A STUDY ON CURRENT ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF TYPHOIDAL SALMONELLAE CAUSING ENTERIC
FEVER IN SCHOOL GOING CHILDREN AND YOUNG ADULTS
Dissertation submitted for
M.D. MICROBIOLOGY BRANCH – 1V
DEGREE EXAMINATION
THE TAMILNADU DR.M.G.R.MEDICAL UNIVERSITY
CHENNAI – 600 032
TAMILNADU
CERTIFICATE
This is to certify that this dissertation titled “A STUDY ON CURRENT ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF TYPHOIDAL SALMONELLAE CAUSING ENTERIC FEVER IN SCHOOL GOING CHILDREN AND YOUNG ADULTS ” is a bonafide record of work done by Dr. ANITHA.M, during the period of April 2016 to March 2017 under the
guidance of Prof.Dr.MANGALA ADISESH, M.D., Professor of Microbiology,
Institute of Microbiology , Madras Medical College and Rajiv Gandhi
Government General Hospital, Chennai - 600003, in partial fulfillment of the
requirement of M.D. MICROBIOLOGY Degree Examination of The Tamilnadu
Dr.M.G.R. Medical University to be held in May 2018.
Dr.R.NARAYANA BABU, MD.,DCH Dr.ROSY VENNILA., M.D.,
Dean, Director,
Madras Medical College & Institute of Microbiology, Rajiv Gandhi Government Madras Medical College & General Hospital, Rajiv Gandhi Government Chennai – 600003 General Hospital,
DECLARATION
I, Dr.ANITHA.M, Post Graduate , Institute of Microbiology, Madras
Medical College, solemnly declare that the dissertation titled “A STUDY ON CURRENT ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF TYPHOIDAL SALMONELLAE CAUSING ENTERIC FEVER IN SCHOOL GOING CHILDREN AND YOUNG ADULTS ”is the bonafide work done by me at Institute of Microbiology, Madras Medical College under the
expert guidance and supervision of Prof.Dr. MANGALA ADISESH M.D.,
Professor, Institute of Microbiology, Madras Medical College. The dissertation is
submitted to the Tamil Nadu Dr.M.G.R Medical University towards partial
fulfillment of requirement for the award of M.D., Degree (Branch IV) in
Microbiology.
Place: Chennai
Date: Dr.ANITHA.M
Signature of the Guide
Prof. Dr.MANGALA ADISESH, MD.,
Professor,
Institute of Microbiology
ACKNOWLEDGEMENT
I wish to express my sincere thanks to the Honourable Dean
Dr.R.NARAYANA BABU, MD, D.Ch ., Madras Medical College & RGGGH,
Chennai for permitting me to use the resources of this Institution for my study.
I express my sincere thanks to Dr. ROSY VENNILA , M.D., Director, Institute of Microbiology, Madras Medical College & RGGGH, Chennai.
I feel fortunate and indebted to be under the guidance of Prof.Dr. MANGALA ADISESH , M.D., Institute of Microbiology, for suggesting the topic for my dissertation and for her valuable advice, guidance in preparing and compilation of my work, throughout my study period. She is a source of inspiration in my endeavours.
I specially thank to our Prof.Dr.U.UMADEVI M.D., for her valuable guidance ,and co-ordinating me in doing Molecular workup for my study at Christian Medical College, Vellore.
I extend my sincere thanks to our Professors Dr. S.THASNEEM BANU
M.D., Dr.R.VANAJA M.D., Dr.C.P.RAMANI M.D., for their support,
guidance and valuable advice.
I extend my whole hearted gratitude and special thanks to my co-guide
Dr.R.DEEPA., M.D., Senior Assistant Professor for her expert guidance and support in doing my study.
I express my sincere thanks to our Assistant Professors
Dr.N.RATHNAPRIYA M.D., Dr.K.USHAKRISHNAN M.D.,
Dr.K.G.VENKATESH M.D., Dr.C.S.SRIPRIYA M.D.,
Dr.N.LAKSHMIPRIYA,M.D.D.Ch., Dr. DAVID AGATHA M.D., and
Dr.B.NATESAN M.D., for their support and guidance in my study.
My sincere thanks to Prof.Dr.T.RAVICHANDRAN.,M.D.,D.Ch., Director and Professor , Institute of Child Health and Hospital for Children for his support and guidance. My sincere thanks to Prof.Dr.K.SRINIVASAGALU M.D., former Director and Professor., Institute of Internal Medicine for his guidance during my study period .
I thank Dr. Evangeline Mary, M.D.,M.B.A.,Department of Community Medicine , Govt. Stanley Medical College, Chennai, for guiding me in analyzing the results statistically .
I would like to thank all my colleagues, and all our technicians and staffs in Institute of Microbiology, Madras Medical College for their support and cooperation.
I feel indebted to my parents who had been an everlasting support and encouragement and for their heartful blessings.
I thank my husband Dr. K. Chandrasekaran M.S, for taking great care, support and encouragement without which this work would not have been possible.
I thank all my patients without whom this study would not have been completed.
TABLE OF CONTENTS
SI.
NO TITLE
PAGE No.
1 INTRODUCTION 1
2 AIMS & OBJECTIVES 4
3 REVIEW OF LITERATURE 5
4 MATERIALS & METHODS 50
5 RESULTS 68
6 DISCUSSION 79
7 LIMITATIONS OF THE STUDY 90
7 SUMMARY 91
8 CONCLUSION 93
9 BIBLIOGRAPHY
ANNEXURE-I ABBREVATIONS
ANNEXURE-II CERTIFICATE OF APPROVAL
ANNEXURE-III PROFORMA
ANNEXURE-IV CONSENT FORM
LIST OF TABLES
S.
NO TITLE
PAGE NO.
1 DISTRIBUTION OF PATIENTS IN THE STUDY POPULATION 68
2 AGE GROUP AND SEX DISTRIBUTION IN THE STUDY
POPULATION 69
3 DISTRIBUTION OF PATIENTS BASED ON HOSPITAL ADMISSION 70
4 CARDINAL SYMPTOMS AMONG STUDY POPULATION 70
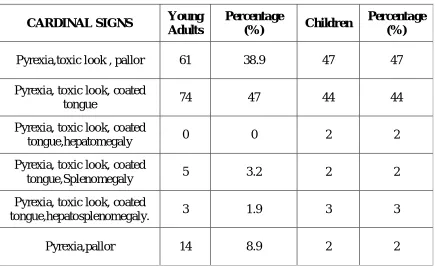
5 CARDINAL SIGNS AMONG STUDY POPULATION 71
6 DISTRIBUTION BASED ON FOOD HABITS 71
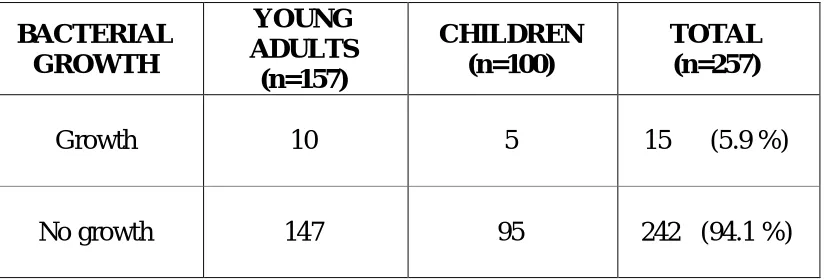
7 DISTRIBUTION OF BACTERIAL GROWTH IN BLOOD CULTURE 72
8 DISTRIBUTION OF PATHOGENS ISOLATED FROM BLOOD
CULTURE 72
9 MONTHWISE DISTRIBUTION OF SALMONELLA ISOLATES 73
10 DISTRIBUTION BASED ON FOOD HABITS AND TYPHOID FEVER 74
11 ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF S.TYPHI AND
S.PARATYPHI A BY DISC DIFFUSION METHOD 74
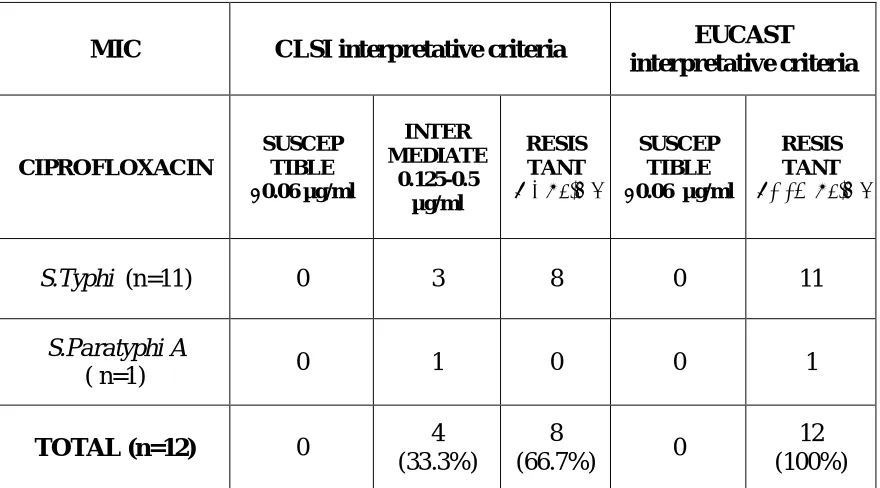
12
DISTRIBUTION OF MIC OF CIPROFLOXACIN BY MICROBROTH DILUTION METHOD –CLSI AND EUCAST INTERPRETATIVE CRITERIA
76
13
ANTIMICROBIAL SUSCEPTIBILITY TESTING PROFILE OF TYPHOIDAL SALMONELLA ISOLATES , MOLECULAR CHARACTERISATION & CLSI AND EUCAST GUIDELINES
77
LIST OF FIGURES
S.
