CIRCADIAN RHYTHM OF BLOOD PRESSURE AND ITS
MODULATION BY THE ANTIHYPERTENSIVE DRUGS IN
HYPERTENSIVE PATIENTS OF SOUTH TAMILNADU
Thesis Submitted to
THE TAMILNADU Dr. M.G.R. Medical University, CHENNAI.
In partial fulfillment of the requirement for the award of the
degree of
Doctor of Philosophy
By
A.J.M. CHRISTINA, M.Pharm.,
Institute of Pharmacology Madurai Medical College
Madurai – 625 020. Tamilnadu.
CERTIFICATE
Dr.N.Murugesh, B.Sc., M.B.B.S., M.Sc (Med)., Ph.D., F.I.C.S. Rtd. Professor,
Institute of Pharmacology, Madurai Medical College, Madurai – 625 020.
This is to certify that this thesis entitled “Circadian Rhythm of Blood Pressure and its Modulation by the Antihypertensive Drugs in Hypertensive Patients of South Tamilnadu” is a bonafied record work of independent research carried out by
Mrs.A.J.M.CHRISTINA, under my supervision and guidance in the Institute of Pharmacology, Madurai Medical College, Madurai – 625 020, and this thesis has not formed previously the basis for the award of any Degree, Diploma, Associateship, Fellowship or other similar title.
Date : Place :
(Prof. M.Nagarajan, M.Pharm) (Dr.N.MURUGESH)
ACKNOWLEDGEMENT
The ecstasy that accompanies the successful completion of any task would be incomplete without thanking the people who made it possible.
To the Lord Almighty I humbly submit this work without whom it would have been unsuccessful.
With due respect, I express my deep sense of gratitude to Dr. N.Murugesh, B.Sc., M.B.B.S., M.Sc (Med)., Ph.D., F.I.C.S., for his encouragement and support throughout the study.
I wish to express my sincere thanks to Prof. M.Nagarajan, M.Pharm., for his support all the time.
I wish to remember and thank Dr. Harihara Subramanian, M.D., Ph.D., Rtd. Professor, Institute of Physiology, Madurai Medical College, who introduced the term “Chronopharmacology” to me, as early as 1994.
I wish to express my thanks to Mr. N.Chidambaranathan, M.Pharm for his help in completing the work.
I thank all my teachers, colleague friends and my students who helped me at different times.
My special thanks to my family members also.
DECLARATION
I hereby declare that the Ph.D thesis entitled “Circadian Rhythm of Blood Pressure and its Modulation by the Antihypertensive Drugs in Hypertensive Patients
of South Tamilnadu” submitted to the Tamilnadu Dr.M.G.R. Medical University,
Chennai is a record of independent work carried out by me in the Institute of Pharmacology, Madurai Medical College, Madurai – 625 020, under the supervision and guidance of Dr.N.Murugesh, Rtd. Professor, Madurai Medical College, Madurai and the thesis has not formed previously the basis for the award of any Degree, Diploma, Associateship, Fellowship or other similar title.
Date : Place :
PREAMBLE
Blood Pressure (BP) in humans exhibits circadian rhythm with high
daytime and low nighttime values. The nocturnal fall is known as ‘dipping’,
which occurs to the extent of 10% to 20% of daytime BP values.
Non-dipping is the absence of or diminished nocturnal fall. The phenomenon of
dipping carries a strong significance by preventing various cardiovascular and
cerebrovascular target organ damage. Dipping Phenomenon has been studied
for the first time in a South Indian population of normotensives and also
hypertensives receiving calcium channel blockers, beta blockers, angiotensin
converting enzyme inhibitors and their combinations. The influence of
various factors such as age, sex and job strain on dipping phenomenon has
also been studied. The significance of dipping in these populations and their
LIST OF ABBREVIATIONS
BP - Blood Pressure
SCN - Suprachiasmatic nucleus
AUC - Area under time – concentration curve
TOD - Target Organ damage
DP - Dipping Phenomenon
NDP - Non Dipping Phenomenon
SBP - Systolic Blood Pressure
DBP - Diastolic Blood Pressure
BB - Beta Blockers
CCB - Calcium channel blockers
ACEI - Angiotensin converting enzyme inhibitors
CO - Cardiac output
TPR - Total Peripheral resistance
LVH - Left Ventricular hypertrophy LVMI - Left Ventricular mass index
CHD - Coronary heart disease
IMT - Intima media thickening
CCA-IMT - Common Carotid artery – Intima media thickening
ECG-LVH - Electrocardiography – Left Ventricular hypertrophy
SCI - Silent cerebral infarcts
WML - White matter lesions
CONTENTS
I. INTRODUCTION 1-17
Rhythmicity in life Biological Clock
Functions of Biological Clock
Classification of Biological Rhythms Chronobiology
Divisions of Chronobiology Chronobiology and medicine Circadian rhythms
Characteristics of Circadian Rhythms Parameters of Circadiana Rhythm Resetting of Circadian Rhythm Chronopharmacology
Complementary concepts of chronopharmacology Chronokinetics
chronesthesy chronergy
Aim of Chronopharmacology
II.
REVIEW OF LITERATURE
18-29
A Tale of Two Phenomena- ‘Dipping’ and ‘Non-Dipping’ Factors influencing dipping and non dipping phenomena.
The three Musketeers
Angiotensin converting Enzyme Inhibitors (ACEI) Calcium channel blockers (CCB)
Beta blockers (BB)
III. PLAN
OF
WORK
30-31
IV.
RESEARCH ENVISAGED
32-50
Part I
Determination of dipping and non-dipping phenomenon of circadian rhythm of blood pressure in a normotensive population.
Determination of dipping and non-dipping phenomenon of circadian rhythm of blood pressure in specific normotensive subpopulations.
Part II
Determination of dipping and non-dipping phenomenon of circadian rhythm of blood pressure in a hypertensive population.
Determination of dipping and non-dipping phenomena of circadian rhythm of blood pressure in the hypertensive subpopulations.
IV.
RESULTS
51-95
V. DISCUSSION 96-118
VI. SUMMARY
119-120
INTRODUCTION
RHYTHMICITY IN LIFE
One of the wonderful creations of God, the earth, rotates on its own axis and revolves round the sun giving rise to light and dark cycles of the day. Shakespeare uses the expression ‘whirligig of time’ to denote the revolving circling movement of time. Correspondingly, all the species on earth exhibit changes in physiology and/or behaviour which in many ways coincide with the light-dark cycle of the day generating rhythmicity.1 Rhythmicity is a part of our life. All living organisms exhibit in some way or other, a form of rhythmicity.Some of these rhythms have a geophysical counterpart in the environment. These are the so called biological rhythms.2 The persistence of biological rhythms as reported, is limited not only to mammalian systems and it has been found to be omnipresent as virtually all forms of life exhibit these rhythms.3 Biological rhythms are an essential component of homeostasis.4 The observation on the relationship between biological rhythms exhibited by various organisms and light-dark cycles suggested the existence of a
biological time keeping system or a biological clock within the organisms.5-9
BIOLOGICAL CLOCK
placed in the interior of a room not exposed to sunlight. This finding suggested that the movement represented something more than a simple response to sun and revealed that those movements were controlled by an endogenous clock.
This biological clock synchronizes the life of the organism with both its external and internal environment.10 In mammals, the biological clock (circadian oscillator) is situated in the suprachiasmatic nucleus (SCN), a small bilaterally paired structure present just above the optic chiasma. Circadian rhythms of sleep-wakefulness cycle and hormone release disappear when the SCN is destroyed and transplantation of fetal or neonatal SCN into an arrhythmic host restores rhythmicity.11 Three functions of the endogenous clock have been discriminated;
1. Rhythm generation
2. Entrainment to light-dark cycle 3. Output from the clock.12
CLASSIFICATION OF BIOLOGICAL RHYTHMS
The biological rhythms according to their repetitive nature and duration are classified as
i. High frequency cycles (e.g. hormone secretion occurring in distinct pulses throughout the day).
ii. circadian (approximately or equal to 24-h) iii. circa mensual (28 days)
iv. circa annual (approximately 1 yr) cycles.14
However, much concern is about the circadian cycle because of its adaptive characteristics and hence has been the subject of numerous experimental and theoretical studies.15
CHRONOBIOLOGY
Chronobiology, the study of biological rhythms was reported to be established by Julian-Joseph Virey.16 His doctoral thesis in medicine which was completed in 1814 in Paris was the first work devoted to biological rhythms. He envisioned biological rhythms to be innate and controlled by living clocks, entrained by periodic environmental changes. He also reported that the effects of drugs vary with the time of administration.
various areas of medicine suggest that the body is not only organized in space with an anatomy, but is organized in time in terms of biological rhythms.
