Dissertation on
“INCIDENCE OF GLAUCOMA IN OCULAR TRAUMA”
Submitted in partial fulfilment of requirements of M. S. OPHTHALMOLOGY
BRANCH III Of
REGIONAL INSTITUTE OF OPHTHALMOLOGY MADRAS MEDICAL COLLEGE
CHENNAI – 600 003
THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY CHENNAI-600 003
CERTIFICATE
This is to certify that this dissertation entitled “INCIDENCE OF GLAUCOMA IN OCULAR TRAUMA” is a bonafide record of the research work done by Dr. A. RANI PRIYADHARSINI, Post graduate in Regional Institute of Ophthalmology, Madras Medical College and Research Institute, Government General Hospital,Chennai-03, in partial fulfillment of the regulations laid down by The Tamil Nadu Dr.M.G.R. Medical University for the award of M.S. Ophthalmology Branch III, under my guidance and supervision during the academic years 2016-2019.
Prof. Dr. M. R. CHITRA, M.S.,
Chief, Glaucoma services ,
Regional Institute of Ophthalmology
Madras Medical College & Research Institute, Govt. General Hospital,
Chennai – 600 008
Prof. Dr. M.ANANDA BABU, M.S. D.O.,
Director and Superintendent,
Regional Institute of Ophthalmology
Madras Medical College & Research Institute, Govt. General Hospital,
Chennai – 600 008
Dr. R. JAYANTHI, M.D., FRCP (Glasg), Dean,
Madras Medical College,
ACKNOWLEDGEMENT
I would like to thank Prof. Dr. JAYANTHI., M.D.,FRCP (Glasg), Dean, Madras Medical College and Research Institute for giving me permission to conduct the study in this Institution.
With due respect and gratitude, I thank Prof.Dr.ANANDA BABU, M.S., D.O., Director and superintendent, Regional Institute of Ophthalmology and Govt. Ophthalmic Hospital, Chennai for permitting me to conduct this study.
Prof.Dr.M.R.CHITRA M.S., Unit Chief, Glaucoma services, and my guide for assigning me this topic for study and guiding me throughout my Post graduate course. I wish to express my sincere thanks for the valuable help, encouragement and guidance at various stages of the study.
My sincere thanks to my Assisstant Professors Dr.R.SARAVANAN, M.S., Dr.T.VIMALA M.S., Dr.C.USHA M.S., D.O., for their timely help and guidance in conducting this study.
I wish to express my sincere thanks to my family, friends and all my colleagues who helped me in bringing out this study.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled, “INCIDENCE OF GLAUCOMA IN OCULAR TRAUMA” is a bonafide and genuine research work conducted by me under the guidance of Prof. Dr. M. R. CHITRA, M.S., Head of Department of glaucoma services, Regional institute of ophthalmology & Government Ophthalmic Hospital. Chennai - 600008.
Dr. A. RANI PRIYADHARSINI
CONTENTS
S.NO TITLE PAGE
NUMBER PART – I
1. INTRODUCTION 1
2. ANATOMY OF ANGLE STRUTURES AND
GONIOSCOPY 2
3. AQUEOUS HUMOR DYNAMICS 8
4. TONOMETRY 16
5. OPTIC NERVE HEAD ANATOMY AND FUNDUS
CHANGES IN GLAUCOMA 24
6. AETIOPATHOGENESIS OF TRAUMATIC GLAUCOMA 29
7. INVESTIGATIONS IN TRAUMATIC GLAUCOMA 51
8. REVIEW OF LITERATURE 65
PART II
9. AIM AND OBJECTIVES 69
10. MATERIALS AND METHODS 70
11. RESULTS 72
12. DISCUSSION 83
13. CONCLUSION 86
PART III
14. BIBLIOGRAPHY 87
15. PROFORMA 89
16 PATIENT INFORMATION FORM 91
17. PATIENT CONSENT FORM 93
18. KEY TO MASTER CHART 94
19. MASTER CHART 98
20. ETHICAL COMMITTEE APPROVAL 107
1
INTRODUCTION
DEFINITION OF GLAUCOMA
Glaucoma is a chronic, progressive optic neuropathy which leads to
characteristics optic nerve head changes with corresponding visual field defect in
which raised intraocular pressure, is the only modifiable risk factor.
CLASSIFICATION OF GLAUCOMA
Classification based on aetiology
A] Primary
B] Secondary
Classification based on mechanism of aqueous outflow obstruction
through anterior chamber angle
A] Angle closure glaucoma
a. Anterior (Pulling mechanism)
1. Contracture of membranes in anterior chamber angle
2. Contracture of inflammatory precipitates
b. Posterior (Pushing mechanism)
1. with pupillary block
2. without pupillary block
B] Open angle glaucoma
a. Pretrabecular (membrane overgrowth)
b. Trabecular (occlusion of intertrabecular spaces)
2
C] Developmental glaucoma
a. High insertion of iris
b. Incomplete development of trabecular meshwork
c. Iridocorneal adhesion
ANATOMY OF ANGLE STRUCTURES:
Angle structure from posterior to anterior –
Ciliary body
Scleral spur
Trabecular meshwork
Schwalbe’s line
Ciliary body – anterior part of ciliary body which lies between the iris root and
scleral spur
Scleral spur- scleral spur is the posterior lip of scleral sulcus. Anteriorly, it is
attached to the corneoscleral meshwork and posteriorly to the longitudinal fibres of
ciliary body. It prevents the collapse of schlemm’s canal.
Trabecular meshwork- it is formed by three portions.
Innermost portion is uveal meshwork, which bridges the iris root and ciliary
body. It has many irregular openings.
Middle one is the corneoscleralmeshwork which is attached anteriorly to
3
Outermost part is the juxtacanalicular meshwork which is lined by
endothelium. It forms a narrow channel between the corneoscleral meshwork and
schlemm’s canal.
Schwalbe’s line- it is termination of descement’s membrane.
GONIOSCOPY
It is the procedure to visualise the anterior chamber angle. It is used for both
therapeutic and diagnostic procedures.
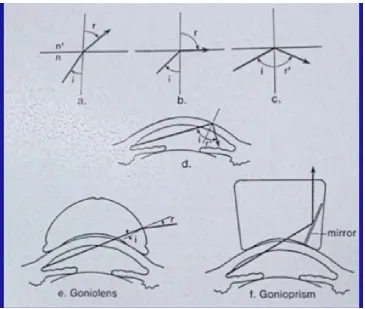
Principles of gonioscopy
• Anterior chamber angle cannot be visualised directly through the intact cornea because light rays from angle structures undergoes total internal
reflection.
• Critical angle – when the light rays travel from higher medium to lower
refractive index (such as from cornea to air), it will be reflected between the
two unless the angle of incidence is less than the critical angle depending
on their refractive index difference.Normal critical angle is 46º for the
4
Figure 1.
A: Light ray is refracted when angle of incidence (i) at interface of two media with
different indices of refraction (n and n) is less than the critical angle.
B: Angle of refraction (r) is 90 degrees when i equals the critical angle.
C: Light is reflected when i exceeds the critical angle.
D: Light from the anterior chamber angle exceeds the critical angle at the
cornea-air interface and is reflected back into the eye.
E and F: Contact lenses have an index of retraction (n) similar to that of the cornea,
allowing light to enter the lens and then be refracted (goniolens) or reflected
(gonioprism) beyond the contact lens-air interface.
