City, University of London Institutional Repository
Citation
:
Burns, D. H., Allen, P. M., Edgar, D. F. ORCID: 0000-0001-9004-264X and
Evans, B. J. W. (2019). Sources of error in clinical measurement of the amplitude of
accommodation. Journal of Optometry, doi: 10.1016/j.optom.2019.05.002
This is the published version of the paper.
This version of the publication may differ from the final published
version.
Permanent repository link:
http://openaccess.city.ac.uk/id/eprint/23065/
Link to published version
:
http://dx.doi.org/10.1016/j.optom.2019.05.002
Copyright and reuse:
City Research Online aims to make research
outputs of City, University of London available to a wider audience.
Copyright and Moral Rights remain with the author(s) and/or copyright
holders. URLs from City Research Online may be freely distributed and
linked to.
www.journalofoptometry.org
REVIEW
Sources
of
error
in
clinical
measurement
of
the
amplitude
of
accommodation
David
H.
Burns
a,b,c,∗,
Peter
M.
Allen
d,
David
F.
Edgar
e,
Bruce
J.W.
Evans
b,c,ea119HighRoad,LondonN28AG,UK
bInstituteofOptometry,56-62NewingtonCauseway,LondonSE16DS,UK
cSchoolofHealthandSocialCare,LondonSouthBankUniversity,103BoroughRoad,LondonSE10AA,UK
dDepartmentofVisionandHearingSciences&VisionandEyeResearchUnit,AngliaRuskinUniversity,EastRoad,CambridgeCB1
1PT,UK
eDivisionofOptometryandVisualScience,SchoolofHealthSciences,City,UniversityofLondon,NorthamptonSquare,London
EC1V0HB,UK
KEYWORDS Amplitudeof accommodation; Accommodative amplitude;
Measurementerror; Clinical;
Push-up
Abstract Measurementoftheamplitudeofaccommodationisestablishedasaprocedureina
routineoptometriceyeexamination.However,clinicalmethodsofmeasurementofthisbasic optical function haveseveralsourcesoferror.Theyarenumerous anddiverse,andinclude depthoffocus,reactiontime,instrumentdesign,specificationofthemeasurementend-point, specificationofthereferencepointofmeasurement,measurementconditions,consideration ofrefractiveerror,andpsychologicalfactors.Severalofthesesourcesofinaccuracyare com-posedofmultiplesub-sources,andmanyofthesub-sourcesinfluencethecommonmethodsof measurementofamplitudeofaccommodation.Considerationofthesesourcesofmeasurement errorcastsdoubtonthereliabilityoftheresultsofmeasurement,onthevalidityofestablished normativevaluesthathavebeenproducedusingthesemethods,andonthevalueofreportsof theresultsofsurgerydesignedtorestoreaccommodation.Clinicianscanreducetheeffectsof someofthesourcesoferrorbymodifyingtechniquesofmeasurementwithexistingmethods, butanewmethodmayfurtherimproveaccuracy.
©2019SpanishGeneralCouncilofOptometry.PublishedbyElsevierEspa˜na,S.L.U.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALABRASCLAVE Amplitudde acomodación; Amplitud acomodativa;
Fuentesdeerrorenlamediciónclínicadelaamplituddeacomodación
Resumen Lamedicióndela amplituddeacomodaciónsehaestablecido comoun
proced-imientodelexamenoptométricoocularrutinario.Sinembargo,losmétodosclínicosdemedición deestafunciónópticabásicatienendiversasfuentesdeerror.Estassonnumerosasydiversas, eincluyenprofundidaddefoco,tiempodereacción,dise˜nodelinstrumento,especificacióndel puntofinaldelamedición,especificacióndelpuntodereferenciadelamedición,condiciones
∗Correspondingauthorat:119HighRoad,LondonN28AG,UK.
E-mailaddress:[email protected](D.H.Burns).
https://doi.org/10.1016/j.optom.2019.05.002
2 D.H.Burnsetal.
Errordemedición; Clínico;
Push-up
delamedición, consideracióndelerrorrefractivo,y factorespsicológicos. Algunasdeestas fuentesdeimprecisiónsecomponendemúltiplessub-fuentes,muchasdelascualesinfluyenen losmétodoscomunesdemedicióndelaamplituddeacomodación.Laconsideracióndeestas fuentesdeerrorenlamediciónplanteadudassobrela fiabilidaddelosresultadosdedicha medición, lavalidezdelosvalores normativosestablecidosquesehanproducidoutilizando estosmétodos,yelvalordelosinformessobreresultadosdelacirugíadise˜nadapararestablecer la acomodación.Los clínicospueden reducirlosefectos dealgunasde lasfuentesde error, modificandolastécnicasdemediciónconayudadelosmétodosexistentes,aunqueeldesarrollo deunnuevométodopodríamejorarlaprecisión.
©2019SpanishGeneralCouncilofOptometry.PublicadoporElsevierEspa˜na,S.L.U.Esteesun art´ıculoOpenAccessbajolalicenciaCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Background
Amplitude of accommodation (AoA) is an eye’s maximum rangeoffocussingpowerataparticulartime.Itisexpressed indioptres.
In the United Kingdom (UK), AoA is the parameter of accommodationthatismost commonlyassessedclinically. Competencein the measurementof AoA, andin noother aspectof accommodation, is statutorilyrequiredof every aspiringUKoptometrist1andmeasurementofAoAisa
rec-ommendedcomponentofaroutineeyeexaminationwhen
‘‘clinicallyappropriate’’.2
‘‘Accommodationrule’’isincludedinthelistoftwenty
principalitems of clinical equipmentrequired for routine
eye examinations in the UK.3 In North America
measure-mentofAoAisoneoftheitemsintheSkeffington21-point
routine.4 AoAisincludedinthesyllabi oftheWorld
Coun-cilofOptometry5 andEuropeanCouncilof Optometryand
Optics.6
AreviewoftheclinicalmeasurementofAoAbriefly
men-tionedsourcesoferror.7Thepresentreviewdescribesthese
sourcesof error in moredetail, facilitating better
under-standingoftheaccuracyofcurrentmethods.
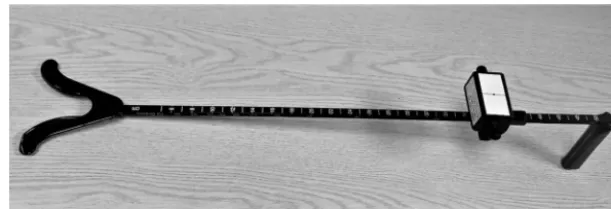
TheRAFRuleistheonlydevicemarketedintheUKfor
theclinical measurementof AoA.Itwasfirstdescribed in
1956.8ShowninFig.1,itisagraduatedrailjustover0.5m
inlengthwithahandleatoneend,abifurcationattheother
endtobeheldagainstthepatient’scheekbones,andbearing
avisualtest-object.Thetest-objectdisplayshigh-contrast
black-on-whiteprintinarangeofsizesandcanbeslidalong
therail.
Methods
of
measurement
FourmethodsofmeasuringAoAareencounteredinclinical
practiceanddescribedintheliterature.Theyarepush-up,
push-down,minuslens,andretinoscopy,andaredescribed
below.
Push-up
Many authors assert that push-up is the most prevalent
method.9---11 Inthepush-upmethodtheexaminerinstructs
thepatienttoreportwhenatest-object becomesblurred
asitisbroughtgraduallynearertotheeye.Deviceswhich
arearulerwithaslidingtest-objectareoftenusedforthis
measurement.TheRAFruleisanexampleofsuchadevice.