DIVISIONS OF CHRONOBIOLOGY
The influence of biological rhythms in life that may be shown in the constructive effect on growth, development and maturation is termed as anachronobiology. Catachronobiology denotes deleterious effects of time and rhythms which may lead to disease.17
CHRONOBIOLOGY AND MEDICINE
Thus the principles of chronobiology have important implications and applications in medicine, as circadian rhythms influence many medical conditions that are routinely seen in the clinic.18-22
Cardiovascular diseases in general and blood pressure in particular are affected by circadian rhythms.23 Different studies conducted in United States report peculiar rhythmcity in various cardiovascular complications. These studies reported that myocardial infarction is more likely to occur on Mondays;24 cardiac death is more common in winter and the risk of dying of cardiovascular diseases is lower in summer.25
declines during the last half of the month and then dramatically increases on the first day of the month.26
Not only the onset and progress of disease, even the diagnosis of various medical conditions may be affected by circadian rhythms. For example, the responses to allergens given intradermally, as in allergen skin testing, is three times greater in early evening than in the morning.27
Circadian rhythms also affect treatment as many cardiovascular medications have been shown to be influenced by circadian rhythms. A significant difference in the therapeutic control of many antihypertensive drugs has been frequently reported following different dosing times. Morning dosing of Perindopril, an ACE inhibitor resulted in excellent control of hypertension for 24-h, while evening dosing in the same patients could control blood pressure only for 12-14 h of the day.28 Likewise the pharmacology of many cardiovascular drugs is influenced by circadian rhythms.29
CIRCADIAN RHYTHMS
CHARACTERISTICS OF CIRCADIAN RHYTHMS
precisely 24.3 h, slightly slower than the light-dark cycle. But many reports available extend it up to 25-h (τapproximately 25-h).31
However this rhythm is synchronized to 24-h day mostly by light-dark cycle and social time cues. These exogenous time signals are known as
zeitgebers.32 Light is a physical zeitgeber33-36 and social zeitgebers also influence the circadian rhythm.37
The first characteristic of circadian rhythms is that they are self sustained in nature i.e. they continue to cycle by themselves even under laboratory conditions in the absence of any external time cues from physical environment. Hence they can be easily distinguished from diurnal rhythms which occur in natural conditions which are mere responses to 24-h environmental changes. Such rhythms i.e. circadian rhythms that are expressed in the absence of any 24-h signal from external environment are called ‛free running’.38 However all diurnal rhythms are found to be circadian.
The next characteristic property of circadian rhythms is their ability to be synchronized or entrained. Although circadian rhythms are found to be free running, zeitgebers such as light-dark cycles are naturally present and hence circadian rhythms are found to align to such time cues. This alignment is said to be the synchrony. However if a shift in the external cues occurs as noted in jet travellers who cross the time zones, the rhythms are found to be aligned to new cues. This alignment is called entrainment. Thus circadian rhythms enable us to adjust better to our environment. So when the lifestyles are altered, symptoms like jet lag and shift lag result. During transmeridian flights, there occurs desynchronization between the circadian rhythms and the external time cue i.e. light-dark cycle. Hence the jet travellers experience signs and symptoms collectively known as jet lag.39 A similar situation is encountered with night shift workers whose desynchrony is known as shift lag.40,41 The symptoms of jet lag and shift lag are summarized below
SYMPTOMS OF JET LAG AND SHIFT LAG
JET-LAG SHIFT LAG
Day time sleepiness Insomnia at night Impaired concentration Slow physical performance Irritability
GI disturbances Depressive symptoms
Sleeping at work
Disruption during day time sleep Decreased attention
Impaired performance Irritability
The symptoms of shift work-related desynchrony have more significance than jet-lag symptoms which are limited to a few days following travel, while symptoms of shift work desynchronosis are quite often chronic. Thus circadian rhythms in humans are a mixture of endogenous and exogenous components derived from the body clock and the interaction between our environment and life style.31
The next important property of circadian rhythm is its ubiquity in nature i.e. circadian rhythms exist in a broad array of biological processes and organisms. Hence the persistence of circadian rhythms is reported to be not limited to mammalian systems alone and they exist virtually in all forms of life.
Another important and final property is that circadian rhythms appear to be generated at cellular level because the rhythms of unicellular organisms are very similar to rhythms of complex mammals.
PARAMETERS OF CIRCADIAN RHYTHM
A biological rhythm can be characterized by its curve pattern (plotting raw data over time) and quantification of four of its parameter.
b. The acrophase, (Φ) is the mathematically estimated span of time taken to reach the crest of the validated rhythm for τ under consideration, with regard to a phase reference.
c. The amplitude (A) is the amount of variability i.e. the crest to trough difference, for the τ under consideration.
d. The mesor (M) is the rhythm adjusted mean for the τ under consideration.
RESETTING OF CIRCADIAN RHYTHM
A representative circadian rhythm in which, the level of a particular hormone varies with time. As this rhythm seems to persist even in darkness it is a free running rhythm.
Tim e Phase Delay
Phase Advance
Le
ve
l
The effects of a rhythm-resetting signal such as exposure to light in animals otherwise kept in continuous darkness can shift the rhythm either back or ahead which may be called as phase-delay and phase-advance respectively. In case of phase advance, the peak levels are reached earlier and in case of phase delay, the peak levels are reached later.
The influence of circadian rhythms in humans suggests that there is an intersection of circadian rhythms and pharmacology and this intersecting, interesting, young field is Chronopharmacology.
CHRONOPHARMACOLOGY
DEFINITIONS OF CHRONOPHARMACOLOGY
Different scientists have defined the term ‘chronopharmacology’ variously. Modern Chronopharmacology investigates as to how drug effects vary with biological timings and endogenous bioperiodicities.46
In a broader sense, Chronopharmacology investigates drug effects a) as a function of biological timing and upon b) parameters (circadian period, peak time, amplitude and adjusted mean) characterizing the endogenous bioperiodicity.47
In other words ‛chronopharmacology’ is the science dealing with optimization of drug effects and minimization of adverse effects by timing the medication in relation to biological rhythms.48
Like this, numerous studies indicate that the effect of same dose of medication may differ in a predictable pattern during 24-h, due to body rhythms in the tissues where the effect is mediated. This study of administration-time dependencies in the behaviour of drugs is Chronopharmacology.
COMPLEMENTARY CONCEPTS OF CHRONOPHARMACOLOGY
To understand the broad field of Chronopharmacology, knowledge about the three complementary concepts of this field viz, chronokinetics, chronesthesy and chronergy is essential [50].
CHRONOKINETICS
Chronokinetics is defined as the predictable rhythmic changes dependent on the time of dosing, in the parameters used to characterize the pharmacokinetics of drugs such as
i. Cmax(maximum concentration in plasma) ii. Tmax(span of time to reach Cmax)
iii. AUC (area under concentration/time curve) iv. t1/2(half life)
Thus chronokinetics deals with the study of the temporal changes in the absorption, distribution, metabolism and elimination51 and hence considers the predictable rhythmic changes in the parameters used to characterize the pharmacokinetics of drugs. Numerous studies have been conducted so far, depicting the chronokinetics of drugs. But a few are worth mentioning.
CHRONOKINETICS IN ABSORPTION
Temporal changes in pharmacokinetics of indomethacin have been substantiated in healthy young volunteers following a single dose administration at different times of a day (0700, 1100, 1500, 1900, and 2300) to young adults. It was found that smallest and latest peaks were recorded in the subjects administered with the drug at 1900 and 2300 while ingestion at 0700 and 1100 led to largest and quickest peak.52
Similarly, kinetic parameters characterizing the absorption of the benzodiazepine, lorazepam exhibit large differences between the morning and evening doses in humans. The absorption t1/2 was found to be three times longer with the evening rather than the morning dosing in all the study participants.53
CHRONOKINETICS IN DISTRIBUTION
In one, round the clock in vitro permeability study of lidocaine, it was observed that lidocaine content of erythrocytes sampled at 2200 was 74% of the plasma concentration while it was only 48% when sampled at 1000.54 In humans circadian changes in plasma protein binding have been reported for anticonvulsant drugs such as diazepam,55 valproic acid56 and carbamazepine,57 all of which show crest in the early morning.
