LIFE EVENTS, PERSONALITY PROFILE,
PSYCHIATRIC MORBIDITY IN SELF INJURIOUS
BEHAVIOUR - A CROSS SECTIONAL STUDY
DISSERTATION SUBMITTED FOR PARTIAL FULFILLMENT OF THE RULES AND REGULATIONS
DOCTOR OF MEDICINE
BRANCH - XVIII (PSYCHIATRY)THE TAMILNADU DR.MGR MEDICAL UNIVERSITY, CHENNAI,
TAMIL NADU.
CERTIFICATE
This is to certify that the dissertation titled “LIFE EVENTS, PERSONALITY PROFILE, PSYCHIATRIC MORBIDITY IN SELF INJURIOUS BEHAVIOUR- A CROSS SECTIONAL STUDY” is the bonafide work of Dr.K. ILAMARAN, in part fulfillment of the requirements for M.D (Psychiatry) (Branch–XVIII) examination of
The Tamilnadu Dr. M. G. R Medical University, to be held in APRIL 2016. The Period of study was from March 2015 toAugust 2015.
HOD DEAN
DECLARATION
I, Dr. K. ILAMARAN, solemnly declare that dissertation titled
“LIFE EVENTS, PERSONALITY PROFILE, PSYCHIATRIC MORBIDITY IN SELF INJURIOUS BEHAVIOUR - A CROSS SECTIONAL STUDY” is a bonafide work done by me at Kilpauk medical college, Chennai, during the period from March 2015 to August
2015, under the guidance and supervision of Dr. S. RAJARATHINAM M.D., DPM., HOD, Professor of Psychiatry, Kilpauk Medical College. This dissertation is submitted to The Tamilnadu Dr. M. G. R Medical University, towards part fulfillment for M. D. Branch – XVIII (Psychiatry), part- III examination.
Place: Chennai
ACKNOWLEDGEMENT
I sincerely thank Prof. Dr. R. NARAYANA BABU, MD., DEAN, Kilpauk Medical College for permitting me to do this study.
I sincerely thank Prof. Dr. S. RAJARATHINAM . M.D., DPM.,
Head of the Department, Kilpauk Medical College for his, concern, care,
guidance and help, and I would like to thank to Dr. R. SARAVANA JOTHI, MD., who has been a source of inspiration and motivation. I would like to express my sincere thanks to Assistant Professor, Dr. M. S. JAGADEESAN, who has guided me in completing this dissertation. I thank my colleagues, and others for their immense help in completing this study. I would be failing if I do not express my gratitude
to all my Teachers at the Department of Psychiatry, Kilpauk Medical College, Chennai for their support and encouragement during this study.
I thank all those patients who participated in the study, without
LIST OF ABBREVIATION
WHO - World Health Organization
SIB - Self Injurious Behaviour
SA - Suicide Attempt
DSH - Deliberate self harm
LAS - Lethality assessment scale
PSLE - Presumptive stressful life events
EPQ90 - Eysenck Personality Questionnaire 90
GHQ12 - General Health Questionnaire 12
CONTENTS
Sl.No. Page No
1. Introduction 1
2. Review of Literature 10
3. Aim and Objectives 26
4. Materials and Methods 28
5. Results 36
6. Discussion 61
7. Summary and Conclusions 75
8. Limitations 78
9. References 79
INTRODUCTION
According to World Health Organization (WHO), Suicide is the
second leading cause of death between 15 and 29 years of age groups,
globally (2012). It’s responsible for 1. 4% of all deaths world wide. WHO
defines suicide act as ‘the injury with varying degrees of lethal intent,”
and that suicide may be defined as a suicidal act with fatal outcome. The
word `suicide' has its origin in Latin; `sui', of oneself and `credere', to kill:
the act of intentionally destroying one's own life. In 2012, India
accounted for the highest suicidal rate. According to WHO report, one
person commits suicide every 40 seconds globally. In the world, most
suicides occur in the South-East Asia region.
Suicide
The term suicide is used to denote self-planned and deliberate
termination of one’s life. It is as old as mankind and is indeed a giant
puzzle. It is a paradox why humans who love to live a full life turn to self
destruction.
Para suicide :-
It is an impulsive act of self – injurious behavior without any prior
planning or intent to die. The harm to self may be done by inflicting
injury or consuming a substance. It is otherwise known as Deliberate
Attempted suicide:-
Among those who attempt suicide, a few succeed, but some
survive due to timely intervention of chance factors in spite of best
planning and clear cut intention to die. They are known as ‘Attempted
Suicide’.
Overlap :-
A person who tries to terminate his life with real intent may
survive. However, an individual who injures himself impulsively without
any real intent to die may lose his life.
Another meaning for suicide in latin word, is self murder. There
are some types of suicides. The general term used for suicide attempt is
self injurious behavior (SIB) which is further subdivided into suicidal
attempt (SA) and nonsuicidal self injury (NSSI).( Chloe A. Hamza ,
Shannon L. Stewart Teena Willoughby,2012 ). Usually the SA are with
intent and NSSI are without intent to die. Non suicidal self injury(NSSI),
which is defined as self-directed, deliberate destruction or alteration of
bodily tissue in the absence of suicidal intent (Nock & Favazza, 2009),
examples are self-cutting, head banging, self-hitting, scratching to the
point of bleeding, and interfering with wound healing. Suicidal behaviors
refer to directly self-injurious behaviors (e. g., suicide attempt, suicide)
severe slashing, and jumping from heights. NSSI and suicidal behaviors
are both forms of self injurious behavior, and therefore they are
sometimes conceptualized as falling along a single self-harm continuum
(Chloe A.et al 2012 )
The suicidal behaviors range from suicidal ideas to completed
suicide. It depends on the various factors like age, gender, socioeconomic
status, occupational status, educational status, and marital status.
Statistics on suicidal behavior varies between different nations. In
developed countries about 10% of the suicides were underestimated,
whereas in developing countries most of the suicides were underreported.
The overall mortality from suicide was underestimated according to
Charlton et al, (1992). Among the suicide attempters, about half of the
them had previous suicide attempts. Most of the suicide attempters had
previous deliberate self harm (DSH) injuries like slashing the hands, legs
and body. In the Indian context most of the individuals with a history of
DSH, are more likely to indulge in further suicidal behavior by drug
overdosages, organophosphorous poisoning , rat killer poisoning, phenol
liquid poisoning and oleander seed poisoning apart from hanging.
Among the suicide attempters, male suicide attempters were found to be
make more violent attempts, with high suicidal intention and lethality.
Most of the male suicide attempts were due to subjective lack of
attempts were due to negative interpersonal events. There are risk and
protective factors for suicide which include cultural, social, psychological
and biological factors. The suicide attempts were due to intensified
effects of risk factors or weakened effects of protective factors. The other
commonly occurring risk factors are elder by age, low socioeconomic
status, low educational status, unmarried people, divorced, widowed,
living alone, unemployment, retirement, students, prisoners, immigrants,
refugees, low social support and lack of social integration.
Suicide rate has been raising in younger males for the past 20
years because of the alcohol misuse, problem in the school and various
psychosocial stressors. Learning model is also a risk factor for suicide,
which is available in the society, culture, institution and mass media. The
relationship in the society has a significant impact in the individual, when
there is a disturbance in the relation between the individual and the
society, the suicidal tendency might occur.
