
1. The incidence of Acute Kidney Injury in hospitalized patients presenting with Acute myocardial Infarction is 28.6%
2. History of hypertension, diabetes, prior CAD, and personal habits such as smoking and alcohol consumption were not significantly associated with development of AKI in acute MI patients in this study.
3. Development of AKI is associated with poor outcome in terms of 5-day in-hospital mortality of acute MI patients, with p= 0.001.
75
76
BIBLIOGRAPHY
[1] Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group (2012) KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int (Suppl 1): 1–138.
[2] Sarnak MJ, Levey AS, Schoolwerth AC et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease,High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation 2003; 108: 2154–2169
[3] Ronco C, Haapio M, House AA, Anavekar N, Bellomo R (2008) Cardiorenal syndrome. J Am Coll Cardiol 52: 1527–1539.
[4] Goldberg A, Hammerman H, Petcherski S, et al. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J 2005;150:330 –7.
77
[6] Goldberg A, Hammerman H, Petcherski S et al. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J 2005; 150: 330– 337.
[7] Jose P, Skali H, Anavekar N, et al. Increase in creatinine and cardiovascular risk in patients with systolic dysfunction after myocardial infarction. J Am Soc Nephrol 2006;17:2886 –91
[8] Goldberg A, Hammerman H, Petcherski S, et al. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J 2005;150:330 –7.
[9] Tokuyama H, Kelly DJ, Zhang Y, Gow RM, Gilbert RE. Macrophage infiltration and cellular proliferation in the non-ischemic kidney and heart following prolonged unilateral renal ischemia. Nephron Physiol 2007;106:54–62.
[10] Chen ZM, Pan HC, Chen YP, et al. Early intravenous then oral metoprolol in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005;366:1622–32
78
[12] Mishra J, Ma Q, Prada A, et al. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J Am Soc Nephrol 2003;14:2534–43
[13] Herget-Rosenthal S, Marggraf G, Husing J, et al. Early detection of acute renal failure by serum cystatin C. Kidney Int 2004;66:1115–22.
[14] Han WK, Bailly V, Abichandani R, Thadhani R, Bonventre JV. Kidney injury molecule-1 (KIM-1): A novel biomarker for human renal proximal tubule injury. Kidney Int 2002;62:237– 44.
[15] Ichimura T, Hung CC, Yang SA, Stevens JL, Bonventre JV. Kidney injury molecule-1: a tissue and urinary biomarker for nephrotoxicantinduced renal injury. Am J Physiol Renal Physiol 2004;286:F552– 63.
[16] Ishani, Areef, et al. "Acute kidney injury increases risk of ESRD among
elderly." Journal of the American Society of Nephrology 20.1 (2009):
223-228.
79
[18] Hoste E, Damen J, Vanholder R et al, Assessment of renal function in recently admitted critically ill patients with normal serum creatinine. Nephrol Dial Transplant. 2005;20(4):747–753.
[19] Goldberg A, Kogan E, Hammerman H, Markiewicz W, Aronson D (2009) The impact of transient and persistent acute kidney injury on long-term outcomes after acute myocardial infarction. Kidney Int 76: 900–906.
[20] Amin AP, Spertus JA, Reid KJ, Lan X, Buchanan DM, et al. (2010) The prognostic importance of worsening renal function during an acute myocardial infarction on long-term mortality. Am Heart J 160: 1065– 1071.
[21] Goldenberg I, Subirana I, Boyko V, Vila J, Elosua R, et al. (2010) Relation between renal function and outcomes in patients with non-ST-segment elevation acute coronary syndrome: real-world data from the European Public Health Outcome Research and Indicators Collection Project. Arch Intern Med 170: 888–895.
80
[23] Fox CS, Muntner P, Chen AY, Alexander KP, Roe MT, Wiviott SD.
Short-term outcomes of acute myocardial infarction in patients with acute
kidney injury: a report from the national cardiovascular data registry.
Circulation. 2011 Jan 1:CIRCULATIONAHA-111.
[24] Bruetto RG, Rodrigues FB, Torres US, Otaviano AP, Zanetta DMT, et al. (2012) Renal Function at Hospital Admission and Mortality Due to Acute Kidney Injury after Myocardial Infarction. PLoS ONE 7(4): e35496. doi:10.1371/journal.pone.0035496
[25] Shlipak MG, Heidenreich PA, Noguchi H, Chertow GM, Browner WS, McClellan MB. Association of renal insufficiency with treatment and
outcomes after myocardial infarction in elderly patients. Annals of
internal medicine. 2002 Oct 1;137(7):555-62.
[26] Goldberg A, Hammerman H, Petcherski S, Zdorovyak A, Yalonetsky S, Kapeliovich M, Agmon Y, Markiewicz W, Aronson D: Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J 150: 330–337, 2005
81
during hospitalization for acute myocardial infarction. Arch Intern Med 168: 609–616, 2008
[28] Parikh CR, Coca SG, Wang Y, Masoudi FA, Krumholz HM: Long-term prognosis of acute kidney injury after acute myocardial infarction. Arch Intern Med 168: 987–995, 2008
[29] Marenzi G, Assanelli E, Campodonico J, De Metrio M, Lauri G, Marana I, Moltrasio M, Rubino M, Veglia F, Montorsi P, Bartorelli AL: Acute kidney injury in ST-segment elevation acute myocardial infarction complicated by cardiogenic shock at admission. Crit Care Med 38: 438– 444, 2010
[30] Goldberg A, Kogan E, Hammerman H, Markiewicz W, Aronson D. The
impact of transient and persistent acute kidney injury on long-term
outcomes after acute myocardial infarction. Kidney international. 2009
Oct 2;76(8):900-6.
