FOLLOWING
MANDIBULAR
SETBACKSURGERY –
A
CEPHALOMETRIC
STUDY
Dissertation Subm itted to
THE TAMILNADU DR. M.G.R. MEDICAL
UNIVERSITY
For partial fulfillm ent of the requirem ents for the degree of
MASTER OF DENTAL SUR GERY
BRANCH – V
ORTHO DONTI CS AND DENTO FACI AL O RTHO P AEDI CS
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY
CHENNAI – 600 032
This is to certif y that Dr. V. SENTHIL KUMAR, Post graduate student (2012 – 2015) in the Department of Orthodontics and Dentofacial orthop aedics branch V, Tamil Nadu Government Dental College and Hospital, Chennai – 600 003 has done this dissertation titled “E VA LUA TION OF
CHANGES I N HY OID BONE POSITION AND PHARY NGEA L
AIRWAY DI MENSI ONS FOLLOWI NG MANDIBULAR SE TBACK
SURGERY – A CE PHALOMETR IC S TUDY” under my direct
guidance and supervision for partial fulfillment of the M.D.S degree examination in April 2015 as per the regulations lai d down b y The Tamil Nadu Dr. M.G.R. Medical Universit y, Chennai -600 032 for M.D.S., Orthodontics and Dentofacial orthopaedics (Branch – V) degree examination.
Guided By
Dr. G.VIMALA M.D.S.,
Professor and Head,
Dept. of Orthodontics & Dentofacial Ort hopaedics, Tamil Nadu Govt . Dental College & Hospital,
Chennai - 600 003
Dr. SRIDHAR PREMKUMAR, M.D.S.,
Principal,
I, Dr. V. SENT HIL KUMAR, do hereb y decl are that the
diss ert ati on titl ed “EVALUATION OF C HANGES IN HYOI D BONE
POSI TION A ND PHARYNGEA L AIRWAY DIM ENSIONS
FOLLOW ING MA NDIB ULAR SE TB ACK SURGERY – A
CEPHALOMETR IC STUDY ” was done in t he Depart ment of
Ort hodonti cs , Tamil Nadu Government Dental Coll ege & Hospit al, Chennai 600 003. I have utiliz ed the facili ties provided i n t he Governm ent Dent al College for the st udy i n part ial ful fillm ent of the requirem ents for the degree of M ast er of Dent al Surger y in the speci alit y of Orthodonti cs and Dentofaci al Orthopaedi cs (Br anch V)
duri ng the co urs e period 2012-2015 under the conceptualiz ati on and
guidance of m y dis sertation guide, Profess or Dr. G. VI MAL A
MDS .,
I declare that no part of the di ssert ati on will be utiliz ed for gai ning fi nanci al assist ance for research or ot her prom otions without obtai ning prior permissi on from The Tami l Nadu Governm ent Dent al College & Hos pit al.
I al so declare that no part of t his work will be publis hed either in the print or el ectroni c m edi a except with thos e who have been acti vel y involved in thi s diss ertat ion work and I fi rml y affi rm that the ri ght t o preserve or publish this work rest s s olel y with the prior permissi on of the P rincipal, Tami l Nadu Governm ent Dental College & Hos pit al, Chennai 600 003, but wit h the vest ed ri ght that
I shal l b e cit ed as the aut hor(s ).
Signature of the PG student Signature of the HOD
M y sincere and heartfelt thanks to Dr. SRIDHAR PREMKUMAR, M.D.S., our Principal and Professor of Orthodontics, Tamil Nadu Government Dental College and Hospital, Chennai – 3,for his continuous and enormous support in allowing me to conduct this stud y and for his constant encouragement and advice during my tou gh phases in curriculum.
With my heartfelt respect, immeasurable gra titude and honour, I thank my benevolent guide, Dr. G. VIMALA M.D.S.,
Professor & Head, Department of Orthodontics and Dentofacial orthopedics, Tamil Nadu Government Dental College and Hospital, Chennai – 3, for her astute guidance, support and encouragement throughout my post graduate course and to bring this dissertation to a successful completion.
I owe my thanks and great honour to
Dr. B. BALASHANMUGAM M.D.S., Professor, Department of Orthodontics and Dentofacia l Orthopaedics, Tamilnadu Govt. Dental College and Hospital, Chennai - 3, for helping me with his valuable and
timel y suggestions and encouragement.
I take this opportunit y to express my gratitu de to my friends and colleagues for their valuable help and suggestions throughout this stud y.
I offer my heartiest pra yers and gratitude to my famil y members for their selfless blessings.
This agreement herein after the “Agreement” is entered into on this... da y of December 2014 between the Tamil Nadu Government Dental College and Hospital represented b y its Principal having address at Tamilnadu Government Dental college and Hospital, Chennai -03, (hereafter referred to as , ’the college’)
And
Dr. G. VIMALA aged 46 years working as professor at the college, having residence address at AP 115, 5t h Street, AF Block, 11t h main road, Anna nagar, Chennai 600040, Tamilnadu (Herein after referred to as the ‘Principal investigator’)
And
Dr. V. SENTHIL KUMAR aged 30 years currentl y studying as postgraduate student in department of Orthodontics in Tamilnadu Government Dental College and Hospital
(Herein after referred to as the ‘PG/Research student and co - investigator’).
Whereas the ‘PG/Research student as part of his curriculum undertakes to research “E VA L U A T ION OF C HA N GE S
IN HY OID B ON E P OS IT I ON A N D P HA R YN GE A L AI R WA Y
D IME N S ION S F OL LOW IN G MA N D IB U LA R S E T BA C K S U R GE R Y – A
C E P HA L OMET R IC ST U DY” for which purpose the PG/Principal
cop yright and confidentialit y issues that arise in this regard.
Now this agreement witnesseth as follows:
1. The parties agree that all the Research material and ownership therein shall become the vested right of the college, including in particular all the copyright in the literature including the stud y, research and all other related papers.
2. To the extent that the college has legal right to do go, shall grant to license or assi gn the cop yright do vested with it for medical and/or commercial usage of interested persons/entities subject to a reasonable terms/conditions including ro yalt y as deemed b y the college.
3. The ro yalt y so received b y the college shall be shared equall y b y all the parties.
4. The PG/Research student and PG/Principal Investigator shall under no circumstances deal with the cop yright, Confidential information and know – how generated during the course of research/stud y in an y manner whatsoever, while shall sole vest with the manner whatsoever and for an y purpose without the express written consent of the college.
5. All expenses pertaining to the research shall be decided upon b y the principal investigator/Co -investigator or borne sole b y the PG/research student (co-investigator) .
till its completion. However the selection and conduct of research, topic and area research by the student researcher under guidance from the principal investigator shall be subject to the prior approval, recommendations and comments of the Ethical Committee of the college constituted for this purpose. 8. It is agreed that as regards other aspects not covered under this agreement, but which pertain to the research undertaken b y the student Researcher, under guidance from the Principal Investigator, the decision of the college shall be binding and final.
9. If an y dispute arises as to the matters related or connected to this agreement herein, it shall be referred to arbitration in accordance with the provisions of the Arbitration and Conciliation Act, 1996.
In witness whereof the parties hereinabove mentioned have on this the day month and year herein above mention ed set their hands to this agreement i n the presence of the following two witnesses.
College represented b y its
Principal PG Student
Witnesses Student Guide
S.NO. TITLE PAGE NO.