Life event stressors prior to suicide attempts had a significant role.
The number of stressors were also important in determining the suicide.
Usually a combination of life event stressors would occur rather than a
single life event stressor. Persons with self injurious behavior would have
lower level of physical well being, psychological well being, social
STRESS:
Stress is a well known cause for mood disorder, mental
disorder and risk factor for suicide attempt. Negative life events lead to
depression, interpersonal problem, occupational problem and self
injurious behavior. Childhood trauma has a significant impact in suicide
behavior. Also unemployment, loss of job, financial problem contributed
towards suicide. The stressors are recent one, which might be weeks to
months prior to suicide attempt.
There was an increased suicidal behavior present in young females
and in low socioeconomic status. (King, Raskin, Gdowski, Butkus, &
Opipari 1990). Chronic physical illness also had a tendency to increase
the suicidal behavior. Stressful life events and social problem happened
in the recent time may lead to suicide (Townsend et al 2001).
There is a terminology known as ‘kindling effect’ otherwise called
Episode sensitization , in which individuals with repeated episodes of
selfharm, bring about neurobiological, cognitive and interpersonal
changes that directly increase the risk of recurrence. In multiple episode,
there is a weak association between stressful life events and suicidal
ideation than person with single attempt of suicide. One of the risk factor
in suicide attempt is job loss and unemployment. (Beautrais et at 1997).
suicide in adults associated with substance abuse. Some of the individual
with life events stressors would attempt suicide within a day of a stressor
(Kenneth R. Conner, 2011). Some other psychosocial stressors also had a
role in suicide, like interpersonal losses, legal issues or disciplinarians,
pregnancy or fear of pregnancy, loss of freedom, loss of self esteem,
physical and sexual abuse.
PERSONALITY:
Most suicide attempts were done by persons with abnormal
personality(Hanet,al;1997,).The risk factors are aggression, greater
impulsivity, substance abuse, antisocial personality disorder, depression,
Bipolar affective disorder I & II and with previous suicide attempt,
genetic factor and life event stressors. Sometimes there is an overlap
between borderline personality disorder and Bipolar affective disorders.
Most of the suicidal attempters had childhood physical abuse or sexual
abuse. The commonly encountered personality disorder in suicides are
borderline personality disorder, Narcissistic personality disorder and
Histrionic personality disorder.
Suicide in Schizotypal personality is understudied. Schizoid
personality disorder is associated with depression, anxiety and
behavior. According to previous study results 70% of the borderline
personality disorder had atleast one suicide attempt in their lifetime.
Borderline personality disorder is also called Emotionally unstable
personality disorder which is further divided into impulsive type and
borderline type, coming under cluster’ B’ personality. Impulsivity is one
of the feature of borderline personality and is frequently associated with
alcohol or any other substance abuse, eating disorder, unprotected sex,
reckless spending, reckless driving, frequent job changes, running away
and self injury and other features are unstable interpersonal relations,
anger outburst, idealization, devaluation, minimization, maximization,
sensitivity to the feeling of rejection, criticism and isolation. There were
an association between substance abuse on recurrent suicide attempts
was found in a study of Berk etal.(2007), but this finding was not
confirmed in Soloff and Chiappetta (2012).
In borderline personality disorder, the time prevalence of suicide
attempt is 3-10%. Men completing suicide in this disorder has been
underestimated being almost twice as women. The reasons for NSSI are
expressing anger, self punishment, distracting oneself from emotional
pain. NSSI is one of the feature of the borderline personality disorder.
This should be actively intervened because there is a possibility of serious
more unsuccessful treatments (Zahl and Hawton,2004; Paris,2007; Soloff
and Chiappetta,2012).
Many of the DSH would lead not only to recurrent DSH but also
to a serious suicide attempt. Personality disorders predispose to major
mental illness like depression, and substance abuse. Among the antisocial
personality disorder 5% commit suicide. Horrocks . J et al (2003) study
showed that emotionally unstable personality and impulsive type
personality trait or disorder was the commonest personality disorder in
self injurious behavior. Personality disorder itself increases the self
injurious behavior. Life events stressors in personality disorders increases
the suicidal ideations. Suicidal proneness, psychological distress have
been noted in schizoid personality, schizotypal personality, borderline
personality, depressive personality and sadistic personality.
Childhood adversity and comorbid mental illness increase the
suicidal rate. Based on the previous studies, that the presence of anxiety
and depressive disorder increases the risk of suicide attempts and
completed suicide (Angst et al., 1999; Sareen et al., 2005; Ten Have et
al., 2009).Heritability contributes 40% in borderline personality disorder.
Some of the studies found that there are some reduction of the areas in the
antisocial traits are risk factors for this personality disorder. (Black,
Blum, Pfohl Hale 2004, Oldham 2006.)
PSYCHIATRIC ILLNESS:
There are psychiatric illness like depression, anxiety, adjustment
disorder, substance use disorder, schizophrenia and bipolar disorders in
which suicide attempt can occur. Among the psychiatric illnesses the
depression is the commonest disorder. According to previous study
results, when there is a combined occurrence of depression and anxiety
the suicidal rate is more common than the depression alone. Anxious
mood may lead to negative thinking, which may be a predisposing factor
for suicide. In India the common psychiatric disorders leading to suicide
attempts are adjustment disorder, depression, substance abuse.
The rate of suicidal attempts are low in India when compared to
Western countries. In Western countries 90% of the suicides were due to
psychiatric illness. According to previous study results 60%-70 % of the
patients with depression would attempt for suicide, 15%-20% of the
Bipolar affective disorder would attempt for suicide and other mood
disorder would contribute to about 10%-15% of suicide, and patients with
REVIEW OF LITERATURE
The term attempted suicide gives a wide meaning from severe and
life threatening attempt to minor gestures. Complete suicide is relatively
uncommon. The suicide should be viewed as a symptom rather than a
disease per se.
PARASUICIDE:
Deliberate self poisoning and self injury term was proposed by
(Kessel, (1965). In the 1970s, Kreitman (1977), who introduced the term parasuicide, in which the individual would have self mutilating behavior
like cutting the skin, but they do not wish to die, the female – male ratio
was 3:1, they will be 4% of the all psychiatric patients, among them 30%
might be having substance abuse.
The parasuicide attempter’s age will be around 20 years and they
will be single or unmarried. The nature of the cut will be delicately, not
coarsely by using razor blade, knife and broken glass. The common sites
were wrist, arms, thighs and legs and the uncommon sites were face,
breast and abdomen. Most of these individuals would be suffering from
a personality disorder and also they will be neurotic and introverted.
Weissman, (1974) study showed that 1-10% of the completed
PSYCHOLOGICAL FACTORS:
The first important psychological insight into suicide came from
Sigmund Freud.
Sigmund Freud, in mourning and melancholia, wrote of aggression
turned inward when one internalizes a lost object and then turns this rage
on to oneself. Edwin Schneidman has written as victim’s unbearable
mental pain “psychache” and how terminally his or her perceptions
narrow and he or she can see only one solution-his or her death.
