A Dissertation on
"A COMPARATIVE STUDY OF BACTERIAL
VAGINOSIS AMONG VITAMIN
–
D DEFICIENT
PREGNANT WOMEN AND NORMAL PREGNANT
WOMEN"
Dissertation Submitted to
THE TAMIL NADU Dr.M.G.R. MEDICAL UNIVERSITY CHENNAI- 600032
with partial fulfillment of the regulations for the award of the degree of
M.S.OBSTETRICS AND GYNAECOLOGY
COIMBATORE MEDICAL COLLEGE, COIMBATORE
CERTIFICATE
Certified that this is the Bonafide Dissertation in "A COMPARATIVE STUDY OF BACTERIAL VAGINOSIS AMONG
VITAMIN –D DEFICIENT PREGNANT WOMEN AND NORMAL
PREGNANT WOMEN" was a work done by Dr.SARANYAA.T and
submitted in partial fulfillment of the requirements for the Degree of
M.S. OBSTETRICS AND GYNAECOLOGY, of The Tamilnadu
Dr.M.G.R Medical University, Chennai.
Date: Professor and Unit Chief
Department of Obstetrics and Gynaecology Coimbatore Medical College.
Date: Professor and HOD
Department of Obstetrics and Gynaecology Coimbatore Medical College.
Date: The DEAN
DECLARATION
I Solemnly declare that the Dissertation titled "A COMPARATIVE STUDY OF BACTERIAL VAGINOSIS AMONG
VITAMIN –D DEFICIENT PREGNANT WOMEN AND NORMAL
PREGNANT WOMEN" was done by me at Coimbatore Medical
College during the academic year Oct 2016 – Sep 2017 under the guidance of Prof. Dr.R.Manonmani M.D., DGO., this Dissertation is submitted to the Tamilnadu Dr.M.G.R Medical University towards the fulfillment of the requirement for the award of M.S. Degree in
Obstetrics and Gynaecology.
PLACE: Dr. SARANYAA.T
ACKNOWLEDGEMENT
I express my gratitude to Dr.B.Asokan, M.S, MCh, the Dean, Coimbatore Medical College Hospital for providing facilities to carry out my project work successfully.
I sincerely thank Prof. Dr.R.Manonmani M.D.,DGO., Chief and HOD, Department of Obstetrics and Gynaecology for her constant guidance and encouragement throughout the period of my study.
I wish to express my thanks to DR.D.Vatsaladevi M.D.D.G.O., DR.Murugalakshmi M.D.D.G.O., Dr.Premakumari M.D.D.G.O., DR.N.Geetha MD.,OG Professors, Department of Obstetrics and Gynaecology, Coimbatore Medical College Hospital, Coimbatore whose knowledge and experience has guided and inculcated in me a sense of confidence.
I also extend my thanks to all my Assistant professors who have constantly motivated me with their words of support and encouragement and entire postgraduate colleagues for their help and support. Last but not the least, I would like to thank all my patients without whose co operation this dissertation would never have been the light of the day.
CERTIFICATE – II
This is to certify that this dissertation work titled "A COMPARATIVE STUDY OF BACTERIAL VAGINOSIS AMONG
VITAMIN –D DEFICIENT PREGNANT WOMEN AND NORMAL
PREGNANT WOMEN" of the candidate DR.SARANYAA.T with
registration Number 221616302 for the award of M.S in the branch of
OBSTETRICS AND GYNAECOLOGY, I personally verified the
urkund.com website for the purpose of plagiarism Check. I found that the uploaded thesis from introduction to conclusion shows the result of 1%
(One) percentage of plagiarism in the dissertation.
INDEX
SR.NO CONTENT PAGE NO.
I INTRODUCTION 1
II AIMS AND OBJECTIVES 3
III REVIEW OF LITERATURE 4-64
IV MATERIALS AND
METHODS
65-67
V OBSERVATIONS AND
RESULTS
68-87
VI DISCUSSION 88-94
VII SUMMARY 95-96
VIII CONCLUSION 97
IX
LIST OF TABLES
SR.NO CONTENT PAGE NO.
I NUGENTS CRITERIA 28
2. VITAMIN D LEVELS 57
3. RDA OF VITAMIN D 60
4. MAX TOLERABLE DOSE OF
VITAMIN D
61
5. AGE DISTRIBUTION 68
6. GESTATIONAL AGE 69
7. PARITY 70
8. BMI 72
9. SIGNS AND SYMPTOMS OF BV 74
10. GRAM STAIN 75
11. GRAM STAIN AND BV 76
12. VITAMIN D STATUS 78
13. VITAMIN D STATUS AND BV 79
14. MATERNAL OUTCOMES 82
15. FETAL OUTCOMES 84
LIST OF FIGURES
SR.NO CONTENT PAGE NO.
1. BV HPE SLIDE 10
2. BV PICTURE 18
3. GRAM STAIN PICTURE 26
4. WET MOUNT PICTURE OF BV 28
5. HAYS CRITERIA 30
6. BV OTHER METHODS 31
7. BV CULTURE 32
8. VITAMIN D CHEMICAL STRUCTURE 41
9. VITAMIN D METABOLISM 1 43
10. VITAMIN D METABOLISM 2 48
11. VDR RECEPTOR 50
12. FUNCTION OF VITAMIN D 51
13.
REPRODUCTIVE FUNCTION OF VITAMIN D
52
14.
AGE DISTRIBUTION 68
15.
BMI 72
16.
17.
GRAM STAIN 75
18.
GRAM STAIN AND BV 77
19.
VITAMIN D STATUS 78
20.
VITAMIN D STATUS AND BV 80
21.
MATERNAL OUTCOMES 83
22.
FETAL OUTCOMES 84
23.
ABBREVIATONS
BV - Bacterial Vaginosis
Vit D - Vitamin -D
AN - Antenatal
PN - Postnatal
PP - Post Partum
BMI - Body Mass Index
GDM - Gestational Diabetes Mellitus
PIH - Pregnancy Induced Hypertension
PPROM - Preterm Premature Rupture of Membranes
PROM - Premature Rupture of Membranes
GA - Gestational Age
OCP - Oral Contraceptive pills
RTI - Reproductive tract infection
IUCD - Intra Uterine Contraceptive device
KOH - Potassium Hydroxide
HPE - Histopathological Examination
POC - Products of Conception
USG - Ultrasonogram
UVB - Ultraviolet Rays B
INTRODUCTION
This study emphasis on the prevalence of Bacterial Vaginosis among pregnant women and its association with Vitamin –D deficiency. It also emphasis their impact on maternal and fetal health.
Bacterial Vaginosis a poly-microbial over growth of predominantly anaerobic bacteria such as GardnellaVaginalis, Mycoplasma hominis, Mobiluncus, Bacteroides, Peptostreptococcus over Normal vaginal flora of Lacto bacilli1,2. This commonly affects the women of reproductive age group and also it is the most common infection among pregnant women1,19.
Bacterial Vaginosis is associated with adverse pregnancy outcomes such as Preterm labour, PPROM, Spontaneous abortion, Recurrent pregnancy loss, Chorioamnonitis, Postpartum Endometritis, Post operative wound infections19,20,21.
Bacterial Vaginosis is a sexually associated disease and also increases the prevalence of other sexually transmitted diseases43.
BV is associated with Vitamin – D deficiency hence better evaluation of this condition will prevent adverse fetal and maternal outcomes.
Vitamin –D is a fat soluble seco-steroid which plays an important role in Calcium and phosphate homeostasis, apart from this it has other non classical benefits like Immuno modulation, infection controll6,8,53etc.,
AIM OF THE STUDY
To identify the association between Bacterial Vaginosis and Vitamin –D deficiency among pregnant mothers.