1. INTRODUCTION 01
2. AIMS AND OBJECTIVES 06
3. REVIEW OF LITERATURE 07
4. MATERIALS AND METHODS 45
5. RESULTS 54
6. DISCUSSION 67
7. SUMMARY AND CONCLUSION 76
S. No. TOPIC PAGE No.
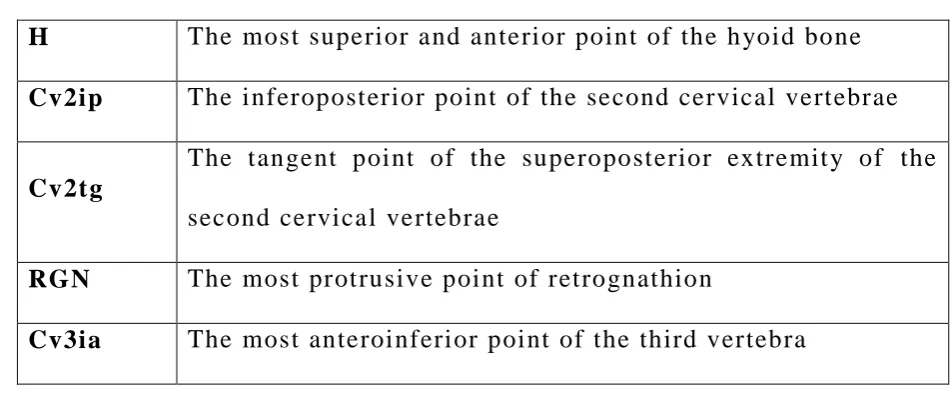
1 Cephalometric Landmarks used in this stud y 50
2 Measurements for Phar yngeal Airwa y Parameters 51
3 Measurements for H yoid Bone Parameters 52
4 Measurements for Dentofacial Parameters 52
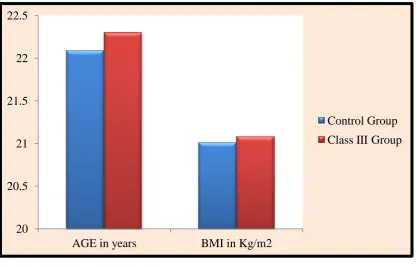
5 Distribution of study subjects based on gender 54
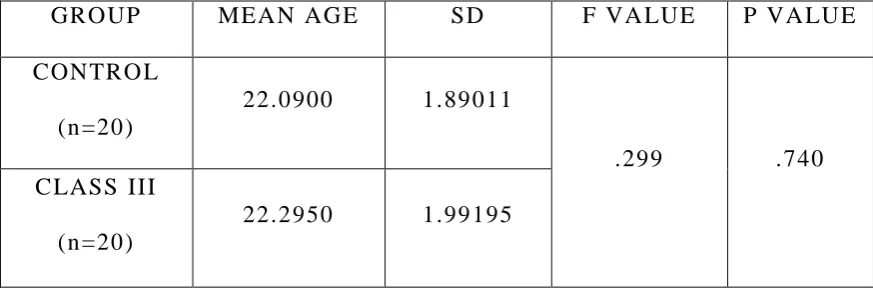
6 Distribution of study subjects based on age 55
7
Distribution of stud y subjects based on Bod y Mass
Index 55
8 Summar y of Class III treatment 56
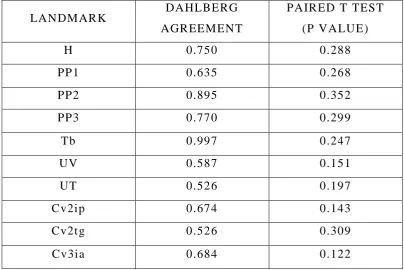
9 Assessment of method error in x coordinate 57
10 Assessment of method error in y coordinate 57
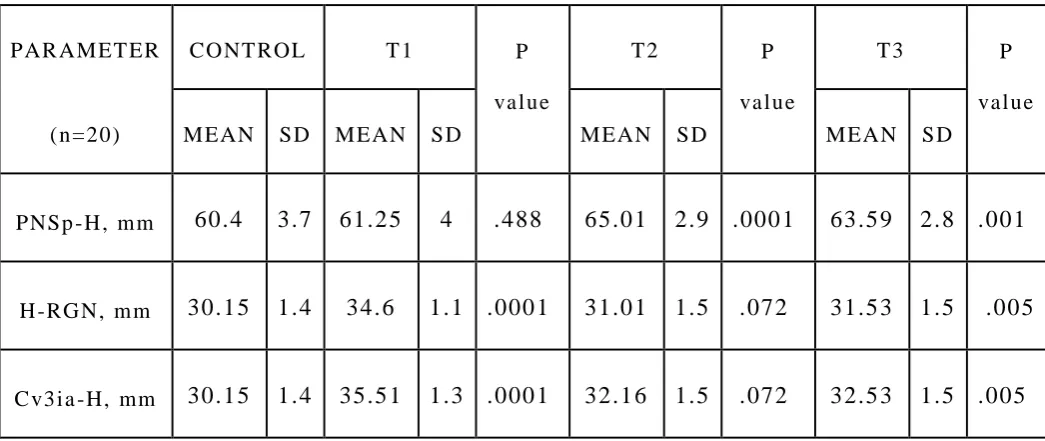
11 Comparison of dentofacial parameters at three stages
of treatment in class III 58
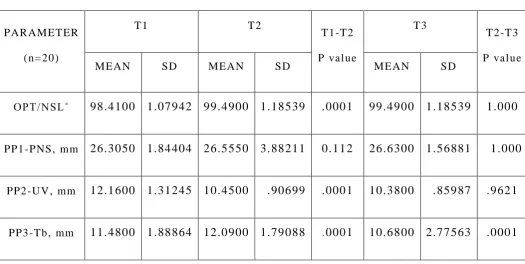
12 Comparison of phar yngeal airwa y parameters at three
stages of treatment in class III 58
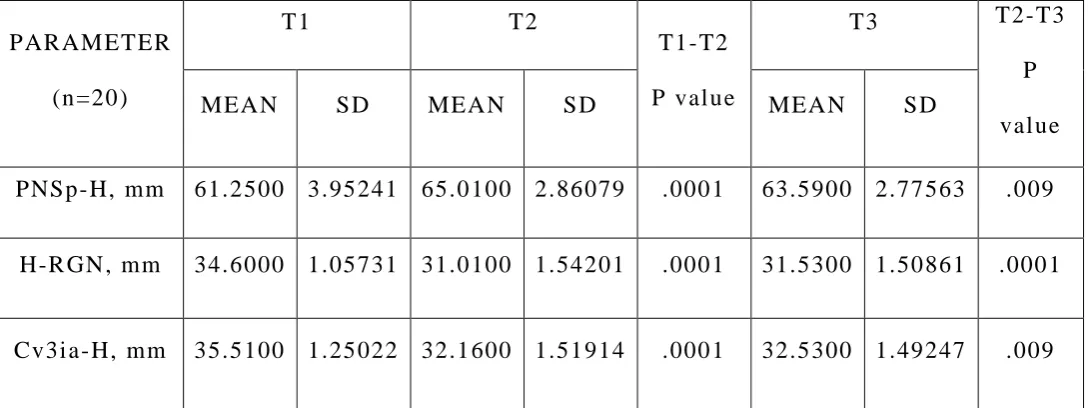
13 Comparison of h yo id bone parameters at three stages
of treatment in class III 59
14 Comparison of dentofacial parameters between control
and class III 59
15 Comparison of phar yngeal airwa y parameters between
control and class III 60
16 Comparison of h yo id bone parameters between control
groups
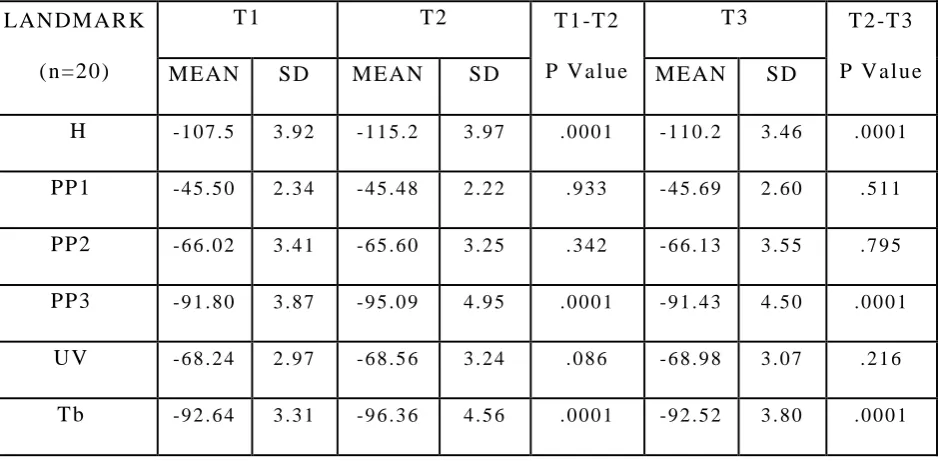
18
Comparison of vertical changes (mm) of landmarks in airwa y and h yoid bone at three times in class III groups
61
19
Comparison of horizon tal changes (mm) of landmarks in airwa y and h yoid bone in control and class III groups
62
20
Comparison of vertical changes (mm) of landmarks in
1. CEPHALOSTAT
2. HP 3545 MFP SCANNER
3. STANDARDIZATION WITH TRANSPARENT GRID
4. STANDARDIZATION WITH ADOBE PHOTOSHOP
5. CEPHALOMETRIC SOFTWARE
6. CEPHALOMETRIC ANALYSIS – LANDMARKS AND
PARAMETERS
7. DIGITIZED CEPHALOMETRIC TRACING CLASS I –
CONTROL GROUP
8. DIGITIZED CEPHALOMETRIC TRACING – CLASS
III PRETREATMENT (T1)
9. DIGITIZED CEPHALOMETRIC TRACING - CLASS
III POST SURGERY (T2)
10. DIGITIZED CEPHALOMETRIC TRACING - CLASS
1
INTRODUCTION
Phar yngea l airwa y space and h yoid bone positions have
been extensivel y studied in orthodontics. Numerous evidences
from cephalometric studies support a link between airwa y
dimensions, h yoid bone positions and maintenance of
dentofacial harmony.
The phar ynx is a 12 –14 cm long musculomembranous
tubular structure, shaped like an inverted cone1. It extends from
the cranial base to the lower border of the cricoid cartilage (the
level of the sixth cervical vertebra), where it becomes
continuous with the oesophagus2.
The phar ynx communicates with the nasal, oral and
lar yngeal cavities via the nasophar ynx, orophar ynx and
lar yngophar ynx respectivel y3. The nasophar ynx and the
orophar ynx have significant locations and functions as the y
form a part of the unit in which respiration and deglutition are
carried out. The nasophar ynx forming the upper part of
respirator y s ystem is connected anteriorl y with nasal cavit y and
posteriorl y it extends as orophar ynx. The orophar ynx extends
from the soft pal ate to the base of epiglottis (from second to
2
orophar ynx at the level of phar yng oepiglottic fold and the
h yoid, and then it continues up to the level of the sixth cervical
vertebra.
The phar ynx is c omposed of three coats: mucous, fibrous,
and muscular. The muscles of the phar ynx are three circular
constrictors and three longitudinal elevators. The constrictors
ma y be thought of as three overlapping cones which arise from
structures at the sides of th e head and neck and pass posteriorl y
to insert into a midline fibrous band, the phar yngeal raphe2. Its
lining mucosa is continuous with that lining the