5
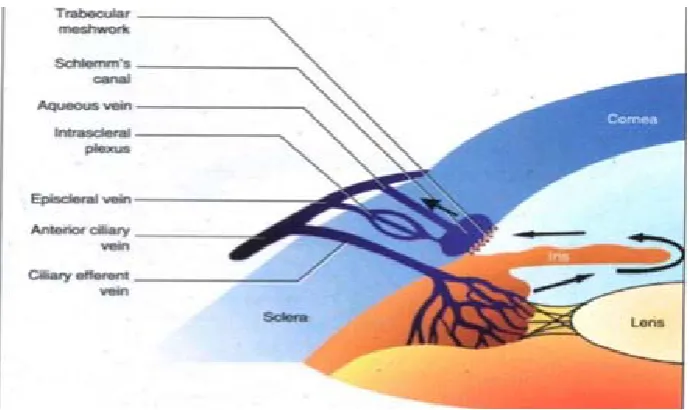
[image:11.595.92.495.101.408.2]GONIOSCOPIC FINDING OF ANGLE STRUCTURE
Figure 2. Angle of Anterior Chamber
Ciliary body (CBB) – It is grey or dark brown in colour. It is wider in
myopes and narrow in hypermetropes.
Scleral spur (SS) - It is a prominent white line located immediately posterior
to the trabeculum. It may be obscured by iris process, iris bombe, peripheral anterior
synechiae.
Trabecular meshwork (TM) –it extends from schwalbe’s line to scleral spur.
It looks faint tan to dark brown. The pigmentation increases with age. Anterior part
of trabecular meshwork is non-functional. The posterior pigmented part is functional
6
Schwalbe’s line- A fine ridge anterior to trabecular meshwork which is
identified by a small build up of pigments. Corneal wedge is useful to identify the
inconspicuous schwalbe’s line. It helps to differentiate wide open with non
pigmented trabecular meshwork (eg; young patients) and angle closer.
Indentation Gonioscopy – It helps to differentiate appositional vs synechiael angle
closure.
GRADING OF ANGLES
Shaffers and Modified Shaffers grading
Grade Angle
width Configuration
Chances of closure
Structures visible on Gonioscopy
0 O degree Closed Closed No angle structures visible
I 10 degree Very narrow High Schwalbe’s line only
II 20 degree Moderately
narrow Possible
From schwalbe’s line to trabecular meshwork
III 20-
35degree Open angle Nil
From schwalbe’s line to
scleral spur
IV 35-45
degree Wide open Nil
7
Limitation of Gonioscopy
Cannot be performed in painful inflamed eye
Hyphema
Compromised cornea
Lacerated or perforated globe
Gonioscopy can be done 6 to 8 weeks after traumatic hyphema.
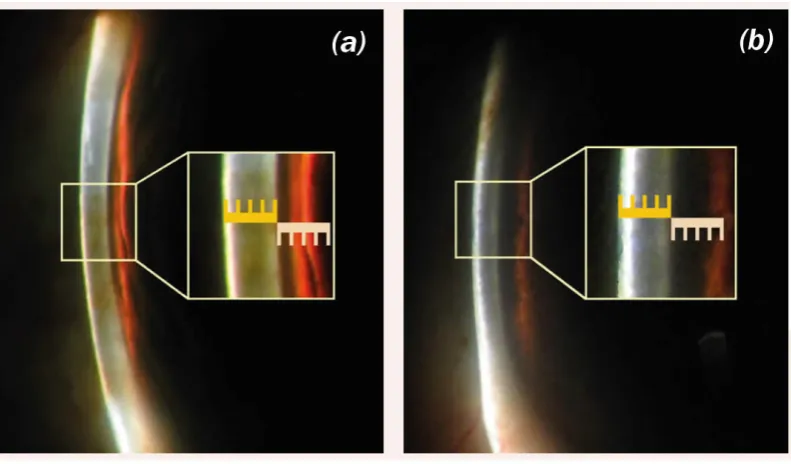
LIMBAL CHAMBER DEPTH IS ESTIMATED BY MODIFIED VAN
HERICK GRADING
On slit lamp examination, the brightest, narrowest, vertical beam of light is
focused at the temporal limbus with the illumination column at 60º from the axis of
microscope. Under maximum magnification, the beam should be kept at the most
peripheral point of temporal limbus.
Closed
angle Absent peripheral anterior chamber
Slit angle Anterior chamber depth extremely shallow
Grade 1 Anterior chamber depth < ¼ corneal thickness
Grade 2 Anterior chamber depth more than ¼ corneal thickness
Grade 3 Anterior chamber depth ¼ to ½ corneal thickness
8
Figure 3. a) Van Herick grade 1 b) Van Herick grade 4
AQUEOUS HUMOR FORMATION
Aqueous humor is secreted by non pigmented epithelial cells of ciliary
process in to posterior chamber, it reaches the anterior chamber via pupil. Aqueous
humor drained through the trabecular meshwork (conventional pathway) and
uveoscleral flow (unconventional pathway)
MECHANISM OF AQUEOUS HUMOR FORMATION
1. Ultrafiltration (under hydrostatic pressure)
2. Active secretion (against electrochemical process)
[image:14.595.110.506.71.303.2]9
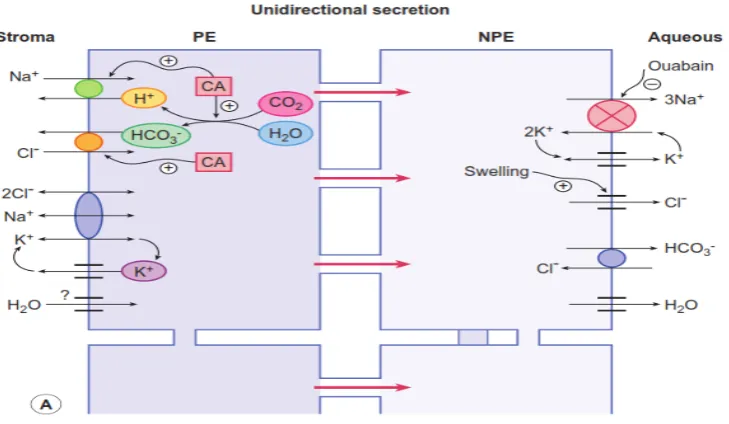
Figure 4. Aqueous Humor Formation
Ciliary processes are the site of aqueous humor formation. Aqueous humor
derived from plasma within the capillary network of ciliary processes. Presently it
agreed that diffusion, ultrafiltration and secretion play arole in aqueous production
at different levels. Major factors are active secretion (70%), ultrafiltration (20%)
and osmosis accounts for 10%.
Plasma secreted into the ciliary process stroma from the ciliary capillaries
due to ultrafiltration and diffusion.
Then it transports into the pigment epithelial cells from stroma by active
transport. Following mechanism are mainly involved in this process:
1. Na+K+2Cl- symport
2. Na+H+ antiport
3. Cl- HCO
10
Then it transports into nonpigmented epithelial cells with low resistance from
pigmented epithelial cell.
Then it transports to posterior chamber by active transport.
VARIOUS SECRETORY PROCESSES
• Sodium
Na-K ATPase
Na –K-2Cl symport
Na-H antiport, Cl-HCO3 antiport
• Bicarbonate
Maintain pH and proper function of Na-K ATPase.
• Potassium
Transport by active secretion and diffusion
• Chloride
Affected by pH and Na+ ion concentration
Rate limiting step in Aqueous flow
• Water
Transport through aquaporin channel
• O2 and glucose pass the BAB by simple and facilitated diffusion.
• Ascorbic acid
11
AQUEOUS HUMOR
It maintains structural integrity of the eyeball and intraocular pressure
It provides clear medium for optical property
It provides nutrition, delivers oxygen and eliminates metabolic waste
It delivers antioxidant like ascorbate and provides local immunity
PHYSIOLOGICAL CHARACTER
pH - 7.2,
Refractive index – 1.36
Osmotic pressure higher than blood
Specific gravity slightly more than water
Total volume – 0.31ml, anterior chamber- 0.25ml, posterior chamber – 0.05ml
Rate of formation – 2 to 2.5microlitre (1% of AC volume/ min)
COMPOSITION
Inorganic ions- increase chloride content, decrease bicarbonate than plasma
Organic ions- lactate, ascorbic acid (30 fold higher than plasma), hyaluronic
acid, hydrogen peroxide.
