ELASTOMERIC LIGATURES VERSUS CONVENTIONAL
ELASTOMERIC LIGATURES IN THE CANINE
RETRACTION PHASE OF PRE ADJUSTED EDGEWISE
APPLIANCE THERAPY : AN IN-VIVO STUDY"
Dissertation Subm itted to
THE TAMILNADU DR. M.G.R. MEDICAL
UNIVERSITY
For partial fulfillm ent of the requirem ents for the degree of
MASTER OF DENTAL SURGERY
BRANCH – V
ORTHO DONTI CS AND DENTO FACI AL O RTHO PAEDI CS
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY
CHENNAI – 600 032
2014 – 2017
ELASTOMERIC LIGATURES VERSUS CONVENTIONAL
ELASTOMERIC LIGATURES IN THE CANINE
RETRACTION PHASE OF PRE ADJUSTED EDGEWISE
APPLIANCE THERAPY : AN IN-VIVO STUDY"
Dissertation Subm itted to
THE TAMILNADU DR. M.G.R. MEDICAL
UNIVERSITY
For partial fulfillm ent of the requirem ents for the degree of
MASTER OF DENTAL SURGERY
BRANCH – V
ORTHO DONTI CS AND DENTO FACI AL O RTHO PAEDI CS
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY
CHENNAI – 600 032
2014 – 2017
ELASTOMERIC LIGATURES VERSUS CONVENTIONAL
ELASTOMERIC LIGATURES IN THE CANINE
RETRACTION PHASE OF PRE ADJUSTED EDGEWISE
APPLIANCE THERAPY : AN IN-VIVO STUDY"
Dissertation Subm itted to
THE TAMILNADU DR. M.G.R. MEDICAL
UNIVERSITY
For partial fulfillm ent of the requirem ents for the degree of
MASTER OF DENTAL SURGERY
BRANCH – V
ORTHO DONTI CS AND DENTO FACI AL O RTHO PAEDI CS
THE TAMILNADU DR. M.G.R MEDICAL UNIVERSITY
CHENNAI – 600 032
This is to certify that Dr.Abdul Shameer CK, Post graduate student (2014
– 2017) in the Department of Orthodontics and Dentofacial orthopaedics branch V, Tamil Nadu Government Dental College and Hospital, Chennai –600 003 has done this dissertation titled “Clinical efficiency of new generation elastomeric
ligatures versus conventional elastomeric ligatures in the canine retraction phase of pre adjusted edgewise appliance therapy : An In-vivo study” under my direct guidance and supervision for partial fulfillment of the M.D.S degree examination in April 2017 as per the regulations laid down by The Tamil Nadu Dr. M.G.R. Medical University, Chennai -600 032 for M.D.S., Orthodontics and Dentofacial orthopaedics (Branch–V) degree examination.
Guided By Dr.G.VIMALA M.D.S.,
Professor and HOD,
Department of Orthodontics & Dentofacial Orthopaedics, Tamil Nadu Government Dental College & Hospital,
Chennai - 600 003
Dr .B. SARAVANAN, M.D.S., Ph.D., Principal,
I, Dr. ABDUL SHAMEER CK, do hereby declare that the dissertation titled“Clinical efficiency of new generation elastomeric ligatures versus
conventional elastomeric ligatures in the canine retraction phase of pre adjusted edgewise appliance therapy: An In-vivo study”was done in the Department of Orthodontics, Tamil Nadu Government Dental College & Hospital, Chennai 600 003. I have utilized the facilities provided in the Government Dental College for the study in partial fulfillment of the requirements for the degree of Master of Dental Surgery in the specialty of Orthodontics and Dentofacial Orthopaedics (Branch V) during the course period 2014-2017 under the conceptualization and guidance of my dissertation guide, Professor and HOD Dr. G.VIMALA MDS.
I declare that no part of the dissertation will be utilized for gaining financial assistance for research or other promotions without obtaining prior permission from The Tamil Nadu Government Dental College & Hospital.
I also declare that no part of this work will be published either in the print or electronic media except with those who have been actively involved in this dissertation work and I firmly affirm that the right to preserve or publish this work rests solely with the prior permission of the Principal, Tamil Nadu Government Dental College & Hospital, Chennai 600 003, but with the vested right that I shall be cited as the author(s).
First of all, I seek the blessings of the Almighty God without whose benevolence; the study would not have been possible.
My sincere and heartfelt thanks to Dr. SARAVANAN M.D.S., our Principal, Tamil Nadu Government Dental College and Hospital, Chennai – 3,for his continuous and enormous support in allowing me to conduct this study and for his constant encouragement and advice during my tough phases in curriculum.
I take this opportunity to thank my parents KMA khader and shahida beevi, my wife Dr febin and my brother Afsal khan for their endless patience during the entire period of this three years of course.
It is my privilege and great honor to express my gratitude to my respected guide and Professor and Head, Dr. G.Vimala M.D.S., Department of Orthodontics and Dentofacial Orthopaedics, Tamilnadu Govt. Dental College and Hospital, Chennai-3, for her conceptualization,patience guidance, support and encouragement throughout the study and during the three years of course.
of Orthodontics and Dentofacial Orthopaedics, Tamilnadu Govt. Dental College and Hospital, Chennai-3, for helping me with his valuable suggestions and encouragement.
I owe my thanks to, Dr.VijaykanthMDS., Dr.G.UshaRao,M.D.S., Dr.M.D.Sofitha, M.D.S., Dr.K.Usha,M.D.S., Dr.D.Nagarajan,M.D.S., Dr.Mohammad Iqbal, M.D.S., Dr.Jayanthi,M.D.S. Dr.Selvarani,M.D.S., Associate and Assistant Professors, Department of Orthodontics, Tamilnadu Government Dental College and Hospital, Chennai-3 for their support and encouragement.
I thank Dr.Praveen ,for helping me with the Statistics in the study.
I offer my gratitude to my patients who expressed complete cooperation for the successful completion of this study
This agreement herein after the “Agreement” is entered into on this day... day of December 2016 between the Tamil Nadu Government Dental College and Hospital represented by its Principal having address at Tamilnadu Government Dental college and Hospital, Chennai-03, (hereafter referred to as the
‘college’)
And
Dr. G.Vimala M.D.S aged 48 years working as professor in the Department of Orthodontics and Dentofacial orthopaedics, at the college, having residence address at AP 11, 5th street, AF Block, 11th main road, Anna nagar,
Chennai 600040, Tamilnadu (herein after referred to as the ‘Principal
investigator’)
And
Dr. Abdul shameer CK aged 29 years currently studying M.D.S (Orthodontics) in Tamilnadu Government Dental college and Hospital (herein afterreferred to as the ‘PG/Research student and co-investigator’).
Whereas the ‘PG/Research student as part of his curriculum undertakes to
research on.“Clinical efficiency of new generation elastomeric ligatures versus
issues including in particular the copyright and confidentiality issues that arise in this Regard.
Now this agreement witnesseth as follows:
1. The parties agree that all the Research material and ownership therein shall become the vested right of the college, including in particular all the copyright in the literature including the study, research and all other related papers.
2. To the extent that the college has legal right to do go, shall grant to licence or assign the copyright do vested with it for medical and/or commercial usage of interested persons/entities subject to a reasonable terms/conditions including royalty as deemed by the college.
3. The royalty so received by the college shall be divided equally by all the parties.
4. The PG/Research student and PG/Principal Investigator shall under no circumstances deal with the copyright, Confidential information and know how generated during the course of research/study in any manner whatsoever, while shall sole vest with the manner whatsoever and for any purpose without the express written consent of the college.
