“AN
OPEN LABEL PROSPECTIVE STUDY ON URICOSURIC EFFECTS OF LOSARTAN IN HYPERTENSIVE PATIENTS WITHHYPERURICAEMIA”
DISSERTATION SUBMITTED TO
THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY
IN PARTIAL FULFILLMENT FOR THE AWARD OF THE DEGREE OF DOCTOR OF MEDICINE
IN
PHARMACOLOGY
DEPARTMENT OF PHARMACOLOGY TIRUNELVELI MEDICAL COLLEGE
BONAFIDE CERTIFICATE
This
is
to
certify
that
the
dissertation
entitled
“AN
OPEN LABEL PROSPECTIVE STUDY ON URICOSURIC EFFECTS OF LOSARTAN IN HYPERTENSIVE PATIENTS WITH HYPERURICAEMIA”submitted by DR.BANUPRIYA K to the Tamilnadu Dr. M.G.R. Medical
University, Chennai, in partial fulfillment of the requirement for the award
of the Degree of Doctor of Medicine in Pharmacology during the academic
period 2014
–
2017 is a bonafide research work carried out by her under
direct supervision & guidance.
PROFESSOR AND H.O.D.
DEAN
Department of Pharmacology,
Tirunelveli Medical College,
Tirunelveli Medical College,
Tirunelveli.
CERTIFICATE
This is to certify that the dissertation
entitled
“AN
OPEN LABEL PROSPECTIVE STUDY ON URICOSURIC EFFECTS OF LOSARTAN IN HYPERTENSIVE PATIENTS WITH HYPERURICAEMIA”presented herein by DR.BANUPRIYA K is an original work done by her in
the Department of Pharmacology, Tirunelveli Medical College , Tirunelveli
for the award of the Degree of Doctor of Medicine in Pharmacology during
the academic period of 2014-2017.
Place : Tirunelveli
GUIDE
Date :
Department of Pharmacology
Tirunelveli Medical College
DECLARATION
I solemnly declare that the dissertation titled
“AN OPEN LABEL
PROSPECTIVE STUDY ON URICOSURIC EFFECTS OF LOSARTAN IN HYPERTENSIVE PATIENTS WITH HYPERURICAEMIA”
is done by
me in the Department of Pharmacology, Tirunelveli Medical College,
Tirunelveli.
The dissertation is submitted to The Tamilnadu Dr.M.G.R.Medical
University in partial fulfillment for the award of the degree of Doctor of
Medicine in Pharmacology.
Place: Tirunelveli
DR. BANUPRIYA K,
Date:
Postgraduate student,
M.D Pharmacology,
Department of Pharmacology,
Tirunelveli Medical College,
ACKNOWLEDGEMENT
First of all, I am grateful to the Almighty for the good health and wellbeing
that were necessary to complete this research work.
I am greatly indepted to Dr. K. Sithy Athiya Munavarah MD., Dean,
Tirunelveli Medical College and Dr. S.M. Kannan MD.,Vice Principal.
Tirunelveli Medical College , Tirunelveli for their valuable support and generous
permission for doing this research work.
I wish to thank with due respect and deep gratitude to Dr. J. Ezhil Ramya
M.D., Associate Professor and Head of the Department of Pharmacology for her
inspiration, guidance and kind help rendered in completing this dissertation.
I would like to express my deepest thanks to Dr.B.Meenakshi M.D.,Associate
Professor for giving kind advice, aspiring guidance, motivation and
encouragement throughout the research.
With deep sense of gratitude , I thank the faculties of the department of
medicine for sharing their implicit knowledge, support and encouragement during
I am immensely grateful to Dr. A. Dulcie Celia M.D.,Assistant
Professor, Dr.A.Geetha Rani M.D., Assistant Professor , & Dr.Shanthi M.D.,
Assistant Professor for their support and advice provided during the research work.
I would like to thank the post graduates of Department of Pharmacology,
for their friendly advice and sharing their illuminating views related to this study.
I also express my sincere thanks to my family members for their moral
CONTENTS
S.No. Topics
Page No.
1. INTRODUCTION
1
2. REVIEW OF LITERATURE
4
3. AIM OF THE STUDY
64
4. METHODOLOGY
65
5. RESULTS
73
6. DISCUSSION
85
7. CONCLUSION
91
8. APPENDIX
I.
Informed Consent Form
II.
EQ-5D Questionnaire
III.
Proforma
IV.
Master chart
V.
Abbreviations
1 INTRODUCTION:
Hypertension is a worldwide epidemic defined as “ Blood pressure in excess of 140/90mmHg”.Around one billion people are estimated to have hypertension, contributing to more than 7.1million deaths per year1.According to the ICMR survey report, the prevalence of hypertension varied from 17-21% in all the states with marginal rural urban differences2.Genetic factor, fetal factor and environmental factors like alcohol,obesity,sodium intake, insulin resistance, stress and humoral mechanism contribute to the etiology of hypertension3.Hypertension has earned the designation “silent killer” because it is asymptomatic, but it can
progressively harm the cardiovascular system4.Forceful flow of blood through cardiovascular system can damage the arterial walls and heart muscle. It eventually contributes to a myocardial infarction. Hypertension can damage the cerebral and renal vessels resulting in stroke and renal disease respectively4. The goal of therapy in hypertension is to reduce the cardiovascular risk of the patients by treating co-morbid conditions and preventing hypertensive end organ damages5.
2
acid in hypertension may be due to reduced renal blood flow and ischemia which will stimulate urate reabsorption and increase in uric acid synthesis respectively8.
Hyperuricaemia is associated with dysfunction of endothelium, disruption of oxidative metabolism, platelet adhesion and aggregation6, 7.Moreover, serum uric acid is positively correlated with blood pressure, body mass index, levels of fasting plasma glucose, triglycerides, high-sensitivity CRP and inversely associated with HDL-c7. Losartan is an antihypertensive drug which blocks the angiotensin II type1 receptors. It also has pleiotropic uricosuric effect by reducing postsecretory reabsorption of uric acid in the proximal tubule of the kidney by inhibiting urate/anion exchanger with placebo like side effect profile. More over this hypouricemic effect does not occur with other angiotensin receptor blockers9,10.According to JNC-8 guidelines, blockade of renin angiotensin aldosterone system is the new first-line therapy for high risk hypertensive patients, so losartan can be given as initial therapy for newly diagnosed hypertensive patients less than 55years old11.
3
other risk factors like obesity,dyslipidemia and hyperglycemia for the assessment of overall cardiovascular risk6.
4 Hypertension definition and epidemiology:
Hypertension is defined as usual office blood pressure of 140/90mmHg or higher12.Raised arterial pressure is the most important public health issue in the western world. Though it is commonly asymptomatic it can be easily detected and treated. But lethal complications can arise when it is untreated13.
Increasing systolic BP and diastolic BP will increase the risk of morbidity and mortality; for example high systolic pressure is associated with 2-3 fold increase in cardiac mortality3.However, epidemiologic studies have confirmed the risk for stroke and cardiovascular disease even with low BP values (for eg: 115/75 mmHg). The artificial dichotomy between “normotension and “hypertension” may delay the intervention until the manifestations of irreversible
vascular disease occurs by elevated BP that were considered normal previously. So the guideline committees continue to debate how far to lower blood pressure with antihypertensive medications and whether to initiate drug therapy for high risk patients with prehypertensive range of 120 to 139/80 to 89mmHg14.
