Rochester Institute of Technology
RIT Scholar Works
Theses
Thesis/Dissertation Collections
11-13-1996
A Better environment for disabled children
Hyun-Sook Lee
Follow this and additional works at:
http://scholarworks.rit.edu/theses
This Thesis is brought to you for free and open access by the Thesis/Dissertation Collections at RIT Scholar Works. It has been accepted for inclusion
in Theses by an authorized administrator of RIT Scholar Works. For more information, please contact
Recommended Citation
ROCHESTER INSTITUTE
OF
TECHNOLOGY
A Thesis
Submitted
to the
Faculty
ofThe
College
ofFine
andApplied Arts
in
Candidacy
for the Degree
ofMASTER OF FINE ARTS
A Better Environment for Disabled Children
By
Lee,
Hyun-Sook
Adviser: Charles F. Lewis
Date: Nov. 13. 1996
Associate Adviser: Nancy Chwiecko
Date: Nov. 13. 1996
Associate Adviser: Cynthia Bock
Date: Nov. 13. 1996
Dean, College of Imaging Arts and Sciences:
Dr. Margaret O. Lucas
Date:
---tr--
e -co-q'l
I,
, prefer to be contacted each
time a request for production is made. I can be reached
at the following address.
39-206 Hyun-Dai Apartment
Kodeok-Dong Kangdong-Gu
Seoul, South Korea
ACKNOWLEDGEMENTS
This thesis has
evolvedfrom my ideas
andexperiences
in interior design,
During
the
pastthree
years,I have been
a graduate studentin Korea
and atR.I.T.,
My
main
focus
has been the
study
ofinterior
design
asit
relates
to the
environment ofthe disabled,
Throughout
this
time,
I have
received supportfrom
many
people.While it
is
impossible
to thank
everyone personally,I take this time
to
acknowledge afew
people whose contributions mademy thesis
possible,I
should point out,however,
that
althoughI
have
received advisement
from
numerous sources,the
responsibility
for
the
content ofthis thesis
is solely
mine,While I
wasexploring
the
thesis,
I discussed
my ideas
withmany
people andI particularly
wouldlike to thank
Charles
F. Lewis
for
his technical
and constructive criticisms.Nancy
Chwiecko
contributed encouragement andI
expressmy
thanks to
her
as well.I
alsothank Cynthia Bock for her
professional comments andinformation
abouthealth
carefacilities,
I
acknowledgeHan-Tae
Yoo,
aKorean
professor, whorecommended
that I study in the United
States,
Additionally, I
thank
the
peoplein Korea
who encouragedme
through
many
difficulties
whileI
waspreparing
to
study
abroad.I
also givemy
thanks to
churchfriends
whothesis.
Furthermore,
I
give specialthanks
to
friends
whostayed
up
many
nightsto
assist mein
making
the
modelsat
R.I.T..
Lastly
I
especially
thank my
siblings andtheir
families
who providedfinancial
and emotional support.I
truly
appreciatethe
supportthat
I have
received overthe
past
three
years.In
return,I have
promisedmy
devotion
and
dedication
in
my
effortsto improve the
living
environments
for the disabled in my
country.By
remembering
the
supportthat
I have
received,I
will alwaysbe
motivatedto
striveto
achievemy
goals ofdesigning
aPREFACE
I have
adream to
create superiorhealth
carefacilities
for the
disabled.
My
father,
whodied
whenI
was18
years old, was a prosperousbusinessman,
an educator,and a
humanist,
He
encouragedmy
academic pursuitsfrom my
childhood,He
alwaystold
me,"I
want youto
help
people who areignored
and oppressed,due to
the
lack
of powerin
our society",Teaching
social studiesin high
schoolhelped
meremember
my father's
wish,I decided to
become
avolunteer
for the
disabled.
After four
years as a volunteerI
acquired
the
certificationto teach the
retarded,At
that
time,
I believed
I
couldbenefit the disabled the
mostthrough
education,The
closerI became to
them,
the
moreI desired to
find
other waysto
help
them,
I
sawthat
the disabled did
not
have
accessto
public places, such as schools,shopping
centers, parks, andtheaters,
because these
facilities
were not equippedto
accommodatethe
disabled.
They
wereisolated
and segregatedfrom the
restof
society due to
ourindifference.
Even
institutions
for
disabled
people were notadequately
equipped withnecessities such as grab
bars,
ramps, sinks, andfire
exitsfor the
disabled.
Moreover,
I discovered the lives
ofmany
more miserable
than
ofthose
living
in
specializedinstitutions,
I then
realizedthat the
mostimportant
thing
for
the
disabled
was not an education,but
abeneficial
living
environment.
As
a result.I decided to study
Interior Design
to
equip
myself sothat I
mightimprove
the
environmentsfor the disabled,
This has led to my
decision
to
design
ahealth
carefacility
for my thesis,
Through this
project,I have learned
a greatdeal
about
designing
interiors for
the disabled.
I
believe
that
aspecially
conducive environment can enhancethe
happiness,
learning
abilities, and morale ofdisabled
people.
I
wouldlike
to
work as aninterior designer
whoimproves
living
environmentsfor the disabled
and aninspector
who evaluatesfacilities
of publicbuildings for
the
disabled in my
country.It is important to
emphasizethat
this
conceptis
aderivative
of philosophical principles, reflectedin judicial
and
legislative
activities whichfocus
onthe
rights ofhandicapped
personsto have
conditions oftheir lives
LIST
OF ILLUSTATIONS
Figure
1,
Al
Sigl
Center,
Elmwood Avenue
82
Figure
2.
One
oldhouse
andTwo dormitorie
83
Figure 3.
Sketches
ofGreek
Temple
84
Figure 4.
Development
ofidea
sketches85
Figure 5.
Site
plan andPergola
86
Figure 6,
Floor
plan ofAdministrative
andMedical
Center---87
Figure 7.
Floor
plan ofGroup
Home
88
Figure 8.
The Administrative
andMedical
Center
89
Figure 9.
The Entrance
ofthe Administrative
andMedical
Center
90
Figure 10,
Circulation
andPublic
area91
Figure 1 1
.Vending
machine area andPublic
restroom,Soiled
utility,
Janitor,
andStorage
92
Figure 12.