82
PROFORMA
Name: Age/sex: Occupation: Address: IP NO:
Diagnosis: Questionnarie:
Medical History: Coronary artery Disease Diabetes mellitus
Systemic hypertension
Drug History:
Personal History: Diet Smoking Alcoholism Physical examination;
Blood Pressure: Pulse rate: CVS: RS:
83 Investigations:
Electrocardiogram: Cardiac biomarkers: Echocardiogram:
Complete Blood count: Triglycerides:
Total cholesterol:
Renal Function Test: At admission At 48 hours Blood Urea
Serum Creatinine:
INTERPRETATION OF RENAL FUNCTION TEST: No evidence of Acute Kidney injury:
Evidence of Acute Kidney injury : Stage 1 : Stage 2 : Stage 3 :
84
PATIENT CONSENT FORM
Study detail: “INCIDENCE OF ACUTE KIDNEY INJURY IN PATIENTS WITH ACUTE MYOCARDIAL INFARCTION”
Study centre : GOVT. ROYAPETTAH HOSPITAL ,KILPAUK MEDICAL COLLEGE, CHENNAI
Patients Name : Patients Age : Identification No. :
I confirm that I have understood the purpose of procedure for the above study. I have the opportunity to ask question and all my questions and doubts have been answered to my complete satisfaction.
I understand that my participation in the study is voluntary and that I am free to withdraw at any time without giving reason, without my legal rights being affected.
85
I agree to take part in the above study and to comply with the instructions given during the study and faithfully cooperate with the study team and to immediately inform the study staff if I suffer from any deterioration in my health or well-being or any unexpected or unusual symptoms.
I hereby consent to participate in this study.
I hereby give permission to undergo complete clinical examination and diagnostic tests including hematological, biochemical, radiological tests.
Signature/thumb impression Signature/thumb impression
of the patient: of the guardian/ relative
Patients Name and Address : Place: Date
Signature of investigator :
86
யஒ த ப வ
ஆ பர : " ர மாரைட ெகா ட ேநாயா க வர ய த கா க
ரக ெசய ழ ேநா க "
ஆ ைமய : அர இராய ேப ைட ம வமைன, பா க ம வ
க , ெச ைன
ேநாயா ெபய :
ேநாயா வய :
அைடயாள எ :
ேமேல ள ம வ ஆ வர க என
ள க ப ட . நா இ வா த ைசயாக ப ேக ேற . எ த
காரண னாேலா எ த ச ட க உ படாம நா இ வா
இ ல ெகா ளலா எ அ ெகா ேட .
இ த ஆ ச ப தமாகேவா, இைத சா ேம ஆ
ேம ெகா ேபா இ த ஆ ப ெப ம வ எ ைடய
ம வ அ ைககைள பா பத எ அ ம ேதைவ ைல என அ
ெகா ேற . இ த ஆ ல ைட தகவைலேயா, ைவேயா
பய ப ெகா ள ம க மா ேட . இ த ஆ ப ெகா ள
87
இ த ஆ ைவ ேம ெகா ம வ அ உ ைம ட
இ ேப எ உ ய ேற .
ப ேக பவ ைகெயா ப ேநாயா ஒ த தர யலாத ைல
ப உ ன ைகெயா ப
ஆ வாள ைகெயா ப
இட :
88
INFORMATION TO THE PATIENT / GUARDIAN
A clinical study titled “INCIDENCE OF ACUTE KIDNEY INJURY IN PATIENTS WITH ACUTE MYOCARDIAL INFARCTION’’ is being conducted in Government Royapettah hospital.
This study is aimed at finding out Kidney diseases at the early stages (Acute kidney injury) in patients who get admitted with heart attack ( Acute myocardial infarction).
From previous studies, we learn that Acute Kidney injury is one of the important complications of Myocardial infarction. It affects the treatment modality ( use of anti-hypertensives, use of contrast dyes, CABG ) and has a prognostic significance both in terms of short and long-term.
89
ஆரா தகவ தா
அர இராய ேப ைட ம வமைன மாரைட உ ளான
ேநாய க ஏ ப த கா க ரக ெசய ழ ைப ப ய ம வ
ஆ நட த ப ற .
இ த ஆ வான மாரைட காக ம வமைன ேச க ப
ேநாய க ட ேத ஏ ப த கா க ரக ெசய ழ ைப
வ க ட ேலேய க பைத ேகாளா ெகா ற .
ைதய ஆ க ஊடாக த கா க ரக ெசய ழ எ ப
மார ைட ேபா ஏ பட ய தைலயாய பா க ஒ என
அ ேறா . அ ேநாய வழ க ப ம வ ைற ஒ
தா க ைத அவ க உட ைல க க ய ய கால
தா க ைத ட கால தா க ைத ெகா ற .
இ த ஆ வா லாக நா மாரைட உ ளா ேநாய க
ரக ெசய பா ைட க கா க ைள ேறா . அ ரக
ெசய பா ைட ேம ேமாச ஆ காத ம வ ைறகைள ைகயாள நம
உத . ேம அ த கா க ரக ெசய ழ ைப உைடய ேநாய கைள
ட கால ெதாட க கா ைவ க அவ க க ய ைவ
ஊ ட ,அவ க ரக பா ேநா ேன ற ைத
க கா க , மாரைட ம வ ெச ேபா ரக பா
92