PHYTOCHEMICAL AND
PHARMACOLOGICAL EVALUATION OF
MEDICINAL PLANTS ON TYPE
II DIABETIC AND ITS COMPLICATION
Thesis submitted to
The Tamil Nadu Dr. M.G.R. Medical University, Chennai
for the award of degree of
DOCTOR OF PHILOSOPHY
in
PHARMACY
Submitted by
K G PRASANTH, M.Pharm.,
Under the guidance of
Dr. R VANKATANARAYANAN, M.Pharm., Ph.D.,
Principal
RVS COLLEGE OF PHARMACEUTICAL SCIENCES, Sulur, Coimbatore -641402
A
DECLARATION
This is to certify that the Ph.D. thesis entitled
PHYTOCHEMICAL AND
PHARMACOLOGICAL EVALUATION OF MEDICINAL PLANTS ON
TYPE II DIABETIC AND ITS COMPLICATION
submitted to The Tamil
Nadu Dr. M.G.R. Medical University, Chennai,
for the award of degree of
DOCTOR OF PHILOSOPHY
in
PHARMACY
was carried out by me under the
supervision of
Dr.R.VANKATANARAYANAN, M.Pharm.,Ph.D.,
Principal,
RVS College of Pharmaceutical Sciences, Sulur, Coimbatore - 641 042, Tamil
Nadu, India.
The contents of this thesis, in full or in parts, have not been submitted
to any other Institute or University for the award of any degree or diploma.
K.G. PRASANTH
ACKNOWLEDGEMENT
I take this opportunity to render my profound sense of gratitude to my
indebtedness and respect full regards to my guide
Dr. R.Venkatanarayanan,
M.Pharm., Ph.D.,
Principal, RVS College of Pharmaceutical Science,
Coimbatore for his assiduous guidance and sedate support during my research
work. Without whom my Ph. D degree would have been only a dream. His wide
knowledge and logical way of thinking have been great value for me.
His understanding, encouraging, personal guidance and care and his
insight have strengthened this study significantly. I will always thank full for his
wisdom, knowledge and deep concern. His constrictive criticism helped me a lot
to focus my views in proper perspectives .I am great full to him for giving me
liberty to carry out my research work independently throughout the course of
study .My respect personal regards are due to him forever.
I am deeply great full to my doctoral committee members
Dr. A.J.M Christina
, Principal, K M College of Pharmacy, Madurai and
Dr. W.D. Sam Solomon
, Professor & Head, Department of Pharmaceutical
analysis RVS College of Pharmaceutical Science, Coimbatore for their
constrictive ideas and suggestion and constant support throughout the work.
I express my grateful tribute to
Department of Pharmaceutics,
RVS
College of Pharmaceutical Sciences for providing me the excellent laboratory
facilities for accomplishing this work.
I also owe to, from the deepest corner of heart and indebtedness to Head of
the Department
Dr. G.Geetha,
PSG College of Pharmacy as I have been
constantly benefited with them and achieved pragmatic direction.
An endeavor such as a Ph.D. is impossible to accomplish without the
generous help and support of
Seniors
and
Colleagues
. I would like to take this
opportunity to thank those whom I was fortunate to know, work and form
friendship. How could I ever forget
Ms.G.Syamala
,
Dr.K.Umaa,
Mr.B. Prem Kumar, Ms. C.Kalaiarasi,
by whom I was inspired for my doctoral
work. I am very much thankful to him for his technical guidance and
comprehensive exchange of ideas during the course of my research work.
I would like to thank my students
Mr. Ananda Babu and B. Sriram
for
their support and help during the course of my research.
I would like to thank my
wife
Preethi .S
and
daughter
Aishwarya
for
their encouragement and prayers for the successful completion of my research
work.
CONTENTS
S.No. Topics
Page
no.
LIST OF TABLES
ii
LIST OF FIGURES
iii
LIST OF ABBREVIATIONS
v
1
INTRODUCTION
1
2
AIM AND OBJECTIVE
15
3
LITERATURE REVIEW
16
4
PLAN OF WORK
35
5
PLANT PROFILE
37
6
METHODOLOGY
39
7
RESULTS AND ANALYSIS
72
8
DISCUSSION
117
9
SUMMARY
131
BIBLIOGRAPHY
APPENDIX
LIST OF TABLES
Sl
No Table No
Title of the table Page
No
01 Table1 Criteria for diagnosis of diabetic 7
02 Table 2 List of plant drug with anti diabetic action 13 03 Table 3 Grouping of normal animals for carbohydrate tolerance test 54 04 Table 4 Grouping of diabetic animals for carbohydrate test 57 05 Table 5 Grouping of animals for the anti diabetic study using
STZ-Nicotiamied 59
06 Table 6 Blood glucose determination 60
07 Table 7 Triglycerides determination 61
08 Table 8 Cholesterol determination 62
09 Table 9 HDL determination 63
10 Table 10 Ash value of the plant Clerodendrum viscosum vent root 72 11 Table 11 Extractive value of the plant Clerodendrum viscosum vent
root 72
12 Table 12 Fluorescent analysis of the plant Clerodendrum viscosum
vent root 73
13 Table 13 Percentage of yield Clerodendrum viscosum vent root 73 14 Table 14 Preliminary phytochemical analysis of the plant extracts
Clerodendrum viscosum vent root 74
15 Table 15 Amount of flavonoid content in different extract
Clerodendrum viscosum vent root 75
16 Table 16 H NMR data of isolated compound from ethyl acetate
extract of Clerodendrum viscosum . 82
17 Table 17 Standard curve of Ascorbic acid for SOD estimation 84 18 Table 18 Percentage of inhibition of ethyl acetate extract of
Clerodendrum viscosum vent root SOD 84 19 Table 19 Standard curve of Ascorbic acid for estimation of NO 84 20 Table 20 Percentage of inhibition of ethyl acetate extract
Clerodendrum viscosum vent root on NO 85 21 Table 21 Standard curve of Ascorbic acid for the estimation of
Reducing power 85
22 Table 22 Percentage of inhibition of ethyl acetate extract
Clerodendrum viscosum vent root reducing power 85 23 Table 23 The IC 50 values of the ethyl acetate extract of
Clerodendrum Viscosum root 87
24 Table 24 Effect of ethyl acetate extract Clerodendrum viscosum vent
root on Carrageenane induced inflammation 92
24 Table 25 Effect of ethyl acetate extract Clerodendrum viscosum vent
root on oral carbohydrate tolerance test in normal rats 93 26 Table 26 Effect of ethyl acetate extract Clerodendrum viscosum vent
root on oral carbohydrate tolerance test on diabetic rats 93 27 Table 27 Effect of ethyl acetate extract Clerodendrum viscosum vent
LIST OF FIGURES
SL No
Figure
No Title of the figure
Page No
01 Figure 1 Generation of reactive oxygen species during hyperglycemic
condition 8
02 Figure 2 Chemical structure of STZ 55
03 Figure 3 Chemical structure of Nicotinamide 56
04 Figure 4 Gallic acid standard curve 75
05 Figure 5 HPTLC analysis of the extract of Clerodendrum viscosum
vent root 75
06 Figure 6 HPTLC analysis of isolated fractions of ethyl acetate extract
of Clerodendrum viscosum vent root 76 07 Figure 7 HPTLC peek display of Clerodendrum viscosum vent root 77 08 Figure 8 HPLC study of isolated fraction of ethyl acetate extract
Clerodendrum viscosum vent root 78
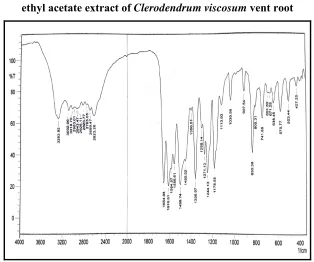
09 Figure 9 FTIR spectrum of isolated compound from ethyl acetate
extract Clerodendrum viscosum vent root 79 10 Figure 10 GCMS spectrum of isolated compound from ethyl acetate
