A STUDY ON THE EFFECTS OF INTRAVENOUS
DEXMEDETOMIDINE ON THE HAEMODYNAMIC
STRESS RESPONSE TO LARYNGOSCOPY
AND ENDOTRACHEAL INTUBATION
DURING GENERAL
ANAESTHESIA
Dissertation
Submitted to
THE TAMILNADU Dr. M.G.R MEDICAL
UNIVERSITY
In partial fulfilment of the requirements for the award
of the degree of
M.D ANAESTHESIOLOGY
Branch X
CERTIFICATE
This is to certify that this dissertation entitled “A study
on the effects of intravenous dexmedetomidine on the
haemodynamic
stress
response
to
laryngoscopy
and
endotracheal intubation during general anaesthesia” is a
bonafide record of the work done by Dr. Rakhi S.P under my
guidance and supervision in the Department of Anaesthesiology
during the period of her postgraduate study for M.D
Anaesthesiology [Branch-X] from 2012-2015.
Dr. V.G.Jayaprakash,
MD[Guide]
ProfessorDepartment of Anaesthesiology Sree Mookambika Institute of
Medical Science Kulasekharam Kanyakumari (Dist) – 629161
Mobile: 9447833999
Dr. Rema. V. Nair,
M.D., D.G.O.,Director
Sree Mookambika Institute of Medical Sciences [SMIMS] Kulasekharam [K.K District] Tamil Nadu -629161
Dr. G.Parvathy
, DNB, DAProfessor and Head
Department of Anaesthesiology Sree Mookambika Institute of
DECLARATION
In the following pages is presented a consolidated report
of the study “A study on the effects of intravenous
dexmedetomidine on the haemodynamic stress response to
laryngoscopy and endotracheal intubation during general
anaesthesia” a randomized clinical trial, on cases studied and
followed up by me at Sree Mookambika Institute of Medical
Sciences, Kulasekharam from 2013-2014. This thesis is
submitted to the Dr.M.G.R. Medical University, Chennai in
partial fulfilment of the rules and regulations for the award of
MD Degree examination in Anaesthesiology.
Dr.Rakhi S.P,
Junior Resident in Anaesthesiology, Department of Anaesthesiology,
Sree Mookambika Institute of Medical Sciences,
ACKNOWLEDGEMENT
I thank God almighty, for all his blessings, without which this work
would not have been possible.
I express my heartfelt gratitude our Director Dr. Rema V. Nair and our
Chairman Dr. Velayudhan Nair who provided me the infrastructure and for
permitting me to carry out this study. They are the foundation pillars of the
various activities that have been initiated in our institution.
I thank my HOD Dr. G.Parvathy whose suggestions, help, critical views
and constant motivation was present throughout the study period. She lent her
full support in times of difficulties that I encountered during this study period.
She is the answer to our prayers when we post graduates were straying during
our study times. It has been a tremendous and wonderful experience to work
under her guidance.
I thank my guide Dr V.G. Jayaprakash for his valuable help, suggestions
and supervision throughout the study. His encouragement from the inception of
this research to its culmination has been profound. He gave me constant
support throughout my post-graduation days without which this dissertation
would not have been completed on time.
I humbly thank Dr.Gopalakrishnan whose support, guidance, help,
critical views and comments kept me in full swing throughout my study period.
His suggestions were very valuable at each stage of my dissertation work. I am
indebted to him for his guidance and support throughout my initial post
I am also grateful to Dr.Subramaniam for his valuable support and
constant encouragement.
I also thank Dr. Rommy Geever, Dr.Prashanthan, Dr.Mahilamani and all
the staff members of Anaesthesiology for their valuable support.
I thank Dr.Mohsina Basheer, my co-pg, for her valuable and timely help
which made me complete my study on time.
I am grateful to my junior post graduates Dr.Suzanne and Dr.Jisha for
the various technical aspects of my study.
I am grateful to my family members for relieving me of my social
responsibilities so that I could fully focus my attention on this study.
Without the whole hearted cooperation of my patients, this thesis would
not have reached a conclusion. I express my sincere gratitude to all my patients
at Sree Mookambika Institute of Medical Sciences, Kulasekharam.
LIST OF CONTENTS
Sl.No.
Contents
Page No
1.
Introduction
1
2.
Aims and Objectives
2
3.
Hypothesis and Scientific Justification
3
4.
Review of Literature
4-75
5.
Materials and Methods
76-80
6.
Statistical Analysis
81-97
7.
Discussion
98-103
8.
Conclusion
104
9.
Summary
105-106
10.
References
107-138
LIST OF TABLES
Sl. No
Tables
Page No
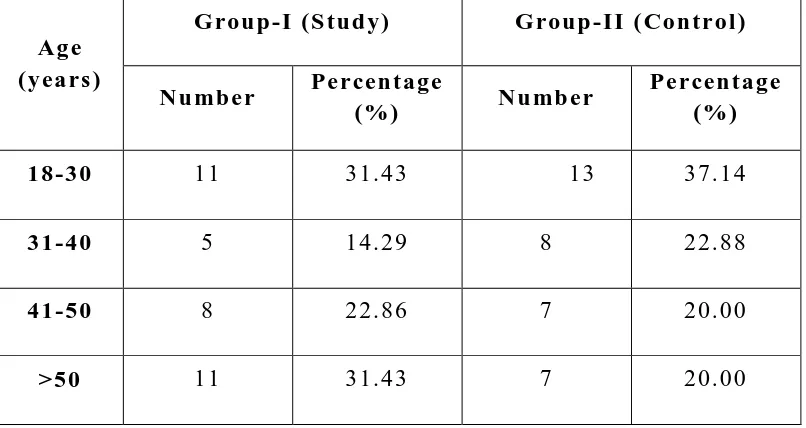
1
Distribution of Sample according to Age
81
2
Distribution of sample according to gender of
patients
82
3
Comparison of mean body weight between controls
and study group
83
4
Comparion
of
American
Society
of
Anaesthesiology score between controls and study
group
84
5
Comparison of number of patients who underwent
different types of surgery in group-I and group-II
85
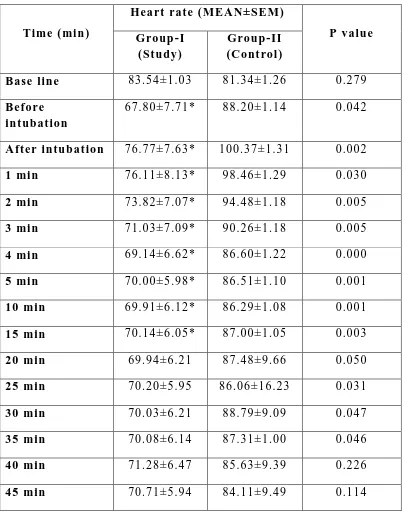
6
Comparison of heart rate changes between groups
at various time intervals
87
7
Comparison of mean systolic blood pressure
changes between groups at various time intervals
89
8
Comparison of mean diastolic blood pressure
changes between groups at various time intervals
91
9
Comparison of mean arterial pressure changes
between groups at various time intervals
93
10
Comparison of Isoflurane concentration used in
Study and Control Groups
95
11
No. of patients receiving supplemental Opioid in
intraoperative period
LIST OF FIGURES
Sl. No
Figures
Page No
1
Chemical structure of dexmedetomidine
49
2
Dexmedetomidine Vial and Ampoule
51
3
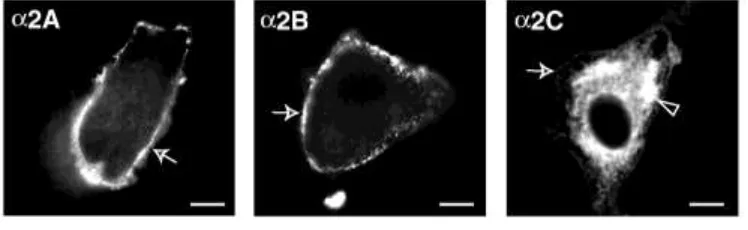
The different α
2adrenoreceptors
53
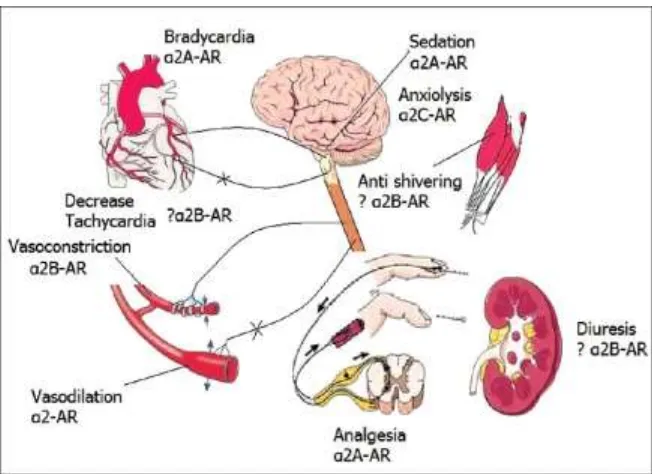
4
Physiology of dexmedetomidine
61
5
Distribution of Sample according to Age of patients
82
6
Distribution of sample according to gender of
patients
83
7
Comparison of mean body weight between controls
and study group
84
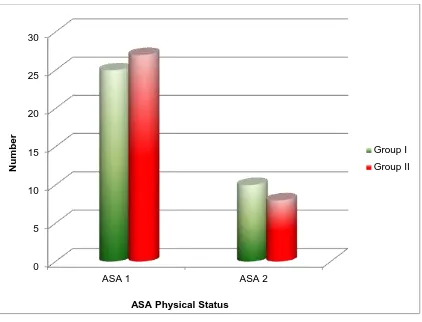
8
Comparion of American Society of
Anaesthesiology score between control and study
group
85
9
Time dependent changes in heart rate of group-I
and group II patients
88
10
Time dependent changes in systolic blood pressure
in group-I and II patients
90
