SCORING SYSTEM IN THE DIAGNOSIS OF ACUTE APPENDICITIS.
Dissertation
Submitted in partial fulfillment of the regulations of
M.S. DEGREE EXAMINATION
BRANCH I GENERAL SURGERY
THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY
CHENNAI
This is to certify that this dissertation titled “A STUDY ON THE USEFULLNESS OF PEDIATRIC APPENDICITIS SCORING SYSTEM IN THE DIAGNOSIS OF ACUTE APPENDICITIS.” is the bonafide work done by Dr. SATHYANARAYANAN M., Post Graduate student (2011 – 2014) in the Department of General Surgery, Government Stanley Medical College and Hospital, Chennai under my direct guidance and supervision, in partial fulfillment of the regulations of The Tamil Nadu Dr. M.G.R Medical University, Chennai for the award of M.S., Degree (General Surgery) Branch - I, Examination to be held in April 2014.
Prof.T.S..JAYASHREE, M.S.,D.G.O Prof. K. KAMARAJ, M.S.,
Professor of Surgery, Professor and Head of surgery, Dept. of General Surgery, Dept. of General Surgery, Stanley Medical College, Stanley Medical College, Chennai-600001.
PROF. S. GEETHA LAKSHMI, M.D., PhD,
The Dean,
I, DR.M.SATHYANARAYANAN solemnly declare that this dissertation titled “A STUDY ON THE USEFULLNESS OF PEDIATRIC APPENDICITIS SCORING SYSTEM IN THE DIAGNOSIS OF ACUTE APPENDICITIS “ is a bonafide work done by me in the Department of General Surgery, Government Stanley Medical College and Hospital, Chennai under the guidance and supervision of my unit chief.
Prof.T.S..JAYASHREE, M.S.,D.G.O Professor of Surgery
This dissertation is submitted to The Tamilnadu Dr. M.G.R. Medical University, Chennai in partial fulfillment of the university regulations for the award of M.S., Degree (General Surgery) Branch - I, Examination to be held in April 2014.
Place: Chennai.
I am highly indebted to my guide Prof. T.S.JAYASHREE, M.S. D.G.O., Professor of Surgery for her constant help, inspiration and valuable advice in preparing this dissertation.
I express my deepest sense of thankfulness to my Assistant Professors Dr. DORAI, M.S. D.Ortho., and Dr. CHITRA M.S., D.G.O.,
for their valuable inputs and constant encouragement without which this dissertation could not have been completed.
I consider it a privilege to have done this study under the supervision of my beloved Professor and Head of the Department
Prof.K. KAMARAJ, who has been a source of constant inspiration and encouragement to accomplish this work.
I express my sincere gratitude to my mentor Prof. P. DARWIN, former Head of Department of General Surgery. I thank him for the constant support, able guidance, inspiring words and valuable help he rendered to me during my course.
I am grateful to the Dean Prof. S. GEETHALAKSHMI for permitting me to conduct the study and use the resources of the College.
It is my earnest duty to thank my parents, wife and friends
without whom accomplishing this task would have been impossible.
Acute appendicitis is the most common surgical emergency worldwide. If not detected early
and treated, it can lead to perforation, peritonitis,& abscess formation. Despite many advances in
imaging modalities, the diagnosis of this condition is essentially clinical. In children, because of poor
development of omentum, the rate of perforation is high. Hence to detect this condition early and
to reduce the rate of negative appendicitis in children, many scoring systems have been developed.
Our study deals with the PEDIATRIC APPENDICITIS SCORING SYSTEM by ,Madhan Samuel. In this
study, about 50 children between the age group 4-15 years of age presenting with acute abdominal
pain to Govt Stanley Medical College were selected and PAS was applied. Each of them were
assigned a score based on 8 variables to a total score of 10.They were into 3 groups those with >8
were taken up for surgery, <4 were discharged and those with scores 5-7 were subjected to imaging
and taken up for surgery if proven by imaging. The groups were compared and the sensitivity of the
test was 97%, specificity was 85 % and positive predictive value was comparable to the original
study. The study showed that PAS can be used as adiagnostic tool in the diagnosis of acute
S. NO. CHAPTER PAGE NO
1. INTRODUCTION 01
2. AIMS AND OBJECTIVES 03
3. REVIEW OF LITERATURE 04
4. MATERIALS & METHODS 64
5. OBSERVATION AND RESULTS 67
6. DISCUSSION 73
7. CONCLUSION 75
8. BIBLIOGRAPHY
9. ANNEXURE
(i) PROFORMA
(ii) MASTER CHART
(iii) INSTITUTIONAL ETHICAL COMMITTEE APPROVAL CERTIFICATE
(iv) CONSENT FORM
INTRODUCTION:
Appendicitis refers to inflammation of the appendix due to 3to
various etiologies and is the most common general surgical emergency
worldwide. Acutely inflamed appendix can be removed surgically either
by laparoscopic or open technique and is the most commonly performed
emergency general surgical procedure. But the diagnosis of acute
appendicitis can be difficult and challenging in certain circumstances.
Though there have been many advances in imaging diagnostic modalities
the diagnosis of acute appendicitis is essentially clinical. Hence various
clinical scoring systems have been developed to diagnose or exclude
appendicitis. Delaying intervention in acute appendicitis or failure to
diagnose at the earliest can result in severe complications especially in
children and elderly. The incidence is about 8% and is common between
ages 10 to 30 with male: female ratio of 1.8:1[1].
Though there are several scoring systems in the adult for diagnosis
of appendicitis the sensitivity and specificity of such scoring system drops
when applied to children due to differences in clinical presentation. Hence
several pediatric appendicitis scoring systems have been developed to
early but is also cost effective and avoids indiscriminate use of imaging
studies in children.
Of these the most commonly used scoring system is the
PEDIATRIC APPENDICITIS SCORING SYSTEM developed by
MADHAN SAMUEL. There are 8 variables that are used to clinically
score and categorize children into 3 categories upon a total score of 10;
namely, those with scores less than 3, and those with 4 to 6 and those with
7 to 10. Those children with scores over 7 had a high probability of
appendicitis and subsequently were taken up for surgery. Those with
scores less than 3 were discharged and subsequently followed up as
out-patients. Those with scores with 4 to 6 were subjected to further imaging
studies and were followed up as in-patients till pain is relieved or another
AIMS AND OBJECTIVES:
To study the usefulness of PEDIATRIC APPENDICITIS SCORE
in the diagnosis of acute appendicitis in children by correlating the clinical
diagnosis obtained by scoring system with intra-operative findings and
REVIEW OF LITERATURE
Berengarius Carpus a professor of surgery at Pavia was the first to describe
vermiform appendix in 1522.