extract Clerodendrum viscosum vent root 79 11 Figure 11 Chemical structure of the isolated a compound 80 12 Figure 12 NMR study of isolated compound of ethyl acetate extract
Clerodendrum viscosum vent root 81
13 Figure 13 Cell toxicity study of ethyl acetate extract of Clerodendrum
viscosum vent root on PC3 cell lines 83 13 Figure13 Cell toxicity study of ethyl acetate extract of Clerodendrum
viscosum vent root on L6 cell lines 83 14 Figure 14 Effect of alpha amylase inhibitory activity of ethyl acetate
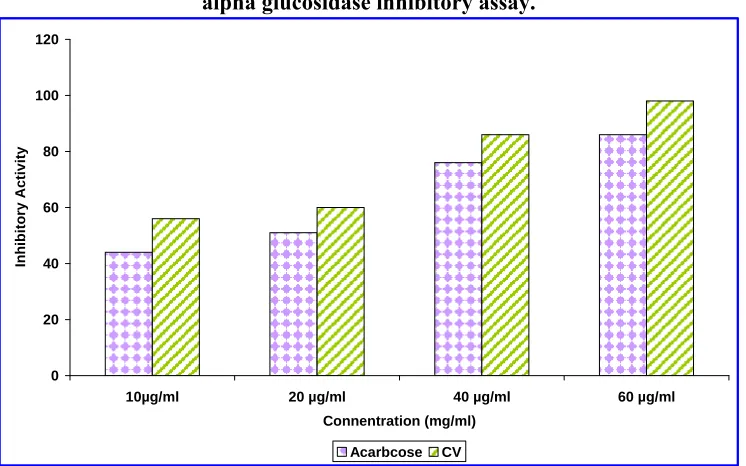
extract of Clerodendrum viscosum vent root 86 15 Figure 15 Effect of alpha glucosidase inhibitory activity of ethyl
acetate extract of Clerodendrum viscosum vent root 87 16 Figure 16 Effect of ethyl acetate extract of Clerodendrum viscosum
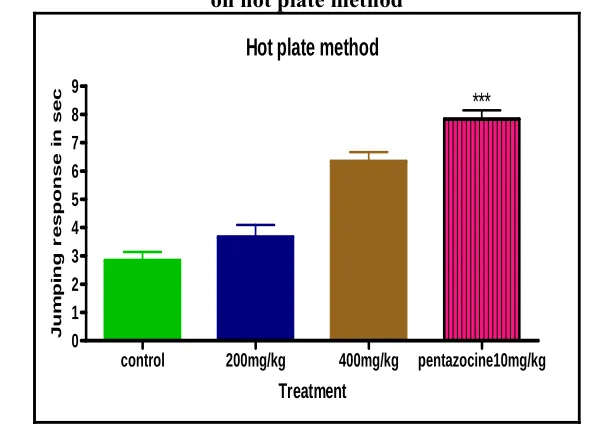
vent root on hot plate induced pain 88
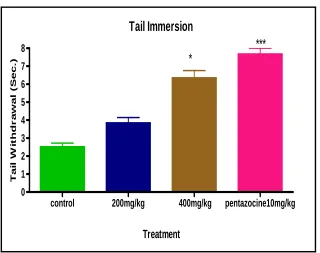
17 Figure 17 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on tail immersion 89
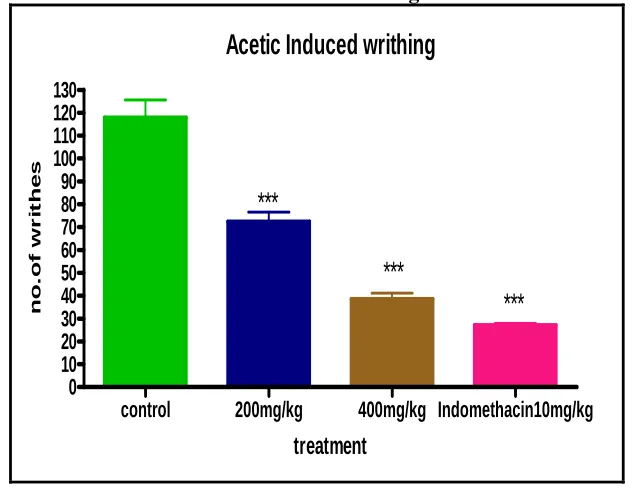
18 Figure 18 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on acetic acid induced writing 90 19 Figure 19 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on formalin induce pain 91
20 Figure 20 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on body weight of the animals 94 21 Figure 21 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on blood glucose level of the animal 95 22 Figure 22 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on total cholesterol 96
23 Figure 23 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on HDL 97
24 Figure 24 Effect of ethyl acetate extract of Clerodendrum viscosum
SL No
Figure
No Title of the figure
Page No
25 Figure 25 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on triglycerides 98
26 Figure 26 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on SOD 100
27 Figure 27 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on CAT 101
28 Figure 28 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on GPx 102
29 Figure 29 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on GSH 102
30 Figure 30 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on LPO 103
31 Figure 31 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on pain sensation in diabetic animals 104 32 Figure 32 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on nerve conduction study 105
33 Figure 33 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on systolic blood pressure 106 34 Figure 34 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on diastolic blood pressure 106 35 Figure 35 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on GLUT 4 expression on L6 cell lines 107
36 Figure 36 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on intensity of expression on GLUT 4 108 37 Figure 37 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on expression on GLUT 4 in rat skeletal muscles 108 38 Figure 38 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on pancreas of rat 109
39 Figure 39 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on aorta of rat 112
40 Figure 40 Effect of ethyl acetate extract of Clerodendrum viscosum
vent root on kidney of rat 113
41 Figure 41 Effect of ethyl acetate extract of Clerodendrum viscosum
List of Abbreviations
LIST OF ABBREVIATIONS
GAD
:
Glutamic acid decarboxylase
HLA
:
Human leukocyte antigen
MODY
:
Maturity onset diabetes of the young
FPG
:
Fasting blood glucose level
HbA
1C
:
Glycosylated hemoglobin
OGTT
:
Oral glucose tolerance test
WHO
:
World health organizations
DM
:
Diabetes mellitus
ROS
:
Reactive oxygen species
OS
:
Oxidative stress
AGEs
:
Advanced glycation end products
LDL
:
Low density lipoproteins
VLDL
:
Very low density lipoproteins
HDL
:
High density lipoproteins
GLP
:
Glucagon like peptide
DPP4
:
Dipeptidyl peptidases
CV
:
Clerodendrum viscosum
UV
:
Ultra violet
HPTLC
:
High performances thin layer
chromatography
HPLC
:
High pressure liquid chromatography
NMR
:
Nuclear magnetic resonance
GC/MS
:
Gas chromatography /mass spectrometer
STZ
:
Streptozotocin
List of Abbreviations
OECD
:
Organization of economic cooperation and
development
SOD
:
Superoxide dismutase
GPX
:
Glutathione per oxidize
CAT
:
Catalase
GSH
:
Reduced Glutathione
LOP
:
Lipid per oxides
GLUT4
:
Glucose transporter 4
L6
:
Rat skeletal muscle cell line
FTIR
:
Fouriertran from infra red spectroscopy
MTT
:
Methyl thiazol tetrazolin bromide
DNA
:
Deoxyribonucleic acid
mRNA
:
Messenger ribonucleic acid
NO
:
Nitricoxide
ATPs
:
Adenosine triphosphate
NADH
:
Nicotinamide adinin dihydrogen
TBAR
:
Thiobarbituric acid reactive substance
TBA
:
Thiobarbituric acid
PCR
:
Polymerized chain reaction
GAPDH
:
Glyceraldehyde -3-phosphate dehydrogenase
IDDM
:
Insulin depended diabetes mellitus
NIDDM
:
Non insulin depended diabetes mellitus
NaCl
:
Sodium chloride
PO
:
Per oral
IP
:
Intra peritoneal
AUC
:
Area under curve
List of Abbreviations
ml
:
Milliliters
mg
:
Milligram
µg
:
Micro gram
NPG
:
N –Para nitrophenyl gluco-pyranoside
HCl
:
Hydrochloric acid
ATM
:
Automated turning machine
KBR
:
Potassium bromide
SPSS
:
Statistical l soft ware for social science
TLC
:
Thin layer chromatography
AVOVA
:
One –way analysis of variance
H
2O
2:
Hydrogen peroxide
w/v
:
Weight / volume
Introduction
INTRODUCTION
Food or ‘Annam’ is the basic necessity of life and existence of living
organism. We all need food to develop physically and mentally and to work at our
maximum capacity, to build our defense against infections and maintain good
health. The traditional diet of Indians are immense varieties and the diversified
preparations not only offer the whole range of nutrients but also activate digestion
and several physiological functions. Until a few years ago, we used to prefer
natural food over refined food and light food (less oily) over heavy food. Our
traditional meals were mostly plant based and very rarely animal based. Both
plant based and animal based food were freshly cooked and eat at home. They
were a combination of cereals, millets, pulses, and spices such as pepper, cumin,
asafetida and coriander with curd and coconut satisfying our energy and protein
requirements. Those who could afford milk, yoghurt, eggs and chicken with small
amounts of animal meat adding to the protein requirement. Conception of
vegetables and fruits contribute to the intake of essential vitamins, minerals and
antioxidants required for supportive and detoxifying functions. The oils we use are
from groundnut, sesame, mustard and ghee which are essential, in small
quantities, to absorb fat soluble vitamins and also contribute to several hormonal
functions. These oils are the important source of fat in Indian diet. More over
being a source of energy, it also adds special flavor and traditional palatability to
the Indian food. The food we eat are balanced, diversified and freshly prepared
but not stored or processed.