phar yngot ympanic tubes, nasal cavit y, mouth and lar ynx1.
The h yoid bone is a horseshoe -shaped bone sit uated in the
anterior midline of the neck between the chin and the thyroid
cartilage. At rest, it lies at the level of the base of the mandible
in the front and the third cervical vertebra behind1 , 3. Unlike
other bones of neck h yoid does not have an y bon y articulations.
It provides attachments for ligaments, muscles, fascia of
cranium and mandible. The two major group of muscles
attached to h yoid bone are suprah yoid and infrah yoid muscles.
Both suprah yoid and infrah yoid muscles have wide range of
3
The h yoid bone pla ys an important and active part in
accomplishing the delicate balance between anterior and
posterior muscle tension relative to the occipital cond yles,
which in turn helps to balance the head as man assumed an
upright posture. It is evid ent that there exists a mutual
correlation between position of the h yoid bone, volume of
phar yngeal airwa y and dentofacial structures
Mandibular prognathism or skeletal Class III
malocclusion is one of the most severe maxillofacial
deformities. Th e word prognathism is derived from Greek
pro (forward) and gnathos (jaw). Mandibular prognathism is a
skeletal deformit y which is characterized b y abnormal
protrusion of mandible. Joffe defined mandibular prognathism
as a disorder of craniofacial growth in which facial profile is
impaired b y excess prominence of mandible. It is genetic and
manifests as familial.
Orthognathic surger y f or mandibular prognathism is done
for two major reasons. One reason is that orthodontic treatment
alone cannot produce a satisfactor y treatment result for
4
other reason is correction of functional problems like chewing
and speaking4.
Mandibular setback using bilateral sagittal split
osteotomy (BSSO) is routinel y done as an orthognathic surgical
procedure to treat mandibular prognathism that results in both
functional and aesthetic improvements. Mandibular setback
surger y can improve the occlusion, masticator y f unction, and
esthetics b y markedl y changing the position of the mandible5.
The orophar yngeal complex is also affected b y a posterior
movement of the mandible. Mandibular setback surger y causes
changes in the position of the h yoid bone and the tongue, and
consequent narrowing of the phar yng eal airwa y space (PAS).
Postoperative changes in the phar yngeal complex ma y inf luence
clinical features such as skeletal relapse and the airwa y size6
Gu et al7 postulated that the postoperative alteration in
position of the hyoid bone ma y cause relaxation of the
suprah yoidal musculature. The possible decreased tension of
suprah yoidal musculature ma y change the balance within the
head and neck musculature. This can result in an increased
5
the mandible forward again . If the orophar yngeal complex
exerts such an influence over a prolonged period, the related
changes in position of the h yoid bone and in the length of the
suprah yoid muscles ma y contribute to skeletal relapse.
Furthermore, the decrease in phar yngeal airwa y size could
induce breathing problems8.
Phar yngeal airwa y narrowing might be a reason for
obstructive sleep apnea (OSA ) 9. OSA is considered a risk
factor for s ystemic and pulmonar y h ypertension and cardiac
arrh ythmias and may increase morbidity and mortalit y1 0.
Therefore it is relevant to evaluate the changes in
nasophar yngeal airwa y and h yoid bone position in subjects with
prognathic mandible, who had combined orthodontic and
orthognathic surgery through mandibular setback.
This retrospective anal ytical cephalometric stud y has
been undertaken to evaluate and compare the phar yngeal airwa y
dimensions and h yoid bone positional changes in patients with
prognathic mandible who underwent mandibular setback
surger y through Bilateral Sagittal Split Osteotomy (BSSO).