CHRONOKINETICS IN METABOLISM
Enzyme activities including those responsible for drug metabolism exhibit large amplitude circadian changes in the hepatic cell and thus can explain the circadian rhythms in the effect of hexobarbital and in acetaminophen.58
CHRONOKINETICS IN ELIMINATION
CHRONESTHESY
Chronesthesy is defined, as the predictable rhythmic changes in the susceptibility of target biosystems to a drug.62 The target biosystem may be located at the molecular level of receptors or elsewhere. Circadian rhythms in various types of receptors and organs have been reported. Statistically significant 24-h rhythms have been validated for various receptors in whole brain homogenates of rats.
The nociceptive receptors in male Wistar rats have been reported to exhibit diurnal rhythm.63 At an organ level, circadian rhythm of human skin reactions in terms of erythema and wheal responses to intradermal injections of histamine has been investigated and found to have a nocturnal crest.64 Hence chronesthesy represents changes found at the level of a target system and influences time dependent changes in pharmacokinetics i.e. chronokinetics.
CHRONERGY
This part deals with rhythmic changes in the integrated overall effects of the drugs. This term takes into consideration the chronokinetics and chronesthesies of organic biosystems involved.65
AIM OF CHRONOPHARMACOLOGY
However during the last three decades, the science of chronobiology has revealed to medicine the importance of the rhythms that exist in biological processes and functions of humans.66 Hence the recent approach for increasing the efficacy of pharmacotherapy by administering drugs at the time of the day when they are best tolerated is gaining momentum.
Chronobiologists suggest that synchronizing drug therapies to body rhythms may provide more effective treatment for a variety of conditions. Hence chronopharmacology, the field of administration-time dependent variations in medications aims at chronotherapy.
Chronotherapy refers to the use of pharmacological approach to clinical treatment in order to enhance the effectiveness of a drug by determining the best biological time for dosing. This chronotherapeutic approach has been extended to many diseases that exhibit significant rhythmic variations. There are well documented rhythmic variations in blood pressure23 heart rate67 and in platelet aggregability.68
substantially lower during sleep.72 It was found that during night, blood pressure drops by 10% - 20% of daytime blood pressure73 and that during 24-h period, there can be as much as 20mm Hg-30mmHg change in blood pressure74. This nocturnal drop or fall in blood pressure by 10%-20% of daytime blood pressure is known as ‛Nocturnal fall’ or ‛Nocturnal drop’ or ‛Nocturnal decline’. Reports state that, the onset of sleep is associated with this nocturnal fall in blood pressure.75
REVIEW OF LITERATURE
Circadian rhythm of blood pressure is characterised by high levels during daytime and lower levels during night, with a 10% - 20% drop in blood pressure at night.73 However a high prevalence of abnormal circadian blood pressure profile is noted in patients with essential hypertension, in diabetes and in primary chronic renal disease.76 The abnormal patterns of circadian rhythm of blood pressure commonly encountered are
(i) Reduced nocturnal decline which is reported to be associated with advanced target organ damage (TOD).
(ii) Excessive nocturnal decline associated with excessive morning surge in blood pressure and orthostatic hypertension.77
(iii) Nocturnal increase in blood pressure instead of nocturnal decline.
The term common in all of these abnormal patterns is ‘Nocturnal decline’.
A TALE OF TWO PHENOMENA – ‘DIPPING’AND ‘NON-DIPPING’
Depending on the extent to which people dip their blood pressure nocturnally, they are classified as ‘Dippers’ and ‘Non-dippers’. A wide range of definitions is used to distinguish ‘Dippers’ from their counterparts, ‘Non-dippers’. In general, subjects with a nocturnal decline in blood pressure between 10% - 20% of daytime blood pressure, are categorised as ‘Dippers’, while those with a nocturnal decline < 10% of daytime average are categorised as ‘Non-dippers’. Non-dippers include not only those with a < than 10% drop but also those who do not show any decline at all.80 Consequently, those with a nighttime decline > 20% are defined as ‘extreme dippers’ and subjects with a nocturnal increase in blood pressure are categorised as ‘reverse dippers’ or ‘risers’.77
A lack of nocturnal fall in blood pressure is present in normotensives too,81 suggesting that high blood pressure is not a necessary condition for ‘non-dipping’ phenomenon. Normotensive and hypertensive ‘non-dippers’ with or without blood pressure circadian rhythm have been reported. The ‘rhythmic non-dippers’ show a blood pressure circadian rhythm which is inverted in phase, demodulated in amplitude.82
Factors influencing dipping and non-dipping phenomenon
Age
A study by Morfis and Howes 1997,83 has shown that dipping is noted in elderly normotensives who show a greater nocturnal decline in systolic blood pressure (SBP) than treated elderly hypertensives.
Sex
The prevalence of non-dipping has been reported in hypertesnive women and it has been found to be associated with adverse prognosis in hypertensive women.84
Race
Blacks appear less likely than whites to have a > 10% drop in nighttime blood pressure.85 The nocturnal blood pressure fall is more pronounced in Europeans than Asians and a high night-day BP ratio has been observed in Asians which has been attributed in part to genetic background, lifestyle or both.86,87
Recent studies in China and Taiwan showed that nocturnal blood pressure dropped by only 2%88-11%89 of the corresponding daytime levels. Normotensive Taiwanese showed a low daytime and high nighttime blood pressure.
del Arco-Galan and Suarez Fernandez have observed that non-dipper condition is changeable and is related to the activity carried out by the subject while awake, as well as quality of sleep.93
The day and night definitions and various formulae for calculating nocturnal decline in blood pressure are given under Part-I of ‘research envisaged’.
RHYTHM GENERATOR
In mammals, physiological rhythms are governed by an autonomous circadian clock in each retina while metabolic and behavioral rhythms are controlled by circadian clock in the SCN of hypothalamus.94 The endogenous circadian pacemaker imposes 24-h biological rhythms through endocrine and autonomic mechanisms.95 For example, the circadian rhythm of heart and liver is regulated via sympathetic and parasympathetic system96 and that of pineal gland via the sympathetic nervous system.97
of autonomic nervous function with gradual blunting of blood pressure.101 Hence it is evident that blunted nocturnal decline is associated with altered functioning of ANS and for the maintenance of normal circadian blood pressure pattern, normal functioning of ANS is a prerequisite.
Large literature states that abnormal patterns of circadian rhythm of blood pressure are associated with cardiovascular and cerebrovascular complications, and hence maintaining a normal circadian rhythm becomes warranted. The significance of abnormal patterns of circadian rhythm of blood pressure is discussed under ‘Results and Discussion’ section.
THE THREE MUSKETEERS
Cushman et al102 in their ALLHAT study recommended that it is a
mistaken notion that most hypertensive patients (>160/100 mmHg) can be controlled by single drug therapy. Because only half the patients respond to single drug therapy even at full dose, a second hypotensive agent is frequently required to obtain adequate blood pressure control.
The significance of altered circadian rhythm of blood pressure suggests that an antihypertensive drug must be prescribed in order to obtain smooth, 24-h blood pressure control which parallels the circadian pattern. Many studies have been conducted with antihypertensive drugs, aiming at restoration of or preserving the circadian rhythm of blood pressure. In this study patients on BB, CCB, ACEI and their combinations were chosen as subjects. Thousands of studies have been conducted so far regarding the therapeutic profile and chronotherapy of these drugs. However only some studies related to circadian rhythm of blood pressure are reviewed here.
ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACEI)
Qiu et al104 investigated whether captopril administered at night can
shift the circadian blood pressure form non-dipper to a dipper pattern in adequately controlled hypertensive patients and reported that it reduced the elevated night/day blood pressure ratio and could restore the diurnal rhythm.
Eguchi et al105 compared the effects of long acting ACE inhibitor
Kuroda et al106 compared the effects of bedtime against morning
administration of long-acting lipophilic angiotensin converting enzyme inhibitor (ACEI) trandolapril, on morning blood pressure in hypertensive patients and concluded that bedtime administration of this long acting ACE inhibitor is a safe and effective means of controlling morning blood pressure in hypertensive patients, without an excessive fall in nocturnal blood pressure.
CALCIUM CHANNEL BLOCKERS (CCB)
Controlled onset, extended release Verapamil constitutes the first chronotherapy of essential hypertension and ischemic heart disease. This study reported effective 24-h control of blood pressure, including attenuation of its rapid rise in the morning without nighttime hypotension with this preparation.107
Calcium channel blockers have been evaluated for their influence on circadian pattern of blood pressure. Conventional short acting calcium channel blocker such as nifedipine at high dose, is associated with an increased risk of myocardial infarction and mortality.108 Hence long acting dihydropyridine CCB are being studied for their impact on circadian blood pressure. Muneta et al109 developed in Japan, Benidipine Hcl, a new long
In another study involving CCB, Kawano et al110 administered
nifedipine CR (controlled release) immediately after awakening in hypertensive patients and confirmed that morning surge in blood pressure was suppressed in these patients without the use of α or β blockers.