Reception
area andWaiting
area93
Figure 13.
Waiting
area,Park
and playground94
Figure 14.
Playground
95
Figure
15.
Office
area96
Figure
16.
Medical
areas,Patient
areas andVisitor's
suite----97Figure
1
7.
Patient
Single
andDouble bedrooms
98
Figure
18,
Medical
area,Patient
area andthe
corridor wall99
Figure 19.
Physical
andOccupational
therapy
room,
Employee's
room,Examination
room,
Patient
Lounge,
andNurse's
station100
Figure 21.
The
patio ofVisitor's
suite and pergolaFigure 22.
Group
Home
Figure 23.
Public
areain
Group
Home
Figure 24.
Living
room andLounge
Figure 25.
Office
area andActivity
roomFigure 26.
Kitchen
andDining
roomFigure 27,
Garage
Figure 28,
Porch
Figure
29.
Example
of aSingle bedroom
anda
Double bedroom
Figure 30.
Circulation,
Utility
area andBathrooms
102
103
104
105
106
107
108
109
1 10
TABLE
OF CONTENTS
ACKNOWLEDGMENTS
iii
PREFACE
vLIST OF
ILLUSTRATIONS
viiI.
INTRODUCTION
1
A. A Brief
History
ofhealth
carefacilities in the United
States
1
B. Proposal
6
C.
Philosophy
10
II. COLLECTION OF
INFORMATION
AND ANALYSIS
14
A. Research
14
B.
Survey
ofAl
Sigl Centenfacilities
and site conditions28C, Code
requirements31
III.
DEVELOPMENT
OF THE
PROGRAM
35
A. Initial Ideas
and schematicdiagram
35
B.
Spatial
relationships38
IV.
APPLICATION
45
A.
ADMINISTRATIVE
AND
MEDICAL
CENTER
1
.Reception
and public areas2,
Medical
areas3, Patient
areas andVisitor's
suite,4.
Utility
areasB.
GROUP
HOMES
..1
.Public
areas .. ,2, Bedrooms
3, Bathrooms
4,
Other
C, EXTERIOR
1
,Parking
lots
2,
Courtyard,
Swimming
pool, andPlayground
3, Ramps
45
46
52
55
61
63
64
69
72
73
75
75
76
77
V. SUMMARY
7
8
I. INTRODUCTION
A Brief
History
ofhealth
carefacilities in
the
United
States
"The
history
ofHealth
carefacilities
started withasylums
for those
suffering
from
mental illness."1Not
untilthe late
seventeenth and eighteenth centuriesdid
demographic
changesforce
an alterationin the
pattern ofwelfare and encourage
the institutionalization
ofthe
mentally disabled.
However,
the
care andtreatment
of mentalillness in
nineteenth-century
America
wasbased
on aphilosophy
whichfused
morality, social values, andscience.
By
the
middle ofthe
century, an extensive network ofstate-supported public
hospitals had
been
established,By
the
end ofthe
nineteenth century, as asylumsbecame
increasingly
custodial anddesperately
overcrowded, newphilosophies were sought.
At that
time,
social and publicresponses
to
suchindividuals
as mental patients andseverely
handicapped
persons,therefore,
werecharacterized more
by
concernfor
life-sustaining
carethan
by
an orientationto
activetreatment.
"It
wasinspired partly
by
horror
stories of overcrowded,inhumane
institutions
andpartly
by
newforms
oftreatment that
allowed
many
patientsto
function
in
smallercommunity
facilities
or even athome
untilthe
1950s,"2In the
1960s,
several critical studiesled to the
establishment of minimum standards
for
residential carefacilities.
These
standards preparedthe way for
deinstitutionalization
andthe
community
health
caremovement.
The decade
ofthe 1970s
saw remarkable changesin
both the
social perspective onhandicapped
persons andin the
number ofhealth
carefacilities based
onthese
changing
perspectives.Two
significant occurrenceshad
tremendous
impact in the
history
ofhealth
care.The first
was
derived from
a report ontwo New York
State
institutions
by
Senator
Robert F, Kennedy.
The
otherimportant impact
resultedfrom
avideotaping
oflife in
aNew York
stateinstitution in the early 1970s.
These two
events
helped to
educatethe
public onthe
poorconditions of
health
carefacilities
andfostered
changein
public opinion andinterest in health
careinstitutions,
In
1972
alandmark decision
was madein
anAlabama
case,It
statesthat
mentally
retarded personshave
a rightto treatment in the "least
restrictive"alternative
to the
objective ofmaintaining
the
greatestdegree
offreedom,
self-determination,dignity,
andintegrity
ofbody,
mind, and spiritfor the
individual
whilehe
or she participatesin treatment
or receives services,"A
resolution was passed
to
recommend 'residentialfacilities
consisting
of smallliving
units, eachreplicating
a normalhome
environmentto the
closest extentpossible'
and
'that
such residential
facilities take
absolute precedence overfurther
capitalinvestments
in
existing
orlarge
scaleinstitutions',"3
In the
1980s,
the
mainfocus
ofthe policy
ofdeinstitutionalization
wasthe
reduction of and prevention ofthe
needfor
residentialliving
in large institutional
environments,
Equally
important
wasthe
promotion ofthe
placement,
with appropriatehabilitation
and supportservices, of people
in
more normalliving
environmentswithin
the
community.With the
promulgation ofdeinstitutionalization
and normalization,there
wasincreased interest in
evaluating
the
qualities ofenvironments,
the differentiation
andtyping
of variouskinds
of environmentsusing
physical,behavioral,
andpsychosocial criteria, and
the
assessment ofindividual
adaptive growth as
it
relatesto
environmental qualities."The primary
social principleunderlying
the
conceptof
the least
restrictive environmentis the
commitmentto
finding
a placefor
handicapped
individuals in
settingsthat
enhance
their
participationin the
society."4The
importance
ofthis
principleis
nottied
merely
to basic
social values, although
in large
measureit
originatedfrom
3
"Residential
facility
fortheRetarded."
NationalAssociationfor Retarded Citizens 1976p3 4
Bruiniks,
Robert H.andLakin,
K.Charlie,
LivingandLearningin theLeast Restrictivethem,
but
stems alsofrom
the fact that it is
a powerfulhabilitation
concept.The
group
home
setting
has
resultedfrom this
concept.In
January
1992,
the
Americans
withDisabilities
Act
(ADA)
became
effective.This Act is the
most significantlegislation
ever enactedfor
people withdisabilities.