Itisusedasfollows.Whenthefirstslightbutsustainedblur
ofthevisualtest-objectisreportedtheexaminernotesthe
positionoftheprintonascalemarkedontherail.Thisscale
shows thedistanceof theprintfromtheeyeandalsothe
AoAasthereciprocal,inmetres,ofthatdistance.Textbooks
ofbasicoptometrygenerallyprovidefullerdescriptions12---15
oftheuseoftheRAFRule,differingmoderatelyfromeach
otherinsomedetailsoftechnique.
Push-down
Thepush-downmethodcanalsousetheRAFRuleandsimilar
devices.The objectismovedawayfromthepatient,from
being toonear for thepatient toresolve, until it can be
seen.
Thismethodparticularlylacksstandardisationof
nomen-clature and of technique. For example, different authors
specify differing end-points. In the earliest description16
of the push-down method the test object is moved away
fromtheeyeuntilthepatientreportswhenitfirstbecomes
‘‘quite clear’’ but in subsequent reports differing
end-pointcriteriawereusedsuchas‘‘sharpandclear’’17 ‘‘just
becomesclear’’18‘‘absolutelyclear’’14and‘‘just
recognis-able’’.15
Namingthemethod,anditsendpointcriterion,presents
someconfusion.Whenthe‘‘justrecognisable’’criterionwas
firstdescribed19 thepush-downapproachwasdescribedas
the ‘‘modifiedpush-up method’’which hasbeen used20,21
inresearchwhereithasbeentermedthe‘‘modified
push-downmethod’’22whichresembledthe‘‘modifiedpull-away
method’’inanotherreport.15However,the‘‘modified
push-downmethod’’inonereport17 differedsignificantlytothe
‘‘modified push-down method’’ in another22 and to the
‘‘modifiedpush-upmethod’’inanother23 allofwhichused
auxiliary fixed-power diverging trial lenses to extend the
Figure1 TheRAFRule.
Minuslens
Intheminuslensmethod24,25negativesphericallenspower
is added to the distance refractive correction until the
patientcannotmaintaintheinitialacuityatapre-set
view-ingdistancewellbeyondtheexpectednearpoint.TheAoA
is given by the maximum power added while the patient
can maintain focus, corrected for the viewing distance’s
vergence.
This method should only be used for monocular
mea-surement and only under monocular conditions. These
limitationsarisebecauseaccommodationandconvergence
worktogetheralthoughthelinkbetweentheiroperationis
notrigid.26,27Therefore,theminuslensmethodmayinduce
more convergence than would be required for the
view-ing distance, causing one eye toover-converge, resulting
indiplopia;or,ifbinocularviewingismaintained,the
pre-settingofconvergencemaylimitaccommodation.However,
unlikethepush-upmethodandsomevariantsofthe
push-downmethod,itonlyrequirestheresolutionofanobject,
andsomaybeeasiertoperform,fortheexaminerandfor
thepatient,thanreportingontheclarityofthetarget.
Retinoscopy
AoA can also be measured using a retinoscope. Although
retinoscopy relies on the clinician’s interpretation of the
retinoscopyreflex,itrequiresnojudgementbythepatient.
ItcanbeusedformeasurementofAoAbystimulating
accom-modationmaximallywhilethepractitionerdeterminesthe
end-point. Several investigators28---31 have described the
techniqueindetail.
This method requirespractitioner skill,judgement and
experience.28,30,32 That may explain why its use has
been reported less often than other methods. The need
to minimise glare from the retinoscope beam in AoA
measurement28,30isanotherdifficultywiththismethod.
Sources
of
measurement
error
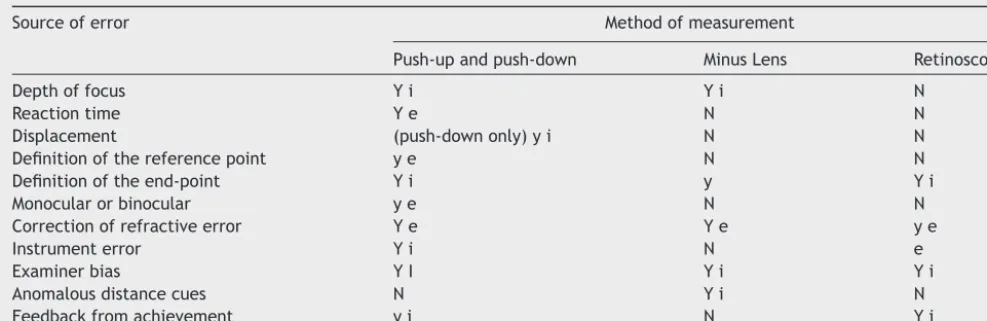
Thereareseveraldistinctsourcesoferrorthataffect
cur-rentclinicalmethodsofmeasuringAoA.Theyarelistedin
Table 1 which also shows the methods affected by each
source of error, andare described inmore detail laterin
thispaper.Theiroveralleffectwouldreducethereliability
ofmeasurement.
Depth
of
focus
Thissourceoferrorwasdefined33astherangeofanobject’s
vergence at the eye without any blur being detected. It
is the result of a wide range of factors, some of which,
suchasdiffraction,cannotbeeliminated,andsome,such
aspupildiameter,thatvary.Therefore,thecontributionof
depthoffocustomeasurementofAoAbyanymethodthat
requirestherecognitionofblurcannotbeaccurately
esti-mated.However,areview34foundthatitwouldbelikelyto
exceedanyothersourceoferror.
During measurement of AoA, by most methods that
requiretherecognitionofblur,thesizeoftheretinalimage
ofthevisualtargetcontinuallychanges.Thesizeisinversely
proportionaltothevisualworking-distance,anddecreases
slightlyduringmeasurementbytheminuslensmethod.This
size-change affects the accuracy of the measurement of
AoA,sincetheeye’sdepthoffocusvarieswithretinalimage
size.47
Ithasbeenproposedthatdepthoffocus,unliketheother
sourcesoferror listedin Table1, isboth an inherentand
abeneficial component of accommodation, ratherthan a
sourceof error. An explorationintothe depthof focusof
theaccommodatedeye35concludedthat‘‘themainpurpose
ofaccommodationisnottomaximiseretinalimagequality
buttoformone thatisgoodenough.’’ Itshould
nonethe-lessbeexcludedwhenmeasuringAoAasdepthoffocusand
accommodationareseparatefunctions.
Reaction
time
Reactiontimeisasourceoferrorthatinfluencesmethodsin
whichmeasurementismadewhilethevergenceofthetest
objectchanges.This errorcanbelimited byreducingthe
rateof change,althoughslower ratesofchange makethe
end-pointlessobvioussoitmaybehardertodiscern.
Reaction timeis the sumof four separate components
thatoccurinthefollowingorderwhentestobjectvergence
changes past the point where noticeable blur (or, in the
push-downmethod,eitherclarityorlegibility)firstoccurs.
Thesecomponentsare:
1. thetimetakentodecidethatthevisualobjectappears
blurredorclear
2. then,thetimetakentovocalisethatdecision
3. followingthat,thetimetakentoregisterthatmessage
4. andfinally,thetimetakentostopthemovementofthe
[image:4.612.143.449.57.161.2]4 D.H.Burnsetal.
Table1 SourcesoferroraffectingtheclinicalmeasurementofAoA.