OBJECTIVES:
1. To estimate the prevalence of Bacterial Vaginosis and Vitamin D deficiency among pregnant population
REVIEW OF LITERATURE
Anne L Dunlop et al investigated the association between serum 25 hydroxy vitamin D, folate, Omega 6 / Omega 3 ratio and bacterial vaginosis during pregnancy3. She reported that a strong association between vitamin D less than 12 ng/ml and folate deficiency less than 5 ng/ml with Bacterial Vaginosis (Nugent’s score more than or equal to 7) during pregnancy
Bodnar et al reported that maternal Vitamin D deficiency is associated with bacterial vaginosis in first trimester of pregnancy. In this cohort study he found a dose response association between 25 hydroxy vitamin D deficiency and prevalence of Bacterial Vaginosis and also the likelihood of Bacterial vaginosis decreases as vitamin D status improves4. There is a strong racial disparity among the prevalence of Bacterial vaginosis
HenselK.J et al found an association between Vitamin D deficiency and bacterial vaginosis. He also states that Vitamin D deficiency was a modifiable risk factor for bacterial vaginosis among pregnant women6. Hence evaluation of Vitamin D supplementation for prevention of bacterial vaginosis in pregnancy and also use of vitamin D supplementation as adjunct therapy for bacterial vaginosis in pregnancy is warranted.
Turner et al also reported an association between increased prevalence of bacterial vaginosis among vitamin D deficient women7. Treatment of vitamin D deficiency in pregnant women reduced the recurrence of bacterial vaginosis, but it doesn’t reduce the recurrence of
bacterial vaginosis in non pregnant women.
Joonjslk shin et al studied the importance of non classical role of vitamin D in pregnancy and in placenta. Placenta produces a response to vitamin D which functions as a modulator of implantation, cytokine production and immune response to infection8. Hence vitamin D deficiency in pregnancy is associated with bacterial infections like Bacterial Vaginosis, Pre eclampsia ,GDM etc.,
modulating immune response to invading infectious agents in the reproductive tract. This raises the possibility that vitamin D sufficiency may upregulate hcap18/LL-37 expression in the reproductive tract thereby affecting the susceptibility to Bacterial Vaginosis.
Dixon et al also identified a positive correlation between circulating hcap18/LL-37 (anti – microbial peptide gene) and serum 25 hydroxy vitamin D10, thereby depicting the role of Vitamin –D in immuno modulatory function.
Bhan et al also observed similar finding. He administrated high dose of vitamin D2 (ergocalciferol) and observed the changes in human cathelicidin (hcap18/LL-37) values, thereby suggesting positive correlation between bacterial infections and vitamin D deficiency11,12.
Adrian F Gombart also discovered that Vitamin D induces cathelicidin antimicrobial peptide gene expression thereby regulating immune function and response against bacterial and viral infection13.
Kearns et al also reported positive correlation between Vitamin D deficiency and infectious diseases14.
catalyses local synthesis of calcitriol. This study recommends vitamin D supplementation during pregnancy is accessible and is a safe way to reduce adverse pregnancy outcome like preterm labor, PROM due to infection, Preeclampsia, GDM etc.,
Urrutia and Throp stated that vitamin D deficiency is related to many adverse pregnancy events like bacterial vaginosis, preterm labour, PROM, preeclampsia, GDM16etc.
Wagner, Taylor, Johnson and Hollis studied the role of vitamin D in pregnancy and lactation17. The study states that Vitamin D maintains calcium and bone metabolism in both mother and foetus, Immuno modulation in mother and also impact of maternal vitamin D deficiency on foetal health.
Abilasha Gupta et al stated that bacterial vaginosis in pregnancy has been associated with preterm labour, PROM, chorioamnionitis, spontaneous abortion, recurrent abortion, PP Endometritis18. They also suggested screening of bacterial vaginosis should start early in pregnancy in women, who are at high risk of preterm labour.
Chitra Jayakrishnan et al studied in detail about the occurrence of bacterial vaginosis and fetal outcomes19, this study found a positive correlation between bacterial vaginosis and preterm labour.
Kiss et al (2004) states that presence of Bacterial Vaginosis at 26-32 weeks of gestation has been shown to associated with preterm labour20.
Flynn et al (1999) also shown that BV increases the risk of preterm labour21.
One study also found that risk appears double when detected early in pregnancy. (21%) when compared to later pregnancy (11 %) –Joesoef et al 1993 :Leitich et al 2003 )
Carey et al used oral Metronidazole to treat BV in pregnancy but did not find any reduction in incidence of bacterial Vaginosis22.
Okun et al women who treated with antibiotic for Bacterial Vaginosis found to have reduction in persistent and recurrent infections23.
Main risk factor for PPROM is infection (Gomez et al 1997 : Mercer et al 2003)24.
THEORETICAL BACKGROUND :
Bacterial Vaginosis
Bacterial vaginosis also known as non specific vaginitis / anaerobic vaginositis/ vaginal bacteriosis/ gardnerella vaginitis.
Bacterial vaginosis is termed as vaginosis rather than vaginitis because it is associated with alteration in normal vaginal flora rather than due to any specific infections1,2. It is a polymicrobial infection in which normal hydrogen peroxide producing lactobacillus is replaced by anaerobes thereby altering the vaginal microbiota.
VAGINAL SECRETIONS
Normal vaginal secretion composed of vulvar secretion from sebaceous gland, sweat gland, bartholins glands, Skene glands, transudate from vaginal wall, exfoliated cells from vagina and cervix, cervical mucus, endometrium, oviductal fluids, microorganisms and their metabolic products.
The vaginal desquamated tissue is made up of vaginal epithelial cells that are responsive to hormones like Oestrogen and Progesterone. The vaginal epithelial composition varies with age and also by hormonal changes.
Superficial cells are the main type of cells in reproductive age group. These cells are the predominant cell type when there is excess oestrogen stimulation (as in proliferative phase of menstrual cycle). Intermediate cells predominance during luteal phase of menstrual cycle which is under the control of progesterone. Parabasal cells predominates in post menopausal lady where there is low level of both oestrogen and progesterone.
producing lactobacilli. This protects against vaginal infection by following ways:
1. Superficial cells under the influence of oestrogen laded with glycogen. The vaginal epithelial cells breakdown glycogen to monosaccharides which can then be converted by lactobacilli to lactic acid. This lactic acid production lowers the pH of vagina to less than 4.5 (acidic pH)
2. The lactobacilli has unique ability to produce hydrogen peroxide thereby preventing the growth of other anaerobes.
ORGANISM NORMALLY OCCURING IN VAGINA1,2
Lactobaacillus
S.Epidermidis
S.Aureus
GBS
E.coli
Klebseilla
Proteus
Propionibacterium Prevotella
Bacteriods.
PHYSIOLOGICAL CAUSES OF LEUCORRHOEA
During puberty
During menstrual cycles - under the influence of hormones
During intercourse
PATHOLOGICAL CAUSE OF LEUCORRHOEA
Non infective causes like
Polyp, Ectopy, OCP use, Pelvic organ prolapse etc.
Infective causes like
PID, Cervicitis, Vaginitis.
DEFENSE MECHANISM PREVENTING INFECTION
VULVAL DEFENSE
VAGINAL DEFENSE
Apposition of vaginal walls
Stratified squamous epithelium
Lactic acid producing DODERLEIN‘S bacilli which reduces the vaginal PH in acidic range and prevents infection and inhibits the growth of other organism
Bacteriocins–acidocins and lactacin.