It
requires
that the
disabled
have
equal accessto
publicaccommodations,
publictransportation,
employment, andtelecommunication
services.All
public and commercialbuildings,
such as restaurants,hotels,
retail establishments, doctors'offices, and
theaters,
mustbe
modified,if
necessary, to
remove obstaclesthat
preventhandicapped
persons
from
using
these facilities.
All
health
carebuildings
andfacilities
mustcomply
withthis Act.
Consequently,
the disabled
nowhave better
environmentssupported
by
these legislative
initiatives.
The ADA significantly increased
social commitmenttoward
enhancing
opportunitiesfor disabled
children.Disabled
childrenhave been
known to have relatively less
ability
to
adaptto
different
settingsthan
non-handicapped children whohave generally
been
raisedin
normal social settings,From
astrictly
educational perspectivehandicapped
children shouldbe immersed in
normalAt
the
turn
ofthe twenty-first
century,knowledge,
expertise, and conducive attitudes
have
continuedto
improve
the
quality
ofliving
environmentsfor
handicapped
children.In the
future,
human
serviceprofessionals will need
to
utilizethe
values ofsociety
to
teach handicapped
children meaningful skills anddevelop
B.
Proposal
The
inclusion
ofaccessibility
features
whendesigning
buildings
andfacilities
is
akey
factor
in
enabling
persons withdisabilities
to
achieveindependence.
Rehabilitation,
treatment,
training
in
activitiesfor
daily
living,
andthe
elimination of environmental
barriers,
will givemany
ofthese
individuals
the
opportunity
to
live,
study, work, andparticipate
in
regularcommunity
activities,This
will supporttheir human
potential regardless of physicaldisabilities,
A
supportiveliving
unit,in
whichboth
staff andenvironment are
designed for the intended
population,is
aprerequisite,
above all,in
improving
the lives
ofboth the
physically
anddevelopmental^
disabled.
During
my
preliminary
research,I
discovered that
most children'sgroup homes
were renovatedhouses
whichwere not
specifically
designed to
accommodatehandicapped individuals,
While
a number of excellentfacilities for
challenged adults andthe
elderly already
exist,
few quality facilities
existfor
childrenin the U.S..
This
mightbe
explainedby
differences in
agedistribution,
The
rapidly
increasing
population ofthe
the U.S.
population was over65
years oldin
1930,
the
1991
figure
was12.6
percent,Older
peopletend to
have
a greater number of chronic
health
problems, requiremore visits
to the
doctor,
require alonger
period ofrecuperation after an
illness,
and need morehospitalization
than
a younger population,"5Consequently,
the federal
and state governmentshave
responded
to their
requests as well asto
business
marketscreated
by
their
construction."Children
receivesignificantly
less
supportthan the
elderly
and adults under65.
Among
the
disabled,
the elderly
receive most support,followed
by
adults under65.
On the
average,the
disabled
elderly
arethe
most preferred group.,.."6While there
are varioushealth
carefacilities
for
different
age groups anddifferent
disabilities,
there
existsmuch room
for improvement.
Relatively
speaking,the
need
for
creating
better health
carefacilities for disabled
children
has been less
consideredthan for the
elderly
in
the U.S..
Adequate
andappropriately
designed group homes
are a
basic
health
care componentfor disabled
children,
if
we acknowledgetheir
rights ashuman beings.
Rather
than any
particular style of architecture,the
needs ofthese
children and modern concepts of socialtreatment
5
JanetR CarpmanandMyronA.
Grant,
DesignthatCares(737NorthMichigan Avenue Chicago IL1993)
p46
should
be the basis for
the
building
plan of a residentialhealth
carefacility.
It
should notbe
expectedto
duplicate
afamily
home,
but
shouldbe
designed
to
create a warm,
attractive,
homelike
atmospherefor their
daily
living,
A
cold,depersonalized
appearance,complicated
layouts,
andinstitutional
restriction ofthe
activities of children's
everyday lives
shouldbe
avoided,The
purpose ofthis thesis is to
explorethe
design
of ahealth
carefacility
with particular consideration givento
the
needs of children with multipledisabilities.
To
achievemy
goals ofaccommodating
their
physical, psychological,and mental
impairment,
I have designed
ahealth
carefacility
whichhas
residential areasfor multiply disabled
children.
My
design
providesfacilities for
living,
socialactivity, medical
treatment,
and physicaltherapy;
in total
three
Group
Homes for the multiply disabled
children.The
children are placed
in
agroup home
according
to their
age and
disability:
Building
A is for
children with multipledisabilities
andimpaired
vision,Building
B houses
childrenover
twelve
years old with multipledisabilities,
andBuilding
C
is
reservedfor
children undertwelve
years old withmultiple
disabilities.
Administrative
offices and aMedical
Center have been
designed
to
achievethe
above-mentioned goals.
The
size ofthe
Administrative
andMedical
Center
would accommodate patients
living
in the three
Group
food
preparation andmanagement.
"From the
point ofview of
the
children, unit services ratherthan
central services andfacilities
are preferable,"7While I
wasdeveloping
conceptsfor my
design,
I
adapted
the
concept ofthe
"village"organization used at
the Al
Sigl Center
for
handicapped
childrenin
Rochester,
New York,
(see Figure
1)
I
determined
that the
independent
"village"approach would
be
mostappropriate
for
handicapped
childrenliving
in
Korea,
a small and overpopulated country, sinceKorea does
notcurrently
provide publictransportation,
The
potentialefficiency
of management anaeconomy
of operation would supportincreased
numbers ofgroup homes for
disabled
childrenin my
country,7
"Standardsfor
Group
HomeService forChildren."C.
Philosophy
ofDesign
Designing
ahealth
carefacility
is
a complex processthat
mustsatisfy
a multitude ofcompeting
criteriaincluding
emphasis on environmental accessibility,To
explore adesign
solution which could meetthe
needs ofmy
nativeland,
I
decided
to
oppose currentAmerican
trends
oftotal
separation ofAdministrative
andMedical
facilities from
residentialfacilities,
My
projectis,
therefore,
composed of numerous areas whichhave
diverse functions
such as offices, medicalfacilities,
andresidential spaces.
