D
SUFAMILY
DETERM
Pr C.S. UBMITTE C.S.Y PLANN
MINANCE
AT M
DOCTUn
rof. Dr.K.I. Jeyaraj A
ED TO THE UNI
Mrs. N
I. Jeyaraj A
NING ME
E AMON
MADURAI
OR OF PH IN NURSI
nder the Gu
RAJALAKResearch Annapacki
Madu
A THE E TAMIL N IVERSITY By N. JESSIE Profes Annapacki Madu
201
ETHODS
NG ELIGI
I DISTRI
HILOSOP N INGuidance of
KSHMI,P Guide iam College urai ESIS NADU DR. Y, CHENNA y E METILD ssor iam College urai2
S AND TH
IBLE CO
ICT
PHY
f
Ph.D.(N).,
e of Nursin
. M.G.R M AI
DA
e of Nursin
HEIR
OUPLES
ng
MEDICAL
AN APPROACH TO ASSESS THE PRACTICE ON PERMANENT
FAMILY PLANNING METHODS AND THEIR DETERMINANCE
AMONG ELIGIBLE COUPLES AT MADURAI DISTRICT
NURSING GUIDE : __________________________________ Prof.Dr.K.Rajalakshmi.M.Sc.,Ph.D.(N).
Guide and Supervisor.
NURSING CO-GUIDE : ________________________________ Prof.K.Helen Rani.R.N.,R.M.,M.Sc.(N).
Co-Guide and Supervisor.
MEDICAL CO-GUIDE : ___________________________ Prof.Dr.V.Radharani.M.B.B.S. Joint Director of Health and Family Welfare Medical Co-Guide and Supervisor.
THESIS SUBMITTED TO THE TAMIL NADU DR.M.G.R.MEDICAL UNIVERSITY,CHENNAI FOR THE DEGREE OF DOCTOR OF PHILOSOPHY
C E R T I F I CA T E
Prof.Dr.K.Rajalakshmi certify that the thesis entitled “An approach to assess the practice on permanent family planning methods and their determinance among eligible couples at Madurai District” submitted for the award of the Degree of Doctor of Philosophy in Nursing by Mrs. N. Jessie Metilda is the record of research work carried out by her during the period from 2008 to 2012 under my guidance and supervision and that this work has not formed the basis for the award of any Degree, Diploma, Associateship, fellowship or other similar title in this university or any other university or institution of higher learning.
C E R T I F I CA T E
This is to certify that the work embodied in the thesis entitled “An approach to assess the practice on permanent family planning methods and their determinance among eligible couples at Madurai District” submitted by Mrs. N. Jessie Metilda for the award of the Degree of Doctor of Philosophy in Nursing is a bonafide record of research done by her during the period of study under my supervision and guidance, and that it has not formed the basis for the award of any Degree, Diploma, Associateship, fellowship or other similar title.
Prof.K. Helen Rani. R.N.,R.M.,M.Sc.(N). Co-guide and Supervisor.
C E R T I F I CA T E
This is to certify that the work embodied in the thesis entitled “An approach to assess the practice on permanent family planning methods and their determinance among eligible couples at Madurai District” submitted by Mrs. N. Jessie Metilda for the award of the Degree of Doctor of Philosophy in Nursing is a bonafide record of research done by her during the period of study under my supervision and guidance, and that it has not formed the basis for the award of any Degree, Diploma, Associateship, fellowship or other similar title.
Prof.Dr.V.Radharani.M.B.B.S. Joint Director of health and family welfare Medical Co-Guide and Supervisor.
DECLARATION
I hereby declare that the thesis entitled “An approach to assess the practice on permanent family planning methods and their determinance among eligible couples at Madurai District” is original research work carried out by me and it was not used previously partly or fully for the award of any degree, diploma, associateship, fellowship or any other similar title.
Signature of candidate
N.Jessie Metilda.M.Sc.(N).
Professor
“I can do all things through Christ Who strengthens me and I will
exalt Him at all times, His praise is always on my lips” Success is the fruit of
hard work. This success was possible due to the collective efforts of so many
eminent personalities to whom I express my gratitude.
At the outset, I am immensely grateful to Prof.Dr.C.Jothi Sophia.Ph.D.(N).,
esteemed Principal, C.S.I.Jeyaraj Annapackiam College of Nursing, Madurai, all the
members of the Management and Prof.Merlin.M.Sc(N)., Vice Principal of C.S.I.
Jeyaraj Annapackiam College of Nursing, Madurai for giving me an opportunity to
undertake the Ph.D programme under the Tamil Nadu Dr.M.G.R.Medical University,
Chennai. I profusely thank them for their good wishes and support for the
successful completion of the study.
I extend my deep sense of gratitude to Dr. Charles.M.S.,M.ch., Medical
Director, Christian mission hospital and Dr.Gabriel.M.Sc.,M.Ed.,Ph.D., Director,
CSI School of education, for their valuable suggestions and constant guidance in
carrying out this study.
I also extend my deep sense of gratitude, respect and regard to my research
guide Prof.Dr.K.Rajalakshmi,Ph.D.(N)., for her constant guidance, highly
beneficial suggestion, precious advice, as well as providing all possible facilities for
successfully carrying out this study, in spite of her busy schedule of work. I consider
it as a great honour and privilege to complete the study under her supervision,
without which the study would not be successful.
I express my deep sense of gratitude and respect to my research Co-guide,
out this study.
I convey my sincere thanks and gratitude to Prof.Dr.V.Radharani,M.B.B.S.,
Joint Director of Health and Family Welfare. Madurai District, who is kind enough
to permit me to undertake this study in the Government Hospitals and Family
Planning Centre. I am immensely thankful for her encouragement during this
study.
I consider this as an honoured privilege to express my gratitude to
Prof.Dr.Angela Gnanadurai. Ph.D.(N)., Vice Principal, College of Nursing,
Karaikonam for her continuous support which had motivated me to successfully
complete my work.
