1
STUDY OF OCULAR HYPOTENSIVE EFFECT AND TOLERABILITY OF FIXED COMBINATION BRINZOLAMIDE 1% AND BRIMONIDINE 0.2% IN INDIAN EYES WITH OPEN ANGLE GLAUCOMA
DISSERTATION SUBMITTED TOWARDS FULFILMENT OF THE RULES AND REGULATIONS FOR
THE M.S. BRANCH III OPHTHALMOLOGY EXAMINATION OF THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY
2
STUDY OF OCULAR HYPOTENSIVE EFFECT AND TOLERABILITY OF FIXED COMBINATION BRINZOLAMIDE 1% AND BRIMONIDINE 0.2% IN INDIAN EYES WITH OPEN ANGLE GLAUCOMA
3
BONAFIDE CERTIFICATE
This is to certify that this dissertation entitled “Study of ocular hypotensive effect and tolerability of fixed-combination Brinzolamide 1% and brimonidine 0.2% in Indian eyes with open angle glaucoma ” done towards fulfillment of the requirements of the Tamil Nadu Dr MGR Medical University, Chennai for MS Branch III (Ophthalmology)
examination to be conducted in April 2018, is the bonafide original work of Dr. Sujitha Ramesh, Post Graduate student in the Department of Ophthalmology, Christian Medical College, Vellore
Dr. Andrew David Braganza, MS The Principal,
Professor and Head of the Department, Christian Medical College,
Department of Ophthalmology, Vellore- 632001 Christian Medical College,
4
BONAFIDE CERTIFICATE
This is to certify that this dissertation entitled “Study of ocular hypotensive effect and tolerability of fixed-combination Brinzolamide 1% and brimonidine 0.2% in Indian eyes with open angle glaucoma ” done towards fulfillment of the requirements of the Tamil Nadu Dr MGR Medical University, Chennai for MS Branch III Ophthalmology examination to be conducted in April 2018, is the bonafide original work of Dr. Sujitha Ramesh, Post Graduate student in Ophthalmology, Christian Medical College, Vellore
Guide
Dr. Arathi Simha R Associate Professor,
Department of Ophthalmology, Christian Medical College, Vellore- 632001.
Co guides:
Dr. Andrew Braganza ( Professor)
5
BONAFIDE CERTIFICATE
This is to certify that this dissertation entitled “Study of ocular hypotensive effect and tolerability of fixed-combination Brinzolamide 1% and brimonidine 0.2% in Indian eyes with open angle glaucoma ” done towards fulfillment of the requirements of the Tamil Nadu Dr MGR Medical University, Chennai for MS Branch III Ophthalmology examination to be conducted in April 2018, is the bonafide original work of Dr. Sujitha Ramesh, Post Graduate student in Ophthalmology, Christian Medical College, Vellore
Dr. Sujitha Ramesh Post Graduate student,
6
ACKNOWLEDGEMENT
At the outset, I want to thank God for bringing me this far and guiding me in every step of my career.
I would like to express my sincere gratitude to my guide, Dr. Arathi Simha R, for her patience, guidance, suggestions, healthy criticism in the conduct of this work, from its inception to the conclusion. Her advice has been invaluable in the final presentation of the thesis in its current form. Her insight into this work and immense knowledge has been invaluable and a great learning experience. Also, her inputs for the statistical analysis were very useful. This is my first insight into research and I feel privileged to have her as my mentor.
I would also like to express my heartfelt gratitude to my co guides Dr. Andrew Braganza and Dr. Lekha Mary Abraham. Their time, patience, suggestions, encouraging and reassuring words, moral support have been pivotal in the completion of this work. There’s a kind of inspiration that’s not much more than doing the right thing in the right way, and I feel
extremely lucky to have Sir and madam as my co guide. Their help was indispensible for this study. I would also like to thank my biostatistician, Mrs. Mahasampath Gowri for helping me with the statistical analysis inspite of her busy schedule.
7
8
TABLE OF CONTENTS
Content Page number
Introduction 1
Aims and Objectives 3
Literature Review 5
Materials and Methods 44
Results 51
Discussion 67
Limitations 73
Conclusion 74
References 76
Annexure
IRB approval letter 95
Patient information sheet 100
Consent form 103
Clinical research proforma 111
Colour plate 115
1
INTRODUCTION
Glaucoma represents a progressive optic neuropathy characterized by nerve fiber layer defects which lead to characteristic optic disc changes and visual field defects (1). It has a multifactorial aetiology with intraocular pressure (IOP) being the only major modifiable risk factor (2).The mainstay of treatment involves lowering of the intraocular pressure by various methods. Although there is no absolutely ‘safe’ pressure that guarantees prevention of progression, lowering intraocular pressure to the low-normal range usually arrests or slows the progression of glaucoma. The two main modalities of treatment include surgical and medical. Usually 25% - 30% reduction in baseline intraocular pressure (3)(4)(5) or achievement of Target intraocular pressure is the goal of treatment. Target intraocular
pressure is defined as the upper limit of the range of measured intraocular pressures adequate to stop progressive pressure induced damage of optic nerve head. Medical management consists of topical administration of various classes of anti-glaucoma medications in the form of eye drops. The anti-glaucoma medications available include β blockers (Timolol 0.5%, Betaxolol 0.5%), alpha adrenergic agonists (brimonidine 0.2%), Prostaglandin analogs
(latanoprost 0.005%, Travaprost 0.004%, Bimataprost 0.03%), Carbonic anhydrase inhibitors (dorzolamide 2% ,brinzolamide 1%) and Parasypathomimetics (Pilocarpine 1-4%).
2
anhydrase inhibitors and Alpha adrenergic agonists (7). However beta blockers cannot be used in asthmatics and patients with heart blocks. Also, in patients with uveitis as well as those planned for intraocular surgeries, prostaglandin analogues are best avoided due to the risk of increased incidence of cystoid macular oedema or worsening of uveitis (8). Carbonic anhydrase inhibitor and Alpha adrenergic agonist are the drugs preferred in these patients. Recently fixed combination Carbonic anhydrase inhibitor and Alpha adrenergic agonist is available in the market. It can be used as first line therapy (9)(10) or added on in patients wherein intraocular pressure control is inadequate with monotherapy with Prostaglandin analogs and Beta blockers are contraindicated(11)(12). The efficacy of fixed combination of carbonic anhydrase inhibitor and alpha adrenergic agonist has been studied in various
3 AIM:
4
PRIMARY OBJECTIVES:
1. To determine the reduction in Intraocular pressure achieved in patients with
open angle glaucoma by the fixed combination brinzolamide1% and brimonidine 0.2% at 1 month as measured during office hours.
2. To determine the tolerability and side effect profile of fixed combination
brinzolamide 1% and brimonidine 0.2% .
Secondary objective:
5
LITERATURE REVIEW:
Glaucoma comprises a multifactorial group of diseases characterised by chronic progressive anterior optic neuropathy that is accompanied by a
characteristic cupping and atrophy of the optic disc, and visual field loss, with elevated intra-ocular pressure being the only modifiable risk factor. (17)
About 12 million people in India are affected by glaucoma accounting for 12.8% of the blindness in the country. Early population based studies reported a prevalence of glaucoma between 2% and 13% (21). The Vellore Eye Survey (VES) reported a prevalence of Primary open angle glaucoma (POAG) as 0.41%, ocular hypertension (OHT) 3.08 %(22). The Andhra Pradesh Eye Disease Survey (APEDS) reported a prevalence of 1.62% for POAG, 0.32% for OHT of the study population (23).
AQUEOUS HUMOR DYNAMICS AND INTRAOCULAR PRESSURE
In the human eye there is a balance between production of aqueous humor as well as its drainage. The intraocular pressure is held in a stable balance
through different mechanisms. The aqueous humor is secreted by the ciliary epithelium lining the ciliary processes. Three physiological processes
contribute to the formation and chemical composition of the aqueous humor: diffusion (5 %), ultrafiltration (15 %) and active secretion (80 %). (18)
6
normal individuals. The diurnal fluctuation in normal individuals is 3-6mmHg (19)(20). Aqueous humor leaves the eye by passive bulk flow via two
pathways: the trabecular route and the uveoscleral route.