5
In India 6-15% of the adults in different surveys have been shown to be suffering from hypertension. At least 8% population is hypertensive in most of the countries. The prevalence of hypertension is not much different in developed and developing countries15.Affecting more than one million people worldwide, arterial hypertension is the common cause of visit to a physician and the leading cause of death.
It is the easily recognized and treatable risk factor for myocardial infarction, stroke, cardiac failure, aortic dissection, atrial fibrillation and end stage renal disease. It is estimated that 1.5 billion persons (one third of the world’s population) will be affected by hypertension due to increasing rates of obesity and aging of population by the year 2025. At present 47% of ischemic heart disease and 54% of strokes occurs due to high BP12.
Risk Factors:
Aging and Pulse Pressure:
6
hypertension occurs with isolated systolic hypertension12. Among elderly, systolic blood pressures of women are higher than men. Among adults, diastolic BP increases progressively with age until 55 years, after which it tends to decrease. The consequence is a widening of pulse pressure beyond the of age 60 years16
Gender and Race/Ethnicity:
Due to the protective effect of estrogen, hypertension is less common in menstruating females17.Hypertension is more prevalent among white population of several European nations, although hypertension is increasing in developed countries due to westernization.
Exacerbating factors: Obesity:
Associated with an increased intravascular volume, activated RAAS, elevated cardiac output and increased sympathetic nervous system. So weight loss can lower the BP modestly18.
Sleep apnea:
Treatment with continuous positive airway pressure will show improvements in blood pressure.
Increased salt intake:
7 Alcohol and Cigarette smoking:
These two may rise blood pressure by elevating the plasma catecholamines.
Exercise:
Aerobic exercise will lower BP in people with sedentary life style. Others:
The relation between stress and hypertention has not been established18 Polycythemia increases blood viscosity and raises blood pressure.
NSAIDs increases blood pressure by 5mmHg and should be avoided in hypertensive patients.
Low potassium in diet can contribute to hypertension so an intake of 90mmol/d is recommended.
Associated factors: Metabolic syndrome:
Metabolic syndrome refers to hypertension with abdominal obesity, insulin resistance, elevated catecholamines, elevated inflammatory markers like C - reactive protein and dyslipidemia with high plasma triglyceride, low high-density lipoprotein. This complex of abnormalities leads to adverse cardiovascular outcomes.
8 Hyperuricaemia:
Hypertension together with hyperuricaemia is a part of the syndrome X. Hyperinsulinemia in metabolic syndrome will elevate sodium reabsorption and will reduce elimination of uric acid. Lowering of uricaemia is indicated in these patients as they remain as a risk factor for cardiovascular disease21.Various studies have confirmed the association between cardiac risk and elevated uric acid among patients with hypertension.
Twenty five percent of untreated hypertensive patients, fifty percent of hypertensive patients taking diuretics and more than seventy five percent patients with malignant hypertension have high uric acid level. Also genetic and dietary factors influence uric acid levels. Baseline uric acid is significantly associated with an increased rate of outcome in the LIFE study of fatal or non fatal myocardial infraction,cardiovascular death and fatal or non fatal stroke6.Various trials implicated that hyperuricaemia may be an independent risk factor for hypertension related mortality and morbidity22.
9
A meta-analysis confirmed that elevated uric acid is risk factor for incident hypertension and the risk is more in women and young individuals 24.
Genetic Determinants:
Adoption, twin, and family studies document a significant heritable component to elevated BP. Family studies conducted on a background of uniform environment shows a 15–35% heritability of hypertension. In twin studies, it was 30–40% in females twins and 60% in males twins. Concordance of BP is greater for monozygotic twins than that of dizygotic twins.
Hypertension is a polygenic disease where one or more genes act along with other risk factors contributing to elevated BP25.
Secondary causes of hypertension: Genetic syndromes
Coarctation of the aorta
Primary hyperaldosteronism, Cushing syndrome,
pheochromocytoma
Hypertension associated with pregnancy, estrogen use
Kidney disease, renal vascular hypertension, hypercalcemia
10 JNC 7 Classification 13,26:
Categories SBP(mm/Hg) DBP(mm/Hg)
BP in normal range <120 <80
Prehypertension 120-139 80-89
Stage one hypertension 140-159 90-99
Stage two hypertension ≥160 ≥100
Isolated systolic hypertension
>140 <90
Pathogenesis of hypertension: Blood pressure:
Arterial pressure is a product of cardiac output and peripheral vascular resistance. Cardiac output is again a product of stroke volume and heart rate.Stroke volume is linked to myocardial contractility and size of the vessels. Peripheral vascular resistance varies with anatomic and functional changes in small vessels. Elevated blood pressure may be due to elevated cardiac output and/or elevated peripheral vascular resistance13.
Increased cardiac output:
1) Expanded fluid volume due to excessive salt consumption or may be because of kidney dysfunction causing retention of sodium
11 Increased peripheral vascular resistance:
1) Functional vascular constrictions Sympathetic nervous system overstimulation Excess stimulation of RAAS
Endothelial derived factors
Genetic alterations of cell membranes
2) Structural vascular hypertrophy
Hyperinsulinemia due to obesity or metabolic syndrome Sympathetic nervous system overstimulation
Excess stimulation of RAAS Endothelial derived factors
Genetic alterations of cell membranes
Essential hypertension:
12
Figure 1:Pathophysiological mechanisms of hypertension27:
Phases of Essential Hypertension: Phase 1:
13
Salt-resistant hypertension in this phase is due to intermittent ischemia caused by fluctuant levels of uric acid and intermittent activation of sympathetic system. Since the kidney is uninjured, the pressure natriuresis remains unaffected. In these individuals sodium loading will result in exaggerated natriuresis28
Phase 2:
On disease progression, arteriolosclerosis of renal vessels associated with tubulointerstitial inflammation will develop which will lead to salt sensitive, renal and volume dependent hypertension. Understanding these phases of hypertension helps us in the prevention and treatment of underlying process29.
More recently, there is proposed theory of role for afferent arteriolar renal vasoconstriction in causing hypertension30.This may be explained by the
mechanism in which renal ischemia attracting the leukocytes and oxidative stress scavenging the nitric oxide in kidney will lead to renal vasoconstriction and causing a heterogenic renin expression. This renal injury will activate the sympathetic system leading to retention of sodium and volume dependent hypertension31.
HYPERURICAEMIA - A MECHANISM FOR ESSENTIAL HYPERTENSION:
Epidemiologic evidence:
14
hypertension, a serum uric acid of >5.5 mg/dL was observed in 89% of essential hypertensive subject, in 30% of those with secondary hypertension and in 0% of control subjects or “white coat” hypertensives24.