CERVICAL DEFENSE
Mucus plug.
Racemose type of glands.
Squamous epithelial lining of ectocervix.
UTERINE DEFENSE
Closure of ostia which prevents any ascending infection to fallopian tubes.
Cyclical shedding of endometrium.
INFECTIONS OF REPRODUCTIVE TRACT
Divided into
1. Infection of lower genital tract
2. Infection of upper genital tract
INFECTION OF LOWER GENITAL TRACT
Lower genital tract infection includes infection of vulva, vagina and cervix, they are also referred to as RTI (reproductive tract infections). some of the infections such as Trichomoniasis, Chlamydial infection, HPV and Gonococcal infection, Syphilis, Chancroid, LGV, Granuloma inguinale are sexually transmitted infections. Others such as Bacterial Vaginosis are sexually associated diseases1,2,19.
PREVALENCE1,2,19,21
Prevalence of lower genital tract infection in INDIA
Based on
History alone -11-72 %
Clinical examination–17-40%
CHARACTERISTICS OF NORMAL VAGINAL FLORA ;
White and odourless
Components are
Secretions from vulval glands
Transudate from vaginal wall
Cervical glands secretion
Endometrial and tubal fluids
Normal flora
Aerobic bacteria
Lactobacilli
Streptococcus and staphylococcus
Gardenellavaginalis
Anaerobic bacteria
Normal PH
3.8–4.5
Microscopy
Desquamated epithelial cells
White blood cells
Lactobacilli
CONDITIONS CAUSING VAGINAL DISCHARGE
Bacterial Vaginosis
Trichomonal vaginitis
Candidal vaginitis
BACTERIAL VAGINOSIS :
disequilibrium increases the pH of the vaginal secretion and also decrease in the release of hydrogen peroxide favouring the growth of anaerobes.
Gardnerella form a biofilm which prevents the action of antibiotics which inturn favours the growth of anaerobes, hence infection is polymicrobial and also recurrence is more common
CLINICAL SYMPTOMS :
Bacterial vaginosis is a most common infection of reproductive age group. This is the most common infection affecting pregnant women.
The Prevalence of Bacterial Vaginosis is between 10 to 35
percent21, depending upon region and race
PREDISPOSING FACTORS :
Poor personal hygiene
Injudicious use of antibiotics
IUCD
Frequent vaginal douching
Cigarette smoking
Increased vaginal pH as after menstruation
Black ethnic group
Lesbians
SIGNS AND SYMPTOMS :
50 percent of women with Bacterial Vaginosis are asymptomatic , while others have
Discharge per vaginum which is white, thin, homogenous discharge
Typical unpleasant fishy vaginal odour
There may be associated pruritis usually non pruritic
Lower abdominal pain
Postcoital increase in discharge and dyspareunia
DIAGNOSIS
Bacterial vaginosis is diagnosed by taking a thorough history, detailed clinical examination and investigations
History
History taking should include the following
Age
Parity
Demographic details
Socioeconomic status
Chief complaints
Presenting illness such as description of vaginal discharge in terms of onset, duration, precipitating factors, colour, consistency, amount, odour, associated pruritis, dysuria, dyspareunia, lower abdominal pain and constitutional symptoms.
Menstrual history
Obstetric history
Marital history–number of sexual partner ,recent change in sexual partner, disease in sexual partner.
Contraceptive history
Any medication history
Past medical /surgical history
Previous similar complaints and antibiotic treatment
Personal history.
Occupational history
CLINICAL EXAMINATION :
General examination
BMI
Systemic examination
Abdominal examination
speculum examination
bimanual examination
Abdominal examination
Look for areas of tenderness
Organomegaly
Presence of mass
Free fluid
Scars, sinuses, engorged veins ,hernia orifices.
Systemic examination
Other systems CVS, RS, CNS examined
Examination of pelvis
Done in dorsal lithotomy position after emptying the bladder with proper lighting after getting consent.
Examination of external genitalia
Vulva , hair distribution ,any skin lesion, introitus, uretheral meatus ,any vaginal discharge
Speculum examination
Using self retaining cuscos speculum with proper lighting
1. Vaginal discharge–colour, consistency ,amount , odour.
2. Bleeding per vaginum
3. Any other lesions, growth in cervix and vagina.
Bimanual examination or abdomino pelvic examination
1. Uterus–position (anteverted or retroverted )
2. Size
3. Shape
4. Consistency
5. Mobility
6. Tenderness
7. Adenexal fullness and tenderness
PROCEDURE :
Along with examination the following procedures done after getting informed written consent.
Cytological screening for cancer cervix –Pap smear
Examination of vaginal discharge
Two High vaginal swab taken from the posterior fornix using sterile cotton tipped swab. One is spread on a slide and fixed and sent to microbiological lab for gram staining. Other KOH is added and look for fishy odour and microscopic examination done.
INVESTIGATIONS :
Investigations include
1. complete blood count including Total count, differential count,
2. Erythrocyte sedimentation rate
3. Pap smear
4. Vaginal smear
DIAGNOSTIC CRITERIA FOR BV.
AMSEL’SCRITERIA :
This criteria is proposed by Amsel in 1984 to establish the diagnosis of bacterial vaginosis
Vaginal discharge –thin, homogenous white or greycolour
WHIFF TEST : Addition of KOH results in fishy odour
Vaginal pH more than 4.5
Presence of clue cells on wet mount microscopy examination
Any 3 out of these 4 is required to establish the diagnosis of bacterial vaginosis.
GRAM STAIN
Gram staining of the vaginal secretion was introduced by Nugent26 in the year 1991.
The technique of gram staining is described in brief
Gram stain
Gram negative bacteria stain red, which is attributed to a thinner
peptidoglycan wall, which does not retain the crystal violet during the
decolouring process.
PROCEDURE :
The process involves the following steps:
2. A decolorizer such as ethyl alcohol or acetone is added to the sample, which dehydrates the peptidoglycan layer, shrinking and tightening it. The large crystal violet-iodine complex is not able to penetrate this tightened peptidoglycan layer, and is thus trapped in the cell in Gram positive bacteria. Conversely, the the outer membrane of Gram negative bacteria is degraded and the thinner peptidoglycan layer of Gram negative cells is unable to retain the crystal violet-iodine complex and the color is lost.
3. A counterstain, such as the weakly water soluble safranin, is added to the sample, staining it red. Since the safranin is lighter than crystal violet, it does not disrupt the purple coloration in Gram positive cells. However, the decolorized Gram negative cells are stained red.
NUGENT’S CRITERIA
The below table represents nugents scoring system
LACTOBACILLUS
GARDNERLLA/
BACTEROIDES
MOBILUNCUS
QUANTITY SCORE QUANTITY SCORE QUANTITY SCORE
4+ 0 0 0 0 0
3+ 1 1+ 1 1+ or 2+ 1
2+ 2 2+ 2 3+ or 4+ 2
1+ 3 3+ 3
A score of more than or equal to 7 indicates bacterial vaginosis
A score of 4-6 indicates intermediate stage of bacterial vaginosis
A score of less than 4 indicates no bacterial vaginosis
ADVANTAGES :
Nugent screening offer advantage over Amsel criteria by Better reliability
Reproducibility
Better sensitivity and specificity
It is the gold standard method in diagnosing Bacterial Vaginosis,
HAY’S CRITERIA :
This criteria was devised by Hay in the year 2002
GRADE 0 : Epithelial cells with no bacteria
GRADE 1 : Normal bacterial vaginal flora (Lactobacilli morphotypes predominant)
GRADE 2 : Reduced numbers of lactobacillus morphotypes with mixed bacterial flora
GRADE 3 : Mixed bacterial flora only, few or absent lactobacillus morphotypes
OTHER METHODS :
Several newers methods are introduced the following are some of them,
CULTURE :
Bacterial vaginosis grows on blood and chocolate agar. It forms hemolytic colonies on human and rabbit blood agar. It is catalase negative and oxidase negative
TREATMENT
Treatment will be recommended for non pregnant women with signs and symptoms of BV27,28. In pregnant mothers treatment will be recommended in all mothers who are positive for BV, some of the recommended regimens are as follows.