5. All expenses pertaining to the research shall be decided upon by the principal investigator/Co-investigator or borne sole by the PG/research student(co-investigator).
this regard.
7. The principal investigator shall suitably guide the student Research right from selection of the Research Topic and Area till its completion. However the selection and conduct of research, topic and area research by the student researcher under guidance from the principal investigator shall be subject to the prior approval, recommendations and comments of the Ethical Committee of the college constituted for this purpose.
8. It is agreed that as regards other aspects not covered under this agreement, but which pertain to the research undertaken by the student researcher, under guidance from the Principal Investigator, the decision of the college shall be binding and final.
9. If any dispute arises as to the matters related or connected to this agreement herein, it shall be referred to arbitration in accordance with the provisions of the Arbitration and Conciliation Act, 1996.
10. In witness whereof the parties hereinabove mentioned have on this the day month and year herein above mentioned set their hands to this agreement in the presence of the following two witnesses.
College represented by its
Principal PG Student
Witnesses Student Guide
S.NO. TITLE PAGE NO.
1.
INTRODUCTION 1
2.
AIMS AND OBJECTIVES 4
3.
REVIEW OF LITERATURE 5
4.
MATERIALS AND METHODS 27
5.
RESULTS 43
6.
DISCUSSION 55
7.
SUMMARY AND CONCLUSION 63
8.
BIBLIOGRAPHY 65
9.
S. No. TOPIC
PAGE No.
[image:10.595.101.517.135.396.2]1
Table 1: Mean measurements in Group A-students t test 46
2 Table 2 : Mean measurements in Group B -students t test 47
3
Table 3 : Mean measurements in Group C-students t test 48
4
Table 4: Mean measurements in maxilla–one way ANOVA 49
5
S. No. TOPIC
PAGE No.
1
Graph 1: canine retraction rates in mandible 51
2
Graph 2: canine retraction rates in maxilla 51
3 Chart 1: canine rotation maxilla 52
4 Chart 2: canine rotation mandible 52
5 Chart 3: molar rotation maxilla 53
6 Chart 4: molar rotation mandible 53
7 Chart 5: anchor loss maxilla 54
1. Figure 1: Discover gel etchant 2. Figure 2: Primer
3. Figure 3: Orthodontic adhesive- 3M, USA
4. Figure 4: Light curing unit
5. Figure 5: Pre-adjusted edgewise bracket kit (MBT prescription, slot size 0.022 X 0.028 in)
6. Figure 6: Preformed bands with Upper double and lower double buccal tubes
7. Figure 7: Slide ligatures (Leone, Sesto Fiorentino,)
8. Figure 8: Slide ligatures (Leone, Sesto Fiorentino,)
9. Figure 9: Super Slick ligatures (TP Orthodontics, LaPorte, Ind)
10. Figure 10: Conventional ligature modules- 3M (Monrovia,CA USA)
11. Figure 11: 0.017 X 0.025-in stainless steel archwires
12. Figure 12: Niti Closed Coil Springs With Eyelets
13. Figure 13: Digital vernier caliper
14. Figure 14: Tension Gauge (Dontrix, TP orthodontics
15. Figure 15: Model with grid
16. Figure 16: Model analysis
17. Figure 17: Molar rotation measurement
18. Figure 18: Canine rotation measurements\
19. Figure 19: Maxillary acrylic plug
20. Figure 20: Mandibular acrylic plug
21. Figure 21: Right lateral view- group C
[image:12.595.114.513.99.763.2]24. Figure 24: mandibular occlusal
25. Figure 25: right lateral view( group B)
26. Figure 26: left lateral view( group c)
27. Figure 27: maxillary occlusal view
28. Figure 28: mandibular occlusal view
29. Figure 29:right lateral view(group C)
30. Figure 30 : right lateral view (group A)
31. Figure 31: maxillary occlusal view
32. Figure 32: mandibular occlusal view
33. Figure 33: right lateral view ( group B)
34. Figure 34: left lateral view ( group C)
35. Figure 35: maxillary occlusal view
[image:13.595.116.512.69.498.2]
1.
Participant information sheet (English)
2.
Participant information sheet (Tamil)
3.
Informed consent form in English
4.
Informed consent form in Tamil
MLP Midline pointer
AWT Anterior wire tip
PWT Posterior wire tip SST Super slick ligature tie
PEA Pre adjusted edgewise appliance
SS Stainless steel
FR Frictional resistance
SLB Self-ligating bracket
T0 (base line)–study models before retraction of canines
T1–T5 Study models at the end of every month for 5months or until
completion of canine retraction whichever is earlier
INTRODUCTION
One of the principal goals in orthodontics is to offer the most effective and efficient tooth movement and this quest for efficiency has stirred the development of innumerable materials in orthodontics intended at optimizing patient comfort and reducing treatment time., Friction being an imperative element in clinical orthodontics affects all stages of treatment and high frictional forces can affect the treatment results along with duration in a deleterious manner.
Resistance to tooth movement is frequently encountered during orthodontic tooth movement, when an archwire slides through the bracket slot (En-masse retraction of anterior teeth) or the bracket slides over the archwire (Individual canine retraction), because attributed to friction between the intermingling components of the orthodontic appliances such as brackets and archwires2. Frictional resistance must be kept to a minimum during sliding mechanics so that orthodontic tooth movement can be generated through light optimal forces7.Many factors have been linked to influence frictional resistance such as bracket-wire interaction, archwire material ,bracket width and interbracket distance, archwire diameter and cross sectional shape, wire stiffness, bracket material and wear of the wire , active torque, bracket-wire angulations, surface roughness of the wire, method of ligation, sliding velocity, and saliva3. Friction (static or kinetic) results from the interaction between an arch-wire and the sides of bracket and ligature.
reduce frictional force from ligation, various ligation methods and materials have been tried like slackened stainless steel ligatures , modified elastomeric modules stainless steel ligatures coated with fluorine-containing resins etc
Quest for finding various modalities to reduce friction at bracket archwire interface has brought in two more types of elastomeric ligatures namely Slide ligatures (Leone, Sesto Fiorentino) and super Slick ligatures (TP Orthodontics, laporte, Ind). Slide ligatures (Leone, Sesto Fiorentino) introduced in 2005,are novel ligatures made of a special polyurethane mix contrived by the injection moulding technique with the claims of lowering the levels of friction duringtreatment mechanics using with pre-adjusted edgewise appliances9. Previous in-vitro studies and a few clinical studies have shown that nonconventional elastomeric ligatures can reduce frictional resistance compared with conventional ligatures during initial levelling and aligning phase of orthodontic treatment16. The Super Slick Ties(SSTTM) is a new polymeric coated ligature tie –manufactured using Metafasix technology, has been marketed by TP Laboratories (La Porte, Ind) with the quoted advantage of potential reduction in treatment time by reduction in friction.
encountered only during retraction stage.Since information regarding friction during retraction stages are not yet clearly reported in the previous scanty studies, this study was undertaken to assess whether there is reduction in frictional resistance while using these non-conventional elastomeric modules when compared to conventional elastomeric modules, during retraction and space closure stages.
AIM AND OBJECTIVES
AIM
To evaluate the clinical efficiency of nonconventional new generation elastomeric ligatures – (Slide, Leone Orthodontic products, Italy) & Super Slick Ties(SSTTM)during individual canine retraction phase of PEA therapy
OBJECTIVES
1. To study the rate of canine retraction ,canine and molar rotation and anchorage loss using nonconventional new generation elastomeric ligatures – (Slide, Leone Orthodontic products, Italy) & Super Slick Ties(SSTTM ) during individual canine retraction phase in maxilla and mandible
2. To study the rate of canine retraction, canine and molar rotation and anchorage loss using conventional elastomeric ligatures.
