EFFICACY OF THREE DIMENSIONAL TITANIUM
MINIPLATES OVER THE CONVENTIONAL TITANIUM
MINIPLATES OSTEOSYNTHESIS IN THE MANAGEMENT
OF ANTERIOR MANDIBULAR FRACTURES
A Di ss ertat ion submi tted
in partial fulf ilment of the requir ements for the degree of
MASTE R O F DENT AL SURGE RY
BRANCH – III
ORAL AND MAXIL LO FACIAL SURGE RY
THE TAMIL NADU DR. M.G.R. ME DI CAL UNI VERS ITY CHENNAI- 600032
ADHI PARASAKTH I DE NTAL COLL E GE AND HOS PIT AL MEL MARUVATH UR – 603319.
DE PART MENT O F ORAL AND MAXIL LO FACI AL SURGE RY CERTI FICATE
This is to certi f y that Dr.M.MAHALAKSHMI, Post Graduat e student (2014 -2017) in the Departm ent of O ral and Maxillofacial Surgery, Adhiparasakthi Dent al C oll ege and Hospi tal , M elm aruvathur – 603319, has done this dissertation titled “EFFICACY OF THREE DIMENSIONAL TITANIUM MINIPLATES OVER THE CONVENTIONAL TITANIUM MINIPLATES OSTEOSYNTHESIS IN THE MANAGEMENT OF ANTERIOR MANDIBULAR FRACTURES.” Under our di rect guidance and supervisi on in parti al fulfi lment of the regul ations l aid down b y the Tam ilnadu Dr.M.G.R M edi cal Uni versit y, Chennai – 600032 fo r MDS., (Branch -III) Oral and Maxillofacial Surgery degree exam i nati on.
Co-Guide Guide
DR.KARTHI KE YAN.,MDS ., DR.GOKKULAKRISHNAN., MDS Professor Professor & HOD
ACKNOWLE DGE MENT
I offer m y ferv ent thanks t o Almi ght y God and m y parent s, for the bl essi ngs showered on me & guidi ng me t hrough ever y st ep.
I am extrem el y i ndebted to Dr.T .Ramesh , MD., Correspondent Adhi paras akt hi Dental C oll ege and Hos pit al, M elm aruvathur, Adhi paras akt hi Inst itute of M edi cal s ci ences , M elm aruvathur for providi ng i nfrast ruct ure &R es ources to perform the m ain dis s ert ati on.
I express m y hum ble gratitude ,sinceri t y& respect t o our est eemed Principal,Prof. Dr.S.Thill ain ayagam MDS. , Adhiparas akthi Dental Col lege and Hospital, M elm aruvathur .
I express m y sincere s olidarit y t o m y est eem ed Guide, Dr.S.Gokkul akri shn an MDS ., Profess or and Head, Department of Oral and Maxillofaci al Surger y, Adhi paras akthi Dent al College and Hospital, M elm aruvathur . I am thankful for his guidance ,constructi ve cri ticism, pati ent heari ng &moral support throughout m y pos tgraduat e cours e& wit hout whi ch this stud y would not have been possi ble.
I am thankful to m y co -guide Dr.M.Karthik eyan MDS . , Departm ent of Oral and M axillofaci al Surger y , Adhiparas akt hi Dent al College and Hospit al , M elm aruvathur , for his const ant support .
I am thankful t o m y teacher Dr.G.S uresh ku mar MDS , Reader Departm ent of Oral and M axillofaci al Surger y , Adhiparas akt hi Dent al College and Hospit al , M elm aruvathur ,for his const ant support.
I am extremel y t hankful to m y post graduates , juni ors &fri ends who have been wit h me t o advi ce &encourage m e.
I dedicat e this work to m y parent s Mr.P.Marudai , Mrs.M.Pappathi and m y hus band Mr.J.Prak ash vad ivelan who have alwa ys s upport ed, encouraged and beli eved in m e ,in all m y endeavours and who so l ovingl y and unselfi shl y cared for me .
DECLARATION
TIT LE OF THE DISS ERTAT ION
Effi cac y of three di mens ional titanium minipl at es over the conventi onal ti tanium
minipl at es ost eos ynt hesi s i n t he managem ent of ant erior mandibul ar
fractures
P LACE OF THE S TUDY Adhi paras akt hi Dent al C oll ege and Hospital, M elm aruvathur – 603319
DUR AT ION OF THE COURSE 3 years
NAME OF THE GUIDE DR.S.Gokkul akris hnan.,M DS NAM E OF C O-GU ID E DR.M .Karthike yan., MDS
I hereb y decl are that no part of the di ss ert ati on will be uti li zed for gai ning financial assist ance or an y promoti on wit hout obt aining prior permi ssion of the Pri nci pal, Adhiparas akthi Dent al C ol lege and Hospital, Mel maruvathur – 603319. In addition, I declare t hat no part of this work wi l l be published eit her in print or in el ect ronic medi a without t he gui des who has been acti vel y invol ved i n dis sert ation. The aut hor has the ri ght to res erve for publis h work sol el y with the permiss ion of the Princi pal , Adhi parasakthi Dent al College and Hospital, M elm aruvathur – 603319
C o - Gu i d e G u i d e & H e a d o f d e p a r t me n t
S i g n a t u r e o f c a n d i d a t e
ABSTRACT
BACKGRO UND:
There are m an y studies in the t reatm ent of m andibul ar fract ures that have been published. The t wo concept of ost eos ynt hesi s are semi ri gi d and ri gid fixation. To overcome the short comi ngs of above techni ques , three di mens ional miniplat es has been em erged. This st ud y was des i gned to evaluat e the effi cac y of 3D tit ani um miniplat e over champ ys mi nipl at e i n ant eri or mandi bul ar fratures.
AI M:
The purpose of t he s tud y was to evaluat e the clinical effi cac y of 3-di mensional tit ani um mini plat es in t he m anagem ent of ant erior mandibul ar fract ures b y pain, occlusal st abi lit y, post operative infection, postop erat ive fragment ri gidit y, wound dehis cence and t he out com es were com pared with that of conventional tit ani um minipl at es
MATE RI ALS AND METHO DS:
RESULTS :
There was si gni ficantl y greater pai n i n Group B pati ents at 1s tweek and 1s t month when com pared to Group A pati ents(Mann -Whitne y U t es t). There was si gni fi cant vari ation in pai n bet ween interval across each cat egori es of Group A and Group B(krus kal -wal lis t est ).The post operati ve infecti on, neurologi cal deficit was stati sti cal l y in si gni fi cant (chi -square t est ).There was no case pres ent ed with wound dehis cence. During post operati ve evaluation occlusal stabilit y and fragm ent ri gidit y were good in all 20 pati ents.
CONCLUS ION:
CONTENTS
S.NO TITLE PAGE
No.
1. INTRODUC TION 1
2. AIM AND OBJ EC TIVES 7
3. GENER AL R EV IEW 8
4. REV IEW OF LITER ATURE 11
5. MATER IA LS AND METHODS 28
6. RESULTS 37
7. DISC USS ION 47
8. CONC LUS ION 56
9. REFERENCES 59
LIST OF FIGURE
FIGURE NO TITLE PAGE NO
Figure 1 Armamentarium 31
Figure 2 Armamentarium 32
Figure 3 3D Miniplates 33
LIST OF TABLES
TABLE NO TITLE PAGE NO
1
Mann- Whitney U test-Comparison Of Pain Score By Visual Analogue Scale In Group A And Group BAt Each Visit
41
2 Hypothesis test summary-Mann whitney u test 42
3 Tabulation Of VAS Score In Individual Visit Of
Each Group (Group A)- Kruskal-Wallis test 43
4
Tabulation Of VAS Score In Individual Visit Of Each Group (Group B)-
Kruskal-Wallis test
44
5 Hypothesis test summary-Kruskal-Wallis test 45
6 Cross Tabulation Of Post Operative Infection In
Both Groups 45
7 Cross Tabulation Of neurological deficit In Both
LIST OF CHARTS
S. NO TITLE PAGE NO
Chart 1 Age wis e di stributi on in Group -A pat ient s 38
Chart 2 Age wis e di stributi on in Group -B pati ent s 39
Chart 3 Compari son of Age distri buti on i n both groups 39
LIST O F ABB REVATIO NS
3D : Three dim ensional
DCP : D ynamic Com press ion Pl at e EDCP : Eccentri c Com pression Pl at e IAN : Inferior alveol ar nerve IMF : Inter Maxill ar y Fixation
Introduction
1
INTRODUCTION
Traum a is defined in general as “a phys ical force t hat res ults in injury”. Injuries to the maxillofacial region are clinically highly
si gni fi cant as the y affect both functi on and estheti cs. There i s oft en a ps ychol ogi cal as pect associ at ed wit h t he injur y s econdar y to pati ents concern regardi ng perm anent s carring and subs equent facial disfi gurement.