I extend my deep sense of gratitude to Dr.Nalini Jeyavantha Santha
Ph.D.(N)., Principal, Sacred Heart College Of Nursing for their valuable
suggestions and constant guidance in carrying out this study.
My hearty gratitude to Prof. Mrs. Vijaya Rani Prince, M.Sc.(N)., M.A.,
M.Phil.(N)., Principal of Bishop’s College of Nursing. Dharapuram, for her
suggestions, precious advice and support for the completion of study.
My special thanks to Prof.Dr.Prince Jeyaseelan.Ph.D., for sparing his
valuable time in editing this manuscript.
My special thanks to Mr.R.Nagarajan. for sparing his time in editing this
manuscript.
I extend my sincere thanks to Prof.V.Mani.M.Phil., Biostatistics for the
I also extend my special gratitude to all the experts for their valuable inputs
of the instrument and learning module to improve the quality of this research work.
I express my sincere gratitude to Mrs.Angelin,M.L.I.S.(Librarian), C.S.I.
Jeyaraj Annapackiam College of Nursing. Madurai for extending necessary help in
the library throughout the course of this study.
Finaly my hearty gratitude are due to my dear Parents Er.Nelson Benjamin,
Mrs.Jeyabai Nelson and my husband Mr.C.R.Baskaran for their blessings and
moral support throughout this endeavour.
My sincere thanks to all the eligible couples, who participated in this study,
The investigator intended to carry out a study “To assess the
practice on permanent family planning methods and their determinance among
eligible couples at Madurai District”. A comparative descriptive design was
adopted for the present study. Conceptual frame work for the study was based on
Pender’s Health Promotion Model. Non-probability convenience sampling technique
was used to collect 400 female eligible couples and 100 male eligible couples as per
the inclusion criteria. The content validity of the tool and learning module was
established by obtaining suggestions from experts. The tool reliability was
statistically significant. Data were collected by using structured interview schedule
on general, specific determinance and practice domains. The pilot study was found to
be feasible. Main study data were obtained from the study subjects who had
undergone permanent family planning in Government Hospitals and Family
planning centre in Madurai District. Learning module pamphlet or C.D. on
permanent family planning method was distributed to the participants and to the
Health Care Provider of the centre for further motivation of the eligible couples to
adopt permanent family planning method. The data were analyzed using descriptive,
inferential statistical methods and interpreted based on the objectives and
hypothesis of the study.
The results of the study include:
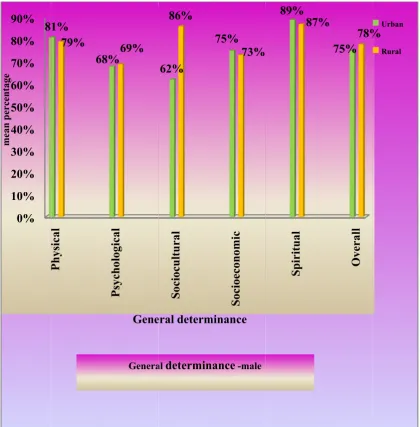
General determinance:
General determinance related to five factors among males the highest mean
percentage 89% and 87% were for spiritual determinance in urban and rural areas
respectively. Among females the highest mean percentage 80% and 75% were for
in rural and 75% in urban were higher compared to the mean percentage 70%
among females in rural and 69% in urban areas.
Difference between the general determinance on permanent family planning
method among urban and rural male eligible couples showed that the overall ‘t’
value (6.553 P=0.000) was highly significant at P<0.001 level. The ‘t’ value for
socio-cultural determinance was significant at p<0.001 level, socio-economic
determinance was significant at p<0.01 level and spiritual determinance was
significant at p<0.05 level. Among urban and rural female eligible couples, the
overall ‘t’ value (3.285 p=0.001) was significant at p< 0.01 level. The ‘t’ value for
physical, socio-economic and spiritual determinance were highly significant at
p<0.001 level and socio-cultural determinance was significant at p<0.05 level.
The overall ‘t’ value (16.499 p=0.000) was for general determinance among
male and female eligible couples in urban and the overall ‘t’ value (15.361 p=0.000)
was for male and female eligible couples in rural area, which were highly significant
at p<0.001 level.
Multiple regression between general determinance and selected demographic
variables among males in urban and rural area showed R2=75% and R2=77%
variance in the criterion variables respectively. Having one or more female or male
children were the most significant determinance to undergo permanent family
planning method among male eligible couples. Among female eligible couples in
urban and rural area showed (R2=74%) and (R2=66%) variance in the criterion
planning method in urban and rural areas.
Specific determinance:- knowledge determinance:
Specific knowledge determinance among males, the mean percentage 74% in
urban and 68% in rural were higher compared to the females’ mean percentage
63% in urban and 61% in rural areas.
Difference between the specific knowledge determinance on permanent family
planning method among urban and rural male and urban and rural female eligible
couples, the unpaired ‘t’ test calculated values revealed that the overall ‘t’ value
(2.457 p= 0.016) and (2.293 p = 0.022) were for knowledge determinance which
were significant at p < 0.05 level respectively.
The overall ‘t’ value (6.605 p=0.000) was for specific knowledge
determinance among male and female eligible couples in urban area and the overall
‘t’ value (5.782 p=0.000) was for male and female eligible couples in rural area
which were highly significant at p<0.001 level.
Multiple regression between specific knowledge determinance and selected
demographic variables in among females urban and rural area showed R2=95.5% and
R2=95% variance in the criterion variables respectively. Having sterilization after
medical termination of pregnancy and during interval period were the most
significant knowledge determinance on permanent family planning method among
female eligible couples. Among males in urban and rural area showed R2=85% and
R2=77% variance in the criterion variables respectively. Having number of children
and type of family were the most significant knowledge determinance on permanent
Specific barrier determinance related to five factors among males the highest
mean percentage 100% was for socio-cultural and 100% was for spiritual barrier
factors in urban and rural areas respectively. Among females, the highest mean
percentage 99% in urban and 94% in rural areas were for spiritual barrier factor.