The functional
characteristics of each space, as wellas
the
relationshipsamong
spaces, mustbe
considered.For
example, an office area must provide efficiency, whilethe
group
home
should stress comfort,incorporating
affirming,
"homelike"
design details
such asincandescent,
residential
lighting
fixtures
in the
dining
room, andresidential
furniture in the
bedrooms.
The
medical area'sinterior
must provide clear visual order and abright,
inviting
atmosphere,focusing
on physical comfort andsocial contact, as well as efficiency.
When
abuilding
mustinclude
severaldiverse
functions,
it is
oftendesirable
to
organize spacesprivacy,
security
and adegree
offreedom
in
shaping
interlocking
space of varied configurations withappropriate
(and
varied) finishes
while stillcreating
aunified composition.
The
primefunction
ofthe
circulation systemis to
getpeople and materials
to their
destinations.
The
circulationpattern,
thus,
shouldbe
clear, safe,
efficient and providesecurity among
various units.Additionally,
"The
Americans
withDisabilities Act
(ADA)
requiresthat
allfacilities
removebarriers that
prevent a
physically handicapped
personfrom
having
equal access
to the
facility...."8Thus,
each part ofthe
building
must provide accessfor
the disabled
such asthose included in my design,
"A
1980s' revolutionin
health
caredesign
stressesthat
medicalfacilities distance themselves from the
"illness"
images
in
favor
of a"hospitality" image."9
Medical
care
is
a combination of science and emotion.The
design, therefore,
mustbalance human
needs andtechnological
needs andthe therapeutic
aspects ofdesign
must alsobe
considered.Important
considerationsinclude the
use ofnature,
art work and
the
architecturalfinishes
selected.Nature is
no
longer limited to the
outdoors.It has become
anintegral
part ofinterior
design.
Atriums,
greenhouses,
8
The American InstituteofArchitects..
Opening
All Doors: The ADAVideoconference. (1735 New YorkAvenue,
NWWashington,
DC200061992)
P67planters,
and aquariums, all allow constantgreening
ofthe indoor
environment.Nature
has been
used as atherapeutic tool for
a widevariety
of patients,including
psychiatric,
pediatric, geriatric,
and rehabilitationpatients,
Plants
providethe
opportunity
for
physicalactivity
and socialinteraction.
Plants
can provideinterest
and
diversion.
The
use of naturaldaylight is
alsoimportant.
A
skylight,
like the
oneI have
designed,
savesenergy
by
reducing
the
needfor
electric-light sources, and moreimportantly,
it
promotes a naturallight
quality
in the
interior,
Art
work canbe
animportant
elementin interior
design,
It
may
foster
emotional stability, comfort,interest,
and stimulation.
Interesting
patterns, colors, shapes, andother
decorations
can encourageimagination,
as well asphysical
activity
and play.Playful
elements aredesigned
to
entice reluctantyoung
residentsthrough
the
doors
ofthe Medical Center.
Carpeted
corridors are often suggested as away to
"soften"
a
harsh health
care environment,Carpeting
is
considered more comfortable and
psychologically
warmthan
mosthard-surface flooring,
Carpeting
has
alsobeen
found to
reduce ambient noiselevels
andinjuries from
falls,
Vinyl
wallcovering
facilitates
easy
clean up, andmay
As it is far
moredifficult to
repairthan
paint, carefulconsideration needs
to
be
givento the
actuallocations
of use,Lighting
is
animportant
elementin
defining
the
characteristics of spaces,Higher light
levels
may
define
special spaces or points ofdecision,
such as reception areas or majorintersections,
Softer
lighting
wouldbe
more appropriatefor
rooms with quiet activities such asbedrooms.
In the design
ofhealth
carefacilities
for
children,II. COLLECTION OF
INFORMATION
AND ANALYSIS
A. Research
Quality
design
will enhancequality
oflife.
Quality
design
resultsfrom
utilizing
past experiencein
architecture andinterior design to improve
uponexisting
design
theories,
Research
is
atool through
whichhealth
careproviders and
designers
candiscover
what residents, staff,and visitors need
in
orderto
gain a sense of comfort andwell-being
in their built
environment,The
purpose ofhealth
carefacility
design
researchis two fold,
One;
to
gain
information
andtwo;
to
apply
that knowledge toward
the
goal ofimproving
the
environment,In
orderto
gaininsight
onimproving
the
quality,efficiency, and
function
ofhealth
caredelivered in
newand
existing facilities,
I
visited severalhealth
carefacilities: four group homes for multiply disabled
children,special
institutions for multiply disabled
children(Al Sigl
Center)
andfor
adults with mental retardation(Monroe
Developmental
Center),
two
nursing
homes
for the
elderly,
and
"On
withLife"
(care
andtreatment
center with acomprehensive
head
injury
rehabilitation programfor the
mentaldisorders
causedby
accidents) in
Ames,
Iowa.
The majority
ofthe
group
homes
I
visitedhad
been
renovated private residences.
These houses did
notof
the
residents.As
aresult,
these
group
homes
have
problems.
Some
group homes
aretoo
smallto
accommodate eight
to ten
children with multipledisabilities.
For
example,
the
width ofthe
corridorsis
less
than four
feet,
whichis too
narrowfor both
a wheelchairand a person
to
pass simultaneously.Although health
carefacilities
such asthe Al
Sigl
Center
andthe
Monroe Developmental
Center in
Rochester,
New
York,
wereinitially
createdfor the
disabled,
they
werebuilt before
1980,
andthus,
exhibitinadequacies
and minimal amenities.Residential
unitsclustered around
the Monroe Developmental Center
create a
very institutional
setting, withthe
interior
environment of each residential unit
resembling
ahospital
or
nursing
facility
ratherthan
ahome.
On the
otherhand,
an example of anideal health
care
facility
is in
Ames,
Iowa.
"On
withLife",
managedby
the
state,is
afacility
for inpatients
who need minor careor
treatment for
mentaldisorders
afterreceiving
hospital
treatment.