Animal studies:
Wide literature review on animals supports the role of uric acid level in the pathogenesis of hypertension32. Animal studies with induced hyperuricaemia in rats activated RAAS and resulted in dysfunction of endothelium demonstrating elevated BP caused by increased urate levels33
Phase 1:
Rise in BP caused by renal vasoconstriction as a result of RAAS activation and oxidative stress was always reversible in phase I by reducing serum uric acid. The renal vasoconstriction is induced by AgII infusion in animal models that were fed on high salt diet.
Phase 2:
15 Figure 2: Uric acid and hypertension32:
Human data:
Experimental animal and human data shows that individuals with hyperuricaemia are at greater risk for hypertension with renal complications. This mechanism is less implicated in elderly individuals, where the stiffening of the aorta is the primary reason 34.
16 Uric acid level and incident hypertension:
The threshold for hypertension is not dependent on monosodium crystals
formation. It could be a lower value like 5.0-5.5 mg/dL which is much lower than
the supersaturation reading of 6.8 mg/dL.
[image:25.612.135.522.310.586.2]A meta-analysis demonstrates a pooled risk ratio of 1.13 for new onset hypertension for every 1mg/dL raise in the uric acid level36.
17
Mechanism for vascular smooth muscle activation by uric acid:
URAT1 is a transporter that promotes the entry of uric acid in vascular
smooth muscles. Upon entry protein kinases and transcription factors are activated
which results in the release of growth factors like chemokines (monocyte
chemoattractant protein-1), platelet derived growth factor, C-reactive protein,
vasoconstrictors (cyclooxygenase II generated thromboxane) and activators of
[image:26.612.135.514.303.523.2]RAAS.38
Figure 4: Activation of smooth muscles by uric acid29:
Hyperuricaemia can result in glomerular hypertension even in the early days of essential hypertension.39
Koch’s postulates and hyperuricaemic hypertension25:
An elevated serum uric acid predicts the development of elevated blood
pressure
18
In rats, raising the uric acid with uricase inhibitor increases the blood pressure
with renal hemodynamic and pathological features as observed in human hypertension
Lowering uric acid level in animals was positively correlated with decrease in
blood pressure
Pilot studies in humans also suggest that lowering serum uric acid can reduce
primary hypertension especially in adults.
Uric acid- Chemical properties and Biological importance:
Uric acid (2, 6, 8 trioxypurine-C5H4N4O3) is an endogenous organic compound which is synthesized in the liver and eliminated through kidney mainly. It is a purine metabolism end product in humans.
Normal value of serum uric acid3.5 to 7 mg/dl in humans
The value is 0.5-1 mg/dL lower for women
Renal reabsorption of uric acid and diet rich in purines contribute to
high serum uric acid 40.
It has antioxidant property due to its double bond but in the presence of altered environment like obesity it becomes a strong oxidant41
Uricaemia and aging:
Uric acid level increases on aging
19 Uric acid production:
Produced from xanthine utilizing the enzyme xanthine oxidase43.
Uric acid excretion:
10% only eliminated via kidneys
Remaining 90% is reabsorbed
Transporters involved in urate reabsorption are 1. SLC22A12 (URAT 1) present in tubular kidney
2. SLC2A9 present in kidney and basolateral in tubule cells
By inhibiting URAT 1, drugs like probenecid, benzbromarone and losartan can lower the uric acid levels. Intestine is important for about 20% excretion of uric acid via ABCG2 transporter23
The factors influencing the renal uptake of uric acid: Serum levels of uric acid
Volume status
Factors affecting renal blood flow
Reabsorption of uric acid in kidney is competitive with organic acids (monocarboxylic) which can be blocked by lactic acid, ketone bodies and oxalic acid
Factors increasing elimination of uric acid: Volume expansion
20 Factors increasing uric acid concentration:
Acute renal failure also increases uric acid by decreased renal excretion.
Drugs like ciclosporin, ethambutol, pyrazinamide and cytotoxic chemotherapy
[image:29.612.113.495.209.556.2]can raise the serum urate 44.
Figure 5:Drugs affecting uric acid synthesis and elimination23:
Factors influencing the concentrations of uric acid: Diet
Obesity
21 Diet:
Purine-rich food items like beer, veal, bacon, meat, mutton, turkey, pork,
duck and goose can raise uric acid
Meat and seafood are associated with raise in uric acid.
Large fructose intake will lead to depression of intracellular phosphate
which hinders the ATP formation resulting in hyperuricaemia.
Vitamin-C, coffee and dietary product intake is inversely related to uric
acid.
Obesity and Metabolic syndrome :
Diabetic patients with hypertension and elevated uric acid are at risk of cardiovascular complications45. High uric acid can rise the odds ratio by 1.6 for developing metabolic syndrome in obese persons46.
Hyperisulinemia in metabolic syndrome will reduce the uric acid excretion leading to hyperuricaemia and moreover synthesis of fatty acids in dyslipidemia will promote purine synthesis thereby elevating serum uric acid.
22 Figure 6:Determinants of Hyperuricaemia40:
Kidney function in relation with uric acid:
Hyperuricaemia and low GFR of 60 ml/min is associated with a relative risk of 2.4 for new onset hypertension when compared to individuals with low serum uric acid. This association between uric acid and new onset hypertension is independent of traditional risk factors.
In patients with already impaired renal function, hyperuricaemia will lead to arteriosclerosis of renal vessels and glomerular hypertension. And also increased risk of insulin resistance which can result in raised blood pressure is more often seen with concomitant kidney disease with hyperuricaemia 48.
End organ damage in hypertension due to hyperuricaemia:
23 Hyperuricaemia and incidence of CAD:
Even after adjusting the confounding factors, the incidence of cardiovascular disease in individuals with high left ventricular mass index and hyperuricaemia was found to be 2.4 times higher than their controls with normal cardiac function and urate levels49.
For every 1mg/dl raise in serum uric acid, the risk of cardiac death increases by 12% and this risk are more common in females when compared to men 50.
Mechanism of Target Organ Damage:
Left ventricular hypertrophy occurs as a compensatory mechanism against abnormal loading conditions and it is the leading step towards the development of full blown cardiovascular disease. Higher uric acid and left ventricular mass index leads to cardiac and renal morbidity manifested by prolonged and uncontrolled hypertension, high pulse pressure, worsening of dyslipidemia and low creatinine clearance. Even after adjusting other clinical risk factors, high serum uric acid level, left ventricular mass index and age are important predictors for cardiovascular disease.
24
monocyte chemoattractant protein-1(chemokine) in the vascular smooth muscle cells, is importantly linked to cardiovascular disease.
Decreased myocardial contraction with severe diastolic filling abnormalities and the damaged myocardium requiring more oxygen is the primary mechanism behind the association of left ventricular hypertrophy and CAD. Severe relaxation impairment of ventricles were observed in hyperuricaemic individuals with left ventricular hypertrophy and this “impaired ventricular relaxation” is linked with the risk of cardiovascular disease.
In addition, uric acid has found to be a proven excellent marker for endothelial dysfunction and ischemia of tissues leading to the development of atherosclerosis. Uric acid itself may induce left ventricular hypertrophy. In experimental in vivo and in vitro animal studies, inflammatory mediators such as cytokines, tumor necrosis factor and various protein kinases released by uric acid has shown to induce cardiac hypertrophy in animals.