Sourceoferror Methodofmeasurement
Push-upandpush-down MinusLens Retinoscopy
Depthoffocus Yi Yi N
Reactiontime Ye N N
Displacement (push-downonly)yi N N
Definitionofthereferencepoint ye N N
Definitionoftheend-point Yi y Yi
Monocularorbinocular ye N N
Correctionofrefractiveerror Ye Ye ye
Instrumenterror Yi N e
Examinerbias YI Yi Yi
Anomalousdistancecues N Yi N
Feedbackfromachievement yi N Yi
YmajoreffectyminoreffectNnegligibleeffectiinherenteffecteeffectcanbeeradicated.
Components1and2listedabovedependonthepatient. Components3and4listedabovedependontheexaminer.
Component1,unliketheotherthree,isinfluencedbythe measurementtechnique.Itincreaseslinearlywiththerate ofchange oftest-objectvergencewhenmeasuring accom-modationwiththeminus-lensmethod,andnon-linearlywith therateofchange oftest-object distancewhen measure-mentisonascaleofdistance11becausedioptricdemandis
inverselyproportionaltoviewingdistance.Attypical
max-imumaccommodation levels, moving the test-object one
centimetrerepresentslessthan 0.1D for aforty-year-old
butabout1Dforaten-year-old.
To reduce this error caused by the target being near
tothe eye at the end-point, extra minus lens power can
beaddedinthetrialframewhenmeasuringhigh levelsof
AoA.13,15,17Althoughitcanbeexpectedtoreducethe
reac-tiontimeerror,albeitunsystematically,itwouldintroduce
error due to anomalous distance cues (another source of
error,describedbelow).Furthermore,whenviewingthrough
extra minus spectacle lenses, AoA may be influenced by
refractiveerror.36
Therefore,itwouldbepreferabletomovethetestobject
ataconstantandslowrateofdioptres,ratherthan
centime-tres,persecond.Constantrateofdioptricchange(0.5D/s)
forpush-upmeasurementofAoAhasbeenreported.37 This
strategywouldspreadreaction-timeerror evenlyoverthe
rangeofresultvaluesbutmaybedifficulttoreliablyachieve
without automation.Researchershave adopted quite
var-ied rates including 0.4cm/s,9 1cm/s,38 2cm/s,39 4cm/s
with participants controlling push-down movement17 and
5cm/s20,40,41 which is so fast that the effect of reaction
timeonthetestresultcouldexceedone-thirdofthe
high-est reportedvalues. Forexample, if thenear point were
at7.5cm(13.3D)movementcouldstopat5cm(20D).This
may be one reason why researchers from the earliest42
to present times38,39,43 obtained particularly high values,
exceeding20D,withthepush-upmethod.
Thesecondcomponentofreaction-timelistedabovemay
increaseifthepatientfeelsapprehensiveaboutthe
proce-dureandhencereluctanttodeclarethatthetestobjectis
blurred.Itmayalsoincreaseifthepatientisaccustomedto
blur.44
It would appearlikely that components2 and 3 listed
above,ofreaction-time,couldbeeliminatedifthepatient,
insteadoftheexaminer,weretomovethetarget.This
pos-sibilitywasaddressedinonestudy45 andnotsupported,as
thestudyfoundslightlyhigherresultswhentheparticipant
heldthetarget,moresowhenusingpush-upthanwhenusing
push-down.However,thedatawerenotpresentedtoenable
anestimateofthestatisticalsignificanceofthisresult.
Fur-thermore,an advantageof theexaminer,notthepatient,
movingthetargetwouldbetoretainsomestandardisation
ofthespeedofmovement.
Some early investigators41,45,46 found lower results for
AoA with the push-down method than with the push-up
method. Later researchers17,18 found similar results with
the twomethods and speculated that the earlier findings
were dueto thedifferencein reaction timebetween the
push-upandpush-downmethods.Anotherstudy40found
sim-ilarresultswiththetwomethods,for25participantsaged
10---40years,citingotherstudiesthatfoundthesameeffect,
buttheirpush-downmethodusedtheend-pointcriterionof
just recognisingthe test-object, giving large errordue to
depthoffocusasshownbyearlierresearch.47Theerrordue
todepthoffocusin push-downtorecognitionwouldhave
tendedtocounterbalancetheerrorduetoreactiontimein
push-up.
Someresearch11,48,49adoptedthestrategyofmovingthe
push-uptestobjectinstepchanges.Thiswouldhave
elimi-natedreaction-timeerrorbecausethetargetwasstationary
duringmeasurement.However,theincreasedtestingtimeof
thisstrategymayhavereduceditsutilityanditsaccuracy.
Displacement
This error is causedby displacement of themoving visual
objectbeyondthe end-point,asfollows.The end-point is
registered when, in the push-downmethod, the observer
detectsthatthetestobject’ssharpnessstopschanging.This
judgementrequirescomparisonofsharpnessatpointsafter
passing the near point, whereas in push-up the observer
seeksforthesharpnesstostartchanging,bycomparingthe
[image:5.612.56.550.74.234.2]Therefore,theend-pointisdisplacedfurtherfromthenear
pointinpush-downbecausethetest-objectmusttravel
fur-therfromtheend-pointtoestablishthatthereisnofurther
improvementinclarity.
Displacement affectsonlythepush-downmethodusing
theend-point criterionofclarity,causing underestimation
ofAoA.Thedisplacementerrorwouldbeexpectedtooccur
in the minus lens method if the end point was a change
fromblurtoclarity,althoughnotinthemoreusual
proce-durewhenthepatientisaskedtodetectadropinacuity13
Displacementwouldincreasewithalargerreactiontimeof
the patient. Displacement does not appear to have been
addressedintheliterature.
Measurement
conditions
Resultswithanymethodofmeasurementcanbeaffectedby
theconditionsofmeasurement.Therefore,theseconditions
shouldbe specified, andstandardisedif possible.In
mea-suringAoA,thereareseveralaspectsofthe measurement
conditionsthatcaninfluencetheoutcomeandtheseare
dis-cussedbelowusingexamplesfromAoAstudies.There has
beennostandardisationoftheseorothertestconditions.
Definitionofthereferencepoint
Astraightlineistheshortestdistancebetweentwopoints,
and the points must be specified when giving the length
oftheline.When measuringAoA,alengthmeasuredfrom
thepatientistheprevalentmeasurementbutthereference
point,wherethelinemeetsthepatient,hasnotbeen
stan-dardised.
Someresearch50,51didnotgiveanyreferencepoint.
Oth-ersreportedmeasuringfromthetargettodifferentpoints
suchas7mmbehindtheanteriorcornealpole,4213or14mm
infrontoftheeye,52theeye,53---55thespectacleplane,16,17,25
thetrialframe,28‘‘thecornealplane’’,11theanteriorpole
of thecornea,56,57 theforehead39 andthe chin.58 Noneof
thesereports gave a reasonfor their choice of reference
point.Thesepositions,someofwhich(suchas‘‘theeye’’)
areimprecise,coveralargeenoughrangetoinfluencethe
resultsignificantlyat moderatelevelsofAoAand
substan-tiallymoreathigherlevels.
Definitionoftheend-point
Definition of the end-point is inherently imprecise in the
retinoscopy,push-upandpush-downmethodsofmeasuring
AoA.
The distance of the retinoscope sighthole from the
patient’seye,typicallythedistancetothespectacleplane,
is known as the Retinoscopy Working Distance (RWD).
Measurement of accommodation by retinoscopy has
gen-erally involved a shorter (often much shorter) RWD than
is usual for determination of distance refractive error
by retinoscopy. In reports of measurement of AoA by
retinoscopy13,17,28---31,51,58---60 the RWD is the outcome
mea-sure.Thiswouldleadtoimprecision,forreasonsincluding
thefollowing:
- the participantis likely to move, altering the distance
fromparticipanttoretinoscope.