They
are assistedby
approximately
eighty
people
including
doctors,
nurses,therapists,
and alarge
number of volunteers
for the
eightto twelve
patients wholive there
astemporary
residents.10The design
of"On
with Life"separates
the
patientarea and
the
administrative area.In the
patient area, allwalls are curvilinear
in
plan.The
walls are covered with10
vinyl
wallcovering
or pastel stained wood.Additionally,
there
are pictures and graphics onthe floor
and walls.The
art work and graphics are used
by
staff as recalltriggers
ofpatient experiences, and
to
assist a patient withrecovery
of a
lost
memory.While "On
withLife"
has necessary
high-tech
equipment and carefacilities,
the
environment alsoprovides warmth, and
the
opportunity
to
recreatememories.
Every
patient roomis
provided with enoughspace
to turn
a wheelchair.Each is
supplied with alarge
accessible closet, a
dresser,
ahigh-back
chair, abedside
table,
atelevision,
a radio, a comfortable side chairfor
visitors, a
bed,
and wide windows withfloral
curtains,Gerald T.
Fehn,
the
director
ofPublic Relations
&
Development for "On
withLife",
indicated his
greatsatisfaction with
the
design
ofthis
facility.
He
boasted
that "On
withLife"
is
one ofthe
best
health
carefacilities
in the United States.
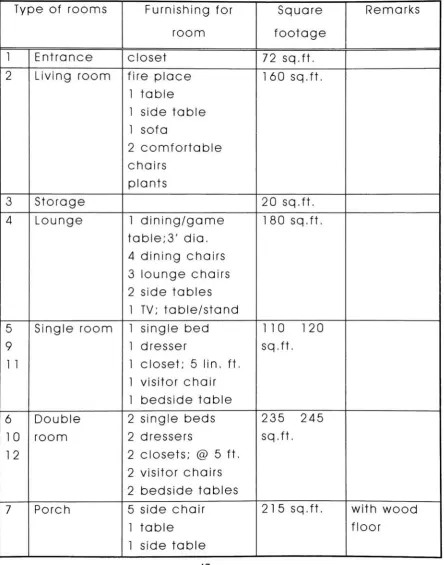
My
research nextled
to
the
development
of abuilding
programincluding
proposedfurnishings,
andsquare
footage,
asfollows
:Group
Home
Type
of roomsFurnishing
for
Square
Remarks
room
footage
1
Entrance
closet72
sq.ft,2
Living
roomfire
place1
table
1
sidetable
1
sofa2
comfortablechairs
plants
160
sq.ft.3
Storage
20
sq.ft. [image:28.534.48.493.103.668.2]4
Lounge
1
dining/game
table;3'
dia.
4
dining
chairs3
lounge
chairs2
sidetables
1
TV;
table/stand
180
sq.ft.5
Single
room1
singlebed
110
120
9
1
dresser
sq.ft.1 1
1
closet;5 lin. ft,
1
visitor chair1
bedside table
6
Double
2
singlebeds
235
245
10
room2 dressers
sq.ft,12
2
closets;@
5
ft,
2
visitor chairs2
bedside tables
7
Porch
5
side chair1
table
1
sidetable
215
sq.ft. with wood8
Bathroom
1
stall1
sink1
shower85
sq.ft.13
Activity
room1
folding
table
1
0
chairs1
wall mountedtack board
send area synthesizer artwork storage audio equipment315
sq.ft.60
sq.ft,14
Bathroom
1 bath tub
w/ seat1
stall1
sink1 10
sq.ft.15
Staff Office
2 desks
2
desk
chairs2 files
2
side chairs1
tack board
1
markerboard
150
sq.ft.16
Storage
with
Cleaning
suppliesshelves
30
sq.ft.1 7
Conference
room
1
table
6
chairs1
markerboard
1
TV
1
VCR
1
projectorcloset
125
sq.ft.18
Refuse
andSoiled
utility
room
19
Kitchen
andDining
roomcounters;
1
6'-6"lin. ft,
1
refrigerator1
table
1
dining
table
6
dining
chairs1
microwave1
range1
dish
washer153
sq.ft. with storageabove and
below the
counter with wheel chair access20
Medication
room1
counter1
sink1
medication cart1
refrigerator55
sq.ft. with onelocked
cabinet above andbelow
the
counter21
Laundry
withLinen
andClean
storage1
washer1
dryer
ironing
counter cabinet wastebaskets
1
sewing
machine55
sq.ft.22
Storage
1 0
cabinets2
cabinets70
sq.ft.23
Staff
Bathroom
1
stall1
sink40
sq.ft,24
Garage
ramp;1
0
'
-6
"lin.
ft.
van
Administrative
andMedical
Center
Type
of roomsFurnishing
for
roomSquare
footage
Remarks
1
Entrance
100
sq.ft. spacefor
storage of
at
least
2
wheel chairs
2
Social
Coordinator's
office
1
desk
1
desk
chair1
file
1
bookcase
2
side chairs100
sq.ft.3
Nurse's
office1
desk
1
desk
chair1
file
108
sq.ft.4
Doctor's
office1
desk
1
desk
chair1
file
1
bookcase
1
tea table
2
side chairs135
sq.ft.5
Dietician's
office1
desk
1
desk
chair1
counter1
refrigerator120
sq.ft. with storage above andbelow the
counter6
Bookkeeping
andMedical
Record
office2
desks
2
desk
chairs6 files
1
safe2
side chairs7
Social
workers' office
2 desks
2
desk
chairs1
file
1
bookcase
3
side chairs155
sq.ft.8
Conference
room
1
conferencetable
1
0
chairs1
makerboard
1
TV
1
VCR
1
screen1
project storage230
sq.ft.9
Administrative
Assistant's
office1
desk
1
desk
chair1
file
1
bookcase
2
side chairs1
15
sq.ft.10
Administrative
office
1
desk
1
desk
chair1
file
1
bookcase
1
cupboard1
tea table
2
side chairs144
sq.ft.1 1
Reception
area
1
information desk
1
desk
chair4
comfort chairs1
table
1
endtable
1
art work200
sq.ft.waiting
areaincluded
12
Garden
trees
birds
bird houses
13
Playground
2
swings with2
slides
1
play house
1
picnictable
with
bench
1
seesaw1
trampoline
650
sq.ft.floor
: cork14
Physical
andOccupational
Therapy
room2 desks
@18"x24"2 desk
chairsw/casters
1
markerboard
1
tack board
1
parallelbar
stairs
1
weight/pulleys4
side chairs1
mattable;
5'x7'1
standing
table
1
bicycle
1
mirror;2'x6'
1
bookcase
2
file
cabinets1
ball
480
sq.ft.15
Employee
areaBreak
room 6'linear
counter1
table
6
dining
chairsmicrowave
refrigerator
coffee maker
Men's locker
roomWomen's
locker
room2comfortable
chairs1
sidetable
6 lockers
1
bench
6 lockers
1
bench
16
Examination
room1
desk
1
desk
chairw/casters
1
sink1
bed
2
side chairsw/arms
cabinet storage
waste
basket
red
bag
wastebasket
230
sq.ft.for
medicalwaste
17
Nurse's
station1
counter16"x7"
2
secretarialchairs
6
lin. ft.