DEFINITION OF TERMS
Primary open angle glaucoma is a chronic, progressive, anterior optic neuropathy that is accompanied by a characteristic cupping and atrophy of the optic disc, visual field loss, open angles, and no obvious causative ocular or systemic condition. In the majority of cases, intra-ocular pressure is elevated above the statistically normal range (>2 standard deviations from the mean, or 21 mmHg) , and is the major risk factor. Normal tension glaucoma refers to typical glaucomatous optic disc cupping
and visual field loss in eyes that have normal corrected intraocular pressure (≤
21 mmHg) open angles, and the absence of any contributing ocular or specific systemic disorders (17)
Pigmentary glaucoma and Pseudoexfoliation (PEX) glaucoma are
secondary open angle glaucomas wherein the pigments and pseudoexfoliation material respectively clog the trabecular meshwork causing raised intraocular pressure.
7
These patients are at a risk of developing disc and field changes due to the high intraocular pressure and often are treated with anti- glaucoma medications to keep the intraocular pressure under control.
TARGET INTRAOCULAR PRESSURE AND THERAPY FOR GLAUCOMA
Target intraocular pressure is defined as the upper limit of the range of measured intraocular pressures adequate to stop progressive pressure induced damage of optic nerve head. Reduction in Intraocular pressure forms the mainstay of management of glaucoma.
Lowering Intraocular pressure to an individualized target level (typically a >25% reduction from initial Intraocular pressure) and maintaining that level reduces the risk of vision loss and improves outcomes (3)(4)(5). Reduction of Intraocular pressure can be achieved by antiglaucoma medications or by glaucoma surgery . Also Intraocular pressure reduction slows the progression of disease.
Antiglaucoma medications in the form of topical medications (drops) include β-blockers (eg. Timolol), prostaglandin analogs (eg.. latanoprost),carbonic anhydrase inhibitors (eg. Dorzolamide, brinzolamide) and α2-adrenergic
agonists (eg.brimonidine) and cholinergic agonists (eg.pilocarpine) (4)(24).
8
DIURNAL VARIATION OF INTRAOCULAR TENSION (DVT) :
The intraocular pressure exhibits a rhythmic pattern which peaks in the morning and troughs in the evening. In normotensive patients , the 24-hr Intraocular pressure fluctuation lies within a 5 mmHg range ( 26). The fluctuations of intraocular pressure is also influenced by body posture, rate of aqueous humor formation. The aqueous production has an nocturnal dip and rises during day in response to circulating catecholamines. Intraocular pressure measured in the sitting position is generally lower than that measured in the supine position at any given time (27).
DVT in Normals
Drance ( 28) measured the Intraocular pressure of 404 normal subjects between 6:00 am and 10:00 pm and results showed that 16% of cases showed a fluctuation more than 6 mmHg, while 42% of them showed their peak pressure at 06:00 am. The mean intraocular pressure fluctuation was 3.7 ± 1.8 mmHg.
In another study by Katavisto et al (20). showed that the highest IOP values at 8.00 am
9
DVT in primary open Angle glaucoma , ocular hypertension and pseudoexfoliation glaucoma :
Wilensky et al. conducted a study [30] with a group of 176 patients with Primary open angle glaucoma and 55 subjects with Ocular hypertension and 18 normal controls who performed home self-tonometry 5 times daily for 4 to 8 consecutive days. These three groups showed well-defined diurnal Intraocular pressure fluctuations with peak at morning or mid-day .The mean fluctuation of IOP was 5.0 mmHg in normal , 5.8 mmHg in patients with primary open angle glaucoma and 6.8 mmHg in patients with ocular hypertension.
Pseudoexfoliation glaucoma patients typically exhibit greater 24-h fluctuation, peak and trough Intraocular pressure than primary open angle glaucoma patients. Konstas et al. (95) showed a 24-h intraocular pressure fluctuation more than 15 mmHg in 35% of pseudoexfoliation glaucoma patients but only in 7.5% of primary open angle glaucoma patients. It reported peak intraocular pressure between 10:00 pm to 6:00 am in 45% pseudoexfoliation glaucoma patients and 22.5% of primary open angle glaucoma patients.
TOPICAL ANTIGLAUCOMA MEDICATIONS :
Definition of pharmacological terms:
Efficacy is defined as maximum therapeutic effect obtainable.
10
Th ratio of dose of a drug producing a toxic effect divided by the dose producing the desired effect is therapeutic index.
Compliance is defined as the degree or extent of conformity to the recommendations about day to day treatment by the provider with respect to the timing ,dosage and frequency.
The rate and extent of absorption across a tissue is referred as bioavailability. Various factors influencing the bioavailability of topical medication are corneal barriers, drug formulation, and drug elimination . The limitations for bioavailability are compliance and efficiency of instillation.(25)
Various classes of topical anti-glaucoma medications:
Parasympathomimetic or Cholinergic agents
They mimic the action of Acetylcholine , which is a neurotransmitter present at the postganglionic parasympathetic nerve endings. Acetylcholineesterase is an enzyme which hydrolyses acetylcholine in order to limit its action.The Parasympathomimetic agents act directly by mimicking acetylcholine or indirectly by inhibiting the
11
receptors Nicotinic and Muscarinic. Of which M1, M2, M3 receptor subtypes are abundantly present in the eye.
Topical agents are
1. Pilocarpine 2. Carbachol
3. Ecthiophate (indirectly acting agent)
Pilocarpine (1-4% ):
It is a directly acting cholinergic agonist which acts on muscarinic receptor. It stimulate the ciliary muscle, causing traction on the scleral spur and the trabecular meshwork, which separates the trabecular sheets and prevents Schlemm’s canal from
collapsing. This mechanical change in the configuration of the meshwork increases fluid conductivity(31)(32). It also causes constriction of iris sphincter muscle and causes miosis which is useful in angle closure as it pulls the peripheral iris away from trabecular meshwork.
It is a water soluble hydrochloride or nitrate and is stable at a slightly acidic pH .
12
at bed time which prolongs and increases drug penetration.( 33). Another delivery system is OCUSERT which is a membrane controlled delivery system for constant release f 20 and 40 micrograms of drug every hour (34). Other delivery systems are soft contant lens and pilocarpine polymer. Pilocarpine effect is additive to most available antiglaucoma medications such as Beta blockers, prostaglandin analogues.
Carbachol (1.5- 3%) :
It is a parasympathomimmetic which acts directly on motor end plate and
indirectly by inhibiting acetyl cholinesterase. It is more potent and has prolonged pressure lowering effect but has poor corneal penetration .Also provides better Intraocular pressure control in early postoperative period.(35)
Echothiphate Iodide (0.06%) :
It inhibits acetyl cholinesterase and prolongs the effect of acetyl choline. It is an indirectly acting parasympathomimmetic and has prolonged action due to slow hydrolyses.
Ocular side effects of Parasympathomimetic drugs: Miosis
Ciliary muscle spasm Headache and browache Lid twitching & pain
13
Increased vascular permeability Cataract formation
Hypersensitivity reactions Stinging, irritation , lacrimation Myopic shift
Cyst of the iris pigment epithelium Rhegmatogenous retinal detachment Cicatricial pemphigoid
Systemic side effects of parasympatomimetic drugs :
Bronchospasm Nausea, vomiting,
Diarrhea, abdominal pain Weakness, fatigue
Paresthesia
Sweating, salivation, lacrimation Hypotension, bradycardia
Depression
Due to the adverse effects of ciliary spasm and miosis and the availability of newer more effective drugs, parasympathetic durgs are nowadays rarely used in the
14
detachment,peripheral retinal degeneration, chronic obstructive pulmonary disease, peptic ulcer, Parkinson’s disease, bradycardia, hypotension and myasthenia gravis.
Parasympathomimetics in the present day is mainly used in the management of angle closure glaucoma for short periods of time in acute angle closure in appropriate cases awaiting definitive management.
Beta blockers or Adrenergic antagonists:
Beta receptors are of three subtypes β1, β2 and β3. Of which Ocular beta adrenergic receptors are β2 subtype. Normally Beta receptor agonists stimulate G protein to
activate adenylate cyclase enzyme which catalyses conversion of ATP to cyclic AMP. Cyclic AMP act as second messenger to trigger a cascade of biochemical events necessary for regulation of ion channels and enzymes in ciliary epithelium which is responsible for aqueous production.