Since serum uric acid has direct relationship with left ventricular mass index and severity of target organ damage, the assessments of these factors by echocardiography might be useful and sensitive in detecting those individuals with cardiovascular disease.
Nondippers in essential hypertension:
25
blood pressure can be defined as a ‘‘nondipping blood pressure profile’’ and such individuals are marked as nondippers.
Increased cardiovascular risk and worst prognosis is seen in nondipping hypertensive individuals when compared with individuals of a normal circadian rhythm. Nondippers have autonomic dysfunction, sympathetic system overactivity and high inflammatory activation. Increased serum uric acid is an independent and strong predictor of nondipping pattern. Moreover, release of inflammatory mediators is more common in nondippers and hs-CRP level is also significantly correlated with hyperuricaemia52.
Sequelae of Hypertension:
WHO classification of stages of hypertension:
Stage 1 no objective signs of organic changes
Stage 2at least has one of the following
Left ventricular hypertrophy
Generalized and focal narrowing of the retinal arteries
Proteinuria and increased serum creatinine (1.2 -2 mg/dl)
Ultrasound or radiological evidence of atherosclerotic plaque
Stage 3both symptoms and signs of organ damage
26 Brain-TIA, stroke, hypertensive encephalopathy
Optic fundi- retinal hemorrhage, exudate with or without papilledema
Kidney-serum creatinine >2mg/dl, renal failure
Vessels-dissecting aneurysm, symptomatic arterial occlusive disease53
The heart:
In hypertensive individuals, cardiac hypertrophy is purely an adaptive mechanism to pressure overload which can lead to dysfunction of myocardium, dilation of heart, CCF and sudden death54.
Morphology:
Hypertension often induces left ventricular pressure overload and hypertrophy without initial ventricular dilation. As a result, thickening of left ventricular wall causes disproportionate increase in the weight of the heart leading to increase in overall cardiac size. On progression, left ventricular wall thickening imparts a stiffness that impairs diastolic filling, often inducing left atrial enlargement55.
Clinical presentation:
27
caused by enlargement of left atrium or congestive heart failure may be the first symptom56.
Blood vessels:
Hypertension accelerates atherogenesis causing degenerative changes in the large and medium sized arterial walls leading to aortic dissection and hemorrhage in the brain.
Morphology:
Two forms of blood vessel disease are associated with hypertension: Hyaline arteriolosclerosis
Hyperplastic arteriolosclerosis57.
Although elderly persons even with normal pressure are frequently associated with hyaline arteriosclerosis, this change is more severe in hypertensive individuals58.
Kidney:
Benign nephrosclerosis:
Defined as renal artery sclerosis with parenchymal defects which includes glomerulosclerosis and prolonged tubulointersititial injury, resulting in reduced functional renal mass59.
Morphology:
28
Histologic examination shows narrowing of the arteriolar lumen due to hyalinization and thickening of the vessel walls (hyaline arteriolosclerosis)54 Clinical Features:
Uncomplicated benign nephrosclerosis rarely causes renal insufficiency and uremia. But usually renal blood flow is moderately reduced and the GFR remains normal or slightly reduced. And rarely, there is mild proteinuria.
Brain:
Lacunar infarctions, slit hemorrhages, hypertensive fatal encephalopathy and massive intracerebral bleed are the consequences of hypertension in the brain and the incidence of these can be reduced by repeated screening for high BP and aggressive drug therapy for the same 54.
Hypertensive Encephalopathy
Is an emergency and life threatening condition with symptoms of headache, confusion, vomiting, convulsions, coma and death commonly seen in individuals with malignant hypertension.
Eye:
29 Hypertensive retinopathy60:
Grade 1: increased tortuousity of retinal vessels and silver wiring of retinal artery
Grade 2: in addition to grade 1, there will be nipping of venules at arteriovenous crossing
Grade 3: Grade 2 and flame shape hemorrhage and cotton wool exudates
Grade 4: papilledema, hard exudate and macular star
In malignant hypertension, retinal detachment occurs.
Diagnosis of hypertension:
The hypertensive individuals should have the following assessments:
A detailed history about the patients and their physical examination
Screening for important cardiovascular risk factors
Screening for causes of secondary hypertension
Identifying cardiovascular complications of hypertension and finding out
other comorbid conditions
Assessing lifestyles which may be a risk factor for raised BP
Determining the tolerability and susceptibility for intervention13.
30
nocturia. Characteristically, this headache occurs in the occipital region and most commonly in the morning. Other common nonspecific symptoms related to hypertension are dizziness, palpitations, easy fatigability and impotence.
Breathlessness in hypertensive patients suggests congestive cardiac failure or left ventricular hypertrophy. Pheochromocytoma, a common cause of secondary hypertension presents with sweating, palpitations and headache. Symptomatic peripheral vascular disease and angina indicate the presence of renal artery stenosis caused by atherosclerosis. Hypokalemia related symptoms like muscle cramps and muscle weakness is seen in individuals with primary aldosteronism.
Cushing’s syndrome individuals suffer from increased body weight, menstrual
problems, and recurrent acne over face, polyuria, edema and muscular weaknes.
Malignant Hypertension may presents with the symptoms of severe headache, visual disturbance, seizures, reversible loss of consciousness and symptoms of cardiac failure.3
Young hypertensive patients with a family history of hypertension will commonly show simple Mendelian resistance.
Diagnosis of secondary hypertension:
Age of onset <30 years or >60 years of age
Difficult to control after therapy initiation
Clinical occurance of hypertensive crisis
31
Measurement of blood pressure:
Routinely all adults must measure blood pressure at least once in every 5
years till 80 years of age. For this purpose seated blood pressure will be measured
after 5 minutes of rest. While standing blood pressure will be measured only in
diabetic patients and in older individuals to exclude the possibility of orthostatic
hypotension. Blood pressure must be measured after emptying the urinary bladder
and should be seated atleast for five to ten minutes with back fully supported and
legs which are not crossed resting on the ground The arm used for measurement of
BP must rest on a table, at the heart-level. A sphygmomanometer with stethoscope
and automated electronic device are the commonly used devices11.A cuff of
at least 40% the arm circumference in width should be attached to a mercury or
aneroid manometer and inflated around the extended arm. The cuff must be
deflated at 2 mm Hg per second and the blood pressure must be measured to the
nearest 2mm Hg.
Auscultation over the brachial artery reveals five phases of korotoff sounds when
the cuff is deflated62.
Korotkoff sounds:
These are sounds produced from under the distal half of blood pressure cuff
between the systole and diastole due to complete collapse of artery followed by
reopening with each beat. As the artery wall opens it causes tapping sound. As the
cuff pressure falls below the diastolic pressure, sound disappears as the vessel wall
32
Phase 1first appearance of sounds denoting the systolic pressure
Phase 2 and 3louder sound
Phase 4sounds with abrupt muffling
Phase 5disappearance of the sounds
Phase 5 provides better measurement of diastolic blood pressure than phase 4, not
only because it corresponds directly with measured diastolic pressure but also
because its identification is less subjective.
At least two consistent readings are required for the estimation of blood pressure .