REVIEW OF LITERATURE
De Franco DJ (1995)17 compared static frictional resistances between Teflon coated stainless steel and clear elastomeric ligatures used with various combinations of brackets and archwires. Stainless steel metal, polycrystalline ceramic and single crystal ceramic 0.022 inch slot brackets were used in blend with stainless steel and nickel titanium archwires of 0.018 inch and 0.016 X 0.022 inch.The results indicated that Teflon-coated ligatures produced less friction than elastomers for all bracket-archwire combinations. Ceramic brackets generally showed greater frictional resistances than stainless steel brackets. The study also suggested that sliding mechanics were best implemented with stainless steel brackets and stainless steel archwires. The study also elicited the usefulness of Teflon-coated ligatures in minimizing the high friction of ceramic brackets when an esthetic appliance is imperative.
Thomas S, Sherriff M and Birnie D(1998)18 investigated the frictional characteristics of two types of self-ligating brackets (‘A’ Company Damon SL and Adenta Time brackets) and two types of pre-adjusted edgewise brackets (TP
Tip-Edge and ‘A’ Company Standard Twin brackets).An instron 1193 testing machine
was used to check the frictional resistance between the bracket wire combinations and the data was evaluated and the results showed that self-ligating brackets produce less frictional resistance than elastomerically tied pre-adjusted edgewise brackets.
different ligation methods, one elastic module and the other stainless steel ligature wire. The frictional forces were measured as the resistance offered by the wire to the direction of movement of the arm. Stainless steel alloys have been proven to allow the least amount of friction among the vast number of materials available to the clinician. Therefore, they do not tax the anchorage units as much as the rest of the wire materials. The study concluded that the lowest frictional resistance was seen in stainless steel, followed by chrome-cobalt alloy, nitinol and copper-Niti. The beta-titanium had the highest frictional values recorded.
Iwasaki LR, Beatty MW, Randall CJ and Nickel JC (2003)20examined the effects of bracket ligation forces and mastication on friction when sliding a bracket along an archwire. The results suggested that vibration introduced by mastication did not eliminate friction when sliding a bracket along an archwire. In addition, there was considerable intra-operator variation, although ligation techniques were well controlled. Variations in clinical ligation forces are likely to be equal or greater than these experimental data. These variations could affect treatment efficiency.
X 0.025 inch stainless steel archwire, saliva-lubricated slick modules can reduce static friction at the module/archwire interface by up to 60%, regardless of the bracket system. The SPEED brackets produced the lowest friction compared with the 3 other tested bracket systems when regular modules were used. The use of slick modules, however, with all of the ligated bracket types tested significantly reduced friction to below the values recorded in the SPEED groups. Loosely tied stainless steel ligatures were found to generate the least friction.
Thorstenson GA and Kusy R P(2003)22coupled rectangular stainless steel (SS) archwires with four SS bracket designs: Mini Diamond Twin, VersaT, Shoulder and Synergy. Mini Diamond Twin brackets ligated with rings and SS ligature wires; VersaT brackets ligated with rings; Shoulder brackets ligated with rings in a figure-8 and a figure-O around the tie-wings; and Synergy brackets ligated with rings around the outer tie-wings and around the inner tie-wings. In both states, the coefficients of friction were similar for the Mini Diamond Twin, VersaT, and Synergy brackets; the values for the Shoulder brackets were slightly greater than for the other three designs. In the passive configuration, the features of the Shoulder and Synergy brackets reduced RS when the rings were not in contact with the archwires. In the active configuration, the binding behavioral patterns of the brackets were not influenced by ligation methods. Thus, these different ligation types and methods only affected the classical frictional component of RS in the passive configuration.
introduced by gum chewing did not eliminate friction. Tipping moments and ligation forces were equally significant in determining frictional forces. As well, there was considerable intra-operator variation in FN Ligation for SS ligatures.
Variations in clinical ligation forces are likely to be equal or greater than these experimental data and have potential to affect treatment efficiency during orthodontic sliding mechanics.
Cacciafesta V(2003)24 measured and compared the level of frictional resistance generated between stainless steel self-ligating brackets (Damon SL II, SDS Ormco, Glendora, Calif), polycarbonate self-ligating brackets (Oyster, Gestenco International, Gothenburg, Sweden)and conventional stainless steel brackets (Victory Series, 3M Unitek, Monrovia, Calif)and 3 different orthodontic wire alloys: stainless steel (Stainless Steel, SDS Ormco), nickel-titanium (Ni-Ti, SDS Ormco)and beta-titanium (TMA, SDS Ormco). The results of the study showed that stainless steel self-ligating brackets generated significantly lower static and kinetic frictional forces than both conventional stainless steel and polycarbonate self-ligating brackets, which showed no significant differences between them. Beta-titanium archwires had higher frictional resistances than stainless steel and nickel-titanium archwires. No significant differences were found between stainless steel and nickel-titanium archwires. All brackets showed higher static and kinetic frictional forces as the wire size increased.
used in combination with a self-ligating bracket (Damon II, Ormco, USA) and a conventional preadjusted edgewise premolar Stainless steel bracket (0.022 inch with 0° tip and torque) without any ligation. Four types of elastomeric module (purple, grey, Alastik or SuperSlick) and a preformed 0.09 inch stainless steel ligature were then assessed as methods of ligation using the same maxillary preadjusted edgewise premolar brackets.Results showed that Damon II self-ligating bracket and unligated conventional stainless steel bracket produced negligible mean frictional forces with any of the wires tested. Stainless steel ligatures produced the lowest mean frictional forces for all wires except 0.017 X 0.025 inch TMA. With the 0.017 X 0.025 inch TMA wire, purple modules produced the lowest mean frictional force. From the results, it may be concluded that there was no consistent pattern in the mean frictional forces across various combinations of wire type, size and ligation method. Under the conditions of this experiment, the use of passive self-ligating brackets is the only current method of almost eliminating friction.
static friction by 23–34% with respect to the small and medium non-lubricated elastomeric ligatures and by 36–43% compared with non-lubricated large ligatures.
Khambay B, Millett D and McHugh(2005)27evaluated the mean tensile force of four different elastomeric modules, the archwire seating force of different ligation methods, and its effect on frictional resistance. Statistically significant differences existed in the mean tensile forces and median archwire seating forces between the elastomeric modules. Grey modules with either size wire produced the lowest median archwire seating force, whereas SS ligatures produced the highest forces. SS ligatures with either wire produced the lowest mean frictional forces, whereas grey modules produced significantly higher mean frictional force (P < 0.01). The force with which the wire was seated into the bracket did not seem to be related to the subsequent amount of mean frictional force produced.
brackets demonstrated greater resistance to sliding than stainless steel brackets. Lubrication reduced the friction with .018-in wires and increased it for0 .019 X0 .025-in wires.
Baccetti T and FranchiL(2006)15 evaluated the frictional forces generated by new nonconventional passive elastomeric ligatures (NCL) and conventional elastomeric ligatures (CL) were compared under dry conditions. The amount of both static and kinetic frictions were minimal (<10 g) in the NCL group in the presence of aligned brackets with both types of wires, whereas it ranged from a minimum for the 0.014-inch superelastic nickel titanium wire to a maximum for the 0.019 x 0.025–inch stainless steel wire when using CL. The amounts of both static and kinetic frictions in the presence of a misaligned canine bracket in the NCL group were less than half of that shown by the CL group. A recently developed passive ligature system is able to produce significantly lower levels of frictional forces in vitro when compared with conventional elastomeric modules.