11
Time dependent changes in diastolic blood pressure
in group-I and II patients
92
12
Comparison of mean arterial pressure changes
between groups at various time intervals
94
13
No. of patients receiving supplemental Opioid in
intraoperative period in Study Group
96
14
No. of patients receiving supplemental Opioid in
intraoperative period in Control Group
LIST OF ABBREVIATIONS
ANP
:
Atrial Natriuretic Peptide
ASA
:
American Society of Anaesthesiologists
ATP
:
Adenosine Triphosphate
AVP
:
Arginine
Vasopressin
BIS
:
Bispectral Index
CABG
:
Coronary Artery Bypass Grafting
cAMP
:
Cyclic Adenosine Monophosphate
CBF
:
Cerebral Blood Flow
CMRO
2:
Cerebral Metabolic Rate of Oxygen
CNS
:
Central nervous system
CPB
:
Cardio Pulmonary Bypass
CSF
:
Cerebro Spinal Fluid
ECG
: Electrocardiogram
ERCP
:
Endoscopic Retrograde Cholangio Pancreatography
FDA
:
Food and Drug Administration
GABA
: Gamma amino butyric acid
ICP
:
Intra Cranial Pressure
ICU
:
Intensive Care Unit
IM
: Intramuscular
IOP
:
Intra Ocular Pressure
LC
:
Locus Coeruleus
MAC
:
Monitored Anaesthesia Care
MAP : Mean Arterial Pressure
NS
:
Normal Saline
PaCO
2:
Partial Pressure of Carbon-di-oxide
PACU
:
Post Anaesthesia Care Unit
ABSTRACT
Background and Objectives:
During induction of general anaesthesia, hypertension and tachycardia caused by endotracheal intubation may lead to cardiac ischemia and arrhythmias. Dexmedetomidine attenuates the hemodynamic response to endotracheal intubation and reduces anaesthetic requirement. The purpose of this study was to evaluate the effect of intravenous dexmedetomidine 1μg/kg given over 10 minutes before induction of anaesthesia and 0.4mcg/kg/hour as maintenance during the surgery, on haemodynamic stress response resulting from laryngoscopy and endotracheal intubation and the haemodynamic stability during surgery.
Materials and Methods:
Seventy patients scheduled for elective surgery were randomized into two groups each having thirty five patients-dexmedetomidine group (Group 1) and control group (Group 2). Heart rate, systolic blood pressure, and diastolic blood pressure were recorded at just before intubation, immediately after intubation, 1, 2, 3, 4, 5 minutes after intubation followed by every 5 minutes till the first 45 minutes of surgery. Anaesthesia was induced with inj.Propofol 2mg/kg IV followed by succinyl choline 2mg/kg for endotracheal intubation. Anaesthesia was maintained with oxygen, nitrous oxide, isoflurane, atracurium. Any further need for analgesia was supplemented by IV fentanyl.
Statistical Analysis:
Results:
Pretreatment with dexmedetomidine 1 ug/kg attenuated the cardiovascular and catecholamine responses to tracheal intubation after induction of anaesthesia. In our present study, the rise in heart rate, systolic blood pressure and diastolic blood pressure after intubation, 1, 2, 3, 4, 5 and 10 minutes after intubation was significantly less in the dexmedetomidine group. The patients in dexmedetomidine group also had better haemodynamic stability during surgery. The requirement of opioids and isoflurane were significantly less in the dexmedetomidine group.
Conclusions:
Intravenous dexmedetomidine significantly attenuates sympathoadrenal response to laryngoscopy and endotracheal intubation and also cause reduction in intra operative anaesthetic requirement, without affecting intraoperative cardiovascular stability
Keywords:
1
INTRODUCTION
Bal anced anaest hesi a protocol s i nclude com bination of drugs o f different cl ass es used wit h specific purpos e s o as to creat e uncons ci ousnes s, m uscl e relaxat ion, anal gesi a and amnes i a. As the drugs are us ed in low t o moderat e doses, t he adverse effects are reduced. So anaest hesi a i nducti on, m aintenance and em ergence are safer, smooth er and comfort able. M ai ntenance of heart rate, blood press ure and depth of a naesthesi a are i mportant in t he int ra -operati ve period. Lar yngoscopy and intubation can l ead t o hemod ynamic stres s respons e which can be controlled b y suit abl e agents . Various drugs like li gnocaine, nifedi pine, Bet a blockers, ni t ro gl ycerine etc. are used to reduce hemod ynami c stress respons e to lar yngos cop y and i ntubati on.
Dexmedetomi dine i s a hi gh selecti ve cent rall y acti ng, pot ent alpha2 adrenergi c agonist with l ess durat i on of action. Alpha 2 to al pha 1 sel ectivi t y for dexmedet omidi ne is 1620:1 compared t o 220:1 for clonidine. Dexmedetomidine has sedati ve, anxiol yti c, anal gesi c and s ympathol yti c propert ies .
2
AIMS AND OBJECTIVES
1. To st ud y i f dexmedet omidi ne can reduce hemod ynami c s tres s respons e to l ar yngoscop y and t racheal i nt ubation.
2. Ass ess hem od ynam ic st abilit y during t he s urger y w hen dexmedet omidi ne is used.
3
HYPOTHESIS AND JUSTIFICATIONS OF THE STUDY
Hypoth esi s
Int ravenous Dexmedet omidi ne decreas es haem od ynam ic st ress respons e duri ng lar yngos cop y and endot racheal int ubation .
Sci entific Jus tification of the Stud y
4
REVIEW OF LITERATURE
Two predict ors of periope rative cardiac morbidit y are increase i n heart rat e and blood press ure . Increase i n heart rat e and acut e h ypert ension del et eriousl y affect m yocardial ox ygen suppl y and dem and. Di fferent t echniques are being t ried to prevent or at tenuate the hem od ynami c effect s fol lowing l ar yngos cop y and t racheal i ntubation, like deepening of anaesthesi a, avoidi ng anti cholinergi c drugs pri or t o surger y, pre-t reat ment wit h li gnocaine, vas odil ators like nitrogl yceri n , bet a blockers, cal cium channel blockers and opioi ds.
5
obs erved a ris e in s ys toli c bl ood pres sure of more t han 100mm Hg foll owi ng endot racheal i ntubati on.
Bedford des cribed t he relat ion of C NS to the cardi ovas cular respons e( 1 0 ). Duri ng l ar yngoscop y a nd endot ra cheal i ntubation, hem od ynami c inst abilit y ensues as l arynx, t rachea and cari na are having s ympat het ic nervous s yst em refl exes whi ch res pond t o subst ances or object s whi ch t he y com e i n cont act with . Ot her el em ent s such as a li ght er pl ane of anaest he si a are also contribut ory t o this stress res pons e.
