COMPARISON OF SHORT COURSE
VS
LONG COURSE OF ANTIBIOTIC
IN ELECTIVE CAESAREAN SECTION
Dissertation submitted to
THE TAMILNADU DR. M.G.R. MEDICAL
UNIVERSITY
In partial fulfillment of the regulations
For the award of the degree of
M.D. BRANCH-II
OBSTETRICS AND GYNECOLOGY
MADRAS MEDICAL COLLEGE
CHENNAI
CERTIFICATE
This is to certify that the dissertation entitled “Comparison of short course
vs. long course antibiotics in elective caesarean section.” is a bonafide
record of work done by Dr. V. M. ANNITH KUMAR in Madras Medical
college, Chennai during the period march 2017 to march 2018 under the
guidance of
Dr. P. Padmavathy MD., DGO.,
Professor of Obstetrics and
Gynaecology, Institute of Obstetrics and Gynaecology Madras Medical
College in partial fulfilment of requirement of MD degree in Obstetrics
and Gynaecology degree examination of The Tamilnadu Dr. M.G.R
Medical University to be held in May 2019.
Dr. S. VIJAYA, M.D., DGO.,
Director I/c.,
Institute of Social Obstetrics
Government Kasturba Gandhi Hospital
Chennai - 600005
Dr. R. JAYANTHI, M.D.,
Dean
DECLARATION
I Dr. V.M. ANNITH KUMAR, Post graduate, Department of Obstretrics
and Gynaecology, Madras Medical college, solemnly declare that this
dissertation entitled
“Comparison of short course vs long course
antibiotics in elective caesarean section”
was done by me at Madras
Medical College during 2016-2019 under the guidance and supervision of
Prof. Dr. P.Padmavathy MD., DGO.,
Professor of Obstetrics and
Gynaecology, Institute of Obstetrics and Gynaecology Madras Medical
College. This dissertation is submitted to the Tamil Nadu Dr. M.G.R.
Medical University towards the partial fulfilment of requirements for
the award of M.D. Degree in Obstetrics and Gynaecology (Branch-II).
Place: Chennai-3
Date:
Dr. V.M. ANNITH KUMAR,
Prof. DR. P. PADMAVATHY
M.D., DGO.,Guide,
ACKNOWLEDGEMENT
I am thankful to the Dean, Dr.R.JAYANTHI M.D., Madras Medical
College, Chennai for allowing to use the facilities and clinical materials
available in the hospital.
It is my pleasure to express my thanks to
Prof. Dr. S.VIJAYA
MD.,D.G.O., Director, Institute of Social Obstetrics, Government Kasturba
Gandhi Hospital for her valuable guidance, interest and encouragement in
this study.
I take this opportunity to express my deep sense of gratitude and
humble regards to my beloved teacher
Dr.P.PADMAVATHY, M.D.,
DGO., for her timely guidance suggestions and constant inspiration enabled
me to complete this dissertation.
I thank all my Professors, Assistant Professors and paramedical Staffs
of this Department of Obstetrics and Gynaceology, Madras Medical College,
Chennai-600003.
I thank all my patients for their cooperation and hence for the success
of study.
CONTENTS
1. INTRODUCTION
1
2. AIMS OF STUDY
4
3. REVIEW OF LITERATURE
6
4 OVERVIEW
14
5. MATERIALS AND METHODS
58
5. RESULTS AND DISCUSSIONS
63
6. SUMMARY
90
7. CONCLUSION
93
8. BIBLIOGRAPHY
95
1
2
Caesarean section is clean and uncontaminated wound. The use of antibiotics is mainly to reduce the partum infections and complications. Thus reducing the post-operative morbidity and mortality. This study attempted to compare the efficacy of short course regimen of antibiotic usage with that of the traditionally used long course of antibiotic in a government tertiary care centre. The group of patients who generally visit our hospital are from a lower socio economic strata, nutritionally challenged and with lesser education background. There is a general apprehension among the consultants working in a government hospital with the usage of a lesser amount of antibiotics. This study plans to see whether this the short course regimen is as effective the long course regimen which is extensively used as of now.
Rigorously defined, prophylactic antibiotics are those given to patients before contamination or infection has occurred. A broader, more practical definition includes clinical situations in which infection or contamination is already present, primary treatment of the infection is surgical, and anticipatory antibiotic administration mainly serves to minimize postoperative wound infection Initial antibiotic therapy is anticipatory, presumptive, or empiric.
3
time microbial contamination might occur. Delaying administration by even a few hours reduces or eliminates the benefit of prophylaxis. Ideally, the agent of choice should be long acting, narrowly focused on the likely bacteria, inexpensive, and have a low incidence of adverse effects.
Despite significant advances in diagnosis, medical management and antimicrobial therapy, sepsis in the puerperium remains an important cause of maternal death. Severe sepsis with acute organ a review of the literature shows that many factors are considered to predispose to such a high rate of infection. These include poor sterile techniques race,~ socioeconomic status.~ maternal age: obesity, lack of prenatal care, prior labour or rupture of membranes number of pelvic examinations preoperative and internal fetal monitoring dysfunction has a mortality rate of 20–40%, rising to around 60% if septicaemic shock develops.
4
5
AIM OF THE STUDY
Primary Objective:
1) To compare the effectiveness short course of antibiotic ( Two dose of Inj Cefotaxime 1g IV) with the routine long course antibiotic in regard to post-operative infective complications in patients who are undergoing elective caesarean section in a Government tertiary care hospital.
SECONDARY OBJECTIVE
6
7
The American Congress of Obstetricians and Gynecologists (ACOG) recommends the use of a single dose of a narrow spectrum first generation cephalosporin, or a single-dose combination of clindamycin with an aminoglycoside for those with a significant penicillin allergy, as prophylaxis for cesarean delivery. However, several studies have suggested that extended spectrum antibiotic prophylaxis may further reduce the risk of postcesarean infection.
In particular, narrow-spectrum antibiotics do not provide adequate coverage for Ureaplasma infection, which has been disproportionately isolated in patients with postcesarean endometritis.
ACOG guidelines currently recommend that antibiotic prophylaxis be administered within 60 minutes of the start of the cesarean delivery. With prior concerns about the sequelae of fetal antibiotic exposure, the former standard practice was administration of narrow-spectrum antibiotic prophylaxis after clamping of the umbilical cord. (1)
8
Given the known increased risk of postcesarean infection for obese patients, it is important to consider the appropriate antibiotic prophylaxis for cesarean delivery in these patients. Although a single dose of a first-generation cephalosporin may maintain a therapeutic level for approximately 3 to 4 hours in most patients, this may not apply to obese women.