Contemporary suicidologists stress that people most likely to commit
suicide are those who have suffered the loss of a love object or have
sustained a narcissistic injury, who experience overwhelming moods like
rage and guilt, or who identify with a suicide victim. According to Freud,
“suicide is an aggression turned inwards against a loved person with
whom the individual has identified himself”
Psychodynamics of suicides:
• It is a plea for help.
• It is a final exit from all bonds.
• It is a threshold of peace and permanent bliss.
• It is a sacrifice and self atonement.
• It an escape from pain & misery.
• It is a beginning of new life through rebirth.
• It is a mastery over death.
• It is revenge against his persecutors.
• It is an act to punish the enmities.
• It is an act of rescue.
BIOLOGICAL FACTORS:
There are some evidence of involvement of biogenic amines in
suicides. According to Julius Axelrod’s study (1970) there is a relation
between suicide and biogenic amine metabolism. Marie Asberg’s (1975)
work on levels of serotonin and noradrenaline levels in the brains of
depressive individuals laid the ground work for a later suicide. Other
neurotransmitters involved in suicides are GABA (gamma amino butric
acid), G protein, glutamate receptors, kinases, BDNF. Some other studies
say that there was a decreased level of 5HT in depressed individuals with
suicide attempt.
SOCIOLOGICAL FACTORS:
Emile Durkheim, a French sociologist emphasized the importance
of social factors in the causation of suicide. According to him, the suicide
rate of a population varies inversely with the degree of social integration
There are 3 types of suicide:
1 . Egoistic
2. Altruistic
3. Anomic
Egoistic suicide:-
Here the individual has little concern for the community (family,
religion or community)
E. g. unmarried, widowed, unemployed, deprived, and bereaved.
Altruistic suicide:-
Here, the individual has excessive integration with to society. The
customs & rules of the society demand his death under certain condition.
Here the individual gives his life as a priced gift to answer the demands
of the society
E . g. sati in India / harakiri of Japan / mass suicide in cult
Anomic suicide:-
Here, the existing relationship between the individual and his
society is shattered all on a sudden
E . g. economic recession, loss of employment, wealth or status
In addition to social integration, status integration is also important as a
protection against suicide (social role like father, teacher, married,
employed, leader) . The more the status, better the social integration and
behaviour increases markedly during this time and the causes are more
social and interpersonal conflicts (Shaffer and Fisher, 1981; Brooksbank,
1985 & Hawton et al., 1982). Hopelessness has been identified as one of
the core characteristics of depression by Beck (1963). The features of
high hopelessness group were anxious and depressed mood, had a strong
wish to die, made a planned attempt, act was done for relief from mental
state, motivated for help and sought help. Rifai et al.,(1994), study shown
that the individuals with suicidal attempts had high scores in
hopelessness.
BIO PSYCHO SOCIAL FACTORS:
The cortico- hypothalamic pituitary adrenal axis, which regulates
adrenal cortical hormone levels and mediates reaction to stress. The
elevated corticotrophin releasing factor( CRF) concentration in CSF and
decreased number of CRF binding sites in the frontal cortices of suicide
attempters were present. Another study shows the alcohol itself decreases
the 5 HT in some areas of brain in depressed individuals. Alcohol is a
well known disinhibitor that increases the impulsivity leading to suicide
attempt.
AGE:
Holding et al., 1977). The rate of Adolescent suicide attempts are
increasing in numbers (Hawton et al. 1982; Brooksbank, 1985). Among the adolescents, suicide attempt was estimated to be about 8%-10% in
their life time. The old age also prone for suicide when they are living
alone without family support, and also if they have associated comorbid
physical and psychiatric illness.
GENDER:
There is a wide disparity about incidence of suicide and gender .
Some western countries shows higher incidence in males, and in
developing countries more incidence was seen in females. The studies by
Garfinkel B. D. et al., (1982), Otto (1972), L. Kotila et al., (1987) and Olfson et al (2005), showed that the higher incidence of suicide occurs in
adolescent females. There is Male–female disparity in completed suicides
among various nations of the world . Female suicide completion rate is
high in srilanka, china, and also in India. Suicide attempts in women are
less violent, less lethal and have less disfigurement. One theory says that
lower rate of suicide in women due to lower rate of alcohol dependence
and abuse in women . Women are more likely to seek medical attention
when they are depressed and they are more accommodative than men,
having better network with friends and family. Suicidal attempts before
MARRIAGE:
Married persons had lesser incidence of suicides while single
persons, never got married persons, divorced, and widowed had a higher
incidence of suicide. Unmarried persons had a higher percentage of
suicide according to Ponnudurai et al., (1986), Ghulam et al., (1995) and
Latha et al., (1996). Family history of suicide is a risk factor for suicide.
Homosexual men and women also had a higher suicidal tendency.
Fleishmann,et,al; (2005) study showed most of the suicide attempters
were married than single in India.
In India joint family concept is still existing, and suicidal attempts
were more common in nuclear family than in joint family. The national
crime records Bureau 2014, showed that, the number of suicides was
high in married men, widowers, than married women, and widows .
EDUCATION
There is no variation in educational level in persons attempting
suicide according to BilleBrahe et al.,(1985). Another study by
Nordentoft & Rubin (1993) alsoshowed that there is no difference
between attempters and general population based on educational levels.
attempts were present in individuals with educational level below
matriculation.
OCCUPATION :
Higher the social status increases the suicidal risk. Professional and
physician had a high risk for suicide. Also other occupations like law
enforcement, dentists, artists, mechanics, lawyers, insurance agents also
had a higher risk. At the same time unemployment also had significant
role in suicide. According to Ramdurg et al.(2012), employed individuals
had a higher suicidal rate than the unemployed persons and also the level
of stressors were more in employed persons. R.Tara e, al (2014)., study
found that, 55% of the suicide attempts were present in individuals with
unskilled workers.
INCOME STATUS:
According to previous study results, most of the suicide attempts
occurred in low socioeconomic status. Previous study by
Thirunavukarasu (1981) have shown that increased incidence of suicides
were present in the low income and social status group. According to
C.T.Sudhirkumar & R.Chandrasekaran,(2000).,58.1%of the participants
PHYSICAL ILLNESS:
There is always a correlation between suicide and physical illness.
Some studies showed if 6 months after a major medical attention, an
individual may attempt suicide. Medical illness contributes to about half
of the suicide attempts. For example if the individual had loss of mobility
which significantly impairs the occupation and disturbs their recreational
activities the risk is more. Disfigurement in females, chronic pain,
persons undergoing hemodialysis, cirrhosis also had a high risk for
suicideattempts. Importantly drugs like reserpine, Corticosteroids,
Antihypertensives, and Anticancer drugs also had a major contributing
factor for suicide in those individuals taking these drugs.