C Pr ys Roberts et al( 1 0 ) dem onst rat ed t he el ectrocardi ographic and hemod ynami c respon ses to induction of anaest hesia fol lowed b y lar yngos cop y and endotracheal intubation. Takashim a K et al( 1 1 ) conduct ed a st ud y t o fi nd out t he real cause for cardi ovas cul ar res ponse to rapi d anaesthesi a induction and endot racheal i ntubati on and showed that the cardiovascular response du ri ng endot racheal int ubation was mainl y the res ult of inserti on of the l ar yngos cope blade. The variations in ECG found during intubation res ult s from stimul ati on of vagus nerve b y l ar yngos cop y. The reason for thes e cardiovas cular fl uct uations was studi ed and conclud ed that pressure ex erted b y the lar yngoscope blade on t he s oft ti ssues adjacent t o the epi glott is probabl y cont ribut ed to the el ect rocardiographic findings .
6
in infants and sm all children, but infrequentl y seen in adul t s also . As this refl ex is mediat ed b y an increas e i n vagal t one at sino-at rial node, it is considered as a monos ynapti c response t o a pai nful st imul us.
Sinus tach ycardi a is the s ympat het ic response to l ar yngos cop y and i ntubati on . Derbys hi re et al( 1 2 , 1 3 ) suggest ed t hat tracheal i ntubation is accompani ed b y b oth increased s ym pat heti c acti vit y and an increased adreno -m edull ar y catechol ami ne acti vit y. The com mon cardi ovascul ar respons es t o t racheal i ntubati on are produced b y thes e s ympat het ic efferents. Thes e pathwa ys are pol ys ynapt i c and travers e from t he vagal and gloss ophar yngeal afferent s t o the s ympat het ic s ys t ems through the brain and spi nal cord causing a di ffuse aut onomi c res ponse , including an increas ed firi ng of the cardio -accel erat or fibres and the rel eas e of norepi nephrine from adrenergi c nerve endings in m an y vascular beds , and rel eas e of adrenaline from the adrenal medull a. As renin rel ease d from t he juxt aglom erular apparatus of kidne y has β adrenergi c acti vit y, renin angi ot ensi n s yst em acti vat ion also pla ys a rol e in t he h ypert ensive change to int ubation.
7
the endot racheal tube was placed in the t rachea. Shribm an et al( 1 5 ) also studi ed the cardiovas cul ar change s to lar yngos cop y wit h or wi thout intubati on. The y demonst rated si gnifi cant and simil ar ri se of blood press ure and ci rcul ating cat echol ami ne concentrati ons wit h o r without intubati on. In tubation causes a hi gher i ncreas e i n heart rat e , whi ch was not seen wi th l ar yngos cop y onl y. Fi nfer et al( 1 6 ) com pared di rect lar yngos cop y with fiberopti c intu bation and found out t hat bot h lar yngos copic and bronchoscopi c int ubat ion res ult ed in s igni ficant increase in blood pressure and heart rat e without an y d ifference bet ween t he groups . It s eem s t hat maxim um i ncrease i n blood pres sure occurs with lar yngoscop y and t he m aximum rise in heart rat e occurs with endot racheal int ubation.
Elderl y pati ent s constitut e a hi gh percentage of both i npati ent and outpati ent hospital popul ation and have an greater incidence of coronar y art er y dis eas e, cerebrovascul ar dis eas e and a hi gher bas eli ne blood pres sure which makes them parti cul arl y suscepti ble to fluctuati ons in bloo d press ure and heart rat e during lar yngoscop y and endotracheal int ubat ion l eadi ng to increas ed ri sk of cerebro vas cul ar acci dent, m yocardial infarct ion, congest i ve cardiac failure or sudden death .( 1 7 , 1 8 )
8
number of non -cardi ac surgi cal pati ents at risk of cardi ac m orbi dit y i s found t o be 7 t o 8 mi llion patients per annum .( 1 9 )
Mangano s tat ed that it is diffi cult to ass ess the inci dence of perioperative cardiac morbi dit y . In t he elderl y group the range i s 2-15%.( 2 0 )
Rose and Tinker( 2 1 ) stat ed that final out com e (i.e. peri operative m yocardi al i nfarct ion, pati ent alive or dea d), should be di fferentiat ed from process out come (i.e. m yocardial is chemi a, h ypertensi on, tach ycardi a during surger y). When process out com e is considered, reduction of t hes e di fferent ph ys i ologi c dis turbance s duri ng anaesthesi a and surger y will be bett er for the pati ent. It i s not ye t proved that reduci ng s uch ph ysiol ogi cal changes actuall y improves final outcom e, as a ver y l arge populat ion stud y is needed to show rel ati vel y small but s igni ficant di fferences.
Goldm an and C aldera( 2 2 ) concl ud ed t hat h ypertensi on and the histor y of cardiac d ys rh yt hmi as were import ant risk fact ors in the issue of whet her preoperative i schemia can be a p redict or of negati ve outcome . Rab y et al( 2 3 ) st at ed that preoperative i schemia was a more i mport ant ris k factor, whi ch was in contrast t o Mongano et al ( 2 4 ) whos e stud y concl uded that post operative ischemi a was more import ant .
9
haemod ynami c effect. Patients requiring stabl e haemod ynami c s incl ude patients with a s ym ptom ati c aortic aneur ys m, ischemi c heart dis eas e, recent m yocardi al infarct ion, int racrani al h ypert ension and cerebral aneur ysm . Sl ogoff and Keats ( 2 6 ) st at ed that most of the is chemi c epi sodes during anaesthes ia were rel at ed to intubati on and s urgi cal sti mul ation, parti cularl y i f t ach ycardi a occu rs. Sim ilarl y Kleinm an et al( 2 5 ) stat ed t hat increas e in heart rat e and an i ncrease in afterload due to l ar yngos cop y and endotracheal i ntubation can be rel at ed wit h m yocardi al ischem ia occurring s econdar y to coronar y arter y vasoconstricti on.
The stud y b y Gol dman and C aldera and editorial b y P r ys Roberts( 2 7 ) gi ve rat ionale for del a ying surger y in pati ent s whose blood press ure cont rol is not optim al. Moreover, Steen et al( 2 8 ), concl uded that al most double the reinfarcti on rat e is s een perioperativel y in pati ent s who had h ypert ens ion preoperati vel y. Stone et al( 2 9 ) s tat ed t hat subst anti al ris k of developi ng m yocardi al ischemi a is more in h ypert ensive patient s unt reated before induction and t hat the ischemi a occurring during t he stres s of induction and i ntubati on was al wa ys associ at ed with ris e in heart rat e .
10
pulmonar y capill ar y wedge pressure and reduced ej ection fraction. An increas e i n heart rate del et eri ous l y affect m yocardi al ox ygen suppl y ( reduced di asto lic fill ing t ime) and dem and (i n creas ed cardiac work load ). Blood pressure has direct rel at i on with cardiac out put and s ys temic vascul ar resist ance. Acut e increas e in blood pressure affects bot h m yocardi al ox ygen suppl y and ox ygen dem and. During s ystemi c h ypert ensi on, peak s ys tolic ventri cul ar wal l t ensi on occurs , whi ch i ncreases m yocardi al ox ygen consumption.
Cardi ac output and sys t emi c vascul ar resist ance are rel ated to each other wit h vari ations i n one resulti ng in a com pensat or y respons e in the ot her. Both heart rate and bl ood pres sure are prim ar y det erminants of bal ance between m yocardi al ox ygen suppl y and ox ygen demand. Heart rat e is there on bot h ox ygen suppl y and ox yge n demand sides of the m yocardi al equ at ion. M yocardi al ox ygen suppl y can increase b y a reduction in heart rat e and ris e i n di ast oli c bl ood pressure, bot h wi thin ph ysi ological limi ts . The y act b y all owing a prolonged diastoli c filling tim e and a greater coronar y perfusi on press ure res pectivel y. M yocardi al ox ygen dem and increas es according to ris e in heart rat e, result ing in a les s di astol ic filling tim e and m yocardi al perfusion time .