Beta blockers act on β2 subtype receptors and causes inhibition of catecholamine
stimulated synthesis of cyclic AMP and results in decrease in aqueous humour production. (Timolol maleate 0.5%, Betaxolol 0.5% ) decrease aqueous humor formation by antagonizing a resting β-adrenergic tone in the ciliary processes. Such a
tone would have to be supplied by either the sympathetic nervous system or circulating catecholamines.(36)
Other mechanism of action are β2 receptors are present in the blood vessels of ciliary
15
mediated vascular constriction . This results in reduced blood supply to ciliary body which reduces capillary perfusion pressure and decreases aqueous formation. (37)(38)
The topical Beta blockers are:
1. Timolol maleate
2. Betaxolol
3. Levobunolol
4. Carteolol
5. Metipranolol
Timolol maleate (0.25, 0.5%)
It is a nonselective β1 and β2 adrenergic antagonist without intrinsic
sympathomimetic activity and membrane-stabilizing properties.
properties. It is available as a solution (0.25% or 0.50%) which can be administered twice daily and as a hydrogel (0.1% or 0.5%) which can be administered once daily
16
anhydrase inhibitors and alpha 2 agonistsThe advantages of fixed combination are increased adherence, decrease in cost and less exposure to preservative. It has short
term escape phenomenon due to an increase in the number of -adrenergic receptors in the ciliary processes under the condition of prolonged -adrenergic blockade.
In about 10–20% of patients may have some loss of drug effect over subsequent months. This is termed as ‘long-term drift’ due to decrease in cellular sensitivity
to adrenergic antagonists.
Betaxolol ( 0.5 or 0.25%):
It is a selective β1-adrenergic antagonist. It does not have intrinsic sympathomimetic
activity and membrane-stabilizing properties. Betaxolol reaches the ciliary epithelium at high concentration and blocks β2 receptors. Other explanations are presence of β1
receptors in ciliary body or a nonadrenergic effect of betaxolol on Intraocular
pressure.( 39) . In addition to reduction in intgraocular pressure by decreasing aqueous humour formation. It has neuroprotective effect and reduce the progression of visual field defects in comparison with timolol (40) .
It also increases retinal sensitivity and relaxes the smooth muscle of retinal arterioles and hence increases retinal blood flow (41). Betaxolol has less effect than timolol to induce β2-adrenergicmediated bronchial constriction and hence can be used in
17
Levobunolol (0.25 or 0.5 %) :
It is a lipophillic non-selective β1 and β2 adrenergic antagonist. It lacks intrinsic sympathomimetic activity . It is equivalent to timolol in its efficacy.
Carteolol (1% or 2%) :
It is a non selective hydrophilic β adrenergic antagonist with intrinsic
sympathomimmetic activity. It has similar efficacy as timolol . Buts as it has intrinsic sympathomimmetic activity it might produce cardiovascular effect such as
bradycardia , hypotension and pulmonary effects..
Metipranolol (0.3%):
It is a lipophilic non-selective β1- and β2-adrenergic antagonist. Its Intraocular pressure lowering effect is similar to Timolol. One of the side effect reported is granulomatous uveitis .( 43 )
Ocular side effects of β blockers: Burning, stinging, itching , irritation
Superficial punctate keratitis, dry eye, decreased corneal sensation
Systemic side effects of beta blockers: Depression , Hallucinations ,confusion
Bradycardia , Arrhythmia , Heart failure ,Hypotension , Heart blocks Airway obstruction/asthma , Pulmonary failure
18
Nausea , Vomiting , Diarrhea , Abdominal cramping
Non selective β blockers are contraindicated in patients with asthma , chronic
obstructive pulmonary disease, sinus bradycardia, and heartblock.
Prostaglandins :
Arachidonic acid metabolism results in production of prostaglandins .Prostaglandin receptors are G protein coupled receptors. There are 4 types of prostaglandin receptors EP, FP, IP and TP which are specific for prostaglandins PGD2, PGE2, PGF2α ,PGI2 or TxA2 .
Topical prostaglandin analogs are :
1. Latanoprost (0.005 %) 2. Travoprost (0.004%) 3. Bimataprost (0.03%) 4. Unoprostone (0.15%)
Mechanism of action :
Prostaglandins reduce intraocular pressure by increasing uveoscleral outflow. It stimulates enzyme which degrades and remodels the extracellular matrix such as metalloproteinases and transcription factors.
19
levels . Hence it increases conventional outflow following calcium dependant tissue contraction.
Latonoprost ,travoprost are all esterified prodrugs and are hydrolyzed by corneal esterases to their active part. Bimataprost is a prodrug with an ethyl amide instead of an isopropyl ester. Hence it is partially hydrolyzed by amidase . No short term escape or long term drift phenomenon is seen with prostaglandins.
Latanoprost (0.005%) :
Latanoprost is a potent prodrug which is rapidly converted by cornea into its active ingredient. It reaches its peak aqueous humor level 1–2 hours after topical
application with a half-life of 2–3 hours. Its peak level in bloodstream is 5 minutes with a half-life of 17 minutes. The acid is metabolized in the liver by oxidation and eliminated through feces and urine. It is used once daily at night. Latanoprost has an additive effect with other antiglaucoma medications such as beta blockers, carbonic anhydrase inhibitors.
Travaprost (0.004%)
Travoprost is a synthetic prostaglandin F2α analogue and is a prodrug. It is an isopropyl ester of prostaglandin F2α agonist. It is hydrolyzed into its active part by
20
analogues travoprost has maximum affinity for the FP receptors followed by bimatoprost,latanoprost and uniprostone respectively.
Bimataprost (0.01% ,0 .03%):
It is a prostaglandin F2α analog where neutral ethylamide replaces carboxylic acid .It has little direct effect on prostaglandin F2α receptors (47) .It is not converted to its active
counterpart and enters into the eye unchanged which acts on prostamide receptor. Compared to other prostaglandin analogues , conjunctival hyperaemia is reported more in bimetaprost .
Isopropyl Unoprostone ( 0.15 %)
This prodrug is a docosanoid which is derived from docosahexanoic acid. It is an analogue of pulmonary metabolite of PGF2α . It also increases conventional outflow.
The ocular side effects are :
The unique side effects of the prostanoids is the darkening and increase in length of the eyelashes, iris discolouration , uveitis and cystoid macular edema. The most common side effects in the three multicenter, international, comparative studies after 6 months of latanoprost treatment were conjunctival hyperemia, foreign body sensation, eye irritation, and superficial punctate keratopathy (52). Other side effects are periocular hyperpigmentation , Blurred vision , Dry eye Superficial punctate keratitis, PG associated peri-orbitopathy, and choroidal effusions
Systemic side effects are uncommon. Few systemic side effects of prostaglandins include
21
Myalgia ,arthralgia , abdominal cramps Cough and possible uterine contraction
Prostaglandin analogs are contraindicated during pregnancy and lactation. (17) Carbonic anhydrase inhibitors (dorzolamide 2% ,brinzolamide 1%)
They are sulphonamide derivatives. It reduces aqueous production through
inhibition of sulfonamide-susceptible carbonic anhydrase isozymes.(48). Carbonic anhydrase is an enzyme for catalytic hydration CO2 and dehydration of H2CO3 in ciliary epithelium. This results in formation of bicarbonate and hydrogen ion which is important in aqueous humor formation. There are multiple isoenzyme forms of carbonic anhydrase enzyme of which type I and II both present in the corneal endothelium and lens. The type II carbonic anhydrase isoenzyme is present in the ciliary epithelium.(53). Carbonic anhydrase inhibitors interferes with the function of enzyme and reduces aqueous production. The enzyme carbonic anhydrase (CA) catalyzes the following reaction:
CO2 + OH-HCO3
-Systemic carbonic anhydrase inhibitors are: 1. Acetazolamide
2. Methazolamide
Acetazolamide :
22
Effective Introcular pressure lowering is achieved by maximum dose which can be given in 250mg four times a day and 500 mg twice day. In pediatric patients dose according to body weight is 5- 10mg/kg six hourly. Intraocular pressure drops in 1–2 hours after oral administration and reaches minimum in 2–4 hours following which returns to baseline in 4–12 hours. In sustained release preparations, Intraocular pressure drops in 2-4 hours, reaches minimum in 8 hours following which reaches baseline in 12-24 hours. It is also available in 500 mg ampoule which can be dissolved in 5- 10ml of distilled water and can be used intravenously or
intramuscularly. Acetazolamide has high plasma protein binding and its half-life is 4 hours. It is actively secreted by renal tubules and passively reasorbed by non-ionic diffusion.