Robinson HE et all in his study demonstrated that moderately obese women with a prepregnancy weight of 90 to 100 kg were 1.6 times more likely to have a wound infection (95% CI, 1.31-1.95), whereas severely obese women (. 120 kg) were 4.45 times more likely to have a wound infection (95% CI, 3.00- 6.61).13 Given the increased amount of poorly perfused adipose tissue and the corresponding increased volume of distribution in obese patients, pharmacokinetic studies suggest that a higher dose of antibiotic prophylaxis be administered in these patients. (3)
meta-9
analysis of six studies (13.4% vs 6.6%, pooled odds ratio 2.06; 95% CI, 1.43-2.98).23 However, both closure techniques have been shown to be equivalent with regard to postoperative pain, cosmetic outcome, and patient satisfaction. (5)
Smaill FM, Grivell RM. In Cochrane date base review concluded that Compared with placebo or no treatment, the use of prophylactic antibiotics in women undergoing cesarean section reduced the incidence of wound infection, endometritis and serious infectious complications by 60% to 70%. (6)
G Justus Hofmeyr, Fiona M Smaill Use of prophylactic antibiotics in women undergoing cesarean section substantially reduced the incidence of episodes of fever, endometritis, wound infection, urinary tract infection and serious infection after cesarean section. Wound infections were also reduced: for elective cesarean section (n = 2015) RR 0.73 (95% CI 0.53 to 0.99); for non-elective caesarean section (n = 2780) RR 0.36 95% CI 0.26 to 0.51]; and for all patients (n = 11,142) RR 0.41 (95% CI 0.29 to 0.43). (7)
10
Huskins, W. C., Ba-Thike, K et all concluded that Prophylaxis was used widely, but only few centers administered prophylaxis to all women. Ampicillin and cefazolin were the principal antibiotics used, but broad-spectrum agents and multidrug regimens were also used commonly. (9)
Norman L. Meyer et all in the study Cefazolin versus Cefazolin plus Metronidazole for Antibiotic Prophylaxis at Cesarean Section concluded that Antibiotic prophylaxis with metronidazole and cefazolin results in fewer postoperative infections, decreased duration of hospitalization, and lower medication cost than cefazolin alone. (10)
J Shetty, S Rajshekhar, A Kamath t two doses of amoxicillin-clavulanic acid is equally effective as triple dose therapy in reducing post cesarean section endometritis. This implies that two dose regimen would decrease the cost to the patient while maintaining very acceptable infection rates. (11)
11
Peter Jakobi et all concluded that Outcomes of febrile morbidity (18% vs 12%) and particularly morbidity caused by endometritis (6% vs 8%, respectively) were similar for single-dose and three-dose groups. In the untreated low-risk group there were no cases of endometritis and the febrile morbidity was comparable to that of the prophylactically treated groups (14% vs 15%). Single-dose cefazolin prophylaxis appears to be comparable to multidose prophylaxis in reducing febrile morbidity after cesarean section. (13)
A.J.M. Roex et in their study the three-dose group showed fewer postoperative infections: as to wound infections (p < 0.05) and therapeutic antibiotic use (p < 0.025) these differences were statistically significant. The numbers of days of hospitalization after the caesarean section also showed differences: 10.6 _t 2.6 versus 9.8 f 1.5 days in the one- and three-dose groups respectively (p < 0.05). It is concluded that, contrary to several reports in the literature, prophylaxis consisting of three administrations of cefoxitin is to be preferred. (14)
12
Stiver HG et all concluded that the The aerobic and anaerobic cervical microflora was determined before operation and on day 4 after operation in groups of women undergoing a clinical trial of prophylaxis with three doses of cefoxitin, cefazolin, or placebo for infectious complications of nonelective cesarean section. Floral shifts occurred post partum, with return of Escherichia coli and Bacteroides fragilis and a decrease in Candida colonization. No significant differences in flora existed preoperatively among patients receiving cefoxitin, cefazolin, or placebo, but by day 4, both antibiotic groups had greater enterococcal colonization. This difference was more marked with cefoxitin than with cefazolin. No difference in E. coli or B. fragilis colonization was noted by day 4 in placebo and antibiotic groups. Resistance developing in isolates in the antibiotic groups was mainly a result of enterococcal colonization. Results of this study indicate that a three-dose cephalosporin prophylactic regimen resulted in a significant selection of resistant enterococcal colonization but there was no increase in nosocomial infection in the antibiotic groups compared to the placebo group. There did not appear to be significant differences in either species selection or antibiotic resistance of aerobic or anerobic microflora between the cefoxitin and cefazolin groups. (17)
13
14
15
History of asepsis
Proper control of wound disease developed around two key moments: the adoption of antiseptic practices from the 1860s and the discovery of antibiotics from the late 1930s.
Early Wound Management
The earliest known attempts to access the dead date to circa 10,000 BC. Skulls collected all through the world show the square and round marks left by the ancient “healers” who ground and scraped the skull with sharpened instruments. Some people survived, as evidenced by the smoothed edges of few Neolithic skulls found in East Africa. Nevertheless, it may be assumed that the mortality and morbidity rates were very high and cannot be accepted to modern standards.
16
Pre-Listerian Philosophies
The growth of medical texts originating from the Golden Age of Greece would provide rules for the practice of medicine for 2000 years. But because of the intellectual stringency of the medical society, spread of ideas, principles and practices of the Greeks would remain idle for the next 2000 years.7 Every few 100 years, bold men dedicated to the principles and the practice of medical arts would challenge the false allegations and even bring out verifiable and acceptable data to support their claims, but their ideas would not make necessary influence to cause change. In the art of wound healing, two problems would be repeated problems: first, the role of pus; and second, the origin and spread of infection.
Laudable Pus
Hippocrates (circa 460–370 BC) was the first to hold an opinion on pus discharge, saying that the formation of pus was not a natural component in the healing process and should be avoided. Similar to ideas of the Sumerians he management protocol involved: cleansing with alchoholic wine, applying a bandage, and then pouring alchoholic wine on the bandage. (22) Claudius Galen (circa A.D. 130–200), a surgeon to the gladiators in Pergamum, idealized Hippocrates and championed Hippocratic doctrines in the practice of medicine.
17
medical practice until the era that is the modern era. Many of his ideas proved to be correct; however, one very important assumption was terribly false: the formation of pus was an important part of wound healing. This idea was aberration from the Hippocratic principles and practice is one that would haunt surgeons and stop the surgical progress till Listers. (19) 1000 years after, Theodoric Borgognoni of Cervia (1205–1298) contradicted Galen’s view of the laudable pus.
18
Transmissibility of Infectious Agents
Another issue that proved elusive to science before the 19th century was the origin and transmissibility of infection, Hieronymus Fracastorius (1478–1553) came up the idea that the cause of infectious disease was from invisible living seeds (seminaria contagionum). In his work, “De contagione,” published in 1546, he described three modes of disease spread: direct contact with infected persons, indirect contact with fomites, and airborne transmission.
Ambroïse Paré (1510–1590), considered the father of modern surgery, similarly believed infection was introduced from the environment. Furthermore, others after Fracastorius and Paré correctly noted the importance of a sterile environment in the prevention of disease transmission.
19
placed into the patients wound. (9) The surgical residents would also be encouraged to place their hands also for the “feel”. Surgeons boots would be used to sharpen the surgical instruments and little or no regard was given to cleanliness or sterility of the instruments, these instruments will be wiped with dirty cloths and the placed back into their velvet carriers and reused. The ground of the post-operative wards will be covered with human excrement, blood, suppuration and the hospital walls splashed with sputum. All these lead to mortality rate of nearly 50%. Consequently, the major cause death will be infections and eighty percentage of the operations afflicted with the so called “hospital gangrene”. (10)
The bad odour of dead bodies and infectious leftovers made some to believe that purulent wounds were caused by particles in the air or bad “humors.” In 1880, William Halsted reportedly operated in tents outside of Bellevue Hospital for better ventilation. (35) The prevailing view was that if infectious particles did exist, then they arose by spontaneous generation.
Infectious Disease and Antisepsis
20
which follow severe injuries are due to the irritating and poisoning influence of decomposing blood or sloughs.” Lister started using carbolic acid on fracture wounds. The wound healed with no signs of suppuration, this leading to averting of amputation, and the mortality rate from amputation came down from 45 to 15%. (3)
21
Advancements in Asepsis
Improving on listerian practices, in 1891 Ernst von Bergmann introduced heat sterilization of instruments, which proved better to chemical sterilization. In 1883 Gustav Neuber of Kieland introduced sterile gowns and caps. and Mikulicz, surgicals caps in 1897. (28) The use of rubber gloves became widespread after 1890 when William Stewart Halsted (1852–1922; Fig. 3) commissioned the Goodyear rubber company to fashion gloves for his nurse to protect her hands from the mercuric chloride solutions used to disinfect the instruments. (31)
Introduction.
22
and are more difficult to treat because therapeutic options are limited. Antibiotic resistance development mainly due to the inappropriate use of antibiotics. Incomplete courses of antibiotic therapies and the unnecessary use of broader spectrum regimens play a role. In addition to antibiotic prophylaxis, it is essential to review all factors that affect infectious risk reduction in obstetrical care. Proper and appropriate skin preparation procedure, which includes hair clipping as opposed to shaving, and effective asepsis of both patient and staff are required. Sterile surgical fields must be ensured, and ongoing quality assessment of sterilization technique, air ventilation, and postoperative wound care is needed. Consistent infection control surveillance and reporting of infectious complications track ability to minimize these morbidities and possibly to identify clusters of infection and the emergence of antibiotic resistant organisms. This will dictate changes to operative routines to respond to evolving microbial diversity that seems inevitable.
