A CROSS SECTIONAL STUDY TO ASSESS OLFACTORY FUNCTION AND QUALITY OF LIFE CHANGES IN PATIENTS WITH ALLERGIC RHINITIS BEFORE AND AFTER MEDICAL THERAPY
A dissertation submitted to the Tamil Nadu Dr. M. G. R. Medical University, Chennai in
partial fulfilment of the requirement for the MS Otorhinolaryngology (Branch IV)
A CROSS SECTIONAL STUDY TO ASSESS OLFACTORY FUNCTION AND QUALITY OF LIFE CHANGES IN PATIENTS WITH ALLERGIC RHINITIS
BEFORE AND AFTER MEDICAL THERAPY
Dissertation submitted to the
THE TAMIL NADU DR. MGR MEDICAL UNIVERSITY, CHENNAI
In partial fulfilment of the requirements for the degree of
MASTER OF SURGERY
IN
OTORHINOLARYNGOLOGY
By
KATTI BLESSI SARA
Register number: 221414353
DEPARTMENT OF OTORHINOLARYNGOLOGY
CHRISTIAN MEDICAL COLLEGE
VELLORE
CERTIFICATE
This is to certify that “A CROSS SECTIONAL STUDY TO ASSESS OLFACTORY
FUNCTION AND QUALITY OF LIFE CHANGES IN PATIENTS WITH ALLERGIC RHINITIS BEFORE AND AFTER MEDICAL THERAPY
” is the bonafide work of Dr. KattiBlessi Sara under my supervision in the Department
of Otorhinolaryngology, Christian Medical College Vellore in partial fulfilment of the
requirements for the M.S ENT Examination Branch IV of the Tamil Nadu Dr. M.G.R
Medial University to be held in April 2017 and no part thereof has been submitted for
any other degree.
Dr. Rupa VedantamMS,DLO
Professor and Head
Department of ENT Unit 3
Christian Medical College&Hospital
Vellore-632004.
CERTIFICATE BY THE HEAD OF THE DEPARTMENT/ PRINCIPAL
This to certify that “A CROSS SECTIONAL STUDY TO ASSESS OLFACTORY
FUNCTION AND QUALITY OF LIFE CHANGES IN PATIENTS WITH ALLERGIC RHINITIS BEFORE AND AFTER MEDICAL THERAPY” is the bonafide work of Dr.KattiBlessi Sara under the supervision of Dr.RupaVedantam,
Professor and head of ENT unit 3 in the Department of ENT, Christian Medical College
Vellore.
Dr.Rita Ruby AnbuselviDr Anna P Pulimood
Professor and Head, Principal
Department of Otorhinolaryngology,Christian Medical College
Christian Medical CollegeVellore.
DECLARATION
I, Katti Blessi Sara, do hereby declare that the dissertation titled “A CROSS
SECTIONAL STUDY TO ASSESS OLFACTORY FUNCTION AND QUALITY OF LIFE CHANGES IN PATIENTS WITH ALLERGIC RHINITIS BEFORE AND AFTER MEDICAL THERAPY” is a genuine record of research done by me under the supervision and guidance of Dr Rupa Vedantam, Professor and head,
Department of ENT-Unit 3, Christian Medical College, Vellore and has not previously
formed the basis of award of any degree, diploma, fellowship or other similar title of
any university or institution.
Vellore Katti Blessi Sara
Acknowledgements
I would like to thank God for giving me this opportunity to study and His divine
providence in helping me to finish this dissertation.
I would like to express my deep gratitude to my esteemed guide and teacher, Professor
and head, Dr. Rupa Vedantam for designing the study, for her constant support,
meticulous guidance without which this dissertation would not have been possible.
I am extremely thankful to Ms. Tunny Sebastian, for all her help in analysing the data
and results.
I would like to thank Dr. Rita Ruby, Professor and head of ENT for her constant support
and words of encouragement.
I would like to thank Dr. Reji Kurien and Dr. Suma Susan for helping me to recruit
their patients in my study and encouraging me to be persistent in my effort.
I would like to thank Dr. Lalee for all her suggestions and help in completing the work
I am very grateful to Dr. Vijay and Dr. Raghav without whose help I would not recruit
the patients in my study.
I am thankful to Professor Juniper for giving me the copy right permission to use the
QOL questionnaire for my study.
I would like to express my thankfulness to Mrs. Bhavani for coordinating the work and
helping me to finish this work.
I would like to thank all my patients for being a part of my study.
I would like to thank Dr.Ebenezer for helping me with the translation of consent forms.
Lastly, I am so thankful to God for my parents, younger brother and younger sister
Esther, for all the technical help and fine tuning my work and continuously cheering me
TITLE
A cross sectional study to assess olfactory function and quality of life changes in
patients with allergic rhinitis before and after medical therapy.
.
DEPARTMENT
Department of Otorhinolaryngology, Christian Medical College, Vellore
NAME OF THE CANDIDATE :KattiBlessi Sara
DEGREE AND SUBJECT : MS ENT
NAME OF THE GUIDE :Dr Rupa Vedantam
BACKGROUND
Allergic rhinitis is a common inflammatory disease prevalent world wide which is
known to affect both olfaction and quality of life. Very little information is available
regarding the impact of medical therapy on these parameters in patient with allergic
rhinitis in the Indian subcontinent.
OBJECTIVES
1)To assess the prevalence of olfactory dysfunction in patients diagnosed with allergic
2) To evaluate associated quality- of –life changes in patients diagnosed with allergic
rhinitis 3) To assess the reversal of olfactory dysfunction and any change in quality –of-life
in affected patients following medical therapy
METHODS
A cross-sectionalhospital based study was conducted prospectively in patients
diagnosed with allergic rhinitis All recruited patients underwent butanol threshold testing for
assessment of olfactory function and assessment of quality of life using a RQLQ questionnaire.
These patients underwent medical therapy with steroidal nasal spray, antihistamines and/ or
leukotriene receptor antagonists for about 8-12 weeks
At the end of therapy, the same tests were administered again. As there is no normative
data for the Indian population, 40 normal individuals were tested to obtain normative
data for olfaction testing.