The overall mean percentage regarding specific barrier determinance among
males 89% and 88% in urban and rural areas respectively were higher compared to
the mean percentage 66% and 58% among females in urban and rural areas
respectively.
Difference between the specific barrier determinance on permanent family
planning method among urban and rural male eligible couples the ‘t’ value (3.860 p
= 0.000) was for socio-economic barrier determinance which was highly significant
at P<0.001 level. Among urban and rural female eligible couples the ‘t’ value for
physical, psychological, socio-economic and spiritual barrier determinance were
highly significant at p < 0.001 level.
The overall ‘t’ value (23.506 p=0.000) was for specific barrier determinance
among male and female eligible couples in urban area and the overall ‘t’ value
(19.059 p=0.000) was for male and female eligible couples in rural area, which were
highly significant at p<0.001 level.
Multiple regression between barrier determinance and selected demographic
variables among male eligible couples in urban and rural area showed (R2=80%) and
(R2=87%) variance in the criterion variables respectively. Most of the samples were
from nuclear family, all the samples were educated, those who had adopted
permanent family planning method were having two or more children. These
variables had influenced in reducing the barrier determinance regarding tubectomy
and rural showed R2=94% and R2=93.9% variance in the criterion variables
respectively. Most of the source of information were through the care providers,
newspapers and relatives. The choice of post partum sterilization, Interval
sterilization, education and the age at marriage between 25 - 30 years, which had
played a major role in adopting tubectomy and who would be able to motivate other
eligible couples to adopt permanent family planning method. Among females the
barrier determinance towards vasectomy was high, hence they avoid their spouse to
undergo vasectomy.
Practice domains:
Practice domains on permanent family planning method among male eligible
couples the highest mean percentage 93% and 91% were for physical domain in
rural and urban respectively. Among females, the highest mean percentage 86% and
85 % were for spiritual domain in urban and rural areas.
Regarding practice, the overall mean percentage 85% and 82% were for males
in urban and rural respectively were higher compared to the mean percentage 80%
and 81% in urban and rural areas respectively among females.
Unpaired ‘t’ test was calculated to analyze the difference between practice
domains on permanent family planning method among urban and rural male eligible
couples and the overall ‘t’ value (5.301 p = 0.000) was highly significant at p <0.001
level. The ‘t’ value for psychological domain, socio economic domain and spiritual
domains were highly significant at p<0.001 level.
Among urban and rural female eligible couples the overall ‘t’ value was
(1.645 p = 0.101).The ‘t’ value for socio cultural domain was significant at p<0.05
level and ‘t’ value for socio-economic domain was highly significant at p<0.001
and female eligible couples in urban, which was significant at p<0.001 level. The
overall ‘t’ value (2.528 p=0.012) was for male and female eligible couples in rural
which was significant at p<0.05 level.
Multiple regression between practice and selected demographic variables
among male eligible couples in urban and rural showed (R2=92.7%) and (R2=78.3%)
variance in the criterion variables respectively. Most of the samples were from
nuclear family received information from care providers and counselling was given
to them, which had reduced their fear and they had high level of practice satisfaction
who would be able to motivate other eligible couples to adopt vasectomy. Among
female eligible couples in urban and rural showed (R2=90.3%) and (R2=85.3%)
variance in the criterion variables respectively. The females who had received
information through care providers and relatives, who were between the age group of
20 - 40 years, having one or more male children and education had high level of
practice satisfaction on permanent family planning method, who would be able to
motivate other eligible couples to adopt permanent family planning method.
Karl pearsons correlation co-efficient was calculated to analyze the relationship
between knowledge determinance and practice on permanent family planning
method among urban and rural eligible couples and there was a positive relationship
between knowledge determinance and practice on permanent family planning
method among female eligible couples in both urban and rural which was highly
significant at p<0.001 level.
It is concluded that for males (p<0.001) and females (p<0.01) the general
determinance had influenced them to undergo permanent family planning in both
on vasectomy (p<0.001) related to physical, psychological, socio-economic and
spiritual barrier determinance compared to males misconception on socio-economic
barrier determinance only (p<0.001) regarding tubectomy. Overall the practice
domains were highly satisfactory (p<0.001) among males after vasectomy when
compared to the female eligible couples after tubectomy p=0.101.
Inculcating knowledge and creating awareness among male and female
eligible couples regarding general and specific determinance on permanent family
planning methods will further facilitate more eligible couples to adopt permanent
CHAPTER CONTENT Page No.
CHAPTER - I INTRODUCTION
Background of the study 1
Need for the study 3
Statement of the problems 7
Aim of the study 7
Objectives of the study 8
Hypotheses 8
Operational definition 9
Assumption 10 Delimitation 11
Conceptual frame work 11
Projected outcome 15
CHAPTER - II REVIEW OF LITERATURE
Part I : Permanent family planning method . 16
Part II : Studies related to general determinance
on Permanent family planning method. 23
Part III : Studies related to specific determinance
on Permanent family planning method. 32
Part IV : Studies related to practice on Permanent
family planning method. 37
CHAPTER - III RESEARCH METHODOLOGY
Research approach 50
Research design 50
Setting of the study 50
Population 51
Sampling technique 51
Sample size 51
Description of the tool and scoring 52
Validity 56 Reliability 56
Pilot study 57
Data collection procedure 59
Protection of human subjects 61
CHAPTER - IV DATA ANALYSIS AND INTERPRETATION 62
CHAPTER - V DISCUSSION 137
CHAPTER - VI SUMMARY 167
CONCLUSION 181
IMPACT OF THE STUDY 187
NURSING IMPLICATIONS 188
LIMITATIONS 189
RECOMMENDATIONS 189
Table
Number CONTENT
Page No.
1.1 Frequency and percentage distribution of the samples according to their demographic data among male and female eligible couples in urban and rural area.
64
1.2 Frequency and percentage distribution of clinical demographic
variable among male and female eligible couples in urban and rural area.