Tab .Metronidazole 500 mg orally twice daily for 7 days
0.75 % metronidazole gel intravaginally once a day for a period of 5 days
Tab. Clindamycin 3 mg twice daily orally for a period of 7 days
Alcohol consumption should be avoided during treatment.
Alternative treatments includes (not approved to use in pregnant
mothers)
Tab. Tinidazole 2 gram orally once daily for 2 days Tab. Tinidazole one gram oral for 5 days
Newer studies for using intravaginal probiotics or lactobacilli is under study follow up after treatment is necessary because persistent or recurrence of disease is common30. Re-treatment with same regimen for recurrence is recommended.
Treatment is recommended for all symptomatic and also asymptomatic pregnant women27,28. Two studies demonstrating the efficiency of oral Metronidazole twice daily for a period of 5 days the study concluded 70% cure rates by using Nugent’s criteria to define cure. Another study demonstrates 80% cure rates by using clindamycin regimen.
and topical therapy hence symptomatic pregnant women can be treated with either vaginal or oral Metronidazole. Many adverse pregnancy outcomes such as preterm labour, PPROM, Spontaneous Abortions, postoperative infections are related to Bacterial Vaginosis. Meta analysis concluded antibiotic treatment does not prevent preterm labour. However in one study oral therapy reduces the late miscarriages and other study pointed out decrease in fetal morbidity such as low birth weight, IUGR etc.
Carey et al used oral metronidazole to treat BV in pregnancy but did not find any reduction in incidence of Bacterial Vaginosis22.
Okun et al states that women who treated with antibiotic for Bacterial Vaginosis found to have reduction in persistent and recurrent infections23.
MATERNAL AND FETAL COMPLICATIONS ASSOCIATED
WITH BACTERIAL VAGINOSIS18,19,20
Some of the maternal complication occurring due to bacterial vaginosis are
Spontaneous abortion
Recurrent pregnancy loss
Preterm labour
PPROM
Chorioamnionitis
Low Birth weight
PP Endometritis
Wound infection
ABORTION
RECURRENT PREGNANCY LOSSES (RPL)
Couples with 3 or more clinically recognized pregnancy losses < 20 weeks18,19 ectopic and molar pregnancies not included
ASRM defines RPL as “ a distinct disorder defined by 2 or more
failed clinical pregnancies”.
Clinical pregnancies–USG proven or by HPE of POC
Incidence 1-2%.
PRETERM LABOUR
Labour before 37 completed weeks, it is defined as presence of uterine contraction of sufficient strength, also in frequency causing progressive effacement and dilatation of the cervix between 20 to 37 weeks of gestation18,19.
Incidence around 10%
Kiss et al (2004) states that presence of Bacterial Vaginosis at 26-32 weeks of gestation has been shown to associated with preterm labour20.
Flynn et al (1999) also shown that BV increases the risk of preterm labour21.
One study also found that risk appears double when detected early in pregnancy.(21%)when compared to later pregnancy (11 %) – Joesoef et al 1993 :Leitich et al 2003 )
Carey et al used oral metronidazole to treat BV in pregnancy but did not find any reduction in incidence of Bacterial Vaginosis22.
Okun et al states that women who treated with antibiotic for Bacterial Vaginosis found to have reduction in persistent and recurrent infections24.
Studies are underway to analyse the benefits of screening and treating both high risk and low risk mothers, results are equivocal.
PPROM19,20
PPROM defined as occurrence of rupture of membranes prior to 37weeks and also before onset of labour.
Incidence around - 3 -18.5 % ( Gunn et al 1970 )
Main risk factor for PPROM is infection (Gomez et al 1997 : Mercer et al 2003)
Bacterial proteases decrease the strength and elasticity of fetal membranes thereby causing PPROM .
Infection with Gonococcal, Trichomonal, Chlamydial, or colonization with GBS and BV (Bacterial Vaginosis) have an increased risk of PPROM, (Edwards et al 1978 : Minkoff et al 1984).
PP ENDOMETRITIS
It is defined as the occurrence of temperature of 38 (100.4 F) on any two days of the first ten days postpartum after first 24 hours.
Main cause is PP Endometritis, organism causing endometritis are commensals of lower genital tract, Bacterial vaginosis etc.,
WOUND INFECTION :
VITAMIN - D
VITAMINS :
Vitamin may be regarded as organic compounds required in the diet in small amounts to perform specific biological functions for normal maintenance of optimum growth and health of organism. The usage of A B and C to vitamins was introduced in 1915 by McCollum and Davis.
CLASSIFICATION :
They first classified only two vitamins–
1. Fat soluble / Lipid soluble (A,D,E,K )
2. Water soluble
There are about 15 vitamins essential for humans.
Fat soluble vitamins absorption is associated with fats, can be stored in liver and adipose tissue. Excess consumption of these vitamins particularly A and D leads to their accumulation and toxic effects
VITAMIN - D
Vitamin D is a fat soluble vitamin. It resembles sterols in structure and functions like a hormone. Vitamin D is called as sunshine vitamin. The synthesis of Vitamin D3 in the skin is proportional to the exposure of sunlight. Dark skin pigment (melanin) adversely influences the synthesis of cholecalciferol.
Vitamin D was isolated by Angus (1931) who named it calciferol.
CHEMISTRY :
During the course of cholesterol synthesis 7 dehydrocholestrol is found as an intermediate. On exposure to sunlight, 7 dehydro cholesterol is converted to cholecalciferol in skin.
SOURCES :
1. Skin synthesize vitamin D when exposed to sun (UV B 290-315nm)
2. Fish liver oil
3. Fatty fish
4. Egg yolk
5. Fortified food –milk cheese
During the course of cholesterol synthesis 7 dehydrocholestrol is found as an intermediate. On exposure to sunlight, 7 dehydro cholesterol is converted to cholecalciferol in skin.
SOURCES :
1. Skin synthesize vitamin D when exposed to sun (UV B 290-315nm)
2. Fish liver oil
3. Fatty fish
4. Egg yolk
5. Fortified food –milk cheese
During the course of cholesterol synthesis 7 dehydrocholestrol is found as an intermediate. On exposure to sunlight, 7 dehydro cholesterol is converted to cholecalciferol in skin.
SOURCES :
1. Skin synthesize vitamin D when exposed to sun (UV B 290-315nm)
2. Fish liver oil
3. Fatty fish
4. Egg yolk
TYPES :
Vitamin D is expressed by
1 Cholecalciferol (Vitamin D3)
2 Ergocalciferol Vitamin D2 (from olant fungi yeast)
ABSORPTION TRANSPORT AND STORAGE :
Vitamin D is absorbed in the small intestine for which bile is essential. Though lymph, vitamin D enters the circulation bound to plasma alpha globulin and is distributed throughout the body. Liver and other tissues stores store small amounts of vitamin D.Vitamin D is incorporated into chylomicrons which convey the vitamins from lymph to systemic circulation. In lymph Vitamin D in chylomicron is transferred to DVP
METABOLISM :
SYNTHESIS OF VITAMIN D :
Vitamin D2 and D3 are not biologically active. They metabolise in body and converted to active form Vitamin D can be synthesized in body by exposure to sunlight32.