6
AIMS AND OBJECTIVES
AIM OF THE STUDY
The Aim of this stud y is to evaluate the change s in h yoi d
bone and phar yn geal airwa y dimensions in patients wit h
prognathic mandible who had undergone mandibular setback
surger y
OBJECTIVES OF THE STUDY
To evaluate the h yoid bone position and phar yngeal
airwa y dimensions in skeletal class III patients who had
undergone mandibular setback surger y at pretreatment
(T1), postsurgical (T2) and post treatment (T3) stages. To evaluate the h yoid bone position and phar yngeal
airwa y dimension in normal skeletal class I patients
To compare the changes in h yoid bone position and
phar yngeal airwa y i n the above two groups
7
REVIEW OF LITERATURE
Numerous studies were found in literature with respect to
the growth characteristics and developmental aspects of
phar yngeal airwa y space, h yoid bone and tongue. The articles
relating to methods of assessing their existent measurements,
variations through the growth period and possible influence of
various orthognathic surgeries over the h yoid and airwa y are
plent y in literature. The most relevant studies are presented
here.
Carmine Durzo et al (1962)1 2 studied the growth behaviour of
the h yoid bone in relation to other craniofacial structures in a
series of five longitudinal cephalometric stud y. The y concluded
that the h yoid bone has a stable vertical position in norm al
individuals, at a level opposite the lower portion of third and
upper portion of fourth cervical vertebra. During growth its
relative position remains constant when it descends as the
cervical vertebrae increase their length and the cranial base and
mandible descend and move awa y from each other. In the
mandibular deformit y cases the h yo id movements followed
closel y those of mandibular growth movements and were
8
movements were also modified as pe r the demands of
maintaining a patent airwa y.
Ian Milne and John Cleall (1970)1 3 conducted a
cinefluorographic stud y on functional adaptation of
orophar yngeal structures at three ph ysiological developmental
phases. The stud y showed that oropharyngeal structures showed
marked abilit y to adapt to change in local dental environment.
Changes in the h yoid position were statisticall y significant in
rest position.
Lee W Graber (1978)1 4 studied the changes in h yoid bone in
30 skeletal class III patients who w ere treated with chin cup
orthopedic treatment for a period of three years between 6 and
9 years of age. The stud y with lateral cephalograms summarized
that a clockwise rotation of mandible occurred with mandible
being positioned in inferior and posterior direction. There was
also a resultant slight posterior and more of an inferior position
of h yoid bone. However neither such positional change of h yoid
bring about an y encroachment of pharyngeal space nor was the
inferior positioning entirel y attributed to growth changes. The
author states that airwa y patenc y is the primar y factor in
9
brought about both functional as well as morphologic
adaptations to the hyoid bone.
James A McNamara Jr (1981)1 5 tried to establish a possible
relationship between upper airwa y obstruction and trend of
craniofacial growth through four case reports consisting of an
ideal long face, a case of adenoidectomy, a case of combined
adenoidectomy and tonsillectomy and a case of late
nasophar yngeal obstruction. All these cases were found to be
having steep mandibular plane. Although the untreated ideal
long face had ver y little changes during follow up period, those
cases whish were treated with surgical removal of airwa y
obstruction were found to have reduced mandibular plane to
satisfactor y extent. The author recommended for further
randomized control trial to validate his observation.
Bibby, Preston (1981)1 6 in their landmark article presented the
novel method to determine the h yoi d bone position referred to
as the h yoid triangle which is formed b y the joining of three
cephalometric points namel y retrognathion, h yoidale and C3.
This method is different in a wa y that most of the previous
articles which studied the h yoid position used cranium as the
10
The authors related the h yoid bone to mandible and cervical
vertebrae and the y claimed that the mandible is at a more
comparable level to the axis of rotation than cranium and hen ce
head movement effect can be minimized and h yoid position can
be more reliabl y determined. The y applied the h yoid triangle in
54 normal class I patients and found a constant relationship
between cervical vertebrae and antero posterior position of
h yoid bone. The y also indicated that h yoid bone serves as a
bon y anterior border to the phar ynx and surprisingl y no sexual
dimorphism was noted.
W.J.B. Houston (1983)1 1 presented an interesting article on
errors in cephalometric measurements. He emphasized the
importance of distinguishing between a measurement bias and
random errors in sampling. He emphasizes that cephalometric
studies are prone to error when the samplin g method is not
randomized and invariabl y leads to measurement bias. When
evaluating individual radiographs, a highl y error prone
measurement relative to its total variabilit y has ver y little value
in clinical assessment. He sa ys that such results should b e
interpreted with caution because it is difficult to specif y limits
11
a part. He adds that adequate error calculation and control is
lacking in man y studies and ma y be grossl y misleading.
Bibby (1984)1 7 also used the same hyoid triangle to evaluate
the h yoid bone position in mouth breathers and tongue
thrusters. In this stud y 18 subjects comprising of mouth
breathing and tongue thrusting group were evaluated with pre
orthodontic lateral cephalo grams. The stud y showed that an y
postural alterations caused b y mouth breathing or tongue
thrusting did not affect the position of h yoid and it was
relativel y stable.
S.C. Cole (1986)1 8 described the difference between the terms
natural head position and natural head posture. These words
were s ynon ymousl y being used in literature to describe spatial
relationship between head and the true vertical or vertebral
column or both. Such generalized assumption leading to
confusion, the author considered the natur al head position
relating to true vertical and natural head posture to cervical
column. After investigating five groups of people, he found that
both these relationships are entirel y different with statistical
significance. Also of interest is that in thos e five anal yzed
12
significant difference and altering the natural head position can
itself produce class II or class III effects.
Ann Wenzel et al (1989)1 9 illustrated the possibilit y of
relationship between posture and airwa y size after mandibular
osteotomy using cephalograms of 52 mandibular prognathic
patients. 12 parameters were used to describe the sagittal and
vertical changes. Significant correlations between posture and
mandibular morpholog y before surgery and after surger y were
present but the other parameter did not have such correlations
with posture and hence concluded that mandibular morpholog y
pla ys a vital role in head posture determination.
Greco et al (1990)2 0 retrospectivel y evaluated the
h ypophar yngeal airwa y over long term after surgical correction
of mandibular h ype rplasia in 11 patients through cephalometr y
and concluded that h ypophar yngeal airwa y space narrows after
surger y and ma y lead to sleeping disorders in isolated cases.
Sorokolit, Nanda (1990)2 1 evaluated the postsurgical changes
following sagittal split ramus osteotomy (SSRO) stabilized with
rigid fixation with lateral cephalograms of 25 individuals with
13
was 5.1 ± 3.0 mm was achieve d. There was a relapse of 0.5 –
1.5 mm in these patients over long term post surgicall y. Though
the relapse was statisticall y significant, it was small enough to
be clinicall y insignificant. The authors claim that SSRO is a
stable surgical procedure.
Athanasiou et al (1991)2 2 studied the position of h yoid bone
and phar yngeal depth in 52 adult mandibular prognathism
patients who were treated with combined orthodontic and
surger y treatment. H yoid bone position and phar yngeal depth
were anal yzed at the level of second and fourth cervical
vertebrae using lateral cephalograms. The results obtained
showed onl y moderate correlations between the second and
fourth cervical vertebrae to their respective ref erence
coordinates. The stud y did not support t heir proposed
h ypothesis that surger y m a y reduce the airwa y and indicat ed
that reflex alteration of phar yngeal, supra h yoid and infra h yoid
muscles could take place.