Fractures of m andibl e are most common bone inj uri es becaus e of its anatom ical promi nence and exposed position i n t he faci al skel et on, accounti ng for 23% - 97% of all faci al fract ures . The mos t common mechanism s of inj ur y to mandible include m otor vehicl e crashes , interpersonal viol ence, and sport injuries. The bod y and post erior region of t he m andi ble are more prone for fract ures.
Introduction
2
fixation b y st rips of Carthagini an l eather gl ued to the skin and the ends were ti ed over the skull.
About 500BC, the In dian surgeon Sushruta wrot e a treatm ent o n operations. He has recomm ended usi ng com pli cated bandagi ng and bam boo spli nts covered wit h a mixture of fl our and glue that were applied under the chin to imm obiliz e t he fract ures for fractured j aws.
During the period of 12t h to earl y 18th centur y , t he barber surgeons us ed the cl assi cal t reatm ent of fractures. Aft er manuall y reset ting the fract ured jaw, ensuring t hat t he norm al occl usion was maint ai ned , and t he mandibl e was im mobilized b y bandages. Various modi ficati ons of bandages were used to im mobilize the lower j aw b y bindi ng it to the upper jaw wit h a bandage that pass ed under t he chi n and over t he head.
The 18th centur y s aw a more s cienti fi c approach em erged in medi cine as a result of advances i n t he knowledge of anatomical and ph ysi ologi cal processes . The new era of s ci entifi c dent istr y was ushered in b y the publi cat ion of a book in 1728 b y Pi erre Fauchard, entit led Traite de chirurgi edent ai re. He i s credit ed with nam e of bei ng the “Father of modern dentistry”. At the turn of the 19th ce ntury, there
Introduction
3
mat eri al s facilit ated the construction of dental s plin t s. These were t he dom ains of the dent al surgeon. Man y refinem ents were int roduced b y improving i nt raoral and extraoral s plint s or the us e of eit her t rans -mandibul ar or circum -m andibular wire fixation to i mmobilize t he mandibul ar fracture directl y or indir ectl y.
In 1826, R odgers di d the first open reductions. He i nsert ed wire sutures i n a cas e of pseudart hrosis of the hum erus . Baudens i s credi ted with bei ng the pi oneer of wiring m andibular fractures, in t he as earl y as 1840 he us ed circumferenti al wire s t o imm obiliz e an obl ique fracture. Soon aft er (1847), Buck has im plied m ethod of drill ing holes in adj acent segm ents and wi ring them t ogether and appli ed wi re s utures directl y to t he fractured bone . Modi fi cations of this technique b y using two doubl e w ires (R os e) and t he fi gure -of-ei ght wire suture (Raas) improved s tabilit y. In 1866, Thom as Gunning des igned the „Gunning splint‟. In 1871, London dentist Gurnell Hammond developed
Introduction
4
Modern t raum atol ogy start ed wit h the devel opm ent of Ost eos ynthesi s. Ge nerall y, m andibul ar fractures are treat ed s urgi call y, either b y ri gi d or semi -ri gid fixati on. Thes e two techniques t hat refl ect almost opposit e concept of m andibul ar osteos ynt hesis. Ri gid fixation is prom ot ed b y t he Arbeit s gemeins chaft fur Ost eos ynthes efra gen (AO) / Associ ati on for t he Soci et y Int ernal Fixation (AS IF). In thi s concept, com press ion, t ensi on, torsion and shearing forces, which develop under functi onal loadi ng, are neutraliz ed b y thick sol id pl at es fixed b y bicorti cal s crews. Dynamic C ompressi on Plating (DCP) and Eccent ri c D ynami c C ompressi on Pl ating (EDCP) pl ates were us ed in t his concept .
Minipl at e ost eos ynt hesi s h ypot hesis was fi rst i nt roduced b y Michel et et al. in 1973, and in fut ure devel oped b y Champ y and Lodde in 1975. The Champy‟s method of semi rigid fixation uses easily bendable monocortical mini plate along an „ideal osteosynthesis line‟.
The developi ng forces are neut ralized b y masti cat or y force t hat produces a nat ural st rai n of compression along the lower border of the mandibl e. Above two t echni ques are ass oci at ed wit h dis advantages , of those s emi - ri gid fixation is a doubt whether thi s fi xation is suffi ci entl y st abl e for fractures t hat cannot be adequat el y reduced.
Introduction
5
s yst ems are avail abl e, rangi ng from the heav y compression plat es t o low profil e plates for midfacial fixation. The thi ckness of plat es ranges from 0.5 to 3.0mm and are m ade ei ther of st ainl es s st eel , vit allium or titanium. Ver y R ecentl y, biodegradabl e, s el f -reinforced pol yl act ide plat es and s crews have been us ed for the internal fixati on of fractures of t he m andibl e with good results. A m ajor breakthrough in t his fiel d was achi eved when "Mosthafa Farm and in 1992 devel oped a new minipl at e s yst em which t akes advant age of the biogeometr y t o provide stable fixati on and he called it a 3 -di mens ional pl ati ng s ys tem. The concept behin d thes e pl at es is t hat of a geom et rical l y clos ed quadrangul ar pl at e, secured with bone screws creati ng stabi lit y i n all three dim ensi ons . C oncurrentl y, changes in m at erial s and desi gns used for plat es and s crews have al so occurred at a st aggering rate. Depending upon the indi vidual m anufacturer's dis creti on, di fferent s yst ems with di fferent m et als have been us ed t o make plat es and screws. The preference t o us e tit anium i n the m anufacture of 3 -D pl at es was obvious due to i ts excell ent properti es li ke res ist a nce to corrosion, good bi ocompatibilit y, pliabilit y and art i fact free im ages in CT s cans and MR I s cans .
Introduction
6
stabilit y in three di mens ions of the fracture s ite si nce it offers good resist ance agains t torque forces.
The aim of thi s stud y was to use the 3 -D t itanium pl at es and screws as per the specifi cations of Mos t afa Farm and. The 3 -D pl ati ng was perform ed i n10 pati ent s wi th ant erior m andi bul ar traum a and 10 pati ent s wit h conventi onal tit ani um minipl at es. This stu d y was to evaluat e t he cl ini cal efficac y of 3 -dim ensi onal t itanium minipl at es over t he conventional tit anium m inipl at es b y pain, occl us al stabilit y, posts urgical infecti on, post operati ve fragm ent ri gidit y, wound dehiscence, neurologi cal defi cit and the outcom es will be com pared with that of conventi onal tit ani um mi nipl at es .
Aim and Objectives
7
AIM AND OBJECTIVES
1. To evaluate the clinical efficacy of 3-dimensional titanium miniplates in the management of anterior mandibular fractures by pain, occlusal stability, post operative infection, postoperative fragment rigidity, wound dehiscence, operative time and the outcomes will be compared with that of conventional titanium miniplates
2. To discuss about various advantages and disadvantages of three dimensional titanium miniplates in Anterior Mandibular Fractures.
3. To emphasize on a simple and less time consuming technique in Semi Rigid Internal fixation of symphysis and parasymphysis region.
4. To realize the importance of shape and design (Architect) of the three dimensional plate and the role it plays in the stabilization of mandible and comparing with conventional titanium champy’s miniplates.