Clado described a fold of peritoneum running from the ovary to the meso
appendix, and since then known as Clado’s ligament.
Reginald Fitz was the first one to coin the term appendicitis.
McBurney in 1889 described his classical sign- tenderness at the point of
two-third and one third junction of the line drawn from umbilicus to
anterior superior iliac spine in acute appendicitis.
Claudius Amyand was the first to remove the appendix in 1735 in a
hernia surgery.
McBurney described his original muscle splitting operation in 1893 and
this was modified by Weir in 1900.
ANATOMY OF THE APPENDIX AND ITS SIGNIFICANCE
The appendix is a derivative of midgut and arises from the cecum as
a small outpouching that gradually elongates into a worm-like tubular
organ.
The cecal diverticulum appears in 6th week of gestation and is the
primordium for both the cecum and the vermiform appendix.
The diverticulum appears as a conical pouch on the antimesenteric
border of the caudal limb of the midgut loop and descends from above.
The distal end of the blind sac retards in growth, thus the appendix-a
vestige of the incomplete development of the cecum, develops.
During the elongation of the proximal colon, the cecum and the
appendix descend from the right upper quadrant of the abdomen to its
The base of the appendix shifts medially during growth due to
excessive growth of right and anterior walls of the cecum.Failure of such
GROSS ANATOMY :
Verminform appendix is a tubular worm-like organ arising from the
cecum. Average human appendix measures 2 to 20 cm in length. The
diameter of the appendix is about 7-8mm. The largest appendix ever
removed measured 26 cm in length from a patient in Crotia.
RELATIONS:
The appendix is related posteriorly to the ilio-psoas muscle and lumbar
plexus of nerves.
Anteriorly its related to the abdominal wall, greater omentum and coils of
intestine.
In cadaver the apex is found medial to mid-point of right inguinal
ligament.
In living individuals the position varies with posture, state of distension of
bowel, muscle tone, and respiration.
In upright posture the cecum and appendix overhangs the pelvic brim.
The tip of the appendix can point toward any organ except toward the
The vermiform appendix has;
1.base attached to the cecum
2. body
3. tip, and
4.a mesoappendix through which the blood supply is derived.
The position of the base is fairly constant in location at about 2cm below
the ileo-cecal valve, but the tip of the appendix is highly variable in
position
BLOOD SUPPLY:
There are 4 patterns of arterial supply for the appendix, namely.,
1.single appendicular artery
2.paired appendicular arteries
3.arterial loop from the anterior cecal,posterior cecal, and ileo-colic
arteries forming accessory appendiceal arteries.
4.anterior and posterior appendicular arteries supplying from the base .Of
Another artery called the artery of Sheshachalam which is a branch
of posterior cecal artery also supplies the appendix.
Veins from the appendix drain into the ileo-colic vein which in turn
drain into the superior mesentric vein
NERVE SUPPLY:
Its innervated by the vagus nerve for parasympathetic supply and the
LYMPHATIC SUPPLY:
Lymphatics drain into the ileo-colic lymph nodes.
These ileo-colic nodes further drain into superior mesentric to the celiac
nodes and finally cisterna chyli.
The lymphatic drainage of the wall of the appendix drains into the lumen
and is different from the lymphatic drainage of the organ.
There is a secondary lymphatic drainage as described byBraithwaite with
the nodes draining into the sub-pyloric nodes anterior to the pancreas.
TOPOGRAPHY OF APPENDIX AND ITS VARIOUS POSITIONS:
In malrotation of the midgut the appendix may be found in the left
iliac fossa resulting in pain in that region in acute appendicitis.In old age
people, the appendix may become cord-like and very rarely the appendix
may be altogether absent.
The location of the appendix can be anywhere from its initial
position in the right upper quadrant of the abdomen in utero to its final
location in the right iliac fossa which is the most common location for the
Also the position of the tip is highly variable and its unusual
position can pose difficulties in diagnosis of appendicitis and also during
surgical removal.
The most common location for the appendix is retrocecal followed
by pelvic position.the following are the percentage of various positions of
the appendix.
Retrocecal-64%
Pelvic -32%
Sub-cecal-2%
Pre-ileal-1% Post-ileal-0.5%
HISTOLOGY:
The appendix histologically has four layers – mucosa, sub-mucosa,
an inner circular and an outer longitudinal muscle layer and a serosa. The
appendicular lumen is stellate in cross-section.
The mucosa of the appendix is rich in mucinous glands and crypts.
The mucosa also contains neuro-endocrine cells , histiocytes and
eosiniphilic cells.
The base of the crypts contain paneth cells with basal nuclues,
conspicuos nucleoli and abundant eosinophilic cytoplasm.
The appendix is essentially a lymphoid rich organ with abundant
lymphoid follicles in its lamina propria – functionally part of the gut
associated lymphoid tissue.These lymphoid follicles get inflammed and
when they do so they can cause acute appendicitis.They are abundant in
Histology of normal appendix
This picture shows mucosa and submucosa and muscularis externa
layers with lymphoid collicles in the lamina propria. The mucosa also
The altered histology in appendicitis
Picture shows epithelial sloughing and extensive neutrophil infiltration of the mucosal and sub-mucosal layer with protein-rich
PATHOPHYSIOLOGY OF ACUTE APPENDICITIS
There are basically two major types of pathological processes involved in
acute appendicitis.
1. obstructive type,
2. non-obstructive type(acute catarrhal).
1.
Obstructive type
:The major cause of acute appendicitis is the obstruction of the
appendiceal lumen. This is due to
1. inspissated stool (fecalith or appendicolith),
2. lymphoid hyperplasia,
3. vegetable matter or seeds,
4. worms- Balantidinum coli, Enterobius vermicularis, Schistosomia
hematobium
5. barium from previous contrast studies.
6. a neoplasm.