RESULTS
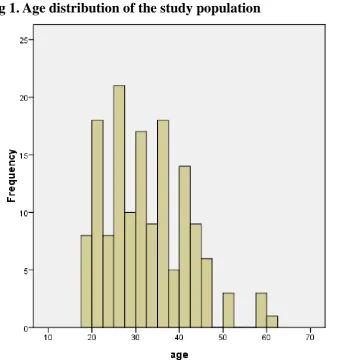
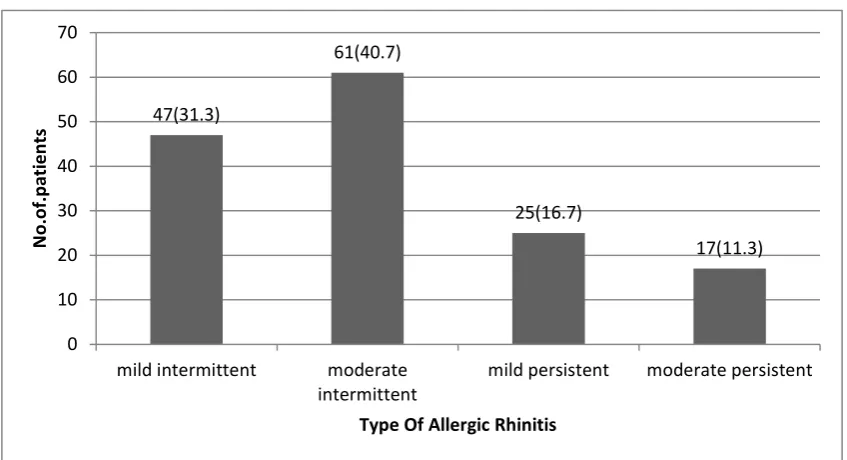
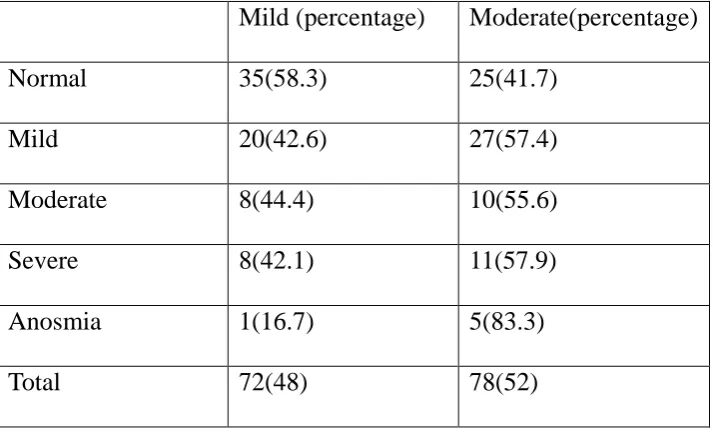
A total of 150 patients with allergic rhinitis were recruited. Most patients (72%)
had intermittent, mild or moderate allergic rhinitis. Smokers were more likely to have
moderate to severe allergic rhinitis than non-smokers (p=0.01). The prevalence of
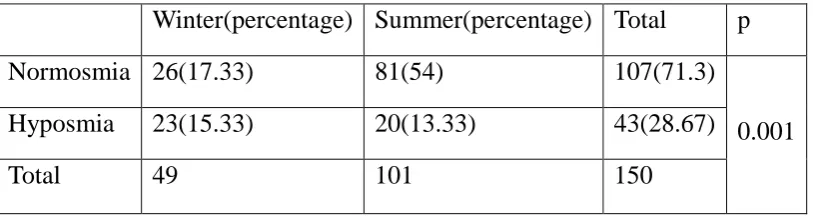
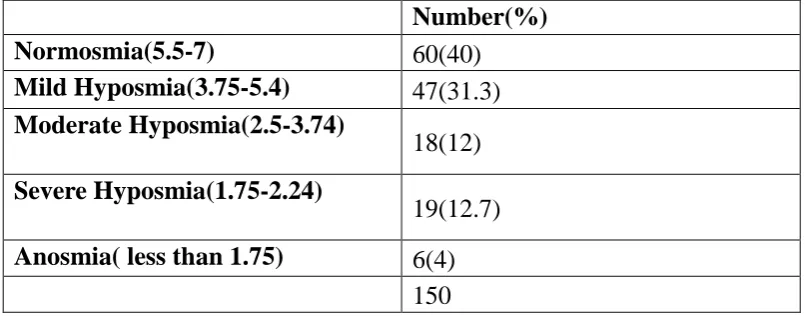
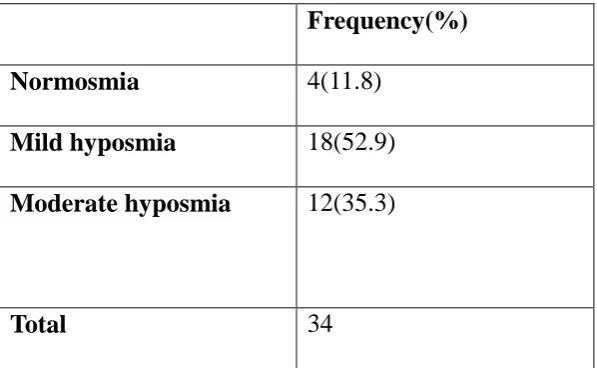
hyposmia in patients with allergic rhinitis was 28.7%. The degree of hyposmia was mild
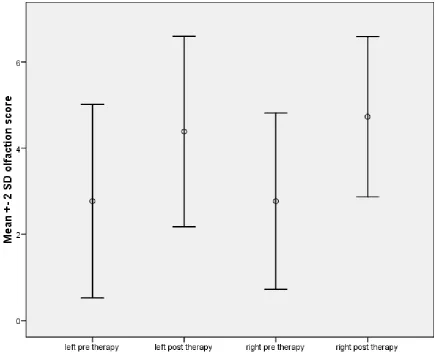
(52.9%) or moderate (35.3%)in the majority. Following therapy, there was a significant
improvement in olfaction scores (p=0.001). Quality of life (QOL)was affected in all
patients with allergic rhinitis and the mean QOL scores were raised, particularly those
significant improvement following therapy (p=0.00)
CONCLUSION
Allergic rhinitis impacts both olfaction and quality of life in Indian patients.
The problem is more pronounced in smokers. With adequate medical therapy which
includes a steroid nasal spray, antihistamine and leukotriene anatagonist, most patients
Contents
ABSTRACT ... 13
TITLE ... 17
Introduction ... 22
Aims & Objectives ... 25
Review of the literature ... 27
ANATOMY and PHYSIOLOGY ... 28
Chemosensory elements in humans ... 29
Histology of olfactory epithelium ... 30
Embryology of Olfaction ... 32
Olfactory pathway... 33
Theories of Olfaction ... 34
Central Pathway for olfaction ... 35
Effect of olfaction with ageing and in disease ... 36
Tests of olfaction ... 37
Allergic rhinitis ... 38
Pathophysiology of sinonasal allergy ... 39
1.Sensitization ... 39
2. Early Phase Response ... 42
3. Late phase response ... 44
SYSTEMIC ACTIVATION ... 48
Clinical manifestations of sinonasal allergy ... 48
Effect of olfaction in allergic rhinitis ... 49
Diagnosis of allergy ... 51
Classification of allergic rhinitis ... 52
Quality of life in sinonasal allergy ... 53
Therapeutic Options in Sinonasal allergy ... 55
Histamine ... 55
ANTIHISTAMINES ... 58
Studies showing the efficacy of antihistamines in allergic rhinitis ... 63
INTRANASAL STEROIDS ... 65
Effect of treatment of allergy on olfaction ... 69
Materials and methods ... 71
Chemosensation, which includes the sensations of both smell and taste, is an
important aspect of the sensory system in human beings. It involves the transduction of
chemicals into sensations. Olfaction is the special sense mediated by sensory cells
located in the olfactory area of the nasal cavity. One of the prime uses of the sense of
olfaction in human beings is that it is helps to act as a surveillance system which
detects the hazards in the environment. The other functions of the olfactory system
include generating feelings of pleasure, promoting adequate nutrition, influencing
sexuality and influencing mood. Any cause of dysfunction could potentially be a
source of emotional distress to the patient(2).
The sensation of olfaction may be affected by various physiological and
pathological conditions. Some of the physiological conditions that can affect the
sensation of smell include age, puberty and pregnancy. A decreased sense of smell may
be associated with certain nasal conditions like allergic rhinitis, atrophic rhinitis and
sinonasal polyposis. Head trauma can sever the olfactory rootlets and cause anosmia.
Tumours of the nasal cavity including olfactory neuroblastoma , a tumour arising from
olfactory epithelium cause anosmia. Various neurodegenerative conditions can
diminish olfaction. A number of air-borne and water borne toxins can damage olfactory
epithelium. Atrophy of the olfactory bulb may be present even at birth or secondary to
an acquired disease leading to anosmia.
In the present study we have aimed to study the degree of affectation of the
with sneezing, watery nasal discharge, nasal obstruction, epiphora and heaviness of the
head. Additionally, patients with allergic rhinitis often complain of decreased smell
sensation. Objective assessment may reveal affectation to a variable degree, however.
Very often, however, the sensation of smell is restored with appropriate therapy of nasal
allergy. Some patients, however, do not recover completely.
In order to study the impact of allergic rhinitis on olfaction, we aim to present the
results of subjective and objective assessment of the olfactory system in patients with
allergic rhinitis both before and after initiation of therapy. Simultaneously, we will also
AIM
A cross sectional study to assess olfactory function and quality of life changes in
patients with allergic rhinitis before and after medical therapy.
