Measuring
movement
fluency
during
the
sit-to-walk
task
A.
Kerr
a,*
,
V.P.
Pomeroy
b,
P.J.
Rowe
a,
P.
Dall
c,
D.
Rafferty
caDepartmentofBiomedicalEngineering,UniversityofStrathclyde,106Rottenrow,GlasgowG40NW,UnitedKingdom bFacultyofMedicineandHealthSciences,UniversityofEastAnglia,Queen’sBuilding,NorwichNR47TJ,UnitedKingdom c
SchoolofHealthandLifeSciences,GlasgowCaledonianUniversity,CowcaddensRoad,GlasgowG40BA,UnitedKingdom
1. Introduction
Visualobservationofmovementfluencyisusedbytherapists toguidetheplanningandevaluationofinterventionsaimedat restoring movement [27]. Improving movement fluency is perceivedbytherapiststobeassociatedwithimprovementsin function[6],andhasbeenshowntorelatetoenergycost[33].Itis akeyobjectiveofthepredominantapproachto neurorehabilita-tion in the United Kingdom [23,31]. There is an underlying assumption,however,thattherapistshaveatacitandcommon understandingof whatconstitutesfluent movement[28].This assumption,rarelytested,couldunderminetherigourofclinical assessmentandcreateanobstacle tothescientificscrutinyof physicalrehabilitation.
Toolsformeasuringmovementfluencyhavebeendeveloped previously using normal movement as a reference for trained observers[2].Insomecasesthesescaleshavedemonstratedgood
prognosticanddiagnosticproperties[26].Howevertheir subjec-tive nature causes reliability problems [21], and they rely on substantial experience and training of observers [20]. To avoid these hindrances Malouin et al. [19] introduced an objective method for quantifying fluency based on a threshold drop in forward momentum while performing the sit-to-walk (STW) movement.Theresultingdichotomous(fluentornotfluent)index wassubsequentlyadaptedintoaclinicalscalebyDionetal.[8]. Thisobjectivemethodofjudgingmovementfluencyfromachange inforwardmomentumispromising;withevidenceofvalidityasa screening tool for mobility problems, e.g. identifying a risk of falling(sensitivity0.96andspecificity0.89)[15].However,asa measurewithasingledimension,itlackscontentvalidity.
Toimprovepatientassessmentandprovidearesearchtoolfor thestudyofmovementdisorders andtheirrehabilitation,valid, objective measurementsof movementfluency areneeded[20]. Themultifariousnatureofmovementfluency,and lackofclear definition,maycontributetothepaucityofobjectivemeasures.A wayforwardistodeconstructfluencyintoseparatevariablesthat canbeclearlydefined,areclinicallyuseful,and,critically,canbe measured.
ARTICLE INFO
Articlehistory:
Received9December2011
Receivedinrevisedform19September2012 Accepted30September2012
Keywords: Fluency Smoothness Co-ordination Sit-to-walk
ABSTRACT
Background: Restoringmovementfluencyisakeyfocusforphysicalrehabilitation;it’smeasurement, however,lacksobjectivity.Thepurposeofthisstudywastofindwhethermeasurablemovementfluency variablesdifferedbetweengroupsofadultswithdifferentmovementabilitieswhilstperformingthe sit-to-walk(STW)movement. Themovementfluencyvariables were:(1)hesitationduringmovement (reductioninforwardvelocityofthecentreofmass;CoM),(2)coordination(percentageoftemporal overlapofjointrotations)and(3)smoothness(numberofinflectionsintheCoMjerksignal).
Methods:Kinematicdatapreviouslycollectedforanotherstudywereextractedforthreegroups:older adults(n=18),olderadultsatriskoffalling(OARF,n=18),andyoungeradults(n=20).Eachsubject performedtheSTWmovementfreelywhileamotionanalysissystemtracked11bodysegments.The fluencyvariableswerederivedfromtheprocessedkinematicdataandtestedforgroupvariationusing analysisofvariance.
Findings:Allthreevariablesshowedstatisticallysignificantdifferencesamongthegroups.Hesitation (F=15.11,p<0.001)wasgreatestintheOARF47.5%(SD18.0),comparedtoolderadults30.3%(SD15.9) andyoungeradults20.8%(SD11.4).Co-ordination(F=44.88,p<0.001)waslowestfortheOARF(6.93%, SD10.99) comparedto boththeyoung (31.21%,SD 5.48) andold (26.24%,SD 5.84).Smoothness (F=35.96,p<0.001)wasbestintheyoungeradults,18.3(SD5.2)inflections,comparedtotheold,42.5 (SD11.5)andOARF,44.25(SD7.29).