23
must be evidence that it reduces postoperative infection. It must also be safe and inexpensive, and it must be effective against organisms likely to be encountered in the surgical procedure. The agent must be administered in a way that ensures that serum and tissue levels are adequate before an incision is made and that therapeutic levels of the agent can be maintained in serum and tissue during surgery and for a few hours (atmost) after the incision is closed. Wound infections—surgical site infections—in the form of cellulitis, abscess, or dehiscence can occur following laparotomy. Pelvic infections, such as an abscess or infected hematoma, are a risk with any surgical procedure that enters the abdominal cavity. Cuff cellulitis is a specific risk for hysterectomy. Endometritis can result from Caesarean section or surgical abortion. Urinary tract infections can occur as a result of any procedure that involves catheterization of the bladder.
A 1999 guideline published by the US Centers for Disease Control and Prevention lists the specific and stringent criteria that must be met for diagnosis of a surgical site infection. Accurate surveillance for SSI monitoring requires followup for 30 days postoperatively, and the trend towards early discharge from hospital makes surveillance a challenge. It is estimated that up to 84% of surgical site infections occur following discharge from hospital.
If prophylactic antibiotics are to be given, they should administered shortly prior to or at bacterial inoculation.
24
half-life of the drug. It has also been suggested that with large blood loss (> 1500 mL), a second dose should be given.
The single most important risk factor for postpartum maternal infection is Caesarean section. Women having Caesarean section have a 5- to 20-fold greater risk of infection than women having vaginal delivery. Rates of wound infection and serious infectious complications can be as high as 25%. There is no consistent application of definitions for SSI, and the practice of post-discharge surveillance varies widely. A recent prospective study with proper application of CDC definitions for surgical site infection with follow up to 30 days post-Caesarean section identified a wound infection rate of 8.9%. It is likely that post- Caesarean wound infection rates are inaccurate, because up to 84% of infections occur after discharge, when surveillance may be lacking.
Endomyometritis, urinary tract infection, wound infection, and sepsis may occur following Caesarean section. Numerous studies have investigated the use of prophylactic antibiotics to reduce these complications, the rates of which are all higher in the case of emergency Caesarean section, with or without the presence of maternal fever and/or chorioamnionitis.
25
the risk of wound infection (RR 0.36; 95% CI 0.26 to 0.51 and RR 0.73; 95% CI 0.53 to 0.99).
There has been debate about the benefit of prophylactic antibiotics for a woman who has an elective Caesarean section with intact membranes and without labour. A meta-analysis of 4 studies found that antibiotic prophylaxis resulted in a decrease in postoperative fever (RR 0.25; 95%CI 0.14 to 0.44) and endometritis (RR 0.05; 95% CI 0.01 to 0.38).
Taken together, these data support the recommendation to use prophylactic antibiotics for all women undergoing Caesarean section.
Controversy also exists about whether prophylactic antibiotics in Caesarean section should be given prior to skin incision or at the time of the umbilical cord clamping. Traditionally, prophylaxis has been delayed in an effort to avoid masking a neonatal infection and to prevent an unnecessary septic work-up. However, recent evidence may change this practice.
A randomized trial compared maternal infectious and
Post-partum fever
26
Postpartum patients are frequently discharged within a couple days following delivery. The short period of observation may not afford enough time to exclude evidence of infection prior to discharge from the hospital. In one study, 94% of postpartum infection cases were diagnosed after discharge from the hospital.
1. Postpartum postsurgical wound infections, 2. perineal cellulitis,
3. mastitis,
4. respiratory complications from anaesthesia, 5. retained products of conception,
6. urinary tract infections (UTIs), and 7. Septic pelvic phlebitis.
Fever is defined as a temperature greater than 38.0°C on any 2 of the first 10 days following delivery exclusive of the first 24 hours. The presence of postpartum fever is generally accepted among clinicians as a sign of infection that must be determined and managed.
Local spread of colonized bacteria is the most common aetiology for postpartum infection following vaginal delivery. Endometritis is the most common infection in the postpartum period.
Other postpartum infections include
Wound infection is more common with caesarean delivery.
27
Flank pain, dysuria, and frequency of UTIs
Erythema and drainage from the surgical incision or episiotomy site, in cases of postsurgical wound infections
Respiratory symptoms, such as cough, pleuritic chest pain, or dyspnea, in cases of respiratory infection or septic pulmonary embolus
Fever and chills
Abdominal pain
Foul-smelling lochia
Breast engorgement in cases of mastitis.
Endometritis
Endometritis is inflammation of the endometrial lining of the uterus. In addition to the endometrium, inflammation may involve the myometrium and, occasionally, the parametrium.
Endometritis can be divided into pregnancy-related endometritis and endometritis unrelated to pregnancy.
The diagnosis of endometritis is usually based on clinical findings, such as fever and lower abdominal pain (see Clinical Presentation).
28
Infection of the endometrium, or decidua, usually results from an ascending infection from the lower genital tract. From a pathologic perspective, endometritis can be classified as acute versus chronic. Acute endometritis is characterized by the presence of neutrophils within the endometrial glands. Chronic endometritis is characterized by the presence of plasma cells and lymphocytes within the endometrial stroma.
Chronic endometritis in the obstetric population is usually associated with retained products of conception after delivery or elective abortion. In the nonobstetric population, chronic endometritis has been seen with infections (eg, chlamydia, tuberculosis, bacterial vaginosis) and the presence of an intrauterine device. The intrauterine device as a factor in the etiology of pelvic inflammatory disease was associated with early forms of the device, in particular, the Dalkon Shield. The incidence of pelvic inflammatory disease is not higher in users of modern intrauterine devices than in non-users.
Genital tract infections
Increased risk of genital tract infections is related to the duration of labor (ie
prolonged labor increases risk of infection), use of internal monitoring devices,
and number of vaginal examinations.
Genital tract infections are generally polymicrobial. Gram-positive cocci
29
organisms involved. Escherichia coli and gram-positive cocci are commonly
involved aerobes.
Mastitis
The most common organism reported in mastitis is Staphylococcus aureus. The
organism usually comes from the breastfeeding infant's mouth or throat.
Thrombosis may occur. Numerous factors cause pregnant and postpartum women
to be more susceptible to thrombosis. Pregnancy is known to induce a
hypercoagulable state secondary to increased levels of clotting factors. Also,
venous stasis occurs in the pelvic veins during pregnancy.
Although relatively rare, septic pelvic thrombosis is occasionally observed in the
postpartum patient, who might have fever.
Urinary tract infections
Bacteria most frequently found in UTIs are normal bowel flora, including E
coli and Klebsiella, Proteus, and Enterobacter species.
Any form of invasive manipulation of the urethra (eg, Foley catheterization)
increases the likelihood of a UTI.
Septic pelvic thromphophelbitis
Septic thrombophlebitis is a condition characterized by venous thrombosis,
inflammation, and bacteremia.The clinical course and severity of septic
thrombophlebitis are quite variable. Many cases present as benign, localized
venous cords that resolve completely with minimal intervention. Some cases
30
refractory to aggressive management, including operative intervention and
intensive care. A number of distinct clinical conditions have been identified,
depending on the vessel involved, but all thrombophlebitides involve the same
basic pathophysiology. Thrombosis and infection within a vein can occur
throughout the body and can involve superficial or deep vessels.
The approach to treatment of septic phlebitis depends on which structures are
involved, the underlying aetiology of the phlebitis, the causative organisms, and
the patient's underlying physiology. Peripheral septic thrombophlebitis is a
common problem that can develop spontaneously but more often is associated with
breaks in the skin. A frequent complication is embolization of infected thrombus
to distant sites, most commonly the lungs, leading to septic pulmonary emboli,
hypoxia, sepsis, and often death. Septic phlebitis of the deep venous system is a
rare, but life-threatening, emergency that may fail to respond to even the most
aggressive therapy.
Septic thrombophlebitis of the IVC or SVC is primarily the result of central venous
catheter placement, with increased incidence in burn patients and those receiving
total parenteral nutrition.Patients are generally very ill appearing with high fever,
and they may also have signs of venous occlusion, including arm and neck edema.
The mortality rate of these infections is high, but cases of successful treatment
have been reported.]
31
parenteral antibiotic therapy in the absence of an undrained abscess or infected hematoma. The development of SPT is enhanced by venous stasis (e.g., obesity, diabetes), vascular injury, or bacterial contamination of pelvic vessels.