OBJECTIVES
1) To assess the prevalence of olfactory dysfunction in patients diagnosed with allergic
rhinitis
2) To evaluate associated quality- of –life changes in patients diagnosed with allergic rhinitis
3) To assess the reversal of olfactory dysfunction and any change in quality –of-life in affected
ANATOMY and PHYSIOLOGY
The nose is an important sense organ in the body and it performs two main functions. It
acts both as a respiratory passage and organ of smell.
The nasal cavity extends from the nostrils to the posterior nasal apertures and is sub
divided into right and left halves by the nasal septum. Each half has a roof, floor, and
medial and lateral walls. Each half measures 5 cm in height, 5-7 cm in length, and
1.5cm in width near the floor. The width near the roof is only 1-2 mm. The nasal septum
is a median osseocartilaginous partition between the two halves of the nasal cavity. The
sensory nerve supply of the nasal septum is mainly derived from trigeminal nerve. The
superior part of the septum is supplied by the internal nasal
branch of the anterior ethmoidal nerve. The posteroinferior part is supplied by the
nasopalatine branch of the pterygopalatine ganglion. Special sensory nerves or
olfactory nerves are confined to the upper part or olfactory area(3).
Olfactory area in humans
This is an area located approximately 7 cm from the anterior end of the nasal cavity
in the roof. It is approximately 1 square centimetre in area and includes the
cribriform plate and adjacent areas of the septum and lateral wall of the nose.This
area can be distinguished from the rest of the nasal mucosa because of its yellow
Chemosensory elements in humans
Human chemosensation comprises of 4 distinct elements.
1.Nervus terminalis..
This has been identified as terminal nerve system which is called as cranial nerve
zero(5).
2.Main olfactory nerve i.e. olfactory nerve
3.Vomeronasal or accessory olfactory system
Olfactory nerve which is the first cranial nerve mediates the sense of smell and
the perception of flavour. This nerve innervates the olfactory epithelium which is
present at the cribriform area(6).
Free nerve endings of the trigeminal nerve which is the fifth cranial nerve
innervates the entire nasal cavity. The nerve endings are sensitive to irritation, burning ,
cooling and tickling sensations. The odorants which are in high concentration stimulate
these nerve endings and they initiate reflexes which increase secretions from nasal
mucous glands, halts the inhalation of potentially noxious and harmful substances
which can damage the lower airway. Cranial nerve zero which has been described in all
the vertebrates including humans comprises of a loose plexus of nerve fibres in the
nasal cavity. These nerves are identified with their nodal points which are present at the
end of these nerve fibres(7).
Histology of olfactory epithelium
Olfactory epithelium which lines the nasal cavity serves the special purpose of
olfaction. It is a pseudostratified columnar epithelium and it contains olfactory
receptors beneath the cribriform plate in the nasal vault. Olfactory epithelium
consists of 4 different types of cells which are olfactory cells, supporting cells, basal
cells and brush cells. Olfactory mucosa is histologically made of three layers, epithelial
layer,basal lamina and lamina propria which adheres to the underlying bone or
Olfactory cells
These cells consist of the cell bodies of bipolar neurons which
aggregate to form the olfactory nerve. The nerve fibres pierce the cribriform plate
and terminate on the dendrites of mitral cells lying in the glomeruli of the olfactory
bulb. The apical poles of the neurons are covered with non motile cilia and they have
olfactory receptors. These receptors contain odorant binding proteins which are
dissolved in the secretions of the Bowman’s glands. The process of dissolving of these
proteins in the secretions of Bowman’s glands is essential for the process of olfaction.
Supporting cells
and act as metabolic and physical support for the olfactory cells(8). The nuclei of
these cells is more apical than the epithelial cells
Basal Cells
These cells lie on the basal lamina of the lining epithelium. These are stem cells
which are capable of division and differentiation into either a supporting cell or
olfactory cell. This constant division causes olfactory epithelium to be replaced in every
2-4 weeks. These cells can be of two types: horizontal basal cells which lines the
olfactory epithelium and more superficial globose basal cells(9).
Brush cells
These are columnar cells which bear microvilli and help in transduction for general
sensation. The nerve fibres are terminal branches of trigeminal nerve. These act as
afferents for non- olfactory signals
Bowmans glands
Bowman’s glands are tubuloalveolar glands located in the lamina propria
of the olfactory epithelium which secrete mucus. These glands are also called olfactory
glands. They deliver a proteinaceous substance to the surface of the mucosa. These
secretions trap and dissolve odorants and present them to the bipolar neurons. Old odors
are washed away by the constant flow from these glands(10).
Embryology of Olfaction
differentiates to form olfactory placodes. Invagination of the central part of olfactory
placodes forms the olfactory sac. The olfactory sac opens anteriorly and the olfactory
organ is the only organ in the body where the cell bodies lie in direct contact with
external environment.
Olfactory pathway
The olfactory pathway can be broadly divided into a peripheral system which
receives the odorant stimuli and a central pathway that processes the stimulus so
generated. The olfactory nerve, like the optic nerve, is considered as part of the central
nervous system, however.
Upto 10- 20 million olfactory cells are present in the nasal mucosa and the cell
bodies of these cells act as primary olfactory receptor neurons(ORN). The proximal end
of the ORN which has unmyelinated axons joins to form myelinated fibres which are
called fila olfactoria. There are about 15- 20 foramina in the cribriform plate.The
olfactory fila pass through the cribriform plate to synapse in the olfactory bulb. As the
pathway is short which communicates the nasal cavity with the central nervous system,
there is a higher chances of damage in this pathway and higher risk of spread of
infection from the nasal cavity to the central nervous system.
The olfactory cilia project down into the mucous layer which is rich in lipids. This
mucous is secreted by Bowmans glands which resides in the olfactory epithelium and
helps in transporting the odorant molecules which interact with the olfactory receptors
Above the mucus layer rests the base of the olfactory epithelium which has basal
cells which divide through mitosis which later form the olfactory receptor neurons and
the turnover of these neurons is 40 days. The receptor neurons has pigmented cells
which are light yellow in humans and the depth of the colour correlates with olfactory
sensitivity
Theories of Olfaction
The steric theory of Odour
Linus Pauling in 1946, illustrated that the specific odour quality is due to the
molecular shape and size of the odor molecule.He suggested that the chemical
molecules which are air borne are smelt only when they fit into the specific receptor
sites. This was like a lock and key mechanism. This receptor is then activated and
couples the G-protein and the signal transduction cascade begins.
The vibrational theory of olfaction
Dyson suggested this theory which states that the vibration of a specific
molecule is associated with odour. This validity of this theory did not last after 1970 as
there were different enantiomers (molecules which are not mirror images of each other)
which were described which have same spectrum in the infra red zone but smelt
Central Pathway for olfaction
Olfactory receptor neurons extend to contact odorants in the atmosphere on
one side of the cribriform plate of ethmoid, while on the opposite side the neuronal
cells bundle to form groups which penetrate the cribriform plate, reaching the olfactory
bulb where they converge. In the olfactory bulb a complex coding and decoding process
occurs before the signals are sent to various parts of the central nervous system. The
detection of odorants starts with a sniff causing turbulent airflow , odorant dissolving
into the mucosa which are transported by chaperons which are the transport molecules
to the specific odorant binding protein, thus producing the olfactory signal. The second
method in olfaction is retrograde, whereby the odorants which arise from the
nasopharynx ascend into the choana, thus reaching the olfactory epithelium.This is an
important pathway for the perception of the flavour of the food. The olfactory
epithelium is provided with myelinated fibres from the trigeminal nerve. The distal
fibres of the trigeminal nerve are between the supporting cells under the epithelial
surface and here they are unmyelinated. They respond to sensory stimuli. After leaving
the olfactory bulb, the second order neurons form the olfactory tract. This tract passes
along the base of the frontal lobe and enters in a complex pattern in the pyriform cortex,
anterior commisure, caudate nucleus, olfactory tubercle, and anterior limbus of the
internal capsule with secondary connections. Here it reaches the olfactory cortex where
Effect of olfaction with ageing and in disease
Olfaction can be disrupted in various diseases. There is perceptual interweaving of the
odour and taste. There is also replacement of the olfactory epithelium with respiratory
epithelium and loss of bulb neurons as age progresses .