The lumen of the appendix is very small with respect to its length,
Obstruction of the lumen causes bacterial overgrowth, and
continuous secretion of mucus by mucinous cells.
This leads to distention of lumen and increase in transmural
pressure.
This distension causes visceral pain experienced by the patient as
periumbilical pain.
Resulting impaired lymphatic and venous drainage causes mucosal
ischemia.
These process combine to cause a localized inflammatory process
which progresses to gangrene and perforation.
Inflammation of the adjacent parietal peritoneum causes localized
pain in the right iliac fossa.
Usually , perforation typically occurs after 48 hours from the onset
of pain and is followed by formation of an abscess cavity .
This abscess cavity is walled-off by small intestine and omentum.
Sometimes , free perforation of the appendix into the peritoneal
cavity may result in peritonitis and peritoneal sepsis.This may
complicate as multiple intra-abdominal abscesses.Sometimes even
Factors encouraging Progression of Inflammation:
(i) Very young or old age.
(ii) Immunosupression.
(iii) Free lying appendix.
(iv) Presence of faecolith.
(v) Purgatives.
(vi) Impaired blood supply.
2.NON-OBSTRUCTIVE TYPE:
In this type, the inflammation commences either at the mucous membrane
of the appendix or in the lymph follicles and terminates either as
1. resolution,
2.ulceration
3. suppuration
4.fibrosis or
5. gangrene.
The infection progresses rapidly once it reaches the submucousal
The organ becomes inflammed, turgid, dusky red and haemorrhage
into the mucous membrane occurs. The distal part of the appendix is often
prone to ischaemia as the artery is intramural and is liable to occlusion by
inflammation and thrombosis thereby, leading to gangrene of the tip of the
appendix.
The non-obstructive type progresses slowly and a protective barrier
is formed and the inflammation does not progress beyond the mucosal
lining and the attack wanes off without sequelae.This is known as acute
catarrhal appendicitis.
But this catarrhal type is notorious to recur causing frequent attacks
many a times a year in few cases. In that case an elective or emergency
appendectomy has to be planned otherwise it may result in chronic
recurring pain.
CHRONIC APPENDICITIS: This is condition of gradual inflammation of
the appendix leading to frequent episodes of right lower quadrant pain.The
clinical features are milder than acute appendicitis but usually complete
Bacteriology of appendicitis:
The normal appendix contains flora that is very similar to that of the
colon.
It contains both facultative aerobic and anaerobic bacteria. Thus the
cultures in perforated appendicitis is polymicrobial in nature, namely,
1. Bacteroides
2. Pseudomonas
3. E.coli
4. Streptococcus viridians species
In patients with acute non-perforated appendicitis, cultures from
peritoneal fluid are frequently negative.
But in patients with peritoneal contamination due to perforation,
cultures are frequently positive with adequate sensitivity to antibiotics for
proper selection of anti-biotics in post-operative period.
Also the virulence of these organisms in extreme enough to cause
Bacteria Commonly Isolated in Perforated Appendicitis
ANAEROBIC PATIENTS (%)
Bacteroides fragilis 80
Bacteroides thetaiotaomicron 61
Bilophila wadsworthia 55
Peptostreptococcusspecies 46
AEROBIC
Escherichia coli 77
Streptococcus viridians 43
Group D streptococcus 27
CLINICAL FEATURES:
HISTORY
Appendicitis should be considered as a differential diagnosis in
almost every patient with acute abdominal pain. Early diagnosis is
important in patients with suspected appendicitis and can usually be made
on the basis of history and physical exam. The typical presentation is an
adolescent male or female with periumbilical pain followed by anorexia,
nausea and vomiting.
The pain then localizes to right iliac fossa as the inflammation
progresses to involve the parietal peritoneum overlying the appendix. This
is a classic pattern of acute appendicitis.
This migratory pain is the most reliable symptom of acute
appendicitis but the symptom is not always present.
The patient may have a bout of vomiting. This is in contrast to
repeated bouts of vomiting that occurs in viral gastroenteritis or intestinal
obstruction. Fever ensues, followed by leukocytosis.
But clinical features may vary. The classic triad of pain followed by
Rarely, patients may have urinary symptoms or microscopic
hematuria, owing to the inflammation of periappendiceal tissues that are
adjacent to the ureter or bladder, and this may be mislead one to consider
ureteric colic as the first in differential diagnoses.
Most patients with appendicitis develop an adynamic ileus and absent
bowel movements, but occasional patients may present with diarrhea.
Some may present with acute small bowel obstruction due to contiguous
regional inflammation and adhesion.
Therefore, appendicitis can be a possible cause of small bowel
obstruction, especially in patients without prior history of abdominal
surgery.
ATYPICAL PRESENTATIONS:
The position of the tip of the appendix can also result in a myriad of
different presentations.
1.Right hypochondrial pain- pulled up cecum or cecum that had arrested in
its path of descent.
2.Diarrheoa- pre and post-ileal type
4.urinary frequency- retro-cecal type of appendicitis with peri-appendiceal
inflammation.
PHYSICAL EXAMINATION :
Acute appendicitis patients typically have a sick look and lie still in bed.
Usually it is accompanied by a low-grade fever ( 38°C) .
Local Examination of the abdomen reveals diminished bowel sounds and
tenderness at the right lower quadrant with guarding.
The exact site of tenderness is most commonly at McBurney's point –
which is at one third of the distance along a line drawn from the anterior
superior iliac spine to the umbilicus-this point is directly over the
appendix.
The normal appendix is a mobile organ, so it may become inflamed at a
point anywhere on a 360-degree circle about the base of the cecum. Hence,
the site of maximal point of tenderness may vary.
Peritoneal irritation is elicited by the findings of guarding on percussion,
or rebound tenderness.
The following signs may be
2. Rovsing's sign- pain in the right iliac fossa on palpation of the left iliac fossa.
3. Obturator sign -pain on internal rotation of the hip in case of a
pelvic appendix.
4. Cope’s ilio-psoas test- pain on extension of right hip in a retro-cecal
appendix.
5. Digital rectal examination- If the appendix is located within the
pelvis tenderness on palpation of the abdomen is minimal, but
anterior tenderness may be elicited during digital rectal examination
on manipulation of pelvic peritoneum.
6. Per-vaginal examination- movement of the cervix may cause
tenderness in a pelvic appendix.