Interpretation: Hesitation,co-ordinationandsmoothnessmaybevalidindicatorsofmovementfluency inadults,withimportantconsequencesforresearchandclinicalpractice.
ß2012ElsevierB.V.Allrightsreserved.
*Correspondingauthor.
E-mailaddress:[email protected](A.Kerr).
ContentslistsavailableatSciVerseScienceDirect
Gait
&
Posture
j our na l ho me pa g e : w ww . e l se v i e r . com / l oca t e / ga i t po st
Normal movementis characteristicallysmooth, co-ordinated andefficient[30]withoutunnecessaryhesitationorrepetition.A workingdefinitionoffluentmovement,therefore,shouldinclude measurabledefinitions oftheseterms:hesitation,co-ordination andsmoothness.
Movement hesitation is frequentlydescribedin neurological conditions [9,22] and musculoskeletal conditions [13] but less frequentlyquantified.Thefreezingofgaitquestionnaire[12]has beenusedinParkinson’sdiseasetoratefrequencyandmagnitude of movement hesitations with good reliability (Cronbach al-pha=0.94)andvalidity(correlationtoastandardfunctionscale during the ‘‘on’’ period was 0.66) but is a subjective, disease specific,tool.UsingmotionanalysistechnologybothKerretal.[15]
andMalouinetal.[19]quantifiedmovementhesitationduringthe STWmovementasapercentagedropinforwardmovementofthe centreofmass,and thisisprobablytheonlyreportedobjective methodformeasuringhesitationduringmovement.
Co-ordination is consistently reported as a characteristic of normalfluentmovement,forupperandlowerlimbmovements, although the term tends to be applied generically, without referencetoameasurabledefinition[23].Metricsbasedaround therelative timingof jointmovements, mostnotably temporal overlapping,have been developed[16,17] as possibleobjective measuresof co-ordinationwithhigherpercentagesof temporal overlapindicatingamorefluentmovement.
[image:2.595.331.524.51.161.2] [image:2.595.330.523.607.720.2]Movementsmoothness,andassociatedtermssuchasquality and efficiency of movement are used by therapists to express impairedmotorcontrolaswellasaguidingprinciplefortherapy
[5,23,31]. The absence of a measurable definition, however,
hampersbothscientificscrutinyandpatientassessment. Defini-tionsbasedonjerk(thirdtimederivativeofposition)havebeen appliedtoupperlimbtherapeuticrobotswithmeanandvariation calculatedasmetricsofsmoothness[25].
Althoughthismethodcouldbeappliedtoanymovement,asyet ithasnotbeenappliedtowholebodymovementssuchaswalking orSTW.
The merging of two separate movements during the STW movement (sit-to-stand and gait initiation [18]) has been recognised as a suitable testing ground for movement fluency
[1,3,8,11,15].Sit-to-walkisafunctional,wholebodymovement.To
date,however,the only fluencymeasurement recorded for the STW movementhasbeenthe dropin CoM velocity,previously mentioned.
Theprimaryaimofthispaperwastopresentnovelanalytical toolstoexpressmovementfluencyinamannerthatissympathetic totherapyobjectivesandwhichmayuncovernewunderstanding ofhumanmovement.Thesecondaryaimwastodetermineifanyof thesetools could statistically distinguish groups of individuals withexpecteddifferencesinmovementfluencywhenperforming theSTWmovement.
2.Methods
2.1.Designandethics
Biomechanicaldatawereextractedfromtheelectronicrecordsofaprevious observationalstudyoftheSTWmovement[15],whichhadethicalapprovalfrom theUniversityandNHSethicscommittees.Allparticipantsgavewritteninformed consentfortheearlierstudy.
2.2.Participants
Threegroupswererecruited:(1)youngadults(n=20,age33.1years(SD,8), mass71.9kg(SD,11.6),height1.72m(SD, 0.1)),(2)olderadults(n=18,age 70.3years(SD,5.4),mass65.8kg(SD,25.8),height1.66m(SD,0.1))and(3)older adultsatriskoffalling(OARF)(n=18,age79.6years(SD,7.5),mass66.2kg(SD, 16.7), height 1.53m (SD 0.1)). Participants were recruited from the local community(oldandyoung groups)andafalls preventionprogramme(OARF group),respectively.
