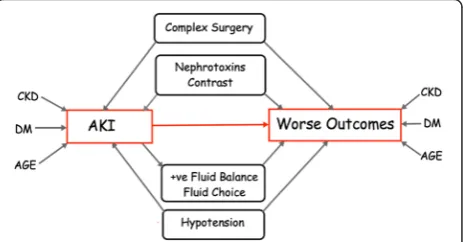
Acute kidney injury: short term and long term effects
Full text
Figure

Related documents
Based on a sample of 129 Polish business students, using hierarchical regression analysis, we investigate the need for cognitive closure (NfC) as an antecedent of entrepreneurial
The descriptive measures for the following parameters: age of cows (years), number of cows/farm, yearly milk yield/cow (kg), duration of preg- nancy, treatment at hours p.p.,
Because of the maturation of appropriate valuation models in barrier options and reset options recently, we could apply the concepts of barrier options and reset options to evaluate
Ob-Rb expression was also increased on day 7, as determined by Western blot within the ipsilateral spinal cord dorsal horn of CCI rats ( C ), with a time course similar to that of
Here the three materials selected which are glass fiber reinforced polymer(E-glass/epoxy), carbon epoxy and graphite epoxy used against conventional steel. The design parameters
In summary, this study shows no effect of GHRH antagonists on proliferation of non-tumor cells and provides a further elucidation of the mechanisms of action of
The bifurcation ratio is the ratio of the number of the stream segments of given order ‘Nu’ to the number of streams in the next higher order (Horton
The association rules generated for the query input by the user using the previous question logs is shown in fig 7.. The experimental data show that the associations