NO TITLE
PAGE NO
1 DISTRIBUTION OF PATIENTS IN THE STUDY
POPULATION 68
2 AGE GROUP AND SEX DISTRIBUTION IN THE
STUDY POPULATION 69
3 SEASONAL DISTRIBUTION OF ENTERIC FEVER 73
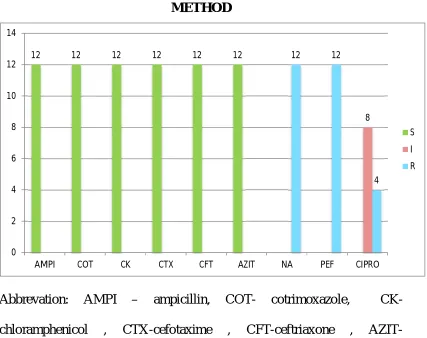
4
ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF S.TYPHI AND S.PARATYPHI A BY DISC DIFFUSION METHOD
CERTIFICATE – II
This is to certify that this dissertation work titled “A STUDY ON CURRENT ANTIMICROBIAL SUSCEPTIBILITY PATTERN OF TYPHOIDAL SALMONELLAE CAUSING ENTERIC FEVER IN SCHOOL GOING CHILDREN AND YOUNG ADULTS” of the candidate DR.ANITHA .M with Registration Number 201514002 for the award
of M.D. in the branch of MICROBIOLOGY. I personally verified the urkund.com website for the purpose of plagiarism Check. I found that the
uploaded thesis file contains from introduction to conclusion pages and result
shows 3 percentage of plagiarism in the dissertation.
1
INTRODUCTION
Enteric fever is a systemic infection caused by the human adapted athogens Salmonella enterica serovar Typhi (S.Typhi). A similar but often less severe disease is caused by S.Paratyphi A, B, and sometimes
S.Paratyphi C. These organisms are the important cause of febrile illness in crowded and impoverished populations with poor sanitation that are exposed to unsafe water and food [1].
Advances in public health and hygiene have led to the virtual disappearance of enteric fever from developed countries , but the disease remains endemic in many developing countries and become a major public health problem [1,2] .The global annual incidence of enteric fever was estimated between 11.9 million and 26.9 million cases , in the year 2010
[3,4]
. Case fatality rate remains 1% ranging between 1,29,000 and 1,61,000 typhoid deaths annually.[4]
The incidence of typhoid and paratyphoid varies geographically , with South-Central and South-East Asia having the highest incidence-typically exceeding 100 cases per 1,00,000 persons-years for typhoid and with lower, variable rates for paratyphoid fever.
2
approximately 2-5% of cases in the absence of appropriate antimicrobial therapy and is strongly dependant on age and sex. [5]
Enteric fever carries a mortality rate of 30 % , if not treated properly, whilst appropriate antimicrobial therapy reduces the mortality rate to as low as 0.5% .[6] Hence, timely treatment with appropriate antimicrobial agents is important for reducing the mortality and morbidity. But the resistance to antimicrobial agents and its changing trends becomes a major challenge in the management of both S.Typhi and S.Paratyphi .
After the first reported outbreak of chloramphenicol resistant S. Typhi
in 1972, there has been a steady increase in the number of multidrug resistant (MDR) strains of S.Typhi-resistance to Ampicillin, Chloramphenicol, Trimethoprim-Sulphamethoxazole - over the next two decades [7,8,9]. But the rate of MDR strains was at a lower range among S.Paratyphi A.[9]
3
leads to emergence of resistance , resulting in clinical failure and delayed treatment response .
The regular revisions of Clinical Laboratory Standards Institute (CLSI) guidelines in the interpretive criteria in 2011 and addition of new fluroquinolones in 2015 and 2016 indicate the urgency and need to revise breakpoints to optimise the dose of fluroquinolones and use of this drug effectively in susceptible clinical isolates[10,11,12]
The most common cause of resistance to Nalidixic acid and decreased susceptibility to fluoroquinolones in serovar Typhi is chromosomal mutation in the quinolone resistance determining region(QRDR) of the DNA gyrase subunit gyrA.[13,14 ]
4
AIMS AND OBJECTIVES
AIM :To determine the current trend of Antimicrobial Susceptibility Pattern of Typhoidal Salmonellae in School going children & Young adults.
OBJECTIVES :
To isolate and identify the Salmonella species causing Enteric fever through blood cultures.
To perform the Antimicrobial susceptibility testing for the isolates.
To do Molecular characterisation of isolates with reduced
5
REVIEW OF LITERATURE
HISTORYBefore the 19th century, typhus and typhoid fever thought to be same disease. Many clinical distinctions were proposed,but none reliably distinguished these syndromes. In 1829 in Paris, P. Ch. A. Louis distinguished typhoid fever from other fevers on the basis of intestinal lymph node and spleen pathology [15]. He described the clinical phenomena of rose spots, intestinal perforation, and hemorrhage.
William Jenner in 1850 settled the dispute between typhus and typhoid fever [16]. He differentiated typhoid fever based on the pathologic evidence of enlargement of the Peyer’s patches and mesenteric lymph nodes. He also noted that prior attacks of typhoid protected against subsequent attacks, this was not the case in fever due to typhus. In 1869, Wilson proposed the term “Enteric fever”, given the anatomic site of infection[17].
6
The genus “Salmonella” was named after Daniel Elmer Salmon, a veterinary pathologist, following the isolation of American-hog-cholera bacillus (S.choleraesuis) in 1885.
In 1896, Pfeiffer and Kalle made the first typhoid vaccine using heat killed organisms [20]. In the same year, Georges Fernand Isidore Widal , a French physician and others demonstrated that convalescent sera from typhoid patients caused the organisms to “stick together in large balls and lose their motility”. He coined the term ‘agglutinin’ to describe this observation .This technique provided a clinical tool for the identification of Salmonella and was used extensively by Kauffman and White during the 1920s to1930s , for classification of over 2000 serotypes. [21].
In 1948, Theodore Woodward et al, reported the successful treatment of Malaysian typhoid patients with Chloromycetin, and thus the modern age of antimicrobial therapy for typhoid fever began.
7
model and powerful genetic techniques available for the study of
S.Typhimurium resulted in wide spread study of this model system of Salmonella pathogenesis.