2.3.Procedure
Allmeasurementsweremadeinamovementlaboratory.Participantsworetight fittingshorts,t-shirtandtrainersandsatonastandardchair(0.44minheight, armlessbutwitha108reclinedbackrest).Reflectivemarkers(diameter0.02m, mass0.03kg)weremountedontotheskinand,wherenecessary,theclothing overlyinganatomicallandmarkssothat11segments(feet,lowerlegs,thighs,trunk, upperandlowerarms)couldbeconstructedusingarigidbodymodel[24].
2.4.Themovementtask
Eachparticipantstartedthetestinsitting,andwasrequestedtowalktoanother chairplacedsixmetresinfrontofthem.Participantsselectedtheirstartingposition andperformedthemovementintheirownpreferredmanner.Eachparticipant performed fiverepetitions of the movement with data from the first three successful (all marker trajectories captured) repetitions used for analysis. Participantsweregivenupto5mintorestbetweenrepetitions.
2.5.Equipment
2.5.1.Marker
MarkertrajectoriesweretrackedinthreedimensionsbysevenMotionCapture Units (Qualisys Medical AB, Gothenburg, Sweden). Data were recordedat a samplingrateof50Hzandthesystemcalibratedtocollectavolumeof4m(saggital plane–Xaxis–directionoftravel)by1.8m(Zaxis–height)by1.5m(Yaxis– coronalplane)metresusingQualysisTrackManager.
2.6.Dataanalysis
Markertrajectorieswerefilteredusingalow-pass4thorderButterworthfilter withcut-offfrequencyof6Hz,andinterpolatedwithamaximumgapfillof10 framesusinganon-uniformrationalB-spline[10].Theresultingdatawereusedto constructa modelofthebodyusingVisual3D(Version3.28,C-Motion,Inc., Rockville,MD,USA)allowingcalculationofjointanglesandtotalbodycentreof mass(CoM)inthreedimensions.
Theonsettime(firstcontinuousforwardmovementoftheCoM)andendtime (endofthefirst swingphase,i.e.firstinitialcontact)wererecordedforeach movementtoallownormalisationofthedatato100%ofthemovement.Thethree fluencyvariables:hesitation,co-ordinationandsmoothness,werethencalculated fromtheresultingprocesseddata.
HesitationwasdefinedasthemaximumdropinforwardvelocityoftheCOM fromtheinitialpeakgeneratedduringtheseatedphase,expressedasapercentage oftheinitialpeakvalue,seeFig.1.
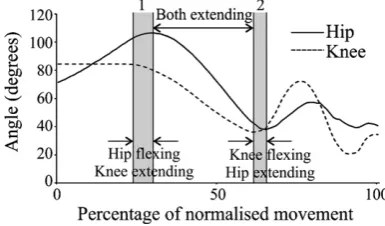
Co-ordinationwascalculatedasthetemporaloverlapbetweenthekneeandhip inthesaggitalplane(asapercentageofthewholemovementtime)duringtwo
Fig.1.Hesitation;definedasthepercentagedropinforwardvelocity.
periods(1)endofinitialhipflexionandstartofkneeextension(timeofknee extension timeofhipflexionending)and(2)endofhipextensionwhilerising andthestartofkneeflexion(timeofkneeflexion timeofhipextensionending), seeFig.2.
SmoothnesswascalculatedasthenumberofinflectionsintheCoMjerksignal, aninflection wasidentified bya logicstatement (MicrosoftExcel 2007)that determinedanegativechangeinthesignal(atimepointgreaterthantheprevious twotimepointsandgreaterthanthetwosubsequenttimepoints)orpositive change(atimepointlesstheprevioustwotimepointsandlessthanthetwo subsequenttimepoints)asillustratedinFig.3.
Eachofthefluencyvariableswascomparedamongthegroupsusingaonefactor ANOVA.Significanteffects(p<0.05)werethenexploredwithaTukeytest.All statisticalanalyseswereperformedinMinitab(version16).