Causes of smell impairment
Intranasal airway obstruction
• Trauma
• Edema
o Allergic, including polyps and vasomotor rhinitis
o Inflammatory ededma
• Exudates
• Neoplasms
• Atrophic rhinitis
• Ageing (mucosal replacement)
• Viral infections
• Toxic chemicals and drugs
Head trauma
• Fracture of the cribriform plate
• Shearing laceration of the olfactory nerves
• Haemorrhage causing intereference with frontal lobes, olfactory bulbs or tracts
Intracranial lesions
Endocrine
• Kallmans syndrome
• Turners syndrome
Psychiatric problems
Tests of olfaction
There are various tests to assess olfactory dysfunction in patients. The tests include the
Sniffin’ sticks test(11), UPSIT(University of Pennsylvania Smell Identification test)(12)
and CCCRC test(Connecticut Chemosensory Clinical Research Centre)(13). The
CCCRC test which is widely used consists of 3 components, viz., threshold testing
using butanol, odour identification and odour discrimination. In the butanol threshold
Each nostril is tested separately. The point of transition between no detection of smell to
identification of smell is considered as the threshold for that individual. Based on the
results of the 3 components of the CCCRC test, a composite score is calculated. A
diagnosis of anosmia, hyposmia and normosmia may be made, depending on the
composite score obtained. As the CCCRC test is easy to perform and can be
administered within a few minutes, it is the preferred test for assessment of olfaction.
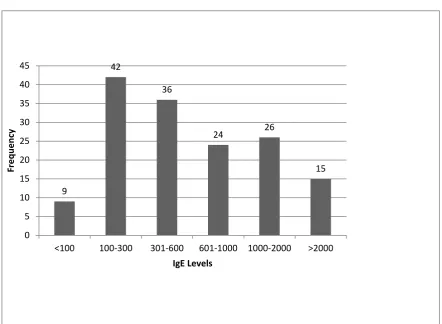
Allergic rhinitis
Allergic rhinitis is a disorder of the nose induced after the exposure to allergen. This is
due to IgE mediated inflammation of the membranes lining of the nose(15). The
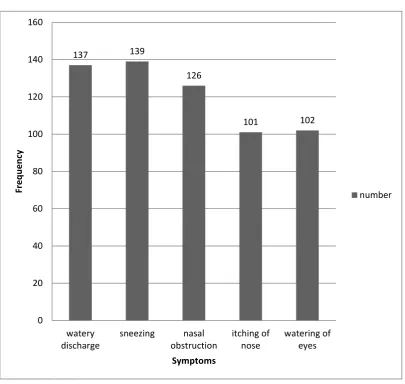
three cardinal symptoms affecting the nose in allergy are sneezing, nasal obstruction
and mucous discharge. Allergic rhinitis is a global health problem and a major illness
causing disability with a prevalence of . Patients from different countries, different
ethnic groups and different ages suffer from this. Allergic rhinitis affects social life,
work and scholastic performance. The economic burden of the disease is always
underestimated(16).
Allergic rhinitis is an inflammation of the lining of the nose and is characterized by
anterior or posterior watery rhinorrhoea, sneezing, nasal blockage and itching
of the nose wherein the symptoms occur on 2 or more consecutive days for more than
one hour on most days. There may be associated ocular symptoms(17).
It is the most common form of non- infectious rhinitis.There is a marked increase
continuous with that of the paranasal sinus mucosa, congestion of the ostia can result in
inflammation and obstruction to the paranasal sinuses.
Pathophysiology of sinonasal allergy
The pathophysiology of allergy is a complex process which involves cell mediators,
chemokines, neuropeptides and adhesion molecules.It is a type 1 hypersensitivity
reaction. The reaction is considered in 4 phases.
1. Sensitization
2. Early phase reaction: subsequent reaction to allergen
3. Late phase reaction
4. Systemic activation
1.Sensitization
Allergens are harmless molecules which do not elicit symptoms in non atopic
individuals. Every allergen has an antigenic epitope which is that part of the allergen
that is the antigenic determinant which is recognised by antibodies, T cells or B cells.
It is that specific region of the allergen where the antibody or immune cell binds. In
individuals who are sensitive, these allergens are not completely cleared by the
mucociliary system and are presented to Langerhans cells and dendritic cells which are
mucosa. These cells contain Birbeck granules which increase in number on exposure to
allergen. The activation of these antigen presenting cells is very important for the
activation of T lymphocytes which are located in the local lymph nodes. The epithelial
surface of the human nasal mucosa has the highest network of thedendritic cells
numbering > 500 per mm3.The epitopes of the allergen are presented by the antigen
presenting cells to the T cell lymphocytes in the local lymph nodes. The
majorhistocompatibility complex (MHC) is a set of cell surface proteins which the
epitopes of the allergens, bind to them and display them on the cell surface for
recognition by T cells. In humans, the MHC is also called human leucocyte antigen
(HLA).Th 2 cells are lymphocytes which are a subset of T cells present in local lymph
nodes which are produced by activated T cell lymphocytes. The stimulation of Th2 cells
produces cytokines. The activated Th2 cells then stimulate B cells which also
recognise the allergen through its epitope and MHC. The activated recognize B
lymphocytes in the local tissues are stimulated toproliferate, form plasma cells and
Once Ig E is produced, it is specifically taken up by the mast cells. The IgE which then
circulates in the blood stream then recognises the epitope of the allergen every time it
is exposed to it. The patient is thus sensitized and responds to subsequent contact with
2. Early Phase Response
The release of histamines, cytokines and prostaglandins in nasal mucosa cause
allergic symptoms like sneezing, rhinorrhoea and itching. These symptoms occur
within minutes of release of these mediators and are associated with them. When an
allergen is cross linked with an IgE, and this complex is attached to the mast cells, there
is degranulation of the mast cells and all the mediators for allergen response are
released. These mediators can be released from mast cells or from the arachidonic acid
on the cell membrane of the mast cells. Histamine is the most important mediator which
causes symptoms of allergic rhinitis. Its action on the sensory nerve endings causes
itching and sneezing. Its action on endothelial cells causes vasodilatation, plasma
exudation and oedema. Histamine acts directly on the mucous cells on the ipsilateral
side and on the contralateral side of the nasal cavity it acts through neural reflex.
reflexes. Histamine acts as the most important mediator in the early phase and to a
limited extent in late phase by acting on the basophil cells. It also has pro inflammatory
and immune modulatory properties. It increases the production of IL-6 and IL-8 by
activation of vascular endothelial cells with consequent cytokine production. PG D2
(prostaglandin) is the predominant prostanoids which is released.
role in asthma and rhinitis. This includes sulphidopeptide leukotriene which belongs to
the family of eicasonoids generated by lipoxygenase pathway. These increases the
vascular permeability and causes edema in the nose and recruits eosinophils and
neutrophils. Kinins may also be involved in allergic rhinitis, in early and late phases.
These are generated from plasma proteins by the action of kininogen. Kinins are found
in nasal secretions following allergic response and are found to cause rhinorrhoea,
sneezing, obstruction and pain. Preformed mediators are released by degranulation of
the mast cells which include Th2 cytokines such as IL-4, IL-5, IL-13, and
proinflammatory cytokines such as IL-6, IL-8, IL-I0 and TNF-alpha. The release of Th2
cells is very important in the regulation of IgE response. The number of mast cells
usually increase in the nasal mucosa during episodes of seasonal allergy.
3. Late phase response
If high doses of allergen is used there is a late phase response in around 50 %of the
individuals. This is primarily an inflammatory response and includes variety of cells
like macrophages, eosinophils, basophils, mast cells, T cells and neutrophils into the
local reaction site. Late phase response causes nasal obstruction and hyperactivity.