7. In perforated appendicitis- the abdominal pain intensifies and is
more diffuse. Abdominal wall muscle spasm increases causing
rigidity. Tachycardia with fever may ensue. The patient appears ill
and is briefly resuscitated with fluid and antibiotics are
administered.
Sometimes pain may improve slightly after rupture of the appendix
LABORATORY INVESTIGATIONS:
The following findings are noted:
1. Leucocytosis- a WBC count of more than 20000 is indicative of
perforated or gangrenous appendicitis.
2. Neutrophilia .
3. Microscopic hematuria
4. Pyuria –in case of ureteric involvement in retro-cecal appendix.
5. C-REACTIVE PROTEIN- elevated levels in a patient with clinical
IMAGING:
X-Ray
findings-In 10-15% of patients a calcified appendicolith may be seen.
In barium enema, failure of the appendix to fill with contrast is a sign of
appendicitis. Upto 20% of normal appendix also does not fill with contrast.
ULTRASONOGRAM-1. Sensitivity -85 %
2. Specificity-90%
POSITIVE FINDINGS in favour of acute appendicitis include;
1. Antero-posterior diameter of the appendix >7mm.
2. Target lesion- a thick-walled, dilated non-compressible, aperistaltic
structure.
3. Appendicolith
4. In appendicular mass,peri-appendiceal fluid collection or mass
formation may be seen.
5. RING of FIRE APPEARANCE- increased flow in case of inflamed
ADVANTAGES-1. Non-invasive
2. No radiation-may be used in children and pregnant females.3.Color
Doppler studies can be done to establish gangrenous appendix.
DISADVANTAGES
-1.Operator dependant
2.In 10-15% of cases, appendix may not be detected.
Hypervascularity of appendix in acute appendicitis
This is well seen in color Doppler USG. The incresded flow appears in
Obliteration of fat plane in the psoas region- psoas sign , a feature of
ULTRASONOGRAM of the abdomen showing inflamed appendix as a aperistaltic, dilated loop –longitudinal view
‘Ring of fire appearance’ in color Doppler in transverse view
This is the diagnostic sign in Doppler USG. This is due to extensive
inflammation and increased flow in peri-appendiceal vesssels and
Appendicular mass in Ultrasonogram
Hetoroechoic mass in the right iliac fossa formed by inflamed
appendix, small bowel, omentum with fluid collectin and abscess
COMPUTED
TOMOGRAHY-Sensitivity- 90%
Specificity -80 to 90%.
Positive predictive value- 75%.
CT findings
include-1. Thickened dilated appendix with diameter more than 7 mm.
2. Target sign-circumferential wall thickening appearing as a halo on CT.
3. Peri-appendiceal fat stranding
4. Appendicular abscess
5. Phlegmon
Target sign in CT
Intense contrast-enhancing appendicular wall in appendicitis. This is
due to hypervascularity and venous congestion and increase in
Appendicolith in CT
Appendicoliths may vary in size and number and appear as
Appendicular mass in contast CT.
Hyperattenuated mass in RIF in contrast CT with peri-appendiceal
DIAGNOSTIC LAPAROSCOPY
Most patients with acute appendicitis can be accurately diagnosed
based on history, clinical exam, laboratory studies, and, imaging, but in
some patients the diagnosis still remains elusive.
For these patients, diagnostic laparoscopy can be of certain value.
D-lap can aid in complete survey of the abdominal organs for other
possible causes of pain.
This technique can be used primarily for women of childbearing age
in whom preoperative pelvic ultrasound or CT scan fails to provide a
diagnosis.
Concerns about the possible adverse effects of a missed perforation
and peritonitis on future fertility sometimes prompt earlier intervention in
this patient population.
The diagnostic laparoscopy can also be therapeutic and
appendectomy is done as a routine if no other alternate pathology is
noted.Other pelvic pathologies that can mimic appendicitis are ovarian
cyst, ectopic pregnancy,meckels diverticulum and mesenteric
DIFFERENTIAL DIAGNOSES:
1.
INFANTS-a. Intussusception- this is a common condition in children and
ileocecal intussusceptions can sometimes mimic perforated
appendicitis. Currant jelly stools. But a palpable mass in right
hypochondrium and emptiness in right lower quadrant (dance sign)
are the key features.
b. Hirshprung ‘s disease
c. Cystic fibrosis
2. PRE-SCHOOL
CHILDREN-a. Acute gastro-enteritis- this presents as diarrhea, vomiting and fever.
The abdomen pain is colicky and periumblical but it can be diffuse
and is often a close differential diagnosis.
b. Intussusception- has colicky intermittent abdominal pain, and
positive Dance sign (Emptiness in right iliac fossa)
c. Meckel’s diverticulitis- pain is typically in the periumblical region
and does not have specific radiation, may have associated diarrhea
d. Mesentric lymphadenitis- this is too common in pre-school children
and is usually secondary to upper respiratory tract infection or
gastro-intestinal tract infection.
3. MALES
a. Pyelonephritis:
- this is an inflammation of the renal parenchyma and pelvis due to
bacteria and variety of other causes.
-Pain is mostly in the flanks.
-Associated with fever and leucocytosis.
-Patient looks toxic and obtunded.
-On lab investigations- pyuria may be seen in urine analysis.
-Non –contrast helical CT is the investigation of choice. It may
detect radio-opague stones and obstructed and dilated pelvi-calyceal
system.
-Urine culture demonstrates organisms
-Treatment- i.v. anti-biotics , hydration, and surgical intervention
b.
-this is inflammation of the colon and secondary to infections or
inflammatory bowel disease, auto-immune, and variety of other causes .
-Symptoms are usually diarrhea and cramping right or left-sided
abdominal pain with tenesmus,bloating, loss or appetite at times.
- treatment is usually antibiotics and treating the cause.
c. Ureteric colic:
-this is the most common entity confused with acute appendicitis.
Symptoms-Pain – the site or pain depends on the location of the calculus. Upper
ureteric calculus has pain in the loin. Ir radiates to the groin.
Lower uereteric calculi have pain in the right iliac fossa radiating to
the external genitalia or medial side of thigh.
Pain is severe enough to cause the patient to “roll-over” bed,
associated with sweating and vomiting.
USG abdomen- this reveals calculus and dilated pelvi-calyceal
system if there is associated hydro-uretero-nephrosis.