3. Results
3.1. Hesitation
TherewasadropinCoMforwardvelocityinallgroupsbutwith significant differences in magnitude (F=15.11, p<0.001). The OARFgroupshowedthebiggestdrop(47.51%,SD18.00)followed bytheoldgroup(30.29%, SD15.86) and thentheyounggroup (20.82%,SD11.43),seeTable1.Posthocanalysisconfirmedthe statisticaldifferencelaybetweentheOARFandbothyoungandold groups.
3.2. Co-ordination
Allthreegroupshad negativevalues atbothoverlapperiods indicating:
(1)The knee begins to extend before the hip ends its flexion movement.
(2)Thekneestartstoflex(tostartthefirstswingphase)beforethe hipendstheextensionmovement.
The magnitude of the overlap, however, varied among the groupsduringthefirst(F=5.28,p=0.008)andsecond(F=44.88, p<0.001) periods. Post hoc analysis identified the OARF (1st overlap 1.47%, SD 9.89and2nd overlap 6.93%,SD 10.99) as beingdifferenttobothyoung(1stoverlap 13.16%,SD9.63and 2nd 31.21%,SD5.48)andtheoldgroup(1stoverlap 11.33,SD 13.02and2nd 26.24%5.84)groupsatthissecondoverlappoint,
seeTable1.
3.3. Smoothness
Smoothnessdifferedsignificantlyamongthegroups(F=35.96, p<.001), post hoc analysis identified the young group (18.25 inflections,SD5.20)asdifferenttoboththeold(42.50,SD11.45) andOARF(44.25,SD7.29),seeTable1.
4. Discussion
Thisstudyfoundsignificantdifferencesinmovementfluency amonggroupsofyoungeradults,olderadultsandOARF perform-ingtheSTWmovement.Asmeasuresoffluency; hesitation, co-ordinationandsmoothness,wereallfoundtovarystatistically.The ability of these measures to discriminate groups of people expectedtoexhibitdifferentcharacteristicsofmovementfluency raiseshypothesesaboutthebiomechanicsofmovementcontrol.
Quantifyinghesitationasareductioninthebody’svelocityfits themeaningoffluidity.Fluidmovement,afterall,iscontinuous movement;ambiguityhoweverexistsastowhatpointareduction invelocitymeansalossoffluidity.WhileDionetal.[8]selecteda reductionof30%ormoreinCoMforwardvelocitytoindicatea non-fluid movement our data points to a value of 50%. The occurrence of hesitation in all three groups suggests it is an invariant part of the movement.During this period (transition between sitting and standing) the body changes direction of movement from predominantly forward to predominantly up-ward,primarilythroughhipandkneeextension.Itappearsthatthe young and old group were able to retain most of their initial forward momentum, suggesting greater mechanical efficiency, whereas the OARF reduced their forward momentum by 50%. Allowinghorizontalmomentumtoreducebysomuch,atthecost ofadditionalmuscleworktoregeneratetheforwardmomentum forgait,islikelytobeadeliberatestrategy.Afearoffalling,for example,couldexplaintheneedtominimisepotentially desta-bilising momenta once standing. On the other hand, reducing momentumcouldsimplyreflect agreater,agerelated,delay in switching from one muscle synergy to another, in this case
Fig.3.Smoothness;definedasthecountofinflectionsinthejerksignal,datafrom twodifferentparticipants.
Table1
Descriptiveandinferentialstatisticsforthethreefluencyvariables.
Fluencyvariable Young Old Oldatriskfalling Anova
Hesitationa
20.82(11.43) 30.29(15.86) 47.51(18.00)*
F=15.11,p<0.001 Co-ordination1b
13.16(9.63) 11.33(13.02) 1.47(9.89)*
F=5.28,p=0.008
Co-ordination2 31.21(5.48) 26.24(5.84) 6.93(10.99)*
F=44.88,p<0.001 Smoothnessc
18.25(5.21)*
42.50(11.45) 44.25(7.29) F=35.96,p<0.001
aHesitation:maximumpercentagedropinforwardvelocityofthecentreofmass(COM)fromtheinitialpeakgeneratedduringtheseatedphase. b
Co-ordination:temporaloverlap(percent)betweenkneeandhipmovementinthesaggitalplaneduringtwoperiods(1)endofinitialhipflexionandstartofknee extension,and(2)endofhipextensionandthestartofkneeflexion.
c
Smoothness:numberofinflections(changeindirectionover2percentagepoints)intheCoMjerksignal. *
[image:3.595.71.265.54.257.2] [image:3.595.40.565.646.699.2]between flexion and extension of the joints. These hypotheses shouldbeexploredinfutureresearch.