8
ENTERIC FEVER
Based on the clinical patterns in Human Salmonellosis , Salmonella serptypes can be grouped into Typhoidal Salmonella and Non-typhoidal Salmonella (NTS) . In human infections , the four different clinical manifestations are Enteric fever, Gastroenteritis , Bacteraemia and other Extra-intestinal complications and Chronic carrier state.
Enteric fever is a severe systemic illness characterized by fever and abdominal symptoms that is caused by dissemination of Salmonella Typhi
9
Epidemiology of Enteric Fever
In contrast to other Salmonella serotypes,the etiologic agents of Enteric fever -Salmonella Typhi and Salmonella Paratyphi A,B, and C
serotypes –have no known hosts other than humans [26].
Burden of illness :
Enteric fever continues to be a major public health problem, with very high social and economic impact because of hospitalization of patients with acute disease and the complications and loss of income attributable to the duration of clinical illness [25] .
Global Scenario :
In 2000, it was estimated that nearly 21.7 million illnesses caused by S.Typhi and 5.5 million illnesses caused by S.Paratyphi A, B,and C
annually and an incidence ranging from 25-1000 cases per 1,00,000 population in endemic regions. The crude and laboratory adjusted estimate was 10.8 and 21.7 million cases of typhoid fever. [1] .
10
Oceania, except for Australia and New Zealand and low in the other parts of the world (10 cases/10,00,000) [1] .
The recent analysis of global typhoid fever morbidity , by Buckle et al in 2010 reported , crude and adjusted estimate counting for low sensitivity of blood culture for isolation of bacteria was of 13.5 and 26.9 million cases.
Indian Scenario :
The estimated prevalence of laboratory confirmed typhoid and paratyphoid was 9.7% and 0.9% respectively. Pooled estimates of incidence were 377 (170-801) and 105 (74-148) per 1,00,000 person years respectively. Typhoid fever showed a significant decline in prevalence over a period of time and was detected among clinically suspected febrile cases or during outbreaks. But Paratyphoid fever did not show any trend over time and there was no clear association with the risk factors involved.Children in the age group of 2-4 years old had the high incidence rate [5] .
11
Case definition : [25]
Confirmed case of typhoid fever
A patient with fever (38°C and above) that has lasted for at least three days, with a laboratory-confirmed positive culture (blood, bone marrow, bowel fluid) of S. typhi.
Probable case of typhoid fever
A patient with fever (38°C and above) that has lasted for at least three days, with a positive serodiagnosis or antigen detection test but without S. typhi isolation.
Chronic carrier
Excretion of S. typhi in stools or urine (or repeated positive bile or duodenal string cultures) for longer than one year after the onset of acute typhoid fever. Short-term carriers also exist but their epidemiological role is not as important as that of chronic carriers. Some patients excreting S. typhi
have no history of typhoid fever.
Mode of transmission : [25,26]
12
street vendors. Shellfish taken from contaminated water, and raw fruit and vegetables washed with sewage contaminated water , have been sources of past outbreaks .The highest incidence occurs where water supplies serving large populations are contaminated with faeces.
Epidemiological data suggest that waterborne transmission of S. typhi
usually involves small inocula, whereas foodborne transmission is associated with large inocula and high attack rates over short periods. The inoculum size (103 to 106 ) and the type of vehicle in which the organisms are ingested greatly influence both the attack rate and the incubation period (highly variable 1- 6 weeks) .
Small number of patients (1-5%) with acute infection develop a chronic carrier state,which has allowed the disease to persist during inter-epidemic periods. Levine et al. (1982) studied the role of chronic carriers as a reservoir of infection in Santiago, Chile, where the crude rate of 694 carriers per 1,00,000 inhabitants was found.
Risk factors
Environmental factors
13
Host factors
Typhoidal Salmonella are able to survive at low gastric pH 1.5. Conditions that decrease stomach acidity like antacids, histamine-2 receptor antagonists (H2 blockers), proton pump inhibitors, past infection with Helicobacter pylori, gastrectomy, and achlorhydria facilitate infection [26] .
Genetic polymorphisms in regulatory region of PARK2 and PACGR, protein aggregate that is essential for breaking down the bacterial signalling molecules that dampen the macrophage response , are found disproportionately in persons infected with S.Typhi, and Mycobacterium leprae [22].
14
CLASSIFICATION AND TAXONOMY
Salmonella is a genus of family of Enterobacteriaceae. Existence of multiple Salmonella speices was taxonomically accepted before 1983.Currently, the genus Salmonella is divided into two species: Salmonella enterica and Salmonella bongori, as a result of experiments indicating a high degree of DNA similarity. Salmonella enterica which contains six species (I,II, IIIa,IIIb,IV and VI) and Salmonella bongori, which was formerly subspecies V. Almost all the serotypes of S.enterica
subspecies I are pathogenic for humans, except for rare human infections with subspecies IIIa and IIIb,that were previously designated as genus
Arizonae.
Members of the seven Salmonella subspecies can be serotyped into more than 2500 serotypes (serovars) based on antigenically diverse surface structures : somatic(O) antigens, the carbohydrate component of lipopolysaccharide, the surface Vi antigen (restricted to S.Typhi and S.ParatyphiC), and flagellar (H) antigen [29,30,31].The name usually refers to the location where the Salmonella serotype was first isolated.
According to the current Salmonella nomenclature system in use at the U.S. Centre for Disease Control and Prevention and World Health Organisation laboratories the full taxonomic designation Salmonella enterica subspecies enterica serotype Typhi can be shortened to Salmonella
15
Classification of Salmonella species and subspecies [32]
Subspecies No of serotypes
within subspecies
Salmonella enterica subspecies enterica(I) 1531 Salmonella enterica subspecies salmae(II) 505 Salmonella enterica subspecies arizonae(IIIa) 99 Salmonella enterica subspecies diarizonae(IIIB) 336 Salmonella enterica subspecies houtenae(IV) 73
Salmonella enterica subspecies indica(VI) 13
Salmonella bongori(Formerly subgenera V) 22
Total (genus salmonella) 2579
Biochemical differentiation of subspecies of Salmonella [30]
Subspecies Enterica Salamae Arizonae Diarizonae Houtenae Indica
Dulcitol + + - - - d
ONPG (2h) - - + + - d
Malonate - + + + - -
Gelatinase - + + + + +
Sorbitol + + + + + -
d-Tartarate + - - - - -
Galacturonate - + - + + +
Mucate + + + - (70%) - +
Salicin - - - - + -
Growth in KCN - - - - + -
Beta
glucoronidase d d - + - d
Lysed by phage
O1 + + - + - +
16
In 2003, a total of 2555 serovars were identified in Kaufmann-White scheme. In 2007, since L.Le Minor described most of the presently known serovars, “Kauffmann-White scheme” was redesignated as “White – Kauffmann-Le minor” scheme.[32]
HABITAT
Salmonellae are primarily intestinal pathogens of human and animals including wild birds, domestic pets, and rodents. They are found frequently in sewage, rivers, and in soil in which they do not multiply significantly. Under suitable environmental conditions, they may survive for weeks in waters and for years in soil.
In contrast to other Salmonella serotypes, the etiologic agents of Enteric fever- S.Typhi and S.Paratyphi A,B, and C – have no known host other than humans [30] .
PHENOTYPE Morphology
17
S.Gallinarum- Pullorum which is non-motile. Most serotypes do not ferment lactose, but nearly 1% of organisms are able to ferment lactose. This property of differential metabolism of sugars can be used to distinguish many Salmonella serotypes; Salmonella Typhi is the only organism that does not produce gas on sugar fermentation.[30]
Culture Characters and Growth Requirements [30,31]
Salmonella grow over a wide temperature range from 15–45o C, optimally at 37o C at pH 4-8. Under special conditions they may proliferate at <48 o C and withstand pH<4. In aerobic and anaerobic conditions they grow readily on ordinary media. Most are prototropic,i.e capable of growing on a glucose-ammonium minimal medium , but some strains are auxotrophic and require enrichment with one or more amino acids or vitamins, e.g. cysteine or nicotinamide ; most Typhi strains require tryptophan.