11
Minor fact ors (whi ch are more or l ess fixed):
1. Met abolism (20%)
2. External work (17%)
3. Activation energy (3%)
Major factors (can be alt ered b y pharm acologi cal or ph ys i cal methods ):
1. S ys toli c wall t ension (30-40%)
2. Contractili t y (10 -15%)
3. Heart rat e
S ys toli c wall t ens i on is the most si gnifi cant determinant of left vent ricul ar work, accounting for 30 -40% of the energy needs of the beating heart . It is di rectl y proport ional to the product of art eri al blood pressure (afterload) and left vent ricul ar fil ling press ure (preload). Therefore an increas e i n eit her of thes e be yond thei r normal rang e wil l cause an i ncrease d m yocardi al work b y i ncreasing s ystolic wall tension. Thi s als o has a linear rel ati on wit h t he m yocardi al ox ygen cons umption. The concept of rat e press ure product (heart rat e x s ystem ic bl o od press ure), i ntroduc ed b y Georta et al (1957) has been found to effecti vel y refl ect changes i n m yocardial ox ygen consumption.
12
associ at ed wit h a ris e in m yocardi al cont ractil it y. Therefore ris e in heart rat e means ris e in m yocardi al work load i .e. increas e in ox ygen dem and.
On the other s ide of the scal e is t he m yocardi al ox ygen suppl y. Suppl y is regul a t ed b y adj us ting coronar y blood flow , whi ch is dependent on coronar y vas cul ar resi stance. As m yocardi al bl ood fl ow occurs in di ast ole, diastoli c bl ood pressure gi ves an estim at e of t he perfusion press ure. A diastolic blood press ure of 60mm Hg is generall y accept ed as a l ower limi t, bel ow whi ch t he perfusion is li kel y t o be com promis ed. Durat ion of di ast ole is anot her important factor affecti ng m yocardi al ox ygen suppl y. At a normal heart rat e of 75/m in ut e, dia stol e occupi es more than 60 percent age of t he cardiac c ycl e. When the heart rat e increas es , s yst oli c i nt erval s change littl e whil e di ast oli c intervals decreas es si gni fi cantl y. At a m aximum heart rat e of 180/mi nut e, di ast ol e occupi es onl y 40 percentage of the cardiac c ycl e. Here, an increase in rat e im pairs the m yocardial suppl y and can lea d t o i s chemi a or i nfarct ion when the balance between ox ygen suppl y and demand i s al r eady compromi sed. Thes e fact s show the i mport ance of at tenuating the st ress respons e .
13
clini cal s cenario and anaesthesi ologis t’s preference. Met hods ma y be les s si gni fi cant compared t o final resul t .
During general anaesthesi a , it i s diffi cult to det ect periods of inadequate m yocardial ox ygenat ion because angina pectoris , the most reliabl e indicator of m yocardial is chemi a cannot be identified. Hence other indices have to be used t o asses s t he adequac y of m yoc ardi al ox ygenation. The rat e pressure product refl e cts the m yoc ardi al ox ygen demand and is obt ained b y multipl yi ng s ys toli c blood pressure and heart rate. R ate pressure product has a cons tant associ ation wit h the ons et of angina pain. Pati ents whos e rat e press ure product w ere over 12000 show ed ischemi c changes in V5 l ead duri ng t he pre -b ypass period of coronar y art e r y surger y (Kapl an 1975). Thus i t is bett er to monitor the rat e pressure product in all pati ent s with coronar y art er y di seas e and mai nt ain it l ess than 12000 duri ng surger y, parti cul arl y during periods of st ress s uch as int ubation.
14
Durati on of lar yn gos cop y has bee n shown t o exert a n important effect on t he s everit y of cardiovas cular respons e. Att empts to reduce stress changes to l ar yngos cop y and endotracheal i ntubat ion could seem t o be the m ost suit able when intubati on is likel y to t ake great er than 30 s econds. This is parti cul arl y si gnifi cant in coronar y arter y dis ease or i nt racrani al h ypert ension. Prolonging l ar yngos cop y great er than 6 0 seconds produces more ris e in pulse rat e and blood pres sure (Stoelti ng, 1977).
Different met hods have been descri bed in lit erat ure to supress the cardiovascul ar respons es t o l ar yngos cop y and endotracheal intubat ion. Som e of them are :
1. Proph yl actic us e of Bet a bl ockers pri or to l ar yngos cop y and endotracheal i ntubation (acebut olol( 3 3 ), propranolol( 3 4 ), at enol ol( 3 5 ), met oprolol( 3 6 ), l abetol ol( 3 7 , 3 8 ) and esmolol( 3 9 ). Side effect s of beta bl ockers i ncl ude bronchospasm, brad ycardi a, h ypot ensi on, cardi ac d ys rh yt hmi as and heart fai lure .
2. Thoraci c epidural anaesthesia (Wat will et al( 4 0 ))
15
4. Us e of cal cium channel blockers( 4 1 - 4 3 ) (i ntravenous verapamil, 10m g nifedipi ne sublinguall y). The y m a y not be abl e t o prevent tach ycardia .
5. Magnesium sul fate i.v( 4 4 - 4 6 ) i nhi bits cat echolami ne releas e.
6. Vasodil at ors s uch as s odium nitropruss ide 1 -2mcg/kg i.v 15s econds pri o r to l ar yngos cop y( 4 7 ), h ydralazine, phentol ami ne, nit rogl ycerine( 4 8 - 5 0 ).
7. 2ml nit rogl yceri ne solution 60m g, 1 mi nut e prior to i nduct ion . (Fassoulaki and Kani ari s( 5 0 )).
8. Nitrogl ycerine oi nt ment 2% appli ed to s kin 12 m inutes before l ar yngos cop y (Elka yam U, Aronow WS)
9. Buprenorphi ne i . v( 5 1 )
10. Fent an yl 1 -2mcg/kg 2 -4 minutes before lar yngos cop y( 5 2 )
11. Alfent anil 15 -30mcg/ kg (Black et al( 5 3 )
12. Sufent anil 0.5 -1m cg/kg (Ka y et al( 5 4 ))
13. ATP( 5 5 , 5 6 ) i v 0.05 and 0.1m g/kg gi ven sim ult aneousl y with start of l ar yngos cop y (Mi kawa et al( 5 7 ))
16
300m cg/ kg/mi n found t hat all t hree dos es si gnifi cantl y reduce d the stres s respons e. (Menkhaus et al( 5 8 ))
15. IV Lidocai ne 1.5m g/kg 3 m inut es before int ubation minimizes blood press ure fluct uat ions after endot racheal intubati on. (Lev & Ros en( 5 9 ))
16. Li docaine gargl es prior t o lar yngoscop y and int ubation. (Stoelting( 6 0 ))
17. Li gnocaine 4% spra y into l ar ynx and t rachea before int ubati on. (Delinker et al( 6 1 ))
18. Fent an yl 6mcg/kg com ple t el y abolished haemod ynami c st ress respons e compa red to att enuation b y 2mcg/kg. (Kautt o U.M et al( 6 2 ))
The m ost recent s tudi es whi ch ai m in control or att enuat i on of haem od ynam ic st ress effects t o lar yngos cop y and i ntubation focus ed on the effect of remifentan yl at various dosi ng regim ens . Remi fent anil in a dose of 1m cg/kg bolus over 30 seconds foll owed b y an infusi on of 0.5mcg/ kg/mi n was found t o effi ci entl y att enuat e the stress respons e t o i ntubati on in a st ud y b y Thompson et al( 6 3 ).
17
anaesthesi a i s pos sibl e b y use of new, more potent alpha -2-adrenorecept or agonists, like m edetomidine and i ts st ereoisomer , Dexmedetomi dine . The i niti al movement for t he us e of α 2 -adrenorecept or agonists in anaesthesi a was a res ult of observati on made i n pati ents who were receiv ed cl onidi ne therap y( 6 4 ) during anaesthesi a. Kaukinen S et al( 6 5 ) demonst rated t he preoperative and postoperat ive use of cloni dine with neurol ept anaesthesi a. This was soon followed b y des cri ption of M i nimum Alveol ar Concentrati on requi rem ent of halot hane b y clonidi ne b y Bloor BC et al( 6 6 ).