PSYCHIATRIC ILLNESS:
Adolescents can be reliable reporters of their suicide potential and
the clinician needs to be sensitive to symptoms of major depressive
disorder in assessing potentially suicidal adolescent (Robbin DR et al,
1985). Adolesent suicide attempters are likely to have mood disorder
about 7 times more than other individuals. Common mental illness prone
for suicide is depression, which is usually associated with another mental
illness. The identifiable risk factors are previous suicidal attempts,
About 15 % of the suicide was reported in depressive disorder,
(Pfeffer CR et al, 1993). There is a strong relation between adolescent suicide attempt, substance abuse and personality disorder (Marttunnen et
al, 1991). If the individual had psychiatric illness they would have 3-12
times of increased risk for suicide than general population. Previous
studies showed that 20% of the suicide attempters had panic disorder and
social phobia. The degree of risk varies in age, gender, diagnosis,
inpatient or outpatient treatment. Suicide among adolescents who had a
history of psychiatric hospitalization occurs approximately nine times
more often than among adolescents in the community (Kuperman et al.,
1988). Increased risk of suicide is present in patients getting inpatients
treatment than outpatient treatment . Major depressive disorder associated
with suicidal behavior (Robbins and Alessi,1985). More than 70% of the
adolescents reported suicide ideation or attempts among adolescent with
a diagnosis of major depressive disorder (Myers et al.,1991).
Suicide is a complex behavior in depression. It varies with age and
gender, risk factor is usually not a single factor but it is a combination of
two or more of risk factors. The high risk factor in geriatric age groups
are facing problem, loss of loved one, change in life style, loss of physical
independence and other physical illnesses. In old age the other medical
family and school pressures, hormonal changes and major life changes. In
suicide, morbidity is difficult to assess but lethality can be assessed
easily. Two third of the individuals with depression are not understanding
as depressed and not taking treatment. Only 50% of the individual with
depression take treatment. Depression is a treatable condition, 80-90% of
the patients will respond to medication . Sometimes antidepressants also
may induce suicide, especially taking medicine for first time and also
patients with age group of less than 25 years. Best way to prevent suicide
is early detection, diagnosis and treatment. Hawton et al (1982) study
shown that that 20 % of the individuals with psychiatric illness had drug
overdosages.
Occurrence of suicide in schizophrenia is similar to general
population (Hawton et al 2005,). The common causes for suicide in
schizophrenia is comorbid mood disorder, recent loss, hopelessness, drug
misuse, substance abuse, previous suicidal attempt. According to
Tiihonen et al(2006), in the first episode of schizophrenia, there is an
twelve fold increased risk of suicide. A study by Miles et al (1977)
shows, the life time risk of suicide in schizophrenia is 10%. The greatest
risk of suicide is present in post psychotic period (Siris & Collegue
2001). The other risk factors in schizophrenia are individuals associated
illness, sometimes responding to hallucinations. Suspicious ideas and
paranoid ideas increase the suicidal attempt.
SUBSTANCE ABUSE:
Substance abuse contributes to about 15% of the suicide attempts.
The factors like interpersonal losses, undesirable life events would cause
symptoms like mood disorders which may result in suicide. If the
substance abuse is associated with antisocial personality disorder and
those with multiple substance abuse, the risk for aggressive, impulsive
and criminal behavior increases leading to suicidal behavior. There is a
high correlation between mood disorder and substance abuse (Pfeffer et
al. 1988). Many a time, it is very difficult to decide whether a particular
death is due to suicide, murder or accident, particularly when there is
associated with alcohol abuse or drug abuse. ‘Psychoactive substance was
a major problem in adolescent populations’ according to Hawton et al
(1982).
Alcohol plays a crucial role in suicide attempt, due to
environmental factor and /or biochemical factors. In chronic course of
alcohol consumption, the individual has to face a various stressors and
interpersonal problem and rejection in the society leading to suicidal
behavior (Murphy GE 1990). According to previous studies they found
aggression and alcohol consumption. Heavy drinking was associated
with increased aggressive behavior, (Placidi GP, Oquendo MA et al.2001)
.According to Conner KR, Duberstein PR et al.(2004), individuals with
alcohol dependence who have completed suicide ,were characterized by
major depressive episodes, stressful life events, interpersonal problems,
poor social support, living alone, high aggression and impulsivity,
hopelessness, severe alcohol use , other substance abuse, serious
medical illness, and prior suicidal attempt. Male gender and older age
above 50, increase the risk for completed suicide. Recent study suggests
that the risk for suicide associated with alcohol dependence increases
with age. When the age increases mood disorder acts as a powerful risk
factor for suicide among problem drinkers. (Sher et al .,2005).
Alcohol dependence is a the maladaptive pattern of alcohol
use,which leads to clinically significant impairment or distress, Alcohol
dependence is manifested as (i) tolerance; (ii) withdrawal; (iii) taken in
larger amounts (iv) there is a persistent desire or unsuccessful efforts to
cut down or control alcohol use; (v) a great deal of time is spent in
activities necessary to obtain alcohol; (vi) important social, occupational,
or recreational activities are given up or reduced (vii) alcohol use is
continued despite of having a persistent or recurrent physical or
Nicotine abuse, Alcohol abuse, Drug abuse & Obesity are slowly
accelerating death by virtue of their medical complications. Hence, they
are called as chronic Suicide.
LIFE EVENTS:
The suicide attempters had four times of stressful life events six
months prior to the suicide attempts when compared to the general
population . Paykel et al., (1974). Schaffer et al (1974) found that 35% of
the suicidal atempters had recently been in trouble, in their study. Recent
life event are significant in adolescent attempters as in adults according to
Cohen et al, 1982. Broken homes are common among adolescent
self-poisoners than adolescents in the general population (Hawton et al.,
1982). Suicidal attempts most commonly follow quarrels with parents or
close partners (White, 1974 & Hawton et al., 1982).
Individuals with suicidal attempts had elevated levels of stress. The
severity of the suicide depends upon the stressors and chronic strains of
the suicidal attempters (Adams et al., 1994). Marttunen MJ et al, (1993)
reported that precipitant stressors were common in adolescent suicides. In
70% of cases stressors were reported in preceding one month.
Interpersonal separation and conflicts were the most common one.
According to Lewinsohn et al.,(1994), the major potential high risk
depression, family history of suicide attempt, long standing physical pain,
lower academic achievement. If the age group is between 20-30 years, the
amount of stresses will be more. (Helmes, Masuda1974, Dekka, Webb
1974). Childhood physical and sexual abuse and any adversity of their
life may lead to suicide attempt. Hawton et al, (1982) study showed that
the risk factors include chronic emotional problems, behavioral problems,
social isolation related to home, school and physical problem mental
illness. Adolescents with greatest risk of suicidal behavior had family
problem, marital problem, poor parent child attachment, exposure to
sexual abuse in childhood. (Fergusson DM et al, 2000)
MODE OF SUICIDE ATTEMPTS:
In India, most of the suicide attempts were done by using
Insecticides poisonings and corrosive poisonings. Easy accessibility and
unrestricted availability of the poisons are reasons for this common
occurrence. Among the insecticides, organophosporous compounds are
more fatal than other insecticides. Other common modes of poisoning are
Rat killer poisoning, phenyl poisoning, Ant killer poisoning, oleander
poisoning and multiple drugs poisonings . For an individual who has
engaged in selfharm, the risk of dying by suicide is significantly higher
Owens et al, 2002), especially during the first 12 months following
self-harm (Hawton et al, 2003).
According to Ponnudurai et al. (1986) the common causes of
suicides were organophosphorus compounds, sleeping tablet, copper
sulphate, self immolation and oleander seed poisoning in a descending
order of percentages. Previous study says that there was a high correlation
between depression scores and suicidal intent scores in individuals with
this mode of suicidal attempt.
AIM
To study the relevance of life events in individuals with self
injurious behavior.
To identify the personality problems in relation with suicide
attempts.
