COMPARISON OF COGNITIVE FUNCTIONS BETWEEN DIABETIC AND NON DIABETIC CHRONIC KIDNEY DISEASE PATIENTS ( STAGE 5D ) AND
ITS CORRELATION WITH SERUM URIC ACID, HEMOGLOBIN AND SERUM FERRITIN LEVELS.
Dissertation submitted to
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY, CHENNAI – 600032
In partial fulfillment of the requirement for the degree of Doctor of Medicine in Physiology ( Branch V )
M.D. ( PHYSIOLOGY ) APRIL 2017
DEPARTMENT OF PHYSIOLOGY COIMBATORE MEDICAL COLLEGE
CERTIFICATE
This dissertation entitled “ COMPARISON OF COGNITIVE FUNCTIONS BETWEEN DIABETIC AND NON DIABETIC CHRONIC KIDNEY DISEASE PATIENTS ( STAGE 5D ) AND ITS CORRELATION WITH SERUM URIC ACID, HEMOGLOBIN AND SERUM FERRITIN LEVELS” is submitted to The Tamil Nadu Dr.M.G.R Medical University, Chennai, in partial fulfillment of regulations for the award of M.D. Degree in Physiology in the examinations to be held during April 2016.
This dissertation is a record of fresh work done by the candidate Dr. K. ARCHANAA, during the course of the study ( 2014 – 2017 ). This work was carried out by the candidate herself under my supervision.
GUIDE:
Dr.D.SELVAM. M.D.,DCH, Associate Professor,
Department of Physiology, Coimbatore medical college. Coimbatore - 14
PROFESSOR & HOD: Dr.N.NEELAMBIKAI. M.D., Department of Physiology, Coimbatore Medical College, Coimbatore – 14.
DEAN:
Dr.A.EDWIN JOE. M.D.,B.L,
DECLARATION
I, Dr. K. ARCHANAA solemnly declare that the dissertation entitled “COMPARISON OF COGNITIVE FUNCTIONS BETWEEN
DIABETIC AND NON DIABETIC CHRONIC KIDNEY DISEASE
PATIENTS (STAGE 5D) AND ITS CORRELATION WITH SERUM
URIC ACID, HEMOGLOBIN AND SERUM FERRITIN LEVELS”
was done by me at Coimbatore Medical College, during the period from July 2015 to June 2016 under the guidance and supervision of Dr.N.Neelambikai. M.D., Professor, Department of Physiology, Coimbatore Medical College, Coimbatore.
This dissertation is submitted to The Tamilnadu Dr. M.G.R. Medical University towards the partial fulfillment of the requirement for the award of M.D. Degree (Branch - V) in Physiology. I have not submitted this dissertation on any previous occasion to any University for the award of any degree.
Place:
Date:
ACKNOWLEDGEMENT
I express my sincere thanks to our respected Dean, Dr.A.Edwin Joe, M.D.,B.L., Coimbatore Medical College, Coimbatore for
permitting me to conduct the study.
I thank Dr.R.Mani, M.D., Vice Principal, Coimbatore Medical College, Coimbatore for her encouragement and suggestions in completing the study.
I am extremely grateful to my beloved and respected Head of the Department of Physiology, Professor Dr. N.Neelambikai, M.D., for her encouragement in helping me to take up this study. I express my heart - felt gratitude to her, for her moral support and encouragement throughout the conduct of the study and also during my post graduate course. I owe my sincere thanks to her.
I will ever remain in gratitude to Dr.R.Shanmughavadivu, M.D., Professor, Department of Physiology for her valuable support and guidance for my study.
I am highly obliged to Dr.P.Murugesan, M.D., Professor, Department of Physiology, for his motivation to perform this work.
My sincere thanks to beloved teachers Dr.A.Moorthy M.D., Dr.S.Kavitha M.D., Dr.E.S.Manikandan M.D., Dr.S.Subhashini M.D.,
Dr.A.Abbass,M.D., Dr.S.Thenmozhi,M.D., Dr.C.N.Angel Deepa, M.D.,
Mrs.D.Revathy M.sc., Assistant Professors, Department of Physiology for their valuable opinion and help to complete this study. I would like to thank all my tutors for their support in completing this study.
I immensely thank Dr. A. Prabhakaran, M.D., DM., The Chief, Department of Nephrology , Coimbatore Medical College Hospital, Coimbatore for their cooperation and support in selecting my study samples.
I extend my heartful thanks to Assistant Professors, Staff Nurse, Dialysis Technicians in the department of Nephrology for their kind help for my study.
I would grossly fail in my duty, if I do not mention here of my subjects who have who gave full cooperation while doing my study.
My sincere thanks to all my fellow postgraduates for their involvement in helping me in this work.
Submission author: Assignment title: Submission title: File name: File size: Page count: Word count: Character count: Submission date: Submission ID:
Digital Receipt
This receipt acknowledges that Turnitin received your paper. Below you will f ind the receipt
inf ormation regarding your submission.
The f irst page of your submissions is displayed below.
201415251 M.d.physiology K.Archa… 2015-2015 plagiarism
Comparison Of Cognitive Function… 100.docx
536.41K 100 14,952 86,802
20-Sep-2016 12:38PM 707433731
Comparison Of Cognitive Functions Between Diabetic Chronic
Kidney Disease And Non Diabetic Chronic Kidney Disease Patients
(Stage 5D) And Its Correlation With Serum Uric Acid, Hemoglobin
And Serum Ferritin Levels
CONTENTS
S.NO CONTENTS PAGE NO
1. INTRODUCTION 01
2. AIMS AND OBJECTIVES 06
3. REVIEW OF LITERATURE 07
4. MATERIALS AND METHODS 41
5. RESULTS 51
6. DISCUSSION 85
7. SUMMARY 98
8. CONCLUSION 99
9. BIBILIOGRAPHY
ABBREVIATION
CKD Chronic Kidney Disease
NIMMHANS National Institute of Mental Health And Neurosciences
NCD Non Communicable Diseases
WHO–SEARO World Health Organisation – South East Asian Regional Office
ESRD End Stage Renal Disease
eGFR EstimatedGlomerular Filtration Rate
MCI Mild Cognitive Impairment
MCI-MCDT Mild Cognitive Impairment - Multiple Cognitive Deficit Type
sLRP Soluble Low density lipoprotein receptor related protein – 1
Apo E Apo lipoprotein E
CD Cluster Differentiation
PSEN Presenilin
NKF National Kidney Foundation
KDOQI Kidney Disease Outcome Quality Initiative
KDIGO Kidney Disease Improving Global Outcome
DN Diabetic Nephropathy
ACE Angiotensin Converting Enzyme
TGF β Tumor Growth Factor β
AGE Advanced Glycation End products
ADA American Diabetes Association LDL Low Density Lipoprotein
HDL High Density Lipoprotein
MMSE Mini Mental State Examination
ADMA Asymmetric Dimethyl Arginine
P – CS P – Cresyl Sulphate
TNF Tumor Necrosis Factor
Hb Hemoglobin
Epo Erythropoietin
HIF-1 Hypoxia Inducible Factor - 1 DMT-1 Divalent Metal transporter - 1
ID Iron Deficiency
IDA Iron Deficiency Anemia
1
INTRODUCTION
Cognition:
The term cognition refers to acquiring a new information, processing
it and storing it for future needs. It includes various domains of
brain functions namely attention, perception, reasoning, memory,
decision making and visuo spatial skills1.