- theexaminerislikelytomove,independentlyofthe
par-ticipant.
- theexaminer ispositionedneartotheparticipant,
per-hapsasnearas10cmorless,thereforeanyerror,suchas
due tomovement or parallax,would bea large
propor-tionofthemeasurement.Inonestudy28 negativelenses
wereaddedtothepatient’sspectacleplanetoincrease
theRWD,perhapstoreducethaterrorbuttheresultsdid
notshowmoreprecisionthanthoseofotherinvestigations
usingretinoscopy.
- theaccuracyofretinoscopydecreasesunpredictablywhen
measuring away from the visual axis32 and this error
increaseswithnearnessof afixed-size targetdisplacing
theretinoscopebeam.
- themeasurementis takensometimeafterreachingthe
end-point.
- themeasurementmayincludeerrorsduetoparallaxsince
therulermayhavetobeheldawayfrompointstowhich
itmeasured.Thiswaswellillustratedphotographicallyin
theresearchreportsthatshowedthisdetail.51,58
- the precision of retinoscopy is proportional to the
RWD.61,62
- the measurement end-point may involve the subjective
judgement ofretinoscopic reflexes thatareparticularly
unusualduetochangesinocularaberrationwith
accom-modationdescribed inother research.63 Thiscouldbea
reason why research51 found substantial inter-examiner
variation, over 20%, in measuring AoA by retinoscopy.
However, excellent reproducibility was found for this
technique in a later and larger study17 in which ten
examiners measured fourteen participants’ AoA using
additionaltrial lensestokeep theRWDbetween14and
67cm.They found that 95% of the measurementswere
within7%ofeachother.
Methodsof measuringAoAthat requirethe participant
tostatewhenatargetisclearor blurredhavealsolacked
apreciseend-point.Someauthors18,28,54,64,65havereported
onyoungparticipantswithwhomthatsubjectiveend-point
wouldbeevenlessreliable, includingone65 whoreported
measuringAoAsubjectivelyinchildrenundertwoyearsof
age.
In the minus-lens method, the end-point depends on
howfinethefocusmustbetodiscernthetarget.Different
researchersusingtheminus-lensmethodhaveuseddifferent
targetsizes,corresponding,forexample,to:
6/624,66
6/6−41
6/925,31
6/9−57
6/12+21
and6/15.17
Someofthesewouldbelikelytointroduceimprecisionof
morethan1Dduetodepthoffocusalone,giventhelarge
reduction(andtheconsequentincreaseindepthof focus)
shown26inpupildiameterathighaccommodationlevels.
Thereisalwayssomeerrorinpinpointingtheend-point
6 D.H.Burnsetal.
measuringlengthislargelyindependentofthelengthbeing
measured, such as in measuring AoA by measuringa
dis-tance.Therefore,end-pointerrorisahigherproportionof
the measurement when higherlevels of AoA (i.e. shorter
distances)aremeasured.
Fortunately, in clinical measurement of AoA, accuracy
at lower levels of AoA tends to be more important than
accuracyathigherlevels.Itcanbeargued thatanAoAof
about4D (morefor hypermetropesreluctanttowear
dis-tancerefractivecorrection)wouldcoveralmosteveryone’s
practicalneeds.
On the other hand, accuracy in higher values may be
useful in identifying change that may be of
pathologi-calsignificance, suchasinteroculardifferenceor outliers
attributabletoapathologicalprocess.Researchhasnotyet
identifiedalevelofaccuracythatmightachievethesegoals.
Monocularorbinocular
Whennotaddressing interoculardifference,measurement
of AoA would generally be binocular, since in everyday
lifeaccommodationisnormallystimulatedunderbinocular
conditions.However,binocularmeasurementisnotalways
possible because of restrictions due to the measurement
methodasshown,forexample,withtheminuslensmethod,
asdescribedpreviously.Thisraisesthepossibilityoferror.
Measurements of one eye or of both together, under
monocularorbinocularstimulation,maydifferbyunknown
amounts,because:
- binocular visualacuityishigherthan monocular67 which
mayaffect thespeed andprecisionof detectionofblur
(or itsabsence)particularlyinmethodsofmeasurement
ofAoAthatareaffectedbyreactiontime.
- convergence induces accommodation and vice versa.
Binocularity requires a fixed degree of convergence for
the object distance. Therefore, the amount of
accom-modation may be influencedby whether the viewing is
monocularorbinocular.
- changesinpupilsize,duetoconvergence,influencedepth
offocus.52
- morenaturalbinocularviewingconditionsmayallow
opti-malexpressionofaccommodation,asfoundinonestudy.68
Thismaybebecausemonocularviewingcangive
anoma-lousdistancecueswhichmaycausetheparticipanttofeel
somewhat disconnected from the task, and would
pre-vent any stereoscopic sense of nearness of the target.
This sense of nearness influences accommodation.83---85
One study52 found that binocular viewing gave higher
results than monocular viewing. However, that
investi-gationtook placea centuryago andthe resultwasnot
supported by any work published sincethen. Moreover,
anotherinvestigation45 didnotshowhigherresultswhen
AoAwasmeasuredbinocularlythanwhenitwasmeasured
monocularly.
- if the AoA of one eye differs from itsfellow, binocular
measurementismostlikelytogivethehigherofthetwo
eyes’amplitudes.
Researchers’ approach to binocularity has varied.
Some54,69 stimulated and measured binocularly, or took
both monocular andbinocular measurements16 or did not
state whether the measurementsweremade monocularly
orbinocularly.70Thosewhousedtheminus-lensmethod24,51
(which,asexplainedabove,cannotgivebinocularresults)
measured monocularly only. In at least one study50 one
eye was covered. Others measured monocularly as they
refractedbyobjectivemeans12,51perhapsastherewerefew
reports ofan objectivemethod thatgaveresults forboth
eyessimultaneously.
Correctionofrefractiveerror
Correction of refractive error before measuring AoA is
importantbecausethemeansphericalrefractivecorrection
mustbeaddedtothemeasurement(andreferencedtothe
samepointasit).Furthermore,latenthypermetropiacould
causesubstantialandvaryingerrors,Moreover,ifspectacles
areworn,theaccommodativestimulusisinfluencedbythe
typeandpoweroftheprescription.71
ThetypeofrefractiveerrormayalsoinfluenceAoAbut
investigationshavenotshowntheinfluence tobelargeor
predictable.Astudy72setouttoreporttheextenttowhich
AoA and refractiveerror were correlated.This study’s 80
participantswereaged18---22yearsandameanofpush-up
andpush-downmeasurementswastaken.The results
indi-catedthatthesignandamountofrefractiveerrorandthe
mannerofonsetofmyopiainfluencedAoA.Theassociation
wasweak but supported by measurements ofpupil
diam-eter since hyperopic participants tended to have smaller
pupils,and hence greater depthof focus,yet lower AoA.
AsimilareffectofrefractiveerroronAoAwasfound48with
thepush-upmethodmodifiedtoreduceerrorsasin
previ-ousworkdescribedabove11 forasimilarparticipantgroup.
Theseresultssuggestthatrefractiveerrorisavariablethat
shouldbecontrolledinAoAresearch.However,normative
studies of AoA have generally not recorded participants’
refractiveerror.