Franchi L, Baccetti T , Camporesi M and Lupoli M (2006)29evaluated the changes in the transverse dimension and the perimeter of the maxillary arch
produced by a low-friction system during the leveling and aligning phases of fixed
appliance therapy.The low-friction protocol consisted of a combination of
preadjusted brackets, superelastic nickel-titanium archwires, and nonconventional
elastomeric ligatures. Results showed that statistically significant increases were
recorded for all dentoalveolar widths and arch perimeter .The increase in arch
perimeter showed a significant negative relationship with the individual perimeter
depth. Hence they concluded that the low-friction system produced statistically
significant increases in the transverse dentoalveolar width and the perimeter of the
maxillary arch during the leveling and aligning phases of treatment with an
average duration of 6 months.
Hain M, Dhopatkar A and Rock P (2006) 30 examined the stability of the coating of an elastomeric module with a polymeric coating and also compared the frictional properties of coated modules with those of other common ligation methods. The six ligation methods tested were regular uncoated, slick coated, conventional silver, easy-to-tie, silicone-impregnated and standard silver modules which were used with standard stainless steel brackets and 0.019 X 0.025 inch archwires and resistance to movement was measured. Two self-ligating brackets Speed and Damon 2 were also tested. The results showed that the Damon 2 self-ligating brackets produced less friction than the other ligation methods, followed by the coated modules. There was no significant difference between the frictional resistance of brackets ligated with regular uncoated, silicone-impregnated and easy-to-tie modules. Speed self-ligating brackets produced less friction than regular uncoated, conventional silver and standard silver modules. Based on the results it may be concluded that Damon 2 brackets produces no recordable friction of ligation and coated modules produced 50% less friction than all other ligation methods except Damon 2. The coating was resistant to the simulated effects of oral environment but different methods of human saliva application were found to affect the frictional properties of the coating.
ligatures (CEL) during leveling and aligning phases. Results showed that
significant differences between CEL and NCEL were found for all tested variables
(P <0.01) with the exception of the 0.014- and 0.016-in wires at canine
misalignment of 1.5 mm. A noticeable amount of force was generated with the
NCEL at all 4 canine positions with all 3 wire sizes (from about 50 to about 150
g). With 4.5 mm of canine misalignment or more, the average amount of released
force with the CEL was approximately zero.
Tecco S, Di Iorio D, Cordasco G, Verrocchi I and Festa F (2007)32 evaluated the frictional resistance generated by conventional stainless steel (SS) brackets (Victory Series), self-ligating Damon SL II brackets, Time Plus brackets and low-friction ligatures (Slide) coupled with various SS, nickel-titanium (NiTi) and beta-titanium (TMA) archwires. The results of the study showed that when coupled with 0.016 inch NiTi, Victory brackets generated the most friction and Damon SL II the least (P < 0.001); with 0.016 X 0.022 inch NiTi, the self-ligating brackets (Time and Damon SL II) generated significantly lower friction (P < 0.001) than Victory Series and Slide ligatures; with 0.019 X 0.025 inch SS or 0.019 X 0.025 inch NiTi, Slide ligatures generated significantly lower friction than all other groups. No difference was observed among the four groups when used with a 0.017 X 0.025 inch TMA archwire.
(Synergy, Rocky Mountain Orthodontics, Denver, Colo) were used. The results concluded that no significant bracket differences were found when binding occurred in second order distances. In an ideal arch alignment, brackets with greater slot lumen have lower frictional resistance. Slot depth, bracket width and labial cover of the brackets with the same archwire influenced first-order rotational control. When a sliding mechanism was used with a third-order inclination change, the brackets with smaller third-order critical contact angles had greater frictional resistance.
Camporesi M, Baccetti T and FranchiL(2007)34 compared the forces generated by 2 types of esthetic brackets Aqua [Leone Orthodontic Products, Sesto Fiorentino, Florence, Italy] and Mystique [GAC International, Bohemia, NY] in association with low-friction ligature systems Slide [Leone Orthodontic Products] and Neo-Clips [GAC International], respectively and the same brackets combined with conventional elastomeric ligatures (CEL) during the leveling and aligning phases. The results of the study concluded that significantly greater amount of force was released with low-friction systems when compared with CEL systems for all the tested variables, with the exception of the 1.5-mm canine misalignment and the 6.0-mm canine misalignment limited to Mystique with Neo-Clips. Similar forces were released with both esthetic low-friction systems. The average amount of released force with CEL was approximately zero at 3.0 mm or more of canine misalignment.
teeth.It was seen that although the amount of horizontal retraction of the maxillary anterior teeth was not different between the two groups, there was mild labial movement of the root apices of the upper incisors in group 2 at T2. There were no significant differences in the degree of anchorage loss of the maxillary posterior teeth between the two groups. Bodily and mesial movements of the upper molars occurred in both groups. Approximately 4 mm of the retraction of the upper incisal edges resulted from 1 mm of anchorage loss in the upper molars in both groups. It was concluded that no significant differences existed in the degree of anchorage loss of the upper posterior teeth and the amount of retraction of the upper anterior teeth associated with en masse retraction and two-step retraction of the anterior teeth.
Franchi L, Baccetti T, Camporesi M and Barbato E (2008)36evaluated the frictional forces generated by 4 types of passive stainless steel self-ligating brackets (SLBs) and by nonconventional elastomeric ligatures (NCEL) and conventional elastomeric ligatures (CEL) during sliding mechanics.Results showed that significantly smaller static and kinetic forces were generated by the SLBs and NCEL (<2 g) compared with the CEL (>500 g). No significant differences were found within the different types of SLBs, or between these and the NCEL. Hence it was concluded thatSLBs and NCEL are valid alternatives for low friction during sliding mechanics.
phases of orthodontic therapy. Results showedsignificant differences were found between UEL and CEL systems for all tested variables (P < .01) with the exception of the canine misalignment of 1.5 mm. The average amount of recorded force in the presence of CEL was negligible with 3.0 mm or greater of canine misalignment. On the contrary, during alignment, a force available for tooth movement was recorded in the presence of both ceramic and stainless steel brackets when associated with UEL. Hence the type of ligature used influenced the actual amount of force released by the orthodontic system significantly more than the type of brackets used (stainless steel vs ceramic).