Cognitive Deterioration:
It has become a major deteriorating health problem in old aged
people creating difficulties to carry out their daily activities and
making them totally dependent on other family members. In India
the rate at which cognition deteriorates is found to be nearly 300%
which is very much greater than high income nations where the rate
of cognitive deterioration is only 100%. Its prevalence in older
generations living in South India was estimated to be around 11.5 %2.
Recently diabetes, hypertension and chronic kidney disease ( CKD )
were found to be the independent risk factors for cognitive
deterioration due to more oxidative stress and altered function of
2
Consequences of cognitive deterioration:
Due to the defect in various cognitive domains, the affected
individuals lose their self-confidence, experience excessive problems
to carry out the routine activities, taking vital decisions in family
at correct times, interacting casually with other members of the
society, approaching doctors or health care facilities to get adequate
treatment for their health problems, all resulting in the isolation of
the individual and major compromise in the living quality and life
span2.
Questionnaire to measure Cognitive function:
Among various questionnaires available, National Institute of Mental
Health And Neurosciences ( NIMHANS ) manual of neuropsychology
battery 2004 is definitely better than other questionnaires because it
contains separate tests covering almost all domains of cognition
namely selective attention, divided attention, sustained attention,
digital vigilance, response inhibition, auditory verbal learning,
planning, visuo-spatial skills, immediate and delayed memory tests
for passage, complex figures and designs in free and fixed conditions
which is missing in other questionnaires. This battery can be used
Rising Trend of Non Communicable Diseases
0 5 10 15 20 25 30
cardiovascular Chronic
respiratory Disease
Cancer Diabetes Kidney and liver
diseases
M o r t a l i t y %
3
Rising trend of Non Communicable Diseases ( NCD ): In recent
years there is a change in the clinical scenario all over the world
with NCD in rising trend compared to the communicable diseases 4
due to the inactive style of living, poor eating habits favouring the
incidence of NCD and also the advancement in the discovery of
various vaccines and drugs keeps the communicable diseases under
control. In 2008, World Health Organisation – South East Asian
Regional Office (WHO – SEARO) estimated nearly 55 % of deaths
were due to NCD and among this one fourth represents premature
death ( < 60 years of age ). By 2030 it is expected that NCD s
contribute to three times more Disability Adjusted Life Years and
approximately 5 times more mortality in comparison with
communicable diseases4.
Inter link between various NCD ‘s:
Diabetes and hypertension have close association with other NCD
like CKD, cardiovascular and cerebrovascular diseases. CKD in turn
amplifies the metabolic disturbances and vascular complications
4 Global burden of CKD:
Even though CKD was not included in 2006 WHO health report,
now it is widely accepted that CKD is a rising health burden
affecting people all over the world. It is also realised that CKD
aggravates other adverse risk factors present in these individuals.
Worldwide prevalence of CKD is found to be 8 to 16%. In 2005
WHO estimated that all over the world, nearly 35 million people
died because of renal failure5.
Scenario regarding CKD in India:
CKD is becoming more prevalent in developing countries like India
because of increase in the number of persons getting affected by
diabetes and hypertension. India has the largest number of diabetics
in the world with a prevalence of 3.8% in rural and 11.8% in urban
individuals. The prevalence of hypertension is found to be 20-40 %
in urban adults and 12-17 % among rural persons. It is found that
25 – 40 % of these patients are likely to develop chronic renal
problems. Nearly 40 % of Type I diabetic patients and 5 to 15 %
of type II diabetic patients end up in End Stage Renal Disease
(ESRD). In India awareness related to renal failure is very poor,
that nearly 50 % of renal disease patients come to the hospital for
CKD and Cognitive Deterioration
Impaired
Cognition
Diabetes and Hypertension Chronic
Kidney disease Oxidative stress
and vascular events
5
stage, where glomerular filtration rate is less than 15 ml/
min/1.73m26. It is also found out that every year nearly 1 lakh
new cases of ESRD are becoming dependent on any one mode of
renal replacement therapy for their survival7 creating more economic
burden to the country.
CKD and Cognitive deterioration:
Nearly 80 % of CKD patients were affected with cognitive
deterioration and the impairment advances as the disease progresses
in its severity8.
In Chronic kidney disease various factors like diabetes, iron
deficiency anemia and retention of uremic toxins results in excessive
oxidative stress,3 poor mitrochondial function 9 and vascular
complications causing neuronal damage 10 and ultimately ends up in
6
AIM AND OBJECTIVES
AIM:
To assess and compare the cognitive functions between diabetic and non diabetic chronic kidney disease patients ( Stage 5D ) and to correlate its relation with serum uric acid, hemoglobin and serum ferritin Levels.
OBJECTIVES:
To assess the cognitive function in diabetic and non diabetic chronic kidney disease patients ( CKD - Stage 5D ) and their age and sex matched controls.