The approachto correctingrefractiveerror hasvaried
between studies and sometimes within individual studies
of AoA.In onestudy,cycloplegiceyedrops wereused52 to
attempttoeliminateaccommodationforthemeasurement
ofrefractiveerror,includinglatenthypermetropia,except
forsomeparticipantsoverage46years,whereasinanother
study16 cycloplegic eyedrops were instilled only for some
participantsyoungerthan20.Neitherstudyexplainedwhy
theyadministeredadrugorgaveanybasisforitsselective
allocation. Itsuse could be supported by anotherstudy72
thatimplicitlyrelatedlatenthypermetropiatoAoA.
IntheearlieststudiesofAoA42,53correctionofrefractive
error was not clearly described. It wasnot mentioned in
somelaterresearch50,54,70anditsmethodofcorrectionwas
moreapproximate thannormal methodsin amore recent
study.73
Taskluminance
Methodsof measuringAoA that requirethe patient’s
per-ceptionofavisualtargetdonotstipulatethatthelighting
of the visual task should be set to a particular level.
However, target perception is influenced by the
Figure2 TwoRAFRules,showingpositionofscalediffers.
described.74 The influenceof taskluminanceonAoA
mea-surementresults,independentoftheeye’sdepthoffocus,
hasbeendemonstrated75andithasalsobeenshown76,77that
taskluminanceinfluencesdepthoffocuswhich,asdiscussed
previously,alsoinfluencesAoAmeasurementresults.
Instrument
error
TheRAFRuleistheprevalentinstrumentusedformeasuring
AoAintheUK.Althoughitisasimpledevice,thereappear
tobefifteensourcesoferror,listedbelow,initsdesignand
production.
Other accommodation rules that have been produced
forclinical usearecurrentlyrarely usedintheUK,tothe
authors’ knowledge, andmay beexpected toshare some
oftheRAFRule’ssourcesoferror.Theyusethesame
gen-eral principle of measurement by locating the near-point
andmeasuringhowfaritisfromtheeye.Practitionersmay
improviseanaccommodationrulebyusingarulerand
hand-heldvisualobject.
EachofthesefifteensourcesoferrorintheRAFRulehas
thepotentialtocauseclinicallysignificanterror.The
resul-ting errors can allbe additive. Theiroverall effect could
beaddressed by revising the design although thishas not
enjoyed a clinically-guided change during its
production-span of over sixtyyears. The fifteen sources of error are
asfollows:
1. ambiguity about which part ofthe sliding component
indicatesthereading;
2. ambiguityregardingwhichscale-graduation(orneither)
thescale’snumbersdescribe,becauseeachnumberis
equidistantbetweentwograduationsandindicates
nei-ther;
3. uncertaintyaboutthelocationofthescale’szeropoint,
asRAFRulesappeartovaryinthedistanceofany
par-ticularscalegraduationfromthecheekrest,asshown
inFig.2whichdepictsthefirsttwoRAFRulessourced
randomlybyoneoftheauthors;
4. the slider’s opaqueness, obscuring interpolation
betweengraduations;
5. theeffectonthelocationofthescalearisingfrom
inter-individual differencesin facial anatomy,at anygiven
distance,d,ofthecheekrestbelowthecornealvertex;
6. the effectof notspecifyingd, mentionedin point(5)
above, asfacial anatomy is not perpendicular tothe
RAFRule;
7. theeffectofnotspecifyingd,asfacialanatomyvaries
betweenpeople;
8. theeffectofnotspecifyingthedistancedonpoint(14)
below;
9. the variabilityofluminance contrastofthe text.The
contrastcouldbestandardisedbybacklightingthetext;
10. the limitsof thescale. ValuesofAoA higherthanthe
measurementrangeoftheunmodifiedinstrumenthave
oftenbeenreported22,37,38,42,78;
11. thevariablelocationoffixationwithinonelineoftarget
print,sincedifferentlettersintheline,whichis27mm
long, areat differentdistances fromeither eye,
pro-ducingdifferingaccommodativedemandofupto0.25
Dwhenmeasuringapproximately6Dofaccommodation
withtheRAFRule.Highererrorsoccuratshortertarget
distances;
12. the effect of target detail size, through depth of
focus34;
13. theeffectofscale intervallinearity,throughreaction
timeaspreviouslydiscussed;
14. thevariabilityofraildeclination.ThisisshowninFig.3,
twopicturestakenoftheinstrumentinroutineclinical
use,showinghowtherulemaybeheldaboveorbelow
theprimarypositionofgaze.
The declinationinfluences theresult,for thefollowing
reason.Thereisaquadrilateralformedbythecornealvertex
orotherreferencepointofmeasurement,thetestobject,
the measurement index on the slider, and the midpoint
between the cheek rests. This quadrilateral is generally
irregular and its shapevaries with the measurement and
theRule’sposition.Theeffectofdeclinationcanbe
[image:8.612.145.444.54.245.2]8 D.H.Burnsetal.
Figure3 RAFRulesinnormaluse,showingvariationofdeclination.
theRuleshownintheupperphotographinFig.3wouldgive
ameasurementofAoAapproximately1Dlowerthanifthe
Ruleweretiltedasinthelowerphotograph.
There is no consensus onhow the RAF Rule shouldbe
held.Guidancevariesbetweenauthorities12,13,15sometimes
picturingtheinstrumenttiltedsubstantiallydowninuse.
Furthermore,therearereportsthatdeclinationofgaze
influences AoA.79,80 Moreover, if the rail is tilted too far
down,the normal narrowing of the palpebral aperture in
downgazemayreducepupilarea,increasingdepthoffocus.
Wherea phoropteris usedinAoAmeasurement,itsrailis
horizontal.
15. The other source of error inherent in the design of
this instrument applies to monocular measurements.
The error is that the rule is placed on the midline
betweenthetwoeyes,ratherthanonthevisualaxisof
theeyebeingmeasured.45Thiswouldinflateresultsby
an amountthatcanbetrigonometricallyestimatedas
about5%atthehighestlevelsofAoAandapproximately
proportionatelylessatlowerlevels,soitisnotaslarge
assome other errorslisted above.Correctionfor this
source of error has been precise,45,72 approximate16
or missing42,78 withthelatterstudiesreportinghigher
uppermeasurementsofAoAthanotherstudies.
Intheabovelistofsourcesoferrorarisingfromapparent
weaknessesin thedesignandproduction oftheRAFRule,
publishedinformationwasnotfoundforitems1---13.
Measurement withthe minus-lens method minifies the
target because it is viewed through negatively-powered
lenses.Thenegativepower,andhencetheminification, is
greater athigherlevelsofmeasurement. Theminification
hasbeencited14,41asapossiblesourceoferror.No
theoret-icalorempiricalreportswerefoundofthesizeofthiserror
beingclinicallysignificant.
Whenviewingthroughspectaclelenses,AoAmaybe
influ-encedbyrefractiveerror,thedegreeofinfluencedepending
onthepowerofthelens.36Thismaybeanadditionalsource
oferrorwiththeminus-lensmethod.66
Examiner
bias
This is a source of error in any measurement that is not
fully automatic. The practitioner examining the patient
will often, and perhaps always, have an expectation of
approximatelywherethemeasurementend-pointshouldbe.
Thatexpectation,and inevitable differencesin technique
betweenpractitioners,mayinfluencehowthemeasurement
istaken(e.g.,thevisualobject’sspeed),whichmayinturn
influencetheresult.Itmayaffectnaivepatientsmore.