Introduction
obesity and related problem like the type 2 diabetic and cardiovascular diseases.
These two obesity problems are the major reasons for the morbidity and mortality
in India.
More over the conception of Junk food in India has increased due to
Globalization and fast growing economy. Junk food refers to the food that tastes
good but is high in calories with little nutritional value. Across the world, different
types of diseases and health problems occur due to regular intake of junk food. In
all the developing and developed countries, younger generations are suffering
more problems with junk food.
1Diabetes is an oldest disease, described in Egyptian manuscript mentioning
as “too great emptying of the urine”. Type 1 diabetes was the first case to be
described in Egyptian manuscript 1500 BCE. Indian physicians have also
identified the disease in the same period and described as “madhumeha”
“or honey in urine. The Type 1 and Type 2 diabetes was identified and classified
by the Indian physician Sushrutha and Charaka in 400-500AD as type 1 associated
with young people and type 2 is associated with overweight. The effective
measures to treat diabetes started after the invention and usage of insulin by
Frederick Banting and Charles Best in 1921.
2,3Diabetes mellitus is a complex metabolic disorder characterized by
increased glucose level and relative or absolute insufficiency of insulin, deficiency
or resistance to insulin on target tissues, which leads to characteristic abnormality
in the metabolism of carbohydrate, lipid and protein. It is well established that
diabetes mellitus is a condition with a range of abnormalities like micro and
macro vascular complications, cardiomyopathy, neuropathy, nephropathy and
retinopathy disorders rather than a single disease state.
4Introduction
Epidemiology
Epidemiology can help in understanding and management of diabetes in
several ways. The epidemiologic studies can quantify changes in pattern and the
burden of disease. Second, identification of risk factors in large epidemiologic
studies may provide insight into pathophysiologic processes related to diabetes.
The study also allows the various factors involved, such as diet, gene,
environment and life style. Type 1 diabetes is autoimmune disorder found in
children or early adulthood stage which accounts nearly 10 % of the total diabetes.
It was estimated that 2.8% of the world’s population had diabetes in 2000 and this
ratio would climb to be as high as 4.4% of the world’s population by 2030.
590-95% of the diabetics belong to type 2 diabetes. The information from the national
diabetic fact sheet released in January 2011 says 25.8 million children and adults
in the United States i.e., 8.3% of the population have diabetes. 1.9 million new
case of diabetes was diagnosed in people aged 20 years and older in the study. In
United States the prevalence of diabetics among the males is 11.8% and in female
is 10.8%. Diabetic incidence is alarmingly increased in the world population also,
it is estimated that the number of diabetic individuals will be double to 180
million in the next 20 years.
6Based on the report of Diabetes Atlas 2006
published by the International Diabetic Federation, the Indian population with
diabetes will increase to 69.9 million from 40.9 million in 2025.. The diabetic
epidemic in India is so called “Asian Indian Phenotype” which has unique clinical
and biochemical abnormalities.
7WHO projected that India will become the fastest
growing population of diabetic patients in the world and will become the diabetic
capital of world.
Introduction
prevalence of diabetics is high in migrated Indian population (2.2%) when
compared with Europeans (1.2%). The occurrence of diabetes is more in south
India when compared with north India. In Tamilnadu, 10.4% of the population has
diabetes when compared with Maharashtra 8.4% and 5.3% in Jharkhand.
9The
overall probability in prevalence of diabetes differs in various parts of the world.
9.1% in Asia, 8.1% in Europe, 12.1% in North America, 4% in Africa. Multiple
logistic regression analysis showed that age, male sex, family history of diabetes,
urban residence, abdominal obesity, generalized obesity, hypertension and income
status were significantly associated with diabetes. Significant risk factors for pre
diabetes were age, family history of diabetes, abdominal obesity, and hypertension
and income status.
10Classification of diabetes
The diabetic patients are classified into two broad categories; type1
diabetes cases with an absolute deficiency of insulin and type2 diabetes with an
insulin resistance and inadequate release of insulin secretion.
Type 1 diabetes
Type1 diabetes or juvenile diabetes is an autoimmune disorder of the
pancreatic
β
cell. In the total diabetic population of the world, type 1 diabetes
accounts only 5-10%. Different markers for immune distraction of the
β
- cell
includes islet cell auto anti bodies, auto antibodies to insulin, auto antibodies to
Glutamic Acid Decarboxylase (GAD) and auto anti bodies to the tyrosine
phosphate IA-2 and IA-2
β
. This disease has a strong association to Human
Leukocyte Antigen (HLA) with linkage to DQA and DQB genes.
11Introduction
destruction of diabetes has a multiple genetic predispositions and is also related to
environmental factors which are poorly defined. These patients are also have the
chance to get other autoimmune disorders.
Type 2 Diabetes
Type 2 diabetes is characterized by insulin resistance and having relative
lack of insulin secretion. Most of the type 2 diabetic patients are obese and obesity
itself causes insulin resistance. There are many different causes of this form of
diabetes where the specific etiology is not known and no evidence of autoimmune
distraction in the
β
cells. The patients who are not obese may have an increased
percentage of body fat which is distributed predominantly in the abdominal region
which is one of reasons for the development of type 2 diabetes. This form of
diabetes is frequently not diagnosed for long period of time because
hyperglycemia develops slowly and usually diagnosed after development of other
complications. Type 2 diabetes has a highi genetic predisposition and is more
common in all ethnic groups. However, the genetics of this disease are more
complex and not clearly defined.
Gestational diabetes
Gestational diabetes is defined as any glucose intolerance with onset or
first recognition of pregnancy. This type of diabetes complicate nearly 7% of the
total pregnancy, early detection is important to reduce the morbidity and
mortality.
12Other specific type of diabetes
Several forms of diabetes are associated with monogenetic defects in the
β
cell dysfunctions and which are referred as maturity onset diabetes of the young
(MODY). This form of diabetes is characterized by onset of hyperglycemia at an
early stage (age of 25 years) due to impaired insulin secretion with minimal or no
defect in insulin action. This disease is inherited in autosomal dominant pattern
with at least six different genetic loci on different chromosomes that have been
identified as on date.