18
Paratyphi A produce relatively small size colonies. ‘Rough’, non-virulent strains (S →R variation) form opaque granular colonies with an irregular surface and indented edge.
Paratyphi B produce large mucoid colonies,or colonies surrounded by thick mucoid ‘slime wall’ made up of ‘M’antigen of Kauffmann ,best developed at low temperature, low humidity and high osmolarity (Anderson and Rogers 1963). The “mucoid wall test” is positive with most strains of Paratyphi B (Kauffmann 1966) [31] .
Most of the strains grow abundantly and give uniform turbidity in liquid medium like peptone water and nutrient broth.On prolonged incubation thin surface pellicle will be seen. ‘ Rough’ (R) variants tends to autoagglutinate , producing granular deposits and sometimes a thick pellicle formation [30].
Various Differential and Selective media are available for the isolation of salmonellae from faeces and other samples that are heavily contaminated with other bacteria [26] .
19
Selective chromogenic medium , such as CHROMagar are more specific than other selective medium. Tetrathionate and Selenite based enrichment broths are often used to facilitate the recovery of low numbers of organisms.
Highly –selective media, such as selenite with brilliant green , reserved in outbreak situations for carrier detection .Wilson & Blair’s brilliant- green bismuth sulphite agar (BBSA) is a valuable isolation medium for S.Typhi.
BIOCHEMICAL ACTIVITIES [30]
Salmonella enterica subspecies enterica can be phenotypically identified by the following biochemical reactions include
1. Fermentation of glucose, maltose, mannitol and sorbitol with the production of acid and gas.(S.Typhi, Gallinarium-anaerogenic).
20 There a few exceptions to these.
Biochemical Reactions Of Salmonella enterica subspecies enterica[31 ,33] BIOCHEMICAL
REACTIONS
INTERPRETATION
Cytochrome oxidase Negative
Catalase Positive
Nitrate reduction Reduces nitrates to nitrites Phenylalanine deaminase
test Fails to deaminate phenylalanine
Hugh Leifsons OF media Shows both oxidative and fermentative pattern Fermentation of glucose Produces acid only or acid and gas
KCN Sensitive
Indole Not produced
Methyl red Positive
Vogue proskaeur Acetoin not produced
Simmons citrate Utilized (except S.Typhi and S.Paratyphi A)
Urease Not produced
Triple sugar iron agar(TSI)
Alkaline/acid with speck of H2S - S.Typhi
Alkaline/acid with gas and no H2S - S.Paratyphi A
Alkaline/acid with plenty of H2S - S.Paratyphi B
Biochemical differences between S.Typhi and S.Paratyphi A [31,33]
Biochemical Test S.Typhi S.Paratyphi A
Glucose fermentation Production of acid only Acid with gas
Xylose fermentation ± -
Arabinose fermentation - +
Mucate fermentation ± Does not ferment
Dulcitol fermentation - +
Rhamnose fermentation - +
d-tartarate Acid only Does not ferment
Lysine + -
Arginine + +
21
ANTIGENIC STRUCTURE [30]
The antigens used to define the serological types of Salmonella include: 1. The O antigens, heat stable polysaccharides that form part of cell wall
polysaccharide (LPS).
2. The H antigen, heat labile proteins of the flagella with diphasic variation
3. Surface Vi antigen, surface polysaccharide that inhibits agglutinabilty of organism by homologous ‘O’ antisera of which Vi antigen of Typhi is most important.
Vi ANTIGEN
Daniels et al (1989) demonstrated that Vi antigen is a capsular
polysaccharide of α-(1→4) linked N-acetyl-D-galactosaminouronic acid variably acetylated at C2/C3positions. It prevents immune serum mediated killing, is antiphagocytic and increases resistance to peroxide. Properties of Vi are determined by structural (via B) and functional (via A) elements at distinct chromosomal sites (Makela & Stocker 1969).
22
Vi is produced by 3 strains of Salmonella serotypes Typhi, Paratyphi C and Dublin, that are genetically distant. The presence of ‘via’ genes in all but a few (1%) strains of Typhi and Paratyphi C suggest Vi is an established property of these serotypes.
Continued laboratory culture of Vi+ strains may lead to loss of Vi production. Daniels et al , in 1989, demonstrated that isolates of Paratyphi C produce less Vi per cell than Typhi , release it more rapidly in the medium and show higher frequency of reversion from Vi+ to Vi- than Typhi.
Vi vaccine gives excellent protection in controlled trials in areas with high attack rates of Typhoid fever. (Felix & Pitt 1934; Robbins and Robbins 1984; Tacker et al.1986; Klugman et al.1987; Daniels et al. 1989) [34,35,36] .
PATHOGENESIS
Salmonella infections begin with ingestion of bacteria in contaminated food or water. Waterborne transmission involves the ingestion of fewer bacilli and has a long incubation period and lower attack rate compared with food borne transmission [37,38].
23
tolerance response that probably facilitates bacterial survival in the stomach and passage to the small intestine [39] .
Interactions with intestinal epithelium and induction of enteritis
Salmonella must evade host antimicrobial factors secreted into the intestinal lumen,including antimicrobial peptides, bile salts, IgA, and traverse a protective mucous barrier before encountering intestinal epithelial cells [40,41] .
Salmonella express an array of distinct fimbriae that contribute to tight adherence to intestinal epithelial cells. Salmonella preferentially adhere to and enter the specialized microfold cells (M cells) that overlie lymphoid tissue within payer’s patches. The bacteria remain in an endocytic vacuole, where they replicate or be transported across the cytoplasm through “bacteria-mediated endocytosis” and released in to the blood or lymphatic circulation.
24
Interactions with Macrophages & Systemic infection
Salmonella sense the acidic environment of the Salmonella -containing vacuole (SCV) and activate various regulatory proteins PhoP and PhoQ, required for adaptation in intracellular environment of host cells. These proteins regulates transcription of over 200 genes which is required for survival within macrophages. PhoQ is the sensor protein for the phagosome environment by sensing acidic pH and antimicrobial peptides to activate gene expression [44-46]
Encoded on SPI-2 is an additional T3SS , which directly delivers the bacterial proteins in to the macrophage cytoplasm favours the survival and promotes virulence.
Host response and immunity
The innate immune system senses invasive Salmonella infections by recognition of lipopolysaccharide by toll-like receptor 4 (Tlr-4), bacterial lipoproteins by Tlr-2 , and flagellin by Tlr-5 by a signalling system Ipaf and peptidoglycan by Nod1,Nod2 [ 47] . Activation of these receptors leads to synthesis of cytokines that orchestrate the inflammatory response and instruct the subsequent antigen-specific immune response.
25
macrophages carry the bacteria to the mesenteric lymph nodes, multiply there and reach blood stream via thoracic duct resulting in primary bacteraemia. Primary bacteraemia being transient , seeds the liver, spleen, lymph node and bone marrow where the bacteria continue to multiply. Following multiplication in large numbers, the bacteria are released into the bloodstream resulting in secondary bacteraemia and leads to the onset of clinical disease.
CLINICAL MANIFESTATION [26]
Salmonella serotypes most often produce characteristic clinical manifestations that have been given the syndrome designations such as gastroenteritis, enteric fever, bacteremia and vascular infection, localized infections and chronic carrier state.
ENTERIC FEVER
26
The incubation period is typically 10 -14 days, but ranges fron 5 - 21 days based on the inoculum ingested and the health and immune status of the person. Following ingestion of the organism, persons may develop enterocolitis with diarrhoeal illness lasting for several days; these symptoms usually resolve before the onset of fever.