Interruptions,orhesitations,inmovementarecommonandare alreadyincludedinsomemobilitytestsduetotheirusefulnessin screeningformobilityproblems,for examplethestopswalking whentalkingtest[7].Ourquantificationofhesitationwithratio,as opposedtocategorical(e.g.didordidnotstopwalking),datamight resolvesomeofthesensitivityissueswiththesetests[14].
Whereas hesitation represents a total body performance measure, the co-ordination calculation examined movement fluidity on an elemental scale (joint movement). This may be more helpful to therapists directly involved in rehabilitation. ComparedtotheOARFgroup,thetwohealthygroups(youngand old)weresimilarintermsofthemeanandvariabilityoftheir co-ordinationsuggestingasimilarmovementstrategywasadopted
[11].Thefirstoverlapperiod(aroundseat-off)sawtheyoungand oldgroupsoverlappingtheirhipflexionandkneeextensionby13% and11%,respectively,ofthetotaltime.Continuedhipflexionwhile thekneestartstoextendsuggestsanabilitytomaintainforward momentumwhilethebodyrises.TheOARFgroup,however,hada verysmalloverlapduringthisperiod(<2%),sothathipflexion ended(reversingtoextension)aroundthesametimeastheknee began to extend. The lack of overlap may be for mechanical reasons;couplingtheextensionmovementsofthekneeandhipto maximisebodylift.
Thesecondperiodofoverlapshowedasimilarpatternbutwith greaterdifferencesfortheOARFgroup.Theyoungandoldgroups wereabletoinitiategait(startofkneeflexion)whilecontinuingto rise(hipextension),thisoverlapwas31%and26%,respectively, andclearlyshowsanabilitytomergetwomovementpatterns,i.e. hipextension(risingfromthechair)andkneeflexion(initiating gait).ThisoverlapwasmuchsmallerfortheOARFgroup,although kneeflexiondidoccurbeforehipextensionended,therewasonly a7%overlap.
The difference, in magnitude of co-ordination, between the OARFandbothhealthygroupssuggestsdifferentstrategieswere employed.Thetwohealthygroupsallowedextensionandflexion of the lower limbs to occur simultaneously, this has several advantages: it reduces the movement time, maintains existing momentum,andtakesadvantageofstoredelasticenergyin the connectivetissue[32].Thisstrategyislikelytobemoreefficient thanthatadoptedbytheOARFgroup.Thisgroupfavouredaless fluidapproachtothemovement,enhancingstabilityby minimis-inghorizontalmomentumwhilerisingandensuringthebodywas uprightandbalancedbeforewalking.
Ourcalculationofsmoothness,basedonjerkofthetotalbody CoM, clearly differentiated the young group from both older groups (old and OARF). Considering the previous similarity betweentheyoungandoldgroupforhesitationandco-ordination this difference was both surprising and intriguing. Smooth movement is not, necessarily, a characteristic of functional movement but it suggests a level of motor control has been attained, particularly when exhibited during a whole body movement that is inherently unstable, and requires distinct phasesofacceleration,asinthecaseofSTW[18].Thedifference in smoothness uncovered between the young and old may represent fine scale changes in motor control, caused by age relatedchangesintheneuromusculoskeletalsystem.Assuchour quantificationofmovementsmoothnessmaybevaluabletofuture researchers.
Calculationsofmovementsmoothnesshaveexistedinrobotic literatureforsometime,particularlyinstudiesinvestigatingthe use of therapeutic robots [4] where the smoothness of the movement(typicallyupperlimb)isusedasanoutcomemeasure. ThemethodusedinthispaperwasappliedtotheCoMmovement which is a derived value from the movement of all tracked
segmentsofthebody(11segments)andisthereforesensitiveto positionalchangeinanysegment,e.g. rapidarmmovement,to gainbalance,willcauseajerk.Calculatingthenumberofjerksin the movement was felt to be appropriate for a whole body movement,butitisalsosensitivetochangesthatmaynotactually be important to the movement itself, for example placing the handsinadifferentposition.