Research of accommodative response81 and fixation
disparity82 has shown that the exact wording of
instruc-tionscaninfluencetheresultsofmeasurement.Significant
differences between five different examiners’ results for
push-up measurement of AoA were found and attributed
to possible differencesbetween examiners’ measurement
techniques.38
Examinerbiasmay besuspected particularlywhen the
generallevelofmethodologicalrigourappearslowandthe
resultsarenotcorroboratedelsewhere.Anormativestudy
[image:9.612.125.452.55.351.2]discussedtheconclusionthatAoAwasinfluencedbyrace70
and another found a 5 D difference between amplitudes
ofaccommodationofurbanandruralchildrenagedfiveto
eight,usingamethoddescribedonlybrieflyandinunspecific
terms.54
Anomalous
distance
cues
Awareness of a visual object’s distance influences
accommodation.83---85 In comparing methods of
measur-ing AoA, the test object is further away in the minus
lens method and measurement conditions aremonocular,
reducingawarenessofproximity.Othermethodsgivehigher
results, todifferingextents.28,41,46,59 The lowest valuesof
all investigations of AoA were obtained using the
minus-lens method with objective measurement (simultaneous
autorefraction).56
Results for AoA with the minus-lens method were
sig-nificantly higherwhen using a shorter viewingdistance.66
Measurement was monocular so the difference was not
attributable to the induction of extra accommodation by
extra convergence. The authors attributed the effect to
proximalaccommodation.
With particularly careful methodology it was found
thataccommodation measured witheitherthepush-up or
the push-down methods washigher when the participant
grasped and guided the target than when the target was
heldandguidedbytheexaminer.45Noreasonforthis
find-inghasbeen demonstratedbut itcouldhave been dueto
variouspsychologicalfactorsincludingincreasedawareness
ofproximitywhentheparticipantconnectedwith,and
con-trolled, thetarget. Accommodationrules suchasthe RAF
Rule maytherefore givehigher measurementsbecauseof
reasonsincludingtheirphysicalcontactwiththepatient.
Feedback
from
achievement
Methods of measurement that reward patients striving to
improvetheirperformancebyfeedingbackhowwellthey
areachievingdiscernment ofdetail,encouragingeffortto
achieve the best visual performance, tend togive higher
results for AoA and other aspects of accommodation.86,87
Encouragementofeffortisadvisedforeventhemostbasic
subjectiveassessmentofvisualperformance.88
The reward for effort differs in different methods.
Obtainingnearness,thegoalforthepatientusingthe
push-up method, probably offers little motivation to produce
higherresults,althoughthismaydependontheinstructions
given.Maximumaccommodativeeffortwouldbemorelikely
tomeetthechallengeofdiscoveringdetailencounteredin
methods suchaspush-downwiththe ‘‘justrecognisable’’
end-point,theminuslens method,andretinoscopywitha
suitable visual object such as a Snellenchart reduced to
about5%ofitsusualsize.
Conclusions
Manysourcesoferrorhavebeendescribedinexisting
meth-odsofmeasuringAoA.Itisnoteworthythatsomanysources
ofinaccuracycanbeidentifiedinasingle-parameter,
long-established,basicandubiquitousclinicalmeasurement.
The sourcesof errordifferconsiderablyintheir nature
andin themagnitudeof their effect.Some arerelatively
systematicwhile othersareofunpredictablesizeor
direc-tionorboth,someaffectlowerreadingsmorethanhigher
readingsandviceversa,someaffectonlycertainmethods
ofmeasurement,someaffectdifferentmethodsdifferently,
someareduetohumanfactorsofthepatientorofthe
prac-titioner,someareduetofactorsoftheequipment,orofthe
method,usedformeasurement.Theiroveralleffectgreatly
reducesthevalidityofclinicalresultswithcurrentmethods.
Themeasurementerrorscausedby thesemanysources
oferrorcanallbereduced(andafewofthemcanbe
erad-icated)bybetterattentiontomeasurementtechniqueand
bythestandardisationofequipmentandmethods.However,
such improvements to existing methods would generally
increasethecomplexity,durationanddifficultyofthe
mea-surement.
Presbyopia is normal for older people and cures for
it would find widespread application. Surgical cures for
presbyopia have long been sought. Compared to optical
management of presbyopia they are risky and can be
costly, but on review89---91 they showed limited success.
Theirvalidationwouldrequireaccurateandreliable
clini-calmeasurementofAoA.Inthefuture,itseemslikelythat
improvements in the measurement of the AoA may have
applicationsinolderpatientsaswellaspeople
convention-allydescribedaspre-presbyopes.
Guidance
for
clinicians
Theindividualpractitionercantakecertainstepstoreduce
AoA measurement-error in current clinical practice,
rel-atively effectively and easily. For example, visual object
detailshouldbeclosetothelimitofresolutionatthenear
point, andthe method usedshould be recorded withthe
measurement.
Whenmeasuringwithdevicesusingarulerwithasliding
visualobject,suchastheRAFRule:
- movementoftheslidershouldbeslow,perhaps
approxi-matelyonedioptrepersecond;
- during measurementthepatientshouldreceive positive
feedbackforeffort;
- theruleshouldbeheldintheprimarypositionofgaze;
- in push-down, the end-point criterion of sharp focus
shouldbeadopted;
- measurementshouldbetoaclear,precisereferencepoint
suchasthecornealvertex;
- anycorrection forrefractiveerrorshouldbereferenced
tothesamepoint;
- thepractitionershouldchecktheindividualrule’s
accu-racybymeasuringthenear-pointdistancewithaseparate
rule;
- the practitioner shouldconsider taking a first
measure-mentusingthepush-upmethodandthenmovingtheslider
away fromthepatient toobtain apush-down
measure-ment. TherecordedAoA wouldbetheaverage ofthese
10 D.H.Burnsetal.
When using the minus-lens method, the visual object
shouldbeasclosetotheeyebeingmeasuredasfeasible,and
minus-lenspowershouldbechangedslowly.Forretinoscopy,
thepractitionermayconsiderreducingerrorbyusinga
nor-malworkingdistancesuchas67cm,addingminuslensesin
thetrialframefortherefractedeye.Thispossiblemethod
doesnotappeartohavereceivedresearchattention.
Notwithstandingthesepossibleimprovementstoexisting
methods,anewAoA-measurementmethodhasbeensought
bythecurrent authors.It isintended tobeacceptable in
clinicalpracticeandtoprovidemorereliablemeasurement.
Theauthorshopetopublishadescriptionofthisnewmethod
andtoreportinitialresultsobtainedwithit.
References
1.General Optical Council (UK). Optometry Core Com-petencies (Stage 1); 2011. https://www.optical.org/ en/Education/core-competencies–core-curricula/index.cfm
[accessed16.01.19].
2.College of Optometrists (UK). The Routine Eye Exami-nation; 2016. http://guidance.college-optometrists.org/ guidance-contents/advanced-search/?searchterm=a42
[accessed16.01.19].
3.College of Optometrists (UK). Equipment List for the Routine Eye Examination; 2016.
http://guidance.college-optometrists.org/guidance-contents/ annexes/annex-1-equipment-list-for-the-routine-eye-examination/[accessed16.01.19].
4.Optometric Extension Program Foundation (USA). 21 Point ExaminationTranslation Guide,https://www.oepf.org/sites/ default/files/21PointExaminationQuickRefe.pdf [accessed 16.01.19].
5.World Council of Optometry. Curricular Support Elements for an Optometry Programme; 2017.
https://worldcouncilofoptometry.info/wp-content/uploads/ 2017/03/curricularsupportelementfinalweb2.pdf[accessed 16.01.19].
6.The European Council of Optometry and Optics. The European Diploma in Optometry Syllabus, Learning Outcomes and Clinical/Practical Competencies; 2017.
https://www.ecoo.info/wp-content/uploads/2016/10/2017 1020Syllabus-andAccreditationself-assessment.pdf
[accessed16.01.19].