More readings may be required if there are variations in the blood pressure
measurement. At initial evaluation, blood pressure is measured in both the arms.
The higher reading will be used for measurements thereafter. When assessing
cardiovascular risk, blood pressure average measured at separate visits will be
most accurate than the measurements done at a single day visit3
Monitoring of the ambulatory blood pressure:
JNC 7 has recommended monitoring of ambulatory blood pressure only in
special cases like white coat hypertension ,treatment resistance, autonomic failure,
hypotension with symptoms ,episodic hypertension and also to know
“nondippers” in whom the blood pressure will not decrease by >10% at night
time13.
This can be done by an automated device which is capable of documenting
blood pressure at more frequent intervals throughout the day. The measured
33
values. The normal upper limit of ambulatory blood pressure reading is 140/90
mmHg in daytime, 125/75 mm Hg at sleep, and 135/85 mm Hg during continuous
measurement for 24 hours. The home blood pressure recordings can be done by
patients themselves in the morning by using the home monitoring devices64.
Physical Examination:
Body habitus like weight and height are measured.
Blood pressure must be measured in both the arms
Standing BP measurement to rule out postural hypotension.
In young individuals, lower extremity BP should be measured even if
femoral pulsations are felt.
Check for hyper and hypothyroidism by palpating neck
Fundus examination for vascular disease and papilledema
Auscultation over carotid and femoral artery for bruits
Auscultation of the heart for loud S2 because of aortic valve closure and
for S4 gallop as a result of atrial contraction.
Palpation of enlarged and laterally displaced apical impulse due to
hypertrophy of left ventricle13.
Carotid bruits, cardiac murmer,S3 or S4 heart sound, neurological
deficit, elevated jugular venous pressure, rales, unequal pulses,
34
radiofemoral delay, tendon xanthoma and central obesity on physical
examination needs investigations for target organ damage or secondary
cause of hypertension.61
Diagnosis of Hypertension:13,18
SYSTEM TEST
Renal Microscopic urinalysis, serum uric acid,albumin excretion, serum
BUN and creatinine,Renal USG and angiography.
Endocrine Serum sodium, potassium, calcium,TSH,urine catechol for
pheochromocytoma,urinary cortisol and dexamethasone
suppression test for cushing syndrome,plasma renin and
aldosterone for primary aldosteronism
Metabolic Plasma blood glucose and lipid profile
Other Hematocrit, ECG for left ventricular hypertrophy and
ischaemia,X-Ray for cardiac size and coarctation of aorta,echo for left
ventricular hypertrophy.
Factors Influencing Risk of Cardiovascular Disease: Age more than 55 years of age
Male gender
35
Post menopausal women
H/O Diabetes Mellitus
Increased waist hip ratio
Increased LDL,total cholesterol,low HDL,high triglyceride
Family history of premature cardiovascular disease with age of onset of less
than 55 years in male and less than 65 years in female.65
MANAGEMENT OF HYPERTENSION: General considerations and goals of treatment:
Primary goal in the treatment of hypertension is prevention of long term
sequelae. Primary concern is to lower systolic blood pressure which is associated
with mortality. Wide pulse pressure reflects high systolic blood pressure and most
accurate predictor of all. High risk individuals can be approached with
nonpharmacological treatment to achieve a significant fall in blood pressure over a
period of 3-6 months. Even after 3 months if the blood pressure is more than
140/90mmHg initiate drug therapy. Discretion is warranted while prescribing
medication for hypertension that may adversely affect cardiovascular risk in other
36
JNC 7 guidelines65 Target blood pressure
Young adults and middle age <140/90mmHg
Diabetic patients <140/80mmHg
Stroke patients <140/85mmHg
Elderly patients with stroke <150/90mmHg
In the absence of hypertensive crisis, blood pressure should be reduced gradually
to avoid cerebral ischemia.
Patient education is more important in treatment plan to promote patient
compliance. Culture and other individual differences among patients should be
taken into consideration before the start of therapy. Physicians should emphasize
that
a) Lifelong treatment is required
b) Symptoms are unreliable tool for severity of hypertension
c) Prognosis improves with proper and continued treatment61.
Primary prevention :
Aims at reducing the incidence of hypertension.
a)Population based strategies: Information and education:
Education about salt intake, diet control and healthy diet through interpersonal
communications and multimedia channels can create favorable environment and
37
Physical activity:
To counter pandemic of obesity in context of nutritional abundance, physical
activity is the public health priority. WHO recommends 30 minutes exercise per
day done atleast 5 times a week. Regular aerobic exercise should be within the
limits of cardiovascular status.
Diet:
Reduce the intake of saturated and tans fatty acids. Adequate dietary intake of
potassium should be there to lower blood pressure and also to prevent stroke and
arrhythmia. Sodium and potassium should be maintained in the ratio of 1:1. Daily
dietary potassium intake should be 50mmol/day.Potassium is rich in fruits and
vegetables. Adequate dietary maintenance of calcium and magnesium are
required.
Limit alcohol intake not more than one ounce (i.e. 30 ml) of brandy, whisky or
rum per day or 24 ounces of beer. DASH diet should be followed which includes
diet rich in fruits and vegetables with limited intake of fat dairy foods, saturated
38
Lifestyle modifications12 Change in blood pressure Fruits,vegetables,diet with low fat Reduce by 6/3mmHg
Moderately intensive aerobic exercise Reduce by 2-5/1-2mmHg
After each cigarette Increase by 10-15mmHg SBP
First morning cup of coffee Increase by 10-15mmHg SBP
10kg weight loss Reduce by 5-20mmHg SBP
DASH diet Reduce by 8-14mmHg SBP
Alcohol moderation Reduce by 2-4mmHg SBP
b) High risk approach:
Middle range of high blood pressure who are not diagnosed as hypertensive
patients but are at risk of developing cardiovascular complications are screened
through this approach. More appropriate for individuals and their physicians but
have little impact on general population. This approach does not alter the
underlying cause of hypertension and deals with only margin of problem. It
requires continued and extensive screening.
Secondary prevention:
Aims to reduce the prevalence of hypertension by early diagnosis and treatment.
This can be done by regular monitoring of blood pressure for all people more than
30 years of age who come in contact with health faculty. New component of
control of non communicable diseases has been added in the job description of
39
Tertiary prevention:
Aims to reduce the disabilities in individuals who have already developed
complications due to hypertension. Family based rehabilitation is necessary.
Drug treatment for hypertension:
Most of the patients will be in need of more than one drug for control of raised
blood pressure. In general, we should either increase the dose of individual drugs
or must add new drugs from different class at 2- to 3-weekly interval time. This
frequent change may be fast or slow which depends on the decision of the
physician. Most of the patients will reach the effective treatment regimen, within 6
to 8 weeks.