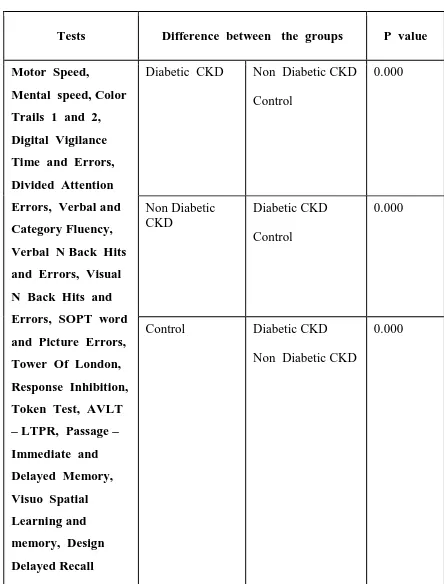
To compare the cognitive function between diabetic CKD, non diabetic CKD and their age and sex matched controls
To measure serum uric acid, hemoglobin, serum ferritin in diabetic and non diabetic CKD patients and their age and sex matched controls.
Aristotle
7
REVIEW OF LITERATURE
Cognition:
The term “cognition” refers to different domains of brain function such as language, learning and memory, executive function, reasoning, decision making, visuo spatial and problem solving. Cognitive impairment refers to the deterioration in these cognitive domains interfering with baseline daily activities of the affected person1,12,13.
History14:
Rennaisance and Phillosophers: They attempted a graphical link describing the anatomy and physiological functions of brain
Aristotle: He was a Greek philosopher and he was considered as first cognitive scientist. According to him cognition begins with inputs from various types of special senses and its integration happens in the brain
Burrhus Frederick Skinner
8
Burrhus Frederic Skinner: He was an American scientist famous for his experiment including skinner box and behaviouralist theory. According to this theory behaviour is a function of the past environment and it can be modified by positive or negative reinforcements. Also Skinner and Watson denoted that brain activities like attention, memory and thinking were hypothetical and its difficult to prove it through experiments.
David Hume ( 1711 – 1776 ): He was a Scottish philosopher who explained
the mechanism of cognition based on association of ideas which occurs
based on three laws proposed by him namely Law of Similarity,
Contiguity and Casualty.
David Hartley ( 1705 – 1757 ): He accepted the association theory and
he added that neural substrates may be responsible for it.
Hermann Ebbinghaus ( 1850 –1909 ) : He was a German psychologist
who did experiments regarding procedural memory and also explained
that learning a poem involves understanding its meaning as well as
learning the words in correct order.
Donald Olding Hebb ( 1904 – 1985 ): He was a Canadian psychologist
who first explained that memory encoding happens when the connections
between neurons were established through repeated use.
Richard Chatham Atkinson and Richard Shiffrin in 1968 first explained
model of memory comprising of sensory, short term and long term
9
Cognitive Domains:
It can be categorised into two major sub divisions namely basic and higher level cognitive functions.
Basic cognitive function includes attention, memory and perception
Higher level cognitive function includes decision making, visuo spatial skills, speech, language and execution.
Let us see the domains one by one in detail15:
1. Attention: It is a complex function involving many other domains of cognition except when it is carried out by habituation. It includes three following subdivisions.
a. Selective attention: It is focussing on particular target by discarding the surrounding distractions. For example in stroop test the word “green” is written in red colour ink and the person is asked to read aloud the colour of the ink in which the word has been written. The person should learn to discard the name and focus only on the colour of the ink to perform this test.
10
c. Sustained attention: It is performing a work with concentration for very long duration. For. Eg. Looking on food stuff to get baked in oven.
Importance of attention: To carry out normal day to day functions without any difficulties one must focus on the necessary things avoiding the distractions, hence attention plays a vital role. Attention also play a major role in safe driving.
2. Memory: It is of two varieties explicit or recognition memory and implicit or reflexive memory
a. Explicit or Recognition memory: It involves association of multiple bits and pieces of information which can be deliberately recalled with conscious effort. It includes two sub divisions.
i. Semantic memory:
It is a long term memory of facts, concepts and words. For instance remembering the Dr. Rajendra Prasad is the first president of India. It takes a little more time to recall especially the names. It is not much affected in elderly. It is stored in different areas in posterior region of neo cortex.
11
b. Implicit or Reflexive memory: It is the knowledge related to performing a task without awareness and it doesn’t require the conscious recall.
c. Working memory: Alam David Baddley and Graham Hitch in 1974 proposed the model of working memory. It is a multi dimensional memory by which an individual works simultaneously based on the information which is stored in the short term memory. For example is remembering the mobile number written in a visiting card by looking at it and then dialling that number without seeing. Prefrontal cortex is the chief centre for working memory.
Its importance: It is essential for understanding the various informations and compiling it together to take appropriate decisions at critical situations in the family as well as while driving to avoid accidents.
d. Procedural memory: It is linked with performing various procedures like playing a guitar or riding a bike.
3. Perception: It is the use of earlier knowledge for understanding the sensory stimuli such as smell, hearing and touch.
Higher Brain Functions15:
12
Its importance: This plays only a submissive role to carry out our daily work because of the major role played by the knowledge which is gained through the experiences of the past.
2. Visuo spatial skill: It is by which a person understands the visual scenario and associate it with the space and understand its position in it.
3. Executive Functions: It is the capacity to plan and carry out their activities in a proper way to reach the target effectively. Pre frontal cortex carries out this function
4. Speech and language: It is the unique property through which human beings share their thoughts with other members of same species.
Structures involved in cognition16:
Pre Frontal Cortex: It is the anterior portion of the frontal lobe which is mainly responsible for the working memory of an individual
Dominant Hemisphere: It plays essential role related to Verbal Tasks Non Dominant Hemisphere: It is responsible for Visuo spatial Skills
13
Parietal Lobe: Primary sensory area 3, 1, 2, secondary sensory and sensory association area 5, 7, 40 helps in recognising the quality of sensation as well as integrating this information for appropriate motor activities to take place.
Temporal Lobe: Primary auditory area 41, 42 deals with understanding the characteristics and direction of sound waves and the auditory association area 22, 21 and 20 are involved in understanding as well as interpretation of words which were dictated.
Occipital Lobe: Primary visual area 17, visual association area 18 and Occipital eye field area 19 are involved in recognising the colour as well as movement of the object and also understanding the meaning of printed words.
Caudate Nucleus: It is a component of basal ganglia, playing essential role in cognition through its complex connections with Frontal lobe and thalamus
Cerebellum: It plays major role in execution function as it is responsible for co-ordination, repetition, modulation as well as to bring about the change in the habitual action.