Treatment –
1. NSAIDS, antibiotics and adequate hydration.
2. Calcium-channel blocker, diuretics and alpha-blockers may be tried.
3. Lithotripsy may be done in resistant cases.
Diverticulitis:
-This refers to inflammation of the diverticula or out-pouchings
from the wall of large or small intestine.
The classical symptoms are left lower quadrant pain, fever and
leucocytosis.
Sometimes, right lower quadrant pain may occur in pre-dominant
right-colon involvement or a very redundant sigmoid colon.
Diagnosis –
CT abdomen is the investigation of choice. 5mm CT cuts are
accurate in diagnosing diverticulosis and in acute diverticulosis,
Treatment
-Uncomplicated diverticulosis may be treated with anti-biotics and
obsercation.
Complications of diverticulosis include perforation with peritoneal sepsis,
bleeding, obstruction, and fistula formation.
Perforation-surgically treated by diversion procedures.
Bleeding and obstruction- resection and anastomosis.
WOMEN OF CHILD-BEARING
AGE-1. PELVIC INFLAMMMATORY DISEASE:
Infection of the female genital tract including the uterus, ovaries,
fallopian tubes.
Associated with menorrhagia, lower abdominal pain and sometimes
fever, dyspareunia,intermensrual bleeding. Cervical motion tenderness and
leucorrhea are important distinguishing features.
2. OVARIAN CYST TORSION:
This is a gynecological emergency and can mimic as acute
appendicitis.
This happens when a large ovarian cyst undergoes twisting at its
pedicle and its blood supply is jeopardized.
This results in congestion and ischaemia of the ovaries and resultant
gangrene may also occur.
Symptoms-Sudden agonizing lower abdominal pain followed by vomiting,
tachycardia and fever.
Doppler USG: Investigation modality of choice. Lack of blood flow to
ovaries on Doppler confirms diagnosis.
Treatment:
This is surgical- laparoscopic ovarian cystectomy or oophorectomy
3. ECTOPIC PREGNANCY:
This presents as severe lower abdomen pain and tenderness in the
hypogastric region. The ectopic pregnancy site can be fallopian tubes(most
common), followed by ovaries and cervix.
Rupture of ectopic pregnancy into the abdominal cavity is a life
threatening complication and can result in severe blood loss and
hemorrghic shock.
Symptoms:
Pain over lower abdomen, pelvic pain or in low back. In ruptured
ectopic, patient may have shoulder pain, which is an ominuous sign cause
of diaphragmatic irritation.
There is associated tachycardia and pallor with signs of fall in BP
and cold peripheries –signs of hemorrhagic shock.
Cullen’s sign- discolouration of peri-umblical region may be seen.
Diagnosis –
Trans-vaginal USG demonstrates absence of gestational sac in the
uterus and presence of adnexal mass. These along with elevated beta-HCG
Treatment:
Unruptured ectopic pregnancy can be treated with methotrexate .
Ruptured ectopic pregnancy needs laparotomy and removal of
conceptus, ruptured part , securing complete hemostasis.
IN PREGNANCY:
The main problem of appendicitis in pregnancy is that the usual
symptoms of appendicitis such as nausea,vomiting, are also found in
pregnancy.
Also the tip of the appendix is shifted up by the gravid uterus and
the site of tenderness is usually at the right hypochondrial region by 5th
month. USG abdomen can be used safely to diagnose and in rare cases
MRI abdomen can also be used. As the chances of fetal loss increases with
peritonitis and sepsis, early surgical intervention is warranted in pregnancy
with appendicitis.
Second trimester of pregnancy is usually safe for surgical procedures.
OLD AGE:
Appendicitis in old age is difficult to diagnose because of atypical
Also appendicitis is thought of as a less likely diagnosis compared to
diverticulosis or colitis and hence missed often. There is also no
leucocytosis due to poor immunity. In elderly the cause for appendicitis
should also be sought as even a cecal or appendicular malignancy could
cause appendicitis hence imaging should be done in all cases.
APPENDICITIS IN INFANTS AND CHILDREN:
The diagnosis of acute appendicitis is difficult in infants and young
children because children are unable to give an accurate history, and acute
nonspecific abdominal pain is common in infants and children. Hence, the
diagnosis and treatment are often delayed, and complications develop. The
clinical presentation in children can be quite similar to nonspecific
gastroenteritis. Hence, the suspicion of appendicitis often is not entertained
until the appendix has ruptured.
Two thirds of young children with appendicitis have had symptoms
for more than 3 days before appendectomy.Because children often cannot
give an accurate history of their pain, the physical examination and other
aspects of the history must be relied on to make the diagnosis. Vomiting,
fever, irritability, flexing of the thighs, and diarrhea are likely early
complaints. Abdominal distention is the most consistent physical finding.
The incidence of perforation in infants younger than 1 year of age is
almost 100%, and although it decreases with age, it is still 50% at 5 years
of age. The mortality rate in this age group remains as high as 5%. In one
series, nearly 40% of children with complicated appendicitis had been
wrongly diagnosed with other causes of abdominal pain.
CLINICAL SCORING SYSTEMS FOR APPENDICITIS:
Acute appendicitis is essentially a clinical diagnosis. The sensitivity
and specificity of clinical methods have proven to be more than imaging
techniques.
To increase the diagnostic rate in appendicitis and reduce the rate of
negative laparotomies, several scoring systems have been developed.
Of these the Alvorado scoring system has been the most commonly
used scoring system and has a sensitivity of 80-85% in various studies.
It is a simple and useful diagnostic tool in adults in picking up cases
early and also reduces rate of negative appendectomies.When combined
with graded compression ultrasonography the diagnostic yield is still
ALVORADO SCORING:
The Alvorado scoring system was first developed by Alfredo Alvorado of Philadelphia in 1986 an Nazreth hospital on a cohort of 305 patients.
Symptoms score
Migratory right iliac fossa pain -1
Nausea/Vomiting -1
Anorexia -1
Signs
Tenderness in right iliac fossa -2
Rebound tenderness in right iliac fossa -1
Elevated temperature >37.5 C -1
Laboratory Findings
Shift to the left of neutrophils >75% -1
Leucocytosis >10,000 -2
The variables used in the scoring have can be remembered with the mnemonic MANTRELS. The scoring system has a maximum achievable score of 10.