Beni Solow et al (1993)2 3 examined natural head position
cephalograms of 50 males with s evere obstructive sleep apnoea
s yndrome between 28 -70 years of age confirmed with a
14
groups of health y samples as control. On evaluation the
craniocervical angulation was found to be extremel y large in
stud y group exceeding b y 1 -2 standard deviation than control
group. The authors suggested this feature to be ph ysiological
adaptation to maintain airwa y patenc y and proposed that
obstructive sleep apnoea could cause increased craniocervical
angle.
Lew (1993)2 4 explained the postsurgical changes in h yoid,
tongue and airway in patients with mandibular subapical
osteotomy in 28 Chinese adults with lateral cephalograms taken
pre and post operativel y. The intermaxillar y space decreased,
tongue moved posteriorl y and h yoid moved inferiorl y at short
term. Over long term the tongue and hyoid relapsed comparable
to their preoperative position, demonstrating their abilit y to
adapt to postoperative changes.
G.F.Shen et al (1994)2 5 gave a detailed cephalometric anal ysis
of upper airwa y in 116 normal Chinese population. The
preliminar y normal values for various hard and soft tissues of
upper airwa y were established for both sexes. The stud y showed
significant sexual dimorphism and pr edicted horizontal position
15
and suggested to use these values to investigate further airwa y
abnormalities.
Eung – Pw on Pae et al (1994)2 6 researched the upper airwa y in
both upright and supine positions using a cephalometr y and
electromyograph y. 20 OSA patients and 10 s ymptom free
patients were investigated. Decrease in orophar yngeal area and
increase in tongue cross sectional area was noted when OSA
patients changed from upright to supine posit ion. The y
concluded that changes in airwa y size due to postural change
from upright to supine should be considered while assessing the
pathogenesis in airwa y.
Enacar et al (1994)2 7 measured the changes in h yoid bone
position, tongue and airwa y changes in 15 mandibular setback
surger y patients with radiographs taken at 3 time intervals. A
decrease in h ypophar yngeal airwa y was noted which was
statisticall y significant and sustained over long term follow up.
The h yoid and tongue moved to an inferior position post
surgicall y. The author enacts that narrowed h ypopharyngeal
space and posteroinferior positioning of hyoid and tongue could
16
Miles, O`Reilly (1995)2 8 conducted a stud y to determine the
reliabilit y of landmark identification for those str uctures most
commonl y reported in the obstructive sleep apnoea literature.
Three judges were asked to identif y specific landmarks on 20
randoml y selected radiographs and 10 superior qualit y
radiographs. The results indicated that the majorit y of the
landmarks could be reliabl y identified, irrespective of the
qualit y of the radiograph. However, the qualit y of the
radiograph did affect identification of the horizontal position of
the h yoid bone and the linear measure of posterior airwa y space
although t hese were not clinicall y significant. The vertical
position of the tip of the soft palate was highl y unreliable,
irrespective of the qualit y of the radiograph. This resulted in
errors in the measurement of soft palate length.
Hochban et al (1996)2 9 raised a question about the chances of
mandibular setback causing sleep related breathing disorders b y
examining 16 consecutive patients who were anal yze d b y
cephalograms at 1 week, 3 months and 1 year after surgery. The
patients were also subjected to pol ysomno graphic evaluation
based on Marburg graded diagnostic protocol for sleep related
17
phar yngeal narrowing noted at in all patients none of them had
evidence of postoperative breathing disorder.
Taylor et al (1996)3 0 studied the pattern of bon y and soft tissue
growth of orophar ynx in 160 health y orthodonticall y untreated
children. The stud y showed that two periods of active growth (
6 to 9 years and 12 to 15 years ) and two periods of quiescence
(9 to 12 years and 15 to 18 years ) were found in the
orophar yngeal soft tissues.
S.E.Martin et al (1997)3 1 anal yzed the effect of age, sex,
obesit y and posture on upper phar yngeal airwa y size in 60 men
and 54 women with age range from 16 – 74 years, in both
seated and supine position using acoustic reflection. The stud y
found that, with increasing age all upper airwa y dimensions
except orophar yngeal junction decreased in size in supine
position. When compared to women, men had increased bod y
mass indices and large r neck circumf erences for an y matched
bod y mass index. Also men had greater changes in
orophar yngeal junction while in supine position. The authors
concluded that upper airwa y decreases with increasing age in
both sex with men prone to greater upper airwa y collapsibilit y
18
Nakagaw a et al (1998)3 2 investigated the upper airwa y changes
in 25 patients (12 males and 13 females) after mandibular
setback surger y b y anal yzing the lateral cephalograms taken at
3months, 6 months and 1 year postoperativel y. The authors
found great sexual dimorphism in their stud y as the pharyngeal
airwa y space and h yoid bone which decreased and moved
inferior respectively at short term continued to do so in males
but relapsed to presurgical position in females.
Murat Ozbek et al (1998)3 3 to prove the claim of prevailing
studies that craniocervical extension occurs in obstructive sleep
apnoea (OSA), conducted a cephalometric and
pol yso mnographic evaluation of 252 adult males. They were
divided into non apneic - snorers, mild, moderate and s evere
OSA groups based on apnoea + h ypo apnoea index. The stud y
confirmed the presence of craniocervical h yperextension in
OSA groups which increased with severit y.
Trenouth and Timms (1999)3 4 studied the association between
functional oropharyngeal airwa y and craniofacial morpholog y
19
positive correlation of orophar yngeal airwa y with length of the
mandible and cranial base angle.
Ayoub et al (2000)3 5 conducted a retrospective stud y to
evaluate the skeletal stabilit y following mandibular setback
surger y for correcting mandibular prognathism through two
t ypes of surgeries namel y sagittal split osteotomy (SSO) and
vertical subsigmoid osteotomy (VSO). Lat eral cephalograms of
31 patients divided into two above said surgical groups were
evaluated at three time points, before, immediatel y after and at
least one year after surger y. The recordings included Euclidean
distance matrix anal ysis apart from the linea r and angular
measurements along the x and y coordinates. The amount of
setback was not statisticall y significant but the amount of
relapse post surger y had statistical significance. There was
posteriorl y directed relapse of VSO group whereas the relapse
occurred in anterior direction in SSO group. The author
suggested that vertical subsigmoid osteotom y to be the better of
the two surgeries in view of relapsing tendenc y occurring in
posterior direction .
Turnbull, Battagel (2000)3 6 beautifull y anal yzed the effects of
20
qualit y of sleep on 32 orthognathic surger y cases. The digitized
lateral cephalograms were prospectivel y anal yzed from two
surgical groups, one treated with mandibular setback and other
with mandibular advancement. The daytime sleepiness changes
were assessed using a questionnaire along with overnight
domiciliar y sleep monitoring. The authors deduced that
retrolingual airwa y dimensions were greatl y reduced in setback
surger y patients, wher eas the same has significantl y increased
in mandibular advancement patients. The sleep study and
questionnaire revealed no significant changes in apnoeic
events. Interesting point of this stud y was that, in patients with
preexisting sleeping disorders, the mandibular advancement
surger y has actually increased the qualit y of sleep.
Tselnik, Pogrel (2000)3 7 retrospectivel y studied the changes in
phar yngeal airwa y space following mandibular setback surger y
in 14 adult patients taken at three time periods viz.
preoperativel y, immediatel y postoperativel y and long term. The
stud y showed a mean mandibular setback of 9.7mm. There was
a 28% decrease in linear distance in h ypophar ynx with mean
phar yngeal space getting reduced b y 1.52 cm2. A strong
correlation was found between quantum of mandibular setback
21
decrease in airwa y occurs over long term post surger y and can
lead to sleep apnea s yndrome in vulnerable individuals.