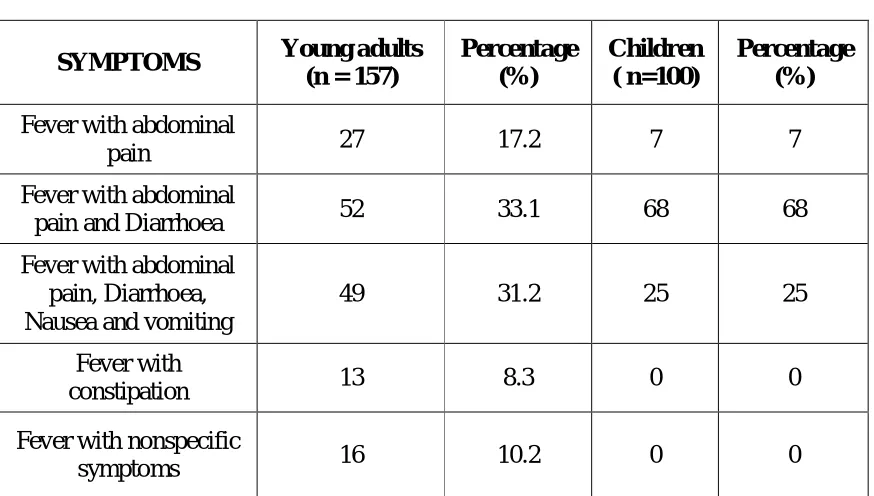
Diarrhoea is common among children under 1 year of age . Constipation is present in 10% to 38% of patients. Fever and abdominal pain are the cardinal manifestations, but only 75% of patients presented with fever and only 30% to 40% of patients will have abdominal pain at presentation [49,50] .Nonspecific symptoms , such as dull frontal headache, chills, diaphoresis, anoexia, cough, weakness, sore throat, muscle pain and dizziness are frequent before fever onset [ 51] .
27
Approximately 20-50% of patients have hepatosplenomegaly, 3% of adults develop necrotizing cholecystitis with localized right upper quadrant pain. Sometimes patient may present as pancreatitis .
2-40 % patients presents with neurologic manifestations, which includes meningitis, neuritis, Guillain-Barre syndrome, and 5% to 10% patients presents as neuropsychiatric illness including apathy, psychosis, and confusion.This so called typhoid state has been described as ‘coma vigil̋’, picking at the bed clothes and muscle twitching are characteristic.
Nearly 10%-15% of patients develop severe disease , which depends on host immune status, strain virulence, inoculums and choice of antimicrobial therapy.Most common complications include Gastrointestinal bleeding (10-20%) and intestinal perforation (1- 3%) occur in third and fourth weeks of illness and results from hyperplasia, ulceration and necrosis of the Peyer’s patches.
Rare complications include endocarditis, pericarditis, orchitis, and focal abscesses and granuloma,arthritis,osteomyelitis,pancreatitis . Hematologic abnormalities associated with typhoid include include leukopenia, anemia, and disseminated intravascular coagulation.
28
CHRONIC CARRIER STATE
0.2% to 0.6% of patients with non typhoidal salmonellosis develop chronic carrier state . Up to 10% of untreated patients excrete
S.Typhi in feces upto 3 months and 1% to 4% develop chronic carriage [53] . The frequency of chronic carriage is higher in infants, women, in persons with biliary abnormalities or concurrent bladder infection with Schistosoma haematobium, and in infants [54,55].
Chronic carriage of S.typhi and S.Paratyphi A has been associated with an increased incidence of carcinoma of the gallbladder and of other gastrointestinal malignancies [56] .
LABORATORY DIAGNOSIS OF ENTERIC FEVER
Clinical diagnosis of typhoid fever is difficult because of lack of specific clinical signs and also due to altered clinical course of the disease due to empirical treatment.
BACTERIAL CULTURE
29
BLOOD CULTURE :
Blood culture processing done by conventional methods or in the recent years automatic blood culture systems are also available.
Conventional blood culture makes use of BHI broth or bile broth or sometimes biphasic media for optimal recovery of salmonella. For the optimum yield of the organism the volume of blood to culture broth in traditional systems should be 1:10 or even more. This dilutes antibacterial substances present in the blood. Commercial blood culture system contains resins , which allows higher volume of blood to be tested in a lesser volume of broth [ 25] .
Conventional blood culture are incubated at 37ºC aerobically. The bottles are examined visually for evidence of growth (hemolysis, turbidity) during 6 -18 hrs. Blind subcultures from BHI broth has to be done on Blood and Mac Conkey agar plates on day 1, even if doesn’t show any signs of growth, there after serial subculturing done on alternative days till 7 days. The growth if any is identified by standard biochemical reactions and confirmed. On day 7, all the blood culture bottles are subcultured before discarded as negative.
30
endemicity, where antimicrobials are taken very often before correct evaluation [ 57,58 ] .
Culture positivity rate is high in first and second week of illness, but in the absence of antimicrobial exposure cultures will still remain positive in third week [ 57,60] .
Sensitivity is further reduced if only small quantities of S.Typhi (<10 organisms/ml ) are present in patients’s blood, frequently it is less than one or less . Hence, volume of blood sample collected for culture enhances the recovery of organism [ 59-63 ]. Increase of yield by 3.2% for each 1 ml of blood sampled [ 64] .
Due to the higher levels of bacteremia in children compared to that in adults, at least 10-15 ml of blood from schoolchildren and adults, and 2-4 ml from toddlers and preschool children should be taken to achieve optimal isolation rates [25] .
31
SUGGESTED BLOOD VOLUMES FOR CULTURES FROM INFANTS AND CHILDREN [64]
Weight of patient(kg) Total Blood Volume (ml) Blood Volume(ml) (Culture 1) Blood Volume(ml) (Culture 2) Total volume for culture (ml) % of total blood volume
≤1 50-99 2 2 4
1.1-2 100-200 2 2 4 4
2.1-12.7 >200 4 2 6 ³
12.8-36.3 >800 10 10 20 2.5
>36.3 >2200 20-30 20-30 40-60 1.8-2.7
LYSIS CENTRIFUGATION SYSTEM [33,64]
32
BONE MARROW CULTURE :
Higher colony counts are present in bone marrow compared to blood and counts not reduced even with 5 days of prior antimicrobial therapy [64,65]. The sencitivity of bone marrow culture is variable 55-90% and specificity upto 30% . Inspite of greater sensitivity, bone marrow culture is of less clinical value because of invasive procedure, pain and expensive when compared to blood culture.
Because amost all S.Typhi and S.Paratyphi are associated with the mononuclear cell- platelet fraction , blood clot culture, centrifuge of blood and culture of the buffy coat fraction, or the lysis direct plating –lysis centrifugation method can substantially reduce the time o isolation of the organism and variably improve sensitivity [66,67] .
SEROLOGICAL TESTS: ANTIBODY DETECTION 1.WIDAL TEST
33
samples taken approximately 10 days apart is required to perform the test ; positive result is determined by a 4-fold increase in antibody titre.
However, in infected patients antibody titres often rise before the clinical onset,making it difficult to determine the 4-fold rise in antibody titre.False negative and false positive results are common when single acute phase serum is used for detection. Knowledge of the background levels of antibodies in local population may aid in better interpretation of the test when performed among patients with high prior probability of infection[67-70]
2.ELISA
Enzyme –linked immunosorbent assays (ELISA) have been use dto study the normal antibody response to LPS, flagella, Vi capsular polysaccharide, or outer membrane protein antigens. Anti-LPS antibodies and Antiflagellum antibodies are more sensitive than Widal “O” and “H” antigen based test [71] .
3. SDS-PAGE
34
4. RAPID SEROLOGICAL TEST [73].
There are a number of commercially available point-of-care rapid serologic tests for enteric fever .
TUBEX TF TEST :
Detects antibody against S.Typhi LPS with an inhibition assay format and a visual result readout, with 56-100% sensitivity and 58-100 % specificity .
TYPHIDOT :
Measures IgM and IgG antibodies against a 50-kDa outer membrane protein of S.Typhi in a immunodot test format, with 67-98 % sensitivity and 58-100 % specificity.
TYPHIDOT M :
Measures IgM antibodies , after removal of IgG antibodies, against a 50-kDa outer membrane protein oh S.Typhi in a dot blot format, with slightly higher of sensitivity 47-98% and specificity of 65-93 %.
ANTIGEN DETECTION
35
health centers . LAT could detect the antigen in 100% of the sera of patients with negative blood culture and positive Widal, indicating better sensitivity as compared to blood culture.