Two forms of Septic thrombophlebitis have been described. The classic form is seen in association with abdominal surgery. This form occurs 2 to 4 days after surgery and is characterized by fever, tachycardia, gastrointestinal distress, unilateral abdominal pain, and, in 50% to 67% of cases, a palpable abdominal cord resulting from acute thrombus formation.
The enigmatic form complicates parturition or pelvic surgery and is characterized by spiking temperatures despite clinical improvement on antibiotics; tachycardia during the temperature spikes; and small, diffusely scattered thrombi in small pelvic vessels. Pelvic findings are minimal in both forms. The diagnosis often may be confirmed by CT scan or magnetic resonance imaging (MRI).
33
Pelvic abscess
The patient who develops fever and abdominal and pelvic pain late in the postoperative hospital course or after hospital discharge may have a pelvic abscess, possibly of ovarian origin. If there is a sudden increase in abdominal or pelvic pain, a rupture may have occurred. A ruptured abscess should be managed as a surgical emergency, proceeding to a laparoscopy or a laparotomy with excision or drainage of the infected mass. The inciting site for an ovarian abscess is a place of recent follicle expulsion or a site of surgical trauma to an ovary in a premenopausal woman. Once again, anaerobes are the predominant bacteria in a pelvic abscess.
34
amenable to a laparoscopic approach with incision and drainage. Copious irrigation and suctioning are critical if this approach is chosen.
35
Ultrasound imaging showing collection in the pouch of Douglas.
Wound infection
The Centers for Disease Control and Prevention (CDC) definitions of surgical
wound infection were modified by Horan et al. This system divides infections into
two major categories: (a) an organ/space surgical site infection (SSI) and (b)
superficial and deep incision infection. An SSI may be in any anatomic area that
was opened or manipulated during a surgical procedure other than the incision
itself. This would include most of the infections that develop after hysterectomy.
It must develop within 30 days of the procedure and be accompanied by one of the
following: diagnosis by a surgeon or attending physician; an abscess or other
evidence of infection identified during reoperation or by radiologic or
histopathologic examination; aseptically obtained organ/space fluid or tissue, the
culture of which resulted in bacterial isolates; or purulent drainage from a drain
36
Surgical wound classification
Class I
Clean
An uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tract is not entered. In addition, clean wounds are primarily closed and, if necessary, drained with closed drainage. Operative incisional wounds that follow nonpenetrating (blunt) trauma should be included in this category if they meet the criteria.
Class II
Clean-contaminated
37
Class III
Contaminated
Open, fresh, accidental wounds. In addition, operations with major breaks in sterile technique (e.g., open cardiac massage) or gross spillage from the gastrointestinal tract, and incisions in which acute, nonpurulent inflammation is encountered are included in this category.
Class IV
Dirty-infected
Old traumatic wounds with retained devitalized tissue and those that involve existing clinical infection or perforated viscera. This definition suggests that the organisms causing postoperative infection were present in the operative field before the operation.
Wound Cellulitis
38
staphylococci, and streptococci cause most of these infections. If wound cellulitis fails to improve, the possibility of resistant organism infection, such as MRSA, or occult abscess should be considered.
Wound Seroma
A collection of serous fluid beneath the skin surface is a seroma. A small
amount of serous drainage may be managed with limited opening of the incision,
drainage, and cleansing. Larger collections may require more extensive incision
and drainage. Antibiotic therapy is not necessary with an uninfected seroma. If a
seroma intermittently or continuously leaks, it may become infected and require
antibiotic therapy.
Deep Wound Infection
When purulent drainage is noted, the wound should be opened widely to allow
drainage and removal of necrotic tissue. The incision should be probed gently
evaluate fascial integrity. If the fascia is intact, healing is hastened by mechanical
debridement followed by loose, wet-to-dry packing with gauze moistened with
saline; dilute hydrogen peroxide (1:1 mixture with saline) or Dakin's solution,
0.5%. Povidone-iodine is to be discouraged because it does not promote the
development of granulation tissue. An antibiotic effective against anaerobes such
as piperacillintazobactam, metronidazole, or a carbapenem must be used.
Evisceration of bowel may occur if the infection involves the fascia. This is a
surgical emergency requiring identification of the defect, freshening of the fascial
39
reinforced closure of the fascia. Some surgeons leave the skin open for delayed
closure; others close it primarily.
Necrotizing Fasciitis
This severe complication results from synergistic bacterial infection of the
fascia, subcutaneous tissue, and skin. This rapidly progressive infection is initially
characterized by pain and toxicity out of proportion to physical findings with
subsequent development with cutaneous necrosis and haemorrhagic bullae.
Perineal necrotizing fasciitis is commonly caused by group A, beta-haemolytic
streptococci, but may be a polymicrobial, synergistic infection with anaerobic
bacteria or Clostridium perfringens. Methicillin-resistant Staphylococcus aureus
has been increasingly identified as a causative agent, and empiric IV antibiotics
may be needed to cover this organism, pending culture data. Diabetes, alcoholism,
and immune compromise all represent significant risk factors for development of
necrotizing fasciitis. Patients usually present with severe pain in the area of
involvement; clinical signs of sepsis; and a viscous, cloudy, malodorous drainage.
The wound edges may be purple or even necrotic. If gangrene occurs in the area
of fasciitis, bullae of the skin and crepitus in the subcutaneous tissue may occur.
Necrotizing fasciitis carries a high mortality potential and may be initially difficult
to recognize. Therefore, a high index of suspicion must be maintained. Although
C/T and MRI scans may be of benefit in the diagnosis of necrotizing fasciitis,
aggressive surgical intervention/exploration and antibiotic therapy with activity
against beta-hemolytic streptococci, anaerobes, enteric gram-negative bacilli, and
40
Parametrial Phlegmon
For some women in whom metritis develops following caesarean delivery,
parametrial cellulitis is intensive and forms an area of induration—a phlegmon—
within the leaves of the broad ligament These infections should be considered
when fever persists longer than 72 hours despite intravenous antimicrobial
therapy. Phlegmons are usually unilateral, and they frequently are
limited to the parametrium at the base of the broad ligament. If the inflammatory
reaction is more intense, cellulitis extends along natural lines of cleavage. The
most common form of extension is laterally along the broad ligament, with a
tendency to extend to the pelvic sidewall. Occasionally, posterior extension may
involve the rectovaginal septum, producinga firm mass posterior to the cervix. In
most women with a phlegmon, clinical improvement follows continued treatment
with a broad-spectrum antimicrobial regimen. Typically, fever resolves in 5 to 7
days, but in some cases, it persists
longer. Absorption of the induration may require several days to weeks.
In some women, severe cellulitis of the uterine incision may lead to necrosis and
separation. Extrusion of purulent material leads to intraabdominal abscess
formation and peritonitis as described above. Surgery is reserved for women in
whom uterine incisional necrosis is suspected because of ileus and peritonitis.
For most, hysterectomy and surgical debridement are needed and are predictably
difficult because the cervix and lower uterine segment are involved with an intense
inflammatory process that extends to the pelvic sidewall. The adnexa are seldom
41
There is often appreciable blood loss, and transfusion may be necessary.
Right sided parametrial phelgmon
Necrotic hysterotomy infection. Severe cellulitis of the uterine incision
42
Necrosis of the uterine incision with gas in the myometrium
Bacteraemia
Infection of the bloodstream can complicate any pelvic infection but is seen
more frequently in association with abscesses, peritonitis, and SPT. Antibiotics
effective against the isolated organism should be used. Duration of therapy for
gram-negative bacteraemia should be 7 to 14 days. Parenteral antibiotics should
be used initially but may be converted to oral if improvement has occurred and the
patient has been afebrile for 24 to 48 hours. Antibiotic duration for S. aureus
bacteremia should be 2 to 6 weeks of parenteral antibiotics due to the frequency
of metastatic infection with serious sequelae, including endocarditis. Infectious
disease consultation should be considered for S. aureus bacteremia or fungemia
due to the high risk of serious secondary complications. Therapeutic intervention
43
Risk Factors for Postoperative Caesarean Infections.
The pathogenesis and mechanism of Cesarean infection varies by different
patient risk groups. Cesarean infections can occur through wound contamination
from skin flora or from intra-uterine seeding from vaginal flora. They can present
as wound infections, endometritis or intra-abdominal abscesses.