Hippocampus: It is vital centre for consolidation of long term memory and behavioural actions
14
Mild cognitive impairment ( MCI ) versus dementia:17
MCI describes a patient with slight cognitive disturbances especially related to memory but not exceeding the diagnostic threshold of dementia, a devastating disorder affecting the elderly people with > 65 years of age17. Hence it is a transitional state between normal cognition as per the age and dementia18. It can be classified into two sub groups MCI – amnestic type where there is memory disturbance and MCI – Multiple cognitive deficit type (MCI – MCDT ) where there is defect in any one cognitive domain excluding memory or deficits in two cognitive domains not exceeding the diagnostic threshold for dementia17.
Studies related to MCI:
Lopez, et al, in his study found out the most common variety of MCI is MCI – MCDT. He also found out that MCI – MCDT gain poor scores in the domains including language, Visuo spatial, processing speed and fine motor activities compared to MCI – Amnestic type17.
15
as well as social activities like involving in family parties, business deals, remembering follow up treatment dates in hospital20,21.
Pathophysiology of Cognitive deficit:
i.) Diabetes and hypertension have independent association with cognitive deterioration due to excessive oxidative stress, deranged metabolism, altered endothelial functions of cerebral vasculature3. ii.)Reduced cerebral blood flow for prolonged periods leads to
impaired metabolism of glucose in the brain and excessive phosphorylation of Tau in mouse models by experimentally inducing unilateral occlusion of common carotid artery. Net result is the unfavourable modification in the synthesis of synaptic proteins, insulin signalling and hexosamine shunt pathway which ultimately leads to the impairment in motor function, memory and visuospatial skills22.
iii.) It is found that amyloid Aβ plaques which gets piled up in the neural tissue because of impaired balance between the production and removal of amyloid plaques in Alzheimer patients is found to be toxic enough to damage the neuronal synapses.23 Aβ plaques generally removed from brain into the blood in the following ways namely,
16
the brain into the blood thereby lowering its level in perivascular spaces.
2) Soluble LRP - mediated endogenous Aβ “sink” action in plasma enhances the cell surface LRP - mediated clearance across the BBB. 3) Apo E mediated clearance of Aβ.
Apo E is a chaperon protein for Aβ plaque removal across the BBB. One of its isoform Apo E 4 removes A β very slowly than other isoforms Apo E 2 and E 3. If Apo E 4 levels increased in an individual by genetic homozygosity there occurs early deterioration of cognition.
4) Clearance of A β by microglia and macrophages
Microglial activation removes neurotoxic plaques from spaces around the blood vessels. Macrophages which are positive for Cluster Differentiation ( C D ) 163 and CD 206 in the perivascular spaces plays the role of antigen presenting cell and help is in phagocytosis of toxic plaques.
5) Direct enzymatic degradation of A β in the brain ( green, enzymes ) Passive drainage of A β along the perivascular spaces occurs because of the pulsatile nature of arterial flow in cerebral vessels. Therefore if there occurs any blockage of its clearance it results in piling up of neurotoxic plaques resulting in deterioration of cognition23.
17
v.) In rodents oligomeric Aβ plaques in hippocampus region decreases the density of the neuronal spines and thereby increases the long term depression23.
vi.)In dementia patients, Autopsy slices of brain and its immunohistochemistry analysis for amyloid proteins and fibrillary acidic protein of glial tissue revealed the presence of axonal destruction and gliosis of corpus callosum which plays significant role in transmitting the information between two cerebral hemispheres Therefore atrophy of corpus callosum roughly correlates with atrophy of brain in dementia patients24. vii.) In rat models it is found that reduced cerebral blood flow
leads to more activation of caspase 3 system resulting in fragmentation of chromatin present in the oligodendrocytes and thereby resulting in myelin degeneration and impaired activities of brain25.
viii.) Hyper intensity of white matter of the brain is independently associated with rapid deterioration of cognition, motor performance and even death of the individual26.
18
Genes involved in early cognitive decline: Mutation in the genes PSEN 1 or PSEN 2 ( Presenilin 1 or 2 ) leads to excessive processing of neurotoxic precursor namely the amyloid precursor protein23. Dutch
variant Aβ peptide gets piled up in the vessels supplying the brain tissue due to the reduced clearance mechanism. Dutch, Italian, Flemich mutant
Aβ peptides causes bleeding in the cerebral vasculature enhancing the inflammation and destruction of neural tissue and thereby aggregating the rapid progression of MCI to full blown dementia23.
CKD
Global Health burden Nowadays, Incidence of Chronic kidney disease is enormously rising worldwide mainly because of increase in the prevalence of other non-communicable diseases like diabetes and hypertension which can lead to chronic renal failure if not diagnosed or adequately treated27,28. In India the prevalence of CKD is found to be nearly 0.8% 29.
KDOQI Classification of CKD
19
classification system based on the glomerular filtration rate irrespective of the etiology and pathology. In November 2004 the international organization Kidney Disease: Improving Global Outcomes ( KDIGO ) held its first conference in Amsterdam. Its recommendations were finally analysed in Paris in December 2004 by the board of directors of KDIGO in Paris and gave a clear cut criteria for defining CKD and its classification and also gave some practical advice on its screening and management27.
Criteria to define CKD27:
Kidney damage for ≥ 3 months, as defined by structural or functional abnormalities of the kidney, with or without decreased GFR, that can lead to decreased GFR, manifest by either:
Pathologic abnormalities; or
Markers of kidney damage, including abnormalities in the composition of the blood or urine, or abnormalities in imaging tests.
20
Modified KDOQI Classification of CKD 27
STAGE DESCRIPTION GFR
1 Kidney damage with normal or rise in GFR >= 90
2 Kidney Damage with mild fall in GFR 89 - 60
3 Kidney damage with moderate fall in GFR/
Early Renal Insufficiency 30 – 59
4 Kidney damage with severe fall in GFR/ Late
Renal Insufficiency 15 – 29
5 End Stage Renal Disease / Kidney Failure < = 15
Term ‘D’ is used if dialysis is started for the patient and ‘T’ if kidney transplant is done for the patient18,27,30.
Measurement of GFR: This is the best way to determine the function of kidney27. GFR can be measured by Clearance of Inulin, 51 Cr – labelled EDTA, 125 I- iothalamate and iohexol. But currently in clinical practice, GFR is estimated by the equation Modification of Diet in Renal Disease ( MDRD ):
21
Features favouring renal injury27:
1. Renal blood flow: 400 ml / 100 g of tissue per minute which is very much greater than other vital organs like liver, brain and heart. So nephrons are highly susceptible to the damage caused by the circulating toxins and harmful agents.