7.BurnsD,EvansB,AllenP.Clinicalmeasurementofamplitude ofaccommodation:areview.OptomPract.2014;15:75---86.
8.Neely J. The RAF near-point rule. Br J Ophthalmol. 1956;40:636---637.
9.Somers W, FordC.Effect of relative distancemagnification onthemonocularamplitudeofaccommodation.AmJOptom PhysiolOpt.1983;60:920---924.
10.GossD.Clinicalaccommodationtesting.CurrOpin Ophthal-mol.1992;3:78---82.
11.Atchison D, Capper E, McCabe K. Critical subjective mea-surement of amplitude of accommodation. Optom Vis Sci. 1994;71:699---706.
12.Keirl A. Accommodation presbyopia. In: Keirl A, Christie C, eds. Clinical Optics and Refraction. London: Elsevier; 2007:132---152.
13.RabbettsR.Bennett&Rabbetts’ClinicalVisualOptics.4thed. OxfordUK:Butterworth-Heinmann;2007:128---131.
14.Rosenfield M. Clinical assessment of accommodation. In: Rosenfield M,LoganN,eds. Optometry:Science,Techniques and Clinical Management. 2nd ed. Edinburgh,UK: Elsevier; 2009:230---232.
15.Barrett B. Assessment of binocular vision and accommoda-tion. In: Elliott D, ed. Clinical Procedures in Primary Eye Care. 4thed.Oxford,UK: Butterworth-HeinemannElsevier; 2013:178---181.
16.TurnerM.Observationsonthenormalsubjectiveamplitudeof accommodation.BrJPhysiolOpt.1958;15:70---100.
17.LeonA, Estrada J,Rosenfield M.Ageand theamplitude of accommodation measured using dynamic retinoscopy. Oph-thalmicPhysiolOpt.2016;36:5---12.
18.BenzoniJ,RosenfieldM.Clinicalamplitudeofaccommodation inchildrenbetween5and10yearsofage.JOptomVisDev. 2012;43:109---114.
19.ScheimanM,WickB.ClinicalManagementofBinocularVision. 1sted.Philadelphia:Lippincott;1994:20.
20.Koslowe K, Glassman T, Tzanani-Levi C, Shneor E. Accom-modativeamplitudedetermination:pull-awayversuspush-up method.JOptomVisDev.2010;41:28---32.
21.Taub M, Shallo-Hoffman J. A comparison of three clinical testsof accommodative amplitudeto Hofstetter’s norms to guide diagnosis and treatment. JOptom Vis Dev. 2012;43: 180---190.
22.ChenA,O’LearyD.Validityandrepeatabilityofthemodified push-upmethodformeasuringtheamplitudeof accommoda-tion.ClinExpOptom.1998;81:63---70.
23.Momeni-MoghaddamH,McAlindenC,AzimiA,SobhaniM, Ski-adaresiE.Comparing accommodative function between the dominantandthenon-dominanteye.Graefe’sArchClinExp Ophthalmol.2014;252:509---514.
24.Sheard C. The determination of the near-point and of the amplitudeofaccommodation.In:OcularAccommodation. Mis-souri:AmericanOptometricAssociation;1920:22---43.
25.WoodruffM.Ocularaccommodationinchildrenaged3to11 years.CanJOptom.1987;49:141---145.
26.MargE,MorganM.Thepupillarynearreflex;therelationof pupillary diameterto accommodationand the various com-ponentsofconvergence.AmJOptomArchAmAcadOptom. 1949;26:183---198.
27.EvansB.Binocularvisionassessment.In:RosenfieldM,LoganN, eds.Optometry:Science,Techniques&ClinicalManagement. 2nded.Edinburgh:Butterworth-Heinemann;2009.
28.WoldR.Thespectacleamplitudeofaccommodationof chil-dren aged six to ten. Am J Optom Arch Am Acad Optom. 1967;44:642---664.
29.Woodhouse M, Meades J, Leat S. Reduced accommodation inchildrenwithDown syndrome.InvestOphthalmolVisSci. 1993;34:2382---2387.
30.Roche O, Roumes C, Parsa C. Techniques de mesure du pouvoir accommodatif chez le sujet phake et le sujet pseudo-phake,distinctionentreinsuffisancesaccommodatives mécaniques et neurologiques. J Fr d’Ophtalmol. 2007;30: 953---960.
31.LeonA,MedranoS, Rosenfield M.Acomparison ofthe reli-abilityofdynamicretinoscopyand subjectivemeasurements oftheamplitudeofaccommodation.OphthalmicPhysiolOpt. 2012;32:133---141.
32.TayE,MengherL,LinX,FergusonV.Theimpactofoffthevisual axisretinoscopyonobjectivecentralrefractivemeasurement inadultclinicalpractice:aprospective,randomizedclinical study.Eye.2011;25:888---892.
33.CharmanW.Forminganopticalimage:theopticalelementsof theeye.In:RosenfieldM,LoganN,EdwardsK,eds.Optometry: Science,TechniquesandClinicalManagement.2nded.Oxford, UK:Elsevier;2009:11.
34.BurnsD,EvansB,AllenP.Areviewofdepthoffocusin measure-mentoftheamplitudeofaccommodation.Vision.2018;2:37.
36.GwiazdaJ, ThornF,BauerJ, HeldR. Myopicchildrenshow insufficient response to blur. Invest Ophthalmol Vis Sci. 1993;34:690---694.
37.EvansB,DrasdoN,RichardsI.Investigationofbinocularand accommodativefunctionindyslexia.OphthalmicPhysiolOpt. 1994;14:5---19.
38.Adler P, Scally A, Barrett B. Test---retest reproducibility of accommodation measurements gathered in an unselected sample of UK primary school children. Br J Ophthal. 2013;97:592---597.
39.CastagnoV,VilelaM,MeucciR,etal.Amplitudeof accommo-dationinschoolchildren.CurrEyeRes.2016;18:1---7.
40.Woehrle M, Peters R, Frantz K. Accommodative amplitude determination:canwesubstitutethepull-awayforthepush-up method?JOptomVisDev.2017;28:246---249.
41.AntonaB,BarraF,BarrioA,GonzalesE,SanchezI.Repeatability intraexaminer and agreement in amplitude of accommo-dation measurements. Graefe’s Arch Clin Exp Ophthalmol. 2009;247:121---127.
42.Donders F. On the Anomalies of the Accommodation and RefractionoftheEye.(W.MooreTrans.).UK:TheNew Syden-hamSociety;1864:207---209.
43.Ovenseri-OgbomoG,OduntanO.Comparisonofmeasuredwith calculatedamplitudeofaccommodationinNigerianchildren agedsixto16years.ClinExpOptom.2017;101:571---577.
44.CufflinM,MankowskaA,MallenE.Effectofbluradaptationon blursensitivityanddiscriminationinemmetropesandmyopes.
InvestOphthalmolVisSci.2007;48:2932---2939.
45.Fitch R. Procedural effects on the manifest human ampli-tudeofaccommodation.AmJOptomArchAmAcadOptom. 1971;48:918---926.
46.RosenfieldM,CohenA.Repeatabilityofclinicalmeasurements oftheamplitudeofaccommodation.OphthalmicPhysiolOpt. 1996;16:247---249.
47.RosenfieldM,CohenA.Push-upamplitudeofaccommodation andtargetsize.OphthalmicPhysiolOpt.1995;15:231---232.