In a retrospective cohort study at a large academic hospital (n = 2739) with 178
postoperative SSIs, risk factors included resident physician practitioner, American
Society of Anesthesiologists (ASA) class more than 3, chorioamnionitis, and
tobacco use. Cesarean sections performed for nonreassuring fetal status were
associated with lower rates of infection.This study was limited in that vaginal
antiseptic preparation and adjunctive azithromycin were not used at this center and
there was provider variability regarding use of staples and subcutaneous tissue
closure, which are known to impact infection rates.
Another retrospective review at a large academic health system found labor arrest,
preterm labor, use of general anesthesia, increased BMI, asthma and smoking were
associated with higher rates of SSI. A case control study at a rural tertiary medical
center identified 218 infections over 6 years using coding data, higher BMI, fewer
years of education, increasing number of prior births, tobacco use, hypertension,
gestational diabetes and emergency Cesarean sections were found to be significant
risk factors for SSI. All patients in this study were in labor or had ruptured
membranes for greater than 4 h.
A secondary analysis of a multicenter clinical trial (n = 2013, 177 SSI) that
44
patients, black race, younger age, nontransverse uterine incision, membrane
rupture greater than 6 h and surgery duration greater than 49 min were associated
with higher rates of SSI.
Risk factors for SSI in resource-limited settings differ somewhat from developed
countries. In Ethiopia, a random sample of a non concurrent cohort of mothers in
labor greater than 24 h revealed that prolonged rupture of membranes, greater
number of vaginal exams, prolonged duration of surgery, wound contamination,
low hemoglobin and junior staff performing the procedure were risk factors for
the development of Cesarean section SSI. In Brazil, in a small case controlled
study (n = 79 SSI cases), duration of membrane rupture was the only independent
risk factor for post Cesarean SSI.
Obese women are at a higher risk for wound complications, SSI, endometritis and
wound related hospital readmission. The rate of complications increases with
greater BMI. Women with very high BMI more than 50 had similar odds of SSI
compared to women with a BMI between 40 and 49, but the odds ratio of wound
separation was 6 times greater in the women with a BMI more than 50.
Based on these studies, increased BMI, gestational diabetes, smoking, emergent
surgery, prolonged labor, rupture of membranes, and prolonged duration and
complexity of surgery are risk factors for SSI. Risk factors vary based on the
different patient populations studied. For example, laboring women with
prolonged rupture of membranes will have different risk factors than women
undergoing elective Cesarean sections as the mechanism of infection is different.
45
variables are collinear and interact with one another. For example, greater number
of vaginal exams is highly associated with duration of labor.
General risk factors
➢ History of cesarean delivery
➢ Premature rupture of membranes
➢ Frequent cervical examination (Sterile gloves should be used in
examinations. Other than a history of caesarean delivery, this risk factor
is most important in postpartum infection.)
➢ Internal fetal monitoring
➢ Pre-existing pelvic infection including bacterial vaginosis
➢ Diabetes
➢ Nutritional status
47
CEPHALOSPORINS
Beta-lactam antibiotics are among the most commonly prescribed drugs, grouped together based upon a shared structural feature, the beta-lactam ring. Cephalosporins cover a broad range of organisms, are generally well-tolerated, and are easy to administer; thus, these agents are frequently used beta-lactam drugs.
CLASSIFICATION OF CEPHALOSPORINS —
49
First generation — Cephalothin is the oldest of the first-generation cephalosporins and was previously used as the prototype of this group. Cephalothin was active against most gram-positive cocci (including penicillinase-producing staphylococci), but did not have clinically useful activity against enterococci, Listeria, methicillin-resistant staphylococci, or penicillin-resistant pneumococci.
Cephalothin was active against most strains of Escherichia coli, Proteus mirabilis, and Klebsiella pneumoniae, but had little activity against indole-positive Proteus, Enterobacter, Serratia, and the non-enteric gram-negative bacilli such as Acinetobacter spp and Pseudomonas aeruginosa. Gram-negative cocci (such as the gonococcus and meningococcus) and H. influenzae were generally resistant. Cephalothin was active against most of the common anaerobic pathogens, with certain exceptions such as Bacteroides species, particularly B. fragilis.
Cefazolin has a similar spectrum of activity to cephalothin, is available worldwide, and is now the only parenteral first-generation cephalosporin available in the United States. Cefazolin achieves substantially higher serum levels than cephalothin, and has a longer half-life of elimination. Cefazolin is less stable than cephalothin in vitro to the type A penicillinase of staphylococci; the relevance of this for clinical therapy, however, is not certain.
50
contrast, they have greater activity against certain gram-negative bacilli; specifically, one subgroup of second-generation cephalosporins has enhanced activity against H. influenzae and another, the cephamycins, has activity against Bacteroides.
Activity against Haemophilus influenzae — In the first subgroup, cefuroxime is available parenterally and orally, and is more active than cefazolin in vitro against strains of Enterobacter and indole-positive Proteus. However, this agent induces the AmpC chromosomal beta-lactamases of these organisms, leading to resistance and failures of clinical therapy.
Cefuroxime is also more active than cefazolin against H. influenzae, and cefuroxime is quite stable to the TEM beta-lactamase in ampicillin-resistant strains. Although cefuroxime is approved for the therapy of H. influenzae meningitis, delayed responses and treatment failures have occurred, and a third-generation cephalosporin is now preferred for therapy of meningitis due to ampicillin-resistant strains. Cefuroxime is also highly active against beta-lactamase producing Moraxella catarrhalis.
51
by induction of chromosomal cephalosporinases of these species and selection of stably derepressed mutants.
Unlike the first-generation cephalosporins, the cephamycins are active against many strains of Bacteroides. The combination of activity against common aerobic and facultative gram-negative bacilli plus Bacteroides has led to the use of the cephamycins in the prophylaxis and therapy of infections in the abdominal and pelvic cavities (where these organisms predominate) (37). The cephamycins have no clear advantages over the first-generation cephalosporins for infections outside of the abdominal and pelvic areas.
Third generation — The third-generation cephalosporin class (38) is marked by stability to the common beta-lactamases of gram-negative bacilli, and these compounds are highly active against Enterobacteriaceae (E. coli, Proteus
mirabilis,
52
infections due to these bacteria can lead to the emergence of resistance during therapy.
The third-generation cephalosporins are less active against most gram-positive organisms than the first-generation cephalosporins and are inactive against enterococci, Listeria, methicillin-resistant staphylococci, and Acinetobacter. Cefotaxime and ceftriaxone are usually active against pneumococci with intermediate susceptibility to penicillin, but strains fully resistant to penicillin are often resistant to the third-generation cephalosporins as well.
Treatment with third-generation cephalosporins may be complicated by superinfection (particularly with enterococci or Candida) or by the emergence of resistance on therapy (particularly when used as single agents for Enterobacter, indole-positive Proteus, or P. aeruginosa infections).
Third-generation cephalosporins are not currently recommended for prophylactic use in surgery.
53
Ceftriaxone has the longest serum half-life of this group (6.4 hours) and can be administered once or twice a day. Ceftriaxone has been particularly recommended for the therapy of penicillin-resistant gonorrhea, Lyme disease involving the central nervous system or joints, meningitis due to ampicillin-resistant H. influenzae, and meningitis in children. One of the complications of ceftriaxone therapy, however, has been the formation in the biliary tract of "sludge" composed of ceftriaxone crystals, causing the syndrome of biliary pseudolithiasis (39).
Activity against Pseudomonas — the other of the third-generation cephalosporins, ceftazidime, has activity against P. aeruginosa. Ceftazidime is quite stable to the common plasmid-mediated beta-lactamases and is highly active against Enterobacteriaceae, Neisseria, and H. influenzae. Ceftazidime is also particularly active against P. aeruginosa and is an effective therapy for serious infections due to P. aeruginosa when the organism is resistant to the anti-pseudomonal penicillins or the patient is penicillin allergic. In addition, it is effective therapy for meningitis caused by P. aeruginosa. As with the anti-pseudomonal penicillins, however, ceftazidime should generally be given at least initially in combination with an aminoglycoside for treatment of serious P. aeruginosa infection, when susceptibilities are unknown. Ceftazidime has poor activity against gram-positive organisms and should be reserved for use in infections proven or highly suspected to be due to P. aeruginosa.