SYNTHESIS IN SKIN :
The UVB rays (290-315 nm) from sun exposure coverts 7 dehydro cholesterol to cholecalciferol (vitamin D3)32.
FACTORS AFFECTING VITAMIN D3 PRODUCTION :
1. Colour of the skin :
METABOLISM :
SYNTHESIS OF VITAMIN D :
Vitamin D2 and D3 are not biologically active. They metabolise in body and converted to active form Vitamin D can be synthesized in body by exposure to sunlight32.
SYNTHESIS IN SKIN :
The UVB rays (290-315 nm) from sun exposure coverts 7 dehydro cholesterol to cholecalciferol (vitamin D3)32.
FACTORS AFFECTING VITAMIN D3 PRODUCTION :
1. Colour of the skin :
METABOLISM :
SYNTHESIS OF VITAMIN D :
Vitamin D2 and D3 are not biologically active. They metabolise in body and converted to active form Vitamin D can be synthesized in body by exposure to sunlight32.
SYNTHESIS IN SKIN :
The UVB rays (290-315 nm) from sun exposure coverts 7 dehydro cholesterol to cholecalciferol (vitamin D3)32.
FACTORS AFFECTING VITAMIN D3 PRODUCTION :
White skin people produces more vitamin D than dark skin people because melanin protects skin against damage from UVB exposure. So darker skin with more melanin allow less UVB to enter the skin. Less UVB , less Vitamin D is produced.
2. Area of skin exposed
More the skin is exposed, more vitamin D is produced. 1000-20000 IU of vitamin D can be produced within minutes. Some cultural practices in India like wearing purdah reduces Vitamin–D synthesis.
3. Altitude :
People live in high altitude and people living near equator produces more Vitamin D
4. Time of the day :
Vitamin D production peaks during the middle of the day.
5. Ageing :
As the skin gets aged, the capacity to produce Vitamin D decreases.
6. Use of sunscreen :
SYNTHESIS IN LIVER :
The cholecalciferol synthesis from the skin transported to liver. In liver, it is hydroxylated at 25th position to 25 hydroxycholecalciferol (25 OH-D3) by a specific hydroxylase (25-hydroxylase). It is called as calcidiol, which has minimal biological activity. Hepatic 25 hydroxylase is a microsomal monooxygenase and it is a product of gene CYP27A1. This enzyme requires cytochrome P450 and NADPH.
25 hydroxy Cholecalciferol is the main storage form of vitamin D, so measurement of 25 hydroxy Cholecalciferol gives amount of Vitamin D in the body.
SYNTHESIS IN KIDNEY :
The 25 hydroxy Cholecalciferol is bound to vitamin D binding protein which is a alpha globulin (VDBP) in plasma. This is taken to kidney, where it is further hydroxylated at first carbon by 1 alpha hydroxylase to1, 25-dihydroxycholecalciferol. Since it contains 3 hydroxyl group, it is called as calcitriol.
The 1 alpha hydroxylase enzyme is located in mitochondria of proximal convoluted tubule and it is a product of gene CYP27B1. This requires cytochrome P450, NADPH and ferrodoxin.
The role of vitamin D is to maintain calcium and phosphate metabolism and also has many nonclassical benefits
FUNCTIONS OF VITAMIN D :
THE VITAMIN D functions are divided into
1. Classical/calcemic effect
2. Nonclassical / extra calcemic effect
CLASSICAL ROLE OF VITAMIN D:
Calcitriol (biologically active form) regulates plasma calcium and phosphate homeostasis46. Its effect is exerted at 3 different levels
1. ACTION OF CALCITRIOL ON INTESTINE :
D receptor (VDR) in nucleus. This inturn binds to VDRE which leads to gene activation by transcription, which codes for calbindin. Calbindin helps in calcium absorption.
2. ACTION OF CALCITRIOL ON BONES :
Calcitriol is essential for bone formation46. D3 stimulates the activity of osteoblast increases the bone mineral density and helps in bone remodeling. Calcitriol along with parathoromone increases the mobilization of calcium and phosphate from bone, thereby maintaining serum calcium and phosphate level
3. ACTION OF CALCITRIOL ON KIDNEY :
Vitamin D3 increases the absorption of calcium and phosphate from renal tubule. It also minimizes the excretion of calcium and phosphate.
REGULATION OF VITAMIN–D SECRETION :
When the calcitriol concentration is adequate, the 24 hydroxylase enzyme in kidney gets activated and vitamin D2 is converted to 24,25 – cholecalciferol, which is less active form of vitamin D thereby preventing vitamin D toxicity32.
NONCLASSICAL ROLES OF VITAMIN D :
1,25 dihydroxy Cholecalciferol receptors are found in almost all tissues of the body. Besides intestine and bone, the receptors are found in heart, brain, macrophages, prostate even in uterus42,44. This shows possibility of vitamin D deficiency in many diseases and also supplementation of vitamin D will help in treating many disorders in near future.
These actions of vitamin D explains the utility of Vitamin D in number of diseases. The endocrine, paracrine and intracrine functions of the vitamin D are under research.
Some of the functions are listed below :
IN KIDNEY
1. Calcium homeostasis
2. Muscle health
3. Bone health
5. Cardiovascular health
6. Neural development
7. Immunomodulation
IN MONOCYTES AND MACROPHAGES :
1. Immuno modulation
2. Control of invading pathogens
3. Prevention of autoimmune diseases
IN PROSTATE/ BREAST/ COLON/ LUNG16:
1. Inhibits cell proliferation
Hence vitamin D deficiency plays an important role in rickets, osteomalacia /osteoporosis and also more likely to play a role in diabetes mellitus, systemic hypertension, cardiovascular diseases, infections like tuberculosis, bacterial vaginosis16,44, etc.., and autoimmune diseases
ROLE OF VITAMIN D IN REPRODUCTIVE HEALTH :
Maternal Vitamin D deficiency is associated with increased risk of gestation diabetes mellitus, eclampsia, bacterial vaginosis and low birth weight infant. The risk of auto and cellular immune abnormalities is increased in women with RPL and vitamin D deficiency.
Vitamin D source of infants result from transfer from stores of mother. (ref . S karras, H fakhoury et al) Low maternal vitamin D levels during pregnancy is associated with many adverse neonatal outcomes like low birth weight, preterm births, detrimental effects on child’s bone and teeth development and risk of infectious diseases. This finding is demonstrated by identifying nuclear Vitamin D receptors and vitamin D activating 1 alpha hydroxylase in deciduas and placenta. This was stated by Evans et al.
HUMAN CATHELICIDIN AND ITS ASSOCIATION WITH
VITAMIN–D AND BACTERIAL VAGINOSIS5,9,10,12:
The Hcap/LL-37 is increased in the presence of bacterial Vaginosis as a protective mechanism against BV infection. Normalisation of the levels after antibiotics treatment for BV proves their association5.
CAMP expression is increased by exposure to Vitamin – D3 and CYP27B1 are expressed by END E6/E7 cell lines of cervix, this enzyme converts inactive form of Vitamin d to active form in autocrine manner, treatment with Vitamin D increases the expression of human cathelicidin Vitamin –D regulates the expression of cathelicidin thereby preventing BV5,9.
This hypotheis is further proven by Lorraine et al and also Dixon et al also identified a positive correlation between circulating hcap18/LL-37 (anti–microbial peptide gene) and serum 25 hydroxy vitamin D9,10.