Carbohydrate, glutathione and urea
Less protein
12
BLOOD AQUEOUS BARRIER
Adjacent non pigmented epithelial cells connected by tight junctions in
apical portion of the cells, forms a blood aqueous barrier.
[image:18.595.172.451.213.542.2]It maintain the chemical composition between the plasma and aqueous
Figure 5. Blood aqueous barrier
AQUEOUS HUMOR DRAINAGE
Conventional or Trabecular pathway (80 -90%)
13
Trabecular pathway
Uveal meshwork
Corneoscleral meshwork
Juxta canalicular trabecular meshwork Trabecular meshwork
Trabecular meshwork
Schlemm’s canal
Aqueous vein of ascher
Episcleral vein conjunctival vein
Anterior scleral artery and angular and palpebral vein
Superior ophthalmic vein
Facial vein and superior
ophthalmic vein
14
Mechanism of aqueous humor transport to schlemm’s canal:
Leaky pores in endothelial cells
Microfilaments contracture
Vacuolation theory
[image:20.595.135.480.218.423.2]Aqueous outflow pump
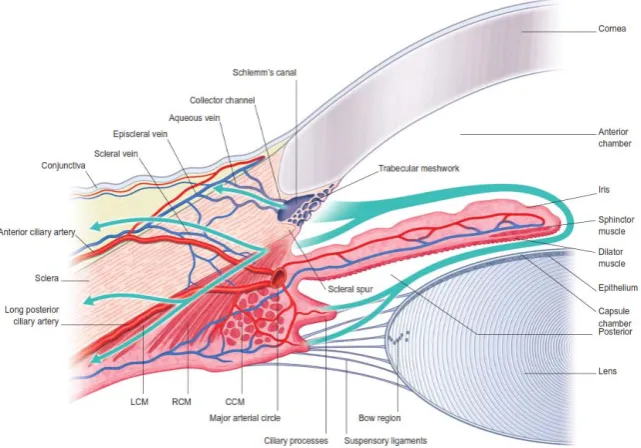
Figure 6. Aqueous outflow system
UVEOSCLERAL OUTFLOW
Pressure independent (10 to 20%)
0.3micro litre /min and independent of IOP
Ciliary body
Suprachoroidal space
Ciliary body venous circulation
Choroid
Sclera
15
Figure 7. Uveoscleral Outflow
Factors affecting blood aqueous barrier
Trauma to the iris (contusion, iridodialysis, sphincter tear)
Mechanical trauma to the lens
Chemical injury like acid, alkali, formaldehyde
Inflammatory mediators
Trigeminal nerve stimulation
Factors affecting aqueous formation
Diurnal variation- 1.5 to 4.5 micro litre /min. aqueous humor production
increase in morning 8 AM to noon. Decrease in midnight to early morning 6AM.
Age
16
Inflammation
Breakdown of blood brain barrier
Blood flow to ciliary body
Factors affecting aqueous outflow
Age
Myopia
Diabetes mellitus
Steroid
Inflammation (inflammatory cells clogged the trabecular meshwork)
Trauma (breakdown of blood aqueous barrier, hyphema, late closure of
cyclodialysis cleft) and Drugs
TONOMETRY
IDEAL TONOMETER
• Should give accurate and reasonable IOP measurement
• Convenient to use
• Simple to calibrate
• Free of maintenance problems
17
TYPES OF TONOMETRY
Newer tonometers
Trans-palpebral tonometry
Dynamic contour tonometry
Ocular response analyser
18
Digital tonometry / Palpation method:
It is an indirect method of measuring the IOP.
Intraocular pressure (IOP) is estimated by response of eye to pressure applied by
finger.
PROCEDURE: Ask the patient looks down and place the Index finger of both
hands over the closed eyelids. One finger is kept stationary which feels the
fluctuation produced by the indentation of globe by the other finger.
GOLDMANN APPLANATION TONOMETRY
It is the Gold standard method for measurement of intraocular pressure.
It is a type of variable force applanation tonometer.
It determines the force necessary to applanate an area of cornea of 3.06 mm
in diameter.
Principle:
Modified Imbert ficks law
It states that the pressure inside an ideal dry, thin walled sphere equals the
force necessary to flatten its surface divided by the area of flattening.
P= F/A
At 3.06 mm of corneal diameter, the resistance to flattening is
counterbalanced by the capillary attraction of the tear film meniscus for the
19
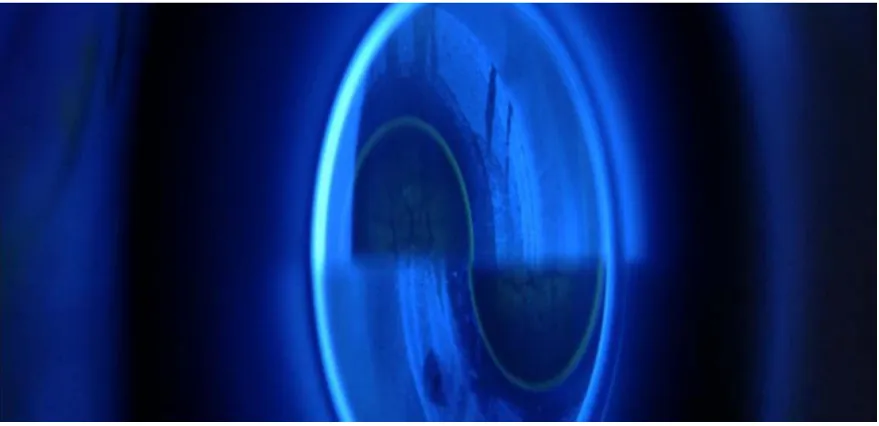
Figure 8. Goldmann Applanation Tonometry
Procedure
Patient is asked not to drink large quantity of fluids for two hours before doing
the test
Explain the procedure to the patient. The patient is instructed to relax, maintain
the position, holds the eye wide open.
Then, one drop of topical anesthesia is placed in each eye, commonly used is
0.5% proparacaine. Moistened fluorescein strip is placed in the lower fornix to stain
the eye.
Contact lens should be removed before fluorescein staining because it stains
the contact lens.
Before using the tonometer tip, we have to clean it with sterilizing solution and
20
The tension knob is set at one grams. If the knob set as 0, the prism head will
vibrate when it touches the eye and produce corneal abrasion.
The 0 mark of the prism is set at white line on the prism holder. Then
illuminate the prism head with cobalt blue filter opened maximally.
The angle between the illumination column and the microscope axis should
be 60º.
The microscope is advanced towards the patient with the examiner observing
from the side until the limbal zone has a bluish hue. The prism should not touch the
lids or lashes.
When viewed monocularly two fluorescent semicircles are seen through the
biprism. The fluorescein rings undergo rhythmic movement in response to cardiac
cycle.
Adjust the tension knob until the inner edges of the two semicircle touch each
other at the midpoint of their pulsations.
Contraindication:
Active eye infection
21
POTENTIAL ERRORS:
Falsely low IOP
Too little fluorescein
Thin cornea
Corneal edema
With the rule astigmatism
Prolonged contact
Repeated tonometry
Falsely high IOP
too much fluorescein
thick cornea
steep cornea
against the rule astigmatism
1mm Hg per 3D
wider meniscus
Widening the lid fissure
excessively
Elevating the eyes more than
15°
Normal intraocular pressure -11 to 21mmHg.
IMPACT-REBOUND TONOMETER (ICARE)
It is an updated version of an indentation tonometer.
It consists of pair of coils coaxial with probe shaft, a solenoid coil and sensing coil.
PROCEDURE
22
The time taken for the probe to return to its resting position and the
characteristics of the rebound motion are indicates IOP and biomechanical
properties of the cornea.
Time taken
longer in eyes with lower IOP and
[image:28.595.107.508.273.529.2] faster in eyes with higher IOP.