2. Glomerular filtration pressure: It is mainly based on high intra glomerular and trans glomerular pressure hence glomerular capillaries are at greater risk for hemodynamic injury.
3. Organizing pattern of microvasculature: Arrangement of glomerular capillary loops and peritubular plexus and also downstream position of tubuli with respect to glomeruli enhances the spread of glomerular injury to tubule interstitial compartment due to exposure to harmful ultra infiltrate and also reduced glomerular blood flow leads to reduced blood flow in peri tubular capillaries resulting in hypoxic damage in tubulointerstitial compartment
Etiology of CKD in India30:
22
Cognitive deterioration in CKD: Cognitive deterioration was more commonly seen in all stages of CKD patients31,32,33. It can be explained based on two hypothesis namely vascular and neurodegenerative hypothesis32.
Vascular Hypothesis: Both brain and kidneys are low resistance end organs. As they are exposed to greater volume of blood flow, these organs are more prone for vascular damage. As traditional vascular risk factors including diabetes, hypertension are often present in CKD patients, they are more prone for lesions in cerebral vasculature as well as white matter leading to cognitive deficit. Also CKD being a highly inflammatory as well as hypercoagulable state, there is great accentuation of the vascular endothelial dysfunction resulting in the deterioration of cognitive functions.
Neurodegenerative Hypothesis: Due to defect in filtration of toxins in CKD patients there occurs retention of uremic toxins which suppresses the production of nitric oxide causing the endothelial dysfunction resulting in cognitive defects32.
Studies related to CKD and cognitive impairment:
23
Conde SA, Fernandes N, Santos FR, Chouab A, Mota MM, Bastos MG in his study also concluded cognitive deterioration was more commonly seen in hemodialysis patients35.
Diabetic Nephropathy ( DN ):
In India, diabetic patients are expected to increase from 40.6 million in 2006 to 79.4 million by 2030. Its prevalence in urban Indian adults is nearly 12.1 %, the onset of which is nearly ten years earlier than their western counterparts36. Poor control of diabetes results in various micro and macro vascular complications37. One among this is DN. Nearly 20 to 30 % of insulin dependent or insulin resistant diabetic patients develop renal problems38.
Diabetic Nephropathy
Stage
Urine with marked
time (μg / min)*
24- hour urine (mg/24h)*
Random Urine Albumin concentration
(mg / l )*
Albumin / creatinine ratio
(mg / g)*
Normoalbuminuria < 20 < 30 < 17 < 30
Microalbuminuria 20 – 199 30 – 299 17 – 173 30 – 299
Macroalbuminuria ≥ 200 ≥ 300 ≥ 174 ≥ 300
24
Genes involved in DN39:
All type- 2 diabetes patients ( Except Causcasians ), those with DD (homozygous deletion genotype ) polymorphism of the angiotensin converting enzyme ( ACE ) genotype have an increased risk for occurrence of DN, severe proteinuria, more chance for rapid progression to renal failure, and higher occurrence of death on dialysis. Three subunits of G- protein at position 825 ( GO3 825 T ) allele is more associated with type- 2 diabetes, with rapid progression to ESRD. Homozygosity for the Z- 2 allele of the aldose reductase gene seen linked with DN in type- I diabetic patients.
Pathological lesion of DN:
Increased thickness of glomerular basement membrane, diffuse schlerosis of mesangium, hyaline arterischlerosis and aneurysms and tubular atrophy and interstitial fibrosis. Extreme expansion of mesangium occurs in half of the patients and it is referred as Kimmelsteil – Wilson nodules41. TGF β has been emerged as a new potential fibrinogenic factor resulting in advancement of DN42.
Diabetes and cognition:
25
control of blood sugar with HbA1C > 7 %36. Structural variations like generalized brain atrophy and white matter hyper intensities in the subcortical regions were reported in both type 1 and type 2 diabetic patients. Atrophy of hippocampus and amygdala were noticed in Type 2 diabetics using MRI. Hippocampus plays a vital function in memory and it has numerous receptors for the hormone Insulin to act over43. As a result there occurs memory disturbances in diabetic patients. Moreover changes in the White Matter of Brain in diabetic patients also leads to defects in various cognitive domains like mental speed, motor speed, attention, execution and memory44.
Mechanism through which Diabetes deteriorates cognition:
1. Increased blood glucose levels may lead to the formation of superoxide anion which is a powerful reactive oxygen species which in turn causes excessive activation of polyol pathway, enhanced formation of advanced glycation end products (AGEs), excess activation of protein kinase C and increased glucose shunting in the hexosamine pathways. Animal experiments proved that there is an increased expression of receptors for Protein Kinase C and AGE ‘s in diabetic rat models45.
26
3. 3–deoxyglucosone, Nε– carboxymethyllisine, N ε – carboxyethyllisine and pentosidine. These play multiple lethal roles like decreasing the availability of Nitric oxide, increasing the adhesiveness of platelets to the vascular endothelium, more activation of white blood corpuscles, affecting the compliance of vascular wall leading to rigid vessels, proliferation of fibroblasts, permanent alteration in the structure and function of various peptides. AGE‘s thereby causes cerebral endothelial dysfunction, vascular thrombosis and neuronal damage leading to decline in cognition10.
4. Increased blood glucose causes neuronal insult through osmotic stress disrupting the BBB and causing easy access for various toxic vascular metabolites to damage the neurons46.
27
Studies regarding diabetes and cognition:
Subha N and Kharan compared the cognitive function of 30 diabetic patients with their age and sex matched controls using Mini Mental State Examination ( MMSE ) and its modified form ( 3 MS ) and found out diabetics score less than their contols47.
Mukherjee P, et al assessed cognition in 50 Type 2 diabetic patients using Kolkata Cognitive Screening Battery and found diabetic patients score less in the domains like fluency, immediate recall and recognition. They treated the diabetic patients and brought HbA1C < 7 and again repeated the same tests for cognition and found out there is a significant increment in the scores related to immediate recall, fluency and recognition. He concluded that controlling blood sugar improves the cognition48.