18
Off-label use of dexmedetom idine outside the IC U incl ud e sedat ion and adjunct anal gesi a in t he operati ng room, sedation for diagnos tic and procedure units , and for other us es such as withdrawal detoxification/am eli orati on i n adul t and p aedi at ri c pati ent s( 7 6 , 7 7 ).
19
Dexmedetomi dine exhibits all t hese effects , whi ch hel ps i n avoidance of som e of the adverse effects of multi agent t herap y .
One o f the hi ghest densiti es of al pha -2 -adrenoreceptors has been foun d in locus coerul eus, m ai n noradrenergi c nucl eus i n brain and a ke y modul ator of vi gil ance. Sedative and h ypnoti c effects of alpha -2 -adrenorecept or acti vati on is at tri but ed to this site of ori gin for the descending medullo -spi nal noradrenergic pat hwa y, whi ch is known t o be a si gnificant modul ator of nocicept ive neurot ransmission . In LC , al pha-2-adrenergi c and opioi dergi c s yst em s are havi ng com mon effector m echanis ms, dem onst rating t hat dexmedetomidine has supras pinal site of action.
It can be concluded from t hes e findi ngs t hat the m ajor anti noci ceptive and sedati ve effects of dexm edetomi dine can be att ribute d t o stim ulati on of alpha -2-adrenorecept ors in l ocus coerulus . M oreover, studies i n t rans genic mi ce have dem onst rated that the alpha -2 -adrenorecept ors subt ype is liabl e for rela yi ng the anal gesi c and s edati ve properti es of dexm edetomi d ine.
20
functi on. The s econd phase of the biphasi c res pons e i s lon ger lasti ng reducti on of mean arteri al blood pressure and concomit ant decreas e in heart rat e. The y proved that dexmedet omidi ne i s wel l tolerated b y all subj ects. In anot her st ud y the y concl uded that i.v dexmedet omidi ne caus ed m ark ed s edation, mild h ypercapni a and h ypoventil ation, a nd an earl y t ransi ent ri s e i n ox ygen consumption. The minim al effect of dexmedetom idine i n ventilation indicat es that al pha-2-adrenoreceptor agoni s ts ma y be useful in providi ng anal ges ia and s edation without ventil at or y depressi on .
21
s ympatheti c tone was associ at ed wit h reduction in heart rate and blood pressure , wi thout an y compensat or y changes found i n the monitored endocri ne s ys t ems, rel ease of AVP and ANP or pl asm a renin act ivit y.
As an int ravenous premedi cant, dexmedetom idine reduces thiopent al requi rem ents (b y ± 30%) for short procedures , reduces the requirem ents of the vol atil e anaestheti cs (b y ± 25%), and more effectivel y attenuat es the haem od ynami c s tress res pons e to endotracheal intubation com pared with 2m cg/ kg of fent an yl . Yildiz et al( 8 2 ) conduct ed st ud y t o see t he effect iveness of dexmedet omidi ne on reducing haem od ynami c st ress changes to lar yngos cop y and t racheal int ubation. The y concl uded that a singl e dos e of dexmedetomi dine adm inist ered preoperativel y results in blunti ng of haemod ynami c stres s respons e during l ar yngos cop y, caus es progres sive increas es in s edati on and decreas es requi rem ent of opioi ds and anaest heti c s . M oreover, dexmedet omidi ne reduc ed not onl y bl ood pressure and heart rate but als o recov er y ti me after the surger y.
22
intravenousl y 10mi nutes pri or to inducti on of anaesthesi a. The dos e of thi opent one s odium requi red was si gni fi cantl y l ess in the dexmedet omidi ne group than in control group and the drug reduced the haemod ynami c respons es to l ar yngos cop y and endotracheal int ubation. C oncentrati on of noradrenaline in t he mixed venous pl as ma was l esser in the dexmedet omidi ne group throughout the phases of induction.
In th e st ud y conduct ed b y Hul ya et al( 8 4 ), a single dos e of 0.5m cg/ kg of dexmedetomidine administ ered preoperati vel y 10minutes before i nduction caus ed si gnificant s edati on, reduction in dos e of t hiopent one and blunted haemod ynami c re s pons e t o intubati on wi thout an y change in recover y charact eri sti cs. J aakol a et al( 8 5 ), demonst rated t hat dexmedetomidine reduced the i ncrease in hea rt rat e and blood pressure during int ubation. Varshali et
al( 8 6 ) showed that dexm edetomi dine causes at tenuation of
23
Similarl y, average increas e in heart rat e was 7% and 21% i n dexmedet omidi ne group and cont rol group respectivel y. Lawrence et al( 8 7 ) ` found that a singl e dose of d exmedet omidine pri or to induction of anaest hesi a reduced the haemod ynami c st ress respons e to both i ntubati on and extubati on.
Bajwa et al( 8 8 ) showed that t he press or res ponse to lar yngos cop y, i ntubation, surger y and extubation were effi ci ent l y decreas ed b y dexm edetomi dine . One hundred pati ents posted for el ect ive general surger y were divi ded int o t wo groups. Group D were gi ven 1m cg/ kg of dexmedet omidine and fent anyl while Group F received 2mcg/kg of fe nt an yl preoperativel y. Anaesthes ia was induced using thiopent al and was maintai ned wi th ox ygen -nitrous oxide and Is oflurane. The mean dos e of fentan yl and isofl urane were al s o reduced si gni ficantl y (50%). The mean recover y time was also s horter i n the dexmedetomidine group.
Turan et al( 8 9 ) dem onst rated t hat without int erfering with the recover y tim e, dexmedetom idine 0.5m cg/ kg gi ven 5mi nut es before the end of s urgery causes st abi liz ati on of h aemod ynami cs, allows eas y extubat ion, provi des a sm oother recover y and all ows earl y neurol ogi cal as sess ment aft er int racranial surgeries .
24
in pati ent s undergoing int racrani al surger y wi thout causing an y increase in the inci dence of h ypotensi ve epis odes and brad ycardi a.
Similarl y Zerrin Oz kose et al( 9 1 ) concl uded that combinati on of preoperati ve l oading and in traoperative intravenous infusion of dexmedet omidi ne caus ed bl unti ng of press or respons e to tracheal intubati on and s urger y, reduc ed requirement of des flurane shortened the recover y tim e, improved haemo d yn ami c st abilit y and reduc ed postoperative pai n level s i n patients who underwent lumbar discectom y u nder desflurane anaest hesi a. In a prospecti ve , random ized, double bl ind tri al, dexmedetomidine infusion (1m cg/ kg or saline placebo) before i nduction was us ed t o reduce the haemod ynami c s tress change to i nt ubation along wit h low dos e fent an yl and etomi dat e in 30 pati ent s who under went m yocardi al revascul ariz ation receiving bet a blocker t reatm ent. After induction the drop in heart rat e was hi gher in the dexm edetomi di ne group as compared wit h placebo gro up. One minut e aft er i ntubation heart rate s i gni fi cantl y rais ed in placebo group whil e i t reduc ed in dexmedet omidi ne group. Incidence of h ypert ens ion whi ch requi r ed t reatm ent was si gnificant l y hi gh er in the placebo group( 9 2 ).
25
range of 0.18 t o 0.35ng/ml ) attenuat es increas e in heart rat e and plas ma nor adrenali ne concent ration s een during em ergence from anaesthesi a. Tul fanigull ari B et al( 9 4 ) studi ed on the effect of dexmedet omidi ne infusi on on recover y out com e vari ables during laparos copic bari atri c surger y. The y found t hat, use of intraoperative dexm edetomi dine i nfusion (0.2 -0.8m cg/kg/hr) reduced fent an yl us e, anti emeti c therap y and the t otal durati on of st a y in PACU. Likewi se Hass an S( 9 5 ) also conc luded in hi s st ud y that Infusi on of dexm edetomi dine i ntraoperativel y reduc ed the total amount of propofol and fent anyl necess ar y to maint ain anaesthesi a, offered a bett er cont rol on the intraoperative and postoperative haem od ynami cs , reduc ed postoperative pai n level s , reduce d the t otal amount of m orphine us ed and s howed a bett er recover y profil e compared to pl acebo.