COAGGLUTINATION TEST:
It is a slide agglutination method that uses killed staphylococci (Cowan I strain) bearing protein A which binds with Fc fragment of IgG specific against somatic O antigen of S.enteritidis.The test will be positive in first week of fever with sensitivity of 86.67% and specificity of 88.83 %. It will become negative after the first week of illness [ 76 ] .
MOLECULAR METHODS
Nuclei acid amplification test, including conventional and real - time PCR, have been developed for the detection of both S.Typhi and S.Paratyphi A mainly in blood sample. Targets include Hd flagellin fliC-d , the Vi capsular gene viaB , the tyvelose epimerase gene ( tyv), the paratose synthase gene (prt), the 16sRNA gene , hilA ( a regulatory gene in Salmonella pathogenicity island [SPI-1] , and the gene encoding 50 kDa outer membrane protein ST50 .
OTHER LABORATORY TESTS
36
coagulopathy and elevated creatitine kinase and liver function tests ( aspartate transaminase and alanine transaminase ) . Liver biopsies demonstrated focal Kupffer cell hyperplasia and mononuclear cell infiltration of the portal space [26] .
DIAGNOSIS OF TYPHOID CARRIERS
Detection of carrier is important public health measure. It is useful for screening food handlers and cooks to detect carrier state. Carrier state can be determined by isolating the organism in stool, bile or urine. The frequency and intensity of bacillary shedding vary widely and it is essential, therefore, to test repeated samples. For the detection of urinary carriers, repeated urine cultures should be carried out.
STOOL CULTURE
37
BILE CULTURE
Culture of bile obtained from a overnight duodenal string capsule provides a sensitivity similar to that of blood culture and helpful in isolating the infectious agent both from patients and carriers.
DETECTION OF Vi ANTIGEN :
Demonstration of Vi antigens has been used as a screening test for the carrier state.The test was found to be 70% sensitive and it still increase with multiple number of samples.
Carrier tracing in cities can be done by ‘sewer swab technique’.
TABLE : DETECTION METHODS AND POSITIVITY RATE DURING DIFFERENT STAGES OF ILLNESS
STAGE OF
ILLNESS METHODS
RESULT (% POSITIVITY )
1 st week Blood culture 95
2 nd week Blood culture 40-50
Widal Test Low antibody titre
3 rd week Blood culture 15-20
Stool and Urine culture 80
Widal Test 100
4 th week Blood culture 5-10
Stool and Urine culture 90
38
VARIOUS TYPING METHODS : BACTERIOPHAGE TYPING [30]
The underlying principle of phage typing is the host specificity of the bacteriophages. Several phage-typing schemes have been developed for serotypes of clinical and epidemiological importance.
Typhi phage types
In 1938, Craigie and Yen , developed the first phage typing scheme based on the principle of phage adaptation for differentiation of Typhi . Progressive adaptations in this scheme were made of Vi phage II, which is specific for Vi (capsular) antigen of Typhi ( Felix and Pitt 1934), is highly adaptable and shows high degree of specificity. The adaptation is due in part to the selection of spontaneously occurring host-range phage mutants by the bacterium and in part to a non mutational phenotypic modification of the phage by the host strain.
In 1947, Craige and Felix, standardized the method of phage typing and with further adaptations the internationally recognized total number of phage type is 106. The scheme is now used in specialised WHO approved reference centers world wide.
39
typing is that A or E1 may be so common in a country as to limit the epidemiological information. These can now be overcome by further discrimination using battery of biochemical test and more advanced molecular typing methods.
BIOTYPING [30]
Subdividing common salmonella serotypes according to their
biochemical characters is of value in epidemiological investigations.
Anderson et al., in 1978 and Barker et al. ,in 1980 explained about the
usefulness of combined phage type-biotype studies.
Combined phage type-biotype studies help:
to determine with greater confidence the fine relationships among
strains
to characterize variants that arise from a strain in the course of its
epidemic spread and
to indicate likely phage type interconversions.
MOLECULAR TYPING METHODS [30]
40
DNA include Plasmid profile typing, Plasmid fingerprinting and Identification of plasmid mediated virulence genes.
Chromosomally based techniques include Ribotyping, Random cloned chromosomal sequence (RCCS) , Insertion sequence (IS) 200, Pulsed field gel electrophoresis and PCR based methods such as Random amplified polymorphic DNA typing (RAPD), Repetitive extragenic palindromic element typing (REP-PCR), Variable number of tandem repeats finger printing (VNTR) The methods most extensively used for epidemiological investigations are plasmid typing, RCCS typing, IS200
fingerprinting. PFGE and AFLP are more recently used methods.
ANTIMICROBIAL RESISTANCE
DEVELOPMENT OF ANTIMICROBIAL RESISTANCE AMONG TYPHOIDAL SALMOELLA STRAINS :
CHLORAMPHENICOL RESISTANCE :
Chloramphenicol, the first successful therapeutic drug of typhoid fever since 1948. Chloromphenicol binds to the 50S subunit of bacterial ribosomes, which inhibit peptide chain elongation.
41
1972 [77]. At about the same time there was a first substantial outbreak in Calicut Kerala, India in which 7 of 13 strains were resistant to chloromphenicol and invitro transmissibility to E.coli was demonstrated by Paniker and Vimala 1972, and in both outbreaks mortality was high [78]. In the succeeding 5 years, outbreaks occurred in several other countries, notably,Vietnam, Indonesia, Korea, Chile, Bangladesh.
Resistance mechanism to chloramphenicol include enzyme inactivation by acetylation of the drugs through chloramphenicol acetyl transferases (CATs).. Resistance to Chloramphenicol was mediated by self transmissible plasmids of the HII incompatibility type (IncHI) during the outbreak . In addition to chloramphenicol resistance,these plasmids often carried genes conferring resistance to other drugs, such as streptomycin, sulphonamides and tetracyclines [79] .Other mechanisms include inactivation by phosphotransferases efflux systems and mutation at target sites and loss of OMP.
MULTI DRUG RESISTANCE
With greater number of reports of chloromphenicol resistant S.Typhi
42
By the late 1980s, Multiple- drug resistance (MDR), defined as resistance to ampicillin, chloramphenicol, and trimethoprim-sulfamethoxazole, was reported from multiple countries [ 80-82] .
Resistance to Ampicillin is mostly by production of β-lactamase
enzymes that hydrolyse the β-lactam ring and sometimes by impaired penetration of drug to target PBP( penicillin binding protein) in the bacteria.
Resistance to Co-trimoxazole also emerged after few years of wide spread use. Low level resistance to trimethoprim is due to drug resistant variants of the chromosomal folA gene encoding the bacterial DHFR . High level resistance is achieved by a bypass mechanism through genes that are plasmid mediated. Some of these genes are dfr1, dfrA 3, dfrA10, dfrB6. Sulphonamide resistance is by mutations in the gene folP that encodes for DHPS. Acquired resistance is by plasmid mediated genes such as sul1 and sul2.
MDR- THE GLOBAL PICTURE
43
98MDa plamid which could be transferred to E.coli (Zhang,1991). In recent reports during 2002 and 2003 isolates of S.Typhi from Malaysia and Indonesia were found to be susceptible to all antibiotics, including Nalidixic acid.
MDR - IN INDIA
After the 1988 outbreak in Kashmir valley including 230 cases, a number of reports of MDR salmonella were reported from different parts of the country. The maximum number of MDR isolates was seen in Central India(71%) whereas it was least in the South(55%) [83].
In 1989 MDR S.typhi was present in Eastern India associated with a 120 MDa plasmid [84]. In 1996, Harish et al reported 33% MDR isolates of
S.Typhi, in Pondicherry. Madhulika et al., in 2003 reported 38.8% MDRST from Pondicherry. Padma Krishnan et al., in Chennai, reported 12% of
S.Typhi isolates were found to be MDR out of a total of 50 isolates showing a significant decline [85]. .In contrast a study in Kerala by Ayana et al in 2007, showed no isolates of MDRST [86] .