It is used in conditions wherein there is an acute elevation of intraocular pressure when topical medications are not effective due to the high pressure causing iris ischemia and non-absorption of topical medications and also for short term management of raised intraocular pressures as seen following routine cataract surgeries, trauma etc.
Methazolamide:
Methazolamide is available in 25 and 50 mg tablets and is less effective than
23
24 hours. Methazolamide less likely to produce urolithiasis than acetazolamide because it causes less suppression of urinary citrate and less alkalinisation of urine (54). Hence preferred in patients with a history of renal stones.
Side effects of systemic carbonic anhydrase inhibitors : Paresthesias of fingers, toes, circumoral region
Electrolyte disturbances such as metabolic acidosis , hypokalemia
Gastrointestinal effects are Metallic taste , Nausea , vomiting , abdominal cramps and urolithiasis.
Central nervous system effects are Fatigue, malaise , Confusion , Depression , Drowsiness , Headache
Agranulocytosis
Rash , Stevens-Johnson syndrome Myopic shift
Contraindicated in patients with hypersensitivity , adrenal insufficiency , hepatic cirrhosis, renal failure, diabetic ketoacidosis , hypokalemia , hyponatremia, pregnancy and lactation.
Topical carbonic anhydrase inhibitors :
24
Dorzolamide (2%) :
Dorzolamide has both a free sulfonamide group and second amine group, which is responsible for good corneal penetration due to lipid and aqueous solubility. It effectively inhibits isoenzymes II and IV, with a weaker effect on isoenzyme I. A small amount of drug is metabolized by the liver to the des-ethyl form and it is excreted by kidneys. Des – ethyl form has inhibitory effect on isoenzyme
I. (55.). Dorzolamide and its metabolite are largely bound to RBC cholinesterase and are not present to any extent as free molecules in plasma hence systemic effects are minimal, but RBC carbonic anhydrase decreased to 21% of normal levels (56). An 8 hourly dose is recommended for monotherapy and 12 hourly dose for
adjunctive therapy. It is available as 2% solution with peak effect seen in 3 hours. It has an additive effect with both aqueous suppressants such as timolol and aqueous outflow enhancing agents such as pilocarpine and prostaglandin analogues . (57)(58) It is well tolerated in children less than 6 years of age compared to oral acetazolamide.
Brinzolamide (1%):
It is lipophillic drug with good corneal permeability and is available as 1%
25
but brinzolamide had significantly less ocular burning and stinging compared to dorzolamide according to Michaud et al (96).
Ocular side effects of topical carbonic anhydrase inhibitors: Stinging , allergy
Dryness , superficial punctate keratopathy Induced myopia
Systemic side effects of topical carbonic anhydrase inhibitors: Metallic taste, gastrointestinal distress,
Urticaria , neutropenia,
Headache, , dizziness, paresthesias Steven Johnson syndrome
Topical carbonic anhydrase inhibitors are contraindicated during pregnancy and lactation. (17)
Adrenergic agonists :
Adrenergic agonists can be classified as non-selective which acts on alpha and beta receptors and selective which acts only on alpha receptors . There are three alpha one adrenergic receptors (α1A, α1B , α1D) and three alpha two adrenoreceptors (α2A , α2B , α2D) . Of which α1A and α2A are found in ocular tissuses.
26
1. Epinephrine 2. Dipivefrin 3. Norepinephrine
Epinephrine (0.5%, 1% or 2%):
It reduces intraocular pressure by decreasing aqueous production via early β
adrenergic mediated effect and increases aqueous outflow facility both conventional and uveoscleral via late α adrenergic mediated effect. It is available as epinephrine
hydrochloride , epinephrine borate, epinephrine bitartarate. The intraocular pressure lowering effect peaks in 2 to 6 hours and returns to baseline in 12 – 24 hours.
Dipivefrine (0.1%):
It is a prodrug and is converted to epinephrine by esterease enzyme in cornea . Dipivefrine has limited sympathomimetic activity. Two molecules of pivalic acid is added to the parent molecule hence dipivefrin is synthetic analogue of epinephrine. And hence it increases lipid solubility and ocular penetration in comparison with epinephrine. It is also converted to other metabolites but action of other metabolites is unknown. Its concentration is 0.1% and intraocular pressure
27
Norepinephrine :
It increases trabecular outflow a through alpha adrenergic mediated effect and thus decreases intraocular pressure. The concentration of epinephrine as topical
administration is 2–4%. However its clinicial effectiveness in humans is limited due to limited intraocular penetration.
The ocular side effects are
Hyperemia , Blepharoconjunctivitis ,Skin blanching, Adrenochrome deposits ,Madarosis, Ocular pemphigoid, Corneal Epithelial and endothelial toxicity, l
acrimal stones, cystoids macular edema and iridocyclitis.
The systemic side effects are
Headache, Tachycardia ,Premature ventricular contractions , anxiety , tremor, Increased blood pressure ,
Cerebrovascular accident and Myocardial infarction.
Alpha1-Adrenergic agonists : Phenylephrine :
Phenylephrine hydrochloride lacks hydroxyl group on 4 position of benzene ring. It is a potent sympathomimetic agent and acts on alpha1-adrenergic receptors .
28
dilatation of pupil inorder break posterior synechiae. It prevents formation of iris cysts hence was mostly used in combination with echothiophate. It can cause an increase in Intraocular pressure in patients with pigment dispersion syndrome due to release of iris pigment. (61)
Alpha 2 –adrenergic agonists 1. Clonidine
2. Apraclonidine 3. Brimonidine
Clonidine (0.125%,0.05%)
Clonidine is the first alpha 2-adrenergic agonis acts both centrally and peripherally which inhibits norepinephrine release and decreases sympathetic outflow system. It used as antihypertensive agent. The topical concentration of clonidine are 0.125% and 0.05%, clonidine which reduces intraocular pressure for 6–8hrs . The 0.125% concentration of clonidine is slightly less effective in reducing intraocular pressure than 2% pilocarpine.( 62). Topical clonidine is generally well tolerated except for minor drowsiness and dryness of the mouth.
Apraclonidine (0.5%)
29
comparison with clonidine. Its reduces intraocular pressure by reducing episcleral venous pressure and increases trabecular outflow.
Brimonidine : (0.2%, 0.15 and 0.1%)
Brimonidine is a selective alpha 2-adrenergic agonist. It reduces intraocular pressure by by reducing aqueous formation and by increasing uveoscleral outflow(49). It has neuroprotective effect in addition. (50) which has been demonstrated objectively in rabbits only and not in human eyes . It is the most commonly used antiglaucooma medication in this group due to its low side effect profile . It was first marketed as a 0.2% concentration solution. Other concentration available are 0.15% and even 0.1% solution. Brimonidine is contraindicated in children due to cardiovascular instability, lethargy and sleepiness. The systemic absorption of brimonidine occurs with peak plasma concentration within 1-4 hours. It is metabolised by liver and eliminated by urinary excretion . It is also available in fixed combination with timolol. It has an additive effect with beta blockers, carbonic anhydrase inhibitors and miotics. As monotherapy it is used as thrice daily dosing and as twice daily if used in fixed combinations.
Systemic side effects of alpha 2 agonists:
Dy mouth, fatigue, drowsiness,
headache, hypotension and bradycardia .
30
Ocular side effects of alpha 2 agonists:
Itching , blurred vision, burning,
follicular conjunctival response, hyperaemia and photophobia.
Alpha 2 adrenergic agonists are contraindicated in infants and children as bradycardia, hypotension, hypothermia , hypotonia , CNS depression and apnea has been
reported.(17)
Monotherapy vs combination therapy:
With monotherapy it is often insufficient to achieve the target intraocular pressure. Combination of drugs is hence often required.
With administration of multiple medications, administration of a second drug within 5 minutes of an initial medication may cause substantial reductions in the concentration of the first drug because of washout of the first drug, thereby potentially reducing overall Intraocular pressure-lowering efficacy (63).
Additionally, exposure to more than one preserved topical medication (and therefore a greater cumulative exposure to irritating preservatives) may increase ocular
symptoms (64)(65) and may predispose patients to discontinue their therapy.
31
medications. Recently fixed combination Carbonic anhydrase inhibitors and alpha2 agonists are available in the market.