67
2.1 Frequency and percentage distribution of general determinance on
permanent family planning method among urban and rural eligible couples.
80
2.2 Frequency and percentage distribution of specific knowledge
determinance on permanent family planning method among urban and rural male and female eligible couples.
81
2:3 Frequency and percentage distribution of barrier determinance on
permanent family planning method among urban and rural male and female eligible couples.
82
2.4 Frequency and percentage distribution of level of practice on
permanent family planning method among urban and rural male and female eligible couples.
83
2.5 Mean, SD and mean percentage wise distribution of general
determinanceon permanent family planning method among male and female eligible couples in urban and rural area.
84
2.6 Mean, SD and mean percentage wise distribution of specific
determinance on permanent family planning method among male and female eligible couples in urban and rural area.
86
2.7 Mean, SD and mean percentage wise distribution of practice on
permanent family planning method among male and female eligible couples in urban and rural area.
88
3.1 Difference between the general determinance on permanent family
planning method among male and female eligible couples in urban and rural.
90
3.2 Difference between the specific determinance on permanent family planning method among eligible couples in urban and rural area. 92
4 Difference between the practice domains on permanent family
planning method among male and female eligible couples in urban and rural area
on permanent family planning method among male and female eligible couples in urban and rural area.
96
6.1 Association between general determinance on permanent family
planning method and selected demographic variables among urban female eligible couples.
97
6.2 Association between the general determinance on permanent family
planning method and selected demographic variables among rural female eligible couples.
100
6.3 Association between the knowledge determinance on permanent
family planning method and selected demographic variables among urban female eligible couples.
103
6.4 Association between the knowledge determinance on permanent
family planning method among rural female eligible couples and selected demographic variables.
106
6.5 Association between the barrier determinance on permanent family planning method among urban female eligible couples and selected demographic variables.
110
6.6 Association between the barrier determinance on permanent family
planning method and selected demographic variables among rural female eligible couples.
113
6.7 Association between the knowledge determinance on permanent
family planning method and selected demographic variables among urban male eligible couples.
116
6.8 Association between the knowledge determinance on permanent
family planning method and selected demographic variables among rural male eligible couples.
117
6.9 Association between the barrier determinance on permanent family
planning method and selected demographic variables among urban male eligible couples.
119
6.10 Association between the barrier determinance on permanent family
planning method and selected demographic variables among rural male eligible couples.
120
7.1 Association between the practice on permanent family planning
method and selected demographic variables among urban female eligible couples.
122
method and selected demographic variables among rural female eligible couples.
124
8.1 Average relationship between general determinance on permanent
family planning method and selected demographic variables among urban and rural male eligible couples.
127
8.2 Average relationship between the specific knowledge determinance on permanent family planning method and selected demographic variables among urban and rural male eligible couples.
128
8.3 Average relationship between the specific barrier determinance on permanent family planning method and selected demographic variables among urban and rural male eligible couples.
129
8.4 Average relationship between the general determinance on permanent family planning method and selected demographic variables among urban and rural female eligible couples.
130
8.5 Average relationship between the specific knowledge determinance on permanent family planning method and selected demographic variables among urban and rural female eligible couples.
131
8.6 Average relationship between the specific barrier determinance on permanent family planning method and selected demographic variables among urban and rural female eligible couples.
133
9.1 Average relationship between practice on permanent family planning method and selected demographic variables among urban and rural male eligible couples.
135
9.2 Average relationship between practice on permanent family planning method and selected demographic variables among urban and rural female eligible couples.
Number
1 Conceptual frame work.
2 Madurai district taluk map.
3 Flow chart on work plan of methodology.
4.1 Frequency percentage of eligible couples according to their religion. 4.2 Frequency percentage of eligible couples according to their occupation. 4.3 Frequency percentage of eligible couples according to their family monthly
income.
4.4 Frequency percentage of eligible couples according to their source of information.
5.1 Frequency percentage of eligible couples according to their type of family.
5.2 Frequency percentage of eligible couples according to their number of
children.
5.3 Frequency percentage of eligible couples according to their number of
male children.
5.4 Frequency percentage of eligible couples according to their number of
female children.
5.5 Frequency percentage of eligible couples according to their usage of
temporary family planning method.
5.6 Frequency percentage of eligible couples according to their service
approached
5.7 Frequency percentage of male eligible couples according to their type of sterilization.
5.8 Frequency percentage of permanent family planning among female
eligible couples during post partum period.
5.9 Frequency percentage of permanent family planning among female
eligible couples during interval period.
5.10 Frequency percentage of reason for interval sterilization among female eligible couples.
5.11 Frequency percentage of permanent family planning among female
among female eligible couples.
5.13 Frequency percentage of usage of condom among male eligible couples
after vasectomy.
5.14 Frequency percentage of sexual life among male eligible couples after vasectomy.
5.15 Frequency percentage of semen analysis among male eligible couples
after vasectomy.
5.16 Frequency percentage of sexual life among female eligible couples after tubectomy.
6.1 Level of general determinance among urban and rural male and female eligible couples.
6.2 Level of specific knowledge determinance among urban and rural male and female eligible couples.
6.3 Level of specific barrier determinance among urban and rural male and female eligible couples.
6.4 Level of practice among urban and rural male and female eligible
couples.
6.5 Mean percentage of general determinance among urban and rural male
eligible couples.
6.6 Mean percentage of general determinance among urban and rural female eligible couples.
6.7 Mean percentage of specific knowledge determinance among urban and
rural male and female eligible couples.
6.8 Mean percentage of specific barrier determinance among urban and rural male eligible couples
6.9 Mean percentage of specific barrier determinance among urban and rural female eligible couples.
6.10 Mean percentage of practice on permanent family planning method among urban and rural male eligible couples.
method among urban male eligible couples.
7.2 Knowledge determinance and practice on permanent family planning
method among rural male eligible couples.
7.3 Knowledge determinance and practice on permanent family planning
method among urban female eligible couples.