European Uremic Toxin Work Group ( EUTox ) Classification: 10
Group Features Examples
Low molecular weight Uremic toxins
< 500 Daltons -
molecular weight; Water soluble
Creatine, Creatinine, Asymmetric and Symmetric Dimethyl Arginine ( ADMA, SDMA ),
Urea, Uric acid, Hyaluronic acid, Oxalate,
Protein bound solutes
< 500 Daltons - molecular weight. Difficult to get
eliminated via dialysis due to protein binding nature
AGE , Interleukis, TNF α, Retinol binding
protein, P – cresyl sulphate ( p-CS)
Middle molecular weight solutes
>5000 daltons molecular weight
Cystatin C, Leptin, Adiponectin, Motilin,
Ghrelin, α 1 acid glycoprotein, β 2
28
Uremic Toxins altering the cognition:
The solutes which normally gets excreted in urine gets heaped up in the body in case of renal dysfunction and exert their toxic effects
Mechanism by which Uremic Toxins exert their lethal effects
1. Enhanced Platelet adhesiveness to endothelium - By indole compounds, vascular cell adhesion molecules
2. Increased activation of White Blood Corpuscles - By guanidine derivatives, p-CS, AGE’s, indole compounds
3. Plaque destabilisation - von willebrand factor, thrombomodulin 4. Decreased availability of nitric oxide - AGE’s, ADMA.
5. Decreased compliance of vascular wall - AGE’s, ADMA 6. Defective repair of vessel wall - indole, guanidine substances
7. Vascular calcification - TNF, leptin, reactive oxygen species, inorganic phosphate
8. Increase in pro – inflammatory markers: α 1 acid glycoprotein
All these changes takes place in all vital organs. Because of endothelial dysfunction in cerebral vasculature and vascular occlusion there occurs neuronal damage resulting in cognitive detorioration10.
Uric Acid
29
soluble in plasma. It is excreted mainly in urine hence kidneys play a vital role in Uric acid metabolism. Remaining 1/3rd of uric acid excretion happens through the degradation by the intestinal flora. Plasma uric acid fluctuates widely based on age and gender. It is meagre in children 3 to 4 mg / dl and later its value increases in men after puberty whereas in case of women it increases after menopause. When serum Uric acid > 7 mg / dl in men and > 5.7 mg / dl in women it is referred as hyperuricemia50.
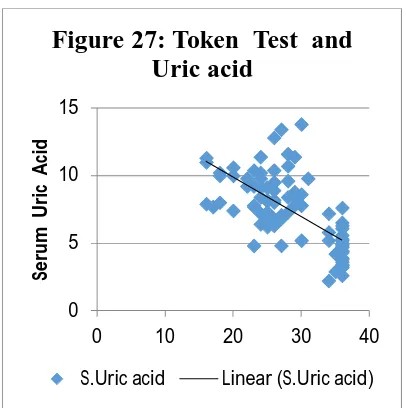
Mechanism by which Uric acid causes cognitive deficits:
Despite being an anti oxidant uric acid is capable to transform into a pro oxidant even when it is mildly elevated or high normal range. Uric acid results in excessive generation of oxygen free super radicles which causes oxidation of lipids, alteration in the synthesis of nitric oxide synthase finally ends up in endothelial dysfunction, atherogenesis and vascular occlusion. This may be the possible mechanism by which mild elevation of Uric Acid is independently associated with rapid decline in cognition and cardio vascular deaths in general population as well as in diabetic and hypertensive patients51,52,53.
Studies related to Uric acid:
30
elevation of serum uric acid affects verbal and working memory and this result is statistically significant52.
Chen J, et al did a large prospective cohort study to examine the
relationship between hyperuricemia and increased all cause mortality and
vascular events in 41,879 men and 48,514 women of age more than 35
years in Taiwan. He found a statistically significant association between
increased serum uric acid and increased vascular events resulting in
mortality even after doing adjustments for age, gender and various co-
morbidities51.
Anemia:
31
WHO Definition of Anemia:
Hemoglobin ( Hb ) < 13 g /dl for men, Hb < 12 g / dl for women55,56,57.
Hb < 12 g / dl for age group between 6 and 14 years and
Hb < 11 g / dl for children of age group between 6 months and 6 years54.
NKF defines anemia as Hb < 13.5 g /dl for men and Hb < 12 g / dl for women28.
Non – Hematological problems of Anaemia:
Anaemia is found to be associated with cognition deficits, increased weakness, decreased motor function, reduced exercise capacity, impaired immunity, left ventricular hypertrophy and hence worsens the quality of life and also increases the risk of death58,59.
Anaemia and CKD:
Anaemia is well known complication seen in CKD patients. It is mainly because of deficiency of iron and erythropoietin or reduced response to erythropoietin. Severity of anaemia increases with advancement in stages of CKD and proteinuria28,60.
32
and as well as mobilisation of Iron from macrophages to blood stream. In CKD due to inflammatory changes and fibroblast proliferation in tubule interstitial spaces there occurs problem in erythropoietin synthesis resulting in anemia28,60.
Mechanism by which Anaemia causes rapid progression of CKD:
Due to reduced oxygen carrying capacity of blood in anaemic patients there occurs renal medullary hypoxia which results in more transcription of Hypoxia Inducible Factor 1 ( HIF - 1 ) gene which is a prime regulator of Epo, Nitric Oxide Synthase, Extra Cellular Matrix, Apoptosis genes. HIF – 1 results in fibroblast proliferation leading to renal interstitial injury and rapid progression of CKD60.
IRON DEFICIENCY ANEMIA ( IDA )
33
enzyme cytochrome b reductase. Iron enters inside the enterocyte via Divalent Metal Transporter 1 ( DMT – 1 ). Iron absorption is high when there is increased demand in the body and also enhanced by Citric acid. Absorption of Iron is retarded by Tannins, Phytates, Calcium, Soya and simultaneous intake of Proton Pump Inhibitors. Iron present inside the enterocyte exits into the circulation mainly via the channel named Ferroportin which is primarily regulated by the hepatic protein Hepcidin which prevents iron from entering into the circulation. Ferrous form of iron gets oxidised to ferric form by the copper based enzyme Ferroxidase hephestin in order to get bound to transferrin which is the primary mobilizing form of iron. Transferrin gets internalised via receptor for transferrin through endocytosis and iron is stored in the ferric form named ferritin which is then re utilised during demand for erythropoiesis. Iron loss happens when the intestinal cells shed over and also in sweat. Normally, iron loss in a healthy adult male is 1 g / day and for a healthy menstruating female it is slightly high 1.5 - 2 g / day. If any disruption occurs in this delicate system of iron balance there occurs deficiency or overload of iron61,62.