The various Fixed-combination medications available include :
1. Timolol with Latanoprost 2. Timolol with Bimataprost 3. Timolol with Travaprost 4. Timolol with Brimonidine 5. Timolol with Dorzolamide 6. Timolol with pilocarpine
Fixed combination dugs have the advantages of ease of administration, increased tolerability, reduction of ocular symptoms through reduced cumulative exposure to preservatives, reduced cost , and very importantly compliance. (92).
Amount of Intraocular pressure reduction (%) achieved by various classes of Antiglaucoma medications :
Among Intraocular pressure -lowering monotherapy treatments, prostaglandin analogs generally provide the greatest Intraocular pressure-lowering efficacy
32
The % reduction is as below:
Prostaglandin analogs (31%–33%) (51)
β-blockers (23%–27%)
α2-adrenergic agonist (25%)
Carbonic anhydrase inhibitors (17%–22%) (51).
Betablocker with prostaglandin (33%)
Carbonic anhydrase inhibitor with Betablocker (26%)
Alpha 2 agonist and Beta blocker (22%)
The 24 hour efficacy of various classes of antiglaucoma medications:
Prostaglandins:
Stewart et al in a metaanalysis found that throughout the circadian cycle , prostaglandin efficacy as monotherapy is fairly uniform ( 67). The peak 24 hour efficacy of prostaglandin is usually 8–12 h after administration (68). With evening dose its efficacy is greater during daytime.(69).
33
Beta Blocker:
The mean circadian efficacy of timolol ranges from 10% to 25% in patients with POAG (71). In another study by Orzalesi et al. (68) established that the nocturnal efficacy was only about half the daytime efficacy. This suggests that there is greater daytime intraocular pressure reduction and a smaller, but still significant, nighttime reduction .(70) ).Beta blockers have decreased nocturnal efficacy which may be explained by normally occurring reduction in endogenous circulating catecholamines at night (72).
Topical carbonic anhydrase inhibitors:
Orzalesi et al. (68) in 24 hour efficacy study compared dorzolamide, timolol and latanoprost and found that mean intraocular pressure was significantly lower with latanoprost whereas there was no significant difference between dorzolamide and timolol . Dorzolamide is as effective as latanoprost in reducing nighttime intraocular pressure (10:00 pm to 6:00 am) and less effective than timolol or latanoprost during daytime (6:00 am to 8:00 pm) (70) .
34
Alpha2 agonists ( Brimonidine ) :
The mean 24 hour Intraocular pressure reduction of brimonidine 0.2 % used twice daily was 14 % to 19%. (67) (73)(74)The 24-h efficacy of brimonidine was similar to dorzolamide at daytime (8:00 am to 8:00 pm) and to timolol at nighttime (10:00 pm to 6:00 am).(70)
In a study by Orzalesi et al showed that brimonidine has minimal effect during late night time and early morning (between 3:00am and 6:00 am) but there is no
significant difference from baseline. (75) .
A 24 hour study peformed by Liu et al. showed that brimonidine given three-times daily reduced the mean daytime Intraocular pressure by 12.5% but had no Intraocular pressure-lowering effect during night which was done in a sleep laboratory with 15 patients of open-angle glaucoma or Ocular hypertension, (76)
35
A study conducted by Stewart et al comparing Brimonidine 0.2% versus dorzolamide 2% each given three times daily showed similar mean Intraocular pressure reduction at both trough and peak efficacy time points.(74)
The 24 hour efficacy of combination therapy :
Combination of prostaglandin analogs and with beta blockers:
1. Combination of latanoprost with Timolol :
A meta-analysis on 24-hour efficacy of Intraocular pressure -lowering medications reported that a combination of latanoprost with timolol showed an average reduction of 33% (67) A study conducted by Larsson et al in 20 patients with ocular
hypertension with 1month follow-up showed that latanoprost with timolol was more efficacious than placebo both at daytime (10:00 am to 10:00 pm) and at nighttime (5.6 and 3.1 mmHg, respectively). (78)
A 24 hour efficacy study which compared (79) timolol used twice daily and combination of latanoprost with timolol dosed in the evening in 34 patients with Primary open angle glaucoma. It showed mean intraocular pressure being reduced from 25 mmHg at baseline to16.4 and 19.3 mmHg in patients with latanoprost and timolol combination and timolol alone.
A 2 month cross over trial conducted in 37 patients with primary open angle glaucoma compared the 24 hour efficacy of Latanoprost with timolol combination with latanoprost alone (80). This study reported that baseline IOP was
36
timolol combination and Latanoprost alone. Also mean and individual time point Intraocular pressure reduction were significantly lower with Latanoprost and timolol combination.
2. Combination of Travoprost with Timolol
In a study comparing 24 hour efficacy of morning versus evening administration of Travaprost with timolol showed significant Intraocular pressure reduction at all time points. In comparison to morning dosing, the evening dosing of Travaprost with timolol showed significant 24 hour intraocular pressure reduction (18.4 vs. 19.2 mmHg) and reduced 24-hr fluctuation (3.8 vs. 5.1 mmHg). (81)
3. Combination of Bimatoprost with Timolol
A 24 hour efficacy study by Konstas et al showed that morning and evening dosing of Bimataprost with timolol was efficacious than bimataprost monotherapy at all time points. In comparison with mean 24 hour intraocular pressure reduction with morning dosing and the evening dosing of bimataprost with timolol (10.2 and 9.8mmHg with P= 0.005), evening dose is more efficacious than morning dose (82)
Another study comparing 24 hour efficacy of combination drug Bimataprost with timolol and Latanoprost monotherapy reported that the mean untreated 24-h IOP was 31.1 mmHg and at the end of 3-months the mean 24-hour intraocular pressure
37
Combinations of Carbonic Anhydrase Inhibitors with Beta-Blockers Combination of Dorzolamide and Timolol :
The 24 hour efficacy of average Intraocular pressure reduction reported with Dorolamide and timolol is 26% based on a metanalysis (67)
A study conducted by Feldman et al compared the 24 hour efficacy of dorzolamide with timolol combination and timolol alone in 232 patients with open-angle glaucoma or OHT . This showed that Dorzolamide with timolol combination significantly
reduced Intraocular pressure at all time points and also resulted in significant daytime reduction of intraocular pressure in comparison with timolol alone (84)
Eren et al. compared 24 hour efficacy of combination Dorzolamide with timolol and Latanoprost with timolol in 33 Primary open angle glaucoma patients which reported that Latanoprost with timolol was more efficacious than Dorzolamide with timolol in lowering the mean 24-h Intraocular pressure (16.3 vs. 17.3 mmHg) and the peak 24-h Intraocular pressure (18.5 vs. 19.9 mmHg).(85)
Another study which compared 24-hour efficacy of Dorzolamide with timolol to that of Timolol with brimonidine showed that Dorzolamide with timolol was more
effective and the difference (mean -0.7 mmHg; 95% CI -1.0 to -0.3;P\0.001) reached statistical significance. (86)
Combination of Brinzolamide and Timolol :
One study showing 24hour efficacy of brinzolamide/timolol and
38
brimonidine/timolol fixed combination (18.0 mmHg) also brinzolamide/timolol fixed combination provided superior Intraocular pressure reduction in late afternoon and in night (6:00 pm till 2:00 am). (87)
Combinations of Carbonic Anhydrase Inhibitors with a Prostaglandin : Dorzolamide/Brinzolamide and Latanoprost :
Three studies have reported the 24-h efficacy of dorzolamide when added to latanoprost found that when dorzolamide was added to latanoprost has an additive oculohypotensive effect than monotherapy.(88) (89).
A study by Nakamura et al.(90) compared the adjunctive 24-h efficacy of
dorzolamide versus that of brinzolamide when added to latanoprost. It showed no significant difference in efficacy between the two drugs brinzolamide versus dorzolamide respectively.