Those with scores >7 – have high probability of appendicitis and are taken up for surgery. Those with scores 5-6 are subjected to further imaging and are subsequently either taken up for surgery or are observed depending on the imaging findings. Those with scores less than 4 are discharged and followed up as out patients.
It had the following statistics:
Sensitivity – 80-85%
Specificity –85-90%
Positive predictive value- 92-96% .
Management of Appendicitis based on modified Alvarado criteria
PEDIATRIC APPENDICITIS SCORE
It was first developed in 2002 by MADHAN SAMUEL of England.
It specifically addresses the symptomatology in children it was
developed because:
1.rebound tenderness as in Alvarado scoring is extremely painful in
children and can make them unco-operative, apprenhensive and hence
should not be used in children.
2.variables such as leucocytosis and polymorphonuclear
neutrophilia had good correlation and cough tenderness were assigned a
score of 2 each to improve accuracy when applied to children. Variables
such as cough tenderness and percussion tenderness are unique to children.
Children with score >8 were taken up for surgery and those with 4-7
were subjected to further imaging re-assessed with PAS and were either
taken up for surgery or were followed up as in-patients depending on
OTHER SCORING SYSTEMS:
The Tzanakis scoring system – This incorporated ultrasound , clinical
findings and lab investigations.
The Appendicitis inflammatory response score
Ohmann scoring
Lintula scoring system
Fenyo-lindbang.
Computerised algorithms were developed for quicker assessment of
SURGERY- OPEN APPENDECTOMY:
Incisions :
1. Mcburney incision- The incision is made obliquely, beginning
inferiorly and medially, and extending laterally and superiorly.
It should be 8 to 10 cm in length, with its most medial extent being
the lateral edge of the rectus muscle
2. Rockey Davis: The incision is made in a transverse direction, 1 to 3
cm below the umbilicus, and is centered on the midclavicular line.
3. Weir extension - medial extension of Rockey Davis.
4. Rutherford Morrisson- lateral extension of Rockey Davis
5. Lanz incision- incision along the langers lines.
STEPS:
With any one of the above incisions, skin and sub-cutaneous layers
are cut. The aponeurosis and muscles of the abdominal wall are split or
incised in the direction of their fibers and peritoneum is reached
After the peritoneum is opened, the appendix is identified by
following the anterior cecal taenia to the base of the appendix.
1. All three taeniae lead to and end at the base of the appendix.
2. The ileocecal junction can usually be identified, just below which is the base of the appendix.
After identification, the mesoappendix is clamped and cut and the base of the appendix is crushed, clamped and cut. Peritoneal lavage is given in abscess and drain is fixed.[3].
Clamping of the mesoappendix in appendectomy
This is done with curved clamps and the meso-appendix is either
Clamping and Ligation of the base of the appendix
LAPAROSCOPIC APPENDECTOMY:
The port sites are chosen as in the figure.
Usually one 10mm camera port and two 5mm working ports are used.
Pneumoperitoneum is attained to a pressure of about 14 mmhg.
Using Maryland forceps and non-toothed or toothed graspers,
mesoappendix is cauterized and base of appendix is ligated by endo-loop
technique.
The appendix is extracted through any of the 5mm ports.
Laparoscopic View of Appendix
The appendix is traced upto its base where it attaches to the cecum
MATERIALS AND METHODS
PATIENTS AND METHODS
About 50 patients presenting to general surgery and pediatric surgery
department in the age group 4-15 years with complaints of acute
abdominal pain were chosen for the study. Detailed history-taking and
complete physical examination were done. The patients were divided into
3 groups based on 8 variables in the PEDIATRIC APPENDICITIS
SCORING system into those with scores >8, those with scores between
5-7, and those with scores <4.
The first group was taken up for surgery,namely emergency
appendectomy either laparoscopically or by open technique. The second
group of patients with score 5-7 was subsequently subjected to
Ultrasonogram of the abdomen and were either taken up for surgery or
followed up as in-patients with periodic re-assessment. The third group of
patients with scores <4 were discharged and followed up as out- patients.
Children who had previous history of appendectomy and those less than 4
Intra-Op finding
Total Yes No
Pas Score
8-10
No. of children 36 1 37 % within Pas Score 97.3% 2.7% 100.0% % with Intra-Op finding 85.7% 14.3% 75.5%
5-7
No of children 6 6 12
% within Pas Score 50.0% 50.0% 100.0% % with Intra-Op finding 14.3% 85.7% 24.5%
Total No of children 42 7 49
% within Pas Score 85.7% 14.3% 100.0% % within Intra-Op finding 100.0% 100.0% 100.0%
Correlation Of Pas Score With Intra-OP Findings
97.3 % of the children with scores 8-10 had appendicitis intra-operatively and 50% of those with scores 5-7 had appendicitis as
Distribution of Incidence of Appendicitis among the study group
Children with scores>8 had 84% of the total no of appendicitis cases.
OBSERVATIONS AND RESULTS
Of the 50 children, 37 of them had PAS scores of 8 or more.12
children had scores between 5-7 and were subsequently subjected to USG
abdomen of which 6 of them had features suggestive of acute appendicitis
and were taken up for surgery. Of the remaining 6 children, 3 had other
mesenteric lymphadenitis and 3 had normal study. These patients were
managed conservatively and they responded well to conservative
treatment. There was 1child with PAS scores less than 4 and were
discharged and followed up.
The intra-operative findings of the 43 patients (37+6) and the
histopathology findings were taken as confirmatory evidence for
appendicitis. Of the 43 patients, 42 patients with scores >5, had inflamed
appendix and one patient with PAS score of 8 had normal appendix.
STATISTICS:
Age & sex:
The average age of children with appendicitis was 9.4 and the
average age in non-appendicitis group was 5.7 years. The sex ratio
INCIDENCE OF APPENDICITIS IN MALE AND FEMALE WITH
PAS SCORES
Male :female ratio was 1.8:1
0 5 10 15 20 25
<4-7 >7-10
DISTRIBUTION OF TYPES OF APPENDICITIS
Uncomplicated appendicitis was the most frequent presentation followed by perforated appendicitis and gangrenous appendicitis. One
case had early mass formation and appendectomy was done.