Adrian F Gombart also discovered that Vitamin D induces cathelicidin antimicrobial peptide gene expression thereby regulating immune function and response against bacterial and viral infection13.
PHARMACOKINETICS :
converted to 25 hydroxy vitamin D and is excreted from the body. The elimination half life of vitamin D is 2 to 3 weeks and the concentration of vitamin D gradually increases and attains plateau around 40-90 days. In vitamin D sufficient persons, researchers proved supplementation of vitamin D will not increase the vitamin D levels in body. The most common circulating form of vitamin D is 25 hydroxyvitamin D. Its concentration is 1000 times more than 1,25 hydroxy vitamin D. 25 hydroxy vitamin D is converted to its active form, 1,25 dihydroxy vitamin D to perform its functions. 1,25dihydroxy vitamin D lasts in circulation for only 3 to 5 days.
ASSESMENT OF INDIVIDUALS VITAMIN D STATUS45,48,49 :
Accurate indicator of vitamin D status of person is by measuring the vitamin D levels.
Vitamin D status can be measured by measuring 25 hydroxy vitamin D levels or by measuring 1,25dihydroxy vitamin D levels. The most preferred analysis is measuring 25 hydroxy vitamin D levels48.
levels of 1,25dihydroxy vitamin D.So assessing 1,25 dihydroxy vitamin D levels may be inaccurate as it may be normal or increased mild to moderate in vitamin D deficiency49. It becomes low in only very severe vitamin D deficiency. 1,25hydroxy vitamin D levels may be inaccurate when there is associated hepatic disease or renal disease or primary hyperparathyroidism.
Hence estimation of 25 hydroxy vitamin D is the most accurate method of assessing an individual’s vitamin D status. Analysing serum
calcium, phosphate and ALP enzyme in a person to assess the vitamin D status of that person is also inaccurate. Among persons with vitamin D deficiency 25% can have normal levels of serum calcium and phosphate and ALP but PTH LEVELS will be elevated. Hence researchers are not in favour of measuring serum calcium and phosphate to assess vitamin D levels of a person.
VITAMIN D LEVELS
In accordance with Endocrinological Soceity
Optimum levels of 25 hydroxy vitamin D is more than 30 ng/ ml. When the levels ranging from 20-29 ng/ml is seen, it is called
When the vitamin D levels range less than 20 ng/ml it is called ‘’Vitamin D deficient’’
Less than 8 ng/ml it is severe deficiency .
Different councils recommends the following cut offs,some of them are listed below.
Researchers proved that level of more than 30 nanograms/ml of 25 hydroxy vitamin D is essential for the normal absorption of calcium. Hence the serum concentration is less than 20 nanograms per ml, symptoms of vitamin D deficiency develops. When the levels are less than 8 nanograms per ml, it is full blown vitamin D deficiency which requires high dose vitamin D supplementation
PREVALENCE OF VITAMIN D DEFECIENCY :
Vitamin D deficiency is a pandemic health issue and it prevails in
VITAMIN–D
COUNCIL
(ng/ml)
ENDOCRINE
SOCEITY
FOOD AND
NUTRITION BOARD
TESTING LABS
DEFICIENT 0- 30 0 -20 0-11 0-31
INSUFFICIENT 31-39 21-29 12-20
the increased prevalence of vitamin D deficiency in India and is around 70-100%21.
Following are the factors which increase the vitamin D deficiency :
1. Obesity
2. Dark skinnedperson’
3. Reduced sunlight exposure
4. Use of sunscreens
5. Consumption of nondairy beverages
6. Lifestyle modification
7. Cultural practices like wearing purdah
8. Associated systemic diseases like
a. Pancreatic insufficiency b. Malabsorption syndromes c. Cystic fibrosis
India, inspite of being a tropical country with adequate sunlight exposure, increase in prevalence of vitamin D deficiency is attributed to cultural practices, malabsorption and malnutrition.
TREATMENT OF VITAMIN D DEFICIENCY :
1. Awareness and health education programme. 2. Adequate sunlight exposure
3. Dietary modification
4. Food fortification–milk cereals 5. Vitamin D supplementation
VITAMIN D SUPPLEMENTS :
Treatment for vitamin D deficiency
Vitamin D deficiency is the most prevalent worldwide.Treatment of the same includes 1,25 hydroxy Cholecalciferol or calcitriol is the most biologically active form of Vitamin D. Vitamin D3 has four times more active potential than Vitamin D2. Hence Vitamin D3 supplements are more commonly used than Vitamin D2. Supplements includes combination of multivitamin strength of 50-100 IU. Vitamin –D can be safely supplemented in pregnancy in any trimester.
RECOMMENDED DAILY ALLOWANCE INSTITUTE OF
MEDICINE 1997 recommends78
1. 200 IU/day–Children and adults upto age of 50
2. 400 IU/day–Adults from 50-70 years
3. 600 IU/day–more than 70 years
But these levels are found to be inadequate hence they revised the guidelines :
INSTITUTE OF MEDICINE GUIDELINES 200578:
doses of vitamin D is essential to correct the vitamin D deficiency92,93,94. Studies have revealed that bolus vitamin D will not lead to equivalent increase in levels of 25(OH) as stated above the response to the vitamin D depends on the baseline Vitamin - D level.
TOLERABLE UPPER INTAKE LEVELS85:
The following table shows the tolerable upper intake levels of Vitamin - D
Tolerable Upper Intake Levels (ULs) for Vitamin D [1]
Age Male Female Pregnancy Lactation
0–6 months 1,000 IU (25 mcg)
1,000 IU (25 mcg)
7–12 months 1,500 IU (38 mcg)
1,500 IU (38 mcg)
1–3 years 2,500 IU (63 mcg)
2,500 IU (63 mcg)
4–8 years 3,000 IU (75 mcg)
3,000 IU (75 mcg)
9–18 years 4,000 IU (100 mcg) 4,000 IU (100 mcg) 4,000 IU (100 mcg) 4,000 IU (100 mcg)
SAFETY PROFILE OF VITAMIN D :
Hypervitaminosis is rare. Toxicity occurs only when high doses of vitamin D is given for prolonged periods61. Single high dose bolus or weekly high dose bolus over short period doesn’t cause toxicity.
SIGNS AND SYMPTOMS OF VITAMIN D TOXICITY :
1. Weakness
2. Polyuria
3. Poor appetite
4. Intense thirst
5. Nausea
6. Vomiting
7. Hypertension
8. Weight loss
The toxicity is mainly due to hypercalcemia63, which includes Hypercalciuria, nephrocalcinosis, nephrolithiasis, hyperphosphatemia.
DRUG INTERACTION
Vitamin D can interact with following drugs. Hence adequate precaution is advised while taking vitamin D with these following drugs
1. Antacids
2. Steroids
3. Anticonvulsants
4. Thiazides
5. Diuretics
6. Hydroxy Chloroquine
7. Barbiturates
8. Alcohol
9. Nicotine
CLINICAL IMPROVEMENT :
Vieth et al stated improvement occurs after 6 months of supplementation. A minimum period of atleast 2 months is required for clinical improvement.
MATERIALS AND METHODS:
SOURCE OF DATA:
100 AN mothers without any high risks of different ages, parity and BMI attending AN OPD clinic of the Department of Obstetrics and Gynaecology of Coimbatore Medical College Hospital for routine antenatal visit.