54
membrane of gram-negative bacteria and a lower affinity than the third=generation cephalosporins for certain chromosomal beta-lactamases of gram-negative bacilli.
Cefepime has similar activity to cefotaxime and ceftriaxone against pneumococci (including penicillin-intermediate strains) and methicillin-sensitive S. aureus. Like the earlier third=generation agents, it is active against the Enterobacteriaceae, Neisseria, and H. influenzae but has greater activity against the gram-negative enterics that have a broad-spectrum, inducible, chromosomal AmpC beta-lactamase (Enterobacter, indole-positive Proteus, Citrobacter, and Serratia). The role of cefepime in therapy of infections due to stably-derepressed mutants of these organisms has not yet been fully defined, but some data suggest that it may be effective. In a study of 96 patients with infections due to laboratory-confirmed AmpC beta-lactamase producing organisms, 96 percent of the isolates were susceptible to cefepime. Among patients who received cefepime, the 30 day mortality rate and duration of hospitalization were similar to those observed in a matched subset of patients who received meropenem.
55
Despite these potential advantages over third-generation cephalosporins, especially against organisms with inducible, chromosomal resistance, comparative trials of third- and fourth-generation cephalosporins have not yet been performed.
A review by the United States Food and Drug Administration (FDA) of cefepime safety data was initiated in 2007 following findings of a meta-analysis that raised concern regarding increased all-cause mortality associated with cefepime use (risk ratio 1.26, 95% CI 1.08-1.49). The FDA reviewed these study data, conducted additional analyses based on other data, and determined that the data do not indicate a higher rate of death in cefepime-treated patients. Cefepime remains an appropriate therapy for its approved indications (40).
Treatment with cefepime may be complicated by superinfection (particularly with enterococci or Candida). Cefepime use also carries a risk of seizures (specifically nonconvulsive status epilepticus), particularly in patients with renal failure for whom the dose is not appropriately adjusted downwards (41).
56
Enterobacteriaceae, Pseudomonas aeruginosa, Acinetobacter baumannii, or Bacteroides fragilis. Two randomized, double-blind controlled clinical trials have suggested that ceftaroline is noninferior to vancomycin plus aztreonam for treatment of complicated skin and soft tissue infections including those due to MRSA, and to ceftriaxone for therapy of community-acquired pneumonia (42 - 44)
The efficacy of this anti-MRSA cephalosporin is not yet known for hospital-acquired MRSA pneumonia or for bacteraemia.
Ceftobiprole is a cephalosporin available in Canada and some European countries (but not the United States) that is also capable of binding to penicillin binding protein 2a, the protein conferring S. aureus resistance to beta-lactam antibiotics (45). It can also bind penicillin binding protein 2x in penicillin-resistant S. pneumoniae. It has in vitro activity similar to that of ceftazidime or cefepimeagainst Enterobacteriaceae; it also has activity against enterococci. In addition, ceftobiprole appears to have a low potential for selection of resistance.
Cefotaxime
57
Absorption
Peak plasma time: IM, 30 min
Elimination
Half-life: Parent drug, 1-1.5 hr; active metabolite, 1-1.9 hr Excretion: Urine
Metabolism
Partially metabolized in liver
Distribution
Widely distributed to body tissues and fluids, including aqueous humor, ascitic and prostatic fluids, and bone; penetrates CSF when meninges are inflamed.
Metabolite: Desacetylcefotaxime (active)
58
MATERIALS
59
Aims and objective:
To compare the effectiveness of a short course of antibiotics i.e. two doses of Injection cefotaxime 1g IV with the routine long course of antibiotic i.e. 3 days of injection cefotaxime 1g IV BD followed by oral antibiotics and compare the post-operative infective complications in patients who are undergoing elective caesarean section in a Government tertiary care hospital. And also to identify which regimen is superior in regards with to infectious morbidity as febrile morbidity, wound induration, wound discharge, wound gaping and any abnormal vaginal discharge.
Place of study:
This study was conducted in Madras Medical College in the department of Obstetrics’ and Gynaecology.
Study design:
Prospective interventional study
Study Period:
This study was conducted between march 2017 to march 2018 for a period of one year.
Participants:
60
Inclusion criteria:
1) Women who had been booked and immunized OG department of Madras Medical College.
2) Women with regular antenatal check-up.
3) Women who are willing to participate in the study and are consenting.
4) Uneventful antenatal period.
5) Antenatal mothers with no history of pre-existing medical illness. 6) Women undergoing elective caesarean section
Exclusion criteria:
1) Hypertensive disorder
2) Any antibiotic treatment 2 weeks prior to surgery. 3) Presence of PROM
4) Diabetes 5) Anaemia
6) Obesity (BMI >25)
7) Immuno-compromised state
8) Prolonged preoperative hospitalization 9) Women allergic to injection cefotaxime Method of Study
61
After careful history taking and examination and ruling out any pre-existing medical disorders, history of infections, history of prior hospital admissions and prior antibiotic administration the women were carefully selected and the
randomized into two groups.
The women were explained about the nature of the study, the study outcome and written informed consent was obtained.
A test dose of injection Cefotaxime was administered intradermally in the forearm to test for any allergies. Patients allergic to injection cefotaxime were excluded from the study.
The women in group 1 were given inj. cefotaxime 1 gm I.V. within one hour of commencement of surgery, the dose is repeated if surgery lasted for more than two hour. Another dose is given 12 hours after the 1st dose in same patient. This is considered the short course regimen.
The women in group 2 were given inj. cefotaxime 1 gm I.V. twice a day for 3 days. Thereafter Tablet cefixime 200mg 3 to 5 days. This was considered as the long course regime.
62
Standard definions
Standard febrile morbidity: oral temperature of > 38.0 o C (100.4” F) for at least 24 h, excluding the first 24 h after operation.
Endometritis: fever, foetid lochia And or uterine tenderness on pelvic examination.
63
RESULTS
AND
64
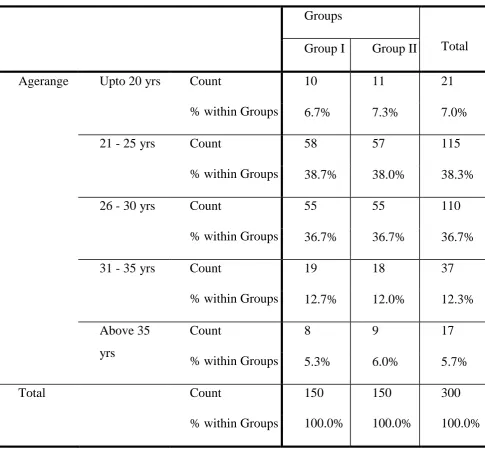
[image:69.595.75.561.158.611.2]Age distribution among the two sudy groups Table 1
Groups
Total Group I Group II
Agerange Upto 20 yrs Count
% within Groups
10 11 21
6.7% 7.3% 7.0%
21 - 25 yrs Count
% within Groups
58 57 115
38.7% 38.0% 38.3% 26 - 30 yrs Count
% within Groups
55 55 110
36.7% 36.7% 36.7% 31 - 35 yrs Count
% within Groups
19 18 37
12.7% 12.0% 12.3% Above 35
yrs
Count
% within Groups
8 9 17
5.3% 6.0% 5.7%
Total Count 150 150 300
65
66
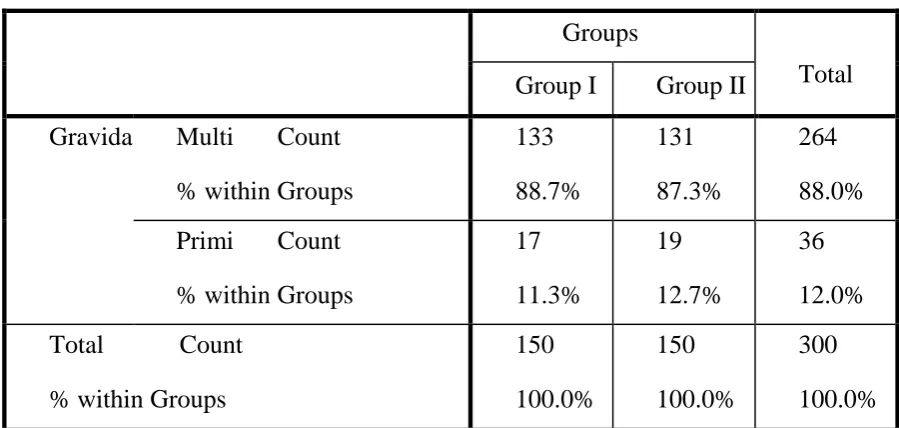
[image:71.595.75.525.159.373.2]Parity group Table 2
Groups
Total Group I Group II
Gravida Multi Count % within Groups
133 88.7%
131 87.3%
264 88.0% Primi Count
% within Groups
17 11.3%
19 12.7%
36 12.0% Total Count
% within Groups
150 100.0%
150 100.0%
300 100.0%
A total of 300 patients were recruited for the study with 150 patients in group 1 and 150 patients in group 2.