Athanasiou (2000)3 8 in his discussion regarding the stud y b y
Tselnik and Pogrel (2000), stated that though two dimensional
cephalometr y has some limitations, meeting certain technical
considerations like standardization of cephalograms and
assessing methodologi cal error can make them provide useful
information for estimation of tongue and nasophar ynx volume.
Stating that sleep related disorders do not occur in sitting and
standing posture, he advocated lateral cephalograms to be taken
in supine position too. He recommends supine endoscopy as a
promising choice since it is associated with apnea -h ypopnea
index and airwa y space.
Achilleos et al (2000)3 9 described the effects of mandibular
advancement surger y on h yoid position, soft palate, tongue and
phar yngeal airwa y through lateral cephalograms taken at 3 time
intervals. The h yoid and vallecula moved anterosuperiorly, the
tongue increased in length transientl y and the soft palate
became more upright at short term. The phar yngeal airwa y
22
making the authors indicate mandibular advancement as a
treatment approach in sleep apnoea patients.
Karim Mobarak et al (2000)4 0 described the long term
stabilit y of 80 consecutivel y treated bilateral sagittal split
osteotomy cases through lateral cephalograms taken on 6
occasions. The results showed mandibular setback to be a fairl y
stable procedure over long term evaluation.
Pushkar Mehra et al (2001)4 1 presented the stud y comparing
phar yngeal airwa y space changes in two groups of high occlusal
plane facial morpholog y patients whose correction included
anticlockwise rotation of maxilla mandibular complex. One
group ( group 1)which underwent double jaw surger y
comprising maxillar y and mandibular advancement and another
group (group 2) which underwent double jaw surger y
comprising maxillar y advancement and mandibular setback
were evaluated with pre and postsurgical lateral cephalograms.
The stud y conclude d that group 1 had an increased pharyngeal
airwa y space of 47% near soft palate and 76% near base of the
tongue. Whereas in group 2, patients had a decreased airwa y
23
Hence either setback or ad vancement of mandible has a
significant effect in altering phar yngeal airwa y dimensions.
Karim Mobarak et al (2001)4 2 assessed the long term changes
in soft tissue profile following mandibular setback osteotomy in
80 consecutive mandibular prognathic pa tients using lateral
cephalograms taken at 6 occasions . The stud y f ound males
having lesser ratios than women with significant changes in
upper lip and chin and also the skeletal rela pse in long term had
a greater influence on soft tissue profile. The auth or
recommended suitable modifications in prediction software
database to allow more accurate treatment simulations.
Liukkonen et al (2002)4 3 studied the long term effects of
mandibular setback surger y on airwa y size through digitized pre
and postoperative radiographs of 22 individuals with mean age
of 30 years. The authors explained that effects of surger y could
graduall y increase upper airwa y resistance in individuals with
insufficient neuromuscular adaptations and hence cases with
larger sagittal discrep ancies should be dealt with bimaxillar y
24
T. Muto et al (2002)4 4 measured the lateral cephalograms of 10
normal patients with head posture taken in five dif ferent
positions (total 50 cephalograms) to obtain a regression
equation and comp ared the relationship of cranio cervical angle
to the phar yngeal airwa y space. The authors found a strong
correlation between OPT/NSL (craniocervical angle ) and
C3-Me (third vertebra to M enton distance), concluding that for
ever y 10 degree increase in OPT/NSL or C3 -Me, phar yngeal
airwa y space increases b y 4mm
Battagel et al (2002)4 5 did a radiographic stud y of 100
Caucasian males of which 50 were non apnoeic snorers and 50
were diagnosed OSA patients. The lateral cephalograms with
patients moving from upright to supine position were anal yzed
and the results showed no significant diff erences between the
two groups. The airwa y behind soft palate showed maximum
constriction of 40%, with area behind tongue showing 20%
decrease, minor area increase in soft palate and h yoid dropping
and moving anteriorl y to maintain its relation with mandib le.
Cakarne et al (2003)4 6 estimated the values for pharyngeal
airwa y sagittal dimensions in three levels - nasal, oral, and
25
dentofacial skeletal morpholog y in comparison with Class I
patients with normal dentofacial morpholog y. Sample size of 32
patients with class III deformity were selected and
cephalometric radiographs were taken before and after
orthognathic surgery, a paired t test was used to evaluate the
difference between class I and Clas s III phar yngeal airwa y
Sagittal dimensions measurements and statistical anal ysis
revealed a highly significant dif ference in naso and
h ypophar yngeal levels. Authors concluded that pre and post
operative changes in phar yn geal airwa y dimensions after
bimaxillar y surger y showed statistically significant increase in
nasophar yngeal airwa y space, with out significant reduction in
oral and h ypophar yngeal level.
Saitoh (2004)4 7 assessed the phar yn geal airwa y morpholog y
changes over long term in patients who underwent combined
orthodontic treatment and mandibular setba ck surger y through
bilateral sagittal split ramus osteotomy. The assessment was
done at three stages pretreatment (T1), after 3 -6 months of
surger y (T2 ) and after 2 or more years after surger y (T 3). He
concluded that significant constriction of phar yngeal airwa y
occurred between T1 and T2 but between T2and T3 there was
26
tendenc y for relapse at T3 and attributed it to the normal
ph ysiological adaptation of phar yngeal structures to the now
stable and improved hard tissue relationships.
Fengshan Chen et al (2005)4 8 proposed a mathematical model
to predict the pharyngeal airwa y space changes b y stud ying 23
female adult patients who were treat ed with combined
orthodontic and mandibular setback surger y through BSSO.
The y anal yzed the lateral cephalograms within 6 months before
surger y (T1) and 1 to 1.5 years after surger y (T2)and gave the
equation as
PAS narrowing = 0.386 - 0.541 ANB (T1 - T2) + 0.253 Co -Gn
(T1 - T2) - 0.098 SN-GoGn (T1 - T2), Where,
ANB - Angle formed b y point A, Nasion and point B.
Co - Cond ylion
Gn - Gnathion
SN-GoGn - Mandibular plane
He added that in patients with predisposing factors like obesit y
and short neck s urger y can lead to sleep apnea s yndrome.
Kaw akami et al (2005)4 9 diligentl y studied the tongue, h yoid
and phar yngeal airwa y in 30 mandibular setback surger y cases,
27
intervals (preoperative, one month later and more than one year
post operativel y). The stud y showed significant downward
movement of h yoid 1 month after surger y but it returned to its
original position in later stages thereb y reducing the retro
lingual airwa y dimension. The author co ncludes that pharyngeal
airwa y relative to tongue and h yoid is maintained at short term
but gets reduced over longer time period and careful
observation is necessar y.
Eggensperger et al (2005)6 gave the treatise about long term
changes in h yoid bone and phar yngeal airwa y size changes after
mandibular setback surger y. 12 patients were chosen and
reviewed through serial cephalograms taken at 1 week. 6
months, 14 months and after an average of 12 y ears post
operativel y. The h yoid bone moved postero inferiorl y and ended
up 1.6 mm posterior to the original position at long term. The
suprah yoid muscles initiall y adapted to the skeletal changes due
to surger y, shortening b y 4mm but later correlated with the
change in h yoid bone. The lower phar yngeal airwa y, after the
initial decrease, remained almost constant over long term. The
middle and upper airwa y continued to decrease over long term
28
Guven et al (2005)5 0 anal yzed the effects of two t yp es of
mandibular surgeries on phar yngeal airwa y and h yoid bone. 30
patients of which 15 treated b y sagittal split ramus osteotomy
(BSSO) and 15 treated b y bod y osteotomy (BO), were anal yzed
using lateral cephal ograms at earl y and long term postoperative
periods. In both these groups a decrease in phar yngeal airwa y
space was noted earl y and late. Though h yoid moved
posteroinferiorl y in earl y stages, it relapsed to the original
anatomic position later. The decreas e in airwa y was less in BO
group when compared to BSSO group.