INFLAMMATORY CELLS AND THEIR REGULATION IN ALLERGIC RHINITS
MAST CELLS
In allergic rhinitis patients, mast cells are found to be in abundance in the nasal mucosal
epithelial compartment. Mast cells play the central role in mechanism of allergic rhinitis.
Iranietal(19) described two types of mast cells depending upon the type of proteases
allergic rhinitis, MC (T) type of mast cells are seen. Mast cells release mast cell
mediators and a variety of cytokines like IL- 4, IL-10. IL-6, IL-13. Mast cells causes
extra cellular matrix interaction which up regulate the cytokine production. This
mechanism helps in mast cell activation even when the concentration of antigen is very
low in the environment. Mast cell induces Ig-E synthesis in B cells and activate IgE-IgE
receptor cascade. Therefore mast cells act as the mediator for immediate response and
also as an immune regulator for the ongoing inflammation process both in intermediate
and late phase reactions.
BASOPHILS
Basophils are found in the nasal secretion of patients in
allergic rhinitis. They also play an important role in allergic inflammation. They are
usually not present in peripheral cells and hence not seen in any of the nasal epithelial
cells. The number of basophils relate with the severity of the disease. They release
histamine and cytokines like IL-4 and IL-3 and they are primarily concerned with late
phase recation
EOSINOPHILS
In any chronic allergic disease, eosinophils have an important role to play. They are
derived from a progenitor cell CD34+. These cells will either develop as eosinophils or
basophils. Eosinophils havebilobed nucleus and they are orange coloured cells. They
Their concentration is highest in nasal secretions. Eosinophilic Cell Protein is the major
constituent of nasal secretions. In the tissue , cytokines like IL-5 keep eosinophils alive
for several days by overcoming programmed cell death. Then eosinophils are matured.
These mature eosinophils contain MBP, ECP and eosinophil derived neurotoxin and
eosinophil peroxidise. They synthesize and release cytokines such as IL-3, IL-5,
proinflammatory cytokines that play an important role in the late phase.Wang etal
studied ECP in nasal secretions of 18 atopic patients and 10 healthy volunteers.
Allergen challenge in these atopics induced an increase in eosinophils that persisted for
10 h and was less at 24 h, whereas levels of ECP in these atopics peaked at 24 h
indicating possible degranulation.
T LYMPHOCYTES
They are among the principal factors that regulate the allergic immune
response in allergic rhinitis. Th1 cells predominantly release IFN- gamma and IL-2
and they are primarily responsible for the delayed hypersensitivity. Th 2 cells are
responsible for IgE release and allergic response. Inflammation of the mucosa is
characterized by infiltration of T lymphocytes both in mucosa and sub mucosa. This
causes a cascade increase in all the cytokines which regulate the allergic response and
induces IgEsynthesis by B cells
MACROPHAGES
Allergic reactions occur in a mucosal environment that is rich in both
lower and upper airways, as alveolar macrophages form more than 90% of the cell
population in bronchial alveolar lavage , but airway macrophages on the nasal epithelial
surface just account for about 1 to 2% of the cells. Still, in seasonal and perennial
allergic rhinitis, a significant increase in macrophages has also been found in the
nose .Langerhans cells represent an important group of dendritic cells in the nose,
characterised by the expression of CD1 and Birbeckgranules . These cells increase after
allergen challenge or in patients with allergic rhinitis and may serve as antigen
presenting cells in the upper airway.
EPITHELIAL CELLS
Epithelial cells are present in the mucosa of the nasal epithelium.
Their primary action is about secretion of mucus and removal of foreign body by the
action of their cilia. They also have a wide range of immunomodulatory activity by the
release of eicasnoids, endopeptidases, chemokines and cytokines. Itis now appreciated
that allergens, on account of their enzymatic proteolytic activity can directly activate
cells . House dust mite allergens have been shown to activate epithelial cells in
vitro,inducing cytokine and chemokine release and thus can induce airway inflammation independent of IgE. It has also been shown that epithelial cells in allergic
individuals are more sensitive to air pollutants like diesel exhaust particles and this has
been attributed to the greater constitutive and pollutant induced release of
ONGOING INFLAMMATORY PROCESS
Structural cells like epithelial cells, residential cells like mast cells and the infiltrated
inflammatory cells like eosinophils, basophils and T cells all play a role in inducing
and maintaining on-going allergic inflammation. While cytokines like IL-4, and IL-13
released from mast cells and T cells help drive B cells toward IgE synthesis and could
contribute to the local IgE synthesis in the nasal mucosa of patients with allergic rhinitis
SYSTEMIC ACTIVATION
Allergic Rhinitis is not just associated with local
response but also a systemic response. This response helps us to explain the link
between the patients who have rhinitis and asthma. In patients with AR without asthma
produces inflammatory response in both the upper and lower airway and increased
bronchial activity. In sensitized individuals, allergen exposure causes a release of many
inflammatory cells and few cells migrate to bone marrow and this recruits the
inflammatory cells like eosinophils and basophils to the target organs.
Clinical manifestations of sinonasal allergy
It is a recently recognised that allergic rhinitis symptoms include more than the classical
watery rhinorrhoea, sneezing and nasal block. It is associated with the impairment of
day to day life of individuals.There is a significant impairment in the quality of life of
social and emotional impairment of the normal function of the individuals(21). Poor
control of the symptoms has a significant impact on the sleep pattern.
There is a genenral impairment in the overall function of the individual at work or at
school(22). The severity of the allergic rhinitis is based on the severity of the
impairment of the normal function of an individual when compared to the other normal
individuals(23).
Effect of olfaction in allergic rhinitis
Allergic rhinitis(AR) is a common inflammatory disease prevalent world wide affecting
10-25% of the population(24). Some studies have shown that the prevalence of
olfactory dysfunction in allergic rhinitis ranges from 21%-23 %(25).Further, olfactory
with perennial AR. There are 2 potential causes for olfactory dysfunction in AR, viz.,
inflammation and obstruction.The degree of blockage is not related to the degree of
olfactory dysfunction. This suggests that olfactory dysfunction is secondary to
inflammatory response which occurs in the nasal cavity(26).
Becker etal have studied olfactory dysfunction using the sniffin’ sticks test in
seasonal and perennial AR and correlated the results with analysis of nasal secretions
and inspiratory rhinomanometry. Of a total of 72 patients, 23 were proven seasonal AR ,
16 were perennial AR and 33 healthy volunteers. The authors concluded that nasal flow
rhinomanometry did not show any significant difference in the three groups. However,
olfactory thresholds were significantly less in the AR group when compared to the
normal control group. Further, there was not much difference in the score between the
seasonal and perennial AR groups. On analyzing the nasal secretions, it was found that
increased levels of eosinophilic cationic protein was present in patients with AR
compared to the control group(27). Guilemany et al studied the impact of sense of smell
in patients with persistent AR. They studied 49 patients with persistent AR and 60
controls. The authors found that there was significant olfactory dysfunction in patients
with persistent AR when compared to the control group.All these patients were positive
for skin allergy test(28).
Some studies have shown that olfactory dysfunction improves in
patients who are treated with intranasal steroids. The mechanism behind this is unclear.
It is possible that reduction of the oedema or inflammation is the cause for this
phenomenon. Other studies have shown a significant reduction in the number of
using the topical steroid mometasonefuroate in a group of patients with AR, the
improvement in inflammation was significantly higher in patients who were
administered mometasonefuroate compared to placebo, showing that inflammation is
significantly reduced in patients using mometasonefuroate(29). Stevens et al studied the
response to topical nasal and oral steroids in patients following endoscopic
polypectomy(30). In this prospective study, 24 patients who were anosmic prior to
endoscopic and nasal surgery, were selected. Most of the patients had either bronchial
asthma or AR or both. Twelve out of 24 remained anosmic postoperatively and did not
respond to either nasal steroids or oral steroids. More patients responded to oral than
topical steroids, however. Alobid et alstudiedthe effect of oral and intra nasal steroids in
severe nasal polyposis. They randomised the patients into two groups after 4 weeks of
steroid washout period. The first group was given 2 weeks of oral steroid followed by
12 weeks of intranasal steroids. The control group which included 22 subjects did not
receive any steroid treatment .Barcelona Smell Test 24 (BAST-24), nasal congestion,
tissue eosinophilia, and nasal nitric oxide were assessed.The authors found that
combined nasal and oral steroids improved olfaction in the cases but not the
controls(31). Very few studies have evaluated the change in olfaction following medical
therapy of AR without polyposis.