To know the occurrence of psychiatric illness in self injurious
OBJECTIVES
1 . To estimate the psychosocial stressors in suicidal attempters.
2. To find out the gender variation in suicide attempts
3. To find out the relation between intention and lethality of the
suicide
4. To find out the various personalities in suicides
MATERIALS AND METHODS
SETTING:
This study was conducted in Department of psychiatry at
Government Kilpauk medical college and hospital, conducted for a period
of six months from March 2015 to August 2015. All participants with
suicidal attempts, referred from other departments for opinion have been
selected for this study. The study was approved by ethical committee of
this college. Informed consent was obtained from all participants.
SAMPLE:
Hundred and ten consecutive samples were selected for this study.
STUDY DESIGN:
Cross sectional study
INCLUSION CRITERIA :
Age 15 and above
EXCLUSION CRITERIA:
Acutely ill
INTERVIEW:
All participants have been selected consecutively, written informed
consent was obtained from all the participants. For those with below 18
years, the consent was obtained from parents also. Each individual was
interviewed about half to one hour in the outpatient department..
Individuals were interviewed, and socio demographic profile was
administered, and enquired about mode of attempt, reason for attempt,
whether any intent or not, and any previous suicide attempts, history of
substance abuse if present its pattern, family history of suicide and
substance abuse, any physical and psychiatric illness of the life partner,
assessed and scales were applied to all the participants and counseled on
the same session of the day and if they needed medications were also
INSTRUMENTS USED
1. Semi-structured proforma.
2. Symptom check list scale 90(SCL 90)
3. General health questionnaire 12 (GHQ12)
4. Beck suicide intent scale (SIS)
5. Lethality assessment scale (LAS)
6. Presumptive stressful life events scale( PSLE scale)
7. Eysenck personality questionnaire (EPQ 90)
SEMISTRUCTURED PROFORMA
This proforma was prepared for this study, which consists of name,
age, sex, place, educational status, occupational status, marital status and
used in part 1 of this proforma. In the second part previous suicide
attempt, family history of suicide and substance abuse and mental illness
and physical illness of the spouse and their children were analyzed.
(APPENDIX 1).
SYMPTOMS CHECK LIST SCALE 90
Symptoms check list contains 90 questions and consists of three
domains, which consists of depressive symptoms, psychotic symptoms
and symptoms related to physical illness. Each questions to be answered,
in each question the distress level was divided into 0, 1, 2, 3, 4, as, not at
all, a little bit, moderate distress, quite a bit distress, extremely distress
respectively. Final score was obtained by summed up and divided.
GENERAL HEALTH QUESTIONNAIRE 12
General health questionnaire contains 12 questions. The authors of
this scale was Goldberg and Williams-1988. The GHQ 12 is a measure of
current mental health, which focused on two areas one is the inability to
carryout normal functions and the appearance of distressing experiences.
To be applied to participants and to be asked whether had a particular
symptom or behavior recently, and final score to be summedup . If the
score is 3 and above, is considered as a significant result.
(APPENDIX III)
BECK SUICIDE INTENT SCALE
The author of this scale was Beck et al (1974). This scale contains
3 domains, one is dealing with circumstances and precautions for suicide
another one deals with self report and risk of the suicide. Total scores
ranges from 0-21 and divided into low intent scale (0-3), medium intent
scale (4-10), high intent scale (11and above). This scale result shows
LETHALITY ASSESSMENT SCALE
This lethality assessment scale contains 5 keys ranges from no
predictable risk to very high imminent risk, depending upon the key
scale, the lethality and imminent risk of the suicide will be assessed. This
scale is adopted from Hoff, L. A (1995) (APPENDIX V).
PRESUMPTIVE STRESSFUL LIFE EVENTS SCALE
The presumptive stressful life events scale (PSLE scale) contains
51 items, the ranges of the scores are from 20 -95, most of the subjects
would have had more than one stressors . The stressors were analyzed for
the previous one year by using this scale. Each item to be scored and
finally to be summed up. Then it will be divided into low, medium, high
stress life events based on scores less than 150, 150-300, and more than
300 respectively. This scale is revised from Holmes & Rahe's Social
Readjustment Rating Schedule (SRRS), because many of the categories
EYSENCK PERSONALITY QUESTIONNAIRE 90
The Eysenck personality questionnaire (EPQ 90) contains ninety
questions, this questionnaire to be given to the participants, they should
answer each question by yes or no type and should not omit any question,
for each question they can take not more than few seconds, finally
depends upon the scoring the individual may come under any of the
category like psychotism, neurotism, introverted, extroverted and
STATISTICAL ANALYSIS
1. Chi square test: This test shows the relationship between two
categorical variables. Its value reflects the strength of this
relationship.
2. For continuous variable, t test (2 groups), one way of Analysis of
variance (ANOVA) (more than 2 groups) were used. If the values
are not following normal, Non parametric ANOVA were used.
p value
The probability that a finding has occurred randomly rather than as
a result of a treatment or other intervention. A p value p < 0.05 is often
considered a significant, but the lower this figure, the stronger the
RESULTS
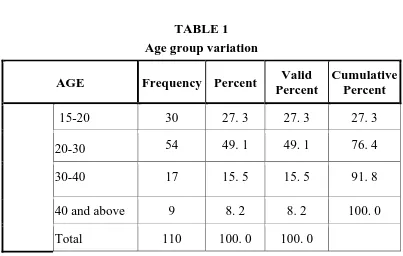
[image:45.612.125.528.87.343.2]TABLE 1 Age group variation
AGE Frequency Percent Valid
Percent
Cumulative Percent
15-20 30 27. 3 27. 3 27. 3
20-30 54 49. 1 49. 1 76. 4
30-40 17 15. 5 15. 5 91. 8
40 and above 9 8. 2 8. 2 100. 0
Total 110 100. 0 100. 0
Table 1 shows, that high number (n=54) of suicides were present in
age group between 20-30 years was 49. 1%, and low percentage were
Table 2 Gender variation
Gender Frequency Percent Valid
Percent
Cumulative Percent
Male 51 46. 4 46. 4 46. 4
Female 59 53. 6 53. 6 100. 0
Total 110 100. 0 100. 0
Table 2 shows, frequency of suicides (n=59) were high in female genders
,the percentage was (53.6%) than males .The male percentage was
[image:46.612.142.502.419.637.2]46.4%(n=51).
Table 3 Educational status
Education Frequency Percent Valid Percent
Cumulative Percent
No formal education
13 11. 8 11. 8 11. 8
Upto twelfth 70 63. 6 63. 6 75. 5
Above twelfth 27 24. 5 24. 5 100. 0
Total 110 100. 0 100. 0
Table 3 shows, higher number of suicidal attempts were present in
percentage was 63. 6% . The individuals who had no formal education
(11. 8%), and who had higher educational level (24. 5%) both these
[image:47.612.127.475.195.465.2]groups had less percentage of suicide attempts.