Likewise Ko and Chan111 studied the impact of amlodipine and nifedipine retard, on ambulatory blood pressure and also left ventricular systolic function in chinese hypertensive, type 2 diabetic patients and proved that both these drugs are effective in controlling 24-h blood pressure and restoring the nocturnal dip in blood pressure.
The study by Ideura et al112 involving the effects of nitrendipine on
circadian variation of blood pressure in patients with renal parenchymal hypertension showed that once daily oral administration of nitrendipine 10mg tablet was effective for 24-h control blood pressure.
White et al113 compared the effects of graded release diltiazem versus
ramipril dosed at bedtime, on early morning blood pressure, heart rate and the rate-pressure product. The reports of this study state that dilteazem extended release, an agent designed to parallel the circadian rhythm of blood pressure and heart rate produced greater reductions in morning heart rate and mean 24-h diastolic blood pressure (DBP).
chronodynamics in harmony with diurnal BP variation, on the 24-h blood pressure profile. It revealed that evening dose was associated with greater reduction in blood pressure during morning hours.
Imai et al115 evaluated the effect of barnidipine, a new dihydropyridine
calcium antagonist, administered once daily, in hypertensive patients and found out that it increased the nocturnal BP decline in hypertensive patients in whom, the decline was low before treatment.
BETA BLOCKERS (BB)
Serkova and Sheverda116 studied the effect of atenolol combined with chlorthalidone on the characteristics of 24-h blood pressure pattern and reported that 24-h, day and night arterial pressure have been reduced.
The effects of a recent alpha and beta blocker, arotinolol, in the treatment of essential hypertension between patients with a dipper and those with a non-dipper profile was investigated by means of 24-h ambulatory blood pressure monitoring (ABPM). It was found that the drug reduced the daytime SBP and DBP in both dippers and non-dippers while the nighttime pressure was reduced more in non-dippers than dippers, without excessively lowering blood pressure in the latter.117
The effect of arotinolol on ambulatory blood pressure in young and older hypertensive patients was investigated by Kuwajima et al118. They
Mc Lay et al119 studied the efficacy and tolerability of felodipine
extended release (ER) 5mg and metoprolol controlled release 50mg given as a combination in hypertensive patients. The results suggested that the combination produced a significant sustained reduction of systolic and diastolic BP over 24-h period.
Cleophas et al120 in 1999, examined the effects of different classes of
antihypertensive drugs on ambulatory blood pressure (ABP) in hypertensive patients. They concluded that beta blockers produced a more stable reduction of blood pressure in patients with mild hypertension, which is less affected by pressor effects through the sympathetic nervous system. Also beta blockers unlike ACE inhibitors and CCB, do not give rise to nighttime hypotension and the selective beta blocker celiprolol could perform better than non-selective beta blocker carvedilol.
The effect of metoprolol on 24-h ABP was studied in hypertensive black males. The nighttime fall in blood pressure was minimised by metoprolol and clinically significant increase in daytime blood pressure was noted in 58% of patients.121
The effect of a beta blocker with intrinsic sympathomimetic activity, carteolol on 24-h ABP was investigated in older and young population. It was found that carteolol reduced daytime systolic and diastolic pressure in both groups, nighttime SBP was not reduced in both groups, but nighttime DBP tended to decrease in the younger group.123
In hypertension, both BB and CCB are drugs with proven efficacy. The combination of a dihydropyridine CCB and a beta-blocker has been evaluated in a randomised double blind study. Twenty-four-hour arterial blood pressure monitoring showed that amlodipine added to atenolol produced a statistically significant reduction of blood pressure and that the reduction of side effects, obtained by adding CCB to a BB confirmed the effectiveness of the combination.124
All these studies have been designed to study the influence of antihypertensive drugs on different variables of the circadian pattern of blood pressure. Also these studies throw light on the fact that antihypertensives must exert adequate control over the altered circadian rhythm of blood pressure commonly seen in hypertension, in addition to lowering of elevated blood pressure.
which has been achieved by comparing it against a normotensive population. The altered circadian pattern has been evaluated in terms of dipping phenomenon(DP) and non-dipping phenomenon(NDP).
PLAN OF WORK
It is very clear from the review of literature that DP is a part of circadian rhythm of blood pressure, the absence of which may lead to cardiovascular and cerebrovascular complications. Hence the present study aimed at determining the prevalence of DP in a hypertensive population who were under treatment. This was compared with the prevalence of DP in a normotensive population. ‘Whether factors such as age, sex and job strain influence DP in both these populations?’ was also the aim of the study. Hence the study was conducted in two parts.
Part-I
1) Determination of DP and NDP in a normotensive population.
2) Determination DP and NDP in the normotensive subpopulations, as given below, which have been formed from the normotensive population.
Normotensive males Normotensive females
Part-II
1) Determination of DP and NDP in a hypertensive population.
2) Determination DP and NDP in the hypertensive subpopulations, as given below, which have been formed from the hypertensive population.
Hypertensive males Hypertensive females
PART I
Determination of Dipping and Non-Dipping Phenomenon of
Circadian Rhythm of Blood Pressure In A Normotensive
Population
Study Population
To assess the dipping and non-dipping status in a normotensive population of South Tamilnadu, 127 subjects were included in the study. Informed consent was obtained from all the subjects and this study was approved by the Ethical Committee constituted for this purpose.
Inclusion Criteria
Subjects with the following characteristics were included in this study. i) Normotensives whose sitting blood pressure was < 135/85mm Hg
on atleast two occasions before the start of the study.
ii) Body mass index, calculated as weight (in Kilograms) divided by height (in meters) squared, between 25 to 27.
iii) No history of hypertension or hypertension related complications (coronary heart disease, heart failure etc)
iv) No laboratory evidence of diabetes mellitus. v) No previous / present lipid lowering treatment.
daytime BP and nighttime fall in BP from which the incidence of dipping phenomenon (DP) and non-dipping phenomenon (NDP) can be assessed in the study population.
The demographic characteristics of the study population are given in Table No. 1 under ‘Results’ section
BP RECORDINGS
Each subject of the normotensive population had BP measurement starting from 6a.m, then at 7 a.m and 8 a.m followed by recording at intervals of 2-h upto 10p.m. and again at 6 a.m. of the next day, on three occasions separated by a period of one week.
DERIVED VARIABLES OF BLOOD PRESSURE
The mean 24-h systolic blood pressure (SBP) and diastolic blood pressure (DBP) were calculated as the sum of the products of interval pressure (mmHg) and interval duration weighted by the total duration(h) of blood pressure monitoring. Each interval BP was taken as the mean of the blood pressure readings at the start and finish of the interval.
Mean 24 h BP = 1 n (BPi) (di) 125 D i=1
Where ‘D’ is the total duration of BP monitoring. ‘n’ is the number of intervals
‘BPi’ is the BP(systolic or diastolic) of the ith interval. ‘di’ is the ith interval duration.
The mean daytime blood pressure was calculated as per the day and night definition ie. day time spans from 0700 (7 a.m.) to 2200 (10 p.m.) and nighttime period is from 2200 (10pm) to 0700 (7 a.m).126,127
The nocturnal dip in BP was the next parameter calculated. It has been calculated in many ways by chronobiologists. The nocturnal dipping in BP is scored as the drop in BP between 10 p.m. and 6 a.m. (clock time) reading.128,129
Nocturnal fall of SBP has also been calculated as (Awake SBP – Asleep SBP/ Awake SBP) where asleep SBP is the mean SBP from the time when the patient went to bed until the time of awakening and awake SBP is the mean SBP during the remaining portion of the day.130
The % of dippers or dipping phenomenon (DP) was calculated using this nocturnal fall in blood pressure. DP has been defined as the nocturnal fall in blood pressure by more than 10% and less than 20% of the mean daytime blood pressure. Nocturnal fall < 10% of mean daytime pressure is termed as non-dipping phenomenon (NDP).131-133
The nocturnal blood pressure dipping (%) can be also calculated as 100 x [1 – (nighttime BP / daytime BP ratio)]135
In this study nocturnal fall in blood pressure was calculated by subtracting daytime from nighttime blood pressure such that a more negative difference indicates a larger fall in blood pressure at night.134
The mean 24-h, daytime, nighttime fall, % of dippers and non-dippers for both SBP and DBP of this population are given in Table No. 2.