Baccetti T, Franchi L and Fortini A(2008)38evaluated the features of
low-friction ligatures during the leveling and aligning phase of fixed appliance
therapy with preadjustedbrackets. The materials used for the study were
conventional elastomeric ligatures on special versatile brackets (Synergy, Rocky
Mountain Orthodontics, Denver, CO, USA), by using lubricated elastomeric
modules, or with loosely tied stainless steel ligatures. Innovative ligatures
manufactured with a special polyurethane mix by injection molding (Slide, Leone
S.p.A., Firenze, Italy) had been then introduced. The “nonconventional”
elastomeric ligature was used on conventional brackets to produce low levels of
frictional resistance in treatment mechanics with the preadjusted appliance. The
results of the experimental testing showed that a combination of the low-friction
ligatures with the super elastic nickel-titanium wires produced a significantly
smaller amount of binding at the bracket/archwire/ligature unit when compared to
Bortoly TG, Guerrero AP, Rached RN, and Rosa EAR(2008)39 evaluated the properties related to sliding resistance of esthetic ligatures. Frictional force of 6 ligatures- 2 conventional, 2 specially coated elastomeric, Teflon-coated (Dupont, Wilmington, Del) stainless steel and stainless steel (control) ligatures were studied by sliding 0.019 x 0.025 inch stainless steel wire through the 0.22 inch slot of stainless steel bracket. The results of the study showed high correlation between frictional and tensile forces of elastomeric ligatures, with reduction of both after 21 days. The demineralizing/remineralizing regimen reduced the frictional forces of ligatures to the same level as the ligatures in artificial saliva. Teflon-coated and stainless steel ligatures showed the lowest initial frictional forces, but there was no difference in friction of stainless steel and post stretched elastomeric ligatures. Based on the results of the study it was concluded that frictional forces generated by esthetic elastomeric ligatures under simulated oral environments are not stable and are more related to tensile force than to surface characteristics of the ligatures
Tecco S, Tete S and FestaF(2009)41 evaluated the frictional resistance when round or rectangular archwires were used in conjunction with low-friction ligatures or conventional ligatures. Results showed that low-friction Slide ligatures with round archwires showed statistically significantly lower frictional resistance than conventional ligatures. When coupled with 0.016 x 0.022 inch nickel titanium and stainless steel, no statistically significant difference was observed among the four groups. But when coupled with 0.017 X 0.025 inch archwires, low-friction ligatures showed statistically significantly greater frictional resistance than conventional ligatures. When coupled with 0.019 X 0.025 inch nickel titanium, low-friction ligatures showed statistically significantly greater frictional resistance than conventional ligatures, but no difference among the four groups was observed with the 0.019 X 0.025 inch stainless steel. No significant difference was assessed among low-friction ligatures of different sizes. From the above results, it was concluded that low friction Slide ligatures showed lower friction compared to conventional ligatures when coupled with round archwires, but not when coupled with rectangular wires.
nonconventional elastomeric ligature bracket systems produced levels of force for tooth movement that were similar to those generated by passive self-ligating brackets.
Jones SP and BihiSB(2009)43 compared the static frictional resistance of a low-friction ligation system against a conventional elastomeric module, and studied the effect of storage in a simulated oral environment on the static frictional resistance of both ligation systems.The results of this investigation demonstrated that the Slide ligatures produced significantly lower static frictional resistance than conventional elastomeric modules in the fresh condition and after 24 hours of storage in a simulated oral environment (p < 0.001). Storage for 24 hours in artificial saliva had no effect on the static frictional resistance of conventional elastomeric modules and the Slide system (p = 0.525).The claim by the manufacturer that the Slide system produces lower frictional resistance than conventional elastomeric modules is upheld.
led to an increase in friction in all bracket-archwire combinations excluding DMX and VSS, which showed no measurable friction at either wire size.
Ravi K, Balasubramaniam MR ,George M and Duraisamy S(2010)45 evaluated the efficiency of SLIDE ligature module during segmental canine retraction by comparison of various parameters like rate of retraction, amount of tipping of canine and molar , amount of rotation in the canine and molar and change in the first molar position. The slide ligatures were randomly allotted to one side of arch (Group1) and the other arch was allotted to control group using conventional ligatures. A force level of 150 gms was used in both quadrants. Patients were recalled every one month to maintain the force of retraction and the replacement of the modules. Canine retraction was assessed intraorally using a vernier caliper. Each measurement was done twice and the mean of two values recorded to give the actual amount of retraction. The rate of retraction was calculated as the amount of canine retraction in mm divided by each time interval. The amount of canine rotation, molar rotation, molar position after retraction, tipping in canine and molar was also determined. It was concluded that slide ligatures can be a suitable alternative to conventional module because of their low friction property, which allows for faster rate of canine retraction.
of apical misalignment a significantly greater amount of orthodontic force was released by SLB or SLCB when compared with CLCB, while no significant differences were found among the three systems at 3 mm of buccal canine displacement. Hence it was suggested that when correction of a large amount of misalignment (6 mm) was attempted, a noticeable amount of force for alignment was still generated by the passive SLB and SLCB systems while no force was released in presence of CLCB.
Dholakia K K and Bhat S(2012)47 compared and evaluate the clinical efficiency of conventional elastomeric ligatures and non-conventional elastomeric ligatures during canine retraction. 20 orthodontic patients (12 females, 8 males) with a mean age of 18.3 years who had undergone therapeutic extraction of all first premolars were taken as the samples. It was observed that the mean rates of canine retraction was 1.7±0.6 mm per month in maxilla and 1.8±0.9mm per month in mandible using slide ligatures when compared to 1.6±0.5 mm per month in maxilla and 1.5±0.5 mm per month for mandible using conventional elastomeric ligatures. The authors concluded that there was no significant difference in rate of retraction in maxillary arch between conventional ligatures and slide ligatures. No significant clinical advantage was observed with non conventional ligatures over conventional ligatures with respect to time required for the complete retraction and prevention of canine tipping or rotations
investigated using stainless steel,nickel–titanium and titanium–molybdenum alloy archwires of several sizes. The results showed that the static and kinetic frictional forces were lower in passive type SLBs (P < 0.05), except in the Smart Clip bracket. The wire materials or wire dimensions in the study showed similar frictional forces with no statistical differences. The wearing effects were not found in bracket slots under SEM observation. Only conventional brackets and mini-Clippy SLB revealed nickel ions via EDS analysis. This study showed that passive SLBs are associated with lower static or kinetic friction forces than those of active SLBs or conventional brackets, but the wear on the bracket slots was not observed in this study.
Sfondrini MF, Fraticelli D, Rosti F, Scribante A and Gandini P(2012)48 evaluated the frictional forces generated by five different orthodontic brackets when used in combination with stainless steel and NiTi archwires in dry conditions at physiological temperature. Frictional forces were measured by Instron Universal Testing Machine. Damon 3MX and Step brackets with Slide ligatures produced statistically lower friction than Quick and conventional brackets with elastomeric ligature. Frictional force increased proportionally to the wiresize; NiTi archwires presented higher frictional resistance than stainless steel archwires. Slide ligatures showed lower fictional values in comparison with elastic ligatures. Stainless steel brackets with new Slide ligature showed frictional forces similar to self-ligating brackets with passive clip.
regarding resistance to sliding. The physical or mechanical variables that influence friction formation during orthodontic treatment are more frequently researched than the biological variables. They should be carefully taken into consideration during the different stages of the orthodontic treatment to increase efficiency in different clinical situations. The technological innovations used to develop new low-friction materials such as the design alterations and the surface treatments seem to present good potential to reduce friction in specific clinical situations.
Queiroz GV, Neto JR, De Paiva JB, Rossi JL and Ballester R(2012)50 describe and compare three alternative methods for controlling classical friction with Self-ligating brackets (SLB), special brackets(SB) and special elastomeric ligatures (SEB). The study compared Damon MX,Smart Clip, In-Ovation and Easy Clip self-ligating bracket systems, the special Synergy brackets and
Morelli’s twin bracket with special 8-shaped elastomeric ligatures. The results concluded that Damon MX, Easy Clip, Smart Clip, Synergy bracket systems and 8-shaped ligatures proved to be equally effective alternatives for controlling classical friction using 0.014 inch nickel-titanium archwires and 0.019 X 0.025 inch steel archwires, while the In-Ovation was efficient with 0.014 inch archwires but with 0.019 X 0.025inch archwires it exhibited friction that was similar to conventional brackets with used elastomeric ligatures..
for the study were slick and slide modules that were compared with regular modules, modules tied in figure of eight fashion, tight stainless steel ligatures and loose stainless steel ligatures. The results of the study showed that Slide modules produce least friction followed by loose stainless steel ligation, slick modules, regular modules, tight stainless steel ligation and highest friction was produced by
regular modules tied in a ‘figure of 8’ pattern. It was also seen that width of the
bracket had no influence on friction produced.