Table 4. Occupational status
Occupation
Frequency Percent
Valid Percent
Cumulative Percent
Student
Housewife
Employed Unemployed
Total
16 14. 5 14. 5 14. 5
12 10. 9 10. 9 25. 5
63 57. 3 57. 3 82. 7
19 17. 3 17. 3 100. 0
110 100. 0 100. 0
Table 4 shows, suicide attempts were more common in employed persons
(n-63) the percentage was 57. 3% than unemployed persons (n=19)
Table 5 Income status
Income per
month Frequency Percent
Valid Percent Cumulative Percent <10000 10000-25000 >25000 Total
72 65. 5 65. 5 65. 5
34 30. 9 30. 9 96. 4
4 3. 6 3. 6 100. 0
110 100. 0 100. 0
Table 5 shows, high percentage of suicides were present in
individuals with monthly income of less than 10000,per month, they
[image:48.612.137.510.450.611.2]contribute to 65. 5% (n=72).
Table. 6 Marital status Marital status Frequency Percent Valid Percent Cumulative Percent Unmarried married
54 49. 1 49. 1 49. 1
56 50. 9 50. 9 100. 0
Total 110 100. 0 100. 0
Table 6, shows that there were a slightly higher rate of suicide
percentage in unmarried population (n=54) was 49. 1%, and percentage in
[image:49.612.159.439.154.575.2]married population was (n=56) 50. 9%
FIGURE 1.
1=unmarried
2=married
Figure 1, says that married persons contributed slightly higher than the
Table 7
Relation between PSLE scale and Educational status
PSLE scale
Education <150 150-300 >300 Total
Uneducated
10 2 1 13
% within education 76. 9% 15. 4% 7. 7% 100. 0% % within PSLE 12. 3% 8. 3% 20. 0% 11. 8% % of Total 9. 1% 1. 8% . 9% 11. 8% Below
twelfth std
55 11 4 70
% within education 78. 6% 15. 7% 5. 7% 100. 0% % within PSLE 67. 9% 45. 8% 80. 0% 63. 6% % of Total 50. 0% 10. 0% 3. 6% 63. 6%
Above twelfth std
16 11 0 27
% within education 59. 3% 40. 7% . 0% 100. 0% % within PSLE 19. 8% 45. 8% . 0% 24. 5% % of Total 14. 5% 10. 0% . 0% 24. 5%
Total Count 81 24 5 110
% within education 73. 6% 21. 8% 4. 5% 100. 0% % within PSLE 100. 0% 100. 0% 100.
0%
100. 0%
% of Total 73. 6% 21. 8% 4. 5% 100. 0%
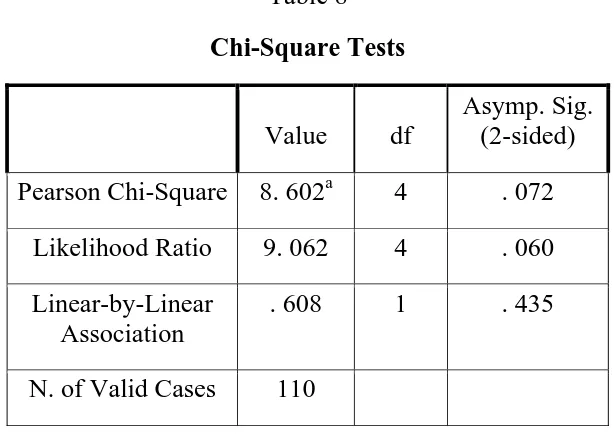
Table 8
Chi-Square Tests
Value df
Asymp. Sig. (2-sided)
Pearson Chi-Square 8. 602a 4 . 072
Likelihood Ratio 9. 062 4 . 060
Linear-by-Linear Association
. 608 1 . 435
N. of Valid Cases 110
Table 7 and 8 shows, the participants were divided into, no formal
education, studied below twelfth standard and studied above twelfth
standard. They had PSLE scores like less than 150, 150-300, >300, and
the percentages were 76. 9%, 78. 6%, 59, 3% respectively and individuals
with below twelfth standard group had highest score (78. 6%) than other
groups. Even though the chi-square does not show significant statistical
result, one important think is 4 of the individuals within a group of below
Figure 1. Relation between PSLE scale and Education
1 = < 150
2 = 150-300
3 = >300
Table 9
Relation between PSLE scale and Occupational status
PSLE scale
occupation <150 150-300 >300 Total
Student
14 2 0 16
% within occupation 87. 5% 12. 5% . 0% 100. 0% % within PSLE 17. 3% 8. 3% . 0% 14. 5% % of Total 12. 7% 1. 8% . 0% 14. 5%
House wife
Count 10 2 0 12
% within occupn 83. 3% 16. 7% . 0% 100. 0% % within PSLE 12. 3% 8. 3% . 0% 10. 9% % of Total 9. 1% 1. 8% . 0% 10. 9%
Employed 46 14 3 63
% within occupn 73. 0% 22. 2% 4. 8% 100. 0% % within PSLE 56. 8% 58. 3% 60. 0% 57. 3%
% of Total 41. 8% 12. 7% 2. 7% 57. 3%
Unemployed 11 6 2 19
% within occupn 57. 9% 31. 6% 10. 5% 100. 0% % within PSLE 13. 6% 25. 0% 40. 0% 17. 3%
% of Total 10. 0% 5. 5% 1. 8% 17. 3%
Total 81 24 5 110
Table 10
Chi-Square Tests
Value df
Asymp. Sig. (2-sided)
Pearson Chi-Square 5. 605a 6 . 469
Likelihood Ratio 6. 518 6 . 368
Linear-by-Linear Association
5. 011 1 . 025
N of Valid Cases 110
Table 9 shows, employed persons had PSLE score 56. 8 % (<150),
58. 3 % (150-300), 60 % (>300), but individuals with unemployment had
PSLE score 13. 6%(<150), 25%(150- 300), 40%(>300), so employed
persons only had high psychosocial stressors than individuals with
unemployment. About 60% of the individuals with employment had
Figure 2
PSLE scale :1=<150
2=150-300
3=>300
Income: 1=<10000/ m, 2=10000-25000/m, 3=>25000/m
The figure 2 shows, highest psychosocial stressors were present in
individuals with income less than 10000 per month, but among the three
Table 11
Relation between marriage and PSLE score
Marital
status PSLE scale
<150 150-300 >300 Total
Unmarried
married
Count 45 10 0 55
% within mar. statu
81. 8% 18. 2% . 0% 100. 0%
% within PSLE 55. 6% 41. 7% . 0% 50. 0%
% of Total 40. 9% 9. 1% . 0% 50. 0%
Count 36 14 5 55
% within mar. statu
65. 5% 25. 5% 9. 1% 100. 0%
% within PSLE 44. 4% 58. 3% 100. 0% 50. 0%
% of Total 32. 7% 12. 7% 4. 5% 50. 0%
Total 81 24 5 110
% within mar. statu
73. 6% 21. 8% 4. 5% 100. 0%
% within PSLE 100. 0% 100. 0% 100. 0% 100. 0%
Table 12 Chi-Square Tests
Value df Asymp. Sig. (2-sided)
Pearson Chi-Square 6. 667a 2 . 036
Likelihood Ratio 8. 603 2 . 014
Linear-by-Linear
Association
5. 799 1 . 016
N of Valid Cases 110
Table 11 and 12 shows, psychosocial stressors were present in both
married (65. 5%) and unmarried populations (81. 8%) but <150 scores
were more in unmarried populations and scores 150-300, (58. 3%), >300
(100%)were present in married populations, which indicates, though the
stressors were present in both groups the severity of stressors were more
in married groups. (p=. 036)
Table 13
Relation between presumptive stressful life events scale (PSLE scale) and Beck suicide intent scale (BECK)
BECK scale PSLE
scale Low medium high Total
<150 63 16 2 81
% within PSLE 77. 8% 19. 8% 2. 5% 100. 0% % within BECK 76. 8% 64. 0% 66. 7% 73. 6% % of Total 57. 3% 14. 5% 1. 8% 73. 6%
150-300 16 8 0 24
% within PSLE 66. 7% 33. 3% . 0% 100. 0% % within BECK 19. 5% 32. 0% . 0% 21. 8% % of Total 14. 5% 7. 3% . 0% 21. 8%
>300 3 1 1 5
% within PSLE 60. 0% 20. 0% 20. 0% 100. 0% % within BECK 3. 7% 4. 0% 33. 3% 4. 5% % of Total 2. 7% . 9% . 9% 4. 5%
Total Count 82 25 3 110
Table 14 Chi-Square Tests
Value df Asymp. Sig. (2-sided)
Pearson Chi-Square 8. 119a 4 . 087
Likelihood Ratio 5. 443 4 . 245
Linear-by-Linear Association 2. 248 1 . 134
N of Valid Cases 110
Table 13 & 14 shows, if the PSLE score is low, the intent of the
suicide will be low likewise if the PSLE score is high the intent of the
suicide also will be high. In low score (<150) of PSLE, the intent in
BECK scale (76. 8%) is low, and in between 150-300 score of PSLE the
BECK scale is (32%) medium, in high score of PSLE >300, the BECK
intent is high(33. 3%). Though it is not statistically significant (p=0. 087)
Figure 3
Figure 3, shows there is no significant correlation between PSLE scores
and lethality of the suicide attempts.