INFLAMMED APPENDIX
PERFORATED APPENDICITIS
NAUSEA VOMITING PYREXIA OF PAIN LEUCOCYTOSIS PMN NEUTROPHILIA RIF TENDERNESS COUGH TENDERNESS
DISTRIBUTION OF SYMPTOMS AND SIGNS
The order of diagnostic index of the variables was 1.percussion
tenderness(85.7%), 2.anorexia(83.7%),
3. Nausea/vomiting,(83.5%) 4.tenderness in the right lower
quadrant,(82%) 5. PMN neutrophilia (77.6%), 6.leucucytosis (77%), 7.,
8.migratory pain(76.9%), all with a p value of <0.01.
The mean temperature for pyrexia was 38.1 C +/- 0.5C, and the mean
leucocyte count was 13,300+/- 1,400.
The mean for PMN neutrophilia was 74%+/-7%.
After assigning the PAS scores the children were classified into
appendicitis(43) and non-appendicitis(7) groups. The appendicitis group
group were taken up for surgery and the non-appendicitis group were
either observed or discharged. The intra-op findings and HPE findings
were correlated and diagnosis confirmed and sensitivity, specificity and
positive predictive values were calculated.
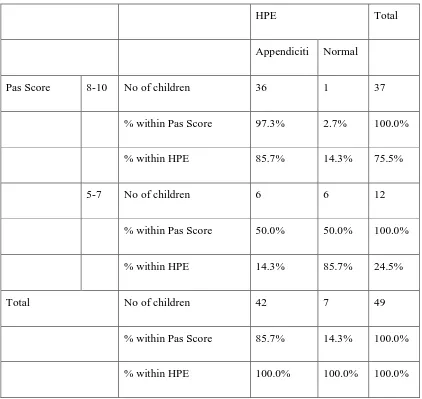
From the table below the overall sensitivity of the test was 85.7%
and specificity was 97.3%. The positive predictive value was 97.3% but
HPE Total Appendiciti Normal
Pas Score 8-10 No of children 36 1 37 % within Pas Score 97.3% 2.7% 100.0% % within HPE 85.7% 14.3% 75.5%
5-7 No of children 6 6 12
% within Pas Score 50.0% 50.0% 100.0% % within HPE 14.3% 85.7% 24.5%
Total No of children 42 7 49
[image:79.612.109.531.69.468.2]% within Pas Score 85.7% 14.3% 100.0% % within HPE 100.0% 100.0% 100.0%
Table correlating PAS SCORE with HPE report
97.3% of children with scores 8-10 had appendicitis confirmed on
DISCUSSION:
DEFINITION OF VARIABLES AND PARAMETERS:
Pyrexia – temperature > 37 .5 C
Leucocytosis- WBC> 10,000
PMN neutrophilia- >75 % of neutrophil count.
Migratory RIF pain- pain initially at the peri-umblical region later on
migrating to right-iliac fossa
Percussion tenderness- tenderness over right iliac-fossa to gentle
percussion
Cough tenderness- tenderness over RIF on asking the child to cough.
Anorexia – decrease in intake of food after the onset of pain.
USG findings suggestive of appendicitis- dilated, aperistaltic,
non-compressible structure in the right iliac-fossa.
Thus, the PEDIATRIC APPENDICITIS SCORING SYSTEM has high
sensitivity,specificity, and positive predictive value and poor negative
DR.MADHAN SAMUEL et all, and the study done by Ran Goldman in
“Prospective Validation of the Pediatric Appendicitis Score” by RAN D.
GOLDMAN, MD, SUSAN CARTER, BSC, DEREK STEPHENS, MD
and “ The prospective validation of PAS on Canadian population by Maala
Bhatt. The statistical inferences were comparable to the original study
CONCLUSION
This study shows that PEDIATRIC APPENDICITIS SCORING
SYSTEM is a useful diagnostic tool in the diagnosis of acute appendicitis
in children. This clinical scoring system can be used in remote areas where
other imaging modalities are unavailable and also can be used in the same
1. SABISTON TEXT BOOK OF SURGERY-18TH EDITION.
2. SKANDALAKIS –SURGICAL ANATOMY
3. SHACKELFORDS TEXTBOOK OF SURGERY OF THE
ALIMENTARY TRACT.- 6TH EDITION.
4. PEDIATRIC SURGERY by PURI AND HALLWORTH
5. BAILEY and LOVE TEXTBOOK OF SURGERY
6. ATLAS OF GI SURGERY by CAMERON.
7. Prospective Validation of the Pediatric Appendicitis Score RAN D.
GOLDMAN, MD, SUSAN CARTER, BSC, DEREK STEPHENS,
MD, ROULA ANTOON, MD, WILLIAM MOUNSTEPHEN, MD,
8. Utility of a scoring system in the diagnosis of acute appendicitis in
pediatric age. A retrospective study. Minerva Chirurgica
2002;57:341-6.
9. Bond GR, Tully SB, Chan LS, Bradley RL. Use of the MANTRELS
score in Childhood appendicitis: a prospective study of 187 children
with abdominal pain. AnnEmerg Med 1990;19:1014-8.
10. Samuel M. Pediatric appendicitis score. J Pediatr Surg 2002;37:
the diagnosis of appendicitis Ped Emerg Care 2004;20:795
[Abstract]
12. Alvarado scoring - practical score for the early diagnosis of acute
appendicitis. Ann Emerg Med 1986;15:557-64.
13. Owen TD, Williams H, Stiff G, Jenkinson LR, Rees BI. Evaluation
of the Alvarado score in acute appendicitis. J R Soc Med
1992;85:87-8.
14. Lamparelli MJ, Hoque HM, Pogson CJ, Ball AB. A prospective
evaluation of the combined use of the modi ed Alvarado score with
selective laparoscopy in adult females in the management of
suspected appendicitis. Ann R Coll Surg Engl 2000;82:192-5.