General Review
8
GENERAL REVIEW
The goal of mandibul ar fract ure i s to reest abli sh normal occlus ion and masti cator y function wi th minim al complications (Gerlach et al., 2007). C onservative m anagem ent was the earl ier option for immobiliz ation of the m andi bl e. it has been achi eved b y dental wi ring, arch bars, cap s plint s and gunni ng s plint s . later surgical t reatment has been developed i n the t reatm ent of mandibul ar fractures both i ntra oral or extra oral l y with transoss eous wiring[schwenzes 1982],l ag s crews[nider dellmann 1982],or bone pl at es [schilli 1975,spi essel 1976].
In open ost eos ynthes is technique ,there was a t rend change from ri gi d fixati on in 1968 t o sem i ri gi d fi xation in 1973. Mi nipl ate osteos ynthesi s was fi rst introduced by Mi chel et et al in 1973, Michel et has st art ed experimenting with monocorti cal non – com press ion miniplat es. he has used small ,easil y bendable,non com press ion mini pl ates anchored with m onocorti cal s crews for the treatm ent of t he m andibul ar fractures.
General Review
9
to obt ain optim al fix ation and st abilit y. Thes e pl at es were sm all and screws are m onocort ical to avoid inj ur y to inferior al veol ar nerve and dentit ion.
3D minipl at es concept was first developed b y Mos tafa Farm and in 1992 . According to Farmand 3D pl at es res embl es geom et ricall y clos ed quadrangular secured wit h bone s crews so that st abili t y can be achi eved b y its confi gurati on t hrough t he t hi ckness can be reduced t o 1mm . The 3D plates are desi gned b y l arge free areas bet ween the pl at e arms and minimal diss ection i s needed for thes e plat es so that blood s uppl y to the bone i s not com promis ed.
General Review
10
Titanium is t he metal of choi ce for fix ati on pl at es since it is the most biocompati bl e implant mat eri al. i t has the minim al advers e reactions, the i ndi cat ion for removal of t he tit anium minipl at es can be defined by individual patient’s complaints.
Revi ew Of Lit erat ure
11
REVIEW OF LITERATURE
Maxi me Champy et al (1978)1 used modified Mi chel et 's (1973) techni que of m andi bular ost eos ynt hesis, whi ch consi sts of m onocort ical juxta-alveolar and s ub -api cal ost eos ynthesis , wit hout com pression and without i nter maxillar y fixati on. Thi s t echnique can be us ed in m an y t ypes of mandi bul ar fracture, si ngl e or m ultipl e, ass ociat ed or isolated, except in the case of a fracture of t he cond yl ar neck and i n t he pres ence of pre-exist ing i nfection.
K.Ikemu ra et al (1984)2 performed biomechani cal tests in 18 adult mal e m ongrel dogs in order t o com pare ri gidit y of the fixation and result ant bone healing of m onocorti cal versus bi corti cal ost eos ynthesi s. The biom echani cal tests reveal ed t hat bicorti cal ost eos ynt hesi s was superi or t o mono cortical in t he ri gidit y of the fixation. However, the results during removal of the pl at e at 14 weeks post operati vel y s howed that there was no apparent di fference bet ween the two. The y suggest ed that monocorti cal osteos ynthesi s is useful in t he t reatment of mandibul ar fract ures, except for fract ures wi th bone defects and commi nut ed fract ures.
Revi ew Of Lit erat ure
12
immediat e reconstruction foll owi ng rem oval of m andibular tumours. Main advant ages wit h cham p y pl at es are the y are sm all, fl exible, easil y adapt abl e and monocorti cal s crews al low them for rapi d surgi cal applicati on.
J.I.Cawood et al (1985)4 evaluat ed mini plate os teos ynthesis b y com paring mini pl ates vers us interm axillar y fixation. He obs erved that the rate of compl ications like m alocclusi on, i nfection , sens or y disturbance were hi gher in t he mi nipl at e group but the minipl at e group had an advant age of earl y recover y of norm al jaw opening and bod y wei ght .
Ikemura et al (1988)5 us ed mi nipl at es i n the t reatment of 66 pat ients with facial bone fract ures. I n si mpl e fractures of the dentulous mandibl e, monocort ical ost eos ynt hesis was perform ed. Extensi ve fractures wit h marked displ aced fragm ent s were treat ed with bicorti cal osteos ynthesi s us ing pl ates. The y report ed compli cations li ke wound dehiscence and pla te expos ure in fi ve pat ient s, one pati ent devel oped a gi ngi val abs cess and two patients report ed with m alocclusi on.
Revi ew Of Lit erat ure
13
tolerated i n infect ed lines if the m ain pri ncipl es (proper curettage, ri gi d os teos ynthesis and speci fic antibi oti cs ) are fol lowed.
Gregory Arthur & Berardo et al (1989)7 gave a sim pli fied method of maxillo-mandibul ar fixation. The y i nt roduced the use of bone screws for achieving int erm axillar y fixati on. According to them, t hi s met hod could be us ed as the sole m eans of fracture treatm ent. Thus i n the earl y and mi d 20th centur y, interm axillar y fi xation met hods becam e ver y popul ar and universall y accepted treatment m odalit y of fractured mandibl e.
W.R.S mi th (1991)8concl uded that the com plicati on rat es of dela yed osteos ynthesi s were similar to t hos e of earl y ost eos ynt hesis. He bas ed his fi ndi ngs on a ret rosp ective stud y of 51 fract ured mandibl es. However, the cont rovers y of compression and non - compressi on methods of fixation did not resol ve.
M. Farmand (1 993)9 developed a new t ype of pl ating s ys tem cal led as a 3 dim ensi onal pl ating s ys t em whi ch was us ed fo r 3-5 ye ars in 140 pati ent s in m axillo faci al surgeri es. He concluded wit h bet ter result s than the other s ys t em and t he compli cati on rat e was al so ver y low.
Revi ew Of Lit erat ure
14
pulmonar y function. Minipl at es are consi dered t o be the best treatm ent for pati ent s with maxillofaci al fract ures.
Seiji Nakamu ra et al (199 4)1 1 conduct ed a stud y over pos toperative com plicati ons of del a yed osteos ynthesi s with st ai nless st eel mini pl at es in 110 pat ients with mandibul ar fractures. In 91 pati ents t he y rem oved plat es once suffi ci ent bon y uni on was obtained, heali ng condi tions and surroundi ng tis sues were exami ned and the y didn't show any s erious problems. So short t erm ret ention wi th m inipl at es will be effective and suit abl e for osteos yn thes is of mandibul ar fractures.
Joerg Wi ttenb erg (1994)1 2 evaluat ed the three -Dim enti onal pl ating s yst em for t he fixat ion of mandibul ar angl e fract ures. He concluded that 3 -D pl at e provided an adequat e st abili t y for mandibular angl e fracture with a reasonable level of s ucces s.
Revi ew Of Lit erat ure
15
M.A. Ku riakose et al (1996)1 4 conduct ed a st ud y to compare th e internal fixati on of mandibul ar fractures using eit her ri gi d 2.7m m AO/ AS IF pl ates or mini -pl ates over a three year period. The y concl uded that bot h plating s yst ems were success ful in restoring functi onal occlusion. Ri gid pl at es required an extra -oral approach wit h the risk of faci al nerve dam age. Inci dence of i nfection and pl at e rem oval was hi gher wi th mini plate. A bett er t reatment outcom e for angle and com minuted fractures was observed wi th ri g i d plat es .
Revi ew Of Lit erat ure
16
J.Tames et al (1996)1 6 conduct ed an i nvitro three dim ensional studi es of loads acros s t he fracture for di fferent fract ure sit es of m andible. In a three dim ensi onal model, bending a nd torsi on mom ent s and s hear forces were compared for five m andi bul ar fract ures in angl e, post erior bod y, anterior bod y, canine and s ym phys is region. The y c oncluded mandibul ar fractures can be divi ded i nto 2 groups wit h one group consisti ng of angl e and po st eri or bod y fract ures, ot her group cons ists of ant eri or bod y, cani ne and s ym ph ysi s fracture with sim ilar load patt erns acros s the fracture.