13Introduction
associated with the mutation in the insulin receptors. Women with these mutations
may have polycystic ovaries and hyper insulinemia.
11Diseases of the exocrine pancreas
Any diseases that injure the pancreas can cause diabetes, diseases like
pancreatitis, trauma, infection, pancreatectomy and pancreatic carcinoma.
11Endocrinopathy
The hypersecretion of several hormones that oppose the action of insulin
cause diabetes example in conditions like acromegaly, Cushing’s syndrome,
glucagonoma, pheochromocytoma .Hyperglycemia is resolved in case of hormone
excess.
11Drug or chemical induced diabetes
Many drugs can interfere with the secretion of insulin; these drugs do not
cause diabetes by themselves, but can influence the diabetic individuals with
insulin resistance. There are many hormones and drugs which impair the insulin
secretion. Examples are nicotinic acids and glucocorticoids fortunately such drug
interactions are less.
11Diabetes due to other infections
Certain viruses have been associated with cell destruction. Diabetes occurs
with congenital rubella infections. In addition coxsakie virus B, cytomegalo virus,
adeno virus and mumps have been implicated in inducing certain cases of
disease.
11Due to change of life style in urban population
Changed life styles especially those having high calorie intake and little
physical activity leads to type 2 diabetes. These types of diabetes are more
prevalent in developing countries.
14Diagnosis of diabetes
Introduction
the retinopathy as the key factor to identify the threshold of glucose level. A new
diagnostic point has been established by this type of studies ,ie, FPG of
≥
126mg/dl (0 7.0mmol/l) and standing plasma glucose value is 2hr of
≥
200mg/dl
(11.1 mmol/l) are more prevalent to diabetes and diabetes associated
retinopathy.
15Advanced glycation end products are widely used markers for
chronic glycemia conditions. Blood glucose level over 2-3 month period of time
can be predicted form the glycosylated hemoglobin (HbA
1c) level, should be less
than 6.5% in controlled FPG levels. HbA
1c has several advantages over FPG like
fasting is not required to predict pre analytical stability and perturbations in the
blood glucose level due to stress and illness. The decision about which test to be
used to assess the patient for diabetes should be left to the discretion of the health
care professional by considering into account the availability and practicability of
testing. The current diagnostic criteria for diabetes are summarized in a following
table1
Table 1: Diagnosis criteria for diabetes
01 HbA1c
≥
6.5%. The test should be performed in 3months once
02
FPG
at least 8 hrs
≥
126mg/dl (7.0mmol/l). Fasting is defined as no of calories intake for
03
2-h plasma glucose
≥
200mg/dl (11.1mmol/l) during OGTT. The test should
be performed as described by the WHO , using a glucose load containing the
equivalent of 75g anhydrous glucose dissolved in water
04
In a patient with classic symptoms of hyperglycemia or hyperglycemic
crisis, a random plasma glucose
≥
200mg/dl (11.1mmol/l).
Pathology and Pathophysiology
Introduction
complications in diabetes. The pancreatic
β
cells are also adversely affected by the
chronic hyperglycemia and are also a target for the secondary complication. The
prolonged hyperglycemia worsens the
β
cells of pancreas and steadily deteriorates
the secretion of insulin.. So glucose in chronic excess causes toxic effects on the
structure and function of the organs, including the pancreatic islets.
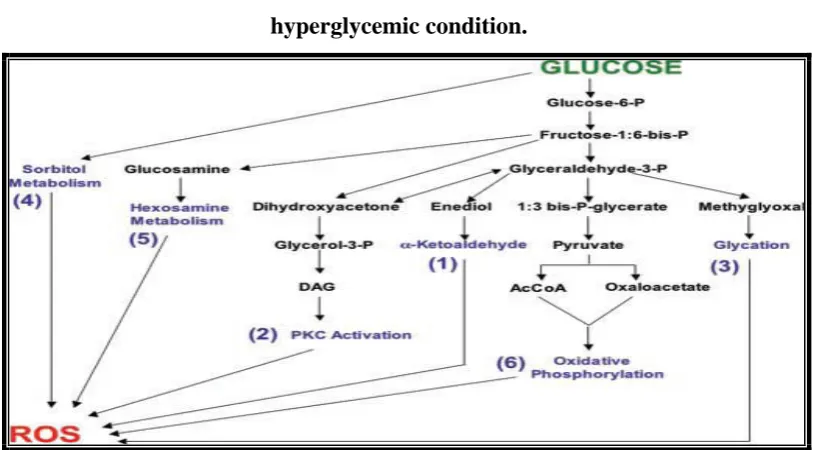
[image:20.595.107.515.446.671.2]In DM due to chronic hyperglycemia, generation and accumulation of
reactive oxygen species (ROS) induced chronic oxidative stress (OS), which has
been postulated to play a central role in the complication of diabetes disorder. In
normal physiological conditions, glucose primarily undergoes glycolysis and
oxidative phosphorylation and converts into energy. In diabetes condition,
excessive glucose level can inhibit the glycolysis and trigger at least six path ways
which are the major contributors for the production of ROS.
16(Fig 1) This
oxidative stress impairs the antioxidant enzyme system like reduced glutathione,
superoxides, catalase, peroxidase etc. The hyperglycemic stress during the
diabetes leads to various complications in diabetes.
Figure 1:Reactive oxygen species generated during
hyperglycemic condition.
Introduction
Microvascular complication
Diabetes mellitus has an increased risk in developing microvascular
complications if it is undetected or left untreated. This can have devastating
impact on quality of life and has a significant burden on health care cost.
Microvascular complications can bring forth the following disorders.
Diabetes retinopathy
It is the most common among various ocular complications of diabetes and
leading cause of new onset blindness. In the initial stage of diabetes retinopathy
there are no symptoms, as the diabetes progress lesion progressed and leads to
serious visual disability. Diabetes retinopathy affects the microvasculature in the
retina and divided clinically into two major types like non proliferative diabetes
retinopathy and proliferative diabetes retinopathy. Appearance of retinal
thickening and exudates within the retina is diabetes macular edema. Visual
impairment in diabetes is by the lesion developed due to proliferative diabetes
retinopathy or macular edema.
17The prevalence of diabetes retinopathy in western
population was reported to be 50.3% in US
18and 6-7% in India
16Diabetes nephropathy
Diabetes nephropathy is the major leading case of end stage renal diseases.
The earliest detectable changes in the diabetes nephropathy is thickening of the
glomerulus where serum albumin will leak more into the urine, which is not
present in the normal urine as in diabetes more number of glomeruli are destroyed.
Renal complication is clinically characterized by increase in rate of urinary
albumin excretion, starting from normal albuminuria which progresses to
microalbuminuria, macroalbuminuria and the end stage of renal diseases.
19Diabetes neuropathy
Introduction
multifocal and autonomic neuropathy. The most related mechanism for peripheral
neuropathy in diabetes is the activation of polyol pathway and accumulation of
polyol , injury from AGEs and oxidative stress. Amputation after foot ulceration
or injury is mainly due to the result of diabetes neuropathy.
20In diabetes
neuropathy complication chronic sensorimotor distal symmetric polyneuropathy is
the most common form. In this type of complication, patients experience burning,
tingling and electrical pain and sometimes experience simple numbness which
leads to painless foot ulcers.
21Pure sensory neuropathy is another type of
neuropathy due to poor glycemic control and fluctuation in diabetes control. It is
characterized by isolated sensory finding without any symptoms of motor
neuropathy. Mononeuropathies have a more sudden onset and involve virtually
any nerves, but most commonly, the median, ulnar and radial nerves. Cranial
neuropathy was also reported but rare.
22Diabetes autonomic neuropathy is
another type which causes significant morbidity and mortality in patients with
diabetes. In this neurological dysfunction most of the organs can be getting
affected, especially sudden deaths due to silent ischemia can occur.