book
shelf
1
back
counter1
tack board
1
markerboard
1
chart rack1
refrigeratorfor
specimens
18
Lounge
withKitchenette
area
1
TV
w/table1
game/dining
table
4
dining
chairs4
comfortablechairs
2 tables
2
sidetables
1
bookshelf
plants1
counter1
refrigerator1
microwave425
sq.ft.19
Medication
1
counter70
sq.ft.room
1
narcoticslocker
1
refrigerator1
treatment
cartdouble
lock
20
Patient
double
bedroom
2
singlebeds
2
bedside
cabinets
2
closets2
dressers
psyc unit
lamp
2 lamps
2
high-back
chairs
2
visitor chairs310
sq.ft. with curtainspecial
lamp
construction
reg,
Shelter
proof
21
Patient
singlebedroom
1
singlebed
1
bedside
cabinet1
closet1
dresser
1
high-back
chair2
visitor chairs22
Patient
bathroom
1
stall1
sink1
bathtub
1
medicine cabinet1 15
sq.ft,23
Visitor's Suite
A,
Living
room1
counter w/sink400
sq.ft.and
1
refrigeratorKitchenette
1
microwave2
dining
tables
6
dining
chairs1
sleeper sofa2
comfortablechairs
1
tea table
1
TV
1
VCR
closet
Interior
plantsB. Bedroom
2
twin beds
1
bedside table
1
vanity
1
tea table
2
side chairscloset
210
sq.ft.C.
Bathroom
1
stall1
sink1
bathtub
80
sq.ft.D, Patio
2
chairs1
table
24
Linen
storage25
Vending
machine area2 vending
machines1
cabinet1
telephone
booth
1
drinking
fountain
75
sq.ft.26
Public
handicap
restrooms:
160
sq.ft. accessibleMen's
1
stallrestroom
1
urinal2
sinks150
sq.ft.Women's
restroom
2
stalls2
sinks27
Soiled utility
1
medical wastebarrel
2
wastebarrels
140
sq.ft.28
Janitor
1
sink30
sq.ft,29
Storage
shelf9
cabinets220
sq.ft.Landscaping
Area
Equipment
Square
footage
Remarks
1
Parking
lot
3400
sq.ft.20'
x
9'
per
car
3
Courtyard
2 barbecue
grills2
tables
4 benches
umbrellas
972
sq.ft, concretepaving
for
sunprotection
4
Swimming
pool6183.45
withfence
pool 75'
1
1/2" x45'-0"
life
safety
equipment
sq.ft.
5
Playground
1
basketball
court2 football
goalposts
B.
Survey
ofAl
Sigl
Center;
facilities
and site conditionsThe Al
Sigl Center
is located
onElmwood Avenue in
Rochester,
New York,
(see
figure
1)
The Al
Sigl
Center
is
anenvironment
that
encourages abilities and growthtoward
independence
for the disabled.
Eight
rehabilitationagencies share and cooperate while
maintaining
their
distinct
missions and programs.Thousands
of children andadults
having
abroad
range ofdisabilities,
enter andmove
freely
aboutthe Al Sigl Center in buildings
designed
to
meettheir
needs.The
Mary
Cariola Children's Center
(MCCC)
is
onepart of
the Al
Sigl's
many
branches;
its
purposeis to
enable children with multiple
handicaps to
reachtheir
greatest potential.
MCCC
serves over450
childrenfrom
birth
to 21
years of age.Mary
Cariola Children's Center
offers residential, educational,
therapeutic,
and supportservices.
Preschool
and school-age educational programsare
individual
programs offeredto teach
childrentasks,
such as
lifting
a spoon andfeeding
oneself,looking
up to
indicate
a"yes"
response,
making
abed,
ordressing
oneself.
Physical
and occupationaltherapy,
speechtherapy, behavior
modification, medical andpsychological consultation, and
nursing
services are alsopart of
the
schoolday,
and are akey
to the
children'sThe location
ofgroup
homes is generally
determined
by
easy
accessto
publictransportation
for
useby
the
staffand children,
Accessibility
of publictransportation
encourages
independent
useby
older childrenin
accessing
technical
and vocational schools,Additionally,
use of public
transportation
alsois
more cost effectivethan
having
stafftransport
childrento
andfrom
variousservices and activities.
Ideally
agroup home is located
with good access
to
hospitals,
clinics, psychiatric services,churches,
schools,
specialized educationalfacilities
aswell as
grocery
andclothing
stores.The
grounds shouldbe
attractive, withlawn,
shadetrees,
andflowers,
and should afford sufficient spacefor
outdoor activities.
In
designing
agroup
home,
suchfactors
as age ofchildren,
behavioral
problems, and physicaldisabilities
should
be taken into
accountin
determining
variationsin
space requirements, arrangement of physical
facilities,
equipment, etc,
to
ensureaccessibility
inside
and outsideof
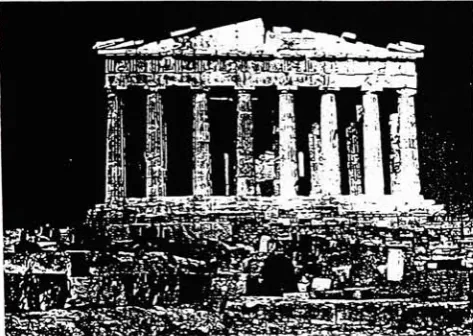
the building.