Choice of antihypertensives:
It is mostly influenced by the age, ethnicity, and other clinical conditions of the
patient (eg, diabetes mellitus, CAD and Pregnancy) Long-acting drugs with single
dosage per day are always preferred over shortly acting drugs which require
40
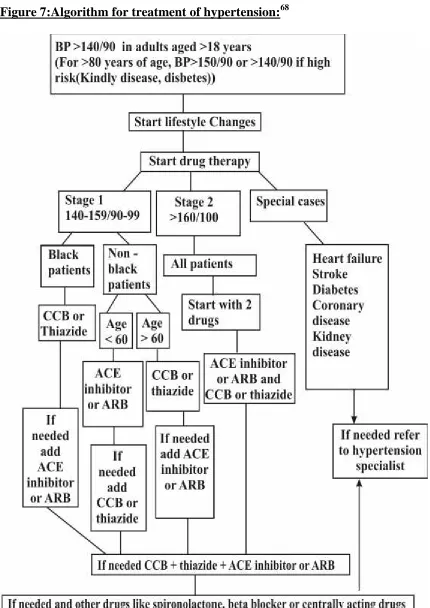
Figure 8:ACD Rule:69
Brief comments on drug classes:
Angiotensin-converting enzyme Inhibitors
?Action - blockade of RAAS
?Beneficial effect by preventing breakdown of bradykinin.
? Adverse effects noted are cough ,dose dependent hyperkalemia and rarely
42
Class13 Examples Dosage/Day Other Uses Contraindications
ACE inhibitors
Captopril 25–200 mg PostMI,
Nephropathy
and CHF
Pregnancy, Hyperkalemia,
Renal failure and Bilateral
renal artery stenosis, Ramipril 2.5–20 mg
Lisinopril 10-40mg
Angiotensin Receptor Blockers:
Action - blockade of AT1 receptor
Vasodilator
No cough like ACEI
No dose dependent adverse effects
Preferred over ACEI
Class13 Examples Dosing /
day
Other uses Contraindications
Angiotensin II antagonists Losartan 25–100 mg CHF, ACEI cough, Diabetic nephropathy Renal failure, Pregnancy, Hyperkalemia and Bilateral renal artery stenosis Valsartan 80–320 mg
43
Thiazide and Thiazide-like Diuretics:
Action by excretion of sodium by kidney
Vasodilator.
Cause reduction in the incidence of strokes and CAD
Chlorthalidone is potent and long acting antihypertensive among the
thiazides
Adverse effects
Hypokalemia can be prevented by combined use of potassium sparing
diuretics
Hyperuricaemia can be reduced by starting with low dose
Hyperglycemia can be prevented by avoiding -blockers or by combining
ACEI13
Calcium Channel Blockers:
Acts by blockade of L type calcium channel in the arterial smooth
muscles
Two types:
Dihydropyridines which dilates mainly arteries and
non-dihydropyridines which has negative inotropic and chronotropic
property along with vasodilatory property thereby preferred in atrial
fibrillation.
44
Important adverse effect is peripheral edema, occurring only at high
doses.
Calcium antagonists13
Examples Dosage/Day Other Uses Contraindications
Dihydropyridines Nifedipine 30–60 mg Angina
Heart failure, 2nd
or 3rddegree heart
block
Non-dihydropyridines
Verapamil 120–360
mg
Supra
ventricular
tachycardias,
Angina,
Post-MI. Diltiazem 180-420 mg
Beta Blockers:
Act by reducing cardiac output and by blocking renin
Least effective when used in black population
Not effective in preventing stroke and CAD
Adverse effects are hyperglycemia, heart block, erectile dysfunction and
fatigability
Combined alpha and beta blocker dugs like labetalol are used in
45
Beta blockers13
Examples Dosing /day
Other Uses Contraindications
Cardioselective Atenolol 25–100
mg Angina, Sinus tachycardia, Congestive heart failure, PostMI, Ventricular tachyarrhythmias
2nd or 3rd degree
heart block,
sick-sinus syndrome,
asthma, COPD, Metoprolol 25–100
mg
Nonselective Propranolol 40–160
mg Combined Alpha/beta Labetalol 200– 800 mg CHF Carvedilol 12.5– 50 mg CHF Alpha Blockers:
Act by blocking arterial alpha adrenergic receptors and thus preventing the
vasoconstriction.
Least used as first line agent
Mainly used in resistant cases of hypertension
Usually combined with diuretics to neutralize the metabolic adverse effects
of diuretics
Beneficial in benign prostate hypertrophy
Alpha antagonists13
Examples Dosing
/day
Other indications
Selective blocker Prazosin 2–20 mg Prostatic hypertrophy
Doxazosin 1–16 mg
Terazosin 1–10 mg
Nonselective blocker
Phenoxybenzamine 20–120 mg
46
Centrally Acting Agents:
Act centrally by blocking sympathetic outflow
Alpha methyl dopa is safe for use during pregnancy
Clonidine patches are available to reduce the withdrawal syndrome of oral
clonidine13.
Direct Vasodilators: Rarely used
Diuretics are often required to counteract their fluid retention
Hypertrichiosis is the main adverse effect of minoxidil
Mineralocorticoid Receptor Antagonists:
Spironolactone was used in older days for heart failure and increased
aldosterone states in resistant hypertension
Eplerenone used in treatment of resistant hypertension
Adverse effects are gynecomastia, erectile dysfunction and hyperkalemia
Cautiously used in patients with low GFR<50%
Followup visits and Monitoring:
After initiating antihypertensive, patients must come for scheduled followup visits
for dosage adjustment atleast at monthly intervals till the control of BP is
achieved. In patients with stage 2 hypertension and/or with comorbid conditions
and complications more frequent followup visits are needed. Serum levels of
47
times/year. Followup visits can be extended to once in 3- to 6-months after
control of raised BP or with achieved BP goal.68
Hypertensive urgencies and emergencies:
Individuals with markedly elevated BP and with acute end organ damage mostly
need a hospital admission and parenteral drug therapy.
Patients with markedly elevated BP but with no acute end organ damage
doesn’t require hospital admission but needs combination of oral antihypertensive
drugs immediately. They must be evaluated for hypertension associated heart and
renal damage. Any identifiable causes of hypertension should be looked for.70
Special considerations:11
Recommendations First line therapy Second line therapy
Third line therapy
Diabetes RAAS inhibitors
(ACE inhibitor or
angiotensin receptor blockers) Calcium channel blockers or thiazide Calcium channel blockers ,RAAS inhibitors and Thiazides
CKD RAAS inhibitors Calcium
channel blockers or thiazide Calcium channel blockers ,RAAS inhibitors and Thiazides
CAD Beta blocker and
48
Stroke RAAS inhibitors Calcium
channel
blockers or
Thiazides
Calcium channel
blockers , RAAS
inhibitor and
thiazide
Cardiac Failure RAAS inhibitors,beta
blocker,Diuretics and
Aldosterone
antagonist
Amlodipine
MANAGEMENT OF HYPERURICAEMIA IN HYPERTENSIVE
PATIENTS:
Non pharmacological management: Low purine diet
Weight reduction
Avoidance of alcohol
Avoidance of drugs causing hyperuricaemia like thiazides, cytotoxic drugs
etc.