23MACROVASCULAR COMPLICATIONS
Cardiovascular diseases
It refers to class of diseases that involves the heart, blood vessels due to
lipids like cholesterol and lipoproteins such as LDL, VLDL.
Introduction
cardiovascular complication. In India, the cardiovascular diseases was the major
reason for the morbidity and mortality associated with diabetes, prevalence of
coronary heart disease is also increasing at an alarming rate in India.
Cerebrovascular diseases
Stroke is another important cause of morbidity and mortality in diabetes
patients. Patients with diabetic have a higher risk of stroke and poor prognosis
when compared with non diabetes subjects. Prevalence of stroke has increased in
India over the past three decades. Diabetes is one of the important risk factors for
the development of stroke. The change in dietary habits (intake of more fats) and
smoking will increase the chance of stroke in diabetes people.
25Economical and social cost of diabetic
A different epidemiological study from various parts of the country
indicates the increase in prevalence of diabetes in the urban population. The most
alarming feature is the shifting of onset of diseases to younger age group. This
will have long lasting adverse effects on the national health system and economy.
The direct and indirect costs for the treatment of chronic diseases with
complications are more. There is urgent need for the cost effective protocol for the
treatment of diabetes care to reduce the morbidity and mortality and the economic
burden on the patients. The World Bank estimated that diabetes will account for
1,870,000 disabilities, with a per capita health expenditure of $21 in India.
26The
cost of diabetes in India study says that INR 4724 occurs towards the outpatient
care expenses. The total indirect cost for a non earning member was estimated as
INR 9748. This would be INR 16831 for an earning member.
27In USA the
economy burden of diabetes was estimated at about 45.2 billion $ and nearly 15 %
of the total health care expense.
28Treatment of diabetes
Introduction
biguanides meglitimide, thizolidinedione and alpha glucosidase inhibitors. Most
of these drugs stimulate pancreas and increase the secretion of insulin. Some may
interfere the absorption of glucose from the gastro intestinal tract. Biguanides like
drugs increase the sensation of insulin receptors to insulin.The newer drugs in this
category is glucagon like peptide -1 (GLP 1) agonist and dipeptidyl peptidase IV
(DPP4) antagonist which regulates the metabolism of insulin .Increases in cost,
inadequate supply of drug, adverse reaction and resistance are the reasons for an
alternative therapy. This increased the emphasis on the use of plant materials as
sources of medicines for diabetes.
Traditional system of medicine
Diseases are born with man and drug came into existence since a very
early period to remove the pain of diseases and cure them. To cure the ailments of
mankind nature has given a complete store house of remedies. The knowledge of
drugs has accumulated over thousands of years as a result of man’s inquisitive
nature, so that we posses many effective means of ensuring good health. Today
these have accumulated a vast store of knowledge concerning the therapeutic
property of different plants.
In India knowledge of medicinal plants is very rich and from age old and
these has been described in Rigveda and Atharvanaveda (3500-1500 BC) from
which Ayurveda has developed.
2921,000 plants, were listed by WHO , which are
used for medicinal purposes around the world. Out of these 2500 species were
found in India and 150 species are used commercially.
30There is an exponential growth in the field of herbal medicine and is
gaining popularity among the developing and developed countries due to its
natural origin and less side effect. Most of the traditional medicines that are in use
from the time immemorial are found to be derived from the natural sources.
31Plant drugs in the treatment of diabetes
Introduction
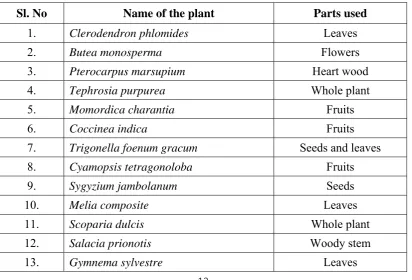
[image:25.595.103.516.470.750.2]out of which some of them are also used in commercial preparations. Eighty five
percent of the antidiabetes plants used most widely around the world are
prescribed in India.
32The list of plants used in the treatment of diabetes is in Table
2.
There is an increased demand among the patients to use the natural products
with antidiabetic activity so as to avoid the side effect associated with the use of
insulin and other proven synthetic hypoglycemic agents. The majority of type 2
diabetes patients are insulin resistant, for whom insulin or oral hypoglycemic
agents which stimulate the insulin release from the pancreas is not the ideal
therapy. The expert committee of WHO on diabetes has recently recommended
and validated scientifically the effect of antidiabetic drug from plant origin used in
traditional medicine.
33Plant source are used as single drug or as a combination of
many plants as formulation for the treatment of diabetes. The drugs which can
control lipid profile, glucose along with other complications can be a better drug
for the treatment of type II diabetes and it is the need of the hour also. Currently
the drugs prescribed are to control glucose level. These drugs may not take care of
the co- morbidities.
Table 2: List of plants with anti-diabetic activity
Sl. No
Name of the plant
Parts used
1.
Clerodendron phlomides
Leaves
2.
Butea monosperma
Flowers
3.
Pterocarpus marsupium
Heart wood
4.
Tephrosia purpurea
Whole plant
5.
Momordica charantia
Fruits
6.
Coccinea indica
Fruits
7.
Trigonella foenum gracum
Seeds and leaves
8.
Cyamopsis tetragonoloba
Fruits
9.
Sygyzium jambolanum
Seeds
10.
Melia composite
Leaves
11.
Scoparia dulcis
Whole plant
12.
Salacia prionotis
Woody stem
Introduction
For the present study we selected the important plant Clerodendrum
viscosum-vent (CV), Family: Verbenaceae. Synonym-Clerodendrum
infortunatum.L known as Bhandirah in Sanskrit and Perugilai in Tamil. It has
been used traditionally for the treatment of type 2 diabetes. It is an important plant
in the Indian system of medicine. It is traditionally used in ethno medicine for its
various medicinal properties which includes the treatment of scorpion sting,
34certain tumors, leprosy and skin diseases.
35Clerodendrum
viscosum
leaves on preliminary chemical analysis are found
to contain saponin, clerodin (a bitter diterpene)
36and some enzymes. Fixed oils
are present in leaves and also which consists of glycerides of lnoleic, oleic, stearic
and lignoceric acid.
37Previous phytochemical investigation of the plant revealed
the presence of alkyl sterols and 2,-(3,4-dehydroxyphenyl) ethanol 1-O-
α
-2
rhamnopyranosyl-(1
→
3)-
β
-D-(4-O-caffeoyl) glycopyranoside (acteoside)
38Clerodendrum viscosum leaves yielded flavone glucuronides (about 0.1
%)-scutellarin and hispidulin-7-0-glucuronide with practically no free aglycones. The
flavonoid pattern of C. indicum and C. infortunatum is similar to C.phlomides and
C.
nerifolium 4 in having the 6-oxygenated flavones occurring mainly as their
glucuronides.
Aim & Objective
AIM AND OBJECTIVE
Plant materials are used in developed and developing countries as home
remedies and over the counter products or as raw materials for the Pharmaceutical
industry. Latest trends have shown increasing demand for phytodrugs, which have
proven anti diabetic and antioxidant potentials. Medicinal herbs and extracts
prepared from them are widely used in the treatment of type 2 diabetes and its
complications. In the present study, an attempt has been made to understand the
role of
Clerodendrum viscosum
-vent Root in controlling the blood glucose level
and the complications (neuropathy, nephropathy and vascular damage) of diabetes
and also understanding the mechanism of drug action and the active compound
responsible for the anti diabetic property of
Clerodendrum viscosum
vent root
The Clerodendrum viscosum vent Root was studied for the Phytochemical
and Pharmacological point of view, so as to arrive at a standard drug for type 2
diabetes and its complications.
Such studies will promote global acceptance and international recognition
of herbal drugs of India, which in turn will contribute to the ailing human society
by relieving various ailments and in improving nation’s economy as well as
individual’s economy and living standards of tribal People.