15. Ramirez JM, Deus J. Practical score to aid decision making in
• NAME : SL. NO:
• AGE /SEX:
• ADDRESS WITH CONTACT NUMBER:
• IP NO:
• DATE OF ADMISSION:
• DATE OF SURGERY:
• DATE OF DISCHARGE:
HISTORY OF PRESENTING ILLNESS:
PAIN ABDOMEN:
•
Site--•
Duration-•
Nature-• Aggravating/relieving
factors-• Radiation of
pain-• H/O NAUSEA/VOMITING IF ANY:
• H/O FEVER, IF ANY:
Whether a known case of Asthma/TB/epilepsy/cardiac
illness
, ,CONGENITAL DISEASESH/O SIMILAR EPISODES IN THE PAST, IF ANY:
H/O SURGERIES IN THE PAST, IF ANY
H/O MAJOR ILLNESS/ HOSPITAL ADMISSIONS, IF ANY
PERSONAL HISTORY:
Whether a smoker or an alcoholic,
FAMILY HISTORY:
TREATMENT HISTORY:
CLINICAL EXAMINATION:
GENERAL EXAMINATION:
SYSTEMIC EXAMINATION:
CVS
RS
PER ABDOMEN PALPATION
RIF TENDERNESS
PERCUSSION TENDERNESS
CLINICAL DIAGNOSIS:
INVESTIGATIONS:
• USG ABDOMEN AND PELVIS
• ROUTINE INVESTIGATIONS(CBC,RFT,CXR,ECG)
• OTHER INVESTIGATIONS(IF ANY):
FINAL DIAGNOSIS:
SURGERY DONE:
INTRO-OP FINDINGS:
S.
NO
NAM
E
AGE SEX I.P.No
N AU SE A/ VOM IT ING A NOR E XI A F EV ER M IG R A T IO N o
f P
AI L EU C O C YTO S IS NE UTR P H IL IA
RIF TEN
D ERNE SS PERC USS IO N TE N DER P AS SC OR E U SG INT RA -OP F IND IN HPE
1 JANARTHANAN 9 M 77178 1 1 - - 1 1 2 2 8 - INFLAMMED TIP OF APPENIX F/S/O
APPENDICITIS
2 KEERTHAN 12 M 77720 1 1 1 - 1 1 2 2 9 - INFLAMMED
APPENDIX
F/S/O APPENDICITIS
3333 3 3 ARUN 11 M 76587 - 1 - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
4 SWETHA 4
½
F 78244 1 1 - - 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
5 HARIHARAN 8 M 79674 - 1 1 - - - 2 2 6 MESENTRIC LYPHADENITIS -
6 SHAIK MOHAMMAD
12 M 79996 1 1 1 - 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
7 IBRAHIM 6 M 80193 1 - 1 - 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
8 MUKESH 9 M 35007 1 1 1 - - - 2 - 5 NORMAL STUDY -
9 PRAKASHI 9 M 82854 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
10 RITHICK KUMAR
11 M 38318 - 1 1 - 1 - 2 - 5 RIF PROBE TENDERNESS INFLAMMED APPENDIX F/S/O
APPENDICITIS
11 MOHAMMAD
YASIM
13 JACKULIN 11 F 39838 1 1 1 1 - 1 2 2 9 - PERFORATED APPENDIX F/S/O APPENDICITIS
14 LAKSHMANAN 7 M 82554 1 1 1 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
15 VALARMATHI 9 F 83830 1 1 - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
16 PRADEEP 8 M 40041 1 1 1 - 1 1 2 2 8 - Normal study Normal study
17 SUMAIYA BANU 12 F 84038 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
18 VENKATESH 9 M 85584 1 - - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
19 SURYA 12 M 84452 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
20 SHRUTHI 7 F 84559 1 1 - - - - 2 2 6 F/S/O APPENDICITIS INFLAMMED APPENDIX F/S/O
APPENDICITIS
21 SARATHY 9 M 85719 1 1 - 1 1 - 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
22 PAVITHRA 12 F 85314 1 1 - 1 1 1 - - 8 - -
23 VICTOR 11 M 85613 1 1 1 - 1 1 2 2 9 - EARLY APPENDICULAR
MASS
F/S/O APPENDICITIS
24 MADHAVAN 7 M 54755 1 1 1 1 1 1 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
25 GOKUL RANI 6 F 86288 - 1 1 - 1 - 2 2 9 F/S/O APPENDICITIS INFLAMMED APPENDIX F/S/O
APPENDICITIS
26 SOMA 9 F 86286 1 - - 1 1 1 2 2 8 - Gangrenous appendicitis F/S/O
APPENDICITIS
29 NARMADHA 4 F 86426 1 1 1 - 1 1 2 2 9 - PERFORATED APPENDIX F/S/O APPENDICITIS
30 VARUN 11 M 57775 - 1 - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
31 SANGEETHA 10 F 86623 1 - 1 - - 1 2 - 5 NORMAL STUDY -
32 RAMYA 12 F 86772 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
33 SUKUMAR 8 M 66020 - 1 - - 1 1 2 2 5 F/S/O APPENDICITIS INFLAMMED APPENDIX F/S/O
APPENDICITIS
34 SIRAJ 10 F 59361 - 1 - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
35 LOGESH 5 M 66217 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
36 MANIKANDAN 7 M 66196 - 1 1 1 1 1 2 2 9 - PERFORATED APPENDIX F/S/O
APPENDICITIS
37 AJAY 9 M 66534 1 1 - - 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
38 DEEPAK 10 M 66644 1 - - 1 - - 2 2 6 F/S/O APPENDICITIS INFLAMMED APPENDIX F/S/O
APPENDICITIS
39 VASANTH 11 M 66848 1 1 - - 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
40 SOFIA 10 F 66900 1 1 1 - 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
41 ADHILAKSHMI 11 F 11111 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
42 HELAN 9 F 67201 1 1 1 - - - 2 - 5 NORMAL STUDY -
-43 SRI DEVI 10 F 12084 - 1 - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
45 KRITHIKA 9 F 67596 1 - 1 - 1 - 2 - 5 MESENTRIC ADENITIS -
-46 ABILASH 12 M 67709 - 1 - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
47 MONISHA 9 F 68714 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
48 GOUTHAM 10 M 67902 - 1 - - 1 - 2 2 6 F/S/O APPENDICITIS INFLAMMED APPENDIX F/S/O
APPENDICITIS
49 EZHILARASI 5 F 68802 1 1 - 1 1 1 2 2 9 - INFLAMMED APPENDIX F/S/O
APPENDICITIS
50 SOLOMON 9 M 70154 1 - - 1 1 1 2 2 8 - INFLAMMED APPENDIX F/S/O