Pharmacological treatment:
Benzbromarone, allopurinol, probenecid, fenofibrate and febuxostat are the
known drugs for the treatment of hyperuricaemia. But these agents can lead to
renal stones by an unexpectedly stronger uricosuric effect and there is a possibility
of attenuating uric acid lowering effect by increasing oxypurinol elimination in
49
These agents have specific side effects like allopurinol causing dose related
gastrointestinal adverse effects and severe rashes ,benzbromarone causing
hepatotoxicity and they commonly cause idiosyncratic adverse effects, which
discourage the use of these agents in hypertensive patients with hyperuricaemia.
Moreover they donot improve endothelial cell function and hemodynamic
impairment and so cannot prevent cardiovascular mortality in hypertensive
patients.23
LOSARTAN:
A promising agent for the treatment of hyperuricaemia in patients with
hypertriglyceridaemia or hypertension.
Uricosuric mechanism :
Losartan potassium being an orally active angiotensin II receptor antagonist is
commonly used in the treatment of hypertension. Its active metabolite E-3174 with
long t1/2 is also a potent antagonist at the AT1 receptor. The first observation of
uricosuric effect of losartan which acts by increasing urinary uric acid excretion
thereby reducing serum uric acid level was noted in a pilot study done in healthy
volunteers in the year 1992.
The fractional clearance of uric acid is expected during the first few hours of
drug intake. Though angiotensin reduces uric acid renal excretion, blockade of the
same is not responsible for the uricosuric effect of losartan. This was further
proved by unaltered uric acid levels after reducing sodium intake or treatment with
50
exchanger URAT1” in the kidney .Blockade of this transporter will inhibit the
urate reabsorption in the proximal tubule of kidney and so promoting uric acid
excretion.71
In most clinical studies, losartan 50 mg once daily dosage increased the
fractional elimination of uric acid.71 These studies showed that after four weeks
treatment with losartan there was a significant reduction in serum uric acid with
corresponding increased excretion of urinary uric acid72 The increase was
moderate, from 3 to 30% and uricosuric effect was maintained even after drug
discontinuation for 3–4 weeks of treatment. Doubling the losartan dose did not
show any further reduction in SUA levels.
Losartan can be combined with diuretics which usually cause hyperuricaemia
as an adverse effect on their chronic use. Losartan raises the urinary pH
significantly which counterbalances the risk of urolithiasis associated with raised
uric acid elimination. This unique property is not seen with other uricosuric drugs.
Due to this additional uricosuric property, Losartan causes significant reduction in
BP71
Based on literature review hyperuricaemia is an important risk factor for
hypertension related morbidity and mortality like stroke and cardiovascular events,
so Losartan is a good antihypertensive in hypertension associated with
hyperuricaemia. Genetic polymorphisms in the URAT1 transporter are associated
with raised BMI, waist circumference, HDL-c, and the syndrome X in
51
dyslipidemia. Losartan has renoprotective effect in hypertensive patients by
reduction in urate and lowering blood pressure23
Description
Losartan potassium is a non-peptide molecule.Its empirical formula is
[image:60.612.167.458.225.426.2]C22H22ClKN6O.
Figure 9:Structural formula of losartan76:
It is soluble in water and alcohols but less soluble in organic solvents like
acetonitrile and methyl ethyl ketone.
5-hydroxymethyl group oxidation in the imidazole ring leads to the formation of
active metabolite of losartan.
CLINICAL PHARMACOLOGY Mechanism of Action
Losartan being an Angiotensin II receptor blocker will bind with the AT1 receptor
which is competitive in nature but the inhibition of Angiotensin II is often
52
Dissociation kinetics of losartan from AT1receptor is very slow
Losartan induced receptor internalization
Alternative binding sites for losartan on the AT1receptor
This insurmountable antagonism leads to sustained receptor blockade of losartan
even in the presence of excess levels of endogenous ligand and with forgotten
doses of losartan.
Losartan potently and selectively inhibits the biological response of Angiotensin II
which includes
Contraction of vascular smooth muscle
Rapid pressor responses
Slow pressor responses
Release of adrenal catecholamines
Vasopressin release
Aldosterone secretion
Enhancement of noradrenergic neurotransmission
Increase in sympathetic tone
Changes in renal function
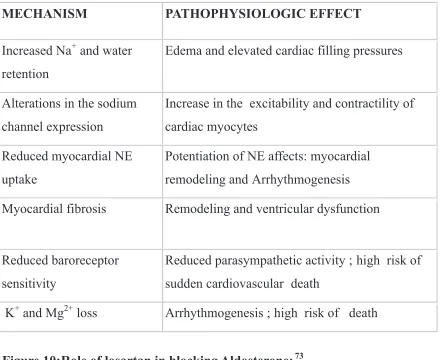
Potential role of Aldosterone:73
MECHANISM PATHOPHYSIOLOGIC EFFECT
Increased Na+ and water
retention
Edema and elevated cardiac filling pressures
Alterations in the sodium
channel expression
Increase in the excitability and contractility of
cardiac myocytes
Reduced myocardial NE
uptake
Potentiation of NE affects: myocardial
remodeling and Arrhythmogenesis
Myocardial fibrosis Remodeling and ventricular dysfunction
Reduced baroreceptor
sensitivity
Reduced parasympathetic activity ; high risk of
sudden cardiovascular death
[image:62.612.88.534.81.441.2]K+ and Mg2+ loss Arrhythmogenesis ; high risk of death
54
The metabolite EXP 3174 being 10 to 40 times more potent than the parent drug
losartan, is also a reversible and noncompetitive inhibitor at the AT1 receptor.
Losartan will not block ion channels or hormonal receptors and it does not affect
the autonomic reflexes. It does not block the degradation of bradykinin
Pleiotrophic effects of Losartan:
Losartan will significantly reduce the proteinuria, fractional elimination
of albumin and IgG. Moreover it will maintain glomerular filtration rate.
Losartan can cause persistent decrease in serum uric acid levels
Act as a competitive antagonist of the thromboxane A2 receptor and
therefore can attenuate platelet aggregation.
Its active metabolite EXP 3179 will reduce the COX-2 mRNA
upregulation and so decreasing the prostaglandin generation.
Losartan in the therapeutic dose of 50 mg daily significantly reduces
serum total cholesterol and total triglyceride levels.74Lipid lowering
property of angiotensin receptor blocker is due to different mechanisms
Activation of PPAR gamma which regulates lipid metabolism
Interaction between the lipid metabolism and angiotensin system75
Pharmacokinetic properties Absorption:
Losartan is absorbed well on oral administration and the first-pass metabolism in
55
inactive metabolites. The systemic bioavailability of losartan is nearly 33% and
the peak plasma concentrations of losartan and EXP 3174 are achieved in 1 hour
and in 4 hours respectively and the plasma half-lives being 2.5 and 6-9 hours,
respectively. No interactions with the food.
Distribution:
It is 99% plasma protein bound drug with volume of distribution around thirty
four litres .It does not cross the BBB
Metabolism :
The biotransformation of losartan is through CYP2C9 and CYP3A4 in the liver
and fourteen percent is converted into EXP 3174.