lethality assessment scale-
1- nopredictable risk of immediate suicide
2-low risk of immediate suicide
3-moderate risk of immediate suicide
4-high risk of imminent suicide
Figure 4.
1=low
2=medium
3=high intent
Figure 4 shows, if the suicidal attempter had low intention, the
lethality of the suicide will have no risk and in medium intent, the
lethality will have medium risk, and in high intent the individual may
Table 14.
Relation between personality (EPQ 90) and Type of suicide
Personality SUICIDE
poisoning Hanging Total
Psychotism Count 6 2 8
% within EPQ 75. 0% 25. 0% 100. 0% % within
SUICIDE
5. 8% 28. 6% 7. 3% % of Total 5. 5% 1. 8% 7. 3%
Neurotism
Count 28 3 31
% within EPQ 90. 3% 9. 7% 100. 0% % within
SUICIDE
27. 2% 42. 9% 28. 2% % of Total 25. 5% 2. 7% 28. 2%
Ambivert
55 0 55
% within EPQ 100. 0% . 0% 100. 0% % within
SUICIDE
53. 4% . 0% 50. 0% % of Total 50. 0% . 0% 50. 0%
Introvert
Count 6 1 7
% within EPQ 85. 7% 14. 3% 100. 0% % within
SUICIDE
5. 8% 14. 3% 6. 4% % of Total 5. 5% . 9% 6. 4%
Extravert
8 1 9
% within EPQ 88. 9% 11. 1% 100. 0% % within
SUICIDE
7. 8% 14. 3% 8. 2% % of Total 7. 3% . 9% 8. 2%
Total Count 103 7 110
% within EPQ 93. 6% 6. 4% 100. 0% % within
SUICIDE
Table 14 shows, suicidal attempts were done by psychotism (n=8)
5. 8%, neurotism (n=31) 27. 2%, ambivert (n=55) 53. 4%, introvert (n=7)
5. 85, extrovert personality types (n=9) 7.8%. Suicide by poisoning was
contributed by (n=103) 93. 6%, and the percentage of hangings were
(n=7) 6.4%. Among all the personality types, commonly occurring
personality in poisonings were ambivert type, and hanging was most
[image:63.612.113.533.319.719.2]commonly attempted by neurotic type personality.
Table 15
Relation between Alcohol and Personality type EPQ
Psychotism Neurotism Ambivert Introvert Extrovert
WITHOUT ALCOHOL
WITH ALCOHOL
Count 6 23 39 7 5
% within ALCOHOL
7. 5% 28. 7% 48. 8% 8. 8% 6. 3%
% within EPQ 75. 0% 74. 2% 70. 9% 100. 0% 55. 6%
% of Total 5. 5% 20. 9% 35. 5% 6. 4% 4. 5%
Count 2 8 16 4 30
% within ALCOHOL
6. 7% 26. 7% 53. 3% . 0% 13. 3%
% within EPQ 25. 0% 25. 8% 29. 1% . 0% 44. 4%
% of Total 1. 8% 7. 3% 14. 5% . 0% 3. 6%
Total Count 8 31 55 7 9
% within ALCOHOL
7. 3% 28. 2% 50. 0% 6. 4% 100. 0%
% within EPQ 100. 0% 100. 0% 100. 0% 100. 0% 27. 3%
Table 15 shows, percentage of suicide in personality wise, without
alcohol use were psychotism- 75%, neurotism- 74. 2%, ambivert -70. 9%,
introvert -100%, extrovert - 55. 6% and with alcohol use psychotism
25%, neurotism 25. 8%, ambivert 29. 1%, introvert 0 %, extrovert 44.4%.
Suicide attempt without alcohol intake, in which introvert types were
common(100%) and suicide attempt with alcohol intake, in which
[image:64.612.151.495.329.689.2]extrovert types were common(44.4%).
Table 16
Relation between Suicide and Alcohol SUICIDE
poisoning Hanging Total WITHOUT
ALCOHOL
WITH ALCOHOL
Count 77 3 80
% within ALCOHOL
96. 3% 3. 8% 100. 0%
% within SUICIDE
74. 8% 42. 9% 72. 7%
% of Total 70. 0% 2. 7% 72. 7%
Count 26 4 30
% within ALCOHOL
86. 7% 13. 3% 100. 0%
% within SUICIDE
25. 2% 57. 1% 27. 3%
% of Total 23. 6% 3. 6% 27. 3% 103 7 110 % within
ALCOHOL
93. 6% 6. 4% 100. 0% % within
SUICIDE
Table 16, shows, among the participants (n=80) 72. 7% were not at
all used alcohol, and alcohol users were (n=30) 27. 3% only. Among the
non alcohol users 96. 3% were done suicide attempt by poisoning, 3. 8%
of the participants were attempted for hanging. With alcohol use 25. 2%
of the participants were done suicide attempt by poisoning, and 57. 1% of
the participants were attempted for hanging. So in this study suicidal
poisoning without was common and attempted hanging with alcohol use
[image:65.612.141.489.319.693.2]was common.
Figure 5
1=poisoning
Figure 5 shows, there is no relation between scores in General
health questionnaires 12, and in individuals with suicidal attempt. In both
groups of suicidal attempts, the GHQ 12 scores were predominently less
[image:66.612.131.534.451.616.2]than 3 only.