J eongmi n Kim et al( 1 8 1 ) (2014), conduct ed a stud y on agitat ion duri ng em ergence followi ng d esfl urane anaesthes ia in paediat rics . The y found out that infusi on of low dos e dex medeto m idine int raoperativel y along wi th fentan yl decreas es em ergence agitation occurri ng aft er des flurane anaesthesia i n paedi atric pati ents undergoing strabis mus surgeri es.
26
Anaesthesiolog y gra de 1 and 2 . The y divided them i n t o t wo groups: Fi rst group received I nj. Dexmedetom idi ne 1µ g/kg over 15m in, which was followed b y 0.5µg/ kg/ hr i nfusion and the other group receive d Inj . Midazolam 0.05 mg/kg sl ow i.v, followed b y an i nfusi on of 0.01m g/kg/hr. Their arteri al heart rat e, blood pressure and sedati on level were mo ni tored. The y concluded t hat Dexmedet omidi ne could be a bett er alt ernative over Midazol am for MAC in ENT s urgeri es done under local anaesthesia.
27
Dal ia Abdel hamid Nasr , et al,( 1 8 4 ) in 2013, conduct ed st ud y on the effecti veness of dexm edetomi dine admi nist ered caudal y on the stress res ponse and postoperative pain i n cardi ac surger y i n children. Fort y pati ents , ( Am eric an Soci et y of Anaesthesi ology 2,3 ), 1-3 - years of age were random l y di vided int o 2 groups; group I received caudal bupivacaine 0.25%, 2.5 m g/ kg and dexmedet omidi ne 0.5 μg/ kg and group II received bupivacaine 2.5 mg/kg and fentanyl 1 μg/kg. They concl uded that caudal dexmedetomidi ne is a useful adjuvant in anaesthesi a for chil dren undergoi ng cardiac surgeri es , it reduces t he cardiovas cul ar and neuroend ocrin e st res s respons e s caus ed b y t rauma and CP B, and it als o provides adequat e postoperative anal gesi a and short tim e to extubat ion.
28
extubation t ime. Dexmedet omidi ne dos es of more than 0.5 µg/ kg di d not exert an y s urplus positi ve effects on cardi ovas cul ar respons es, but did s i gni fi cantl y prol ong t he extubation ti me.
Ashraf M. Eskandr, et al, ( 1 8 6 ) in 2014, conduct ed a stud y to evaluat e t he effect s of addi ng dexmedetomidine to local anaestheti cs on t he s ens or y and motor block of t he s ubt enon block i n pati ents undergoi ng phacoemulsi ficati on cat aract s urger y. 6 0 patient s of Ameri can Soci et y of Anaes thesiolog y grade 1 -3, aged bet ween 18 and 70 years, posted for phacoemul sifi cat ion cat aract surger y were random l y assi gned t o 2 equal groups. In cont rol group , pati ents were gi ven 2 ml mixture cont aining 2% li gnocaine and 0.5% bupi vacaine and Dexmedetomi dine group were given 2 m l of a m ixture cont aining 2% li gnocaine and 0.5% bupivacaine pl us dexmedetomidine (0.5 μ g/ kg). Ons et and durati on of sensor y and m otor bl ock was recorded. P ai n whil e admi nist ering an aesthesi a and during surger y was graded and recorded. Int raocul ar pressure, hem od yn ami c, and s edation param e t ers were recorded before and after surger y. The st ud y demonst rat ed that adding dexm edetomi dine (0.5 μ g/kg) in a mixture of 2% li gn ocaine and 0.5% bupivacai ne i n subt enon block for pati ent s undergoing cat aract phacoem ulsi fi cat ion surger y, resulted in rapid ons et and prol ongation of anal gesi a and akines ia with decreas ed i ntra ocul ar pressure and stable hemod ynami c changes .
29
com plicati ons and m ort alit y fol lowing cardi ac surger y. The s tud y was done on 1134 pati ents who had coronar y art er y b ypass surger y and CABG plus val vul ar surger y or other procedures . Am ong thes e pati ents 568 received dexmedet omidi ne infusi on intravenous l y w hil e 566 did not. Mortalit y and postoperative maj or cardiocerebral advers e events like st roke, coma, peri operati ve m yocardial infarction, heart block, or cardiac arrest were the prim ar y out com es m easured . S econdar y out com es were kidne y fai lure, sep ti cemi a, deli rium , ventil at ion hours needed post operati vel y, lengt h of st a y in hospit al and readmi ssion withi n 30 -da ys . The stud y demonst rated that cardi ac s urgi cal patients who received i ntravenous dexmedet omidi ne i nfusi on aft er cardiopulmonar y b ypas s had a bett er in -hospit al, 30 -da y, and 1 - year survival rat e. The us e of dexmedet omidi ne perioperativel y al so caused si gni fi cant reducti on in inci dence of postoperative com plicati ons incl uding deli rium . There were no evidences of advers e hem od ynami c effects of d exmedetomidine i n pati ent s who under went cardi ac s urger y.
30
adj ust ed i ntraoperati vel y to a bispect ral in dex of 70 -80. In t he P ACU , the sedation s core was ass es sed ever y 10 minut es unti l di scharge. The degree of pain was asses sed hourl y for t he fi rst 12 hours and at 18 and 24 hours pos toperat ivel y. Durati on of anal gesi a and need of rescue anal gesi a were cal cul at ed. Thi s stud y concl uded t hat intravenous sedati ve dos es of dexmedet omidi ne can prol ong t he anal gesi c effect of supracl avi cul ar brachial pl exus nerve block and m aint ain a const ant cardiores p i rat or y st atus. These properti es make it an i deal adj uvant especi all y in pat ients with is chemi c heart diseas e.
31
vomiting. Sedat ion caus ed b y dexmedet omidi ne offers additional com fort t o t he pati ent.
Moham ed Ess am Abdel -M eguid, ( 1 9 0 ) in 2013, di d a research to det ermine the effi c i en c y of dexmedetom idine to achi ev e fast tracking and im provement of pos toperat ive pain m anagem ent in pati ents undergoi ng off-pum p coronar y art er y b ypass surger y. 3 0 pati ent s post ed for off -pump CABG were di vide d into 2 groups: Group I were gi ven dexmedetomi dine 0.5 ug/kg/ hour infusi on just aft er the an aesthesi a induction foll owed b y 0.3 ug/kg/hour on shi fti ng to the IC U whi ch was continued up t o 12 hours aft er extubati on. Group II pati ent s were given norm al s aline at a si milar volum e and i nfusion rat e visual analog scal e of 10 -100 was informed well to all t he pati ent s at the tim e of pre-anaesthes ia check -up. Managem ent of Pos toperative pai n was done usi ng morphine. Extubati on tim e and vis ual analog s cal e was not ed ever y t wo hour l y for 12 hours after extubation. In concl usion, dexmedetomidine as an adjunct to an aes theti c m anagem ent of off-pump CABG provides a bett er qualit y of postoperative anal gesi a with opi oid -s paring effect, whil e at achi evi ng the ultim ate goal in managem ent of off -pump coronar y art er y b ypas s whi ch i s fas t tracking of pat ients.
32
dexmedet omidi ne therap y were compared wit h val ues duri ng the init ial hours of dexmedet omidine adminis trat io n. Dexmedetomidi ne i s an att racti ve adjunct drug for treating of severe al cohol wit hdrawal as it is capabl e of providi ng s edation and reduc ing autonomi c h yp eractivi t y with potenti all y decreas ed incidence of respirator y di stress and deli rium than found whil e using benzodi azepi ne. It i s part icularl y useful when the s ym ptom s are refractor y to even hi gh dos es of benzodi azepines, as it acts through pat hwa y independent of GABA. Here, adj unct therapy using dexmedet om idine in pat ients wit h severe al cohol wi thdrawal who were poorl y cont roll ed on, or were experi encing si gnifi cant side effects with traditional treatm ent led t o a decreas e in al cohol withdrawal scori ng, reductions in benzodiaz epine dosing, and decreas es in heart rate and bl ood pr es sure.
33
inci dence of post operative agit ation and shi veri ng al ong wit h hem od ynami c st abili t y and no respirator y depres sion.