Figure 9. I care
ADVANTAGES
Icare can be used without anesthetizing the eye because the probe is extremely light and its contact with the cornea is very short .
Used in situations when patients are unable to be seated or measured at the
23
DISADVANTAGES
Tend to read slightly higher than the Goldmann.
Accuracy falls off in scarred corneas.
Mackay marg tonometer
Principle - constant area and variable force, applanation contact tonometer.
It is used for the measurement of IOP in eyes with edematous, scarred or irregular
cornea.
It is also accurate when used over therapeutic or soft contact lens
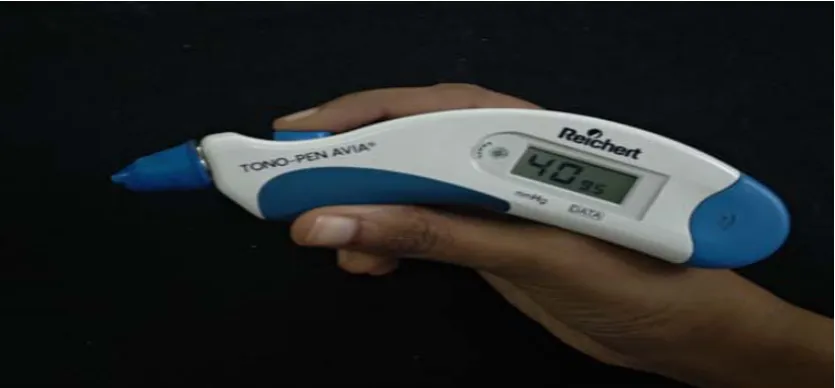
Tonopen :
Principle- same principle of mackay marg tonometer
Its portable and battery operated.
The probe tip is protected by disposable latex which reduces infection
transmission.
[image:29.595.99.517.523.717.2]The device displays the average of 10 independent reading.
24
OPTIC NERVE HEAD ANATOMY
The normal optic nerve consist of 1.2 million axons which originate from the
the cell bodies of the ganglion cells of the retina. The distal part of the optic nerve
is optic nerve head. Nerve fibres arise from the ganglion cell layer which travel in
the superficial retinal nerve fibre layer. Then they make 90º turn and remain at the
outer edge of optic nerve head which is called as neuro- retinal rim. The axons from
the central region occupies the superficial layer of retina. The neuroretinal rim is
reddish orange in colour because it consist of capillaries, glial cells and astrocytes.
The axons exit the globe through the lamina cribrosa. Optic cup is the centre of optic
nerve head which is pale due to visibility of lamina cribrosa and connective tissues.
DIVISIONS OF OPTIC NERVE HEAD
Surface nerve fibre layer- it is formed by the axons of ganglion cells which
is supplied by the retinal arteries and intraocular branches of central retinal artery.
Prelaminar region- it is composed of axons, astrocytes and astroglial tissue
which are more than surface nerve fibre layer. This region receives blood supply
from the direct branches of posterior ciliary arteries.
Lamina cribrosa- it consists of series of fenestrated collagen plates, through
which axons of nerve fibre layer pass to the retrolaminar region. Larger pores and
less connective tissue support are present in inferior and superior areas. It receives
25
The retrolaminar region- Myelinated axons start from this region. It receives
blood supply from posterior ciliary arteries and small branches from central retinal
artery and pial plexus.
OPTIC NERVE HEAD EVALUATION
There are various methods to measure optic nerve head clinically:
Direct ophthalmoscope- The Welch-Allyn 5º spot light diameter is 1.5 which
is used to measure the optic disc size.
Slit-lamp biomicroscopy- On slit-lamp examination with hand held high
power convex lens like volks 60D (magnification 1×), 78D (×1.1), 90D(×1.3), optic
nerve head can be measured. These measurements are not influenced by distance of
the lens or by refractory errors up to 8D of ametropia but influenced by axial length.
FUNDUS CHANGES IN GLAUCOMA
Normal optic disc is vertically oval, 1.5 mm in diameter. Neuro retinal rim
lies between disc margin and cup. Normally it is pink in color. It follows ISNT rule.
That implies, inferior neuro retinal rim is the broadest, followed by superior, nasal
and temporal neuro retinal rim. As glaucoma advances, neuro retinal rim will be
thinned out and lost.
CUP DISC RATIO
• It is expressed as diameter of the cup as a fraction of diameter of optic disc.
Vertical cup disc ratio is more important than horizontal cup disc ratio,
because pores are larger in superior and inferior poles and also less glial
26 • Cup disc ratio of > 0.3 or
• Asymmetry of cup disc ratio >0.2 between two eyes are considered
significant.
[image:32.595.125.485.190.425.2]• Disc size is also important while measuring cup disc ratio
Figure 11. Neuro Retinal Rim Thickness
[image:32.595.151.463.480.730.2]27
Laminar dot sign – it is due to loss of neural tissues, leading to exposure of
underlying laminar pores.
BARING OF CIRCUMLINEAR VESSEL
As the neuroretinal rim recedes, normal circumlinear vessel which outlines
the cup will be bared from cup margin.
BAYONETTING OF VESSELS- Double angulation of the vessels
Due to loss or absent of neuroretinal rim, the vessels pass through the
[image:33.595.174.442.340.534.2]overhanging edges of the cup and take sharp angulation at the cup margin.
Figure 13. This picture depicts Cup disc ratio 0.9, circumferential Neuroretinal rim thining and bayonetting of vessels
RETINAL NERVE FIBRE LAYER
Retinal nerve fibre layer will be seen as striations in light reflex. On red free
filter retinal nerve fibre layer defects can be visualized as darker areas of slit or
28
PERIPAPILLARY PIGMENTATION
There are 2 zones, alpha and beta zones.
- Beta zone lies between outer alpha and optic disc margin. It occurs due to
atrophy of retinal pigment epithelial layer, reduction in photoreceptors and choroidal
degeneration. Changes in Zone beta is significant in glaucoma. It produces absolute
scotoma.
- Zone alpha is the outer zone, which lies external to beta zone. It occurs due
[image:34.595.94.527.372.599.2]to retinal pigment epithelial changes.
29
TRAUMATIC GLAUCOMA
Traumatic eye injury is one of the most common causes of unilateral
blindness worldwide. Glaucoma is a common and often devastating consequence of
ocular trauma.
Traumatic glaucoma can be present as secondary open angle or secondary
closed angle glaucoma. Transient or prolonged elevation of intraocular pressure in
early or late phase after trauma which damage the trabecular meshwork and other
structures predisposing traumatized eye to the development of glaucomatous optic
nerve head changes.
Traumatic glaucoma can occur in following condition
1. Blunt injury
2. Penetrating injury
3. Chemical injury
4. Thermal injury
5. Radiation exposure
30
MECHANISM OF GLAUCOMA FOLLOWING OCULAR TRAUMA
GLAUCOMA FOLLOWING BLUNT INJURY
a. Early onset
1. Trauma to trabecular meshwork
2. Inflammation
3. Hyphema
4. Traumatic lens subluxation with pupillary block
5. Traumatic lens swelling with pupillary block
6. vitreous filling the anterior chamber
7. Schwartz matsuo syndrome (fluctuation in intraocular pressure associated
with retinal detachment accompanied by tears of nonpigmentary epithelium
of the ciliary body.)
b. delayed onset
1. Angle recession
2. Ghost cell glaucoma
3. Hemolytic glaucoma
4. Peripheral anterior synechiae
5. Posterior synechiae with pupillary block
31
Figure 15. Iridodialysis
GLAUCOMA FOLLOWING PENETRATING INJURY
a. Flat anterior chamber with formation of peripheral anterior synechiae
b. Inflammation
c. Ghost cell glaucoma
d. Hyphema
e. Lens subluxation with pupillary block
f. Traumatic lens swelling
g. Lens particle glaucoma
h. Epithelial downgrowth
i. Fibrous ingrowth
32
Figure 16. Postop central corneal tear suture with subconjuctival hemorrhage
CHEMICAL INJURY
TYPES OF CHEMICAL INJURY
Alkaline agents
It will penetrate the ocular tissues deeply and may lead to glaucoma. Dicrotic
pressure rise is noted - immediate pressure rise followed by normal pressure for
sometimes and again rise in intraocular pressure.