7.4 Knowledge determinance and practice on permanent family planning
A Letter seeking permission to conduct the study. i Ethical clearance from the institutional ethical committee
Ethical clearance from the study centre
B Letter seeking experts opinion for content validity of the tools
ii
C List of expert for content validity of the tools iii
D Letter seeking experts opinion for content validity of the learning module
v
E List of expert for content validity of the learning module vi
F Tool vii
Male & Female English Male & Female Tamil
G Learning module on permanent family planning lx
Male - English & Tamil Female - English & Tamil
CHAPTER I
INTRODUCTION
Background of the Study
The most sparking current global discussion on population issues include
environmental, health and justice. Compulsory population control is needed to help
preserve the earth and to tackle the dangers of population explosion.(1) Doses of the
antidote would be carefully rationed by the Government to produce the desired family
size.(2) The global total fertility rate currently stands at 2.53 children per woman.
Population control focus on the health, rights, and well-being of women.(3)
Worldwide, nearly 40% of pregnancies are unintended and 80 million
unintended pregnancies occur each year.(4) An estimated 350 million women in the
developing countries either did not want their last child, do not want another child or
want to space their pregnancies, but they lack access to information, affordable means
and services to determine the size and spacing of their families. In the developing
world, an estimated figure of 5,14,000 women die annually of complications arise out
of pregnancy, anaemia and abortion.(5) Out of which 86% of deaths occur in
the sub-Saharan Africa region and South Asia.(6,7) In the United States, during 2001,
almost half of the pregnancies were unintended.(8)
India is currently the second most populous country in the world and
awareness on healthy family living habits is woefully lacking or inadequate. With
large sections of the female population adopting family planning compared to male
population, resulting in ill-effects of female occupation, their productivity house
anaemia. So a close inspection of the nature of these inequalities/infirmities reveal the
root causes lying at the core of the great obstacle to live or lead a satisfactory healthy
life in our nation.(9)
The fertility rate is not declining as fast as expected. The total fertility rate in
India during 2009 was 2.7, the total marital fertility rate was 5.4. Various factors such
as a strong preference for a son, the low status of women, a high infant mortality, high
illiteracy level, inadequate target free health-care facilities and irregular follow-up
play a major role in keeping eligible couples away from accepting contraception. The
wide variations of existing customs, beliefs, barriers such as lack of awareness,
negligence of small family responsibilities and socio-economic development among
Indians lead the people generally in favour of a large family size and thereby are not
in favour of adopting methods of contraception.(10 )
In developing countries, especially in India deep rooted influencing factor
towards life practice including socio-cultural, religious concepts such as beliefs,
customs, superstitions regarding pregnancy, child birth, health and the role of the
mother are still widely prevalent. Women are more vulnerable to the health risks
associated with child bearing causing anaemia, physical weakness, psychologically
overloaded with family care and socio-economic burden, These contribute to high
rates of maternal morbidity and mortality. Family planning plays a crucial role in safe
guarding the health of women.(11)A planned family is the best environment for child’s
overall development. When children are effectively parented, they feel better about
People generally perceive that the family planning program is mostly meant
for the women as they are bearers of the children. Some common beliefs such as
adopting a contraceptive method may reduce a man’s masculinity and contraception
impairs the health of working men,” also act as a barrier for the adoption of the family
planning program by men. Women experience physical, psychological, socio cultural
and socio-economic stress from previous pregnancy, delivery and strain of taking care
of the child. When mother’s health is disturbed/debilitated whole family’s routine will
be disturbed a lot, as she has an important role in the family to maintain the healthy
and satisfactory family life.(13) In cultures where patriarchy is accepted as the only
proper family structure, men and women may be trapped in a pattern of relationships
and dependencies that can frustrate them both. Women and men both feel the stress
and strain. As a result, wives are increasingly vocal about their burden and
frustration; husbands are withdrawing from family responsibilities which gives
unsatisfactory family life.(14) Community involvement can help to counter this by
ensuring that men to accept permanent family planning to achieve small family
norm, which in turn could help in reducing the burden of the women physically,
psychologically, socio-culturally and socio-economically to lead a healthy and
satisfactory life which may help to hear the healthy women's voices along with
healthy men's voices in the community.(15,16)
Population problem has three dimensions, it is concern with the number of
people versus limited amount of material resources, people versus cultural resources
and society’s ability to satisfy eligible couples’ total needs such as physical,
psychological, socio-cultural, socio-economic and spiritual domains. As nurses, it is
essential to know the various determinance such as influencing factors, barrier factors,
make both the male and female eligible couple to be aware of the concept of planning
the families which leads to live a healthy and satisfactory life.
Need for the Study
The global population increases at a rate of around 150 people per minute,
220,000 people per day and 80 million each year. Around 90% of these population
increase the share from third world countries with their population doubling every 37
years.(17 ) Therefore, the best solution in this global fight to reduce the population is to
implement and expand family planning programmes.(18) Globally, men have not
shared equally with women in the responsibility for fertility regulation. Family
planning efforts have been directed almost exclusively towards women and there is
lack of male involvement in family planning programs. In developing countries, the
number of children men have indicate their social status and wealth, so men's
acceptance for contraception is low. Population specialists believe that introduction of
new no scalpel method for male could go in hand with a realization of the economic
cost of children, thereby increasing male involvement.(19)
As per 2011 census India's total population is 1.21 billion (121 crore). India
has 623.7 million males (62.37 crore men) and 586.5 million females (58.6 crore
women).The urban population was 31.2% of the total population. The Indian
population has increased to 1.21 billion with a decade growth of 17.64%. India with
2.4% of the world's surface area accounts for 17.64 % of its population.( 20) The
lowest total fertility rate in the world is China which had a total fertility rate of
0.41.(21)In 2009, India had a higher fertility rate than China, Iran, Myanmar (Burma)
and Sri Lanka.(22) The fertility rate in India was 2.7 in 2009.(23 )The total fertility rate
reproductive rate is exactly one.(24,25) The goals under National population policy
stated to promote vigorously the small family norm to achieve the expected total
fertility rate. One of the primary goals of the policy was to reduce the total fertility
rate to 2.1 by 2010. Fertility rate in India continues to be above the replacement level.