To identify and isolate the active principle responsible for the
antidiabetic
activity
of
Clerodendrum viscosum
vent root by UV, HPTLC
Technique, Mass spectroscopy studies and NMR studies
Toxicity studies -To prove the safety aspects of
Clerodendrum viscosum
vent root by carrying out the acute toxicity and
in vitro
cell toxicity
studies.
To study the role of
Clerodendrum viscosum-vent
in controlling blood
glucose, lipids and free radicals formation in STZ –nicotinamide induced
diabetic rats
Literature Review
LITERATURE REVIEW
Prevalence of diabetes
Population based methodology was used in the study to assess the
prevalence of diabetes .The study that was conducted in 91 countries, was used to
calculate age and sex specific diabetes prevalence. The population included in the
study was 20-79 years range. The pattern of diabetes varies considerably
according to countries’ economic status. For developed countries, the majority
with diabetes are aged over 60 years, whereas for developing countries most
people with diabetes are of working age, between 40 and 60 years. This difference
is likely to still be present in 2030. In 2030 there will be an increase of 7.7%
especially in adult population ie, estimated increase in diabetic adult population
was 439 million in 2030. The reason for the increase in diabetes in adults is
mainly due to urbanization in developing countries and associated with more
sedentary life style. The study concluded that diabetes is continuing to be an
increasing international health burden. Ageing and urbanization are increasingly
adding to the burden of diabetes in developing countries.
39Literature Review
The age of onset in India has been shifting towards ever-younger people
even within the past decade among Indians in their late teens, ‘adult-onset’
diabetes already manifests itself more often than does ‘juvenile onset’ diabetes.
obesity is a risk factor for diabetes both in India and in the West, the disease
appears at a lower threshold of obesity in India, as is also the case in China, Japan
and other Asian countries.
Indians with diabetes are less
likely to develop
blindness and kidney disease,
but much more likely to suffer coronary artery
disease at a relatively young age.
14Prevalence rate of NIDDM in the migrant and native Indians in affluent
areas suggest the high genetic risk for diabetes in ethnic Indians. Age, urban-rural
factor, body mass index and abdominal adiposity (waist: hip ratio) were positively
associated with NIDDM. Migration from rural to urban environment with changes
in life style may have contributed to the increased prevalence of diabetes. The
prevalence of IDDM was 0.26/1000 with a peak age of 12 years at diagnosis. This
first population based study of prevalence of IDDM in South India has suggested
that IDDM is not rare and is higher than that reported from many other Asian
countries.
40Diabetes and pathogenesis
Type 1 and type 2 diabetes are characterized by progressive
β
-cell failure.
Apoptosis was the main form of
β
cell death in both forms of the disease. It has
been suggested that the mechanisms leading to nutrient and cytokine-induced
β
cell death in type 2 and type 1 diabetes, respectively, shares the activation of a
final common pathway involving interleukin (IL)-1
β
, nuclear factor (NF)- KB
and Fas. We review herein the similarities and differences between the
mechanisms of
β
-cell death in type 1 and type 2 diabetes. In the insulitis lesion in
type 1 diabetes, invading immune cells produce cytokines, such as IL-1
β
,tumor
necrosis factor (TNF)-
α
and interferon (IFN)-
γ
IL-1
β
and/or TNF-
α
plus IFN-
γ
Literature Review
of ER stress and by the release of mitochondrial death signal which execution of
beta cell death. Chronic exposure to increased levels of glucose and free fatty
acids (FFAs) causes
β
-cell dysfunction and induce
β
cell apoptosis in type 2
diabetes. High glucose level exposure of the beta cell has two effects, initially
triggering “glucose hypersensitization” and followed by apoptosis, via different
mechanisms. High glucose, however, does not induce or activate IL-1
α
, NF-KB,
or inducible nitric oxide synthase in rat or human
β
cells in vitro or in vivo in
Psammomys obesus. The ER stress caused by FFAs will leads to
β
cell apoptosis
which is independent to NF-KB and NO independent. Cytokines and nutrients
trigger
β
-cell death by different mechanisms. First one is the NF-KB–dependent
mechanism that culminates in caspase-3 activation for cytokines and an NF-KB–
independent mechanism for nutrients. This argument against a unifying hypothesis
for the mechanisms of cell death in type 1 and type 2 diabetes fails and suggests
that different approaches will be required to prevent -cell death in type 1 and type
2 diabetes.
41Diabetes mellitus was a syndrome of hyperglycemia and altered
metabolism of carbohydrate, fat and protein metabolism associated with absolute
or relative deficiency in insulin secretion or insulin resistance.
42It is also
characterized by polyuria, albuminuria, renal enlargement and an increase in
serum creatinine value. Developing premature atherosclerosis due to independent
risk factors such as hyper triglyceridemia and hypertension are the major risk in
diabetes.
43The hyperglycemic tissue damage is to a particular subset of cells like
capillary endothelial cells in the retina ,mesangial cell in the renal glomerulus and
neurons and schwann cells and peripheral nerve cells .These cells are not able to
reduce the glucose entry in hyperglycemic conditions like other cells which leads
to cell damage. In high glucose concentration aldose reductase also reduces
glucose to sorbitol and later oxidizes to fructose. In the process of reducing
glucose to sorbitol aldose reductase consumes the cofactor NADPH,
which reduces the amount of reduced glutathione leading to oxidative stress.
44Literature Review
Different forms of peripheral neuropathy in diabetes may manifest in are sensory,
focal,multifocal and autonomic neuropathies. Diabetic neuropathy is the main
reason for the amputation which occurs after the foot ulceration or injury.
12The developments of diabetic complications are the major reasons for the
mortality and morbidity in the diabetic patients. The complications are mainly
developed due to the oxidative stress during the hyperglycemia.Oxidative stress
mediated diversion of glycolytic intermediates into pathological pathways are the
key elements in development of diabetic complications. It is understood that
during diabetes, glycolytic path ways slow down and accumulate intermediates
like phospofructokinase, glyceraldehyde -3- phosphatedehydrogenase (GAPDH)
and pyruvate kinase. The ROS produced in the mitochondria due to the
accumulation of intermediates and their conversion into toxic byproducts initiates
the damage. The ROS migrates to the nuclease and produces the damage to the
DNA which results in the activation or the inactivation of glycolytic enzymes.
6Advanced Glycolytic end products formation is one of the major reason
for the development of diabetic complications. The AGE formation produced the
damage to the cell by three different mechanisms. The first mechanism is at the
endothelial cells by modifying inter cellular proteins, mainly the protein involved
in the regulation of gene transcription. The second mechanism is the AGE
precursor that diffuses from the cell and modifies the nearby intercellular matrix
molecules. This modification alters the signaling between the matrix and the cell
causing endothelial cell dysfunction. The third mechanism is by the diffused AGE
precursors that binds with the circulatory proteins like albumin and attach to the
AGE receptor and release the inflammatory cytokines and growth factors that also
cause vascular damage.
45Literature Review
insulin resistance and change in the release of endothelial derived factors
.sustained hyperglycemic state causes increased inter cellular concentration of
glucose metabolism in endothelial cells. Due to the hyperglycemic load causes
changes in the mitochondrial dysfunction and increase oxidative stress and
activation of protein kinase C .The oxidative stress and other factors increased the
expression of endothelin1, a changed balance between vasodilatation and
vasoconstriction and induction of adhesion molecules which causes the
endothelial dysfunction.