FLUROQUINOLONES [87]
44
with the addition of a fluoride atom solved the problem with a broadened spectrum of activity including Gram positives and a good systemic action.
Mechanism of action
The important targets of fluoroquinolones are bacterial enzymes DNA gyrase and DNA topoisomerase IV with 2 pairs of subunit. DNA gyrase is a tetramer with 2 subunit, gyr A and gyrB (A2B2) encoded by gyr A and gyr B genes respectively. DNA gyrase is responsible for introducing negative supercoils into DNA and for relieving topological stress during replication. The active site of the enzyme is located at the 122nd aminoacid, which is usually tyrosine. Subunits of topoisomerase IV and parC and par E (A2B2), encoded by parC and pare genes respectively, associated with decatenating the daughter replions.
45
to occur following cessation of treatment, when the drug is eliminated slowly over a few weeks.
Mechanism of resistance
Resistance to FQs is by two mechanisms, target and non target. Alteration in the target enzymes, DNA gyrase and topoisomerase IV is an important mechanism of resistance. Other non target mechanisms include decreased accumulation either by efflux or by decrease uptake of drug and plasmid mediated quinolone resistance.
46
Topoisomerase IV is considered a secondary target for quinolones in salmonella. Quinolone resistance mutations in parC occur at codon Ser 80 or less frequently at codon Glu84 and are invariably associated with gyrA mutation that give phenotypic expression for parC mutation [88] .
In 2003, parC mutations were reported in Salmonella isolates which were both sensitive or had reduced susceptibility to ciprofloxacin. Therefore all parC mutations do not appear to play a role in resistance. Isolates with a single gyrA mutation were less resistant to fluroquinolones than those with an additional par C mutation (Tyr57 Ser or Ser80 Arg), while those with double gyrA mutations were more resistant [ 89] .
Efflux pump decreases the accumulation of drug inside the bacterial cell due to increased efflux , caused by mutation leading to over-expression of AcrAB-TolC efflux pump.
NARST AND CIPROFLOXACIN
47
soon observed that a number of isolates with a MIC of 0.125-1.0µg/ml that were susceptible to ciprofloxacin by disc diffusion were associated clinical failure i.e no remittance after 7 days of treatment. These were resistant to nalidixic acid both by disc diffusion and MIC (32µg/ml). they were termed NAR or NARST [7,8].
NAR IN INDIA
Kadhiravan et al (2005) did a study on 60 blood culture –proven typhoid fever patients. All the 60 isolates were sensitive to ciprofloxacin by disc diffusion testing and had MIC of 0.016 to 2 mcg/ml. 37% of isolates were MDRST and 78% showd resistance to NA. Study showed Nalidixic acid resistance was 82% sensitive and 100% specific for identifying isolates low level resistance to ciprofloxacin. Authors concluded that fluroquinolone breakpoints of NCCLS guidelines need to be redefined and quinolones cannot be used as a first line drugs against S.Typhi infection.
Harish et al (2006) in a prospective study obtained 51 Salmonella
isolates from blood samples of 629 clinically suspected enteric fever cases between 2004-2005. Of the 51 salmonella, 27(53%) were S.typhi and 24 (47%) were S.paratyphi A. Among 27 isolates of S.typhi only 2were sensitive to Nalidixic acid and rest were resistant to nalidixic acid. All the NARST strains had MIC of ≤1µg/ml for ciprofloxacin, ofloxacin and
48
≤1µg/ml for all the three quinolones,while 4 had ciprofloxacin MIC between 8-32µg/ml. Authors concluded because of increased resistance to fluoroquinolones and high prevalence S.Paratyphi may emerge as the main cause of enteric fever in India.
PEFLOXACIN - AS A SURROGATE MARKER FOR QUINOLONE RESISTANCE
Earlier in 2012 the interpretative breakpoints for ciprofloxacin had been revised, where the susceptibility cut off using disc diffusion was raised from 21 to 31 mm and the MIC value was lowered from 1 to 0.06 µg/ml. In 2013, the disc diffusion interpretative criterion of levofloxacin and ofloxacin for S.Typhi was removed . Meanwhile , the MIC interpretative criteria for levofloxacin and ofloxacin have been lowered to ≤ 0.12 µg/ml susceptible, 0.25-1 µg/ml intermediate and ≥ 2 µg/ml resistant.
Various studies globally reported false negative results of ciprofloxacin susceptibity while using Nalidixic acid as a surrogate marker[90,91]. Nalidixic acid does not detect plasmid mediated reistance of fluoroquinolones.
49
50
MATERIALS AND METHODS
This study was conducted at the Institute of Microbiology and Institute of Child Health and Hospital for Children , Egmore, Chennai- in association with Institute of Internal Medicine, Madras Medical College & Rajiv Gandhi Government General Hospital . Molecular characterisation was done at Department of Clinical Microbiology, Christian Medical College ,Vellore .
Study Design : Cross-sectional study.
Study Duration : One year (June 2016-May 2017).
Ethical Consideration :
All patients satisfying the inclusion criteria will be documented , and taken up for the study after obtaining informed written consent in both regional language and English. This study was reviewed and approved by Institutional Ethics Committee .
Sample size : 257 patients.
Sample size ( n) calculated using the formula, n = Z2 x P(1-P ) / d2
51
Statistical Analysis : Descriptive statistics , SPSS version 21.
INCLUSION CRITERIA :
Febrile children and young adults in the age group of 5-24 years admitted as inpatients and outpatients with one or more of the following criteria will be included.
Fever more than 3 days duration
Symptoms of Enteric fever such as abdominal pain, altered bowel habits, nausea, vomiting, and signs such as pyrexia,toxic look, coated tongue with sparing of margins, splenomegaly, hepatomegaly, hepatosplenomegaly.
EXCLUSION CRITERIA:
Patients who were on antibiotics for the past one week .
Patients with fever accompanied by other localising signs &symptoms.
SAMPLE COLLECTION AND TRANSPORT :
52
Preparation of site :
1. Peripheral vein to be drawn was chosen and disinfected using 70% alcohol.
2. Skin over the venipuncture site was cleansed with 70 % alcohol in a circular fashion, approximately 5 cm in diameter , rubbed vigorously and allowed to air-dry.
3. Starting in the centre of the circle , 2% tincture of iodine was applied in ever-widening circles until the entire circle has been saturated with iodine, it was then allowed to dry for 1minute.
4. Sterile needle was inserted into the vein and blood was drawn , transferred to 50 ml of BHI broth, making 1: 5 or 1:10 dilution of blood in broth.
5. After the sample was collected , the site should be cleansed again with 70% alcohol.
Time of collection : [24]
53
SAMPLE PROCESSING :
Incubation Conditions :
Blood culture bottles was incubated aerobically at 370 C for 18-24 hours. All the blood culture bottles were examined for evidence of growth (hemolysis , turbidity ) during 6 - 18 hours of incubation. Blind subcultures were done on Nutrient agar plate, Mac Conkey agar plate,5% Sheep Blood agar plate, after 24 hours of incubation .Then further subcultures were done after 48 hours, 72 hours and 1 week of incubation .
IDENTIFICATION OF SALMONELLA : [31,33] COLONY MORPHOLOGY :
On Nutrient agar plate colonies of Salmonella species were large 2- 3 mm , moist, translucent, low convex, discrete colonies with smooth surface with entire edges.
On Blood agar, Salmonella species form moist greyish non haemolytic colonies and on MacConkey agar plate produce lactose non fermenting colonies.
54
GRAM STAIN :
Salmonella was gram negative bacilli measuring approximately 2-4 x 0.6 µm, uniformly stained with parallel sides and rounded ends, non-capsulated, non-sporing.
Presumptive identification of the isolates were done using standard biochemical tests such as Hugh Leifson’s oxidative fermentative test, Nitrate reduction test, Indole production, Methyl red and Voges Proskaeur reaction, Citrate utilization ,Urease production, Phenylpyruvic acid test, 1 % carbohydrate fermentation test for Glucose, Lactose, Xylose, Arabinose and Moeller’s Decarboxylation test [Table 3,4].