Combination of an Alpha-2 Agonist and a Beta-Blocker: Brimonidine and Timolol
39
STUDIES ON FIXED COMBINATION BRINZOLAMIDE 1% AND BRIMONIDINE 0.2% :
Fixed combination brinzolamide and brimonidine being only recently available in the market, there are only few studies evaluating this fixed combination
Nguyen et al (16) conducted a randomizied controlled trial (N= 690) fixed component Brinzolamide / Brimonidine (BBFC) with that of its components brinzolamide and brimonidine . At the 3-month primary endpoint, mean
intraocularpressure of the BBFC group was significantly lower than that of either the brinzolamide group or the brimonidine group (P ≤ 0.005) across all time points. A
total of 143 patients experienced at least 1 treatment-related adverse event (AE; BBFC group, n = 58, 26.2%; brinzolamide group, n = 44, 18.8%; brimonidine group, n = 41, 17.4%), the majority of which were ocular Adverse events such as blurred vision,eye irritation,pain ,pruritus,conjunctivitis,conjunctival hyperaemia,dry eye .
40
adverse events (n = 7 in each group), none of which was related to treatment. No new or increased risks were identified with use of BBFC relative to either monotherapy. This study showed that, after six months of treatment, the safety profile of BBFC was similar to that of its individual components and its Intraocular pressure-lowering activity was similar to its efficacy at three months, when it was superior to both brinzolamide 1% alone and brimonidine 0.2% alone.
Another study by Katz et al (15) enrolled a total of 660 patients. At 3 months, the mean Intraocular pressure of the brinzolamide-brimonidine group (16.3-19.8mmHg)
was significantly lower than that of either the brinzolamide group (19.3-20.9 mm Hg;
P≤0.002) or the brimonidine group (17.9-22.5mmHg; P<.001) across all time points.
One of 10 serious adverse events (chest pain, brinzolamide group) was judged as
treatment related. A total of 129 patients experienced at least 1 treatment-related
adverse effect (brinzolamide-brimonidine, 22.9%; brinzolamide, 18.6%; and
brimonidine, 17.3%; P=.31), most of which were ocular. This registrational study
provides evidence that the fixed combination of brinzolamide, 1%, and brimonidine,
0.2%, can safely and effectively lower Intraocular pressure in patients with open-angle
glaucoma or ocular hypertension, showing significantly superior Intraocular
pressure-lowering activity compared with either brinzolamideor brimonidine monotherapy
41
This study by Realini et al (94) enrolled a total of 1350 patients (BBFC,N=437;
brinzolamide, n=458; brimonidine,n=455). Baseline mean Intraocualar pressure levels
were similar among the three treatment groups. At 3 months, mean Intraocular
pressure of the BBFC group was significantly lower than that of either monotherapy
group (P<0.0001) at all the four time points. A total of 272 patients (20.1%)
experienced at least one treatment-related Adverse effects (BBFC, 24.6%;
brinzolamide, 18.7%; brimonidine, 17.4%), the majority of which were ocular
Adverse effect. One serious Adverse effect, moderate intensity chest pain, was
considered related to brinzolamide treatment and resulted in study discontinuation.
This analysis strengthens the conclusions drawn from the two individual phase 3
studies showing that, in patients with open-angle glaucoma or ocular hypertension,
BBFC had significantly superior Intraocular pressure-lowering activity compared
with either brinzolamide or brimonidine alone and a safety profile consistent with that
of its individual components
This study by Aung et al (14) showed that Baseline diurnal Intraocular pressure was similar among groups (mean ± standard deviation: BBFC, 25.9 ± 0.19 mmHg;
42
The most common adverse drug reactions were ocular side effects, including
hyperemia, blurred vision, allergic-type reactions, and discomfort. The incidence of hyperemia of the eye was slightly lower with brinzolamide than with BBFC and brimonidine, whereas blurred vision and ocular discomfort were slightly more common with BBFC than with brinzolamide or brimonidine. Brinzolamide 1% and brimonidine 0.2% fixed combination administered BID had a significantly greater Intraocular pressure -lowering effect than either brinzolamide or brimonidine alone and displayed a safety profile consistent with its individual components
Gandolfi et al (6) showed that The mean diurnal Intraocular pressure change from baseline with BBFC (least squares mean ± standard error -8.5 ± 0.16 mmHg) was noninferior to that with BRINZ +BRIM (–8.3 ± 0.16 mmHg; mean difference -0.1 mmHg; 95% CI -0.5 to 0.2 mmHg.The most common ocular adverse drug reactions were hyperemia of the eye (reported as ocular or conjunctival hyperemia), visual disturbances, ocular allergic reactions, and ocular discomfort .Common systemic adverse drug reactions included dysgeusia, oral dryness, and fatigue/drowsiness. Brinzolamide 1%/brimonidine 0.2% fixed combination was as well tolerated and effective as concomitant therapy with its components. BBFC reduces treatment burden in patients who require multiple Intraocular pressure-lowering medications .
Greater reductions in mean Intraocular pressure with Brinzolamide 1% with
43
brinzolamide, and 3.0–6.3 mmHg with brimonidine).(93) Thus, the therapeutic benefit of Brinzolamide 1% with brimonidine 0.2% occurs shortly after initial administration (ie, within the first 2 weeks) and continues for up to 6 months.
Stefano et al (92) conducted a phase 3 multicenter 6-month trial in which he evaluated the efficacy of fixed-combination brinzolamide 1%/brimonidine 0.2% (BBFC) versus concomitant administration of brinzolamide 1% plus brimonidine 0.2% . 890 patients were randomly allocated to two groups in this study .The mean diurnal IOP change from baseline with fixed combination brinzolamide and
brimonidine (−8.5 ± 0.16 mmHg)was non inferior to that with concomitant
administration of brinzolamide and brimonidine (–8.3 ± 0.16 mmHg) with a mean difference −0.1 mmHg; 95% CI −0.5 to 0.2 mmHg. Also the most common ocular
side effects reported were conjunctival hyperemia , ocular allergic reactions, and ocular discomfort. Some systemic adverse drug reactions included dysgeusia, oral dryness, and drowsiness.
44
MATERIALS AND METHODS:
This is a hospital based cross sectional observational study conducted in the Department of Ophthalmology, Christian Medical College, Vellore.
Patients who visited the General Outpatient Department (OPD) of the Department of Ophthalmology, Christian Medical College, Vellore who fulfilled the eligibility
criteria were included in the study . An information sheet describing the aim and methodology of the study were given to all the participants. The information sheet was available in English and Tamil. The content of the information sheet was read out and explained to illiterate patients. Following this, an informed consent was obtained from each participant in a language understood by him/her. After obtaining an informed consent, a complete ophthalmic & systemic history and ophthalmological
examination was performed on all patients. A medical history from each subject was obtained, including a list of all systemic medications. The examination included subjective and objective refraction, best corrected Snellen’s visual acuity, slit lamp
examination, intraocular pressure measurement by Goldman applanation tonometry, gonioscopy and dilated fundus examination including stereoscopic biomicroscopic examination of the optic disc with 90 D lens. Field testing was done with Humphrey Field Analyser , Central Corneal Thickness measurements was done as a part of the routine management of glaucoma not specifically as a part of the study design.
45
Inclusion criteria:
1. Above the age of 18
2. Patients newly diagnosed to have Primary open angle glaucoma,
Pseudoexfoliation glaucoma, pigmentary glaucoma or Ocular hypertension with intial intraocular pressure office hour ≥21mmHg .
3. Open angles on gonioscopy
Exclusion criteria:
1. Intraocular pressure more than 36 mmHg at diagnosis or during treatment
wash out
2. Cup-to-disc ratio 0.80 (horizontal or vertical measurement) in either eye 3. History of any antiglaucoma medications in the past 6 weeks.
4. History of using steroid eye drops within the past 1 month
5. Any patient with more than 1 recording of IOP less than 21 mm Hg out of the 3 IOP recordings at 8am , 12pm and 4pm during baseline visit.