Table 17
Relation between symptom check list 90 (SCL 90) and Suicide
Suicide
N Mean
Std. Deviation
Std. Error Mean
SCL90 poisoning 103 12. 31 11. 906 1. 173
hanging 7 16. 00 13. 026 4. 923
Table 18
Independent Samples Test
Levene's Test for Equality of Variances
t-test for Equality of Means
F Sig. t df
SCL 90
Equal variances assumed
. 024 . 876 -. 789 108
Table 19
RELATION BEWEEN SYMPTOM CHECK LIST 90(SCL 90) AND RECURRENT SUICIDAL ATTEMPT
RECURRENT N Mean
Std. Deviation
Std. Error Mean
SCL 90
Recurrent 21 21. 76 13. 050 2. 848
First attempt 89 10. 37 10. 636 1. 127
Table 17, 18 and 19, shows there were no statistically significant
test result in relation to suicide and symptom check list 90 questionnaire
and also no relation between SCL 90 and recurrent suicide attempts.
(p=0. 876)
Table 20 COMORBID PSYCHIATRIC ILLNESS
Table 20, shows the only personality disorder commonly presented
with suicide attempts was borderline personality disorder (n=31)
contributing to 28%, the common psychiatric disorder associated with
suicides were depression (n=19) contributes 17% and other disorders like
adjustment disorder (n=3) 2. 7%, alcohol induced psychosis (n=2) 1. 8%,
schizophrenia (n=1) 0. 9%, acute stress reaction (n=1) 0. 9%, conduct
disorder (n=1) 0. 9%. So 52.7% of the participants was suffering from
PSYCHIATRIC
ILLNESS NUMBER PERCENTAGE
Border line personality disorder
31 28 %
Depression 19 17 %
Adjustment disorder 3 2. 7 %
Alcohol induced psychosis
2 1. 8 %
Conduct disorder 1 0. 9 %
Acute stress reaction 1 0. 9 %
Schizophrenia 1 0. 9 %
psychiatric illness. Among the participants 19% (n=21) of them had
deliberate self harm scars (DSH), usually they had a recurrent suicidal
tendency, the duration between DSH to suicidal attempt varied from 6
months to many years in our study.
Among the participants, 30% (n=33) had comorbid substance use
disorder and it varies from harmful use to dependent pattern. 10% of the
participants had suicidal attempts under the influence of alcohol (n=11)
and they attempted by both in insecticide poisoning mode and hanging.
Recurrent suicidal attempts were present in 20% (n=22), in this study
recurrent suicidal attempts were commonly present in borderline
DISCUSSION
This theme is rarely discussed in Indian context. Its needed to consider the personality colouring of these individuals and know how
prone these individuals are to commit deliberate self harm and self
injurious behavior. It is also needed to consider the incidence of severe
mental illnesses in these individuals and how frequently they are prone
for self injurious behavior. In normal individuals without any
psychological disturbances many adverse life events force them for an
impulsive acts of self harm. Hence it is imperative to know about the
modifiable risk factors and the relationship between life events and
deliberate self harm. Hence this study is the need of the hour in the
present context.
AGE:
In this study, self injurious behavior was most commonly occurs
between the age groups of 20-30 years (49.1%). Most of the studies
related to suicide had shown that common age groups for suicide attempt
were between 15-30 years . R.Tara,G.V.Ramana Rao(2014), study shown
that common age group for suicides were between 15-35 years, so our
study had a similar findings as with previous studies. Lewinsohn et al,
hopelessness, recent stressful events, family violence and lower academic
achievement.
Previous study results shown that suicidal behavior increases
markedly during adolescence (Shaffer&Fisher,1981;Brooksband,1985). It
has been found across various studies that the incidence of attemptd
suicide was greatest in young adults (Morgan,et al,1976,Holding et
al.1977).
GENDER:
Our study shows, that frequency of suicidal attempts were
commonly present in females gender (53.6%). R. Tara, G. V. Ramana
Rao study(2014)., had showed that 60% of the suicidal attempters were
female in their studies. White (1974), Otto (1972) and Keith Howton et
al.,(1982), and Indian study by Sudhirkumar et al. (2000) all these studies
indicated that females were the common gender in suicide attempts.
Olfson et al (2005), this study shown that higher incidence of suicides
occur in adolescent females. In compared with previous studies, girls
outnumbered the boys in attempting suicide according to Garfinkel et al.,
(1982), Garfinkel B. D. et al., (1982), Otto (1972),L. Kotila et al., (1987).
EDUCATION:
Our study shows that educated individuals especially those who
have completed below twelfth standard had more vulnerability for
suicidal behavior (n=7) (63. 6%). Nordentoft & Rubin (1993) showed
that there were no difference between attempters and general population
in educational levels. According to previous study results, our study result
does not show any significant variation in educational level in relation to
suicide attempt.
OCCUPATION:
Our study says, compared to unemployed participants, the
participants with employment had a high suicidal rate (57.3%),and also
the level of stressors were more in employed persons. Ramdurg et al
(2012), study had shown, that more suicidal attempts were present in
employed persons than unemployed persons and they assessed the
stressor scores which were high in employed persons. When dealing with
psychosocial stressors in relation to employed persons, the level of
stressors were more in individuals with employment than individuals with
unemployment. R.Tara. G. V.Ramana rao (2014) study shown that, 55%
of the participants attempted suicides were only unskilled workers.
unemployment. So our study results had similar finding as with previous
study results.
MARRIAGE:
Our study results shows that there was a slight increase in suicide
attempts in married populations (50.9%) than in unmarried populations
(49.1%). Fleischmann A et al 2005, study says that increased frequency
of suicides were present in married than unmarried persons and Ramdurg
et al 2012, study also shown the similar findings .In which our study had
a similar finding with previous study. But Unmarried persons had a
higher percentage of suicides according to Ponnudurai et al., (1986),
Ghulam et al., (1995) and Latha et al., (1996) .
ECONOMIC STATUS:
The frequency of suicidal attempts were more common in
individuals with income of less than 10000 per month in our study.
White (1974), Morgan (1975), study shown, that most of the suicide
attempts were come under lower middle socioeconomic status not from
very low socioeconomic status, so our study also had a similar finding as
with previous studies.A study by Thirunavukarasu (1981) have shown
that, increased incidence of suicide in the low income and social status
PSYCHOSOCIAL STRESSORS:
We divided the stressors level into three types like <150, 150-300
and > 300 in PSLE scale. In this study, we found family conflict, marital
conflict and financial loss were the most common stressors in this
participants. Among the participants those who had educational level
below twelfth standard had a highest psychosocial stressors scores
(78.6%).When compared to unemployment, the participants with
employment had high scores in PSLE scale (60%). Osvath et al,(2004).,
reported that 80% of the suicides were due to life events like job problem,
financial problem, unemployment. P. N. Sureshkumar et al,(2013).,
reported in his study that suicidal behaviors were due to psychosocial
stressors like family conflict, financial conflict and marital conflicts.
Our study shows that psychosocial stressors were present in both
married and unmarried populations but high PSLE scores from 150-300,
and above 300 scores were present only in married populations but
Shivkumar et al (2003)., study shown that risk of suicide attempts were
more common in single or unmarried persons. Paykal et al,(1974) study
shown that life events in the preceding years had 4 times higher risk than
the general population. According to Fergusson DM et al (2000), that
adolescents with greatest risk of suicidal behaviour had family problem,
marital problem, poor parent child attachment, exposure to sexual abuse