CONSTRUCTION OF CHRONOGRAM
The mean values of systolic blood pressure (SBP) and diastolic blood pressure (DBP) of the population at each timing were calculated. The 24-h rhythm was fitted with timing on X-axis and the mean values of SBP and DBP on Y-axis and illustrated as chronogram 1.
Determination of Dipping and Non-Dipping Phenomenon of
Circadian Rhythm of Blood Pressure In Specific Normotensive
Subpopulations
1) Normotensive males 2) Normotensive females 3) Normotensives aged > 50 4) Normotensives aged < 50 5) Normotensives employed 6) Normotensives unemployed
Determination of Dipping and Non-Dipping Phenomenon of
Circadian Rhythm of Blood Pressure In Specific
Subpopulations of Males And Females
METHOD
To assess the extent of modulation of dipping and non-dipping of the circadian rhythm of blood pressure by the factor sex, in a subpopulation of males alone blood pressure measurements were done as mentioned under the “blood pressure recordings” in part -1. Informed consent was obtained from all the subjects. The mean SBP and DBP of the subpopulation at various timings were calculated.
CONSTRUCTION OF THE CHRONOGRAM
A similar study was conducted in a subpopulation of females alone. The circadian rhythms for SBP and DBP are given in chronogram 3.
Determination of Dipping and Non-Dipping Phenomenon of
Circadian Rhythm of Blood Pressure In Specific
Subpopulations of Normotensives Aged Above 50 and Below 50
METHOD
To assess the extent of modulation of dipping and non-dipping of the circadian rhythm of blood pressure by the factor age, in a subpopulation of normotensives aged above 50, blood pressure measurements were done as mentioned under the “blood pressure recordings” in part -1. Informed consent was obtained from all the subjects. The mean SBP and DBP of the subpopulation at various timings were calculated.
CONSTRUCTION OF CHRONOGRAM
The 24-h circadian rhythm was fitted with the timings on the X-axis and the mean SBP and DBP values of the subpopulation at various timings on the Y axis. The 24-h rhythms of SBP and DBP are given in chronogram 4.
Determination of Dipping and Non-Dipping Phenomenon of
Circadian Rhythm of Blood Pressure In Specific
Subpopulations of Employed And Unemployed Normotensives
METHOD
Job strain is reported to influence the human blood pressure. Hence to assess the extent of modulation of dipping and non-dipping of circadian rhythm of blood pressure by job strain this study was designed. Both males and females employed and aged between 25-55 were selected as the subjects. The blood pressure was recorded as mentioned under ‘BP recordings’ in part -1 after getting the informed consent from the subjects. The mean values of SBP and DBP of the subpopulation were calculated for each timing.
CONSTRUCTION OF THE CHRONOGRAM
The 24-h rhythm was fitted with the timings on the X axis and mean values of SBP and DBP on Y axis. The rhythms of SBP and DBP are given in chronogram 6.
A similar study was conducted in an unemployed population. The rhythms for SBP and DBP are given in chronogram 7.
PART II
Determination of Dipping and Non-dipping Phenomenon of
Circadian Rhythm of Blood Pressure In A Hypertensive
Population.
METHOD
STUDY POPULATION
The study population was composed of 276 hypertensive patients who have already been on treatment with the following antihypertensive drugs/combinations viz Beta blockers (BB), Calcium channel blockers(CCB), and Angiotensin converting Enzyme inhibitors (ACEI) and their combinations.
INCLUSION CIRTERIA
Subjects with the following characteristics were included in this study i) Hypertensive patients whose sitting BP was not > 150 mmHg
systolic and 95mmHg diastolic on atleast two occasions before the start of the study.
ii) No history of hypertensive related complications (coronary artery disease, heart failure and renal insufficiency etc).
iii) No laboratory evidence of diabetes mellitus. iv) No previous/present lipid lowering treatment.
Determination of Dipping and Non-Dipping Phenomenon of
Circadian Rhythm of Blood Pressure In Specific Hypertensive
Subpopulations
To assess if dipping and non-dipping phenomena were influenced by the factors such as sex, age and job strain, the Hypertensive population was divided into 6 subpopulations as given below.
Hypertensive males Hypertensive females Hypertensives aged > 50 Hypertensives aged < 50 Hypertensives employed Hypertensives unemployed
The patients of the main hypertensive population and the subpopulations were found to be on the following 7 types of drug/combinations and hence grouped under 7 categories.
Beta blockers(BB) alone - Category 1
Calcium channel blockers (CCB) alone - Category 2 Angiotensin converting enzyme Inhibitors (ACEI)alone - Category 3
BB + CCB - Category 4
CCB + ACEI - Category 5
ACEI + BB - Category 6
The number of patients in the 7 categories of the main hypertensive population and subpopulations is given as Venn diagram 1-7.
Venn diagram 1 - Illustrating the total number of
HYPERTENSIVES ON DIFFERENT
ANTI HYPERTENSIVE DRUGS / COMBINATIONS
Category 1 - Beta Blocker (BB)
Category 2 - Calcium Channel Blockers - CCB
Category 3 - Angiotensin Converting Enzyme Inhibitors (ACEI) Category 4 - BB + CCB
Category 5 - CCB + ACEI Category 6 - ACEI + BB
36 42 41
44 38
38
37
Category - 2 Category - 4
Category - 5 Category - 6
Category - 7
Venn diagram 2-
HYPERTENSIVE MALES ON DIFFERENT Anti HYPERTENSIVE DRUG / COMBINATIONS
Illustrating the number of
19 21 22
23 20
20
20
Venn diagram 3 - Illustrating the number of
HYPERETENSIVE FEMALES ON DIFFERENT
Anti Hypertensive DRUG / COMBINATIONS
16
21
19
21
19
18
17
Venn diagram 4 - Illustrating the number of
HYPERTENSIVES AGED > 50 on different anti hypertensive drug
Combinations
17 22 19
23 21
22
18
Venn diagram 5 - Illustrating the number of
HYPERETENSIVE AGED < 50 of different anti hypertensive drug
Combinatitons
n = 134
18 20 22
21 18
16
Venn diagram 6 - Illustrating the number of
HYPERTENSIVES EMPLOYED on different anti- hypertensive drug Combinations
n = 145
18 23 21
23 21
22
17 19 20
21 18
16
20
Venn diagram 7 - Illustrating the number of
HYPERTENSIVES UNEMPLOYED on different anti hypertensive drug Combinations
RECORDING OF BLOOD PRESSURE
Blood Pressure was recorded in each subject in the following way
The first measurement was recorded at 6 a.m. then at 7 a.m and 8 a.m. followed by measurements at 2-h intervals till 10 p.m. Recording of blood pressure was completed with the last reading at 6 a.m. of the following day. Thus recording which started at 6 a.m. of the previous day ended with the final recording at 6 a.m. of the following day.
Calculation of the variables of the circadian rhythm of blood pressure
The mean 24-h blood pressure, mean daytime blood pressure, nighttime fall in blood pressure, % of dippers for both systolic Blood pressure (SBP) and diastolic blood pressure (SBP and DBP) of the main hypertensive population and the subpopulations were calculated in the following way.
1) The above mentioned parameters were calculated for all the categories of the main hypertensive population and for each subpopulation.
2) The % of dippers of the subpopulations was calculated from the % dippers of the categories of the subpopulations. The other parameters were calculated from the subjects of each subpopulation.
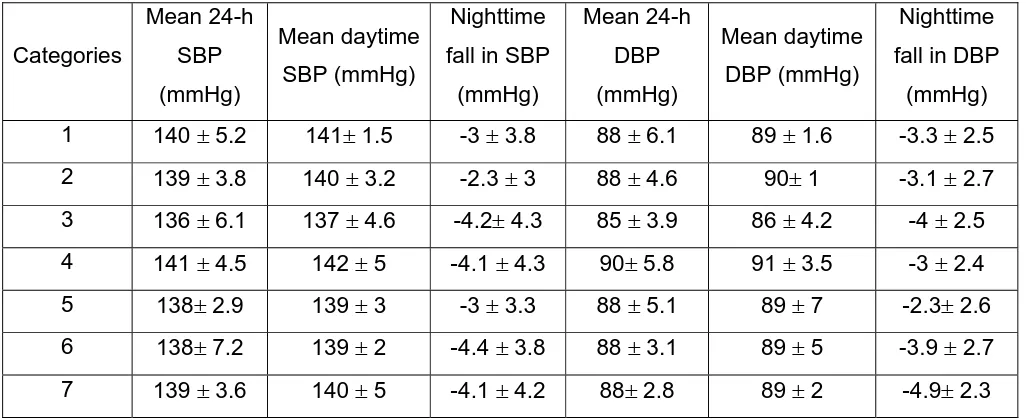
The mean 24-h, daytime and nighttime fall in SBP and DBP of the 7 categories of hypertesnive population and that of the total hypertensive population are given in Table No. 6 and 7 respectively.