6. History of intraocular surgery including laser procedure within 3 months of
enrollment in the study 7. Ocular surface disorders 8. Pregnant and lactating women
9. History or evidence of ocular inflammation or infection within the last 3 months
46
11. Ocular trauma any time in the past
12. Active or prior severe, unstable, or uncontrolled cardiovascular, cerebrovascular, hepatic, or renal disease that would prevent safe administration of topical a-adrenergic agonists or carbonic anhydrase inhibitors, according to the investigator
13. Patients on oral Beta blockers
14. Current or anticipated treatment with any psychotropic drugs that augment adrenergic response (e.g., desipramine, amitriptyline)
15. History of Hypersensitivity to a-adrenergic agonist drugs (e.g., brimonidine),
topical or oral Carbonic anhydrase inhibitor (brinzolamide), sulphonamide derivatives, or any components of the study medication
16. Diabetic patients on Insulin therapy
Methodology :
Patients eligible for the study were examined at baseline, 2weeks ± 2 days and at 4weeks ± 2 days. At each visit all patients underwent routine ophthalmological examination which includes Best corrected visual acuity, slit lamp examination and fundus examination with 90 D condensing lens. Patients were evaluated for any conjunctival hyperemia, discharge, papillae or follicles, corneal Punctate epithelial erosions, anterior chamber flare or cells followed by intraocular pressure
47
At all visits intra ocular pressure were measured at 8 am (±1 hour), 12 pm (±1 hour), and 4pm (±1 hour). At 1 month visit patients were admitted for 24 hour phasing and IOP was measured at 8am (±1 hour),12pm (±1 hour) , 4pm (±1 hour),8pm(±1
hour),12am(±1hour) and 4 am (±1hour)
After the IOP measurement at the baseline visit , patients were started on fixed combination brinzolamide (1%) and brimonidine (0.2%) (Simbrinza ) twice a day. Patients were instructed to instill eye drops preferably at the same time every day (8 a.m. and 8 p.m.)
Patients were then reviewed at 2 weeks to check Intraocular pressureand to assess for any ocular and systemic side effects as below
Ocular surface adverse effects :
Hyperemia grading – Redness: None/ Mild / Moderate / Severe (Grading will be done by standard clinical photograph) (40) (pg 115 )
Burning : Mild** / Moderate** / Severe**
Watering: Mild / Moderate / Severe
Pain : Mild / Moderate / Severe
Pricking/foreign body sensation/irritation: Mild / Moderate / Severe
Sensation of dryness: Mild / Moderate / Severe
Itching, Swelling around the eyes: Mild / Moderate / Severe
48
**Mild : did not interfere with patients activities of daily life
**Moderate: interfered to some extent with patients activities of daily life, but not severe enough to consider discontinuation of the drug
**Severe: Interfered significantly with patients activities of daily life i.e severe enough to consider discontinuation of the drug or actually lead to the patient to discontinuing the drug
Systemic side effects:
Drowsiness, somnolence, dryness of mouth, altered taste sensations, fatigue
Any patient with ocular side effects which were graded as severe, as well as patients with any systemic side effects were taken out of the study and started on other anti-glaucoma medications as per routine standard of care. Also any patient who presented with these side effects prior to the 2 week scheduled visit were taken out of the study and started on other anti-glaucoma medications as per routine standard of care
Patients were asked to continue the drops and were subsequently seen at 4 weeks ± 2 days .Similar to the previous visits patient underwent routine ophthalmological examination which includes Best corrected visual acuity, slit lamp examination and fundus examination with 90D condensing lens. Patients were evaluated for any conjunctival hyperemia, discharge, papillae or follicles, corneal Punctate epithelial erosions, anterior chamber flare or cells followed by intraocular pressure
49
In addition to the office hours IOP in order to obtain the diurnal IOP profile, patients were admitted for phasing and additional IOP measurement were obtained at 8pm(±1 hour),12am(±1hour) and 4 am (±1hour).
At the end of the study period patients who had no side effects were continued on Simbrinza if the target IOP was achieved and the patient could affird the medications. If the target IOP was not achieved or the patient could not afford long term
50
FLOW CHART:
Identification of individuals with newly diagnosed open angle glaucoma not any antiglaucoma medications fulfilling the criteria from general Outpatient ,department of ophthalmology
Informed consent and recruitment
Questionnaire, routine ophthalmological examination and relevant investigations.
Baseline Intraocular pressure will be measured at 8 am (±1hr), 12 pm(±1 hr), 4pm (±1hr)
Patients will then be started on fixed combination of brinzolamide1% with brimonidine 0.2% twice a day
At 4 weeks , questionanaire for side effects , routine ophthalmological examination, Intraocular pressure will be measured at 8am (±1hr), 12pm(±1 hr ) , 4pm (±1hr) , 8pm (±1hr), 12 am (±1hr ) and 4 am (±1hr)
51
RESULTS:
The study was conducted between March 2017 to August 2017.
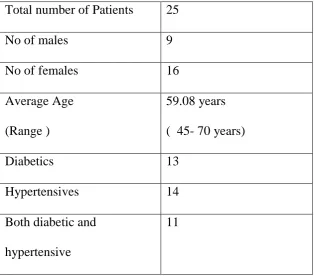
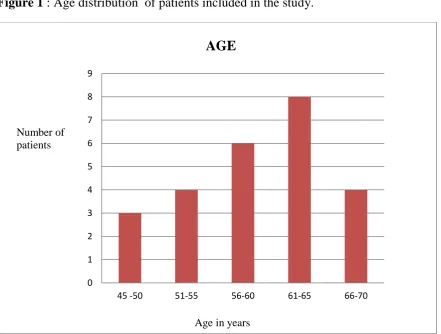
[image:59.595.67.382.421.697.2]25 patients were recruited into the study of whom 9 were males and 16 females (Table 1). Most of the patients were in the sixth or seventh decade. (Figure 2 ).Out of the 25 patients 13 were diabetics, 14 were hypertensives and 11 were both diabetic and hypertensive. None of the patients had heart block, bradycardia, cardiac failure, renal or liver diseases which are contraindications for use of brimonidine / alpha agonists. Of the 14 hypertensives in the study none of them were on beta blockers. . Also none of 13 diabetics in our study were on insulin.
Table 1: Demographic data
Total number of Patients 25
No of males 9
No of females 16
Average Age (Range )
59.08 years ( 45- 70 years)
Diabetics 13
Hypertensives 14
Both diabetic and hypertensive
52
Figure 1 : Age distribution of patients included in the study.
0 1 2 3 4 5 6 7 8 9
45 -50 51-55 56-60 61-65 66-70
AGE
Number of patients
53
Ocular diagnosis - Type of glaucoma among the participants
[image:61.595.66.534.195.348.2]Details of the distribution of type of glaucoma are given in (Table 2. and Figure2):
Table 2: Distribution of type of glaucoma among the participants
Type of glaucoma Frequency Percentage
Ocular hypertension 21 84%
Primary open angle glaucoma
4 16%
[image:61.595.77.526.413.718.2]Pseudoexfoliation glaucoma 0 0%
Figure 2 : Distribution of type of glaucoma among the study patients
Majority of the participants were ocular hypertensives.
84%
16%
OCULAR DIAGNOSIS
OCULAR HYPERTENSION
54
Pretreatment baseline intraocular pressure values (office hours ):
[image:62.595.67.430.292.525.2]The average pre-treatment baseline IOP (average of the three IOP recordings at 8am, 12pm and 4pm)was 25.04± 2.55mmHg. Details of the IOP at each time – 8am, 12pm and 4pm are given in ( Table 3)
Table 3: Pre treatment baseline intraocular pressure (office hours)
Time Pre treatment IOP (Mean ± SD)
8am 25.48± 2.90 mm Hg
12pm 24.96 ± 2.79 mm Hg
4pm 24.68 ± 3.06 mm Hg
55
Post -treatment intraocular pressure at 1 month (office hours):
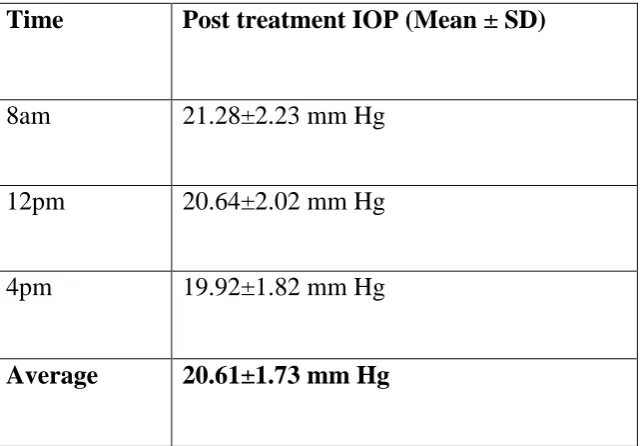
[image:63.595.69.390.290.513.2]The average post -treatment baseline IOP (average of the three IOP recordings at 8am, 12pm and 4pm) at 1 month was 20.61 ± 1.73 mm Hg. Details of the IOP at each time – 8am. 12pm and 4pm are given in ( Table 4 ).