SLIDE AGGLUTINATION TEST : [31]
Confirmation of the isolates were done by Slide agglutination test using specific antisera- Polyvalent ‘O’ antisera, and Salmonella Typhi ‘H’ ,
Salmonella Paratyphi ‘AH’ and ‘BH’ ( Institute of Preventive Medicine, Guindy ).
Procedure :
55
2) Using a sterile inoculating loop portion of pure growth from a fresh subculture in a non-selective medium (Nutrient agar plate) was taken and emulsified in a drop of physiological saline (20 µL) and mixed thoroughly in a ‘Control’ ring.
3) Rocked the slide back and forth and observed for any autoagglutination under a bright light and over a black background . 4) The saline suspension was carefully examined to ensure that it is
even and does not show any clumping . If still autoagglutination occurs ,the culture is cannot be serotyped.
5) Test was further proceed if there is no autoagglutination .
6) Emulsified a portion of pure growth in a drop of physiological saline in ‘Test’ ring and a drop of (equal volume ) of Polyvalent ‘O’ antisera was added and mixed well.
7) Tilt the slide back and forth and observed for agglutination .Clumping was seen within 30 seconds to 1 minute, if the reaction was positive, .
8) Similarly the test was proceeded for flagellar antigens , using polyvalent ‘H’ antisera for S.Typhi isolates, ‘AH’ for S.Paratyphi A
56
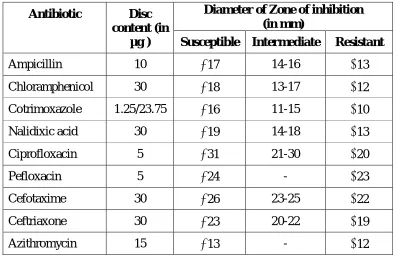
ANTIBIOTIC SUSCEPTIBILITY TESTING : [94] KIRBY-BAUER DISC DIFFUSION METHOD :
Antibiotic susceptibility testing of the isolates was done by Kirby-Bauer disc diffusion method according to Clinical Laboratory Standards Institute (CLSI -2016) guidelines for the following drugs - Ampicillin (10 µg), Chloramphenicol (30µg), Cotrimoxazole (1.25/23.75 µg). Ciprofloxacin (5µg), Nalidixic acid(30 µg),Pefloxacin(5 µg ),Cefotaxime (30 µg),Ceftriaxone (30 µg), Azithromycin(15 µg).
3-4 well isolated , morphologically similar colonies were taken with a sterile loop and inoculated into peptone water and incubated at 370 C for 2 hours. Turbidity was adjusted to 0.5 McFarland standards and a lawn culture was made on Muller-Hinton agar and appropriate antibiotic discs were placed. Plates were incubated at 370 C for 16-18 hours.The zones of inhibition were measured and interpreted according to CLSI 2016 guidelines-M100- S26 document. Quality control was done using ATCC E.coli 25922 strain.
57
TABLE : KIRBY-BAUER DISC DIFFUSION METHOD
Antibiotic Disc
content (in µg )
Diameter of Zone of inhibition (in mm)
Susceptible Intermediate Resistant
Ampicillin 10 17 14-16 13
Chloramphenicol 30 18 13-17 12 Cotrimoxazole 1.25/23.75 16 11-15 10
Nalidixic acid 30 19 14-18 13
Ciprofloxacin 5 31 21-30 20
Pefloxacin 5 24 - 23
Cefotaxime 30 26 23-25 22
Ceftriaxone 30 23 20-22 19
Azithromycin 15 13 - 12
MINIMUM INHIBITORY CONCENTRATION ( MIC ) : [ 94,95,96]
Determination of Ciprofloxacin minimum inhibitory concentration (MIC) by using broth-micro dilution method (BMD) :
58
WEIGHING ANTIMICROBIAL POWDER :
1000 X Volume (ml) X Concentration (µg/ml) Weight (mg) = --- Potency (µg/mg)
P = Potency of the antibiotic base, 980 µg/mg V = Volume of distilled water required, 10 ml C = Final concentration of the solution, 1024 µg/ml
W = Weight of the antibiotic substance to be dissolved in distilled water,10.44 mg.
PREPARATION OF ANTIBIOTIC STOCK SOLUTIONS :
A stock solution containing 1024 ug/ml of the antibiotic to be tested was prepared i.e., 10.44 mg of antibiotic powder was weighed and dissolved in 10 ml of distilled water. The required dilutions of the antibiotics were made by doubling dilutions from 1024 µg /ml to 128 µg/ml . Range of concentration of antibiotics was decided by breakpoints determined by CLSI 2016 guidelines .
QUALITY CONTROL STRAINS :
59
INOCULUM PREPARATION :
1. Inoculate 2- 3morphologically similar colonies of 24 hours pure growth from nutrient agar plate into 1.5 ml nutrient broth. Incubate at 370 C for 2 hours and then adjust to 0.5 McFarland standards.
2. 100 µl of 0.5 McFarland adjusted inoculum is transferred to 2 ml of physiological saline and used as final inoculums for performance of MIC testing.
PROCEDURE :
1. 96 well microtitre plate was chosen and labelled for Quality control strain ( Positive control- E.coli ATCC), Test isolates and Sterility control.
2. 100 µl of Cation Adjusted Muller Hinton Broth (CAMHB ) was added in all the wells .
3. First column in microtitre plate was the Growth control for the isolates containing 100 µl of sterile drug free CAMHB, and 10 µl of corresponding inoculum suspension.
4. Last row was the sterility control of medium containing 100 µl of CAMHB.
60
from higher to lower concentrations (labeled as 128 µg/ml t0 0.06 µg/ml).
6. 10 µl of the final inoculum was added to the well of microtitre plate. 7. 10 µl of final inoculums was streaked on nutrient agar plates for
purity check.
8. Nutrient agar plate and sealed microtitre plates were incubated at 37 0 c for 16-18 hours
INTERPRETATION OF RESULTS :
1. Purity of inoculum suspension in Nutrient agar plate was checked . 2. The growth in positive control well was checked .
3. The growth ( turbidity ) in Growth control well of the corresponding isolates were confirmed.
4. Minimum inhibitory concentration (MIC) was read as the lowest concentration of the antibiotic without visible growth / turbidity.
MOLECULAR ANALYSIS OF CIPROFLOXACIN RESISTANCE GENES: [ 97,98 ]
61
Genomic DNA Extraction :
1. Pure growth from 24 hours culture from nutrient agar plate was emulsified in 200 µl of physiological saline and vortexed .
2. DNA extracted using Automatic DNA extracter-QIA symphony SP (Qiagen-Boston).
UNIPLEX PCR DETECTION OF gyrA , gyrB and parC GENE:
Uniplex PCR was performed with the Applied Biosystems VeritiTM 96-well Thermal cycler (Thermo Fisher Scientific ). For each of the DNA sample a reaction mix was prepared with the following components.
REACTION MIX COMPOSITION :
S.No COMPONENTS REACTION VOLUME
FOR EACH CYCLE
1 Master mix 10µl
2 MilliQ water 4µl
³ Q solution 2µl
4 Primer mix 2µl
62
CYCLING CONDITIONS :
Cycling conditions for 30 cycles run- gyrA,gyrB,and parC -
1 Initial Denaturation 920 C 5 min
2 Denaturation 920 C 1min
3 Annealing 620 C 1min
4 Extension 740 C 2min
5 Final Extension 740 C 1min
PRIMERS : [99]
Antimicrobial Resistance gene sequence for Salmonella species.
S.No Oligo
Name 5 < ---Sequence --- >3 Base Pair
1 gyrA F TGTCCGAGATGGCCTGAAGC
347 bp
2 gyrA R TACCGTCATAGTTATCCACG
3 gyrB F CAAACTGGCGGACTGTCAGG
345 bp
4 gyrB F TTCCGGCATCTGACGATAGA
5 parC F CTATGCGATGTCAGAGCTGG
270 bp
6 parC R TAACAGCAGCTCGGCGTATT
AGAROSE GEL ELECTROPHORESIS :