By the end of the eleventh five year plan (2012), the Health and family welfare
department demographic goals in Tamil Nadu is to achieve 1.4 total fertility rate.(26)
Madurai District is one of the important districts in Tamil Nadu state. The
district has 13 blocks and 7 Taluks. The taluks include Madurai North,
Thirumangalam, Usilampatti, Peraiyur, Madurai South, Melur and Vadipatti. As per
2001 census, the population of Madurai District was about 25.8 lakhs and it
constituted four percent of the population of the state population, out of which 13.0
lakhs were males and 12.8 lakhs were females. Around 56% of the population of the
district live in urban areas. The sex distribution of the population showed that 5.7
lakhs were males and 5.6 lakhs were females in rural area and 7.3 lakhs males and
7.1 lakhs females were from urban area.(27)
In Madurai District the subject of family planning has become more of a
female planning with very less involvement of men opting for the simple procedure.
The latest statistical report from the Deputy Directorate of Madurai District
2009-2010 showed that 2,97,828 females had tubectomy and 160 males had vasectomy.The
2010-2011 statistics revealed that 3,05,606 females had tubectomy and 168 males
had vasectomy. The 2011-2012 statistics stated that 3,16,233 females had tubectomy
Based on the statistical reports the researcher felt that the men's attitude is
much more important in the adoption of permanent method of contraception in
limiting the family size. Male method accounts only for 0.1% of current permanent
contraceptive use. Vasectomy is safer and easier to perform in health centres than
tubectomy. As males are the main decision makers in Indian households, activities
need to focus on imparting knowledge on reproductive health for both men and
women about the correct solution for barrier factors towards family planning and
advantages of small family. (30,31)
Hence, this study was aimed to assess the general and specific determinance,
such as physical, psychological, socio cultural, socio-economic and spiritual factors,
knowledge and barrier factors which had influenced the eligible couple to adopt
permanent family planning method. Also aimed to focus practice on permanent family
planning method related to satisfaction on physical, psychological, socio-cultural,
socio-economic and spiritual domains among eligible couples, there by identifying the
general determinance, specific determinance and practice related to satisfaction on
permanent family planning method. The researcher also had aimed to prepare a
learning module on male and female permanent family planning method, which will
help the eligible couples to motivate other eligible couples to adopt permanent family
planning method. So, as a nurse it is important to take the responsibility of educating
and motivating the rural and urban eligible couples to be aware of permanent family
planning practices to reduce the barrier factors among male eligible couples which
will help in reducing the family burden of the women and also to have a satisfaction
Statement of the Problem
An approach to assess the practice on permanent family planning methods
and their determinance among eligible couples at Madurai District.
Aim
To identify the influencing general determinance such as physical,
psychological, socio-cultural, socio-economic and spiritual aspects on permanent
family planning method, knowledge determinance as motivating factor on permanent
family planning method and specific barrier determinance on permanent family
planning method among eligible couples in urban and rural areas. Also to examine the
practice on permanent family planning method related to satisfaction on physical,
psychological, socio-cultural, socio-economic and spiritual domains among eligible
couples in urban and rural areas.
Objectives
1. To assess the determinance and practice on permanent family planning
method among urban and rural eligible couples.
2. To compare the determinance on permanent family planning method among
urban and rural eligible couples.
3. To compare the practice on permanent family planning method among
urban and rural eligible couples.
4. To find the correlation between the knowledge determinance and practice on
permanent family planning method among urban and rural eligible couples.
5. To find the association between the determinance on permanent family
planning method and selected demographic variables among urban and rural
6. To find the association between the practice on permanent family planning
method and selected demographic variables among urban and rural eligible
couples.
7. To find the average relationship between determinance on permanent family
planning method and selected demographic variables among urban and rural
eligible couples.
8. To find the average relationship between practice on permanent family
planning method and selected demographic variables among urban and rural
eligible couples.
Hypotheses
H1 There is a significant difference between determinance on permanent family
planning method among urban and rural eligible couples.
H2 There is a significant difference between practice on permanent family
planning method among urban and rural eligible couples.
H3 There is a significant correlation between the knowledge determinance and
practice on permanent family planning method among urban and rural eligible
couples.
H4 There is a significant association between the determinance on permanent
family planning method and selected demographic variables among urban and
rural eligible couples.
H5 There is a significant association between the practice on permanent family
planning method and selected demographic variables among urban and rural
H6 There is a significant relationship between determinance on permanent family
planning method and selected demographic variables among urban and rural
eligible couples.
H7 There is a significant relationship between practice on permanent
family planning method and selected demographic variables among urban and
rural eligible couples.
Operational Definitions
Approach: In this study it is a way to find out the determinance and practice
on permanent family planning method among eligible couples.
Assess: In this study it refers to the measurement by using instrument with the
score to measure the level of determinance which include the factors such as general
factors, specific factors and also practice domains on permanent family planning
method among eligible couples.
Determinance: It means the factors which help to decide the nature or
outcome. In this study it refers to the decision making concept based on general
determinance such as physical, psychological, socio-cultural, socio-economic,
spiritual aspect which is measured by five point rating scale. Specific determinance
such as knowledge factor on permanent family planning method which is measured
by multiple choice questions. Specific barrier determinance related to physical,
psychological, socio-cultural, socio-economic and spiritual aspect among eligible
couples regarding permanent family planning method which is measured by check
list.