46Progression of coronary artery calcification (CAC) over an average of 2.6
years (range, 1.6 to 3.3) was assessed in a cohort of patients with type 1 diabetes
and nondiabetic subjects 19 to 59 years of age. In this nested case-control sub
study, plasma adiponectin levels were measured in 101 cases with significant
CAC progression and in 205 controls. Controls were oversampled on the basis of
age, gender, diabetes status and presence of baseline CAC. In conditional logistic
regression adjusted for baseline, CAC volume and other significant predictors of
CAC progression, adiponectin levels were inversely related to progression of
CAC in diabetic (OR, 0.47; 95% CI, 0.24 to 0.94) and non diabetic (OR, 0.15;
95% CI, 0.05 to 0.40 for a doubling in adiponectin levels) subjects. Adjustment
for additional cardiovascular risk factors did not change this association. In
conditional logistic regression models by quartiles of plasma adiponectin levels,
the probability value for trend was statistically significant for all participants
(P0.001) and non diabetic participants (P<0.001) and was borderline for type 1
diabetics (P0.08). Low plasma adiponectin levels are associated with progression
of CAC in type 1 diabetic and non diabetic subjects independently of other
cardiovascular risk factors.
47Literature Review
transcription factors PDX-1 and MafA and can also accelerate rates of apoptosis.
This pathophysiologic sequence sets the scene for considering antioxidant therapy
as an adjunct in the management of diabetes.
16Neuropathy is one of the most prevalent, devastating and costly
complications of diabetes. Distal symmetrical sensorimotor polyneuropathy
(DPN) is the leading cause of nontraumatic limb amputation. Diabetic autonomic
neuropathy (DAN) can affect virtually any body system and is associated with
greatly increased morbidity and mortality and can have a profound influence on
quality of life. Several biochemical mechanisms of nerve and neurovascular
damage have been identified and excessive production of reactive oxygen species,
or “oxidative stress”, is thought to be a common etiologic factor. Diabetic
neuropathies can be diagnosed with relatively simple tests of peripheral and
autonomic nerve function. Treatment of diabetic neuropathy should always begin
with efforts to optimize glycemic control and with patient education. There are
now many useful pharmacologic approaches to treat painful neuropathy and most
manifestations of autonomic neuropathy, but disease modifying treatments other
than strict glycemic control await a more complete understanding of the
underlying mechanism of diabetic neuropathy and the development of
pharmacologic agents based on this emerging knowledge.
48Literature Review
(HRO
2), as well as, non-radical species such as H
2O
2and hydrochlorous acid
(HOCl). RNS includes free radicals such as; NO and nitrogen dioxide (NO
2), as
well as non-radicals such as peroxynitrite (ONOO–), nitrous oxide (HNO
2) and
alkyl peroxynitrates (RONOO).
49Diabetes is one of the stress related disorder. Diabetes mellitus has been
shown to be a state of increased free radical formation. The existence of oxidative
stress resulting from increased free radicals has been postulated in diabetes.
Animal, human studies and in vitro experiments suggest the role for oxidative
stress, via an increased formation of free radicals in the pathophysiology of many
complications of diabetes, such as neurological, cardiovascular, retinal and renal
types.
50Moreover, glucose is in itself pro-inflammatory and increases the levels of
acute-phase inflammatory markers, including tumor necrosis factor-alpha
(TNF-
), interleukin (IL)-6 and C-reactive protein (CRP). These acute-phase
inflammatory markers are associated with insulin resistance and metabolic
syndrome, suggesting a role for chronic low-grade inflammation in
DM2 . Therefore, treatment aimed at reducing the degree of oxidative stress and
the production of pro-inflammatory cytokines in DM2 appear to be warranted.
51The endothelium is the common target of all cardiovascular risk factor,
and functional impairment of the vascular endothelium in response to injury
occurs long before the development of visible atherosclerosis.
The endothelial cell behaves as a receptor-effect or structure which senses
different physical or chemical stimuli that occur inside the vessel and therefore,
modifies the vessel shape or releases the necessary products to counteract the
effect of the stimulus and maintain homeostasis. The endothelium is capable of
producing a large variety of different molecules which act as agonists and
antagonists, therefore balancing their effects in opposite directions. When
endothelial cells lose their ability to maintain this delicate balance, the conditions
Literature Review
and T lymphocytes). The inflammatory response is incited and fatty streaks
appear, the first step in the formation of the atheromatous plaque. If the situation
persists, fatty streaks progress and the resultant plaques are exposed to rupture and
set the conditions for thrombogenesis and vascular occlusion.
Oxidant products are produced as a consequence of normal aerobic
metabolism. These molecules are highly reactive with other biological molecules
and are referred as reactive oxygen species (ROS). Under normal physiological
conditions, ROS production is balanced by an efficient system of antioxidants,
molecules that are capable of neutralizing them and thereby preventing oxidant
damage. In pathological states, ROS may be present in relative excess. This shift
of balance in favor of oxidation, termed ‘oxidative stress’, may have detrimental
effects on cellular and tissue function, and cardiovascular risk factors generate
oxidative stress.
Both type 1 (insulin-dependent) and type 2 (non-insulin-dependent)
diabetic patients have mostly been described under enhanced oxidative stress, and
both conditions are known to be powerful and independent risk factors for
coronary heart disease, stroke, and peripheral arterial disease. Hyperglycemia
causes glycosylation of proteins and phospholipids, thus increasing intracellular
oxidative stress. Nonenzymatic reactive products, glucose-derived Schiff base,
and Amadori products form chemically reversible early glycosylation products
which subsequently rearrange to form more stable products, some of them
long-lived proteins (collagen) which continue undergoing complex series of chemical
rearrangements to form advanced glycosylation end products (AGEs). Once
formed, AGEs are stable and virtually irreversible. AGEs generate
ROS with consequent increased vessel oxidative damage and atherogenesis.
52Literature Review
conversion of reversible Schiff base adducts and then to more stable,
covalently-bound Amadori rearrangement products. Over a course of days to weeks, these
early glycation products undergo further reactions and rearrangements to become
irreversibly cross-linked, fluorescent protein derivatives termed advanced
glycation end products (AGEs). There is a growing body of evidence that AGE
and their receptor RAGE (receptor for AGEs) interaction elicits oxidative stress,
inflammatory reactions and thrombosis, thereby being involved in vascular aging
and damage. These observations suggest that the AGE–RAGE system is a novel
therapeutic target for preventing diabetic vascular complications. In this paper, we
review the pathophysiological role of the AGE–RAGE-oxidative stress system
and its therapeutic intervention in vascular damage in diabetes. We also discuss
here the potential utility of the restriction of food-derived AGEs in diabetic
vascular complications.
53Literature Review
resulting in impairment of both IRS/PI3-K/Akt-mediated endothelial function and
NO production. This article summarizes the PI3-K/Akt pathway-mediated
contraction and relaxation responses induced by various agents in the blood
vessels of diabetic animals.
54Diabetic models
Literature Review
The release of reactive oxygen species (ROS) has been proposed as a
cause of streptozotocin (STZ)-induced b-cell damage. This initiates a destructive
cascade, consisting of DNA damage, excess activation of the DNA repair enzyme
poly (ADP-ribose) polymerase and depletion of cellular NAD1. Metallothionein
(MT) is an inducible antioxidant protein that has been shown to protect DNA from
chemical damage in several cell types. Therefore, we examined whether over
expression of MT could protect b-cell DNA and thereby prevent STZ induced
diabetes. Two lines of transgenic mice were produced with upto a 30-fold
elevation in b-cell MT. Cultured islets from control mice and MT transgenic mice
were exposed to STZ. MT was found to decrease STZ-induced islet disruption,
DNA breakage, and depletion of NAD1. To assess in vivo protection, transgenic
and control mice were injected with STZ. Transgenic mice had significantly
reduced hyperglycemia. Ultrastructural examination of islets from STZ-treated
mice showed that MT prevented degranulation and cell death. These results
demonstrate that MT can reduce diabetes and confirm the DNA damage
mechanism of STZ-induced b-cell death.
57Literature Review
poly (ADP-ribose) polymerase inhibitor. These data strongly indicate that
STZ-induced b-cell death is not caused by elevated intracellular O-GlcNAc levels, but
instead likely involves poly (ADP-ribose) polymerase in the mechanism.