The mean 24-h, daytime and nighttime fall in SBP and DBP of the 7 categories of subpopulations of males, females, hypertesnives aged above and below 50, hypertesnives employed and unemployed are given in Table No. from 8-13.
The mean 24-h, mean daytime, nighttime fall in SBP and DBP of hypertesnive subpopulations and % of dippers and non-dippers for SBP and DBP of the subpopulations are given in Tables 14 and 15 respectively.
The comparison of the derived variables of blood pressure between the normotensive and hypertesnive subpopulations is given in Tables form 16-21. The comparison of the derived variables of blood pressure between the normotensive and hypertensive populations is given in Table No.22.
CONSTRUCTION OF CHRONOGRAMS
RESULTS
Blood Pressure
Arterial blood pressure is generated by the interplay between blood flow and the resistance to blood flow. It reaches a peak during systole (systolic pressure) and a nadir at the end of diastole (diastolic pressure). The arterial blood pressure is recorded as systolic pressure over diastolic pressure. Pulse pressure, the difference between systolic and diastolic pressure is an indicator of the tone of the arterial walls. Arterial blood pressure can be defined hemodynamically as the product of cardiac output (CO) and total peripheral resistance (TPR) ie BP = CO x TPR.136
Under normal physiological conditions the arterial blood pressure stays within narrow limits. It may reach its height during physical and emotional stress and fall to its lowest level during sleep. Blood pressure tends to be lower in women than men and it rises with age. In general, blood pressure is higher in winter than in summer and this factor may be partly responsible for the higher mortality from cardiovascular diseases in winter.137
It is well known that the incidence of hypertension is high in males.138 Hence a separate study was conducted in specific subpopulations consisting of males and females alone, to study the influence of sex on the circadian rhythm of blood pressure.
Large literature states that blood pressure increases with age.139 However recent studies correlate that blood pressure changes accompanying aging may be due to stress.140 Many studies which have been conducted so far correlate job strain with increase in blood pressure.141-145 Hence DP and NDP of circadian rhythm were determined in separate subpopulations consisting of normotensives aged above and below 50 and normotensives employed and unemployed to assess the influence of age and job strain on the circadian rhythm of blood pressure in this population.
Results of DP and NDP of Circadian rhythm of blood pressure in the Normotensive population.
Chronogram-1 illustrates the 24-h SBP and DBP profile of the normotensive population. During daytime both the SBP and DBP were higher than the mean 24-h SBP and DBP though not statistically significant. The mean nighttime decline in SBP and DBP were –7.1 ± 5.4mm Hg and –6 ± 3.1mm Hg respectively. The % nighttime decline to mean daytime blood pressure was < 10% in case of both SBP and DBP. This was reflected in the % of dippers in the normotensive population ie. in this population 60 ± 4 were dippers for SBP ie their nighttime decline was > 10% of mean daytime systolic blood pressure. The mean % of dippers for DBP was 57 ± 4 i.e. 57 ± 4% of the population showed a nighttime decline > 10% of 80 ± 3 mm Hg (mean daytime DBP). The percentage of non-dippers for SBP and DBP were 40 ± 4 and 42 ± 2 respectively, which was significantly lower than the % of dippers.
RESULTS OF DP AND NDP OF CIRCADIAN RHYTHM IN SPECIFIC SUBPOPULATIONS
MALES
respectively. But only the mean % of dippers of DBP in males was statistically significant from mean % dippers of DBP of the female population (P<0.05). The percentage of non-dippers for SBP and DBP were 47 ± 4 and 33 ± 7 respectively. The percentage of dippers was significantly higher than that of non-dippers in males with regard to DBP only and it was insignificant with regard to SBP.
Females
Chronogram-3 illustrates the SBP and DBP profile of the subpopulation of females. The mean daytime SBP and DBP were 118 ± 5 mmHg and 77 ± 6 mmHg and slightly higher than 24-h SBP and DBP (insignificant). Though these values were less then those observed in males they were not statistically different from that of males.
The mean nighttime decline in SBP and DBP were –7.9 ± 5.6 mmHg and –5.4 ± 2.5mmHg respectively. The nighttime decline to mean daytime blood pressure was < 10% in case of both SBP and DBP. The % of dippers for SBP and DBP were 65 ± 7 and 48 ± 3 respectively. The percentage of non-dippers for SBP and DBP were 36 ± 9 and 52 ± 6 respectively. The DP was not significantly different from NDP in this subpopulation for both SBP and DBP.
NORMOTENSIVE POPULATION AGED ABOVE 50
mmHg respectively. The mean nighttime decline for SBP and DBP were –6.2 ± 5.3 mmHg and –4.1 ± 3 mmHg respectively. Hence the % dippers in this population was 47 ± 6 for SBP and 48 ± 4 for DBP respectively. The percentage of non-dippers for SBP and DBP were 53 ± 8 and 51 ± 5 respectively. The incidence of DP was not significantly higher than NDP in this subpopulation for both SBP and DBP.
NORMOTENSIVE POPULATION AGED BELOW 50
The chronogram-5 illustrates the SBP and DBP profile in the normotensive subpopulation aged < 50. The mean daytime blood pressure for SBP and DBP were 120 ± 6mm Hg and 78 ± 5 mm Hg respectively. The nighttime decline in SBP and DBP were –8.3 ± 5.2 mmHg and –6.3 ± 2.8 mmHg respectively. Hence the % of dippers was statistically higher for both SBP and DBP in this subpopulation than non-dippers and when compared to the population aged > 50. The percentage of non-dippers for SBP and DBP were 21 ± 5 and 31 ± 4 respectively, which was significantly lower than that of DP of this subpopulation.
NORMOTENSIVE POPULATION EMPLOYED
phenomenon (DP) and hence % of dippers for SBP and DBP were 40 ± 3 and 38 ± 4 respectively. The % of dippers for SBP and DBP (P< 0.05) was significantly lower than the dippers of the unemployed population. The percentage of non-dippers for SBP and DBP were 60 ± 5 and 62 ± 6 respectively. The percentage of dippers was significantly lower than non-dippers in this subpopulation.
NORMOTENSIVE POPULATION UNEMPLOYED
Chronogram-7 illustrates the SBP and DBP profiles of the subpopulation of unemployed subjects. The mean daytime SBP and DBP were 119 ± 3 mmHg and 79 ±5 mmHg respectively. The nighttime decline for SBP and DBP were –8.5 ± 5.7 mmHg and –7.1 ± 1.1 mmHg respectively. The % of dippers for SBP and DBP were 84 ± 7 and 82 ± 6 respectively. The incidence of dipping was significantly higher for both SBP and DBP when compared to non-dipping within this population and to that of the employed subpopulation. The percentage of non-dippers for SBP and DBP were 17 ± 4 and 18 ± 4 respectively. Likewise, NDP was significantly lower in this subpopulation against the employed subpopulation.