Acidic chemicals
33
Mechanism of raised intraocular pressure following chemical injury
1. Early phase ( minutes to hour) due to scleral shrinkage and prostaglandin
release
2. Intermediate phase due to inflammation, acute swelling of lens and posterior
synechiae
3. Late phase ( weeks to months) due to trabecular scarring and formation of
posterior synechiae
Management
Early phase- Antiglaucoma drugs like Beta-adrenergic antagonist, Alpha2
adrenergic agonist, carbonic anhydrous inhibitors and hyperosmotics.
Intermediate phase-
Topical corticosteroids use with caution, because of the risk of stromal
lysis.
Oral corticosteroids - to reduce inflammation.
Cycloplegic/ Mydriatics- to alleviate pain, prevent synechiae formation.
Late phase
Filtering surgery
Glaucoma shunt device
34
THERMAL INJURY
Rarely cause raised intraocular pressure
Mechanism of raised intraocular pressure is due to orbital congestion and
massive periorbital swelling
Treatment- lateral canthotomy
RADIATION DAMAGE
Raised intraocular pressure is due to neovascular glaucoma or intraocular
hemorrhage. It has a poor prognosis.
ELECTRICAL SHOCK
Raised intraocular pressure due to venous dilatation, contracture of
extraocular muscle and pigment dispersion.
CAUSES OF OPEN ANGLE GLAUCOMA IN OCULAR TRAUMA
Early – Inflammation, Hyphema and Lens particle glaucoma.
Late – Angle recession glaucoma, Ghost cell glaucoma, Hemolytic glaucoma, and
Retained intraocular foreign body (e.g: Hemosiderosis glaucoma)
CAUSES OF CLOSED ANGLE GLAUCOMA IN OCULAR TRAUMA
Early causes
1. Flat anterior chamber leading to peripheral synechiae,
2. Anterior subluxation of lens with pupillary block,
3. Anterior dislocated lens with pupillary block,
35
Late causes
1. posterior synechiae with pupillary block,
2. Peripheral anterior synechiae,
3. Epithelial ingrowth
4. Late closure of ciliary cleft
5. Fibrous downgrowth
TRAUMATIC IRITIS
Traumatic iritis produces both open angle and closed angle glaucoma. In
acute inflammation IOP is low, due to ciliary shock and reduced aqueous
production.
Distruption of blood aqueous barrier causes release of protein and
inflammatory cells in anterior chamber which results in increased viscosity of
aqueous humor.
Trabecular meshwork is obstructed by inflammatory cells and debris
Scarring and dysfunction of outflow channels (trabecular meshwork)
Forward displacement of iris- lens diaphragm by uveal effusion
Neovascularization in the angle
Posterior synechiae with pupillary block
Peripheral anterior synechiae
36
CLINICAL FEATURES
Pain, redness, photophobia, defective vision
Corneal edema, circumcorneal congestion
Anterior chamber – flare, cells
TREATMENT
Topical Cycloplegics - to reduce ciliary spasm, prevent the formation of
synechiae, break the formed synechiae, reduce release of inflammatory cells, open
the corneal lamellae to increase drug penetration
Topical corticosteroids (used with caution because of possibility of steroid
induced glaucoma)
Filtering surgery with adjuvant antimetabolite therapy
Glaucoma drainage device such as Molteno, Baerveldt, and Ahmed implants.
HYPHEMA
DEFINITION
Blood in the anterior chamber of the eye is called hyphema. It results from
iris or ciliary body tear leading to bleeding from anterior ciliary and iris stromal
vessels. Hyphema occurs in both blunt and penetrating injury.
Sickle cell patients are more prone for rebleed and glaucomatous changes
37
PATHOGENESIS
In penetrating injury, hyphema develop by direct injury to the iris, ciliary
body, trabecular meshwork and their blood vessels.
In blunt trauma, due to compressive force on eyeball, it causes stretching of
the limbal tissue, scleral expansion, peripheral displacement of aqueous, increase
the pressure in the angle which injure the angle structures (tear in the anterior face
of ciliary body), iris (iridodialysis, sphincter tear, iridoschisis), lens and posterior
segment.
MECHANISM
Obstruction of trabecular meshwork by blood cells and fibrin
Secondary fibrosis and descemetization of angle leads to late rise in
intraocular pressure which is very rare.
GRADING OF HYPHEMA
Grading by volume of anterior chamber filled with blood after layering of the
red blood cells.
Grade I Less than one third of anterior chamber
Grade II One third to one half of the anterior
chamber
Grade III One half to nearly total
38
Figure 17. Grading of hyphema
[image:44.595.94.528.373.657.2]39
MANAGEMENT
Conservative management
Monitor daily for 3 to 5 days to look for rebleed and measurement of
intraocular pressure.
Bed rest in semi upright posture, limitation of activity to prevent rebleed.
Discontinue use of anticoagulant medications if any.
Antifibrinolytic agents such as Aminocaproic acid or tranexamic acid
Usually total resorption occur within 5 to 7days.
Patient with raised intraocular pressure
Medical management-
Topical Cycloplegics- to alleviate pain by relieving ciliary spasm, prevent
posterior synechiae formation.
Topical steroids and oral steroids- inhibition of fibrinolysis and stabilization
of blood ocular barrier.
Antiglaucoma medications- beta blockers, alpha2 adrenergic agonist, carbonic
anhydrase
Inhibitors (should not be used in sickle cell patients). In cases of intraocular pressure
more than 30mmHg, intravenous mannitol 200ml IV every 12hours should be given.
Surgical management-
Anterior chamber irrigation and aspiration
Indications:
To prevent corneal staining
40
Failure in the control of intraocular pressure elevation medically
One proposed guidelines for intervention are IOP of 60mmHg for 2days
IOP of 50mmHg for 5days
IOP of 35mmHg for 7days.
If IOP higher than 30mmHg for more than 24hours in sickle cell patients, surgical
intervention should be considered.
• Intracameral injection of tissue plasminogen activator
COMPLICATIONS
Corneal blood staining
Rebleeding
Pupillary block
Peripheral anterior synechiae, posterior synechiae
Amblyopia (early intervention is needed in pediatric hyphema)
ANGLE RECESSION GLAUCOMA
It is a type of secondary open angle glaucoma.
Angle recession refers to a tear between the circular and longitudinal fibres
of the ciliary body.
Presents with an elevated intraocular pressure up to years after blunt
trauma.
This condition may be underdiagnosed because onset is often delayed and
because of history of injury may be distant or forgotten.
Clinically, patients with angle recession glaucoma are usually detected
41
CLINICAL FEATURES
Anterior chamber- deep or irregular
Signs of previous injuries like iridodialysis, iris sphincter tear, rosette
shaped cataract, trabecular meshwork pigmentation.
Gonioscopy – angle recession (irregular widening of ciliary body band)
seen
Chances of developing glaucoma in angle recession:
Angle recession <180 degrees- glaucoma is unusual
Angle recession >180 degrees - 4 to 9%
[image:47.595.90.541.401.699.2]Angle Recession >270 degrees- higher risk of chronic glaucoma
Figure 19. Angle recession
42
PATHOGENESIS
Blunt injury to the globe
Sudden indentation of cornea
Anteroposterior compression
Equatorial expansion
Hydrodynamic effect which displaces aqueous laterally
Shearing force applied to the angle structure shearing of anastomosing
branch of
Anterior ciliary arteries
Tear between the longitudinal and
Circular muscle of ciliary body HYPHEMA
ANGLE RECESSION
Trabecular dysfunction
CHRONIC Elevated IOP
43
Figure 20. Blunt Injury
TREATMENT
Antiglaucoma medications - Beta blockers, Alpha adrenergic agonists,
carbonic anhydrase inhibitors, prostaglandin analogues.