Revi ew Of Lit erat ure
17
A.M. Ford yce et al (1999)1 8 conduct ed a ret rospecti ve s tud y and report ed t hat i ntermaxillar y fix ation was not usuall y necess ar y t o reduce m andibular fractures. Sixt y -six pati ents had t heir fractures reduced manuall y to obt ai n anat omi cal reduction wit hout t he us e of intraoperative IM F. Fort y-ni ne were treat ed conventi onall y using intraoperative IM F. The t wo groups were broadl y simil ar in severit y and t ype of fracture. IM F was not used routinel y post operati vel y. Overall there were si gni fi cantl y fewer oc clus al dis crepanci es i n the earl y post operati ve period in t hose pati ents t reat ed b y anatomi cal reduction (6/66 com pared wit h 16/ 49, P = 0.002) but there was no difference i n t he fi nal outcome of the occl usion between the t wo methods of reduction.
Rob ert. H.Mathon g et al (2000)1 9 conduct ed a retrospective st ud y t o revi ew of non union of m andibul ar fract ures from 1994 to 1998. Th e adequac y of reducti on and appropriat eness of t his fixation techni que were evaluat ed b y anal ys is of pos t -operative im aging studie s. In 906 pati ent s with 1,432 mandibul ar fractures, there were 25 nonunion com plicati ons . The y concl uded that incidence of non - uni on appears to be unchanged overti me regardl ess of varied and advanced m ethods of fixation and reduction.
Revi ew Of Lit erat ure
18
treat ed b y MM F and 20 b y R IF. Opti cal densit y of the bone arou nd the fracture l ine was as sess ed and concluded t hat use of R IF resul ts in more rapid bone mineraliz ation.
Ashraf F. Ayoub et al (2003)2 1 conduct ed st ud y to com pare dimac wires with arch bars for IM F. The y st at ed t hat m ean tim e required for the appli cati on of di mac wires was s i gni ficantl y l ess than that of arch bar. Needl e sti ck i njuries were si gni fi cantl y l ess with di mac wi res. Oral h ygiene m aint enance will be diffi cult with arch bars and t here will be peri odont al dam age.
Marisa A.Cab rini Gab ri elli et al (2003)2 2 revi ewed the us e of 2.0mm minipl at es for t he fi xation of m andi bul ar fract ures . 191 pati ents who experi enced a t ot al of 280 m andibul ar fract ures that were treated with 2.0mm mi nipl at es were reviewed. Mi niplat es were used i n the s am e positi ons des cribed b y AO/ AS IF. No int erm axill ar y fixati on was used. The overall incidence of compl icati ons, incl uding infections was similar to t hos e described for more ri gid methods of fixation.
Revi ew Of Lit erat ure
19
concl uded that open reduction and int ernal fix ation, fracture displ acem ent of 5 mm or m ore, and a normal preoperat ive IAN neurosensor y ex ami nati on were ass oci at ed wi th an i ncreas ed risk for det eriorat ion of the IAN neurosensory s core aft er treatment of mandibul ar fractures .
Fabio Rocci a et al (2005)2 4 carri ed out stud y over t he int ermaxillar y fixation using i ntraoral corti cal bone screws. Sixt y -t wo pati ents with mandibul ar fract ures, t r eat ed b y i nt ermaxillar y fixation using thes e screws, were evaluat ed. C ompli cations li ke i at rogeni c dam age to dental root s (1.5%), 4.9% of t he screws were covered b y oral mucos a and 1.9% were lost . M al occlus ion was observed in one patient (1.6%) and lack of consoli dat ion of a di spl aced fract ure of the m andibul ar bod y i n another pati ent.
Andrew JL et al (2005)2 5 conduct ed a s urve y to s uggest an evolution in the management of m andibul ar angl e fractures. Accordi ng t o them, onl y six percent (6%) of surgeons pr eferred the us e of 3 -D plates i n angle fracture. Thes e unique plat es are com pos ed of l inear, square or rect angul ar unit s and ma y theoret icall y provide increas ed torsi onal stabilit y. The y t ypi call y us ed this pl at e i n s ym ph ys eal/ paras ym ph ys eal fractures, wh i ch are under a great degree of t orsional strain t han other areas of m andi bl e.
Revi ew Of Lit erat ure
20
Claud e et al (2005)2 6 carried out a retros pecti ve evaluati on of 37 pati ent s wit h non -comminut ed m andibular angl e fract ures fixat e wit h transorall y pl aced curved 2.0 -mm 3 -dimensional st rut pl at es. Two pati ent s devel oped infecti ons requiri ng plat e removal and re -applicati on of f ixat ion. Bot h of t hes e pati ent s had a m olar i n the fracture line that was l eft i n pl ace during t he fi rst operat ion. One pati ent developed a mucos al wound dehiscence without consequence. The y concluded that this pl at e i s low in profil e, strong yet mall eabl e , facili tat ing reduction and stabiliz ation at both t he s uperior and inferior borders . The infecti on rat e of 5.4% found in t his s tud y com pares favourabl y with t hat seen wit h reconst ruction plates
R. Mukerji et al (2006)2 7 had done a hi stori cal pers pecti ve stud y on princi ples of the t reatm ent of m andibul ar fractures from t he anci ent period to the recent past . Spl inting of t eeth is an ol d wa y of immobili sing fractures but modern biom at eri als has changed clini cal practice towards pl at ing the bone and earl y re storation of function. He pres ent ed a bri ef hi stori cal overview of techniques and s ys tems that have been used for st abili sation of m andi bul ar fract ures .
Revi ew Of Lit erat ure
21
age and gender, severit y and t ype of ori ginal t raum a, and fracture sit e, soci al , economic and cultural factors in china.
Alkan. A et al (2007)2 9 evaluat ed the biomechani cal behaviour of different mini plate fixation t echniques for the t reatm ent of fractures of the m andibular angle. Twent y sheep hemi -mandi bles were used t o evaluat e 4 di fferent plating t echniques. The groups were fixed with Cham p y's t echnique, bi pl anar pl at e placem ent, monopl anar pl at e placement, and 3 -di mens ional curved angl e st rut plat e pl acement . The biom echani cal behaviour of t he groups for the forces (N) that caus ed displ acem ent of 1.75mm was compared using the Instron software program and di spl acem ent graphi cs . The stud y demonst rat ed that 3D strut pl at e's t echni que had great er resist ance t o com p ress ion l oads t han the Champ y's t echni que.
Revi ew Of Lit erat ure
22
Hasan hu snu kork maz (2007)3 1 had done a st ud y b y fi ni te elem ent model t o form ulat e biochemi cal j usti fication for st abl e fixation on a fractured m andi bl e. Minipl at es were investi gated and recomm endati o ns were made about locations, ori entat ion, t ype, selecti on, number, positi on and t ype of plat e s yst em . Longer pl at e in s uperi or position and shorter plat e i n inferior position produced a more st abl e condition. In the st ud y, resul ts were obt ained on t he ch oi ce of parti cular size, thickness , desi gn or confi gurati on for applicati on.
J. Zi x et al (2007)3 2 conduct ed a stud y t o evaluate the us eful nes s of 3 -D mini plate for open reduction and monocorti cal fi xation of mandibul ar angle fractures. The m ean operati on tim e from i ncis ion to wound closure was 65 minut es. Two patient s had a mucos al wound dehiscence with no cons equences . None developed an infection requi ring a pl at e rem oval. The y concl uded t hat t he 3 D pl ating s ys tem i s suit abl e for fixati on of sim ple m a ndibul ar fractures and i s an eas y t o use alternati ve to conventi onal mi niplat es . 3D pl ating ma y be contraindi cat ed in pati ents in whom i nsuffi ci ent int erfragm entar y bone contact caus es minor stabilit y of fractures .
Revi ew Of Lit erat ure
23
for count eracti ng t he torque forces, and operative tim e is l es s becaus e of simult aneous st abilization at both superior and inferi or borders.