Malkoc et al (2005)5 1 evaluated the reproducibilit y of tongue,
h yoid and airwa y dimensions on standardized lateral
cephalograms. The lateral cephalograms were taken f or 30
patients, each three times at 30 minutes interval and were
anal yzed using twelve parameters and subjected it to statistical
anal ysis. The stud y resulted in no statisticall y significant
differences between these three sets of measurements and he
concluded that natural – head - position cephalograms can ver y
reliabl y used for measuring airwa y dimensions, tongue and
29
Oscar Martin et al (2006)5 2 assessed the nasophar yngeal soft
tissue patterns in 91 patients of Complutense universit y dental
school Madrid, who had ideal occlusion and no histor y of
airwa y abnormalities or sleeping disorders. The anal ys is of
digitized lateral cephalograms revealed a different
nasophar yngeal soft tissue pattern in men and women with men
having a larger nasal fossa and adenoidal ti ssue than women.
The length of the nasal fossa significantl y correlated with upper
airwa y thickness. The changes in upper airwa y dimensions were
mainl y dictated b y the upper airwa y thickness. Cranial base
length was significantl y related to the nasal fossa length and
thickness of lower phar yngeal airwa y.
Korkmaz Sayinsu et al (2007)5 3 aimed at evaluating the
measurement error variabilit y between a hand traced
conventional lateral cephalogram and a computer traced,
scanned and digitized cephalogram. 30 cephalograms f or each
method were deployed, the scan having a 300 dpi resolution and
the software being Dolphin imaging version 9.0, with two
operators performing both these processes twice. Statistics
showed no appreciable inter or intra operator variabilit y for
95% confidence limits. The y concluded that computer software
30
measurement errors when compared to traditional hand traced
cephalograms.
Fengshan Chen et al (2007)5 4 conducted a beautiful stud y of
comparison on short and long term changes between skeletal
class III patients treated b y bilateral sagittal spit osteotom y
onl y and patients treated b y combined Lefort one osteotomy and
mandibular setback. These patients were anal ysed at three
intervals viz. 6 months before surger y, 3 -6 months after surger y
and at least 2 years after surge r y. The mandibular setback group
had significant constrictio n of oral and h ypophar yngeal airwa y
size at short term and long term follow up. Surprisingl y the
bimaxillar y surgery group showed constriction onl y in short
term follow up whereas in long term fol low up no significant
changes were noted. He suggests that bimaxillar y surger y
should be performed for skeletal class III patients whenever
possible rather than single jaw surger y to prevent pharyngeal
airwa y narrowing a possible predisposing factor for ob structive
sleep apnoea.
Toshitaka Muto et al (2008)5 5 gave another equation utilizing
linear regression anal ysis for predicting airwa y space in
31
cervical vertebra and Menton (C3 – Me) was calculated in 29
female adults using lateral cephalograms before and 1 year after
treatment. The equation used is y = - 21.105 + 0.402x ( y: PAS;
x: C3-Me; r = 0.854). Comparing the predicted value with
conventionall y me asured value had more or less t he same
average with difference being ± 1.5mm.
Kitagaw ara et al (2008)5 6 determined the pharyngeal
morpholog y changes and respirator y f unction during sleep in 17
adult skeletal class III patients after bilateral sagittal split
ramus osteotom y. Phar yngeal airwa y was anal yzed using lateral
cephalograms and pulse oximetr y was used to measure the
arterial ox ygen saturation (SpO2) during sleep. No significant
changes were noted in the orophar yn geal region but h yoid was
found to be inferiorl y positioned. Althoug h decreased ox ygen
saturation was noted during sleep just after surger y, the patients
improved 1 month after surger y. However the author warns that
careful follow up is needed in potential sleep disorder patients.
T. Muto et al (2008)5 7 evaluated the phar yngeal airwa y and
soft palate changes in 49 women after bilateral sagittal split
osteotomy through radiographs obtained at 2 intervals. The
32
flexion, decreased SNB angle b y 3.9 degrees, decreased
phar yngeal airwa y b y 2.6 mm at retro palatal and 4.0mm at
retro lingual region and increased soft palate thickness b y
3.2mm. The study showed that setback surger y markedl y
decreases phar yngeal airwa y space sof t palate morphology.
Marsan et al (2008)5 8 examined the lateral cephalograms of 25
Turkish female mandibular prognathic patients treated with
combined orthodontic and mandibular setback surger y through
BSSO. Assessment was done before and 1.5 years after surger y.
The phar yngeal airwa y reduced and so ft palate length was
increased with significant change in lower facial morpholog y.
The author owes these changes to the normal ph ysiological
adaptation to the improved hard tissue relationships after
surger y.
Chang-Min Sheng et al (2009)5 9 conducted the research on
developmental Changes in phar yngeal airwa y depth and h yoid
bone position from childhood to young adulthood. The y
anal yzed the lateral cephalograms of 239 normal Taiwanese
who were divided into three groups based on age. In both th e
genders, the phar yngeal airwa y depth increased from mixed to
33
phar yngeal airwa y depth. The h yoid bone positions were
different in permanent dentition with association to mandibular
morpholog y in v ertical plane.
Aboudara et al (2009)6 0 compared the efficac y of airwa y space
deduction between a conventional lateral cephalogram and a
three dimensional cone beam computed tomograph y. Citing the
previous articles which have questioned the reliabilit y of lateral
cephalograms, he conducted this stud y to validate their claim if
it were true. The stud y resulted in a volumetric error range of
0% to 5% in cone beam computed tomograph y and a moderatel y
high correlation between airwa y volume and area. However
there was considerable variabilit y in the airwa y volumes for
similar airwa y in lateral cephalograms. He concluded that cone
beam computed tomograph y to be more effective than lateral
cephalograms.
Grauer et al (2009)6 1 assessed the airwa y shape and volume in
62 non growing patients who belonged to different dentofacial
skeletal pattern using computerized cone beam tomograph y.
Instead of rel ying on linear measurements this stud y emplo yed
virtual three dimensional surface models to deduce the airwa y.
34
with sagittal jaw relation and so was between airwa y volume
and size of the face. Incidentall y there was no significant
relationship to the vertical proportions. The class II patients
had a forwardl y in clined airwa y while the class III had a more
verticall y oriented one. He concluded that airwa y volume rather
than shape differs with different vertical jaw relationships and
for sagittal relationships the y both vary.
Toru Kitahara et al (2009)6 2 h ypotheticall y tested the stabilit y
of hard and soft tissues after subjecting 45 female adult patients
to either intraoral vertical osteotomy or sagittal split ramus
osteotomy. The lateral cephalograms were anal yzed at three
standard time intervals. While the pretr eatment evaluation
showed no significant differences in these two groups, the post
treatment evaluation showed the mandible being positioned
more posteriorl y in IVRO group. The soft tissue M enton was
located more backward too. The authors concluded that pa tients
treated with IVRO surger y had a more posterior relation of
mandible compared to SSRO and advised to take this feature in
consideration while planning treatment.