Prevalence of IDA:
34
reproductive age group. National Health and Nutrition Examination Survey IV states that 50 % of CKD stages 2 – 5 patients suffer from absolute or relative ( functional ) iron deficiency60.
Absolute and Relative Iron deficiency:
In CKD, both absolute and relative iron deficiency are common. Absolute IDA is defined as depletion of iron stores with serum ferritin less than 100 ng / ml or transferrin saturation < 20 %.
Functional or relative IDA is defined as adequate tissue iron store with serum ferritin level more than 100 ng/ml but reduced iron saturation. Relative IDA is more common in CKD patients and is mainly because of generation of more inflammatory cytokines that impair the response of tissue to the hormone erythropoietin, thereby inhibiting the mobilisation of iron from the tissue stores to erythroblasts. Due to chronic inflammation, CKD patients have increased levels of interleukin -6 increases the synthesis and secretion of hepcidin, a protein synthesised in liver which inhibits gut absorption of iron and also retards the transport of iron from the reticuloendothelial system to bone marrow thereby increasing the occurrence of Functional Iron Deficiency Anemia60,62.
Mechanism by which IDA causes decline in Cognition:
35
neuronal myelination, decreased synthesis, packaging, release and degradation of neurotransmitters like dopamine, number of receptors over which dopamine acts63. In iron deficiency, the function of frontal lobe gets compromised . Defects in cognition can manifest in any age group people and earlier diet modification with iron rich food and iron supplementation may improve the symptoms of cognitive decline63. Laboratory Parameters In Iron Deficiency Anemia:
1. Serum Ferritin - Reduced ( Normal or High in Relative Iron Deficiency )
2. Serum Transferrin Receptor - Reduced 3. Plasma Iron - Low
4. Total Iron Binding Capacity ( TIBC ) - High
5. Transferrin Saturation = ( Plasma Iron / TIBC ) X 100 - Low57.
Serum Ferritin:
History:
36
Biochemistry of Ferritin:
Serum Ferritin is a 24 subunit protein made up of two isoforms H , L.
“ H ” isoform is heavier than “ L ” and it is isolated from human heart and its gene is present on chromosome 11 q
“ L ” isoform is lighter and it is isolated from human liver and its gene is present on chromosome 19 q.64
In inflammatory conditions there occurs increased transcription of “H” isoform genes65.
Source of Ferritin: Hepatocytes, Kupfer cells and Macrophages65.
Main Functions: Stores iron in the ferric form. It can be re utilised whenever there is increased demand for erythropoiesis. A healthy adult male with normal ferritin level of 50 - 100 ng / mL would be expected to have 500 - 1000 mg of iron stores ( nearly 1 : 10 ratio ). It is also a acute phase reactant getting enormously elevated during inflammation.62 Some studies revealed the significant association between higher ferritin levels and hospitalization and death rate in hemodialysis patients66.
Measurement of Serum Ferritin:
37
Management of IDA in CKD:
1. Iron Supplementation For Absolute Iron Deficiency
2. Erythropoietin Stimulating Agents + Iron Supplementation for Relative Iron Deficiency60.
Studies regarding anemia, iron deficiency and cognition:
Murray - Kolb and Beard tested the relationship between the functions of cognitive domains and severity of anaemia and iron deficiency in women of reproductive age group using Cognition Abilities Test and also reassessed the same after 16 weeks of giving iron supplements. Women who have Iron deficiency got poor scores in domains like learning, attention and memory. Women who responds well to the iron supplements showed 5 times increment in domains like learning and attention and 7 times increment in case of memory. So they concluded that Iron is indispensable for cognitive performance in all age group67.
38
Hypertension in CKD affecting Cognition:
Middle age people with hypertension in middle age were prone to suffer from cognitive dysfunction in later life68,69. Hypertensive patients found to get less scores in various domains of cognition including Execution, Visuo spatial skills, attention, learning and memory. Their MMSE score related to attention, calculation, orientation, immediate recall is found to be lower in hypertensives70.
Mechanism by which hypertension affects cognition:
1. High Blood Pressure leads to alteration in the function of endothelium, oxidative stress, stiffening of arteries which ultimately affects the blood flow to the brain and causes derrangements in the metabolism taking place in the brain leading to cognitive deficits71.
2. Long duration hypertension is lethal to oligodendrocytes. It also causes astrocytes to swell and enhances the phagocytic activity of the microglial cells.
39
Studies related to Hypertension and cognition:
Kalaitzidis RG, et al investigated the risk factors associated with deterioration of cognition in CKD as well as hypertensive patients. He noted down that patients with pulse pressure > 60 mm Hg have more cognitive derrangements68.
Duron E, Hanon O in their study concluded that diabetes and hypertension in middle age is associated with rapid deterioration of cognition and also insisted the usefulness of antihypertensive drugs to achieve betterment in the function of various cognitive domains71.
Lipid abnormalities and cognitive deficit: LDL/HDL ratio alteration, elevated triglycerides speeds up the lipids to get deposited in the bood vessels reducing the cerebral blood flow hence ending up in accelerated deterioration of cognition. Statin therapy found to cause improvement in verbal memory75,76. Recently through DNA extraction and genetic mapping the significant modifying role played by 3-hydroxy-3-methylglutaryl-CoA reductase gene in onset of MCI was revealed77.
Studies related to CKD and Cognition:
Elias MF, et al assessed the cognitive disturbances in CKD patients after adjusting for cardio vascular diseases. He found out CKD patients perform poorly related to domains like Visuo spatial attention, memory and processing speed Immediate recall, Delayed recall and Planning78.
40
concluded that moderate CKD patients has impaired cognition in various domains learning, visual attention and concentration79.
41
MATERIALS AND METHODOLOGY
Study design: Case - Control study
Study place: The study was conducted in the department of Physiology, in association with department of Nephrology and Biochemistry,
Coimbatore Medical College and Hospital, Coimbatore.
Study period: The study was conducted from July 2015 to June 2016. Study subjects:
Inclusion criteria:
30 diabetic CKD and 30 non diabetic CKD patients of both gender with age group between 18 and 60 years, with eGFR less than 15 ml / min /1.73 m2, for more than 3 months of duration were included in this study. Age, gender, BMI and education matched normal individuals were used as controls.