P.D.Rib ei ro -juni or et al (2010)3 4 evaluat ed t he convent ional and locking mini plat e/ screw s ys t em for t reatment of m andibular angl e fracture t hrough an i nvit ro stud y. 60 pol yurethane hemi m andi bles were assi gned int o 4 groups. In group 1 and group 2, t wo conventional G1 and locking G2 s crews and mini plates were installed. The hemi mandibl es were loaded i n compressi ve s trength until a 4m m displ acem ent was obs erved bet ween the segm ents vert i call y or horizont all y. The y concl uded locking plat e/s crew s yst em s provi de greater resi stance t o displ acement, long l ocking mi nipl at es provide greater s tabilit y than short ones.
Revi ew Of Lit erat ure
24
L. Gandi et al (2012)3 6 conducted a stud y t o evaluat e effi cac y of three dimensional (3 -D) tit ani um mini pl at es in the m anagem ent of mandibul ar fractures in 20 pati ent s over a period of 2 yrs prospect ivel y. Finall y the y concluded because of t he clos ed quadrangul ar geomet ric s hape, and t he ease of contouring and adapting to bon y fragm ent s, 3 -D tit anium minipl at es provide good st abiliz ation of fractured fragm ents in th ree dim ensi ons.
Gau rav et al ( 2012) 3 7 conduct ed a prospect ive cl ini cal trial st ud y. The y concluded that three dim ens ional pl at es st abilize the bone fragm ents in three dimensions because of t he closed quadrangul ar geomet ri c s hape, and the e ase of cont ouri ng and adapting.
Y.Gu ruprasa et al (2012)3 8 conduct ed a st ud y over 3 -D tit anium minipl at es in m anagem ent of m andibul ar fractures. The y concl uded that t hree dim ensi onal pl at es st abil ize the bone fragm ent s in three dimensions. Due to bett er st abil it y IMF is not necess ary, t hereb y enhanci ng the overall com fort, convenience and wellbei ng of the pati ent s. As tit ani um is most biocompati bl e mat eri al secondar y operative procedure for pl at e removal may not be necess ar y .
Revi ew Of Lit erat ure
25
minipl at es. It uses l ess er forei gn m ateri al, reduces the operat ion ti me and overall cost of t he treatm ent.
Mahamoud E.Khal i fa et al (2012)4 0 conduct ed a com parati ve st ud y over 3 -D t itanium plat es versus conventional tit anium mi nipl ates in fixation of anterior mandibul ar fractures . Intraoperativel y durat ion of surger y was m easured from the tim e of i nci sion till the closure of wound. Subs equent postoperative clini cal follow up for m al occlus ion, neurosensor y defi cit , wound breakdown, infecti on and presence of malunion/ non -union was performed. P ostoperative radi ographs were taken t o assess the gap bet ween fracture s egm ent s. Al l pati ents were foll owed up clinicall y and radi ographi call y for 6 months postoperativel y. Fi nall y, he noti ced t hat the 3D minipl at e s ys tem is a bett er and easier m et hod for fixati on of m andibul ar fr act ures , com pared to the conventional mini -pl ate. But there is a limit ation to us e in cas es of oblique fractures and t hos e invol ving t he m ental nerve as well as there is exces sive im plant m at eri al because of the extra verti cal bars.
Naresh ku mar e t al (2012)4 1 conducted a st ud y of tit anium mini plate osteos ynthesi s of mandibul ar fractures. The y concluded that t he titanium miniplat e and s crew s yst em exhibits good s trength, negli gible com plicati ons ,excell ent biocom patibili t y and good resul ts
Revi ew Of Lit erat ure
26
B. Pawan ku mar et al (2012) 4 2conduct ed a C omparati ve stud y of three dim ens ional s t ainl es s st eel pl at e versus s tai nl ess s teel minipl at e in t he m anagem ent of mandibul ar paras ymph ysi s fract ure. The y concl uded that the fi xation of m andibular fracture wit h 3D plates provides three dim ensional st abil it y and carries l ow morbidit y and infection rat es. The onl y probable limit ation of thes e pl at es ma y be excessive im plant m at eri al due t o the ex tra verti cal bars incorporat ed for countering the t orque forces and in cas es where t he fracture line pas sing through the ment al foramina regi on.
Sadhasivam Gokkul a Kri shnan et al(2012)4 3 conduct ed an anal ys is stud y of post operat ive com pli cations and effi cac y of 3D miniplat es in fixation of mandibul ar fractures.The results of this prospect ive st ud y showed t hat 3D ti tanium mini pl ates were effecti ve i n t he t reatment of mandibul ar fractures and overall compli cation rat es were l ess er.
Revi ew Of Lit erat ure
27
E.A .El morass i et al (2014)4 5 conduct ed a stud y of Three-dimensional versus standard mi nipl at e fixation in the managem ent of mandibul ar angl e fractures: a s ystemati c review and m eta-anal ys is. The result s of t his m et a -anal ysis s howed l ower post operative com plicati on rates with the use of 3D mi nipl ate fixati on i n compari son with the use of s tandard mini pl ate fixation in the managem ent of mandibul ar angle fractures.
Materials and Methods
28
MATERIALS AND METHODS
The stud y conduct ed is a Prospective, R andomiz ed clinical in vi vo stud y on pati ents att endi ng the Departm ent of C asualt y i n
Melm aruvathur Adhi parasakthi Inst itut e of M edi cal S ci ences and in Departm ent of Oral and Maxill ofacial surger y, Adhi paras akt hi Dent al College and Hospital, Mel maruvat hur, Tamil nadu with ant erior
mandibl e fractures . Ethi cal cl earance for the stud y was obt ained from the Instit ution al review board, APDC &H (R eference No: 2014 -M
D-BrIII-S AD-06). All the s ubj ects part icipat ed in the st ud y were inform ed about the nat ure of the stud y and all t he parti cipants si gned an informed consent form.
Tot all y 20 pati ent s wit h Ant erior M andibular Fra ctures were sel ected according to inclusi on, exclusi on crit eri a.
SOURCE O F DAT A
Pati ents s eeki ng treatm ent for Ant erior M andibul ar Fractures
reporting to Depart ment of Oral & M axillofacial Surger y, Adhi paras akt hi dental college and hospit al, M elm aruvathur, Tamilnadu
METHO DS O F DATA COLLECT ION
All 20 pati ents had undergone Open Reduction and Int ernal Fixati on (OR IF) under General Anesthesia for t reat ment of Ant erior
Materials and Methods
29
All patients in age group of 18 -60 yea rs Mandi bul ar fractures invol ving S ymph ys is & Paras ym ph ys is regi on.
As per surgical pri nci ples all pati ent s underwent preoperative
evaluati on i n the foll owing aspects Cas e histor y
Clinical examination
Radi ologi cal exami nation
Hem at ologi cal eval uation
S ys temic evaluation
Pati ents were evaluat ed preoperativel y, i nt raoperati vel y and postoperativel y for vari ous param et ers. Pre operati ve and post
operative orthopant omogram (OPG ) was considered mandat or y to check for preoperati ve dis pl acem ent of fract ured s egm ent s and also for adequac y of post operati ve reduction and fixation. Al l pati ents were
foll owed up for a minimum of 6 m onths post operativel y. P ost operative clinical evaluation will be done at imm ediat e post operative,
1s t week, 1s t m ont h, and 6n d month respectivel y.
PL ATE DESI GN
Materials and Methods
30 MATE RI ALS
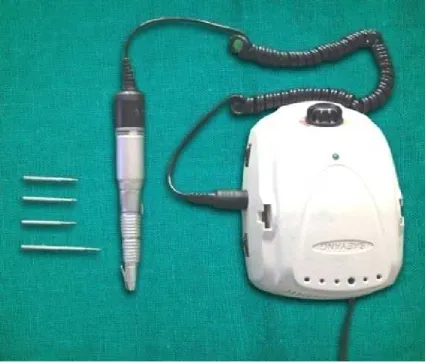
1. Arm am ent arium for surger y(Fi gure 1&2)
2. Three dimensi onal ti tani um mi ni plat es and s crews (Fi gure 3 )
3. Conventi onal C ham py’s mini pl at e (Fi gure 4)
1. Plates
a. C ompositi on : Tit ani um (Grade 2) N - 0.03%
C-0.10% H- 0.015%
Fe - 0.03 % O - 0.25 %
Titanium (R est ) %
Four hol e tit anium three dim ensi on pl ate Length of the pl ates : 9mm
Breadth : 9mm Thi cknes s : 2mm 2. Screws
a. T ype : Non compres sion, mono cort ical s crews with hexagonal head
Materials and Methods
31
ARMAME NTARI UM
[image:43.595.92.527.209.522.2]Materials and Methods
32
ARMAME NTARI UM
[image:44.595.84.511.183.546.2]Materials and Methods
33
3D miniplates u sed in group A p ati en ts
Fi gure 3
Champ y’s miniplate used in Group B patien ts.