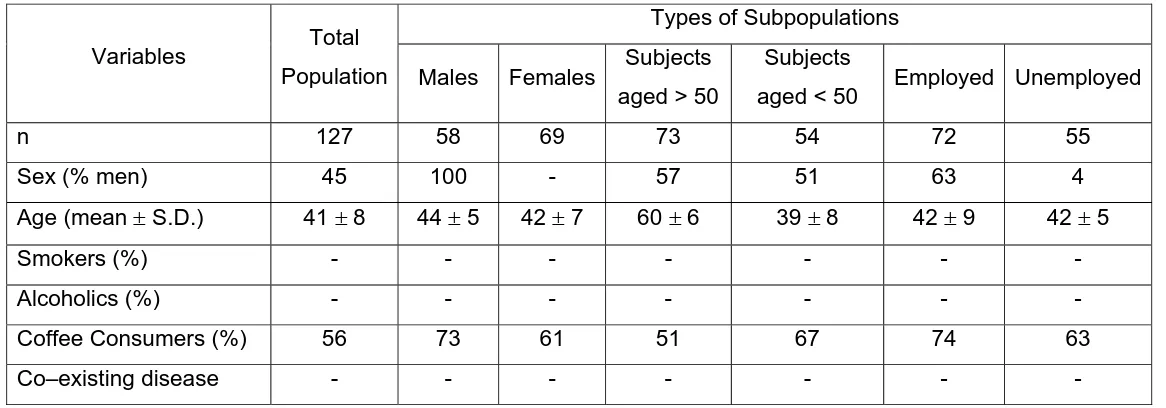
TABLE NO - 1
Demographic Characteristics Of The Study Population (Normotensives)
Types of Subpopulations
Variables Total
Population Males Females Subjects
aged > 50
Subjects
aged < 50 Employed Unemployed
n 127 58 69 73 54 72 55
Sex (% men) 45 100 - 57 51 63 4
Age (mean ± S.D.) 41 ± 8 44 ± 5 42 ± 7 60 ± 6 39 ± 8 42 ± 9 42 ± 5
Smokers (%) - - - -
Alcoholics (%) - - - -
Coffee Consumers (%) 56 73 61 51 67 74 63
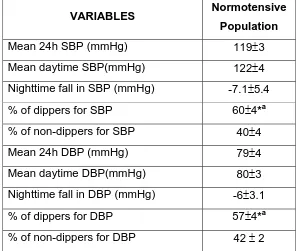
TABLE NO - 2
Descriptive statistics of 24-h blood pressure profiles in a normotensive population.
VARIABLES Normotensive
Population
Mean 24h SBP (mmHg) 119±3
Mean daytime SBP(mmHg) 122±4
Nighttime fall in SBP (mmHg) -7.1±5.4
% of dippers for SBP 60±4*a
% of non-dippers for SBP 40±4
Mean 24h DBP (mmHg) 79±4
Mean daytime DBP(mmHg) 80±3
Nighttime fall in DBP (mmHg) -6±3.1
% of dippers for DBP 57±4*a
% of non-dippers for DBP 42 ± 2
SBP – Systolic Blood Pressure, DBP – Diastolic Blood Pressure
Students ‘t’ test was used to compare % of Dippers against Non-dippers.
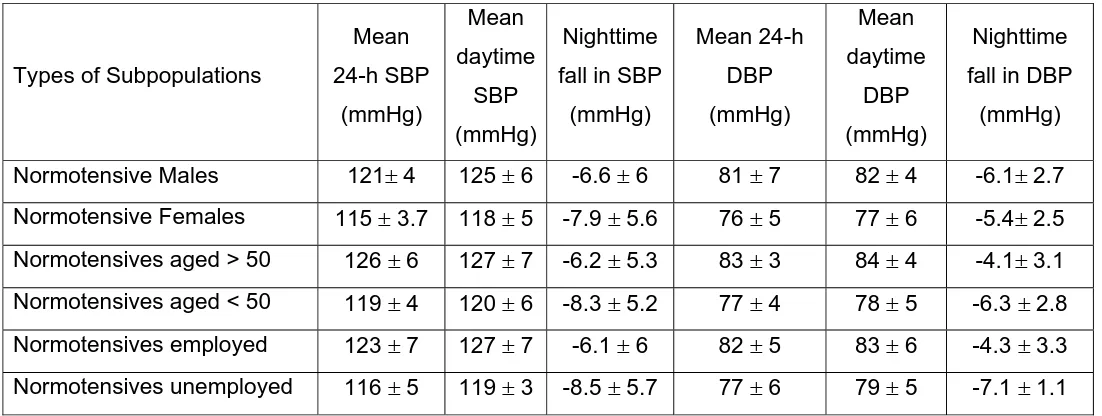
TABLE NO - 3
Descriptive statistics of 24-h blood pressure profiles in normotensive subpopulations.
Types of Subpopulations
Mean 24-h SBP (mmHg) Mean daytime SBP (mmHg) Nighttime
fall in SBP
(mmHg) Mean 24-h DBP (mmHg) Mean daytime DBP (mmHg) Nighttime
fall in DBP
(mmHg)
Normotensive Males 121± 4 125 ± 6 -6.6 ± 6 81 ± 7 82 ± 4 -6.1± 2.7
Normotensive Females 115 ± 3.7 118 ± 5 -7.9 ± 5.6 76 ± 5 77 ± 6 -5.4± 2.5
Normotensives aged > 50 126 ± 6 127 ± 7 -6.2 ± 5.3 83 ± 3 84 ± 4 -4.1± 3.1
Normotensives aged < 50 119 ± 4 120 ± 6 -8.3 ± 5.2 77 ± 4 78 ± 5 -6.3 ± 2.8
Normotensives employed 123 ± 7 127 ± 7 -6.1 ± 6 82 ± 5 83 ± 6 -4.3 ± 3.3
Normotensives unemployed 116 ± 5 119 ± 3 -8.5 ± 5.7 77 ± 6 79 ± 5 -7.1 ± 1.1
Statistics : Students ‘t’ test was used to compare 2groups.
(Males vs Females, Normotensives aged > 50 Vs < 50, Normotensives employed Vs Unemployed)
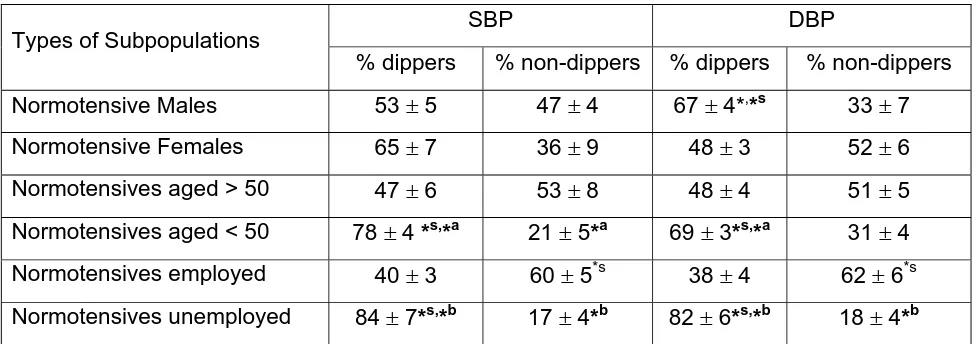
TABLE NO - 4
Dippers and Non-dippers in the normotensive subpopulations.
SBP DBP Types of Subpopulations
% dippers % non-dippers % dippers % non-dippers
Normotensive Males 53 ± 5 47 ± 4 67 ± 4*,*s 33 ± 7
Normotensive Females 65 ± 7 36 ± 9 48 ± 3 52 ± 6
Normotensives aged > 50 47 ± 6 53 ± 8 48 ± 4 51 ± 5
Normotensives aged < 50 78 ± 4 *s,*a 21 ± 5*a 69 ± 3*s,*a 31 ± 4
Normotensives employed 40 ± 3 60 ± 5*s 38 ± 4 62 ± 6*s
Normotensives unemployed 84 ± 7*s,*b 17 ± 4*b 82 ± 6*s,*b 18 ± 4*b
Statistics : Students ‘t’ test is used to compare between 2groups
Males vs Females- *implies significance (p < 0.05)
Normotensives aged > 50 Vs < 50 -*a implies significance (p<0.05)
Normotensives employed Vs Unemployed - *b implies significance (p<0.05)
Chronogram 1
24-h SBP and DBP Profile in Normotensives
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
Chronogram 2
24-h SBP and DBP Profile in Normotensive Males
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
Chronogram 3
24-h SBP and DBP Profile in Normotensive Females
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
Chronogram 4
24-h SBP and DBP Profile in Normotensives aged > 50
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
Chronogram 5
24-h SBP and DBP Profile in Normotensives aged < 50
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
Chronogram 6
24-h SBP and DBP Profile in Normotensives employed
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
Chronogram 7
24-h SBP and DBP Profile in Normotensives unemployed
0 20 40 60 80 100 120 140
7 a.m. 8 a.m. 10a.m. 12 a.m. 2 p.m. 4 p.m. 6 p.m. 8 p.m. 10 p.m. 6 a.m
Time
Blood pressure (mmHg)
RESULTS OF DP AND NDP IN HYPERTENSIVE POPULATION
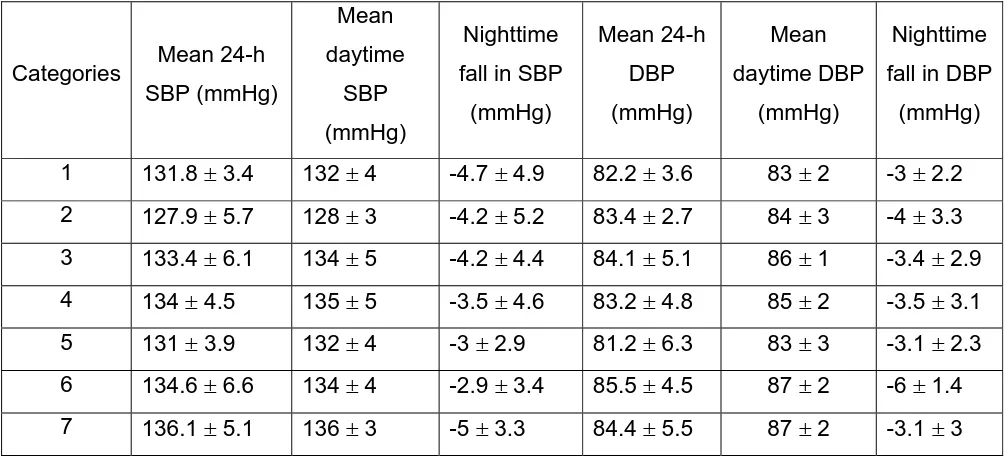
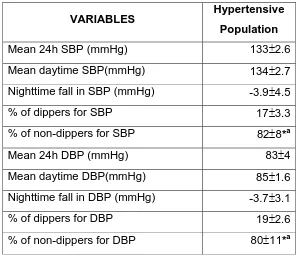
The mean 24-h SBP and DBP, daytime SBP and DBP, nighttime fall in SBP and DBP in all the seven categories are given in table No.6. The same parameters along with the % of dippers and non-dippers of hypertensive population are given in Table No.7.