Bayri R, Yilmaz HN, Koc E and KucukkelesN(2013)52 evaluated the frictional values of 3 different ligation methods with different bracket types using a crowded configuration. Three aesthetic conventional brackets (monocrystalline ceramic,polycrystalline ceramic, microfilled copolymer) and 1 metal bracket were evaluated in terms of friction. The results of the study showed that nonconventional elastomeric ligature produced the lowest friction. It also revealed that bracket material and ligation type affect frictional resistance. Monocrystalline ceramic brackets showed the highest frictional resistance. Polycrystalline ceramic brackets showed higher frictional resistance than metal brackets except when ligated with nonconventional elastomeric ligatures. Microfilled copolymer brackets presented significantly lower frictional values compared with other conventional brackets with all ligation methods. Nonconventional elastomeric ligation showed the lowest friction values followed by elastomeric modules and metal ligatures.
Condò R, Casaglia A, Armellin E, Condò SG and
ligatures (Leone® S.p.A.), ring-shape, grey,polyurethane ligatures (Micerium® S.p.A.) and grey, polyurethane, Slide low-friction ligatures (Leone® S.p.A.). Transparent O-ring ligatures showed significant volumetric and structural changes. The external rounded shape was rather maintained, while the internal shape tended to appear square. Both external and internal diameter significantly increased (p<0.005 and p<0.0001 respectively) while the thickness decreased ( p<0.005) when analyzed with t-test. Polyurethane ring-shape ligatures retained the initial ring design. Both external and internal diameter increased (p<0.0001),while the thickness remained almost unchanged. The internal border was more squared, and showed jagged edges with continuous and irregular extroversions. Grey, polyurethane Slide low-friction ligatures showed a reduced dimensional change. There was a slight increase in two dimensions, length and width, (14-16%) (p<0.05 and p<0.001) while there was not significant decrease in thickness (10%). From SEM analysis of ligature morphology it emerges that latex and polyurethane O-ring ligatures endure significant volumetric and structural changes, after clinical use, index of a greater degree of friction and early loss in functionality.Grey, polyurethane Slide low-friction ligatures presented limited variation in size after clinical use
results of the study showed that conventional ligation produced the greatest friction regardless of wire or bracket combination used. The self-ligating system exhibited less friction than low-friction ligation with smaller round wires and with higher dimension archwires it exhibited greater friction. The study concluded that slide low-friction ligatures produced reduced friction with both metallic and ceramic brackets in comparison with self-ligating brackets.
Reddy VB., Kumar TA, Prasad M, Nuvvula S, Patil RG and Reddy
MATERIALS AND METHODS
MATERIALS
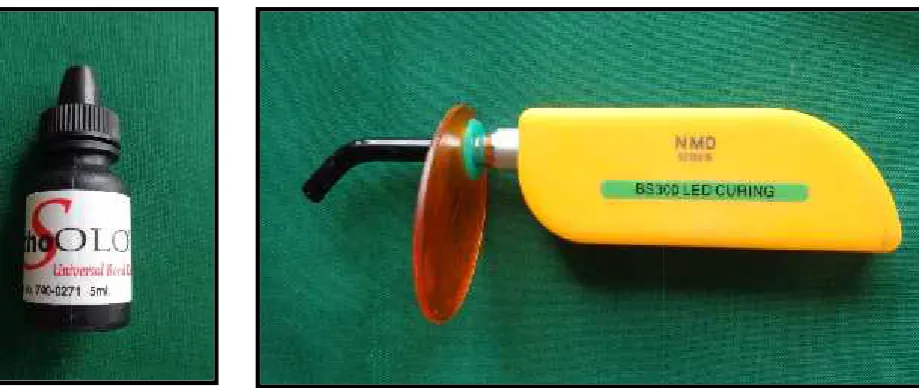
1. Discover gel etchant (Libral Traders, Mumbai, India) 2. Primer (Orthosolo,Ormco Corporation, Italy)
3. Othodontic adhesive (3M , monrovia, USA) 4. Light curing unit (Dentmark,india)
5. Preformed bands (Captain Ortho, Libral Traders, Mumbai, India)
6. Upper double and lower double buccal tubes (0.022-in, MBT prescription slot)
7. Pre-adjusted edgewise bracket kit (MBT prescription, slot size 0.022 X 0.028 in)
8. 0.017 X 0.025-in stainless steel archwires (G&HFranklin, IN, USA)
9. Non-conventional ligature modules -Super Slick ligatures (TP Orthodontics, LaPorte, Ind), & Slide ligatures (Leone, Sesto Fiorentino,) 10. Conventional ligature modules- 3M(Monrovia,CAUSA)
11. Niti Closed Coil Springs With Eyelets(Ormco Corporation, Orange, Calif)) 12. A tension Gauge (Dontrix, TP orthodontics,Ind)
13. A digital vernier caliper (Digimaticcaliper; mitutoyo, kawasaki, japan) of 0.01-mm sensitivity,
STUDY PARTICIPANTS SELECTION
Amongst out patients attending the Department of Department of orthodontics and dentofacial orthopedics, Tamilnadu Government Dental College & Hospital(Chennai, India) 30 patients with Angle’s Class I malocclusion with
of all four first premolars, requiring maximum anchorage of posterior teeth were selected for the study. Informed consent was obtained from all patients, according to the recommendations of The Institutional Ethics Committee of Tamilnadu Government Dental College & Hospital, Chennai, India.
CRITERIA FOR SELECTION INCLUSION CRITERIA
1. Healthy individuals and not under any routine medication 2. Age group: 14–24 years
3. Class I molar relationship (± 1mm) and overjet not exceeding 5mm 4. Bidental protrusion requiring extraction of all first Premolars
5. Well aligned maxillary and mandibular incisors with minimum crowding (<3.5 mm)
6. Completely established permanent Dentitions (except 3rd. molar) 7. All teeth anatomically normal and vital
EXCLUSION CRITERIA
1. Previous history of mouth breathing, thumb sucking, tongue thrusting or orthodontic treatment
Split mouth study was done with one of side of the arch, where the canine was ligated with non-conventional ligature mode was considered as the experimental side while the other side of the arch, where the canine was ligated with conventional mode served as control side. The assignment of experimental and control quadrants were done randomly. The 30 subjects with 120 quadrants were divided randomly into 3 groups, namely A , B and C.
Group A (15 patients selected randomly) received nonconventional elastomeric ligatures- Slide ligatures (Leone, Sesto Fiorentino),{figures 7,8} on canine brackets on one side and conventional ligature mode on the other side (3M modules). Therefore, 15 quadrants in the maxillary arch and 15 quadrants in mandibular arch were experimental sides while the 30 contralateral quadrant served as control sides.
Group B (15 patients selected randomly) received nonconventional elastomeric ligatures (super slick ligatures TP orthodonticsTM){ figure 9} on canine brackets on one side and conventional ligature mode on the other side (3M modules). Therefore, 15 quadrants in the maxillary arch and 15 quadrants in mandibular arch were experimental sides while the 30 contralateral quadrant served as control sides .
METHODOLOGY
Extraction of all first premolars was performed. Brackets with 0.022’ slots
with the MBT prescription were bonded. Initial alignment and levelling of both arches were done by using 0.016-in nickel-titanium and 0.016×0.022-in nickel titanium archwires. The nickel-titanium wires were replaced by 0.017×0.025-in stainless steel archwires, and arch levelling continued. Once alignment and levelling of the arches were achieved, maxillary and mandibular study models were made and the distances between the central pit of the first molar and the canine tip were measured with the digital vernier calliper and were considered as the baseline value to evaluate the amount of canine retraction in subsequent intervals.