If medical therapy fails, surgical management is advisable.
Surgical procedures
Trabeculectomy with antimetabolites
Glaucoma drainage devices
Laser therapies- Nd: YAG laser trabeculopuncture
Argon laser trabeculoplasty
44
GHOST CELL GLAUCOMA
It occurs in intraocular haemorrhages especially in vitreous hemorrhage.
It is a type of secondary open angle glaucoma in which degenerated red
blood cells (ghost cells) in the vitreous cavity enter the anterior chamber through the
disrupted anterior hyaloid face and obstruct the aqueous outflow facility.
Following trauma, surgery or retinal disease, blood enters the vitreous
cavity. Fresh erythrocytes in the vitreous cavity transformed into ghost cells which
are khaki coloured, spherical and less pliable. So it cannot pass readily through the
trabecular meshwork and accumulate there leading to temporary obstruction of
aqueous outflow.
Clinical features
Pain, corneal edema, pseudohypopyon which is rarely associated with a layer
of fresh red blood cells ( candy stripe sign) khaki coloured cells in anterior chamber,
corneal endothelium and angle of anterior chamber.
DIAGNOSIS
Ghost cell glaucoma is confirmed by anterior chamber paracentesis,
aspirated fluid is tested under phase contrast microscopy or millipore filter and
staining with hematoxylin eosin. TREATMENT
Medical management- Antiglaucoma drugs
Surgical management- Anterior chamber wash
45
HEMOLYTIC GLAUCOMA
In this type, RBC laden macrophages accumulate in the trabecular meshwork
and obstruct the aqueous outflow temporarily.
Treatment: Antiglaucoma medications. If tension is not controlled with
medications, Filtering surgery and Cyclodestructive procedures can be done.
HEMOSIDEROTIC GLAUCOMA
It occurs due to intraocular hemorrhage. Hemoglobin which is released by
the degenerative red blood cells is engulfed by the trabecular endothelium. It
obstructs the aqueous outflow pathway.
LENS INDUCED GLAUCOMA
LENS SWELLING
Blunt or penetrating injury may alter the lens fibres, lens capsule. It results in
hydration of lens which leads to lens swelling. Swollen lens causes the forward
displacement of the lens iris diaphragm which reduces the iridocorneal angle.
It causes angle closure glaucoma secondary to pupillary block.
46
LENS DISLOCATION OR SUBLUXATION
Blunt trauma
Rupture of portion of zonules
Subluxation of lens dislocation of lens
posterior anterior
Aqueous flow obstruction from vitreous blocks the angle pupillary block
posterior chamber to anterior chamber
ANGLE CLOSURE GLAUCOMA
forward displacement of lens-iris diaphragm
reduce iridocorneal angle Angle closure glaucoma
47
Treatment
Lens removal with anterior vitrectomy for anterior dislocation of lens
[image:53.595.104.513.173.450.2]Pars plana vitrectomy with lens removal for posterior dislocation of lens
Figure 21. Anterior dislocated lens
LENS PARTICLE GLAUCOMA
Rupture of lens capsule resulting in liberation of lens material which obstruct
the trabecular meshwork and increase the intraocular pressure. It occurs most
commonly in penetrating injury,rarely in blunt trauma.
Management
Medical – Topical cycloplegics, steroids, Antiglaucoma drugs
48
RETAINED INTRAOCULAR FOREIGN BODY
If the retained intraocular foreign body is Organic, it produces
inflammation. Iron produces siderosis and copper produces chalcosis.
Early IOP rise is due to inflammatory reaction caused by foreign body.
Siderosis – Excess iron from retained foreign body cause tissue damage which
leads to iris heterochromia, rust like deposits in the corneal endothelium, anterior
lens surface and in trabecular meshwork. In the trabecular meshwork, iron deposits
produce sclerosis and loss of intertrabecular space. It cause outflow obstruction
which leads to rise in intraocular pressure and optic nerve head changes.
Chalcosis- Copper is also toxic. It produces more retinal damage than
glaucomatous changes.
PERIPHERAL ANTERIOR SYNECHIAE
Peripheral anterior synechiae form due to apposition of peripheral iris
against the trabecular meshwork as a result of pupillary block or posterior pushing
mechanism.
Pupillary block occurs in uveitis when the pupil is secluded by 360º
posterior synechiae or by occluding pupillary membrane. If the pupillary block is
not corrected immediately, iris bombe and peripheral anterior synechiae will
develop. Other causes of pupillary block include anterior subluxated lens and
49
In the presence of inflammatory cells, membrane forms between the iris and
the trabecular meshwork and the membrane contracts and form peripheral anterior
synechiae.
Ocular injury results in inflammation, blood in anterior chamber, flat anterior
chamber which leads to iridocorneal apposition and pupillary block. Penetrating
[image:55.595.89.522.284.533.2]injury commonly results in peripheral anterior synechiae
50
DIFFERENCE BETWEEN PERIPHERAL ANTERIOR SYNECHIAE AND
IRIS PROCESS IN GONIOSCOPY
PERIPHERAL ANTERIOR
SYNECHIAE IRIS PROCESS
Broad, irregular Fine, lacy
Extend upto schwalbe’s line
Extend upto inferior portion of
trabecular meshwork
Bridge the underlying structures,
Interference in seeing the angle
structures
Follow the concavity of recess
No interference to see the structure
In indentation gonioscopy- PAS drag
the iris vessels with them Do not affect movement of the iris
LATE CLOSURE OF A CYCLODIALYSIS CLEFT
Ciliary body is separated from scleral spur due to trauma. It results in
temporary or permanent hypotony. Late closure of cyclodialysis cleft reduces the
trabecular meshwork permeability which affects aqueous outflow leading to
increase in intraocular pressure. Cyclodialysis cleft usually involves less than
51
Figure 23. Cyclodialysis Cleft
INVESTIGATION MODALITIES
PERIMETRY
Types of perimetry
Static perimetry-
A stimulus is presented at a known location for a known duration with
varying luminance to find local threshold.
Kinetic perimetry-
A stimulus of known luminance is placed in an unseen area (outside
the border of hill of vision) and move towards seeing area to find the local threshold.
Generally performed centripetally. The hill of vision is found by approaching it
horizontally.
52
AUTOMATED PERIMETRY
• Humphrey
• Octopus
PROGRAM
HUMPHREY
• 30-2
• 24-2
• 10-2
OCTOPUS
• G1
• G2
• M2
TESTING STRATEGIES
Octopus
Normal
Dynamic
TOP (Tendency oriented
perimetry)
Humphrey
SITA (Swedish Interactive
Oriented Perimetry)
SITA fast
Full threshold
RELIABILITY INDICES
• False positives/ positive catch trial
False positive response represents the tendency of the patient to press the
trigger not in response to seeing a stimulus but at random, either as a response
to audible cue or due to the expectation of stimulus.
Trigger happy patients can also respond to stimuli in blind spot leading to
53
Abnormal high sensitivity white scotoma
• False negatives/negative catch trial
Failure of the patient to respond to stimuli, which are suprathreshold
to the sensitivity already measured at that point or adjacent point due to
patient inattention or fatigue or high threshold.
High false negatives can also be a result of disease rather than
inattentiveness of the patient.
High false negatives cloverleaf pattern.
• Fixation loss
Patient response to stimuli at the location of the blind spot (Heiji
krakau). Pseudo fixation losses are due to headtilt or anatomical variations.
Perimetry is unreliable if fixation loss is more than or equal to 20%
• Gaze tracking
Monitoring the eye movement of the patient during visual field testing.