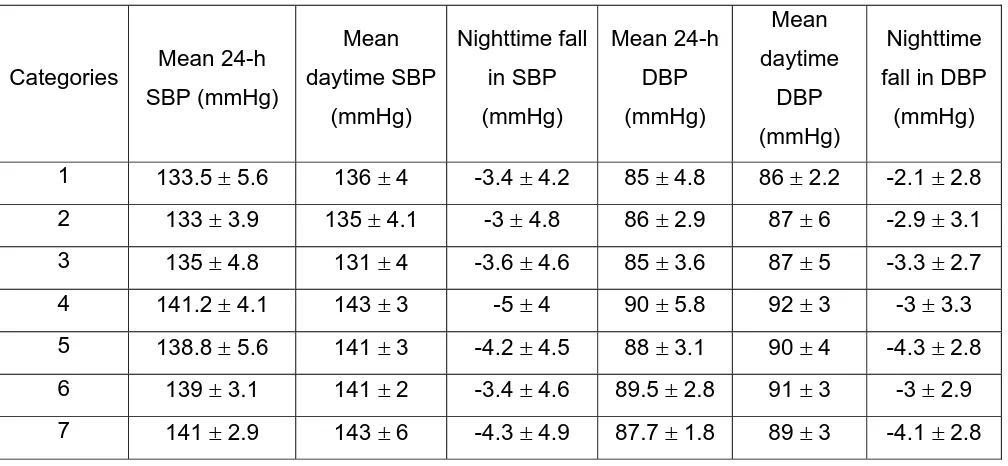
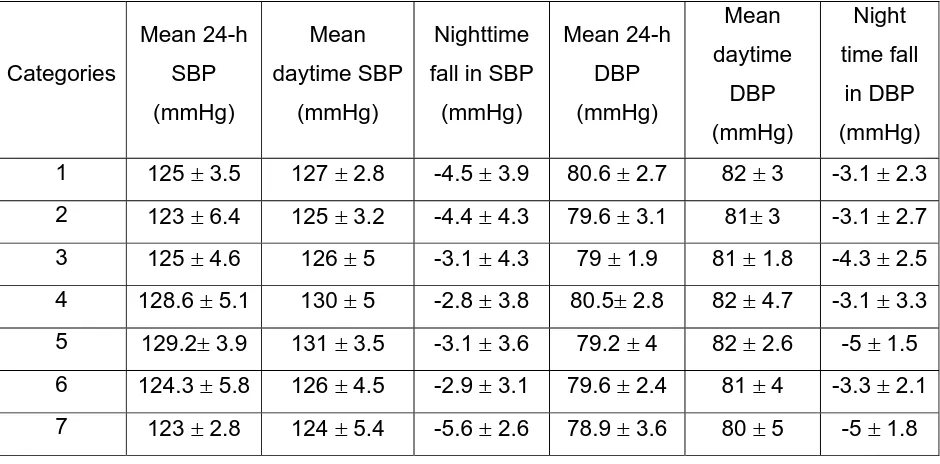
The mean 24-h SBP and DBP, daytime SBP and DBP, nighttime fall in SBP and DBP in the seven categories of the hypertensive subpopulations are given in Tables from 8-13.
No statistical significance has been found between the categories for the 24-h SBP and DBP, daytime SBP and DBP and nighttime fall in SBP and DBP in the hypertensive population and subpopulations. The daytime SBP and DBP were found to be slightly higher than the mean 24-h SBP and DBP in all the categories though they were not statistically significant.
The mean 24-h SBP and DBP, daytime SBP and DBP, nighttime fall in SBP and DBP of the hypertensive subpopulations is given in Table No.14. No statistical significance was observed between the subpopulations except the mean 24-h SBP, which was significantly lower in hypertensive females against males, hypertensives aged below 50 against hypertensives aged above 50 and hypertensives unemployed against hypertensives employed.
non-dippers for both SBP and DBP was significantly lower in all the hypertensive subpopulations.
The comparison of these parameters between hypertensives males and normotensives males is given in Table No.16. In this same way, the comparison between hypertensive and normotensive females, hypertensives and normotensives aged above 50, hypertensives and normotensives aged below 50, hypertensives and normtensives employed and umemployed are given in Tables 17 to 21 respectively.
The comparison of these parameters between the hypertensive and normotensive population is given in Table No.22.
In all the categories of the subpopulation and the main hypertensive population the mean daytime SBP and DBP were slightly higher than the mean 24-h SBP and DBP though they were not statistically significant.
Hence in this hypertensive population of South Tamil Nadu, it is observed that the incidence of DP was lower than that NDP.
COMPARISON BETWEEN NORMOTENSIVE AND HYPERTENSIVE POPULATIONS
TABLE NO - 5
Demographic Characteristics Of The Study Population (Hypertensives)
Types of Hypertensive Subpopulations
Variables
Total Number
of
Hypertensives
Hypertensive
Males
Hypertensive
Females
Hypertensives
aged > 50
Hypertensives
aged < 50
Hypertensives
empolyed
Hypertensives
unemployed
n 276 145 131 142 134 145 131
Sex (% men) 56 100 - 62 39 58 47
Age (mean ± S.D.) 46 ± 8 40 ± 8 47 ± 7 61 ± 8 43 ± 5 40 ± 9 46 ± 8
Smokers (%) - - - -
Alcoholics (%) - - - -
Coffee Consumers (%) 38 46 49 33 24 61 52
Duration of
TABLE NO - 6
Descriptive Statistics of 24 h blood pressure profile in Hypertensive Population under 7 categories of drug / combinations
Categories Mean 24-h
SBP (mmHg) Mean daytime SBP (mmHg) Nighttime
fall in SBP
(mmHg) Mean 24-h DBP (mmHg) Mean daytime DBP (mmHg) Nighttime
fall in DBP
(mmHg)
1 131.8 ± 3.4 132 ± 4 -4.7 ± 4.9 82.2 ± 3.6 83 ± 2 -3 ± 2.2
2 127.9 ± 5.7 128 ± 3 -4.2 ± 5.2 83.4 ± 2.7 84 ± 3 -4 ± 3.3
3 133.4 ± 6.1 134 ± 5 -4.2 ± 4.4 84.1 ± 5.1 86 ± 1 -3.4 ± 2.9
4 134 ± 4.5 135 ± 5 -3.5 ± 4.6 83.2 ± 4.8 85 ± 2 -3.5 ± 3.1
5 131 ± 3.9 132 ± 4 -3 ± 2.9 81.2 ± 6.3 83 ± 3 -3.1 ± 2.3
6 134.6 ± 6.6 134 ± 4 -2.9 ± 3.4 85.5 ± 4.5 87 ± 2 -6 ± 1.4
7 136.1 ± 5.1 136 ± 3 -5 ± 3.3 84.4 ± 5.5 87 ± 2 -3.1 ± 3
Statistics – One way anova followed by Newmankeul’s multiple range test was used. No statistical
significance was observed among categories regarding mean –24-h, mean daytime, nighttime fall for both