Practice: In this study it refers to the self expressed responses related to the
activities satisfied within three/six months after adopting permanent family planning
method among male and female eligible couples related to physical, psychological,
socio-cultural, socio-economic and spiritual domain which is measured by five point
Permanent Family Planning Methods: In this study permanent family
planning method refers to an operation whereby resection of a segment of both the
fallopian tubes and the cut ends are ligated to achieve female permanent sterilization
termed as tubectomy and also refers to a procedure whereby resection of a segment
of both the vas deferens tubes and the cut ends are ligated to achieve male permanent
sterilization termed as vasectomy or no scalpel vasectomy.
Eligible Couples: In this study eligible couple refers to married men and
women within the age group of 20 to 45 years having one or more than two children.
Among such eligible couples females those who were admitted and undergone
permanent sterilization during immediate postpartum period within seven days or
within three months of interval period after delivery or after medical termination of
pregnancy within five months of the last delivery in Government hospital or in
Family planning centre are referred as female eligible couple and males those who
had undergone permanent sterilization in Government Hospital or in Family planning
centre are referred as male eligible couple.
Assumption
The factors influencing will be an important criteria for the eligible couples to
adopt permanent family planning method.
The practice domain satisfaction on permanent family planning method among
female eligible couples may be low compared to male.
Several factors contribute to the decrease in fertility.
Family planning helps the eligible couples to practice a satisfied healthy life
style.
Influencing factors for adoption of family planning method differ from each
Delimitations
Married men and women within the age group of 20 to 45 years having one
or more than two living children.
Male eligible couple is those who had adopted permanent family planning
method.
Female eligible couple is those who had adopted permanent family planning
method during post partum period within seven days or within three months of
interval period after delivery or after medical termination of pregnancy within
5 months after the last delivery.
Sample size was limited to 500 eligible couples based on power analysis.
Sample subjects were limited to Madurai District only.
Conceptual Frame Work
Pender’s Health Promotion Model (2002 revised) was adopted for the present
study. The Health Promotion Model proposed by Pender (1982 revised 2002), was
designed to be a “complementary counterpart to models of health protection”. It
defines health as a positive, dynamic state, not merely the absence of disease (Pender,
2002) Health Promotion is a model that describes the multidimensional nature of
persons as they interact within their environment to pursue health. It helps to focus
on identifying the determinants of health promoting life style.
The Model focuses on the following three areas:
1. Individual characteristics and experiences.
2. Behaviour specific knowledge and affects to motivate health promoting
behaviour.
Main focus is on cognitive, perceptual and modifying factors and participation
in health promoting behaviour. The model also identifies the factor that influence the
health promotion activities. The health promotion model notes that each person has
unique personal characteristics and experiences that affect subsequent actions. These
variables can be modified through nursing actions. Health promoting behaviour is the
desired behavioural outcome and is the end point in the health leading to enhanced
functional ability and satisfactory life at all stages of development.
1. Modifying Factors:
In the present study the modifying factors include:
a) Demographic characteristics such as age, religion, residence, occupation,
education, income and source of information.
b) Biological characteristics such as age at marriage, number of years after
marriage, type of family, number of living child, male child, female child,
whether used temporary family planning method, service approached,
counselling, informed consent, sterilization procedure, reason for adopting
permanent family planning method, number of pregnancy, gravida and
abortion.
c) Interpersonal influences such as information on permanent family planning
received from health care provider, mass media (TV), relatives and
newspapers.
d) Situational factors include access to health centres and availability of
environmental options to adopt permanent family planning method.
e) Behavioural factors include previous experience of others, knowledge on
permanent family planning method and skill in health promoting actions by
2. Behaviour Specific Cognitive Perceptual Factors:
Cognitive perceptual factors are considered to be the primary motivational
mechanism for acquiring and maintaining health promoting behaviour. In the present
study it include:
a) Perceived control: Person perceive that they have control over their own
health and use preventive measures. In this study eligible couple have
control over the misconception and take correct decision based on their
determinance before adopting permanent family planning method.
b) Perceived Self Efficacy: Judgment of personal capability to organize and
execute a health-promoting behaviour. In this study eligible couples
adopted permanent family planning method based on self motivation, self
awareness and self capacities to achieve a good healthy coping life style.
c) Perceived health status: Subjective positive or negative feeling that occur
before, during and following behaviour based on the stimulus properties of
the behaviour itself. In this study activities that affect the eligible couples
healthy life after adopting permanent family planning method such as nature
of work, work load, physiological, psychological, socio-cultural, socio-
economic and spiritual imbalance are assessed.
d) Perceived benefit: Anticipated positive outcomes that will occur from
healthy behaviour may facilitate satisfactory coping practice in life. In this
study adoption of permanent family planning method facilitate good self
coping abilities, family coping abilities in relation to physical,
e) Perceived Barriers: Anticipated imagined or real blocks and personal
costs of understanding a given behaviour. In this study, internal barriers
such as physical, psychological, interpersonal aspects and external barriers
such as socio-cultural, socioeconomic and spiritual aspects are assessed.
Lack of knowledge, ignorance and misconception in decision making about
permanent family planning method among eligible couple leads to poor
motivating concept and unhealthy coping life style.
3. Behavioural Outcome
Cues to action: Immediate competing demands (low control) and preferences
(high control). In this study, person adopted health promoting behaviour based on
internal origin success i.e personal awareness of the permanent family planning
method and increased feeling of well being. External origin success includes
conversations, mass media, news papers, information about permanent family
planning method and its health benefits. Based on internal and external origin, the
eligible couples adopted permanent planning method which is of high control and
were able to develop and live a healthy coping life physically, psychologically, socio-
culturally, socio-economically and spiritually.
Health Promoting Behaviour: End point or action outcome directed toward
attaining positive health outcome such as optimal well-being, personal fulfilment and
productive living. In this study practice of permanent family planning method by
eligible couples will enhance good individual health, healthy family life and
population explosion of the nation will be controlled.
Effective plan of action leads to positive health promoting behaviour to
achieve better satisfied personal, family health and able to motivate the
Ineffective plan of action leads to negative health promoting behaviour due
to unsatisfied personal, family health and unable to motivate the future
eligible couples to adopt permanent family planning method. (32)
Projected Outcomes
The determinants and practice of permanent family planning method will
serve as a basis to educate the urban and rural eligible couples about
permanent family planning method.