In Humphrey, it is represented as a graphical diagram at the bottom of visual
field printout.
Factors affecting Automated Perimetry
• Background luminance
• Stimulant size
• Fixation control
• Refractive errors
• Cataracts and other media opacities
• Miosis
54
[image:60.595.90.531.106.568.2]INTERPRETATION OF RESULTS
Figure 24.Octopus Perimetry
Validity of the test
• False positive response: >33% unreliable
• False negative response : >33% unreliable
• Short term fluctuation: Normal =1-3dB
55
Glaucoma Hemifield test
• 5zones in the upper field are compared to mirror images of those in the
lower field.
If value in the two zones differ to an extent that found in
- <0.5% of the normal population (highly sensitive)
- <1% of normal population (outside normal limit)
- <3% of the normal population (borderline)
- <5% of the normal population (can be a normal plot)
ANDERSON CRITERIA
i. A cluster of 3 or more non edge points in a location typical of
glaucoma all of which are depressed on the pattern derived plots at
p<5% ; and one of which is at p<1% level on 2 consecutive fields.
ii. A CPSD or PSD (in SITA) that occurs in less than 5% of normal fields
on 2 consecutive fields
iii. A GHT outside normal limits on 2 consecutive fields.
GLOBAL INDICES IN OCTOPUS
• Mean sensitivity – represents the arithmetic mean of the threshold
determined at all the points in that field. It is represented in dB.
• Mean defect – is the arithmetic mean of the difference between the values
56
measure of generalized depression rather than a focal change. Normal value
is -2 to +2 dB
• Loss variance – represents the local non uniformity of the visual field loss.
It reflects focal alterations rather than an overall depression of the field. Loss
variance more than 6decibel is significant.
• Short term fluctuation – is obtained by testing the thresholds twice at the
same locations and is used to determine the corrected loss variance. It
represents the intra-test variability.
• Corrected loss variance – represents the non uniformity of the field
independent of the short term fluctuations
INDICES IN HUMPHREY FIELD ANALYZER (HFA)
• Visual field index : It is a measure of patient’s overall visual field function
expressed as a percentage, the normal age-adjusted value being 100%
• Mean deviation (MD): (mean defect in octopus) It gives an indication of the
overall sensitivity of the field.
• Pattern standard deviation (PSD) : It is a measure of focal loss or variability
within the field taking into account any generalized depression in the hill of
vision. An increased PSD is therefore a more specific indicator of
57
[image:63.595.95.521.91.322.2]Types of glaucoma field defects
58
ARTEFACTS
• Obstruction
i. Rim artefacts
ii. Ptosis
iii. Media opacities
iv. Angioscotoma
• Miosis
• Refraction artefacts
High power plus and minus lenses
B SCAN
It is a non-invasive technique.
It is useful in conditions where fundus examination is not possible because of
[image:64.595.114.501.492.708.2]hazy media.
59
Uses in ocular trauma
• Media opacities like hyphema, corneal opacity and Intumescent cataract
• To find out Intraocular foreign body
• Measure Angle anatomy- angle recession
• Subluxated and dislocated lens – dislocated lens looks like round or globular
structure in the vitreous.
• Posterior capsule status
• Vitreous hemorrhage- small white echoes with low amplitude spikes.
• Posterior vitreous detachment- undulated membrane in the retinochoroidal
layer that moves with movement of the eye. On A-scan it appears as a tall
spike, but not as tall as the spike of the retinal detachment.
• Retinal detachment- detachment of retina from the chorio-scleral layer with
100% amplitude tall spikes. It is attached however, to the optic nerve and the
ora serrata. B-scan is used to findout the extent of retinal detachment,
mobility of the detached retina, configuration and proliferative vitreoretinal
changes.
• Peripheral retinal tear- larger tear easily detectable by breached and rolled
out tissue. Small tears need meticulous examination.
• Uveal effusion- effusions are notable for their anterior angle and extension
to the ora serrata.
• Choroidal detachment- smooth, dome shaped, thick membranous structure
60
• Endophthalmitis- generally opacities are noted and membrane formation in
severe cases. Associated findings are choroidal thickening, choroidal
detachment, retinal detachment and intraocular foreignbody.
• Intraocular foreignbody
ULTRASOUND BIOMICROSCOPY
UBM is used to identify fine structural details and thus makes it extremely
helpful in understanding conditions where structural alteration in the tissues
contribute to the pathogenesis. It is extensively used in glaucoma followed by
anterior intraocular and surface tumors.
Role of UBM in traumatic glaucoma:
It is a non-invasive procedure
High frequency and less penetration of tissues.
Useful in diagnosis and management of ocular trauma when view is limited
by media opacities and abnormal anterior segment anatomy.
Uses in ocular trauma
• To find out intraocular foreign body,
• Angle recession – widening of the anterior chamber angle
• Uveal effusion
• Cyclodialysis cleft- disruption of interface in between the sclera and ciliary body leading to direct communication between the
anterior chamber and suprachoroidal space.
61
• Iris hemorrhagic cyst
• Subluxated or Dislocated lens
[image:67.595.98.546.153.436.2]• Peripheral anterior synechiae
Figure 27. Angle Recession
DISADVANTAGES
This procedure can be performed in Supine position only.
It requires a plastic or silicone eyecup to hold a coupling medium, hence it is
difficult to perform in uncooperative patients, children, recently operated and ocular
62
OPTICAL COHERENCE TOMOGRAPHY
OCT has become a routine part of the management of macular and other
retinal diseases. The same machine can be used for the assessment of glaucoma and
has been widely used for this purpose.
• Peripapillary retinal nerve fibre layer (RNFL)
This involves the acquisition of a circular scan of the retina around the optic
nerve head
• Optic nerve head
Radial cross sectional scans permit an objective and repeatable assessment of
disc morphology, with reasonable discriminatory value.
• Ganglion cell complex analysis
It involves measurement of retinal thickness at the macula in an attempt to
detect early stage glaucomatous damage. Using older time domain OCT, it was
found to be regarded as inferior to assessment of other parameters such as
peripapillary RNFL assessment; with newer OCT technology interest in GCC
analysis has been renewed and it is regarded as comparable and supplementary
• Progression analysis software has been introduced on several machines,
providing a computed assessment of the extent of damage over time
presented in graphical form
63
ANTERIOR SEGMENT OPTICAL COHERENCE TOMOGRAPHY
• It is used to study the normal anatomy and physiology of iris and anterior
chamber angle structures.
• Screening of angle closure.
• Plateau iris
• Malignant glaucoma
• Efficacy of laser peripheral iridotomy
[image:69.595.89.525.356.647.2]• Patency of Glaucoma drainage device.
64
Figure 29. Angle recession with choroidal hemorrhage
Advantages
It is a noncontact method therefore do not cause indentation of the angle by
placement of the scleral cup on the eye.
It is a more physiological examination as patient is imaged sitting upright.
Shorter imaging time and rapid image acquisition.
It is very safe to scan eyes with filtering blebs, uncooperative patients,
children and recently operated cases
Disadvantages
Unable to image structures posterior to iris as the optical beam cannot
65
REVIEW OF LITERATURE
Ajite KO, et al.
This study was conducted to findout the frequency, clinical types and
treatment modalities of traumatic glaucoma (7)
Totally 365 ocular trauma patients were taken for analysis. All of them were
subjected for complete ophthalmic evaluation like Visual acuity, Slit lamp
examination, Intraocular pressure measurement, Optic disc stereoscopic evaluation
by 78D, Gonioscopy and Perimetry. They excluded patients who were already under
treatment of glaucoma.
Among them 31 patients (8.5%) were diagnosed as traumatic glaucoma. The
range of age was 10 to 79 years (median 45 years± 3 years). Males were more likely
to be affected than females about 2:1 ratio. The clinical type of secondary open angle
glaucoma (54.8%) was higher than the secondary angle closure glaucoma (45.2%).