67
Graph 2
68
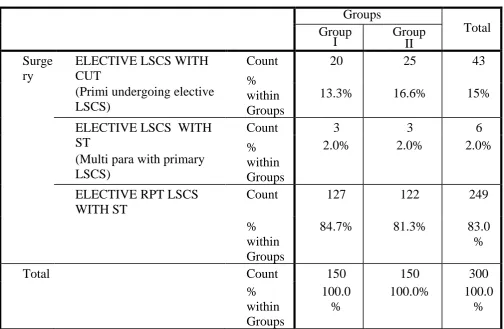
[image:73.595.79.584.199.528.2]Type of surgery Table 3
Among the 150 patients in group 1, the number of Primi undergoing elective LSCS was 20 (13.3%), the number multi gravida undergoing elective LSCS were 3 (2%) and Number of Multipara with Previous lscs undergoing elective repeat lscs was 127 (84.7%).
Groups
Total Group
I Group II Surge
ry
ELECTIVE LSCS WITH CUT
(Primi undergoing elective LSCS)
Count % within Groups
20 25 43
13.3% 16.6% 15%
ELECTIVE LSCS WITH ST
(Multi para with primary LSCS)
Count % within Groups
3 3 6
2.0% 2.0% 2.0%
ELECTIVE RPT LSCS WITH ST
Count 127 122 249
% within Groups
84.7% 81.3% 83.0
%
Total Count 150 150 300
% within Groups
100.0 %
69
And among the 150 patients in group 2, the number of Primi undergoing elective LSCS was 25 (16.6%), the number multi gravida undergoing elective LSCS were 3 (2%) and Number of Multipara with Previous lscs undergoing elective repeat lscs was 122 (81.3%).
Type of surgery
Graph 3
70
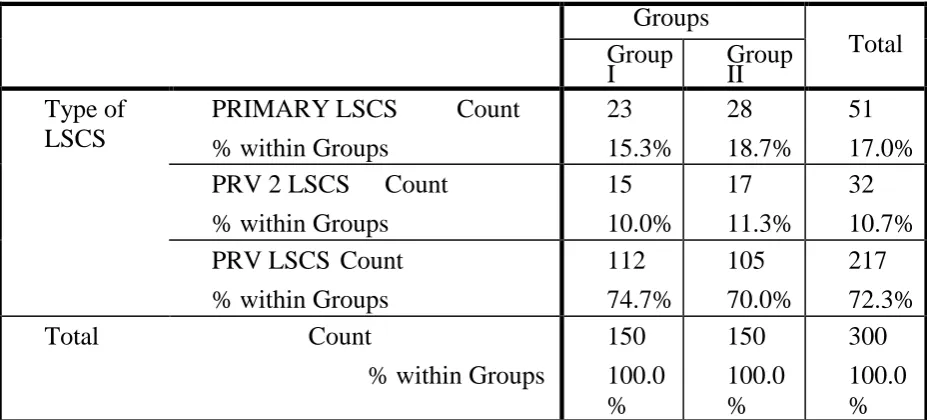
[image:75.595.69.533.132.342.2]TYPE OF LSCS
Table 4
Groups
Total Group
I Group II Type of
LSCS
PRIMARY LSCS Count % within Groups
23 15.3% 28 18.7% 51 17.0% PRV 2 LSCS Count
% within Groups
15 10.0% 17 11.3% 32 10.7% PRV LSCS Count
% within Groups
112 74.7% 105 70.0% 217 72.3%
Total Count
% within Groups
150 100.0 % 150 100.0 % 300 100.0 %
In group 1 the Primary LSCS rate was 15.3% (23), Previous 2 LSCS 10.0% (15) and Previous lscs was 74% (112).
71
The types of LSCS Graph 4
72
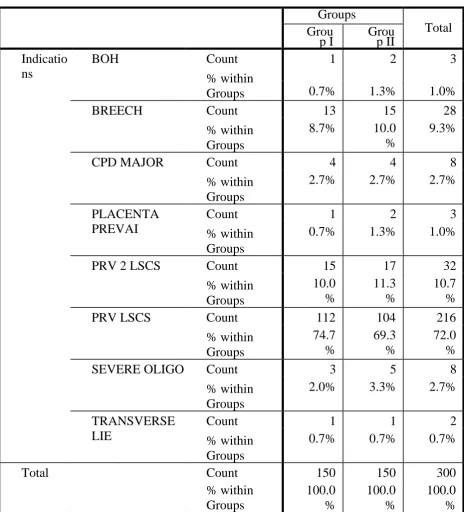
[image:77.595.69.534.162.675.2]Indications for LSCS Table 5
Groups
Total Grou
p I Group II Indicatio
ns
BOH Count
% within Groups
1 2 3
0.7% 1.3% 1.0%
BREECH Count
% within Groups
13 15 28
8.7% 10.0 %
9.3% CPD MAJOR Count
% within Groups
4 4 8
2.7% 2.7% 2.7% PLACENTA
PREVAI
Count % within Groups
1 2 3
0.7% 1.3% 1.0% PRV 2 LSCS Count
% within Groups
15 17 32
10.0 % 11.3 % 10.7 %
PRV LSCS Count
% within Groups
112 104 216
74.7 % 69.3 % 72.0 % SEVERE OLIGO Count
% within Groups
3 5 8
2.0% 3.3% 2.7% TRANSVERSE
LIE
Count % within Groups
1 1 2
0.7% 0.7% 0.7%
Total Count 150 150 300
% within Groups 100.0 % 100.0 % 100.0 %
73
Indications for Elective LSCS within groups Graph 5
74
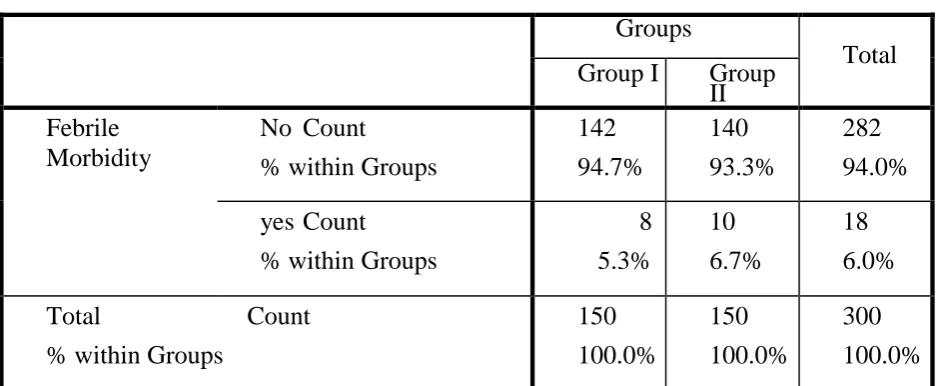
[image:79.595.67.536.157.350.2]Febrile morbidity Table 6
Groups
Total Group I Group
II Febrile
Morbidity
No Count
% within Groups
142 94.7% 140 93.3% 282 94.0% yes Count
% within Groups
8 5.3% 10 6.7% 18 6.0%
Total Count
% within Groups
150 100.0% 150 100.0% 300 100.0%
Fever was noted in a total of 18 patients. In which 8 patients (5.3%) were in group 1 and 10 patients (6.7%) were in group 2. The P value was the above value is 0.6 which is statistically insignificant.