One large
oldhouse
andtwo
vacantdormitories
which
belong
to the New York State Psychiatric
Center,
stand opposite
the Al
Sigl
Center
onElmwood
Avenue, (see
figure
1,2)
Renovation
or removal ofthese
buildings
wasunder
discussion
by
the Monroe
County
Legislature
atthe
time
ofmy
initial
research.Initially, my
analysisregarding
site
for
my
Thesis
proposal.From this
site,disabled
children could go
to the Al Sigl Center
onfoot
using
anunderpass or overpass
to
connectAl
Sigl Center
withthe
Group
Homes.
In
addition,
Monroe
Community
Hospital,
Highland
Hospital,
Strong
Memorial
Hospital,
Highland
Park,
and
many elementary
schools arelocated
nearby.By
car,shopping
malls anddowntown
areonly
ten
minutes away.The
areais
alsolocated
on severalbus
routes.Upon further
examinationI
determined
that,
whilethis
site was
appropriate,
stringent code requirements couldnot
be
accommodatedin the
existing
buildings
withoutcompromising
the
project's program.I then decided to design
a prototypefacility
whichC. Code
requirementsIn the
United
States,
there
are a number of codesthat
are applicableto this kind
of project,These
codesinclude
the
Americans
withDisabilities
Act
(ADA),
American
National Standards Institute (ANSI),
the State Mental Health
Code,
Social
Services,
American National
Standards,
andStandards
for
Group
Homes Services
for
Children.
Barrier-Free design for
people withdisabilities
is
now mandatedby
Federal law
underthe ADA
of1990,
whichbecame
effective
in
1992.
This Act
sets guidelinesfor
accessibility
to
places of public accommodation and commercialfacilities.
These
guidelines areto be
appliedto the
design,
construction,
and alteration of suchbuildings
andfacilities.
The American National
Standards
Institute developed
the first handicapped
accessibility
standard(known
asANSI
Al 1 7.
1)
in 1
96
1
.This
standard statesthat
"these
specifications and
these
guidelines arebased
upon adultdimensions
andanthropometrics."
"
If
buildings, facilities,
or portions
thereof
serve children primarily,the
architectand
interior designer
should adjustthe dimensions
andother provisions
to
makethem
suitablefor
children.11
American NationalStandards
Institute,
American NationalStandard(11 West42nd"The
publicaccommodations
section ofthe ADA
affects patient and visitor areas
in
health
carefacilities,
According
to the
law,
in
new construction ofhealth
carefacilities,
all public and common areas mustbe
fully
accessible
to
everyone.Fifty
percent ofthe
rooms mustbe
accessiblein
an extended carefacility
and/ornursing
home,
and100
percentin
special carefacilities
such asrehabilitation centers."12
The
following
are someADA
andANSI
guidelinesthat
apply
to this
project:(1)
Corridors:
"The
minimum clear widthfor
singlewheelchair passage shall
be 32 inches
atany
pointand
36
inches
continuously, and minimum widthfor
two
wheelchairsto
passis
60
inches." 13(2)
Accessible bedrooms
musthave
a60-inch-diameter
circularmaneuvering
space.(3)
On
each side of patientbeds,
minimum clearfloor
space of36 inches is
neededin
accessiblepatient rooms.
(4) Readily
accessibledoors
musthave
32
inches
ofclear width.14
(5)
Health
carefacilities
must providehandrails
along
circulation routes, and
resting
areas with seatsalong
lengthy
corridors.Handrails
provide physical supportfor individuals
withimpaired
vision and ambulationproblems.
Handrails
mustbe
rounded ontop
and12
Ibid,
DesignThatCares,
p218 13Ibid,
American NationalStandards.
pl6 14behind
to fit
a person'shand
anddesigned to be
between
1
1/4 inch
and1
1/2 inches in
diameter.
(6)
Grab bars
in the
bathroom
mustbe
mountedbetween 32
and34 inches
from the floor
and1
1/2
inches
from the
wall.(7)
Public
rest rooms andbathrooms
should providemore wheelchair-accessible
toilet facilities than
currently
requiredby
code,according
to
ANSI,
anagency
which providestechnical design
criteriafor
building
codes and other regulations.(8)
According
to the
ADA,
accessible routes withinthe
boundary
ofthe
site shallbe
providedfrom
publictransportation
stops, accessibleparking
andpassenger
loading
zones, and public streets orsidewalks
leading
to
building
entrances.(9)
Buildings, facilities,
elements, and spacesthat
areon
the
same site shouldbe
connected.(10)
Ramps:
Any
part of an accessible route with aslope greater
than
1
:20 shallbe
considered a ramp.The
maximum slope of aramp in
new constructionshall
be
1:12,
andthe
maximum risefor any
ramp
runis limited to 30 inches.
(1
1)
New
constructionis
also requiredto
make atleast
50
percent of all public entrances accessible.Accessible
entrancesto
enclosedparking,
pedestriantunnels,
and elevated walkways are also required.15In
additionthere
arefire
code guidelinesfor group
homes for
children.These
standards require"All buildings
should
be
located,
constructed,
and equippedto
guardagainst
hazards.
Housing
for
children shouldcomply
withstate, provincial, and
local fire
regulations and shouldbe
periodically inspected
atleast
once a year."16All buildings
should
be
carefully
examinedfrom the
standpoint ofmaximum
fire
protection.New
buildings
shouldbe
offire-resistant materials.
Old buildings
shouldhave
sprinkler andsmoke
detectors.
Fire
exits,doors,
andhallways
shouldbe
well
lighted
andidentified
by
back-lit
exit signs,These
areas also need
to be kept
clear andready for
use,There
should
be
morethan
one exitfrom
allbuildings
andfrom
each
floor,
An
automaticfire
control systemis
important
to
the safety
of children and staff,All
electrical andheating
installations
shouldbe
approvedby
the
Underwriters'
Laboratory
and shouldbe installed
accordingly.
Where
storage of gasoline,kerosene,
fuel
oil,or other
highly
flammable
materialis
necessary, adequateprovisions should
be
madeto
meet all requirements ofsafety
andfire
codes,Group
homes
in New
York
State
must alsocomply
withrigorous
New
York
State
Mental Health Guidelines
andSocial
Services Guidelines.
III.