SS Harsoor, et al (1993), in 2013, conduct ed a research t o as sess the effect s of i ntra venous dexmedet omidine on s ensory, m otor, haemod ynami c paramet ers and sedati on during subarachnoid bl ock procedures. A tot al of 50 pati ents undergoing infraum bili cal and l ower limb surgeri es under s ubarachnoid bl ock were sel ect ed. Group I received int ra venous dexmedetom idine 0.5 m cg/kg bol us over 10 min before s ubarachnoi d bl ock, followed b y 0.5 mcg/kg/h infusi on throughout t he surger y. Group II recei ved simil ar vol ume of norm al sali ne i nfusion. Ti me for onset of s ens or y and mot or blockade, cephal ad l evel of anal gesia and durati on of anal ges ia were not ed. Sedation s cores usi ng R ams a y S edati on Score and haem od ynami c paramet ers were as sess ed. The stud y concluded t hat i ntravenous suppl em ent ati on of loadi ng dos e of dexmedet omidi ne 0.5 m cg/ kg foll owed b y i n fusi on at 0.5 mcg/kg/h hast ens the ons et of sensor y block and prolongs t he duration of s ensor y block, anal gesia and m otor block wit h l ess er i nci dence of brad yc ardi a. Moreover, i ntravenous dexmedet omidi ne s uppl ement ation duri ng subarachnoid block produces adequat e arousabl e s edation without caus ing respi rator y depression.
34
post ed for el ecti ve surgical procedures bel ow umbi licus under s pinal anaesthesi a were doubl e bli nd divi ded t o one of the three groups. All pati ent s re cei ved 0.5% h yperbaric bupivacaine 2.5 ml s pinal anaesthesi a. Group I Pati ent receiving i ntravenous normal s al ine 10 ml over 10 minut es, 10 minut es before s pinal anaes thesi a with 0.5% h yperbari c bupi vacai ne 2.5 m l and normal sali ne 10 m l over 10 minut es aft er 30 minutes of spinal anaesthesi a. Group II P ati ents were given dexmedet omidi ne 1 μg/ kg i .v. over 10 minut es , 10 m inutes before spinal anaesthesi a. Group III pat ients were gi ven dexmedetomidine 1 μg/kg i.v. over 10 minutes after 30 minutes of spinal anaesthesia. The stud y concl uded that Int ravenous dexmedetomi dine prol onged spinal bupivacaine s ensor y blockade i n both t he groups and al so provided sedati on and additional anal gesi a.
35
intraoperative fent an yl consumption, art eri al bl ood gas anal ys is, plas ma cortisol l evel, tim e for em ergence and t otal recover y from anaesthesi a were recorded. S edati on score was as sess ed at 15, 30 and 60 minutes aft er ext ubation and tim e to complai n pain was recorded. The stud y dem ons trated that dex medetomi dine or esm olol wit h sevofl urane are s afe agents for cont roll ed h ypot ensi on and bot h are useful i n provi ding ideal surgical fi eld duri ng functi onal endos copi c sinus s urger y. Com pared wit h esmol ol, dexmedet omidi ne offers t he benefit of inherent anal gesic, s edati ve and anaes theti c sparing effect.
36
Ust a B, et al ( 1 9 7 ), i n 2011, conducted a s tud y for evaluating t he effect of dexmedetomidine admini strati on on shi veri ng duri ng spi nal anaesthesi a. Sixt y pati ents posted for elective mi nor surg eries under sub arachnoid block with h yperbaric bupivacaine, were selected. The y were gi ven either sali ne or dexmedetomi dine . Mot or block was assess ed. The occurrence of shiveri ng was evaluat ed b y a blinded obs erver aft er the complet ion of inj ection of drug in the subarachnoid space. The y found t hat infus ion of d exmedetom idine postoperativel y causes si gnifi cant reduc tion of shivering associ at ed wit h s ubarachnoid block during m inor s urg eri es wit hout causing an y m ajor side effect. So, the stud y concluded that dexm edetomi dine infus ion is effective for preventi on of shivering and for providin g sedation for patients duri ng subarachnoid block .
37
anaesthesi a care unit were evaluat ed. The y concluded t hat dexmedet omidi ne 0.75 or 1.0µ g/kg i.v. can provide effective proph yl axi s for agai nst post operati ve shi vering as well as an anal gesi c effect. Although pot enti al for i ntraoperative requirem ent for at ropi ne, sedati on i n t he imm ediat e recover y period and dela yed extubation tim e with dexm edetomi di ne was observed, t here were no m aj or clini cal impacts on the overall recover y from anaesthes ia .
38
maint enance of adequate depth of anaesthesi a wit h s table haemod ynami cs .
S S Hars oor, et al , ( 2 0 0 ) in 2014, conducted a stud y for evaluat ing the effect of int ravenous dexm edetomi dine infusion during general anaesthesi a for abdominal surgeries on bl ood gl ucos e levels and on Sevoflurane requirement s during an aest hesi a. 40 pati ents posted for abdominal surger y under general an aesthesi a were divided i nto Dexmedetomi dine group and Placebo group of 20 each. Dexmedetomi dine group were given loading dos e of Inj. Dexmedetomi dine at 1 μ g/ kg/10 minutes dilut ed to 20 ml, fol lowed b y maint enance wit h 0.5 μ g/ kg/ h., till the end of surger y. Pl acebo group received si mil ar volum e of IV normal s aline. An aest hesi a was maint ai ned usi ng nitrous oxide, ox ygen and sevoflurane keepi ng ent rop y bet ween 40 and 60. The stud y concl uded that Dexmedetomi dine as a prean aestheti c medi cation and i ntraoperative infusion was effective in at tenuating m et aboli c stres s respons e to m ajor surgeri es as i ndi cat ed b y s tabl e blood gl ucose l evels . It also reduced intraoperative an aest heti c requi rem ent and had si gnifi cant an aestheti c sparing propert y during entrop y guided general an aesthesi a. Moreover, continuous i ntraoperative admi nist ration of Dexmedetomidine does not affect int raoperative cardiovascul ar st abil it y.
39
50 pat ients posted for lower abdom inal and lower lim b surger y were incl uded. Each pat ient was gi ven 4 ml of 0.75% isobari c ropi vacaine + 5 mi crogram dexmedet omidi ne . Pul se rat e and b lood press ure were recorded at interval s of 1, 2, 5, 10, 20, 30 minute s and 1, 2 and 3 hours. Post operati ve pai n scores were ass es sed using VAS. The pati ent s had excell ent hemod ynami c stabilit y and good pos toperative anal gesi a to t he com bination of ropivacai ne and dexmedetomi dine .
Pri yam Sai ki a, et al,( 2 0 8 ) in 2014 found the us e of dexmedet omidi ne , i n the postoperative managem ent of a trans oral odont oidectom y patient and requi red m echani cal ventilation. Dexmedetomi dine at 0.5-0.7 μ g/ kg/ h was used for post operative managem ent and continued unt il extubation of trachea and provided sedati on l evel of Ri chmond Agi tat ion -S edati on S cal e −1 t o −2. He was easil y arous abl e and co -operat ive duri ng neurologi cal evaluations. Dexmed etomi dine was st opped 22 h after complet ion of surger y. Within 15 min his R ichm ond Agitat ion -S edation S cal e rose t o a score of 0, and t rachea was extubat ed sm oothl y. The y concl uded that dexmedet omidi ne , by its opioid sparing effect and pres erved att enti ve behavior, is a us eful adjunct t o m ulti modal anal gesi c regi men i n postoperative patients who needs s edoanal gesi a for m echani cal ventilation.
40
dexmedet omidi ne and intrat hecal buprenorphine as an adjuvant to 0.5% h yperbari c bupivacai ne for lower abdomi nal s urgeri es. Sixt y pati ent s aged 18 -60 years posted for el ective lower abdom inal surgeri es . The pati ent s were randoml y allott ed to 2 groups for recei ving i ntrathecal 3ml of 0.5% bupivacine with 60µ g of buprenorphine in group I or 3ml of 0.5% bupi v acaine with 5µ g of dexmedetomi dine i n group II. The ons et time t o peak s ensor y level, motor bl ock, duration of mot or block, sedati on, haemod yna mic vari abl es, anal gesi a and an y advers e effects were not ed. The duration of m otor and sensor y block in dexmedet o midi ne group was 413 mi nut es and 451 m inut es whi ch was considerabl y different from 205 mi nut es and 226 m inut es of buprenorphi ne group. Also duration of anal ges ia was 493 m inut es in dexmedet omidi ne group compared to 289 minutes of buprenorphine group. The y concluded that i ntrat hecal dexm edetomi dine 5µ g when com pared to i ntrat hecal buprenorphine 60µ g causes longer duration of sensor y and m otor block. The requirem ent for additional s edation and rescue anal gesi a was l ess i n dexmedetomi dine group and the haemod ynami cs were comparable i n bot h the groups without causing an y si gni ficant si de effects.