STUDY PERIOD:
October 2016 to September 2017
SAMPLE SIZE:
100 Antenatal Women.
STUDY DESIGN
Prospective study
Inclusion criteria:
1. Women >= 18 years
2. Singleton fetus - primigravida or multi gravida without any associated fetal anomaly
4. BMI ranging from 19 to 35
5. ANC with and without white discharge per vaginum and other pelvic symptom.
Exclusion criteria:
1. Patient refusal
2. Presence of any pelvic pathology
3. Prior antibiotic treatment (within 2 weeks)
4. Bleeding per vaginum
5. GDM, PIH complicating pregnancies and other Obstetric high risk cases are excluded.
6. Medical disease complicating pregnancy
7. History of intake of drugs like calcium, vitamin D, Oral contraceptives.
METHOD OF RANDOMISATION:
Sealed Envelope method
METHODOLOGY:
After obtaining written informed consent, 100 patients aged 21 to 35 years old adult females in mid gestation period (11 – 26 weeks ) attending the AN OPD clinics at Government Coimbatore medical college hospital ,Coimbatore enrolled for the study.
Each patient visiting our AN OPD enquired about their age, BMI, parity index, chief complaints, detailed menstrual history, obstetric history, any pelvic pathology, past medical and surgical history taken. General, systemic and detailed pelvic examinations were done. Sterile high vaginal swabs were taken for microbiological examination and a blood sample for analysing serum 25(OH) vitamin D3 level. Patients were followed throughout their pregnancy and 6 weeks postpartum.
RESULTS AND ANALYSIS
[image:82.595.159.527.148.315.2]The study is under taken under following divisions
Table 1. AGE
The frequency of occurrence in accordance with age are listed below, 14% belongs to <20 years of age
62% belongs to 20-30 years of age 24% belongs to >30 years of age.
Age Frequency Percent
<20 yrs 14 14.0
20-30 yrs 62 62.0
>30 yrs 24 24.0
Total 100 100.0
RESULTS AND ANALYSIS
The study is under taken under following divisions
Table 1. AGE
The frequency of occurrence in accordance with age are listed below, 14% belongs to <20 years of age
62% belongs to 20-30 years of age 24% belongs to >30 years of age.
14
62 24
Age
Age Frequency Percent
<20 yrs 14 14.0
20-30 yrs 62 62.0
>30 yrs 24 24.0
Total 100 100.0
RESULTS AND ANALYSIS
The study is under taken under following divisions
Table 1. AGE
The frequency of occurrence in accordance with age are listed below, 14% belongs to <20 years of age
62% belongs to 20-30 years of age 24% belongs to >30 years of age.
<20 yrs 20-30 yrs >30 yrs
Age Frequency Percent
<20 yrs 14 14.0
20-30 yrs 62 62.0
>30 yrs 24 24.0
Table 2. GESTATIONAL AGE :
Frequency Percent
<12 weeks 65 65.0
12-16 weeks 35 35.0
Total 100 100.0
Among the study population 65% belongs to <12 weeks of gestation 35% belongs to 12- 16 weeks of gestation.
Gestational Age * Signs and Symptoms of BV (Fishers exact test)
Signs and Symptoms of BV
Total
P value
Absent Present Gestational
Age
<12 weeks No 48 17 65 0.263 % 73.8% 26.2% 100.0%
12-16 weeks
No 22 13 35
% 62.9% 37.1% 100.0%
Total No 70 30 100
% 70.0% 30.0% 100.0%
Table 3. PARITY :
Frequency Percent
Primi 37 37.0
2nd Gravida 43 43.0
>=3rd gravida 20 20.0
Total 100 100.0
Among the study population
37% are Primigravida.
43% are 2ndgravida
Parity * Signs and Symptoms of BV (Chi-square test)
Signs and Symptoms
of BV
Total P value
Absent Present
Parity Primi No 28 9 37 0.247
% 75.7% 24.3% 100.0%
2nd Gravida No 31 12 43
% 72.1% 27.9% 100.0% >=3rd
gravida
No 11 9 20
% 55.0% 45.0% 100.0%
Total No 70 30 100
% 70.0% 30.0% 100.0%
Table 4.BMI
The following shows the frequency of distribution of BMI among study population
Frequency Percent
<30 63 63.0
>30 37 37.0
Total 100 100.0
Among the study population 63% have BMI < 30
37% have BMI >30
37
Table 4.BMI
The following shows the frequency of distribution of BMI among study population
Frequency Percent
<30 63 63.0
>30 37 37.0
Total 100 100.0
Among the study population 63% have BMI < 30
37% have BMI >30
63
BMI
Table 4.BMI
The following shows the frequency of distribution of BMI among study population
Frequency Percent
<30 63 63.0
>30 37 37.0
Total 100 100.0
Among the study population 63% have BMI < 30
37% have BMI >30
From this bar diagram we infer that there is a significant association between BMI and Vitamin D status
Deficiency increases with increasing BMI.
0 10 20 30 40 50 60 70 <30 30 29 31
From this bar diagram we infer that there is a significant association between BMI and Vitamin D status
Deficiency increases with increasing BMI.
<30 >30 BMI 30 4 29 7 3 15 1 11
BMI & Vitamin D Status
Vitamin D Status Severe
Vitamin D Status Deficient
Vitamin D Status Insufficient
Vitamin D Status Optimal
From this bar diagram we infer that there is a significant association between BMI and Vitamin D status
Deficiency increases with increasing BMI.
Vitamin D Status Severe
Vitamin D Status Deficient
Vitamin D Status Insufficient
Table 5. Signs and Symptoms of BV
Frequency Percent
Absent 70 70.0
Present 30 30.0
Total 100 100.0
In the study group those with signs and symptoms in pertaining to Bacterial vaginosis are present in only30% of the population remaining around 70 % have no signs and symptoms of BV. most of them are asymptomatic in this study.
70 30
Sign & Symptoms of BV
Table 6.Gram Stain
Frequency Percent
Negative 66 66.0
Positive 34 34.0
Total 100 100.0
From the above pie chart we infer that among the study population those who are screened for BV 34 % have gram stain positive which is done based on nugents criteria and about 66%are gram stain negative
66 34
Gram Stain
Gram Stain * Signs and Symptoms ofBV (Fishers’ exact test)
Signs and Symptoms
of BV
Total Sig
value
Absent Present
Gram Stain Negative No 58 8 66 0.000** % 87.9% 12.1% 100.0%
Positive No 12 22 34
% 35.3% 64.7% 100.0%
Total No 70 30 100
% 70.0% 30.0% 100.0% ** Significant at 1% level of significance
The above results are analyzed with Fischer’s exact test which
shows statistical significance between signs and symptoms of BV and gram staining.
From this comparison we infer that those with gram stain positive have signs and symptoms present .gram staining using nugents criteria is a specific method to diagnose bacterial vaginosis.
0 Negative Positive G ra m S ta in 12
Gram Stain & Signs and Symptoms of BV
From this comparison we infer that those with gram stain positive have signs and symptoms present .gram staining using nugents criteria is a specific method to diagnose bacterial vaginosis.
20 40 60 80
58 12
8 22
Gram Stain & Signs and Symptoms of BV
Signs and Symptoms of BV Absent
Signs and Symptoms of BV Present
From this comparison we infer that those with gram stain positive have signs and symptoms present .gram staining using nugents criteria is a specific method to diagnose bacterial vaginosis.