Thediscriminantvalidityofthesemeasurescouldbeusefulin clinicalpractice.Consideringtheprominenceofmovementfluency inrehabilitationliterature[16,21,23,29],bothdiagnosticallyand asaguidetotherapists,itsmeasurementhaspotentialvalue.The methods presented in this paper may not readily translate to clinicalpracticeduetotheinstrumentationanddataprocessing involved, however the strategic use of accelerometers and gyroscopes may provide a method of clinically applying these techniques.Intermsofeleganceofdata,thereisanargumentthat thesethreemeasuresofmovementfluencycouldbeassimilated intoonevalue,however,asthevariablesarealldirectlyrelatedto eachother,acompositevaluewouldrequirefurthertesting.
5. Conclusion
Thispaperoutlinedamethodformeasuringmovementfluency during the STW movement. Applying them to three groups of peoplewhowereexpectedtoexhibitdifferentlevelsofmovement control identified that all movement fluency variables had discriminant validity. The operational definitions and reference datacan providea frameworkfor further development ofboth laboratoryandclinicallybasedmeasurestomovementfluency.
Funding
Therewasnofundingassociatedwiththisstudyorwritingof thispaper.
Acknowledgements
Theauthorswouldliketoacknowledgetheinitialcontribution ofthelateDr.KateKerrandProfessorBrianDurward.Thetimefor Dr. Andrew Kerr was funded by the Efficacy and Mechanism Evaluation programme, funded by the MRC and NIHR, with contributionsfromtheCSOinScotland,NISCHRinWalesandthe HSCR&D,PublicHealthAgencyinNorthernIreland.
Conflictofintereststatement
Theauthorsdeclarethatthereisnoconflictofinterestinthe conductionofthisstudyorwritingofthispaper.
References
[1]AbergAC,FrykbergGE,HalvorsenK.Medio-lateralstabilityofsit-to-walk performanceinolderindividualswithandwithoutfearoffalling.Gaitand Posture2010;31(4):438–43.
[2]BoyceWF,GowlandC,RosenbaumPL,LaneM,PlewsN,GoldsmithC,etal. Measuringqualityofmovementincerebralpalsy:areviewofinstruments. PhysicalTherapy1991;71(11):813–9.
[3]BuckleyTA,PitsikoulisC,HassCJ.Dynamicposturalstabilityduring sit-to-walktransitionsinParkinsondiseasepatients.MovementDisordersOfficial JournalOfTheMovementDisorderSociety2008;23(9):1274–80.
[4]CelikO,MalleyMKO,BoakeC,LevinHS,YozbatiranN,ReistetterTA. Normal-izedmovementqualitymeasuresfortherapeuticrobotsstronglycorrelate withclinicalmotorimpairmentmeasures.IEEETransactionsonNeuraland RehabilitationSystemsEngineering2010;18(4):11.
[5]CirsteaMC,LevinMF.Compensatorystrategiesforreachinginstroke.Brain 2000;123(5):940–53.
[7]deHoonEW,AllumJH,CarpenterMG,SalisC,BloemBR,ConzelmannM,etal. Quantitativeassessmentofthestopswalkingwhiletalkingtestintheelderly. ArchivesOfPhysicalMedicineAndRehabilitation2003;84(6):838–42. [8]DionL,MalouinF,McFadyenBJ,RichardsCL.Assessingmobilityandlocomotor
coordinationafterstrokewiththerise-to-walktask.Neurorehabilitationand NeuralRepair2003;17:83–92.
[9]ElbleR.Gaitanddementia:movingbeyondthenotionofgaitapraxia.Journal ofNeuralTransmission2007;114(10):5.
[10]FerrisDP,GordonKE,SawickiGS,PeethambaranA.Animprovedpowered ankle–footorthosisusingproportionalmyoelectriccontrol.GaitandPosture 2006;23(4):425–8.
[11]FrykbergGE,AbergAC,HalvorsenK,BorgJ,HirschfeldH.Temporal coordina-tionofthesit-to-walktaskinsubjectswithstrokeandincontrols.ArchivesOf PhysicalMedicineAndRehabilitation2009;90(6):1009–17.
[12]GiladiN,ShabtaiH,SimonES,BiranS,TalJ,KorczynAD.Constructionof freezingofgaitquestionnaireforpatientswithParkinsonism.Parkinsonism andRelatedDisorders2000;6(3):165–70.
[13]HuangY-C,WeiS-H,Hsing-KuoWangH-K,LieuF-K.Ultrasonographicguided botulinumtoxintypeaforplantarfasciitis:anoutcome-basedinvestigationfor treatingpainandgaitchanges.JournalofRehabilitationMedicine2010;42:4. [14]HyndmanD,AshburnA.‘‘Stopswalkingwhentalking’’asapredictoroffallsin
peoplewithstrokelivinginthecommunity.JournalofNeurology Neurosur-geryandPsychiatry2004;75(7):994–7.