48.AllenP,O’LearyD.Accommodationfunctions:co-dependency andrelationtorefractiveerror.VisRes.2006;46:491---505.
49.Sergienko N, Nikonenko D. Measurement of amplitude of accommodation in young persons. Clin Exp Optom. 2015;98:359---361.
50.AyrshireStudyCircle.Aninvestigationintoaccommodation.Br JPhysiolOpt.1964;21:31---35.
51.Rutstein R, Fuhr P, Swiatocha J. Comparing the amplitude ofaccommodation determinedobjectively and subjectively.
OptomVisSci.1993;70:496---500.
52.DuaneA.Studiesinmonocularandbinocularaccommodation with their clinical applications. Trans Am Ophthalmol Soc. 1922;20:132---157.
53.Kaufmann J. Die absolut und relativ accommodationsbre-iteindenverscheidenenlebensaltern.(Inauguraldissertation, GeorgAugustUniversitat,Göttingen);1894.
54.EamesT. Accommodationin schoolchildren, aged five,six, seven,andeightyears.AmJOphthalmol.1961;51:1255---1257.
55.MossS, KleinR,KleinB.Accommodative abilityin younger-onsetdiabetes.ArchOphthalmol.1987;105:508---512.
56.Anderson H, Hentz G, Glasser A, Steubing K, Manny R. Minus-lens---stimulatedaccommodativeamplitudedecreases sigmoidallywithage:astudyofobjectivelymeasured accom-modativeamplitudesfrom age3.InvestOphthalmolVisSci. 2008;49:2919---2926.
57.AndersonH,StuebingK. Subjectiveversusobjective accom-modativeamplitude:preschooltopresbyopia.OptomVisSci. 2014;91:1290---1301.
58.McLelland J, Saunders K. The repeatability and validity of dynamicretinoscopyinassessingtheaccommodativeresponse.
OphthalmicPhysiolOpt.2003;23:243---250.
59.HokodaS,CiuffredaK.Measurementofaccommodative ampli-tudeinamblyopia.OphthalmicPhysiolOpt.1982;2:205---212.
60.JimenezR,GonzalezM,PerezM,GarciaJ.Evolutionof accom-modativefunctionanddevelopmentofocularmovementsin children.OphthalmicPhysiolOpt.2003;23:97---107.
61.CorboyJ,NorathJ,ReffnerR,StoneR.TheRetinoscopyBook: AnIntroductory Manualfor EyeCareProfessionals. 5thed. Thorofare,NJ,USA:Slack;2003:31.
62.Atchison D.Objectiverefraction.In:Rosenfield M,LoganN, EdwardsK,eds.Optometry:Science,TechniquesandClinical Management.2nded.Oxford,UK:Elsevier;2009:190.
63.AldabaM,VilasecaM,ArjonaM,PujolJ.Age-relatedchanges inaccommodationmeasuredwithadouble-passsystem. Oph-thalmicPhysiolOpt.2013;33:1---8.
64.SternerB,GellerstedtM,AndersS.Theamplitudeof accom-modationin6---10-year-oldchildren---notasgoodasexpected!
OphthalmicPhysiolOpt.2004;24:246---251.
65.ChenA,O’LearyD,HowellE.Nearvisualfinctioninyoung chil-dren.PartII:Amplitudeofaccommodation.OphthalmicPhysiol Opt.2000;20:188---190.
66.Momeni-Moghaddam H, Wolffsohn J, Azimi A, Babaei-Malekkolaei E. Effect of targetdistance on accommodative amplitudemeasuredusingtheminus-lenstechnique.ClinExp Optom.2013;97:62---65.
67.Pointer J. Influence of selected variables on monocular, interocular, and binocular visual acuity. Optom Vis Sci. 2008;85:135---142.
68.Otake Y, Miyao M, IshiharaS, et al. Anexperimental study ontheobjectivemeasurementofaccommodativeamplitude underbinocularandnaturalviewingconditions.TohokuJExp Med.1993;170:93---102.
69.Kragha I. Amplitude of accommodation: population and methodological differences. Ophthalmic Physiol Opt. 1986;6:75---80.
70.CoatesW.AmplitudesofaccommodationinSouthAfrica.BrJ PhysiolOpt.1955;12:76---81.
71.Rosenfield M.Accommodation.In: ZadnikK, ed.TheOcular Examination: Measurements and Findings. 1st ed. Philadel-phia,USA:WBSaunders;1997:97.
72.McBrien N, Millodot M. Amplitude of accommodation and refractiveerror.InvestOphthalmolVisSci.1986;7:1187---1190.
73.Ovenseri-OgbomoG,KudjawuE,KioF,AbuE.Investigationof amplitudeofaccommodationamongGhanaianschoolchildren.
ClinExpOptom.2012;95:187---191.
74.Westheimer G. Visual acuity. Annu Rev Psychol. 1965;16:359---380.
75.Johnson C. Effects of luminance and stimulus distance on accommodation and visual resolution. J Optic Soc Am. 1976;66:138---142.
76.CampbellF.Thedepthoffocusofthehumaneye.JPhysiol. 1966;125:29---30.
77.TuckerJ,CharmanW.Thedepthoffocusofthehumaneyefor Snellenletters.AmJOptomPhysiolOptics.1975;52:3---21.
78.SternerB,GellerstedtM,SjöströmA.Accommodationandthe relationshiptosubjectivesymptomswithnearworkforyoung schoolchildren.OphthalmicPhysiolOpt.2006;26:148---155.
79.RippleP.Variationofaccommodationinverticaldirectionsof gaze.AmJOphthalmol.1952;35:4---1630.
80.AtchisonD,ClaydonC,IrwinS.Amplitudeofaccommodation for different head positions and different directions ofeye gaze.OptomVisSci.1994;71:339---346.
81.StarkL,AtchisonD.Subjectinstructionsandmethodsoftarget presentationinaccommodationresearch.InvestOphthalmol VisSci.1994;35:528---537.
82.Karania R, Evans B. The Mallett Fixation Disparity Test: influenceof testinstructions& relationship withsymptoms.
12 D.H.Burnsetal.
83.Heath G. The influence of visual acuity on accommodative responses of the eye. Am J Optom Arch Am Acad Optom. 1956;33:513---524.
84.Rosenfield M, Gilmartin B. Effect of target proximity on the open-loop accommodative response. Optom Vis Sci. 1990;67:74---79.
85.HungG, Ciuffreda J,Rosenfield M.Proximal contributionto alinearstaticmodelofaccommodationand vergence. Oph-thalmicPhysiolOpt.1996;16:31---41.
86.Winn B, GilmartinB,Mortimer L, EdwardsN. Theeffectof mentaleffortonopen-andclosed-loopaccommodation. Oph-thalmicPhysiolOpt.1991;11:335---339.
87.Gray L, Winn B, Gilmartin B, Eadie A. Objective concur-rent measures of open-loop accommodation and vergence
under photopic conditions. Invest Ophthalmol Vis Sci. 1993;34:2996---3003.
88.ElliottD,FlanaganJ.Assessmentofvisualfunction.In:Elliott D,ed.ClinicalProceduresinPrimaryEyeCare.4thed.Oxford, UK:Butterworth-HeinemannElsevier;2013:35.
89.Bowling B. Kanski’s Clinical Ophthalmology. 8th ed. Cam-bridge,UK:Elsevier;2016:246.
90.Pallikaris I, Kontadikis G, Portaliou D. Real and pseudoac-commodationinaccommodativelenses.JOphthalmol.2011,
http://dx.doi.org/10.1155/2011/284961.