Diagnosis of allergy
The diagnosis of Allergic rhinis is based upon the concordance of the history and
diagnostic tests. The typical symptoms include watery nasal discharge, sneezing and
Diagnostic tests include skin allergy test and an increased IgE levels in the blood. Skin
Allergy test which is commonly used is prick and puncture test(32). The modified skin
prick test by Pepys is the current test which is commonly used(33). Negative and
positive controls are used in this test. Negative control consists of the diluents which are
used to preserve the allergen vaccine(34). A rare dermographic patient can produce
wheal and flare to the diluents which are used(35). Positive control is used to detremine
the supression by medication and the technique of administartion of the test. The usual
positive control which is used is histamine dichloride (36)
Classification of allergic rhinitis
Mild
Normal Sleep
Normal daily activities
Normal Work and School
No troublesome
symptoms
Intermittent symptoms ≤4 days per week Or ≤ 4 weeks
Persistent symptoms
4 days per week and > 4
weeks
Moderate-Severe One or More Items
Abnormal sleep
Impairment of daily
activities sports, leisure
Problems cause at school or
work
Quality of life in sinonasal allergy
Allergic rhinitis causes impairment in the performance of daily functions by
patients thus affecting the quality of life both in children and adults. Patients can also
suffer from sleep disorders, emotional problems and imapirment in routine social
activity and social functioning.
Olfactory function is an important component of quality of life (QOL) and mental
health in patients with sinonasal disease(37). Various indicators have been used to
assess the quality of life in patients with sinonasal disease. These include SF-36
QOL(short form health survey), SNOT 22(sino nasal outcome test), ESPRINT 15.
RSDI(rhinosinusitis disability index), RQLQ (rhinoconjuctivitis and quality of life) and
HRQL (health related quality of life). SF -36 is a generic QOL instrument which does
not specifically address olfaction or allergy(38). In contrast, the ESPRINT-15
(short-form instrument to measure health-related quality of life in adults suffering from
allergic rhinitis) questionnaire, which was first developed and validated on a Spanish
population, is unique in that it assesses QOL in patients with allergic rhinitis(39). The
instrument contains 15 items covering 5 domains, viz. Symptoms (5 items), daily
activities(3 items), sleep (3 items), psychological affectation(3 items) and wellness (1
item). Items are scored using a 6 point Likert scale, ranging from 0 to 6. In a study on
patients with mild, moderate and severe AR, Valeroetalfound that there were significant
differences in the global score and individual scores of ESPRINT QOL between the
various categories. Juniperetalhave designed RQLQ questionnaire to assess the
quality of life in patients with rhinoconjunctivitis with or without allergic in origin. This
in 7 domains (activity limitation, sleep problems, nose symptoms, eye symptoms,
non-nose/eye symptoms, practical problems and emotional function). There are 3
‘patient-specific’ questions in the activity domain which allow patients to select 3
activities in which they are most limited by their rhinoconjunctivitis. Patients recall how
bothered they have been by their rhinoconjunctivitis during the previous week and to
respond to each question on a 7-point scale (0 = not impaired at all - 6 = severely
impaired). The overall RQLQ score is the mean of all 28 responses and the individual
domain scores are the means of the items in those domains.
A number of studies have shown improvement in QOL after
therapy in patients with AR. Mir etal in their review have concluded that the burden of
AR on school going children and the impact of it on their quality of life is significant .
They have also found that intranasal corticosteroids have been the best treatment in AR
thus far .Canonica et alhave studied the effect of quality of life in AR. They used an
online survey and telephonic interview of 3635 people with AR. The authors found that
many patients have poor quality of life secondary to AR .Kalpiagolu et alsimilarly
evaluated the quality of life in patients with asthma and AR and a combination of
both.They studied a total of 316 patients out of which 232 had AR, 40 had asthma and
44 had both diseases. The authors used the SF 36 and HRQL questionnaire to assess the
quality of life. They found that AR has a minor role on quality of life. Juniper et al
validated and developed a questionnaire to assess the quality of life in children with
rhinoconjunctivitis.The authors developed a questionnaire which was accurate and
used to assess QOL in patients with AR.
Therapeutic Options in Sinonasal allergy
Histamine
Pharmacology
The biogenic amine, histamine acts as a major mediator for inflammation and
anaphylaxis and gastric acid secretion and a major role in neurotransmission. It acts
through 4 classes of receptors
Chemical structure
It’s a hydrophilic molecule consists of an imidazole ring and an amino
group. These two rings are connected by two methylene groups. The pharmacologically
active form of the histamine is the monocationic form. H3 and H4 receptors have a
higher affinity that H1 and H2. The four receptors can be activated by any nalogue of
histamine.
Distribution and Biosynthesis of Histamine
Histamine is present in almost all the mammalian tissue ranging from <1
to >100microgm. The mast cell is the predominant storage site for the histamine in most
tissues. The concentration is high in those cells where mast cells are high like skin,
bronchial mucosa and intestinal mucosa.
Synthesis, storage and Metabolism
Its formed by the decarboxylation of the amino acid histidine by the enzyme
L-Histidine decarboxylase. This enzyme is present in the every mammalian tissue that
blood. These cells store histamine in secretory granules and they have the ability to
synthesize histamine. Non mast cells sites of histamine formation consists of gastric
mucosa, epidermis and neurons within the CNS. Turnover is rapid at the non mast cell
site as the histamine is not stored but released continuosly. There are two major paths of
histamine metabolism in humans. The most important one is ring methylation to form
N-methylhistamine . Most of the N-methyl histamine is then converted to N-methyl
imidazole acid by monamineoxidase(MOA)
Release and functions of endogenous histamine
Histamine plays a central role in immediate hypersensitivity and allergic responses.
As it is released from the storage granules, it interacts with IgE antibody on the mast
cell surface. And thus participates in the entire hypersensitivity response. Histamine has
a major role in neurotransmitter release and also gastric acid secretion.
Role in Allergic Response
The principal target cells of immediate hypersensitivity is mast cells and basophils.
As a part of the allergic response to an antigen. IgE antibodies are generated and bind to
the surface of mast cells and basophils via a receptor. Antigen bridges the IgE
molecule via FceR1 and activates signalling pathways in mast cells and basophils.
Pharmacological Effects
Receptor-effector coupling and mechanisms of action
Histamine receptors are GPCR . H1 receptor is coupled to GQ11 and activate adenylyl
cyclase pathway, where as H3 and H4 receptors inhibit adenylyl cyclase
pathway.Stimulation of H1 receptors on smooth muscle cause contraction, whereas
Histamine Receptors
Ash and Sehild predicted the existence of histamine receptors.
H1 and H2 receptors
These receptors are widely distributed in the peripheral and central nervous
system..Histamine exerts local or wide spread effects on smooth muscles and glands.It
causes itching and stimulation of secretion from nasal mucosa. In lungs it contracts the
bronchial smooth muscles and in gut causes contraction of smooth muscles and apotent
stimulator of gastric acid secretion. Bronchoconstriction and contraction of gut and
nasal mucosal secretion are mediated by H1 receptors. Gastric acid secretion are
mediated by H2 receptors.