Chi Square tests for the Febrile morbidity – Table No -7
Value df Asymp. Sig. (2-sided) Exact Sig. (2- sided) Exact Sig. (1- sided) Pearson Chi-Square Continuity Correctionb .236a .059 1 1 .627 .808
Likelihood Ratio .237 1 .626 Fisher's Exact
Test
.809 .404
75
Graph 6
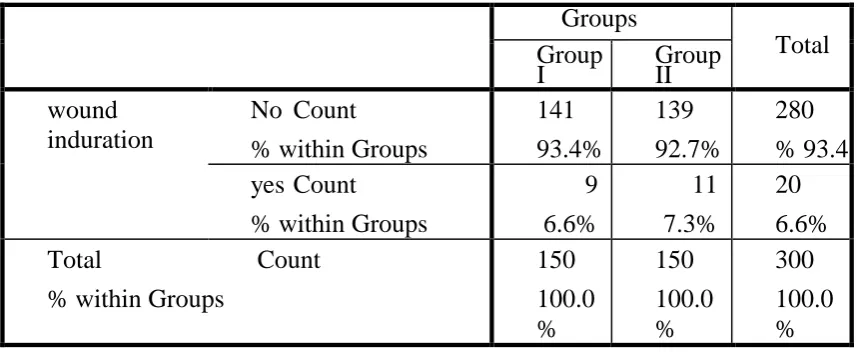
76 Wound Induration Table 8 Groups Total Group
I Group II wound
induration
No Count
% within Groups
141 93.4% 139 92.7% 280 % 93.4 yes Count
% within Groups
9 6.6% 11 7.3% 20 6.6%
Total Count
% within Groups
150 100.0 % 150 100.0 % 300 100.0 %
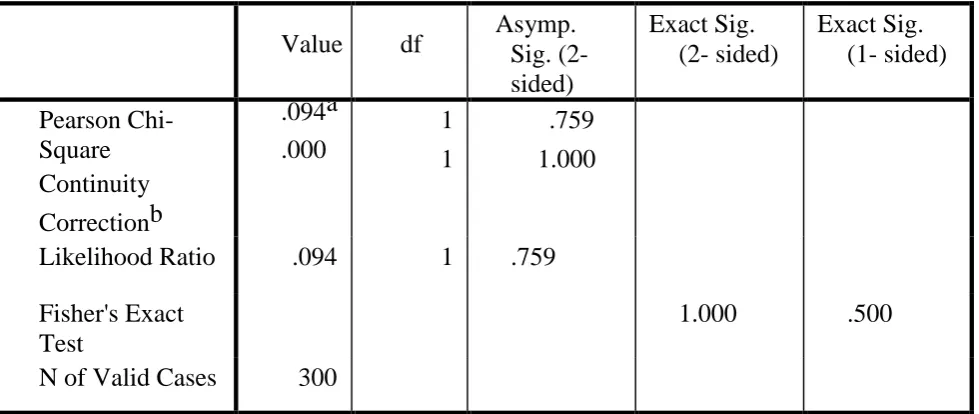
The total number of women with wound induration was 20 of which the 9 (6.6%) were in group 1 and 11 (7.3%) were in group 2 . The p value was 0.09 which is statistically insignificant.
Table No 8 the p Value for the wound induration group 1 and group 2
Value df Asymp. Sig. (2-sided) Exact Sig. (2- sided) Exact Sig. (1- sided) Pearson Chi-Square Continuity Correctionb .094a .000 1 1 .759 1.000
Likelihood Ratio .094 1 .759 Fisher's Exact
Test
[image:81.595.69.535.532.717.2]77
Graph no 7
Pie chart depicting wound induration in group 1 and group 2 .
wound induration
78
[image:83.595.88.539.160.346.2]Serous wound discharge Table 9
Groups
Total Group
I Group II Serous wound
discharge
No Count
% within Groups
145 96.7% 144 96.0% 289 96.3% yes Count
% within Groups
5 3.3% 6 4.0% 11 3.7%
Total Count
% within Groups
150 100.0 % 150 100.0 % 300 100.0 %
Total of 11 (3.7%) patients had serous wound discharge in our study of which 5 (3.3%) were from group 1 and 6 were from group 2. The p Value for the two groups is 0.09 which is statistically insignificant.
Table 10
Value df Asymp. Sig. (2-sided) Exact Sig. (2- sided) Exact Sig. (1- sided) Pearson Chi-Square Continuity Correctionb .094a .000 1 1 .759 1.000
Likelihood Ratio .094 1 .759 Fisher's Exact
Test
1.000 .500
[image:83.595.59.549.512.719.2]79
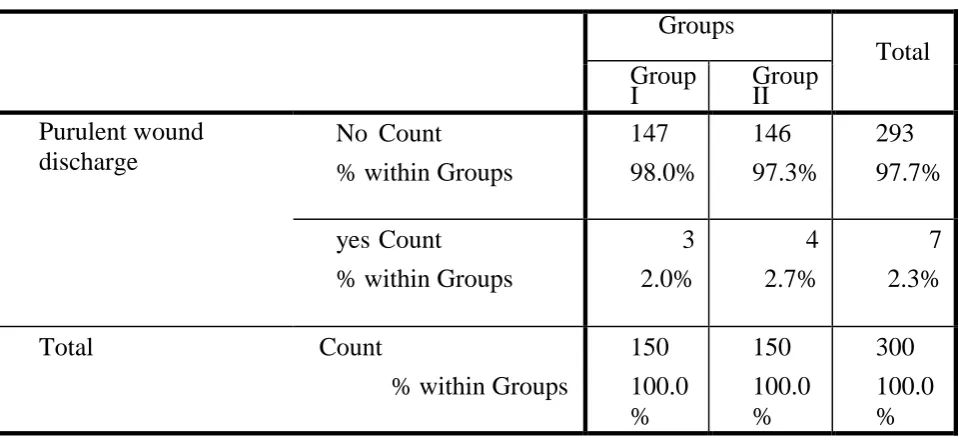
[image:84.595.63.543.189.409.2]Purulent wound discharge
Table 11
Groups
Total Group
I Group II Purulent wound
discharge
No Count
% within Groups
147 98.0% 146 97.3% 293 97.7% yes Count
% within Groups
3 2.0% 4 2.7% 7 2.3%
Total Count
% within Groups
150 100.0 % 150 100.0 % 300 100.0 %
In a total of 300 patients totally 7 (2.3%) patients developed pus discharge out of which 3 (2.0%) were from group 1 and 4 (2.7%) were from group 2. The p value is insignificant for both groups.
Table 12
Value df Asymp. Sig. (2-sided)
Exact Sig. (2- sided)
Exact Sig. (1- sided) Pearson Chi-Square Continuity Correctionb .146a .000 1 1 .702 1.000
Likelihood Ratio .147 1 .702
Fisher's Exact Test 1.000 .500
[image:84.595.48.557.572.745.2]80
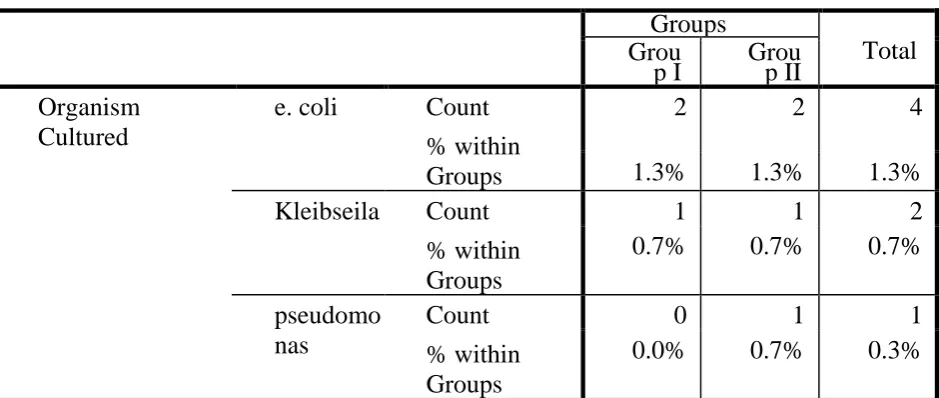
[image:85.595.68.538.220.419.2]Organisms cultured from the wound discharges.
Table 13
Groups
Total Grou
p I Group II Organism
Cultured
e. coli Count % within Groups
2 2 4
1.3% 1.3% 1.3% Kleibseila Count
% within Groups
1 1 2
0.7% 0.7% 0.7% pseudomo
nas
Count % within Groups
0 1 1
0.0% 0.7% 0.3%