The canines were ligated to the arch wires with nonconventional elastomeric ligature - Slide Slide ligatures (Leone, Sesto Fiorentino)and Super Slick ligatures (TP Orthodontics, LaPorte, Ind)in group A and B respectively. In a perfect instance of individual canine retraction, just the canine bracket slides over the archwire. Therefore, all teeth other than the canines in group A and group B were ligated with conventional elastomeric ligatures.
DATA COLLECTION Study model were done at:
T0- (base line)–before retraction of canines
T1 – T5: At the end of every month for 5months or until completion of canine retraction whichever is earlier.
The data collected from the study models were: 1. Rate of canine retraction
2. Anchor loss
3. Amount of canine rotation 4. Amount of Molar rotation
DETERMINING RATE OF CANINE RETRACTION
From the study models, to measure rate of canine retraction, an oval acrylic button with wire jigs were made for each maxillary and mandibular arch. The acrylic button was made in palatal rugae region, in maxillary arch, as rugal area does not change with orthodontic treatment. In the mandibular arch, an oval acrylic button was made on the lingual side. Four wires made of dimension 21x 22 inch SS were embedded in in the acrylic button. The outer ends of the anterior wires, called “Anterior Wire Tip”(AWT) made to touch the canine tips while the in the posterior wire, called “Posterior Wire Tip”(PWT), the outer ends measured
model was used to make the plug, which was then fitted to the successive models taken at monthly interval. The perpendicular distance between the canine tip and the PWT of the same side wasmeasured using a digital vernier calliper and was considered to be the amount ofdistal movement of the canine . Again, measurements made with a calliper were repeated after 7 days. Readings at the end of each interval were subtracted from the readings of the previous interval or the base reading to obtain the amount of canine retraction in that interval. The rate of canine retraction was calculated as the amount of extraction space closed divided by the time (number of intervals) required for complete space closure. This was recorded in millimetres per month .The measurements to 0.05 mm were recorded by the same operator. The landmarks used in measuring the teeth were consistent for both the rate and the anchorage loss.
DETERMINING ANCHORAGE LOSS
calliper and was considered as the amount of mesial movement of the molars. Again, measurements made with a caliper were repeated after 7 days
DETERMINING CANINE ROTATION
All study measurements were performed on the dental casts. Before taking the measurements, the median raphe on maxilla and midline pointer (MLP) in mandible( wire extending from the acrylic plug in the midline between the incisors) and the canine mesial and distal edges were marked with a pencil on the model( figure 20). The rotation of upper canines was calculated by the angle formed between the median palatine suture (maxilla)or midline pointer (mandible ) and a line passing through the mesial and distal contact points of the canines57. Total rotation was considered to be the difference between the values of T0 and T5. The angle(x) between midline perpendiculars and the line through the mesial and distal edges of the canine was measured with a protractor (figure 18) and reiterated after 7 days to check reproducibility and thus the rotation of the canine was recorded59.
DETERMINING MOLAR ROTATION
COLOR PLATES
Figure 1: Discover gel etchant Figure 3: Orthodontic adhesive-3M, USA
Figure 4: Light curing unit Figure 2: Primer
[image:49.595.98.558.371.565.2]COLOR PLATES
Figure 1: Discover gel etchant Figure 3: Orthodontic adhesive-3M, USA
Figure 4: Light curing unit Figure 2: Primer
COLOR PLATES
Figure 1: Discover gel etchant Figure 3: Orthodontic adhesive-3M, USA
Figure 7: Slide ligatures (Leone, Sesto Fiorentino,)
[image:50.595.55.570.101.262.2]Figure 8: Slide ligatures (Leone, Sesto Fiorentino,)
Figure 6: Preformed bands with Upper double and lower double
buccal tubes Figure 5: Pre-adjusted edgewise bracket kit
[image:50.595.65.575.354.551.2][image:51.595.86.561.98.273.2]
-Figure 9: Super Slick ligatures (TP Orthodontics, LaPorte, Ind)
Figure 10: Conventional ligature modules- 3M(Monrovia,CA USA)
-Figure 9: Super Slick ligatures (TP Orthodontics, LaPorte, Ind)
Figure 10: Conventional ligature modules- 3M(Monrovia,CA USA)
-Figure 9: Super Slick ligatures (TP Orthodontics, LaPorte, Ind)
[image:51.595.182.450.356.571.2]Figure 11:0.017 X 0.025-in stainless steel archwires
[image:52.595.341.560.94.273.2]Figure 12: Niti Closed Coil Springs With Eyelets
Figure 13: Digital vernier caliper Figure 14: Tension Gauge (Dontrix, TP orthodontics
Figure 11:0.017 X 0.025-in stainless steel archwires
[image:52.595.76.317.382.567.2]Figure 12: Niti Closed Coil Springs With Eyelets
Figure 13: Digital vernier caliper Figure 14: Tension Gauge (Dontrix, TP orthodontics
Figure 11:0.017 X 0.025-in stainless steel archwires
Figure 12: Niti Closed Coil Springs With Eyelets
Figure 15: Model with grid
AWT
[image:53.595.113.268.81.243.2]PWT
[image:53.595.112.300.314.471.2]Figure 16: Model analysis
Figure 17: molar rotation measurement
Figure 18: canine rotation measurements
Figure 19: Maxillary acrylic plug Figure 20: Mandibular acrylic plug
[image:53.595.389.578.315.472.2]y x PWT PWT PWT AWT AWT AWT MLP Figure 15: Model with grid
AWT
[image:53.595.384.570.543.699.2]PWT
Figure 16: Model analysis
Figure 17: molar rotation measurement
Figure 18: canine rotation measurements
Figure 19: Maxillary acrylic plug Figure 20: Mandibular acrylic plug
[image:53.595.115.308.545.701.2]y x PWT PWT PWT AWT AWT AWT MLP Figure 15: Model with grid
AWT
PWT
Figure 16: Model analysis
Figure 17: molar rotation measurement
Figure 18: canine rotation measurements
Figure 19: Maxillary acrylic plug Figure 20: Mandibular acrylic plug
Pre-treatment pictures of GROUP A
Figure 23: maxillary occlusal view Figure 24: mandibular occlusalview Figure 21: Right lateral view- group C Figure 21: Left lateral view- group A
Pre-treatment pictures of GROUP A
Figure 23: maxillary occlusal view Figure 24: mandibular occlusalview Figure 21: Right lateral view- group C Figure 21: Left lateral view- group A
Pre-treatment pictures of GROUP A
[image:54.595.67.564.137.295.2] [image:54.595.95.567.369.567.2]Pre-treatment pictures of GROUP B
[image:55.595.72.577.131.329.2]Figure 26: left lateralview( group c) Figure 25: right lateralview( group B)
Figure 27: maxillary occlusal view Figure 28: mandibular occlusal view
Pre-treatment pictures of GROUP B
Figure 26: left lateralview( group c) Figure 25: right lateralview( group B)
Figure 27: maxillary occlusal view Figure 28: mandibular occlusal view
Pre-treatment pictures of GROUP B
Figure 26: left lateralview( group c) Figure 25: right lateralview( group B)
[image:55.595.83.577.412.623.2]Post-treatment pictures of GROUP A
Figure 32: mandibular occlusal view Figure 31: maxillary occlusal view
Figure 30 :right lateral view
(group A)
Figure 29:right lateral view(group C)
[image:56.595.75.577.411.626.2]Post-treatment pictures of GROUP A
Figure 32: mandibular occlusal view Figure 31: maxillary occlusal view
Figure 30 :right lateral view
(group A)
Figure 29:right lateral view(group C)
Post-treatment pictures of GROUP A
Figure 32: mandibular occlusal view Figure 31: maxillary occlusal view
Figure 30 :right lateral view
(group A)
Post-treatment pictures of GROUP B
Figure 33: right lateral view( group B) Figure 34: left lateral view( group C)
[image:57.595.332.570.387.569.2] [image:57.595.95.313.388.573.2]RESULTS
The study included 30 Class I bialveolar protrusion patients between the age group of 14-24 years in the permanent dentition who visited the Department of Orthodontics, Tamilnadu govt dental college and hospital. The sample was randomly divided into three groups : the study groups-{slide ligature group (A) ,super slick ligatures (B)} and the control group (C-conventional).