Gram Stain & Signs and Symptoms of BV
Signs and Symptoms of BV Absent
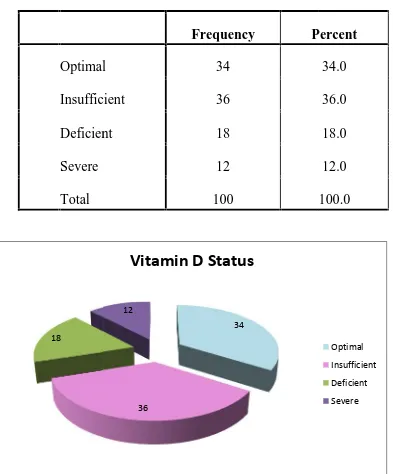
Table 7.Vitamin D Status among study population :
Frequency Percent
Optimal 34 34.0
Insufficient 36 36.0
Deficient 18 18.0
Severe 12 12.0
Total 100 100.0
Among the total population under study who are screened for vitamin d deficiency and are categorized based on 25 (OH ) vitamin D levels we found that 34% have optimal levels ,36%are insufficient , 18% are deficient and 12 % are severely deficient .this pie chart shows the distribution of vitamin D deficient among the study population.
18
Table 7.Vitamin D Status among study population :
Frequency Percent
Optimal 34 34.0
Insufficient 36 36.0
Deficient 18 18.0
Severe 12 12.0
Total 100 100.0
Among the total population under study who are screened for vitamin d deficiency and are categorized based on 25 (OH ) vitamin D levels we found that 34% have optimal levels ,36%are insufficient , 18% are deficient and 12 % are severely deficient .this pie chart shows the distribution of vitamin D deficient among the study population.
34
36 12
Vitamin D Status
Table 7.Vitamin D Status among study population :
Frequency Percent
Optimal 34 34.0
Insufficient 36 36.0
Deficient 18 18.0
Severe 12 12.0
Total 100 100.0
Among the total population under study who are screened for vitamin d deficiency and are categorized based on 25 (OH ) vitamin D levels we found that 34% have optimal levels ,36%are insufficient , 18% are deficient and 12 % are severely deficient .this pie chart shows the distribution of vitamin D deficient among the study population.
VITAMIN–D STATUS AND BACTERIAL VAGINOSIS :
This study aim to analyze the relation between the presence of vitamin D deficiency and the occurrence of bacterial Vaginosis.
Signs and Symptoms
of BV
Total Sig
value
Absent Present
Vitamin D Status
Optimal No 28 6 34 0.000**
% 82.4% 17.6% 100.0%
Insufficient No 30 6 36
% 83.3% 16.7% 100.0%
Deficient No 8 10 18
% 44.4% 55.6% 100.0%
Severe No 4 8 12
% 33.3% 66.7% 100.0%
Total No 70 30 100
From the above observation we found that prevalence of Bacterial Vaginosis is more in patients with Vitamin –D deficiency, there is a significant statistical association between them, this is well depicted in the following bar diagram.
0 Negative Positive G ra m S ta in 3 5
Gram Stain & Vitamin D Status
From the above observation we found that prevalence of Bacterial Vaginosis is more in patients with Vitamin –D deficiency, there is a significant statistical association between them, this is well depicted in the following bar diagram.
20 40 60 80
31 31 5 4 14 0 12
Gram Stain & Vitamin D Status
Vitamin D Status Optimal Vitamin D Status Insufficient Vitamin D Status Deficient Vitamin D Status Severe
From the above observation we found that prevalence of Bacterial Vaginosis is more in patients with Vitamin –D deficiency, there is a significant statistical association between them, this is well depicted in the following bar diagram.
Gram Stain & Vitamin D Status
Vitamin D status with Gram Stain
Descriptive Statistics
N Minimum Maximum Mean Std. Deviation
Vitamin D Status 100 7.10 82.50 39.8400 24.32219
Vitamin D status with Gram Stain
Gram Stain Mean N Std. Deviation P value
Negative 45.6000 66 23.91881 0.001**
Positive 28.6588 34 21.27584
From this above bar diagram we infer that there is a strong positive association between Vit D deficiency and occurrence of gram stain positivity which is diagnostic of Bacterial Vaginosis and the prevalence of bacterial vaginosis.
MATERNAL AND FETAL OUTCOMES OF STUDY
POPULATION :
MATERNAL OUTCOME
Frequency Percent
Chorioamnionitis 2 2.0
PP Endometritis 7 7.0
Puerperal fever 8 8.0
Wound infections 5 5.0
Normal 78 78.0
Total 100 100.0
Among the 100 study sample
2% developed chorioamnionitis.
7% developed PP Endometritis.
8% developed Puerperal fever.
MATERNAL OUTCOME
0 10 20 30 40 50 60 70 80
chorio amnionitis
2
MATERNAL OUTCOME
chorio amnionitis
pp endometritis
puerperal fever
wound infections
normal
7 8 5
78 MATERNAL OUTCOME
Maternal Outcome * Gram Stain
Gram Stain
Total
P value Negative Positive
Maternal Outcome
Chorioamnionitis No 1 1 2 0.043* % 50.0% 50.0% 100.0%
PP Endometritis No 4 3 7
% 57.1% 42.9% 100.0%
Puerperal fever No 3 5 8
% 37.5% 62.5% 100.0%
Wound infections No 1 4 5
% 20.0% 80.0% 100.0%
Normal No 57 21 78
% 73.1% 26.9% 100.0%
Total No 66 34 100
% 66.0% 34.0% 100.0% *Significant at 5% level of significance
FETAL OUTCOMES
Frequency Percent
Preterm labour 10 10.0
PPROM 7 7.0
Spontaneous Abortion 3 3.0
Normal 80 80.0
Total 100 100.0
Among the study population 7% had PPROM
10% had preterm labour 3% had spontaneous abortion
0 10 20 30 40 50 60
1 1 4
FETAL OUTCOMES
Frequency Percent
Preterm labour 10 10.0
PPROM 7 7.0
Spontaneous Abortion 3 3.0
Normal 80 80.0
Total 100 100.0
Among the study population 7% had PPROM
10% had preterm labour 3% had spontaneous abortion
4 3
1
57
3 5 4
21
FETAL OUTCOMES
Frequency Percent
Preterm labour 10 10.0
PPROM 7 7.0
Spontaneous Abortion 3 3.0
Normal 80 80.0
Total 100 100.0
Among the study population 7% had PPROM
10% had preterm labour 3% had spontaneous abortion
Fetal outcome * Gram Stain Gram Stain Total P value Negative Positive Fetal outcome Preterm Labour
No 2 8 10 0.000**
% 20.0% 80.0% 100.0%
PPROM No 1 6 7
% 14.3% 85.7% 100.0%
Spontaneou s Abortion
No 1 2 3
% 33.3% 66.7% 100.0%
Normal No 62 18 80
% 77.5% 22.5% 100.0%
Total No 66 34 100
% 66.0% 34.0% 100.0%
Preterm labour PPROM Spontaneous Abortion Normal
Fetal outcome * Gram Stain
Gram Stain Total P value Negative Positive Fetal outcome Preterm Labour
No 2 8 10 0.000**
% 20.0% 80.0% 100.0%
PPROM No 1 6 7
% 14.3% 85.7% 100.0%
Spontaneou s Abortion
No 1 2 3
% 33.3% 66.7% 100.0%
Normal No 62 18 80
% 77.5% 22.5% 100.0%
Total No 66 34 100
% 66.0% 34.0% 100.0%
0 20 40 60
Preterm labour PPROM Spontaneous Abortion Normal 10 7 3
Fetal outcome * Gram Stain
Gram Stain Total P value Negative Positive Fetal outcome Preterm Labour
No 2 8 10 0.000**
% 20.0% 80.0% 100.0%
PPROM No 1 6 7
% 14.3% 85.7% 100.0%
Spontaneou s Abortion
No 1 2 3
% 33.3% 66.7% 100.0%
Normal No 62 18 80
% 77.5% 22.5% 100.0%
Total No 66 34 100
% 66.0% 34.0% 100.0%