H3andH4 receptors
H3 receptors are auto receptors. They inhibit histamine release and modulate releasof
otherneurotransmitters.H3 receptors high constitutive activity, histamine release is
tonically inhibited and inverse agonist will thus reduce receptor activation and increase
histamine release from histaminergic neurons. Therefore H3 agonist promote sleep and
antagonist promote wakefulness.H4 receptors are found in cells of haematogenic
origin like eosinophils, basophils, monocytes and mast cells. Activation of H4 receptors
in these cells induces cellular shape change, chemotaxis , secretion ofcytokines and up
regulation of adhesion molecules. This suggest that, H4 antagonist can be used in
Effect of histamine release on increased capillary permeability
The effect of histamine on small vessels causes efflux of plasma
protein and fluid into extracellular spaces and increases lymph flow thus causing
edema.H1 receptors are the major mediators of this response. Increased permeability is
caused by histamine activation of H1 receptors on post capillary venules. This contracts
the endothelial cells and exposes the basement membrane which is freely permeable to
plasma proteins and fluid.
Triple response of Lewis
Intradermal injection of histamine produces a characteristic response known as the
triple response. This consisits of
• Localised red spot a few millimetres around the site of injection within a few
seconds and reaches its maximum in less than a minute.
• A brighter red ‘flush’ or ‘flare’ extending more than 1cm beyond the red spot
develops more slowly.
• A wheal that is seen within 1-2 minutes occupies the same area as the original
red spot.
Initial red spot results from direct vasodilating effect of histamine, flare is due to
histamine induced stimulation of axon reflexes that causes vasodilation indirectly and
wheal is histamines capacity to increase the capillary permeability
ANTIHISTAMINES
Antihistamine was first described by Bovet and Staub in 1937. The initial substance
colleagues described pyrelamine maleate an effective antihistamine which was used
clinically. In 1980, non sedating antihistamines were developed for the treatment in
allergic responses.
Pharmacological properties Chemistry
All the H1 receptor antagonists are inverse agonists that reduce the constitutive activity
of the receptors and compete with histamine. This causes antihistamine binding to the
receptor thus causing inactive conformation. If a histamine binds to the receptor it
causes active conformation. Like histamine, many of the antihistamines
contain a substituted ethylamine moiety. Unlike histamines it’s a tertiary amino group
linked by 2 or 3 atom chains to two aromatic substances.
Mechanism of action
Immediate hypersensitivity reactions : Anaphylaxis and allergy
Histamine is the most potent autocoid released in hypersensitivity reactions. The
symptoms ensuing its contributions varies from species to species. Therefore the
protection offered by H1 antagonist also varies from species to species. In humans,
itching and edema formation are well suppressed, however its effect on blood pressure
is not very marked.
Capillary permeability
H1 antagonists block increased capillary permeability ,edema and wheal caused by
histamine. H1 antagonists suppress the action of histamine on nerve endings, thus
Classification of antihistamines
Antihistamines which are used in allergic rhinitis belong to H1 antagonist group
These drugs are classified into classified into first and second generation antihistamines
primarily based on the ability to cross the blood –brain barrier. The second generation
antihistamines primarily act on the peripheral H1 receptors and have a reduced ability to
cross the blood brain barrier. They are thus less sedating in action. The drugs included
in these 2 classes are seen in the table .The differences between the 2 classes of
antihistamines is also listed .
First generation antihistamines
• Tricyclic dibenzoxipens
• Ethanaloamines
• Ethylenediamines
• Alkylamines
• Piperazines
• Phenothiazines
• Piperadines
Second generation antihistamines
• Tricyclic
• Alkylamines
• Piperazines
• Piperadines
Chemical Classification of H1 antihistamine
Alkylamines
Ethanolami
nes
Ethylenediam
ines
Phenothiazi
nes
Piperazin
es
Piperidine
s
Brompheniramin e Carbinoxamin eAntazoline Promethazine Buclizine Azatadine
Chlorpheniramin e
Clemastine Tripelennamine Trimeprazine Cyclizine Cyprohepta
dine Dexchlorphenira
mine
Dimenhydrin ate
Pyrilamine Mequitazine Meclizine Ketotifen
Pheniramine Diphenhydra
mine
Oxtamide Loratadine
Dimethindene Doxylamine Hydroxyzi
ne
Desloratadi ne
Triprolidine Phenyltoxami
ne
Cetirizine Bilastine
First-Generation H1 antihistamines Second-Generation H1 antihistamines
Usually administered in three to four daily
doses
Usually administered once or twice a day
Cross the blood-brain barrier (lipophilicity ,
low molecular weight, lack of recognition
by the P-glycoprotein efflux pump)
Do not cross the blood-brain barrier
(lipophilicity , high molecular weight,
recognition by the P-glycoprotein efflux
pump)
Potentially cause side-effects
(sedation/insomnia/hyperactivity/convulsio
ns)
Do not cause relevant side-effects
(sedation/fatigue/hyperactivity/convulsio
ns)
Case reports of toxicity are regularly
published
No reports of serious toxicity
No randomized, double-blind,
placebo-controlled trails in children
Some randomized, double-blind,
placebo-controlled trails in children
Lethal dose identified for infants/young
children
Do not cause fatality in overdose
Therapeutic uses of antihistamines
H1 antagonists play an important role in the symptomatic treatment of various
immediate hypersensitivity reactions.
H1 antagonists are most useful in acute allergic reactions with symptoms of rhinitis,
urticaria and conjunctivitis. These drugs are treated for seasonal allergic rhinitis and
conjunctivitis. They relieve the symptoms of sneezing, rhinorrhoea and itching of nose
and throat. These drugs are used for acute phase of symptoms. They are not effective of
chronic phase of symptoms.
Adverse effects
The most important adverse effect is sedation. The next important side effect is loss of
appetite, nausea, vomiting, epigastric pain, constipation and diarrhoea. Owing to the
antimuscarinic actions there are effects like dryness of throat, mouth and respiratory
passages.
Antihistamines used in Allergic rhinitis
Cetrizine
It is a second generation piperazine. It has minimal anticholinergic
effects. It has also negligible penetration into the brain but is associated with a higher
incidence of drowsiness. The active enantiomer levocetrizine is more potent and less
drowsy when compared to that of the first genetation drugs.
Fexofenidine
This drug is a second generation piperadine. They are highly selective H1 receptors.
They lack significant anti cholinergic actions and penetrate poorly into the CNS.
Studies showing the efficacy of antihistamines in allergic rhinitis
study, for 2 weeks, in patients with seasonal allergic rhinitis. The first week of the study
was an open label period where all the patients received fexofenadine 60 mg twice daily.
A small number (25-33%) of patients had persistent symptoms. These patients(334)
were divided into 3 categories. The first group received only azelastine nasal spray, the
second group received azelastine with fexofenidineandthe third group received placebo
nasal spray each for 1 week of duration. The authors concluded that those patients who
were administered azelastine nasal spray as monotherapy as well as those given
fexofenidine and azelastine nasal spray together responded well for seasonal allergic
rhinitis and showed no difference in their response.(41)Those patients that received
placebo nasal spray showed
Berkowitz etalanalysed the results of two studies . These studies were double blinded
randomized controlled studies which compared the effect of fexofenifine and
pseudoephedrine with a placebo in seasonal allergic rhinitis. These studies recorded
allergic rhinitis symptoms for 2 hours after dosing and 30 minute interval for 4 hours.
The primary end point was the onset of action which was measured in the symptom
score. The secondary end point was to include the absolute and total change in the
percent score of the symptoms. A total of 1693 patients were screened in which 786
were randomized. The authors concluded that the patients with fexofenidine had onset
of action at 45 minutes and the effect lasted for a total duration of 6 hours.
(42)Guilemanyetal studied the impact on smell in allergic rhinitis and reversal of the
same after the use of antihistamines. The study group included 27 patients who had
symptoms, endoscopy, skin prick test, acoustic rhinometry, peak nasal inspiratory flow,
nasal nitric oxide and olfactory test (Barcelona smell test) were performed in all patients
with persistent allergic rhinitis at baseline and after 7 days and 30 days of treatment with
levocetrizine 5mg or placebo. The study population was randomized into 2 groups, with
14 receiving levocetrizine and 13 receiving placebo.