Study models were recorded were taken at the end of alignment (T0) and continued at the end of every month for 5months or until completion of canine retraction whichever is earlier. Rate of canine retraction, Anchor loss, Amount of canine and molar rotation in each quadrant were estimated from the study models. The data obtained from this study was evaluated and comparisons were made within the group and between the study group and the control group.
Means, standard deviations, and level of significance were determined. One way ANOVA was to compare difference between 3 groups. Student t test was done to find the significance of study parameters within 2group. P value < 0.01 indicated strong significance. P value between 0.01 and 0.05 (0.01<P<0.05) indicated moderate significance. For intergroup comparison test was done with level of significance at P = 0.05.
[* Moderately significant ( P value:0.01<P0.05) ** Strongly significant (P value : P0.01)]
CANINE RETRACTION RATE
In maxilla the mean rate of canine retraction on Group A , group B and group C was 1.674+0.092, 1.187+0.156 and 1.147+0.113respectively .[The difference in the rate of retraction was statistically significant , ie, p<0.0001[table4]
In mandible the mean rate of canine retraction on Group A , group B and group C was 1.765+0.099,,1.300+0.099 and 1.270+0.111 respectively . The difference in the rate of retraction was statistically significant,ie,p<0.0001[table2]. t value of each group is given in table 1, 2 and 3.Graph 1 and graph shows the mean canine retraction rates in each einterval
ANCHORAGE LOSS
In maxilla the group A had a mean anchorage loss of 1.054mm with a standard deviation of +0.174while group B had a mean anchorage loss of 1.080mm with a standard deviation of +0.188. The group C had a mean anchorage loss of 1.715mm +0.163.The difference in the mesial movement of the maxillary molar was statistically significantie ,p<0.0001[table 4]
CANINE ROTATION
Group A had a mean canine rotation of 8.550+1.506 in maxilla and 8.930+1.474 in mandible. Mean canine rotation for group B was 5.300+1.386 in maxilla and 5.830+1.096 in mandible. Group C had a mean canine rotation of 6.100+1.315in maxilla and 6.880+1.813in mandible. The difference in the amount of rotation was statistically significant ie,p<0.0001[table 4 and 5]
MOLAR ROTATION
TABLES
Student t test-Group A
Group Group A T p
CRR Maxilla 1.674+0.092
2.607 0.014
CRR Mandible 1.765+0.099
Canine Rotation Maxilla
8.550+1.506
0.711 0.482
Canine Rotation Mandible
8.933+1.474
Molar RotationMaxilla
2.583+0.735
1.345 0.189
Molar RotationMandible
2.900+0.541
Anchorage loss Maxilla
1.054+0.174
0.560 0.579
Anchorage loss Mandible
1.024+0.113
CRR- canine retraction rate
Student t test- group B
group Group B T p
CRR Maxilla 1.187+0.156
2.368 0.025
CRR Mandible 1.300+0.099
Canine Rotation Maxilla
5.300+1.386
1.168 0.252
Canine Rotation Mandible
5.833+1.096
Molar RotationMaxilla
2.216+0.549
1.995 0.055
Molar RotationMandible
2.650+0.639
Anchorage loss Maxilla
1.080+0.188
2.412 0.022
Anchorage loss Mandible
0.952+0.083
Student t test- group C
group Group C T P
CRR Maxilla 1.147+0.113
3.007 0.005
CRR Mandible
1.270+0.111
Canine Rotation Maxilla
6.100+1.315
1.354 0.186
Canine Rotation Mandible
6.883+1.813
Molar RotationMaxilla
2.216+0.700
2.375 0.024
Molar RotationMandible
2.783+0.604
Anchorage loss Maxilla
1.715+0.163
1.001 0.325
Anchorage loss Mandible
1.664+0.111
[image:63.595.77.537.66.567.2]CRR- canine retraction rate
Oneway ANOVA- maxilla
Group Group A Group B Group C F P
CRR Baseline Maxilla T0
0 0 0 NA NA
CRR Maxilla T1 1.615+0.140 1.298+0.086 1.263+0.092 59.382 <0.001
CRR Maxilla T2 1.630+0.106 1.236+0.109 1.193++0.099 94.372 <0.001
CRR Maxilla T3 1.651+0.124 1.122+0.125 1.189+0.123 86.956 <0.001
CRR Maxilla T4 1.601+0.130 1.178+0.151 1.173+0.123 58.350 <0.001
CRR Maxilla T5 1.574+0.092 1.187+0.156 1.147+0.113 66.116 <0.001
Canine Rotation Maxilla
8.550+1.506 5.300+1.386 6.100+1.315 23.409 <0.001
Molar Rotation Maxilla
2.583+0.735 2.216+0.549 2.216+0.700 1.656 0.200
Anchorage loss Maxilla
[image:64.595.59.557.90.514.2]1.054+0.174 1.080+0.188 1.715+0.163 105.903 <0.001
Oneway ANOVA
Group Group A Group B Group C F P
CR Baseline Mandible T0
0 0 0 NA NA
CR MandibleT1 1.688+0.111 1.276+0.099 1.283+0.107 82.239 <0.001
CR MandibleT2 1.751+0.061 1.310+0.072 1.269+0.098 173.199 <0.001
CR MandibleT3 1.706+0.121 1.284+0.071 1.260+0.092 118.021 <0.001
CR MandibleT4 1.685+0.121 1.307+0.074 1.288+0.115 73.187 <0.001
CR MandibleT5 1.665+0.099 1.300+0.099 1.270+0.111 74.407 <0.001
Canine Rotation Mandible
8.933+1.474 5.833+1.096 6.883+1.813 15.153 <0.001
Molar RotationMandible
2.900+0.541 2.650+0.639 2.783+0.604 0.656 0.523
Anchorage loss Mandible
[image:65.595.60.554.73.510.2]1.024+0.113 0.952+0.083 1.664+0.111 306.573 <0.001
BASELI
NE T0 T1 T2 T3 T 4 T 5
CANINE RETRACTION
MANDIBLE GROUP A 0 1.688 1.751 1.706 1.685 1.665 CANINE RETRACTION
MANDIBLE GROUP B 0 1.276 1.31 1.284 1.307 1.3 CANINE RETRACTION
MANDIBLE CONTROL 0 1.283 1.269 1.26 1.288 1.27
0 0.2 0.4 0.6 0.81 1.2 1.4 1.6 1.82 Am ou nt o f c an in e re tr ac tio
n
MEAN CANINE RETRACTION
BETWEEN GROUPS
BASELI
NE T0 T1 T2 T3 T4 T5
CANINE RETRACTION