[image:45.595.195.406.127.274.2]Materials and Methods
34 STUDY VARIABLE S
Stud y vari abl es incl uded careful pre -operati ve, int ra -operat ive
and post-operati ve asses sm ents .
Pre-op erati ve Ass es s ment
T ype of fract ure & associated faci al i njuries.
Fracture displ acement in terms of Mi ld/ Moderat e/ S evere.
Occlusal evaluation.
Intraop erative Ass ess ment
Adequac y of exposure.
Plat e adapt ati on i n t erm s of Good/ S ati sfactor y.
Plat e handling tim e.
Stabili t y of fract ur e fragm ent.
Pos t op erative Ass ess ment
Pain, Parest hesia, S wel ling
Wound dehis cence, Infection
Fragment stabilit y
Occlusal int egrit y
Malunion/ nonunion
Neurological defi cit
O PERATI VE MANAGEME NT
Of tot al, 20 pati ents were operat ed under General Anest hesia.
Materials and Methods
35
placed in al l pati ent s. Face preparati on was done usi ng P ovidone -Iodi ne. St andard draping procedure w il l be carried out.
Int ra oral sit e was prep ared using 5% Povidone - Iodi ne sol uti on.
Infilt rat ion of l ocal anest het ic (2% l ignocaine wi th 1: 2,00, 000 Adrenal ine) will be gi ven l aterall y on both sides of t he fracture sit e. Two t ype of Incisi ons were us ed to approach the fracture sit e,
curvol inear i ncision for 12 pati ent s, vesti bul ar incision for 8 pati ents .
Ful l t hi cknes s mucoperios teal flap was elevat ed and rais ed t o expos e t he fracture site. Aft er adequate exposure, fracture segm ents was manipulat ed and reduced t o att ain t he norm al anat omi c positi ons
for fixation. After m anual reducti on IM F was done with ideal occlus ion.
Aft er achi evi ng adequate reduction & IMF, Three Dim ensi onal Minipl at e (10 cas es ) and champ y's conventi onal mini plate ( 10 cas es )
was adapted to fit onto the cont our of M andibl e. Bur hol es was drill ed usi ng st andard TC burs of si ze 702 under copi ous s ali ne
irri gation. S crews were ins erted to st abil ize t he pl at es i n pos ition.
Fol lowing adequat e fixation, sit e was i rri gat ed wit h bet adi ne and
sali ne. Aft er achi evi ng hemostasis, wound cl osure was done using 3 -0 vicr yl s utures. IM F was rel eas ed, occlusi on and int ra operative
Materials and Methods
36 Pos top erati ve Drugs
Inj ection Taxim (Cefotaxim) 1 gm I.V (twice dail y)
injecti on Met ronidaz ole 500m g I.V (t hri ce dail y)
Inj ection Voveran (Diclofenac) 75 m g I.M (t wice dail y)
Resul ts
37
RESULTS
This s tud y was done in the Departm ent of Oral and Maxillofacial
Surger y, Adhi paras akthi Dent al Coll ege, M elm aruvathur wit h a sample size of 20 pat ient s with m axillofacial t raum a.
Stud y subj ects were divided int o t wo groups.
Group A - OR IF wit h 3D tit ani um mi nipl at es Group B – OR IF wit h conventional mini plat es
The operat ive procedure -Open reducti on and i nternal fixat ion
was perform ed under general anaesthes i a (OR IF) to the selected subj ects.
Fol low -up was done in ea ch group and were ass ess ed for
Pain -b y vis ual analogue s cale
Post-surgi cal infecti on -b y clinical as sess ment of fever, s welli ng,
pus dis charge
Fragment stabilit y-bi manual pal pat ion
Occlusal int egrit y-b y cli nical examination Neurological defi cit – pin and prick t est
and t he data's were compared st atis tical l y using M ann -Whit ne y
U t est, chi -square t es t.
Resul ts
38
2. Bim anual palpation was perform ed at first week, first mont h of each group to evaluat e the appropri at e positi on of t he fract ure site
3. Radi ograph (Di git al Ort hopantam ogram ) was performed in preoperative, Im mediat e post -operative, fi rst m onth, and si xth month of each group to evaluat e Fragment stabilit y
The results are
1. The m ean age of 10 pati ent s i n Group A was 31 years .The m ean age of 10 patients in Group B was 31.8 years[ chart1&2 &3]
Age wis e dis tributi on in Group -A p ati ents
Chart 1
0 0.5 1 1.5 2 2.5 3 3.5
age ≤20 21-30 31-40 41-50
No of patients
Resul ts
39
Age wis e dis tributi on in Group -B pati en ts
Chart 2
Comp arison of Age distributi on in both groups
Chart 3
0 0.5 1 1.5 2 2.5 3 3.5
age ≤20 21-30 31-40 41-50
No of patients
no of patients
0 0.5 1 1.5 2 2.5 3 3.5
age ≤20 21-30 31-40 41-50
Resul ts
40
2. The comm on etiol og y was road t raffic accidents (RTA) i n all 20 pati ent s.
3. The m ost common fract ure was at paras ymph ys is(55%)and second com es paras ymph ys is wi th angl e and thi rd comes paras ymph ys is with cond yl e(10%) followed b y s ym ph ysi s(5%) and fi nall y s ym ph ys i s wit h angle(5%) [chart 4]
Type of fracture
Chart 4
4. As per the average preoperative pain score in Group A was 3.9 and Group B was 4. Mann Whitne y U t est was applied to com pare the average pai n scores .There was si gnificant l y great er pai n at post operati ve 1s t week and 1s t m onth. but there was no si gni fi cant difference bet ween the groups at i mmedi ate post operative, 3r d month and 6t h month.(Table 1 &2]
parasymphysis
parasymphysis with angle
parasymphysis with condyle
symphysis
Resul ts
41
Mann - Whitn ey U tes t
Comp arison Of Pain Score By Visual Analogue S cal e In Group A and Group B
At Each Visi t S.no Durati on
of visi t
Group Nu mb er Mean rank
Standard error
P value 1. Im m edi at e
post op da y
Group A
10 10.50 .000 1.000
Group B
10 10.50
2 At fi rst week
Group A
10 7.50 10.513 .023*
Group B
10 13.50
3 At fi rst month
Group A
10 6.00 11.413 .000*
Group B
10 15.00
4 At thi rd
month
Group A
10 8.00 9.934 .063
Group B
10 13.00
5 At sixth
month
Group A
10 10.50 1.000 1.000
Group B
10 10.50
Signi ficance l evel is .05
Resul ts
42
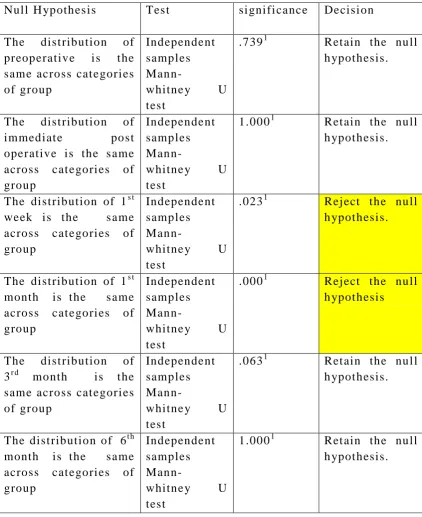
Hypoth esi s test su mmary -Mann whitn ey U test
As ym ptom ati c s i gni ficances are displa ye d. The si gni ficance l evel i s .05
1
[image:54.595.86.509.124.642.2]Exact si gni fi cance i s displa yed for t his t est. Table 2
Null H ypothes is Tes t si gni fi cance Decisi on
The dist ribution of preoperative i s t he sam e across cat egori es of group
Independent samples
Mann-whitne y U test
.7391 Ret ain the null h ypot hesis.