DEVELOPMENT
OF THE DESIGN
A. Initial
ideas
and schematicdiagram
When I
began
developing
the design
ofthis
facility,
I
felt that the
spirit ofhuman
dignity
neededto be
the
focus
of
this design.
When I
decided
to
incorporate
the design
of
three
Group
Homes
for
disabled
children with anAdministrative
andMedical
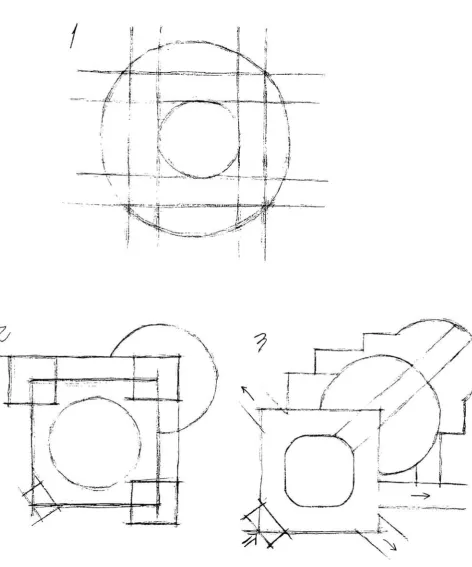
center,I first
considered amodular space organization with symmetrical
geometry
similar
to
aGreek
temple, (see Figure
3)
Drawing
onmy
ideas,
I
was careful notto
destroy
the
harmony
ofbalance
and proportion, or mirroredimages. (see Figure
4)
To
develop
the
schematicdesign,
I
sketched asquare which
had four
angles,(see Figure
4)
I
alsoconsidered
the
shape ofthe Al
Sigl
center, whichis
composed of several rectangles,
(see Figure
1)
I imagined
that
one angle couldbe for
the Administrative
andMedical
Center,
andthe
otherthree
angles couldbe
for
the three
Group
Homes.
The four
corners couldbe
used aspathways
between the
Group
Homes
andthe
Administrative
andMedical Center.
Easily
comprehensible circulationis
important to
any
building, particularly
for first-time
visitors, staff, andI
addedthe
shape of a circleto
create spaces andclarify
circulation paths,
(see Figure
4)
The
mannerin
whichthese
spaces are arranged clarifiestheir
relativeimportance
andfunctional
or symbolic rolein
abuilding's
organization.
The
spatial organization ofbuildings
andthe
spaces within
them
is
dependent
upon a number offactors
such as:
functional
proximities,
dimensional
requirements,hierarchical
classification ofthe
spaces,
and requirementsfor
access,
light,
or view.After
considering
a number of methodsto
organizespace and
revising
the
program,I
determined
that
acentralized organization would work
best for this
facility
asit
would provideeasy
accessbetween the
Administrative
and
Medical
Center
andthe three
Group
Homes.
This
method also permitted
development
of small-scale spacesin the
Group
Homes
along
withlarge
spacesin the
Administrative
andMedical Center.
Centralized
organization utilizesforms that
arerelatively
compact andgeometrically
regular and canbe
used
to
serve as an object-form within adefined field
orvolume of space.
"Centralized
organizationis
a stable,concentrated composition
that
consists of a number ofsecondary
spaces grouped around alarge, dominant.
central space,"17
(see Figure
5,6,8,10,13)
This
differentiation
among
the secondary
spaces allowsthe
17
FrancisD.k..
Ching,
Architecture FormSpace & Order(VanNostrand ReinfoldCompany,
Inc.1979)
p206form
of centralized organizationto
respondto
varying
conditions of
its
site.I
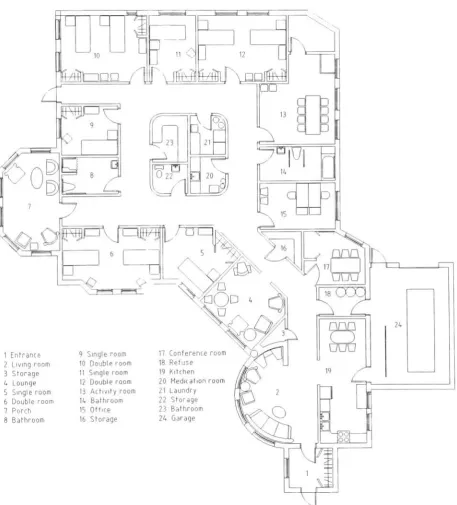
also applied radial organizationto the
Group
Home
spaces.
"Radial
organization of space combines elementsof
both
centralized andlinear
organizations."18(see Figure
7,22,30)
Strictly
speaking, centralized organizationis
anintroverted
schemethat focuses inward
onits
centralspace;
radial organizationis
an extroverted schemethat
reaches out
to its
context.With its linear
arms,it
canextend and attach
itself to
specific elements orfeatures
ofits
site.As
with centralized organizations,the
centralspace of radial organization
is generally
regularin form.
The
radiating
arms can alsodiffer from
one anotherto
respond
to their individual
requirements offunction
andcontext.
This
arrangement resultsin
adynamic
patternthat
visually
suggests a rotational movement aboutthe
central space.
18
B. Spatial
relationshipsThere
are severaltheories that
guidethe
creation ofspatial relationships.
My
goalis to
synthesizethe theories
of spatial relationships
to both
separate andjoin these
diverse functions, (see Figure
5)
"Adjacency
is the
most commontype
of spatialrelationship.
It
allows each spaceto be clearly
defined
and
to
respond, eachin its
own way,to its functional
orsymbolic requirements."19
Through the
use of an adjacentrelationship,
two
spacesthat
are separatedby
distance
can
be linked
by
athird,
intermediate
space.The
intermediate
space candiffer
in form
and orientationfrom
the
othertwo
spaces.The intermediate
space can,if
large
enough,become the
dominant
spacein the
relationship, and
be
capable oforganizing
a number ofspaces about
itself,
The degree
of visual and spatialcontinuity that
occursbetween two
adjacent spaces willdepend
onthe
nature ofthe
planethat
both
separatesand
binds
them
together,
In
my
site plan,the
Administrative
andMedical
Center
arelinked
withthe three
Group
Homes through
the
use of an adjacent relationship.
The Center
alsois
separated
from the three
Group
Homes
through
the
use of19