61% patients had very low vision (moderate to severe visual impairment). Peripheral
anterior synechiae (29%), adherent leucoma (16.1%), hyphema (16.1%) were
common clinical findings in this study(7).
Osman, et al.
This study evaluated the incidence and risk factors of glaucoma after open
globe injury.
They selected 775 patients who underwent repair of open globe injury over a
period of 15years were retrospectively reviewed from medical records. They were
66
Their analysis revealed that age more than 18 was critical for traumatic
glaucoma. Incidence of post-traumatic glaucoma was 5.3%. Risk factors of
glaucoma were Zone II injury (p=0.027), penetrating injury (p=0.0008%), lens
injury (p=0.011), vitreous hemorrhage (p=0.002%) and presence of intraocular
foreign body (p<0.0001)(8)
Turalba et al.
In this study, they evaluated predictors and outcomes of increased IOP after
open globe injury. This retrospective, case control study reviewed the records of
658 patients with open globe injury over a period of Febraury 1999 to January
2007(19).
This study concluded that 17% patients developed increased IOP after
trauma. Risk factors for increased IOP were increasing age p<0.001, hyphema
(0.025), lens injury (p<0.0001%) and zone II injury (p=0.0254)(19). Early diagnosis
and timely intervention had improved the visual acuity and normalization of IOP
over time.
Girkin, et al.
This study analysed the association between baseline structural and
functional ocular characteristics and risk of developing posttraumatic glaucoma after
penetrating injury.
3,627 patients of penetrating injury were taken for analysis. This study
concluded that risk of developing glaucoma was 2.67%. Risk factors included
67
Girkin, et al.
This study was designed to evaluate risk factors for glaucoma in blunt trauma.
Total of 6021 patients who experienced blunt ocular trauma were taken for
analysis. They were followed over the period of 6 months(18).
This study concluded that 6months incidence of developing glaucoma in
blunt ocular trauma was 3.39%(18). They determined several independent predictive
factors like poor initial visual acuity ( worse than 20/200), advancing age, lens
injury, angle recession, and hyphema.
Wang WQ, et al.
This study determined the classification and management of early secondary
glaucoma associated with ocular trauma(21).
They classified secondary glaucoma associated with trauma by their clinical
findings: hemorrhagic type, chamber angle injury type, lens related type, synechiae
and proliferation type(21). They concluded that early secondary glaucoma associated
with trauma was complex.
Bai et al.
In this study, they classified the glaucoma into three stages according to the
time interval between trauma and development of glaucoma like early, intermediate,
late stages. In early stage (1 – 4weeks), there were 33 cases due to inflammation, 36
cases due to hyphema and 22 cases were lens induced. In intermediate stage
(1-6months, 3 cases due to pupillary block and 2 cases due to phacoanaphylaxis)(9). In
68
Stanic, et al.
This study presented the frequency, clinical forms and therapeutic results of
traumatic glaucoma in 511 patients(10). They submitted all injured eyes to visual
acuity examination, Gonioscopy, slit lamp examination, fundus examination,
intraocular pressure measurement and perimetry.
They concluded that traumatic glaucoma was found in 6.6%. It was more
frequent in contusion injuries than perforation injuries. The patients with traumatic
glaucoma were 9 -86 years of age (mean 60.2.). Males were more affected than
females. One third of the patients were blind and one half had visual acuity below
0.1(10).
69
AIM
• To study the incidence of glaucoma in ocular trauma in tertiary care
centre.
OBJECTIVES
• To study the incidence of different types of glaucoma in ocular trauma
70
METHODOLOGY
200 Patients with Ocular trauma reporting to the glaucoma clinic Regional
Institute Of Ophthalmology for one year duration from 01. 05. 2017 to 01. 05.2018,
Government Ophthalmic Hospital will be registered, consent obtained and
evaluated.
INCLUSION CRITERIA
• Patients with Blunt injury/ Penetrating injury/ Chemical injury/ Thermal injury.
EXCLUSION CRITERIA
Patients with
• Pre-existing open angle glaucoma/ angle closure glaucoma
• Pre-existing ocular diseases such as those with anterior segment infections and inflammation.
METHODS
In our study of 200patients with ocular trauma,detailed history was recorded.
They were subjected for the following examination
• Visual acuity by Snellen’s chart,
• Anterior segment evaluation with Slit lamp examination,
• Fundus examination by direct ophthalmoscopy and slit lamp
biomicroscopy using 90D, Indirect ophthalmoscopy,
• IOP measurement by Goldmann applanation tonometer / Rebound
71
• Gonioscopy,
• Automated perimetry,
• B scan, Ultrasound Biomicroscopy, X-ray orbit if needed.
FOLLOW UP
All the patients were followed up weekly for the first two weeks, biweekly
for a month and then monthly for 12months. Patients were asked to visit hospital as
early as possible whenever they have any complaints.
STATISTICAL ANALYSIS PLAN
72
RESULTS
ANALYSIS OF 200 CASES
In our study of 200cases with age group from 4 -81years, the mean age of
ocular trauma is 35.76 years.
GENDER DISTRIBUTION
GENDER NUMBER PERCENTAGE
Female 39 19.5
Male 161 80.5
Total 200 100
Chart 1
Males (80.5%) were more affected than females (19.5%).
19.5
80.5
Gender Distribution
73
MODE OF INJURY
MODE OF INJURY NUMBER PERCENTAGE %
AGRICULTURE 19 9.5
ASSAULT 25 12.5
DOMESTIC 40 20
FIRE CRACKER 12 6
INDUSTRIAL 49 24.5
RTA 26 13
SCHOOL 8 4
SPORTS 21 10.5
TOTAL 200 100
Chart 2
In our study, the most common mode of injury is industrial (24.5%) followed
by domestic injury (20%).
0 5 10 15 20 25 Agriculture
Assault Domestic Fire Cracker Industrial RTA School Sports
74
TYPE OF INJURY
TYPE OF INJURY NUMBER PERCENTAGE %
BLUNT 103 51.5
PENETRATING 87 43.5
CHEMICAL 8 4
THERMAL 2 1
TOTAL 200 100
Chart 3
In our study, blunt injury is more common than penetrating injury.
0 10 20 30 40 50 60
Blunt Penetrating Chemical Thermal
Type of Injury
75
AGENT CAUSING INJURY
AGENT CAUSING INJURY NUMBER PERCENTAGE %
ACID 2 1
ALKALI 5 2.5
BALL 19 9.5
FIST 16 8
METAL 56 28
OTHERS 7 3.5
STICK 19 9.5
STONE 43 21.5
SHARP INSTRUMENT 11 5.5
WOOD 22 11
TOTAL 200 100
Chart 4
In our study, metal is the most common agent causing injury followed by
stone.
0 5 10 15 20 25 30 acid alkali ball fist metal others stick stone sharp instrument wood
Agent Causing Injury
76
INCIDENCE OF GLAUCOMA
Glaucoma Frequency Percentage % Cum.
Absent 173 86.5 86.5
Present 27 13.5 100
Total 200 100
Chart 5
Over a period of one year of our study, 13.5% of patients developed glaucoma
after ocular trauma.
0 10 20 30 40 50 60 70 80 90
Absent Present
Glaucoma
77
GENDER DISTRIBUTION
Gender Distribution in Glaucoma Frequency Percentage %
Female 8 29.63
Male 19 70.37
Total 27 100
Chart 6
AGE DISTRIBUTION IN TRAUMATIC GLAUCOMA
The mean age of patients with traumatic glaucoma was 41years.
Female, 29.63%
78
LATERALITY
LATERALITY NUMBER PERCENTAGE %
RE 10 37.04
LE 17 62.96
Total 27 100
Chart 7
In our study, left eye was more affected than right eye.
0 10 20 30 40 50 60 70
RE LE