The dist ribution of immediat e post operative is the s ame across cat egori es of group
Independent samples Man
n-whitne y U test
1.0001 Ret ain the null h ypot hesis.
The dist ribution of 1s t week is the s ame across cat egori es of group
Independent samples
Mann-whitne y U test
.0231 Rej ect the null h ypot hesis.
The dist ribution of 1s t month is t he s ame across cat egori es of group
Independent samples
Mann-whitne y U test
.0001 Rej ect the null h ypot hesis
The dist ribution of 3r d month is t he sam e across cat egori es of group
Independent samples
Mann-whitne y U test
.0631 Ret ain the nul l h ypot hesis.
The dist ribution of 6t h month is t he s ame across cat egori es of group
Independent samples
Mann-whitne y U test
Resul ts
43
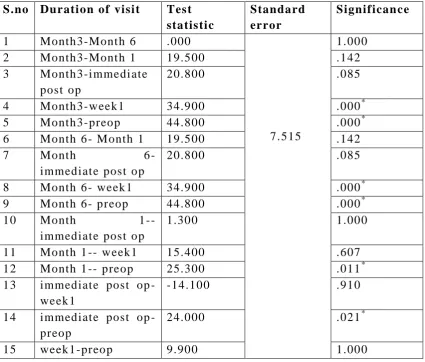
Kruskal -Walli s t est was applied t o find out t he pai n s core vari ati on in pre-operati ve, Im mediat e post -operat ive, at fi rst week, 1s t month, 3r d month and 6t h month wit hin each groups. There was si gnifi cantl y vari ation in pain s cores across cat egori es of period in bot h Group A and Group B [Tabl e3&4&5].
Kruskal -Wallis tes t
Tabulati on Of VAS Score In Indi vidual Vis it Of Each Group (Group A)
S.no Durati on of visi t Tes t statisti c
Standard error
Significan ce 1 Month3-Mont h 6 .000
7.515
1.000
2 Month3-Mont h 1 19.500 .142
3 Month3-i mmedi ate post op
20.800 .085
4 Month3-week1 34.900 .000*
5 Month3-preop 44.800 .000*
6 Month 6 - M onth 1 19.500 .142
7 Month 6 -
immediat e post op
20.800 .085
8 Month 6 - week1 34.900 .000*
9 Month 6 - preop 44.800 .000*
10 Month
1--immediat e post op
1.300 1.000
11 Month 1 -- week1 15.400 .607
12 Month 1 -- preop 25.300 .011*
13 immediat e post op - week1
-14.100 .910
14 immediat e post op - preop
24.000 .021*
15 week1-preop 9.900 1.000
[image:55.595.87.513.319.681.2]Resul ts
44
Kruskal -Wallis tes t
Tabulati on Of VAS Score In Indi vidual Vis it Of Each Group (Group B )
S.no Durati on of visi t Tes t statisti c
Standard error
Significan ce
1 Month 6 - M onth 3 7.750
7.6 b25
1.000
2 Month 6 -
immediat e post op
15.500 .631
3 Month 6 - M onth 1 26.750 .007*
4 Month6-week1 37.500 .000*
5 Month 6 - pre op 47.500 .000*
6 Month3-i mmedi ate post op
7.750 1.000
7 Month3-Mont h 1 19.000 .191
8 Month3-week1 29.750 .001*
9 Month3-preop 39.750 .000*
10 immediat e post op - Month 1
-11.250 1.000
11 immediat e post op - week1
-22.000 .059
12 immediat e post op - preop
32.000 .000*
13 Month 1 -- week1 10.750 1.000
14 Month 1 -- preop 20.750 .098
15 week1-preop 10.000 1.000
Resul ts
45
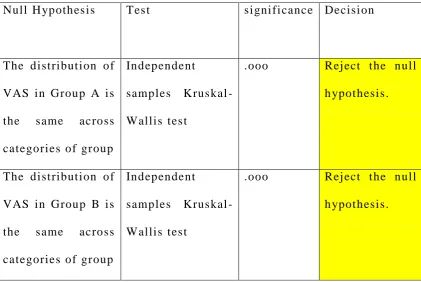
H ypothesis test su mmary -Krus kal-Wallis tes t
As ym ptom ati c s i gni ficances are displa ye d. The si gni ficance l evel i s .05 Table 5
5. Pati ents were evaluat ed post operativel y at Imm ediat e post -operative, fi rst week, 1s t month, 3r d month and 6t h mont h in both groups for si gns of i nfection. The post -operative infect ion was seen i n one cas e of Group A and t wo cas es of Group B. It was st atis ticall y i nsi gnificant b y chi -square t est[Tabl e6]
Cross Tabulation Of Pos t Op erative Infecti on In Both Groups Group Infection Nu mb er
Chi-square value
Result
1. Group A Present 1
0.39
Not si gnifi cant P>0.05
Abs ent 9 2 Group B Present 2 Abs ent 8
Table 6
Null H ypothes is Tes t si gni fi cance Decisi on
The dist ribut ion of VAS in Group A is the s ame across categories of group
Independent samples Kruskal -Wallis tes t
.ooo Rej ect t he null h ypot hesis.
The dist ribut ion of VAS in Group B is the s ame across categories of group
Independent samples Kruskal -Wallis tes t
[image:57.595.84.512.97.382.2] [image:57.595.87.509.99.381.2]Resul ts
46
6. occlus ion was evaluat ed preoperativel y and pos t operativel y. All the 20 pati ents had deranged occlusion at the t ime of t hei r report to the hospit al. Aft er surger y occl usion was correct ed to norm al in all 20 cas es.
7. No cas e report ed wit h wound dehi scence in all 20 pati ents
8. Bim anual palpati on was perform ed at fi rst week, 1s t month of each group to evaluat e the appropri at e positi on of t he fract ure site. No case reported with al tered positi on whil e doing bimanual pal pation
9. Radi ographs were t aken to evaluat e fragm ent st abilit y at pre-operative, Imm edi at e post -pre-operative, 1s t m onth, and 6t h month. In both the groups no pati ents present ed with fragm ent st abili t y. 10. B y using pin and prick t est neurologi cal defi cit was evaluat ed.
Neurological defi cit was not pres ent in Group A patients and seen i n 1 case of Group B patient[Tabl e7 ].
Cross T abulation O f neurological d efici t In B oth Groups
Group Infection Nu mb er Chi-square value
Result
1. Group A
Present 0
1.05
Not si gnifi cant P>0.05
Abs ent 10
2 Group
B
Present 1 Abs ent 9
[image:58.595.85.511.569.724.2]Dis cuss ion
47
DISCUSSION
An y report of st ud y on mandibul ar fractures must be initi at ed first wi th a dis cus sion of the hi stor y of m andi bl e fract ures and evolution of treatm ent . Wri tings on m andibl e fractures appeared as earl y as 1650 BC, when an Egyptian pap yrus des cri bed the examinati on, di agnosis, and t reatm ent of mandibl e fract ures and ot her surgical ailm ents . The cas e i n whi ch a mandibl e fract ure was des cribed was thought to be incurabl e and therefore was not treat ed; patient subs equentl y di ed.
Hippocrat es described di rect reapproxi mation of the fract ure segm ents wit h t he use of ci rcumdent al wires , simil ar t o t oda y’s bridl e wire. He advocat ed wi ring of the adj acent t eeth wit h external bandaging t o i mmobilize the fract ure. Man y aut hors and ph ysi ci ans have des cribed t he t reatm ent of m andibl e fract ures . Ideas h ave vari ed, but all t reatm ents were s ubtl e modi fi cations of the Hi ppocrati c concept of reapproximat ion and imm obiliz ation.