Degerliyurt et al (2009)6 3 experimented the possibilit y of
35
through mandibular setback or bimaxillar y surger y using
computed tomograph y (CT). 34 women and 13 men with
skeletal class III deformities were screened pre and post
operativel y with CT and the results showed decreased
anteroposterior and cross sectional dimension of pharyngeal
airwa y in setback group in both sexes. The bimaxillar y group
had onl y the mid sagittal dimension reduced. The statistical
significance was lac king for both these groups in
anteroposterior dimension. The author highlighted that no
sexual dimorphism is present in airway relating to orthognathic
surger y.
Toru Kitahara et al (2010)6 4 had the purpose of examining 46
Japanese women having skeletal c lass III malocclusion for
changes in phar yn geal airwa y space stabilit y and positional
change of h yoid bone. Of the 46 subjects, 25 underwent single
jaw mandibular setback surger y through bilateral sagittal split
ramus osteotom y (SSRO) and 21 underwent bilateral intraoral
vertical ramus osteotom y (IVRO). The control group comprised
of 30 women volunteers who had normal occlusion. The
assessment was done at 3 stages; preoperative, im mediatel y
after surger y and after postsurgical orthodontic treatment. To
36
space compared to control group which was significantl y
reduced after setback surger y. In the SSRO group the h yoid
moved in an upward and forward direction with lower border of
phar yngeal airwa y following it. But in IVRO group, the h yoid
bone and the anterior border of airwa y moved in backward
direction. The authors concluded that narrowing of airwa y
occurs post surgicall y i n IVRO group but occurs during surger y
in SSRO group. An added note is that the postsurgical airwa y of
class III group is comparable to the pre -treatment airwa y of
class I control group.
Ashok Kumar Jena, Satinder Pal Singh (2010)6 5 studied the
sagittal mandibular development effects on the dimensions of
the awake phar yng eal airwa y passage in 91 patients classified
into three groups as normal, prognathic and retrognathic
mandible. Their stud y showed the length of the soft palate
significantl y smaller in m andibular prognathism subjects than
in subjects with mandibular retrognathism. The thickness of the
soft palate was significantl y greater among subjects with
mandibular prognathism than in subjects with normal and
retrognathic mandibular development. The s agittal mandibular
development had no effect on the dimensions of the
37
Zhe Zhong et al (2010)6 6 evaluated the Upper Airwa y among
different Skeletal Craniofacial Patterns in Non -snoring Chinese
Children. Two groups of subjects were studied. A group of
subjects with a normo divergent facial pattern was divided into
three subgroups according to ANB angle (Class I, II, or III). A
second group of subjects with a normal sagittal facial pattern
was divided into t hree subgroups according to the FH -MP angle
(low angle, normal angle, or high angle) In the group of
subjects with a normodivergent facial pattern, a significant
tendenc y for reduced upper airwa y dimension in the inferior
part (palatophar yn geal and h ypopha r ynx) was found in the
Class III, Class I, and Class II subgroups, in that order. In the
group of subjects with a normal sagittal facial pattern, the
superior part of the airwa y (nasophar yngeal and
palatophar yngeal) decreased with increasing mandibular pla ne
angle.
Rodrigues et al (2010)6 7 compared the validit y of digitized
cephalograms through indirect method with direct digital
radiographs. The y obtained the indirect digital radiographs
through two digital cameras at a fixed distance of 25cm and 60
38
with the direct digital radiographs. The images from the
scanner showed clinicall y insignificant differences. The images
from camera placed at 60 cm were clinicall y acceptable while at
25cm the images were largel y distorted.
Manish V aliathan (2010)6 8 compared the changes in
orophar yngeal volume after extraction vs non extraction
treatment using cone beam computed tomograph y in twent y
patients. The patients were matched for age, gender, body mass
index and other variables. While the de ntal parameters showed
significant changes from pretreatment to post treatment there
were no significant changes in orophar yngeal airwa y volume in
extraction and non -extraction patients.
Sooshin Hw ang et al (2010)6 9 deliberated the h yoid, tongue,
phar yngeal airwa y and head posture changes in 60 class III
patients treated with mandibular setback surger y through
intraoral vertical ramus osteotomy (IVRO). Of these 45 patients
had an additional Lefort I osteotomy performed. Lateral
cephalograms were assessed a t 4 time periods. The results
showed h yoid moving inferoposteriorl y and tongue moving
posteriorl y. The h yoid relapsed antero superiorl y during
39
airwa y and remained so even during the observation p eriod with
Lefort I osteotomy having no signi ficant effect on airwa y.
Craniocervical h yp erflexion was also noted. The author calls
for close monitoring of airwa y space post surger y through
IVRO.
Austin Phoenix et al (2011)7 0 examined the h yoid bone
changes in adolescents treated with rapid maxillar y expansion
b y measuring the hyoid bone to mandibular plane distance using
lateral and frontal cephalograms. The sample consisted of 138
subjects treated with RME and 148 control subjects treated
without RME. The RME groups had decreased lateronasal
width, inter premolar width and increased h yoid to mandibular
plane distance when compared to non RME group to begin with.
However there were statisticall y significant changes in those
parameters after treatment. The tongue length did not show an y
significant changes through treatment in all these patients.
Kyung-Min Oh et al (2011)7 1 studied the form and size of the
phar yngeal airwa ys in Preadolescents among various skeletal
patterns, using cone -beam computed tomograph y. The
inclination and the volume of the phar ynge al airwa y were
40
cephalometric variables. The stud y concluded that Children
with Class II malocclusion have more backward orientation and
smaller volume of the phar yngeal airwa y than do children with
Class I and III malocclusion. Inclination of the oropharyngeal
airwa y might be a ke y factor in determining the form of the
entire phar yngeal airwa y and is related to head posture
Yoshihiko Takemoto et al (2011 )7 2 anal ysed the pharyngeal
airwa y in 25 prognathic girls and compared it with 15 girls with
normal occlusion using lateral cephalograms. The stud y showed
that prognathic girls had a significantly wider lower pharyngeal
airwa y when compared with control group. The mandible in
prognathic girls tends to be p ositioned more anteriorl y,
resulting in a wider lower phar yngeal airwa y.
Sara M. Wolfe et al (2011)7 3 conducted a serial cephalometric
stud y on Craniofacial growth of Class III subjects six to sixteen
years of age at three time points ,6 –8, 10–12, and 14–16 years
of age. She compared the Class I subjects with the Class III
subjects and found that class III subjects had signif icantl y
larger mandibular plane angles, gonial angles, mandibular
ramus heights and corpus length, and SNB angles. Maxillar y
41
remained smaller in Class III subjects Lower face height,
maxillar y-mandibular differential, and mandibular bod y length
were also significantl y larger and increased significantly more
between 6 and 16 years of age in Class III subjects. She
concluded that AP maxillomandibular relationship of Class III
subjects worsens over time. AP discrepancies are primaril y due
to excessive mandibular growth, which produces a protrusive,
h yperdivergent phenot ype.
Ashok Kumar Jena, Ritu Duggal (2011)7 4 anal ysed the h yoid
bone position in subjects with different vertical jaw d ys plasias
79 north Indian adults with age range of 15 to 25 years were
selected and were divided into three groups based on their
FMA. The cephalometric stud y concluded that anteroposterior
position of h yoid bone was significantl y f orward in subjects
with low FMA and also the axia l inclination of h yoid bone
closel y f ollowed the axial inclination of mandible.
Hakan, Palamo (2011)7 5 evaluated the nasal passage and
orophar yngeal volumes for different dentofacial patterns b y
dividing 140 patients into class I class II and class III gr oups
who were further subdivided based on SNA and SNB angles.