[15]KerrA,RaffertyD,KerrKM,DurwardB.Timingphasesofthesit-to-walk movement:validityofaclinicaltest.GaitandPosture2007;26(1):11–6. [16]KrasovskyT,LevinMF.Review:towardabetterunderstandingofcoordination
inhealthyandpoststrokegait.NeurorehabilitationandNeuralRepair2010; 24(3):11.
[17]KrebsHI,VolpeBT,FerraroM,FasoliS,PalazzoloJ,RohrerB,etal.Robot-aided neurorehabilitation:from evidence-based to science-based rehabilitation. TopicsinStrokeRehabilitation2002;8(4):16.
[18]MagnanA,McFadyenBJ,St-VincentG.Modificationofthesit-to-standtask withtheadditionofgaitinitiation’’.GaitandPosture1996;4(3):232–41. [19]MalouinF,McFadyenB,DionL,RichardsCL.Afluidityscaleforevaluatingthe
motorstrategyoftherise-to-walktaskafterstroke.ClinicalRehabilitation 2003;17(6):674–84.
[20]MorrisDM,UswatteG,CragoJE,CookEW,TaubE.ThereliabilityoftheWolf MotorFunctionTest forassessingupperextremityfunction afterstroke. ArchivesofPhysicalMedicineandRehabilitation2001;82:5.
[21]PomeroyVM,PramanikA,SykesL,RichardsJ,HillE.Agreementbetween physiotherapistsonqualityofmovementratedviavideotape.Clinical Reha-bilitation2003;17(3):264–72.
[22]RahmanS,GriffinHJ,QuinnNP,JahanshahiM.Thefactorsthatinduceor overcome freezingof gait in Parkinson’s disease.BehaviouralNeurology 2008;19(3):9.
[23]RaineS,MeadowsL,Lynch-ElleringtonM.Bobathconcept:theoryandclinical practiceinneurologicalrehabilitation.NewJersey:JohnWiley&Sons;2009. [24]RileyPO,SchenkmanML,MannRW,HodgeWA.Mechanicsofaconstrained
chair-rise.JournalofBiomechanics1991;24(1):77–85.
[25]RohrerB,FasoliS,KrebsHI,HughesR,VolpeB,FronteraWR,etal.Movement smoothnesschangesduringstrokerecovery.JournalofNeuroscience2002; 22:8297–304.
[26]SchmidhauserJ,CaflischJ,RoussonV,BucherHU,LatalB.Impairedmotor performanceandmovementqualityinvery-low-birthweightchildrenat6 yearsofage.DevelopmentalMedicineandChildNeurology2006;48(9):4. [27]SchneibergS, McKinley P,Gisel E, SveistrupH, LevinMF. Reliability of
kinematicmeasuresoffunctionalreachinginchildrenwithcerebralpalsy. DevelopmentalMedicineandChildNeurology2010;52:6.
[28]SelmanTJ,MorrisRK,ZamoraJ,KhanKS.Thequalityofreportingofprimary testaccuracystudiesinobstetricsandgynaecology:applicationoftheSTARD criteria.BMCWomensHealth2011;11:8.
[29]SkjaervenLH, KristoffersenK, GardG. Aneyefor movement quality: a phenomenologicalstudyofmovementqualityreflecting agroupof phy-siotherapists’understandingofthephenomenon.PhysiotherapyTheoryand Practice2008;24(1):13–27.
[30]ThelenE.Motordevelopment:anewsynthesis.AmericanPsychologist1995; 50(2):16.
[31]TysonSF,ConnellLA,BusseME,LennonS.WhatisBobath?AsurveyofUK strokephysiotherapists’perceptionsofthecontentoftheBobathconceptto treatposturalcontrolandmobilityproblemsafter stroke. Disabilityand Rehabilitation2009;31(6):9.
[32]ZamparoP,AntonuttoG,CapelliC,GirardisM,SepulcriL,diPramperoPE. Effects ofelasticrecoilonmaximal explosivepowerof thelowerlimbs. EuropeanJournalofAppliedPhysiologyandOccupationalPhysiology1997; 75(4):289–97.