The symptoms score after 7 and 30 days were noted. Significant improvement in loss of
smell was observed after 7 days of levocetrizine treatment. This study
concludedthatlevocetrizine was effective against symptoms of persistent allergic
rhinitis and also caused an improvement in the loss of smell. The improvement in
olfaction was believed to be secondary to reduction in nasal inflammation rather than
nasal patency(43).
INTRANASAL STEROIDS
Effect of steroids on inflammatory response Molecular level
The action of the glucocorticoids(GC) begins at the molecular
level when the glucocorticoid crosses the cell membrane and binds to the GC receptor.
These receptors are present in the in the cytoplasm of the cell and are in an inactive form
maintained by heat shock proteins. GC disrupts the heat shock proteins which enables
the diffusion of GC into the nucleus of the cell. GC exerts its anti inflammatory
response using two pathways. The first pathway is transactivation where in the
receptor molecule which binds the GC encodes the anti inflammatory gene. The second
inflammatory response of the cell(44).
Cellular level
GC inhibits the function of the infiltrating inflammatory cells into the nasal mucosa.
GC also inhibits the cytokines and maturation of the mast cells. It inhibits the histamine
release from basophils , enhances the apoptosis of eosinophils and reduces the
recruitment of antigen presenting cells likethe Langerhans cells and dendritic cells. It
also reduces the numbers of Th2 cells. It has also an anti inflammatory effect on nasal
mucosal constituent cells such as epithelial cells, vascular endothelial cells and
fibroblasts(45).
Doses
Intranasal steroids are better than any other drugs in the management of nasal block,
congestion and rhinorrhoea. They exhibit their anti inflammatory effect by inhibiting
production and release of cytokines. They decrease the vascular permeability and down
regulate the secretion of the mucous glands. Their onset of action is slow and the
maximum efficacy develops over weeks and days. In extreme congestion, nasal steroid
will not reach the mucosa and hence a decongestant is used initially and the steroid is
used after that(46). Topical steroids can be used regularly and the usage can be
commenced before the onset of pollen season.
Fluticasone propionate, beclomethasone, mometasone and budesonide are the most
commonly used nasal steroidal sprays used. Fluticasone propionate contains 50 mcg
per spray and the maximum dosage that can be given is 200mcg. Fluticasone furoate
contains 27.5 mcg per spray and the maximum dosage to be given is 110mcg per day.
Beclomethasone contains 42 mcg per spray and a total dose of 168 mcg per day can be
given. Mometasone contains 100mcg per spray and a maximum of 400mcg can be
given per day. Nasal sprays are administered into each nostril at regular intervals as
once daily or twice daily doses.
Side effects
Intra nasal steroids can cause drying of the nose, crusting and resultant epistaxis.
Fluticasone causes a decrease in the endogenous secretion of cortisol but there is no
effect on adrenal suppression. Few studies show that there is a minimal decrease in the
skeletal growth. Sivametal performed a randomized double blinded placebo controlled
parallel clinical trial in 17 patients who had symptoms of impaired olfaction. The
subjects received MometasoneFuroate or placebo for 2 weeks. Nasal peak inspiratory
treatment. Nasal cytology samples were obtained from each visit and the biopsy
specimen of the olfactory epithelium was obtained at the end of the study and was
scored for inflammation. The results of this study showed that the patients on
Mometasonefuroate had improved quality of life, olfaction, nasal symptoms and
inflammation. Histological analysis of the olfactory epithelium showed that there were
fewer eosinophils in patients who received Mometasonefuroate(29). Julliossonsetal
performed a double blinded placebo controlled study of 25 patients with allergic rhinitis
who were administered a 4 week treatment of topical fluticasone. The authors also
studied the relationship between the tissue density of mast cells, tissue histamine levels
and levels of markers of mast cell activation after an allergen challenge of the nasal
mucosa in these patients following therapy with fluticasone. . Nasal biopsies were
obtained before and after treatment. Mast cell density, tryptase levels and tissue
histamine levels were evaluated. At 2 weeks intervals nasal challenges were performed
for 8 weeks. The symptoms of nasal allergy were assessed after each challenge.
Treatment with fluticasone propionate did not influence mast cell density or tissue
histamine concentration. However, there was a reduction in nasal symptoms and
tryptase in nasal lavage. This study showed that measurement of tryptase is an indicator
of both mast cell activation and efficacy of topical steroid treatment(47).
LEUKOTRIENE ANTAGONISTS
Leukotriene antagonists act by inhibitingcysteinyl leukotrienes which are the
important mediators of allergic rhinitis. There are two drugs which come under this
cysteinyl leukotriene receptors(48).
Mechanism of action
Cysteinyl leukotrienes (C4,D4 andE4)cause increased microvascular permeability,
inflammatory cell chemotaxis, mucus secretion and neuronal stimulation and
bronchoconstriction. Compared to histamine, leukotrienes C4 and D4 are 1000 times
more potent as bronchoconstrictors. These drugs are used often singly or in
combination with antihistamines in the therapy of allergic rhinitis.
These drugs are well absorbed orally, highly plasma protein bound and metabolized by
hepatic enzymes like CYP 2C9. The plasma half life of monteleukast is 3-6 hours(49).
Side effects
These drugs have few side effects, like headache and rashes.
Mast cell stabilisers Sodium cromoglycate
This is a synthetic chromone derivative and inhibits the degranuation of the mast
cell. Release of mediators from mast cell is prevented(50).. Long term treatment
reduces the cellular inflammatory response. Sodium cromoglycate is not absorbed
orally. It is administered as an aerosol. It is not a nasal decongestant. But regular usage
as a prophylactic can produce symptomatic improvement in patients.
Effect of treatment of allergy on olfaction
The medical treatment of Allergic Rhinitis includes predominantly intranasal
corticosteroids , antihistamines and leukotriene antagonists. Corticosteroids have a
Allergic Rhinitis. At the local site they cause membrane stabilisation and alteration in
the release of mediators and inhibits the migration of cells. This mechanism is helpful in
the restoration of the olfactory functiom at the olfactory mucosa. The advantage of
using a steroid nasal spray is that high drug concentration is provided at the target
receptor site and there is a minimum risk of side effects. Wober etal assessed the effect
of azelastine in 211 children less than 13 years of age. These childern were treated with
Azelastine nasal spary for 2 weeks. There was a significant reduction in the symptoms
of these children who were treated with sprays. The olfaction has significantly
improved from 72.1% to 94.6%(51). Gamberdella etal has compared in a randomized
control study the effect of loratidine tablet with azelastine nasal spray. They have not
found a statistically significant difference in the olfactory function of the patients in
both the groups. Meltzer etal assessed the eefcet of treatment with mometasone on 41
individuals for 2 weeks. Olfactory fucnction was assessed with CCCRC test pre and
post treatment. They have found that there was a significant increase in the odour
threshold for the patients when treated with mometasone when compared to that with
placebo(52). In a recent trial of Higaki etal in 2012, have studied the effect of 12
weeks of mometasone versus 4 weeks of placebo and 8 weeks of mometasone, and 12
weeks of placebo during the pollen season. Interstingly, they have found that there was
Study Design:
This is an observational prospective study
Study Population:
All patients who report to the ENT OPD who fit into the ARIA criteria of allergic
rhinitis.
Inclusion Criteria:
• All patients diagnosed with allergic rhinitis
• Patients aged 18 years or greater
• Patients should not have used steroidal nasal sprays at least 2 weeks prior to the
first test
• Patients without degenerative disease, neurological conditions or malignancy or
recent nasal surgery
Exclusion Criteria
• Patients below the age of 18 years
• Patients who has obvious nasal pathology like sinonasal polyps, Gross deviated
nasal septum which is touching the lateral wall of the nose and malignancy
• Patient