41
and 65 yea rs who underwent surgeri es of s pine were divided i nto 2 groups . 1s t group pat ient s were given 20 ml of 0.2% ropi vacaine and 1 μg/kg of dexmedetomidine while 2n d
group were given 20 ml of 0.2% ropivacaine and 2 μg/kg of clonidine via the epidural catheter. Onset of anal gesi c acti on , t ime of peak acti on, duration of anal ges ia, cardiores pi rat or y param eters , requi rement of res cue I.V anal gesi cs and side-effects were noted. The y concluded that the epi dural rout e provided adequate anal gesi a i n spi ne surgeri es i n terms of vi sual analogue s cale s core and overall pati ent satis faction and i t el uded the requi rement of int ravenous anal ges ics i n both groups . Dexmedetomi dine was found t o be a bett er neuraxial adj uvant to ropi vacaine as compared to cl onidi ne for provi si on of earl y ons et and long las ting post-operative anal gesia and st abl e haem od ynami c paramet ers.
42
neuroendocrinal st ress respons e t o s urgi cal t raum a and cardio pulmonar y b ypass and in provi ding adequate pos toperat ive anal gesi a and short tim e t o extubati on.
Li li J iang, et al ,( 2 1 2 ) in 2014, conduct ed a s tud y to invest i gat e whether dexm edetomidine is capabl e of att enuati ng rat pulmonar y dam age induced b y ischemi a -reperfusion injur y, whi ch i s a t ype o f acut e st erile lung injur y. From the study, the y suggested a pot enti al clini cal appli cation of dexmedetomidine for reducing l ung ischemi a -reperfusi on injur y in an experiment al m odel .
43
measured, in dex pulmonar y vas cul ar resistance and i n dex s yst emi c vas cul ar resist ance and cardiac in dex were calcul ated. Each patient was then given a 10 minut e infusion of dexmedetomidine of 1μ g/kg, 0.75μg/kg or 0.5μg/kg. The same measurements and calculations were done agai n at the end of t he infusi on. Initi al l oading doses of dexmedet omidi ne were associ at ed with considerable s ys t emi c vas oconst ri ction and h ypert ensi on, but analogous res pons e was not seen in the pul monar y vascul ature, even in paedi at ri c pat i ents with pulmonar y arteri al hypert ension. The y concl uded that d exmedetomi dine do not s eem to be contrai ndi cated i n paedi at ric pati ents havi n g pulmonar y h ypert ens ion.
44
esmolol and cont rol groups as compared to t hat in dexmedetomi dine group. The y s tat ed that admini strat ion of a si ngl e dos e of dexmedet omidi ne prior to general anaesthesi a i nducti on was an effective met hod for at tenuating t he hem od ynami c res ponse t o t racheal intubati on.
45
Pant D, et al ,( 2 1 6 ) i n 2014 conduct ed a stud y t o compare the effects of sublingual midazol am and dexmedetom idine us ed for prem edi cating children. The st ud y enrol led hundred chil dren of age 1 to 12 years pos ted for orchidopex y, i ngui nal herni a repair or circumcision under general anaesthesi a. The sel ect ed children were divided int o t wo groups of 50 each. P ati ents in group I were gi ven subli ngual mi dazol am 0.25 m g/kg as prem edicati on , whil e thos e in group II recei ved sublingual dexmedetom idine 1.5µg/ kg as prem edi cation . S edat ion was ass essed. The y concluded that s ublingual dexmedet omidi ne offers a bett er preoperati ve s edation compared t o subli ngual mi daz olam in all the age groups and also provides a smoot her i nducti on of anaesthes ia and em ergence parti cul arl y in t he pres chool chil dren.
46
effects were eval uat ed in the perioperative peri od. End-ti dal sevofl urane concent ration of dexm edetom idine group was si gnifi cantl y reduced in 23.8 -67% com pared to s aline group during surger y. Incidence of em ergence agit ation found lower in dexmedetomi dine group t han i n s ali ne group. Postoperative pain was s i milar and discharge tim e did not var y bet ween the gro ups. MAP and heart rate were consi derabl y l ower in dexm edetomidine group during s urger y. The y concluded that infusion of dexmedetomi dine i ntraoperati vel y reduced s evoflurane requi rements and reduced agit ation during em ergence wit hout an y del a y in dischargi ng the paediatri c pat ient s who undergo am bul ator y surger y. Anaest hes iologi sts should be caut ious about brad ycardi a and h ypot ension.
47
induction scores were done. Dexmedet omidine 2 μ g·kg− 1 i .v. given 30 mi nut es before inducti on of anaesthes ia provi ded si gni fi cant att enuati on of increase in m ean art erial press ure caus ed b y i ntubation respons e. Vari ati ons in heart rat e and bi -spectral index also show that dex medet om idi ne prem edicati on causes effecti ve att enuation o f respons e t o int ubati on . Preoperative dexmedet omidi ne 2 μ g·kg− 1 also pro vides optimal -s edation and smoother anaest hesia i nduction. Prem edicati on of dexmedet omidi ne is effect ive i n reducing cardiovas cul ar and arousal res ponses to t racheal i ntubat ion.
48
Sukhmi nder J it Si ngh Bajwa , et al, ( 2 2 0 ) in 2011, conduct ed a stud y for com pari ng the effi cienc y a nd clini cal charact eri sti cs of dexmedet omidi ne and cl oni dine, i n epi dural anaesthesi a wit h special att enti on on thei r s edative properti es and an abilit y for provi ding smoot h int ra-operati ve and post -operat ive pain reli ef. The s tud y was done i n 50 adult femal e s of age 44 to 65 years post ed for vaginal h yst erectom y. The pati ents were divided into 2 groups of 25 patients each. Group I was given 17 ml of 0.75% epi dural ropivacaine and 1.5 μg/kg of dexmedetomidine, whereas group II were given a mixture of 17 ml of 0.75% ropivacaine and 2 μg/kg of clonidine. Onset and durati on of anal gesi a, sensor y and mot or block l evels, s edation and advers e effect s were not ed. The y concluded that dexmedetomidine is a bett er adj uvant for neuraxi al anaesthesi a when compared wi th clonidine for obt ai ning earl y onset of anal gesi a, optimal s edat ion and prolonged post -operative anal gesi a.
49
considerabl y less morphi ne for anal gesia . Cont inuous admini s tration of dexmedet omidi ne throughout the IC U sta y did not affect ox ygen saturation, respi rator y rat e, weaning duration, or tim es t o extubation. Most of t he patient s who received dexmedetom idine could maintai n blood pres sures i n the norm al range, wit hout an y rebound. H ypertension, ri gors and atel ect asis occurred more often i n t he cont rol group, whereas h yp otension and brad yc ardi a were s een more oft en i n the dexmedetom idine group.
All thes e s tudi es l ed to conclusion t hat dexmedet omidi ne a hi ghl y speci fi c al pha2 agoni st drug poss ess es sedative, anxiol yti c,
s ympathol yti c, anal gesi c and h ypnoti c properti es and provi des perioperative haem od ynami c stabilit y.
Ph armacology
Dexmed etomidin e
[image:62.595.216.420.503.626.2]50
Ph ysi coch emi cal Characteri sti cs
Dexmedetomi dine i s the d -enant iom er of m edetomi dine, a subst ance that has been used for sedati on and anal gesi a i n vet erinar y m edi cine for m an y years. It is hi ghl y specifi c for t he α2 recept or ( α2 /α1 200:1), making it a compl et e alpha2 agonist .
Dexmedetomi dine i s included in im idazol e subclass of alpha2
recept or agonists li ke cl oni dine, and i ts st ructure is i llustrat ed in Fi g 1. It is freel y s olubl e i n water .
Preparation of Solu tion
Dexmedetomi dine is avail abl e as 100m cg/ ml. It must be dilut ed in norm al s aline t o achi eve t he required concent rat i on before