Table 4: Post- treatment intraocular pressure (office hours)
Time Post treatment IOP (Mean ± SD)
8am 21.28±2.23 mm Hg
12pm 20.64±2.02 mm Hg
4pm 19.92±1.82 mm Hg
56
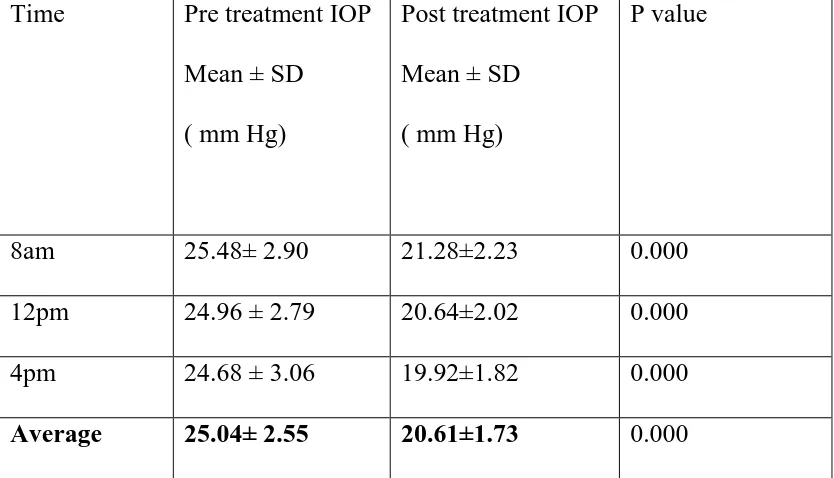
Comparison of pre-treatment and post treatment intraocular pressure (office hours):
The mean pre- treatment IOP was 25.04±2.55mm Hg and post- treatment IOP was 20.61±1.73 mm Hg. There was a 4.43 ± 3.13 mm Hg reduction in IOP which was statistically significant (Table 5).
[image:64.595.67.484.422.661.2]The paired wise comparison between pre-treatment and post-treatment according to time is shown in (table 5, Figure 3 and 4 )
Table 5: Comparison between pre-treatment and post-treatment intraocular pressure (Office hours)
Time Pre treatment IOP Mean ± SD
( mm Hg)
Post treatment IOP Mean ± SD
( mm Hg)
P value
8am 25.48± 2.90 21.28±2.23 0.000
12pm 24.96 ± 2.79 20.64±2.02 0.000
4pm 24.68 ± 3.06 19.92±1.82 0.000
Average 25.04± 2.55 20.61±1.73 0.000
57
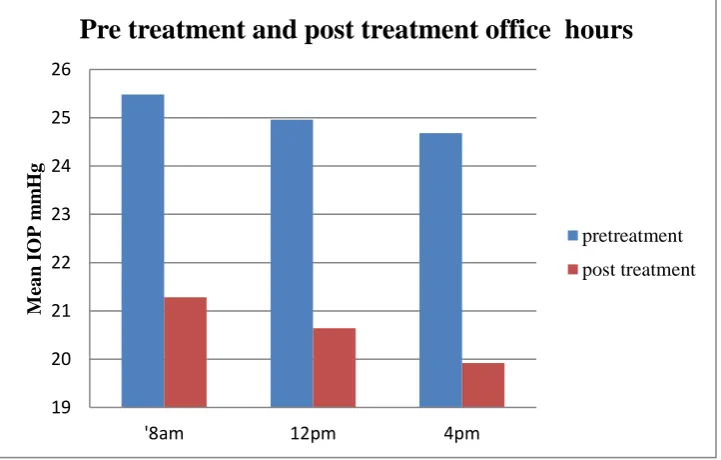
Figure 3: Comparison between pre-treatment and post-treatment IOP according to time (Office hours)
Figure 4: Comparison between pre-treatment and post-treatment IOP according to time (Office hours) in bar graph
Paired wise comparison between pre-treatment and post-treatment in office hours showed significant reduction in IOP at all office time recordings.
19 20 21 22 23 24 25 26
'8am 12pm 4pm
Me an I OP m m Hg
Pre treatment and post treatment office hours
pretreatment post treatment 19 20 21 22 23 24 25 26
'8am 12pm 4pm
M ea n IO P m m H g
Pre treatment and post treatment office hours
pretreatment
[image:65.595.75.436.454.684.2]58
Amount of reduction in IOP pre and post treatment (office hours):
The average reduction in IOP was 4.43 ± 3.13 mm Hg (17.69% , Range 4.76-
[image:66.595.67.427.221.462.2]36.58%). The IOP reductions at various time points were similar as shown in Table 6.
Table 6: Fall in intraocular pressure during office hours
Time Fall in IOP
Mean ± SD ( mm Hg)
Reduction of IOP in percentage
8am 4.2± 2.75 16.48%
12pm 4.32 ±3.33 17.30%
4pm 4.76 ± 3.14 19.28%
Average 4.43± 3.13 17.69%
Though the drop in IOP post-treatment was significant, the amount of reduction in IOP was less as compared to that reported in other studies. Hence we looked at
individual patient data of these 25 patients – there were 4 patients in whom intraocular pressure reduction was ≤2 mm Hg post treatment as compared to pre- treatment. This poor response could most likely be due to non-compliance rather than the patients being non-responders as lack of response to both the components of the fixed
59
was 20.38±1.72 mm Hg. The average drop in intraocular pressure was 5.00±3.54 mm Hg. There was 19.70% (range 9.98 – 36.58 %) reduction in intraocular pressure.
Distribution of amount of IOP reduction among patients:
[image:67.595.73.474.273.572.2]The details of percentage of IOP reduction among patients is given in (figure 5 )
Figure 5 : Distribution of amount of IOP reduction among patients
Most patients had IOP reduction between 11-20% (13 patients ) and 21-30 % (6patients).
0 2 4 6 8 10 12 14
0-10% 11-20% 21-30% 31-40%
Distribution of amount of IOP reduction
% of IOP reduction
% of IOPreduction
60
24 hour IOP profile of patients on fixed dose Brinzolamide 1% and brimonidine 0.2% at 1 month:
Diurnal variation (phasing) of IOP post- treatment:
Patients on treatment at the 1 month follow up were admitted to evaluate the nocturnal and early morning IOP. IOP was checked at 8am, 12pm, 4pm, 8pm, 12am and
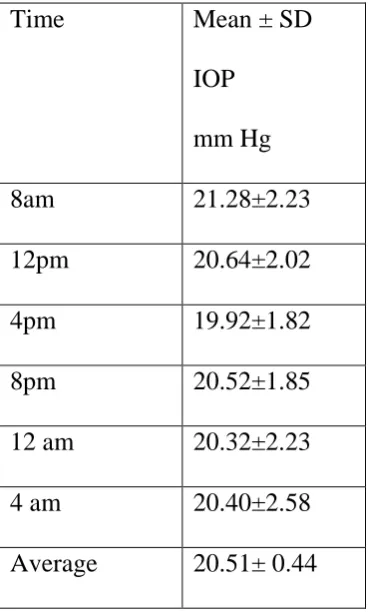
[image:68.595.67.252.320.628.2]4am.The IOP at each of these times is shown in Table 7 and Figure 6.
Table 7: Post- treatment 24 hour intraocular pressure phasing measurement
Time Mean ± SD
IOP mm Hg
8am 21.28±2.23
12pm 20.64±2.02
4pm 19.92±1.82
8pm 20.52±1.85
12 am 20.32±2.23
4 am 20.40±2.58
61
Figure 6 : Diurnal variation of intraocular pressure post treatment
There was a tendency for intraocular pressure to rise from early morning 4am till it peaked at 8am and subsequently decline till late in the afternoon when the intraocular pressure recordings were at the lowest levels at 4pm. There was again a small rise in the intraocular pressure till 8pm after which it plateaued till 4am . Subsequently the intraocular pressure tended to rise to reach the peak at 8am.
Intraocular pressure fluctuated the least during night between 8pm to 4am. However comparison with pre-treatment nocturnal intraocular pressures was not possible as patients were started on treatment after office hour baseline IOP measurements and not admitted for full day phasing prior to treatment. Irrespective of pre-treatment nocturnal intraocular pressure , nocturnal intraocular pressure post- treatment showed good control of intraocular pressure with minimal fluctutation during night- sleep hours. 19 20 21 22 23 24 25 26
'8am 12pm 4pm 8pm 12am 4am
Me an IO P m m H g