58The anti-hyperglycemic action of Hei-Shug-Pian, the fire-processed
product of the root of Aconitum (Aconitum carmichaeli), was investigated in
streptozotocin-induced diabetic (STZ-diabetic male wistar rats 200 to250 gm) rats.
At 120 min following oral administration of Hei-Shug-Pian at doses ranging from
12.5 to 50 mg/kg, plasma glucose of STZ-diabetic was found to be decreased in a
dose-dependent manner. Under treatment conditions wherein plasma glucose was
lowered, the uptake of glucose into soleus muscle was increased and the
incorporation of glucose into glycogen of hepatocytes was enhanced. Blockade of
opioid receptors eliminated the plasma glucose-lowering effect of Hei-Shug-Pian
Moreover, Hei-Shug-Pian treatment failed to lower plasma
glucose in opioid -receptor knockout diabetic mice. The results obtained in this
study support the hypothesis that Hei-Shug-Pian lowers the plasma
glucose concentrations of STZ-diabetic rats through activation of opioid
µ-receptors of peripheral tissues, resulting in enhanced glucose utilization.
59Literature Review
In Africa the diabetes mellitus and other ailments are treated using stem
bark extracts of Terminalia superba Engl. and Diels and Canarium schweinfurthii
Engl. The evaluation of anti-diabetic effects of the methanol/methylene chloride
extracts of the stem barks on streptozotocin (STZ)-induced diabetes were carried
out using male rats. Diabetes was induced using 60 mg/ml of Streptozotocin
through subcutaneous administration. 150 mg/kg and 300 mg/kg of extract was
administered daily for 14 days to the rats received Streptozotocin two days prior.
At 300 mg/kg, the two extracts (Terminalia superba and Canarium
schweinfurthii), significantly showed at least 67.1% and 69.9% reduction in blood
glucose level, respectively, while insulin (three units) given subcutaneously and
once daily, had 76.8% reduction compared to diabetic untreated control rats.
Similarly, the weight gains were 6.6% and 4.9%, respectively, and were
comparable to the normal rats, whereas, sham control rats lost 14.1% body weight.
Still with the same dose, there was 68.5% and 58.5% (p < 0.001) significant
decrease in food consumption and 79.7% and 64.0%
(p < 0.001) in fluid intake by diabetic rats treated with the respective plant
extracts. At the end of the second week, the insulin-treated rats showed 56.4% and
75.8% decrease in food and fluid intake compared to an augmentation for diabetic
control rats, 43.0% and 383.8%, respectively. These results showed that the plant
extracts can reverse hyperglycemia, polyphagia and polydipsia exhibited by
streptozotocin, and thus, they have anti-diabetic properties.
61Free radical scavenging and antioxidant activity
Literature Review
evaluated in the liver, kidney and heart tissues of diabetic rats by measuring
malondialdehyde (MDA) and glutathion (GSH) levels. The results were compared
to the diabetic control groups. EtOAc Fr. was found to have rich in polyphenolics
and exhibited a significant antihyperglycaemic and antioxidant activity equipotent
with the reference hypoglycaemic agent (tolbutamide), when evaluated in diabetic
rats.
62The interest in possible health benefits of flavonoids has increased owing
to their potent antioxidant and free radical scavenging activities observed in vitro.
On the other hand, the antioxidant efficacy of flavonoids in vivo is less
documented and their prooxidant properties have described in vivo. They are able
to cause oxidative damage by reacting with various biomolecules, such as lipids,
proteins and DNA
63The present study was carried out to evaluate the in vitro antioxidant and
reactive oxygen species scavenging activities of Terminalia chebula, Terminalia
belerica and Emblica officinalis fruit extracts. 70% methanol extract were studied
for the in vitro free radical scavenging activity. Scavenging ability of the extracts
for radicals like DPPH, hydroxyl, superoxide, nitric oxide, hydrogen peroxide,
peroxynitrite, singlet oxygen, hypochlorous acid were also performed to
determine the potential of the extracts. The evidences can be concluded from the
study of the 70% methanol extract of the fruits of Terminalia chebula, Terminalia
belerica
and
Emblica officinalis, imposes the fact that they might be useful as
potent sources of natural antioxidant.
64Literature Review
The inhibition of alpha-glucosidase and alpha-amylase, digestive enzymes
of carbohydrates, can santly reduce the post-prandial increase of blood glucose
and therefore can be an important strategy in the management of blood glucose
level in type 2 diabetic and borderline patients. Currently, there is renewed interest
in plant-based medicines and functional foods modulating physiological effects in
the prevention and cure of diabetes and obesity. The plant kingdom is a wide field
to search for natural effective oral hypoglycaemic agents that have slight or no
side effects. More than 1200 plant species have been recorded to be used
empirically worldwide for their alleged hypoglycaemic activity. Therefore, natural
alpha-glucosidase and alpha-amylase inhibitors from plant sources offer an
attractive strategy for the control of hyperglycaemia. In this article reviews recent
data on plant extracts and isolated natural compounds that are being tested for
their anti diabetic activity, highlights the ongoing research and considers the
future persepctives.
66Literature Review
Herbal medicines have been used since prehistoric times by different
cultures worldwide for the treatment of diabetes. The present study evaluated the
effect of Ficus racemosa Linn. (Moraceae) stem bark on carbohydrate
hydrolyzing enzymes, viz., porcine pancreatic amylase, rat intestinal
alpha-glucosidase, sucrase and almond beta-alpha-glucosidase,by using different in vitro
model systems. In addition, the effect of the treatment was also studied. Untreated
F. racemosa bark (FRB) significantly inhibited (p < or = 0.05) alpha-amylase,
alpha-glucosidase, beta-glucosidase and sucrase in a dose-dependent manner.
Heat treatment of the sample comparably increased alpha-amylase,
alpha-glucosidase, and sucrase inhibitory activities, while a marginal decrease in
beta-glucosidase inhibitory activity was observed; however, no statistical
differences were observed . Untreated FRB showed IC
50values of 0.94% and 280,
212, and 367 microg/ml for alpha-amylase, alpha-glucosidase, beta-glucosidase,
and sucrase, respectively, while the IC
50values for heat treated FRB were 0.58%
and 259, 223, and 239 µg/ml, respectively. Further, a significant correlation
(p <or =0.01; r=0.791) was observed between alpha-amylase, alpha- glucosidase,
beta-glucosidase and sucrase inhibitory activities of both untreated and heat
treated FRB. The observations clearly says that inhibition of carbohydrate
hydrolyzing enzymes is one mechanism through which F. racemosa stem bark
exerts its hypoglycemic effect in vivo. Therefore, the potential exists to explore
the utilization of F. racemosa stem bark in the development of nutraceuticals and
functional foods for the management of diabetes and related symptoms/
disorders.
68Literature Review
skeletal muscle. In the diabetic rats decreased GLUT4 mRNA levels in white and
brown adipose tissue and the concentration of the messenger remaine unaltered in
red and white fibers of skeletal muscle. The interaction of benfluorex and diabetes
on GLUT4 protein expression showed a tissue-specific pattern. Benfluorex
treatment to some extent prevented the decrease in GLUT4 protein in white and
brown adipose tissue and in white muscle associated with diabetes. In contrast,
diabetes and benfluorex caused an additive decrease in GLUT4 expression in red
skeletal muscle. The effects of benfluorex on GLUT4 content in tissues from
diabetic rats showed the absence of alterations in GLUT4 mRNA levels,
suggesting a modification of translational or posttranslational steps. Benfluorex
did not ameliorate the hyperglycemia of diabetic rats. Our results indicate that red
and white skeletal muscle respond to diabetes and benfluorex in a heterogeneous
manner, which suggests the existence of differences in the mechanisms that
regulate GLUT4 expression. In the study data indicate that GLUT4 expression in
muscle and adipose tissue can be regulated by modification of translational or
posttranslational steps.
69