Dis cuss ion
48
Before the advent of modern appl i ances, inst ruments and techni ques used in the t reatment of mand ibul ar fractures, m an y ingenious devi ces were m arket ed for the treatm ent of m andi bl e fractures. Each had i ts own i ndi vidual advantages, but as a group the y fai led t o provide di rect , st able reduction and immobiliz ation of t he mandibul ar s egments4 7.
Moder n t raum atol ogy start ed wit h the devel opm ent of Ost eos ynthesi s and t here is drasti c shift from closed t echniques to open techni ques. Ri gid fi xation is prom oted b y t he AO/ AS IF. DCP and EDCP plat es were used in this concept. The D ynami c compressi on plat es wer e desi gned with a special confi gurati on of the s crew hol e to allow compressi on across the fracture when the s crew head is full y ti ght ened. The t wo hol es adj acent to the fracture are drill ed to caus e com press ion across t he fracture and the out er hol es are d rill ed with a pas sive positi on4 8.
Dis cuss ion
49
Generall y, fracture in t he s ym ph ys is require two pl ates, bod y fracture one plat e below the roots of premolar teet h and angl e fract ure requi res one pl at e along the oblique ridge. The neut ral zone cl os el y foll ows the cours e of the i nferior alveol ar nerve. The portion of a fracture passi ng through the neut ral zone does not have di splacem ent force on it when an occlusal load is pl aced; a compressive force is applied to the inferior border of t he m andibl e and mentum . In thi s com press ion zone, fulcrum occurs when force is appli ed to the occlusal surface all owi ng for a point around which a fract ure will rotat e.
Cham p y et al1 approached the t reatm ent of fractures of the mandibl e from a di fferent approach. They des cri bed the m andibl e as a parabol a with a thi ck out er cort ex and a thi nner i nner cort ex with a cent ral s pongiosa. His group was fel t that the thick out er cort ex provided ost eos ynthesis screws with good anchorage, parti cularl y chin and behind the thi rd molar. The y felt that sm all er plat es pl ace d in thi s ideal ost eos ynt hesis line with monocort ical s crews were all that was needed to achi eve healing under functional l oads.
Dis cuss ion
50
premol ar regi on. In addition thes e forces produce predominantl y torsi onal movem ent s wit hin the mandibular s ym ph ys is that i ncreas e in strength t owards the mi dline. B y pl acing t he pl at es at t he most biom echani cal l y favourabl e sit e t o ne ut ral ize tension forces causing fracture dist racti on, one can mi nimiz e pl ate t hickness , wit h the consequent advant age of i ncreased mall eablit y1 6. Therefore the techni cal advant ages of mini pl ate ost eos ynthesis are as foll ows:
1. Small and easil y adapted. 2. Mono -corti cal appli cation4. 3. Int ra oral approach.
4. Funct ional st abilit y.
Dis cuss ion
51
plat es for midfacial fixation. The thickness of plates ranges from 0.5 t o 3.0mm and are m ade either of st ainl es s steel, tit anium , or vital lium. Recentl y 3D pl at es, biodegradabl e, self -reinforced pol yl acti de pl ates and s crews have been used f or the i nt ernal fixat ion of fract ures of t he mandibl e with good results .
Dis cuss ion
52
Principl es of three -dimensional pl at e osteos ynt hesis
Tissue di ssecti on onl y i n t he vici nit y of the pl anned ost eotom y
or fracture li ne
The t hree-dim ensi onal pl at es are pos itioned paral lel t o the
osteotom y or fract ure li ne
The connect ing arms of the pl ate should be positi oned
rect angul ar to the fractured li ne.
The 3D minipl at e its elf was a misnomer as t he pl at es t hem sel ves were not 3 -di mensi onal, but holds the fracture s egments ri gi dl y b y resist t he 3 -dim ens ional forces nam el y sheari ng, bendi ng and torsi onal forces that act upon t he fract ure site in functi on.
The us e of 3D mi ni plat es i n mandi bul ar fracture fixati on s o for not becom e es tablished. In recentl y publi shed s urve y b y GEAR et al2 5, among 104 AO/AS IF surgeons, onl y 6% use t his t ype of pl at e.
In the pres ent s tudy 10 cases of max illofaci al trauma with mandibul ar fract ures patients t reat ed wit h open reduct ion and i nternal fixation using 3 -D mini plates and 10 cases using conventional minipl at es.
Dis cuss ion
53
s ymph ys is (5%) and finall y s ymph ysi s with angl e(5%). In a stud y of 191 pati ents of 280 mandi bul ar fractures frequent l ocati on was the angle region (28.21%), paras ymph ys eal (21.07%) i n order of frequenc y2 2.
The tim e requi red for the adapt ati on and fixation of the plat e at the fracture sit e was recorded . In our st ud y the oper ating tim e required for t he adapt ati on and fixati on of 3D pl at e was les s. ZIX et al3 2 and others on 3D pl at e who report ed reduced operating tim e because 3D plat e is geomet ri c confi gured pl at e whi ch consist of two horizontal bars i nterconnect ed with two ve rtical bars . So singl e 3D plat e stabilized the fract ure both at superior and inferi or border at a tim e, hence ti me is saved in pl ate fixation. Post operati ve radiographi c evaluati on i n patients showed excell ent reducti on i n bot h groups.
Alper Alkan et al2 9 carri ed out an in -vit ro stud y to evaluate the biom echani cal behaviour of four di fferent t ypes of ri gid fixation s yst ems with s emi -rigid fixati on s yst em that are used currentl y. The stud y demonst rated that 3D struts pl ates had great er res istance to compression loads than the Champy’s technique. Gunter et al4
Dis cuss ion
54
Seiji Nakamura et al1 1 and ot hers noti ced post operative com plicati ons li ke malocclusion(3.6%), exposure of minipl at e (3.6%), del a yed union (1.8%) and infecti on (1.0%) in 110 pat i ents with mandibul ar fractures. Post operative compli cations m a y be due to inadequate reduction and st abil izati on, dela y i n t reatment , t eeth in fracture line, fail ure to provide anti bioti cs, alcohol or drug abuse.
Claude Guim ond et al7 used 2mm three di mens ional curve d angl e strut pl at e; the y noti ced l ow morbi dit y a nd i nfection rate. In our st ud y we noti ced post operative infecti on in one patient in Group A and two pati ent s in Group B . No occlusal di screpancies were encount ered duri ng t he pos toperative peri od with an y pati ent , s o the result obt ained with occl usion was good with three dim ensional plating.
Dis cuss ion
55
J.M.Witten berg et al1 7 used 3 -D pl at es in mandibul ar fract ures and the y noti ced that the us e of 3 -D pl at es easi er to pl ace i nt ra oral l y. Becaus e of cl os ed quadrangular geom etric shape and eas e of contouring and adapti ng to bony fragm ents it provi de good st abi l izati on in t hree dimensions. So t here is a l ow morbidi t y and infection rat e.
The onl y probabl e li mitati on m a y be excessi ve im plant material due to extra vertical bars for count eri ng the t orque forces and i n case where t he fracture li ne passing t hrough t he mental forami na.
Conclusi on
56
CONCLUSION
This stud y was conduct ed in 20 pati ent s of mandibul ar fractures with an aim of eval uating t he effi cac y of 3D tit anium mi nipl at es i n t he managem ent of ant erior m andibul ar fracture s. Com plicati ons encount ered during thei r us e were also recorded and report ed in this stud y. Out of 20 total pati ents of ant erior m andibular fract ures, 10 cases of Group A treat ed b y 3D pl at es and 10 cas es of Group B treat ed b y conventional m inipl at es, the res ulting ost eos ynt hesis were evaluat ed wit h cert ai n param et ers.
The age of pati ents were ranged from 18 to 60 years i rres pective of sex. The procedures were done under general anest hesi a. Ost eos ynthesi s was done as per t he principl es advis ed b y the Cham p y for li near pl at es and b y Farm and for 3D plat es.
Pati ents were kept on foll ow up for 6m onths and eval uat ed for the treatm ent results and compli cati ons.
The following concl usions were drawn from the stud y:
1. 3D pl at es were i ndeed eas y and simpl e to us e. Si gni fi cant reduction in operating tim e could be a chi eved with the us e of 3D plates whi ch m akes i t a tim e -s aving.