Exclusion criteria:
Patients with history of cerebro vascular accident, brain tumors, psychiatric disorders, thyroid disorders, seropositive cases
( HIV + ), acute kidney injury, ischemic heart disease, congestive cardiac failure, gout on treatment with hypouricemic drugs, major visual disturbances, hearing impairment and past h / o of head injury with loss of consciousness, h / o alcohol intake > 120 g / week or 13 units / week were excluded.
42
Methodology
Every test was performed after getting consent from the patient and also giving clear instructions regarding its procedure.
Study protocol
History taking and clinical examination: A detailed clinical history was obtained from the subject to know about the duration of the current symptoms, control of blood glucose and also to rule out head injury, psychiatric illness, stroke and acute kidney injury. General examination followed by systemic examination was done.
Measurement of anthropometric indices: The anthropometric indices of study subjects were measured using portable weighing machine and a stadiometer. Their BMI was calculated by the formula given by the Quetelet’s Index, BMI = ( Weight in Kilogram ) / ( Height in metre)2 Measurement of blood pressure: Subject was made to sit comfortably and correct size cuff was tied in left mid arm and blood pressure was recorded using palpatory and auscultatory method.
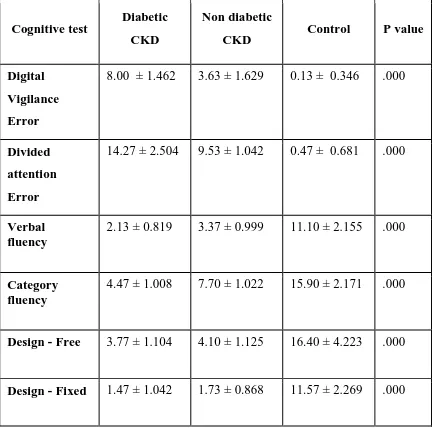
NIMHANS Neuropsychology Battery 2004
Domains Sub – Categories Tests
Speed Motor Speed Finger Tapping Test
Mental Speed Digital Symbol Substitution Test
Attention
Focussed Attention Color Trails Test 1 and 2 Sustained Attention Digital Vigilance Test Divided Attention Triads Test
Executive Functions
Phonemic Fluency Controlled Oral Word Association Test
Category Fluency Animal Name Test Visual Fluency Design Fluency Test Verbal Working
Memory
Verbal N Back Tests – 1 and 2 version
Visual Working
memory Visual N Back - 1 and 2 versions Internally guided
Verbal and Visual Memory
Self Ordered Pointing Tests
Planning Tower Of London Test Response Inhibition Stroop Test
Comprehension Verbal comprehension Token Test
Learning and memory
Verbal Rey’s Auditory Verbal Learning Test
Logical Passage - Recall Test Visuo Spatial Complex Figure Test Visual Learning and
Memory
43
Assessment of cognition:
After giving clear instructions their cognition was tested using NIMHANS Neuropsychology Battery - 2004. It consists of 18 tests to check various cognitive domains.
Motor speed: The subjects were asked to sit comfortably with their hands placed on an even surface . They were asked to spread their fingers well and do the tapping with the right index finger alone as fast as possible. The same procedure was done in 5 trials each lasting for ten seconds with a break of 30 seconds between 3rd and 4th trial. Every time the number of taps was noted. The subjects were asked to repeat the same trials using their left index finger. The mean no. of taps performed by each hand was calculated and this gives the score for motor speed in each hand separately.
Mental speed: Digital Symbol Substitution Test ( DSST ) :
Number symbol key was present in the top portion of the test sheet. The subjects were made to sit comfortably and test sheet was provided to them. The concept of substituting the symbol for the digits was explained clearly and practice for first 10 squares was given. Then the test was begun and the time taken by the subjects to complete the task were noted down and this gives the score of mental speed.
44
pink in case it was an odd number and yellow colour circle was used if it was an even number. After explaining the practice sheet, the subject was asked to denote the numbers in the test sheet orderly and the time taken by the subject to finish the task was noted down and this gives the score for the focussed attention of the subject.
Color Trails 2: Similar to Color Trail 1 it also had a practise sheet and test sheet with only difference that all digits were printed twice in pink as well as yellow coloured circles. Subject was instructed clearly with the help of practice sheet that he must point out the digits successively with an extra concept in his mind that he should touch the digit in pink circle omitting the same printed in yellow circle if it was an odd number and vice - versa for an even number. The total duration to finish the task gives the score for the focused attention domain of the subject.
Digital Vigilance Test: Test paper contains randomly distributed digits from 1 to 9 in 50 rows and 30 columns. The subject was asked to strike off the digits six and nine alone in all the rows as soon as possible. Time taken to complete the test and errors made were noted down. Both depict the sustained attention of the subject.
45
word followed by the written digit. Total number of word errors and digit errors made by the patient gives the score for divided attention of the subject.
Controlled Oral Word Association Test ( COWA ): The subject was clearly illustrated to tell more number of words beginning with the letter given by the examiner without any repetition and also he was instructed to avoid the names representing a place or an individual. This test was carried out in mother tongue Tamil. Subjects were also informed if the letter “ Ma” was given they can also say words starting with “Maa”, “ Mi”, “Mee”, “Mu”, “Moo” etc. 3 such trials were carried out with each trial lasting for 1 minute. Mean number of new words told by the subject in all 3 trials gave the phonetic fluency score of the subject.
Animal Names Test: Subject was asked to say as many animal names as possible in one minute but omitting the names of reptiles, amphibians and birds. Total number of new names told by the subject gave the category fluency score of the subject.
Design Fluency:
Free condition: The subject was asked to draw as many new designs as possible in 5 minute duration without drawing similar designs, rangoli, geometrical shapes, meaningful pictures or embroidery patterns.
46
Score: Total number of correct designs which matched the given instructions was noted down and this gave the design fluency score of the subject.
Verbal N Back Test: It measures verbal working memory.
1 Verbal 1 Back Test: Thirty randomly ordered consonants was read aloud to the subject in a speed one word per second and the subject was asked to raise the hand whenever the constant was repeated successively.
2 Verbal 2 Back Test: Another set of constants were read aloud and patient was asked to respond whenever the constant
reappears after an intervening constant.
Score: There are two types of scores for verbal 1 and 2 Back tests based on correct responses and number of errors which includes both omission and commission
Visual N Back Test: It measures visual working memory.
It consists of 36 cards with a black dot randomly printed on it.
Visual 1 Back test: Just like verbal n back test the subject should raise the hand whenever he see the dot in same position in successive cards.