Excretion:
The clearances of losartan and EXP 3174 are due to renal and hepatic elimination
which is affected in individuals with impaired hepatic function. The kinetics of
losartan and EXP 3174 have linear relationship until the dose of 200mg. Losartan
and EXP 3174 cannot be removed by using haemodialysis.76
THERAPEUTIC USES Hypertension :
Losartan is used in the treatment of hypertension. In clinical studies, once-daily
administration of 50mg losartan for stage 1 and 2 essential hypertension showed
significant reduction in both systolic and diastolic BP and the antihypertensive
56
paralleled the natural diurnal rhythms. Discontinuation of losartan will not cause
rebound hypertension.
Hypertensive patients with left ventricular hypertrophy:
A reduced incidence of stroke was noted in these patients during losartan
treatment
Reno protective in patients with DM and nephropathy:
Losartan delays the progression of renal disease by reducing the incidence of
raised serum creatinine, end stage kidney disease and death. It causes a reduction
in proteinuria.
Heart failure:
Indicated in improving symptoms and reducing mortality
Treatment of hyperuricaemic patients with hypertension:
Losartan is indicated in hypertensive patients with hyperuricaemia for reducing
serum uric acid and for increasing the urinary uric acid elimination.
Gout:
Losartan has a modest uricosuric effect and may be an option for those who are
intolerant to probenecid and are hypertensive.
Portal hypertension:
Losartan is safe and potent agent in the treatment of portal hypertension with
57
Dosage of losartan:
Losartan effects are not affected by food intake.
Hypertension and hypertensive patients with hyperuricaemia
50 mg administered once daily and the maximal effect is seen after 3-6 weeks of
drug therapy.
For reducing the incidence of stroke in hypertensive patients with CAD
The initial dose is 50 mg of losartan given once daily. A low dose of diuretics like
thiazide can be combined or else the dose of losartan can be raised to 100 mg/day
based on the BP.
Reno protective dose in diabetic patients with macroalbuminuria
Initial dose is 50 mg /day. The dose can be up titrated to 100 mg/day based on the
BP. It can be combined safely with insulin, oral hypoglycemic agents and other
antihypertensive drugs.
In volume depleted patients
Initial dose of 25 mg/day is recommended
Patients with renal dysfunction
Generally no dosage alterations are needed in mild impairment. But in moderate to
severe renal failure and in patients on dialysis, the initial dose may be reduced to
58
Patients with hepatic dysfunction
Dosage reduction is compulsory and the initial starting dose preferred must be low
as 25mg
Pediatrics
Losartan use in individuals who are less than 18 years is generally not
recommended.
Old age
Up to 75 years of age: No dosage alteration is required More than 75 years of age: A low initial dose of 25 mg/day.
Contraindications •Pregnancy
Losartan is contraindicated during pregnancy and requires immediate drug
stoppage if pregnancy is detected. Animal studies with losartan have demonstrated
fetal and neonatal injury and death. In humans beings the risk is more during the
second and third trimester because the fetal renal perfusion depends on RAAS
development which begins during the second trimester.76
•Hypersensitivity
Any history of hypersensitivity to losartan, other ARBs or any excipients added
59
Drug interactions:
In clinical pharmacokinetic studies, no significant drug interactions of losartan
were noted with hydrochlorothiazide, cimetidine, ketoconazole, erythromycin,
digoxin, warfarin and phenobarbital. Fluconazole and rifampicin will reduce the
levels of active metabolite of losartan.
Concomitant use of potassium-sparing diuretics or foods rich in potassium can
result in fatal hyperkalemia. On the other hand antihypertensive effect of losartan
may be reduced by NSAIDs such as indomethacin and steroids.76
Undesirable effects :
Losartan is generally well-tolerated and the overall occurrence of adverse effects
of losartan is similar to placebo. Adverse effects are usually mild and transient in
nature and do not require stoppage of drug. The most common adverse effects
observed with Losartan therapy are dizziness,easy fatigability, vertigo,
hyperkalemia, hypotension and gastrointestinal adverse effects like
nausea,vomiting and diarrhea while the rare and uncommon side effects are
60
STUDIES RELATED TO PLEIOTROPIC EFFECTS OF LOSARTAN:
1. A study on losartan 50 mg when given for 1 month in 10 hypertensive patients
showed decrease in proximal sodium reabsorption,microalbuminuria and increase
in renal uric acid clearance without altering GFR and renal plasma flow.Renal
function was well preserved which may be of clinical interest when adjuant
diuretic therapy is required.77
2. Lang RM et al conducted a study in heart patients which showed that 12 weeks
oral administration of losartan was well tolerated .Functional capacity and clinical
status of patients with heart failure in whom treatment with ACE inhibitor when
replaced with losartan for 12 weeks remained the same. Treadmill exercise time ,6
minutes walk test,dyspnea fatigue index and left ventricular ejection fraction also
did not change significantly when an ACE inhibitor was replaced by Losartan.So
Losartan was well tolerated in patients with heart failure and was comparable to
enalapril with regard to improving exercise tolerance78.
3. A study done by Schneider AW et al, reported that Losartan was safe and highly
effective in the treatment of portal hypertension in patients with cirrhosis and
portal hypertension without compromising renal function and none of the patients
had deterioration of liver function79.
4. A study on 13 hypertensive patients with hyperuricaemia and gout who were on
losartan 50 mg once daily or irbesartan 150 mg for 4 weeks showed a decrease in
61
increasing losartan dose to 50 mg BD did not further decrease serum uric acid.This
demonstrated dose dependent uricosuric effect of losartan80.
5. Kramer C et al demonstrated detectable serum levels of EXP3179 in patients in
concentrations that exhibit anti-inflammatory and antiaggregatory property in vitro
by abolishing COX2 mRNA upregulation and COX dependent thromboxane A2
and prostaglandin F2alpha generation. This proved the anti-inflammatory and
antiaggregatory properties of losartan81.
6. The Losartan Intervention for Endpoint (LIFE) Reduction in Hypertension
Study demonstrated the superiority of losartan compared with adrenergic receptor
antagonist (atenolol) with regard to reducing stroke incidence in hypertensive
patients with associated left ventricular hypertrophy. The losartan group showed
less frequent new onset diabetes mellitus with better tolerability than the atenolol
group82.
7.A study done in 25 hypertensive patients after 3 months treatment with either
losartan or trandopril showed improvemet in insulin sensitivity by decreasing
sympathetic system activation and reduction in HbA1c due to low in vitro
formation of advanced glycated end products in losartan group.Von willebrand
factor and homocysteine levels were also reduced in losartan group when
62
8. A study done by Rayner BL et al, on 59 patients with hypertension and
hyperuricaemia associated with diuretics were added on either Losartan or
candesartan.Both the drugs lowered blood pressure and fibrin which may explain
reduction of stroke in hypertensive patients but losartan had an additional
advantage of reducing uric acid84.
9.A study done by Seok Min Kang et al explained the anti-inflammatory and
antiproliferative properties of losartan in which it inhibited the uric acid
stimulated proliferation and inflammatory signaling by modulation of uric acid
transporter in cultured rat aortic vascular smooth muscle cells(33% reduction
p<0.05).This may predict beneficial effect of losartan on vascular changes85.
10. Nindita Y et al demonstrated the effect of losartan and benzbromarone on the
level of urat1 mRNA in transfected HEK 293 cells. Losartan caused significant