Will help to enrich total physical, psychological, socio-cultural, socio-
economic and spiritual status of the eligible couples which in turn helps to
improve the wellbeing of the family, protect and prevents the family from
various health hazard. Thus helps in reducing the population explosion of the
nation.
Adequate knowledge and creating awareness using pamphlet or C D among
male and female eligible couples regarding permanent family planning will
reduce the barrier determinance which will further facilitate effective adopters
of permanent family planning to motivate other eligible couples to undergo
MODIFYING FACTORS
BEHAVIOUR SPECIFIC COGNITIVE PERCEPTUAL
FACTORS
HEALTH PROMOTING BEHAVIOURAL OUTCOME
Demographic Data
Age, sex, religion, residence, education, occupation, income, source of information.
Biological Factor:Year of
marriage, age at marriage, type of family, living child,No. of male child, No. of female child, usage of T.F.P.M, service approached,counselling, male sterilization, number of para, gravida, abortion, sterilization postpartum, interval, M.T.P. Its reason. and spouse permission,its reason, condom usage, sexual activity and sperm test.
Interpersonal influences:
Information on P.F.P.M. – health care provider, mass media, relatives and news paper.
Behavioural Factor: Previous
knowledge on P.F.P.M
Situational Factor:Access to
health centre to adopt P.F.P.M. Selfesteem, self motivation and personal competence.
General
determinance:Moderate &
high level.
Specific Knowledge
determinance: Moderate
& adequate level.
Specific barrier
determinance: High score
(low misconception).
Practice: Moderate level
& high level.
Tool Component
General determinance:
Structured interview schedule using rating scaleon determinance: physical, psychological sociocultural,socioecon omic and spiritual factor.
Specific Knowledge determinance:
MCQ to assess the knowledge factor.
Specific barrier determinance:
Check list on barrier factor.
Practice:
Rating scale on practice of P..F.P.M.
General determinance:
Low level.
Specific knowledge determinance:
Inadequatelevel.
Specific
determinancebarrier:
Less score (high levelmisconception)
Practice: Low level.
Learning Module. Ineffective- unable to motivate others. Effective-
able to motivate
[image:41.595.99.787.88.540.2]CHAPTER – II
REVIEW OF LITERATURE
Review of literature is an important step in the development of a research project. It
involves systematic identification, location, scrutiny and summary of written
materials that contain information on a research problem. (33)
The literature gathered from an exclusive review is depicted under the following
headings:
Part I - Permanent family planning method.
Part II - Studies related to determinance on permanent family planning
method among eligible couples.
Part III - Studies related to specific determinance on permanent family
planning method among eligible couples.
Part IV - Studies related to practice on permanent family planning
method among eligible couples.
Part I- Permanent Family Planning Method:
Family planning is a way of thinking and living that is adopted voluntarily
upon the basis of knowledge, attitude and responsible decisions by individuals and
couples, in order to promote the health and welfare of the family group and this
contribute effectively to the social development of the country.(34)
According to Engender Health Organization (2002) report, the permanent
family planning method by male sterilization or vasectomy, is the interruption of the
male reproductive capacity for the purpose of permanently ending fertility. This is
be performed as an outpatient procedure. In a vasectomy, each vas deferens is cut so
that sperms are not released during the ejaculation. No-scalpel vasectomy was
developed and first performed in China during 1974. Instead of a scalpel, two
specialized instruments namely a ringed clamp and a dissecting forceps are used.
Because the scrotal skin puncture made with the dissecting forceps is so small, sutures
are not needed. No-scalpel vasectomy offers several advantages over conventional
vasectomy. It is cost effective, with no complications and less pain during the
procedure. In addition, it offers relatively less follow-up period and earlier
resumption of sexual activity after surgery. Because it requires no scrotal incision,
No-scalpel vasectomy is believed to decrease men’s fears about vasectomy.
Vasectomy procedure time is shorter when skilled providers use the No-scalpel
approach. Compliance with post vasectomy follow-up has been shown to be poor,
with a maximum of 45% of men not returning for any follow-up. This suggest that
current follow-up protocols do not work very well, even under favourable
circumstances. In general, vasectomy is highly effective and one of the most reliable
contraceptive methods available. (35)
Hugh H.(2002) focused on the need for a multidisciplinary approach to
address programmatically the critical issues that determine male participation in
reproductive health. It is imperative that health service providers include men as
partners in reproductive health by adopting a life-cycle approach which identifies the
services they need in a way that is both culture and gender sensitive. Major strategies
to improve male participation in reproductive health must include education, training,
promotion and service delivery. Men must be targeted through education and
promotion to share sexual, contraceptive and parenting responsibilities and to plan
health professionals through adequate training in the counselling of men and couples,
increased condom availability and provision of male-friendly services. (36).
According to Engender Health Organization (2002) report, recorded data on
the incidence of vasectomy are difficult to obtain, as vasectomy is neither widely
available nor commonly used in many countries. However, while sterilization use is
greatly weighted toward female sterilization. Data for the past 15-20 years reveal that
in some countries male sterilization represents an important family planning method.
Moderately high estimates of vasectomy incidence seen in Sri Lanka and Thailand
is around 5 per 1000 population. These countries have a fairly well-developed family
planning and sterilization programme that includes vasectomy. In contrast,
incidence in India remains relatively low with an estimated five-year average of 1
per 1,000. Acceptance of vasectomy has been less in Latin America: Brazil has the
highest incidence in the region, an average of 3 per 1000 for the five years prior to the
most recent survey, while in Colombia, Guatemala and Mexico the average was just
1 per 1000 only. Vasectomy data for China and the Republic of Korea have the
highest among Asian countries. Vasectomy data for Hong Kong suggest that it is
popular there also. (37)
Corey L.(2009) reported that the overall prevalence of vasectomy is lower in
developing countries. In Asia, with the exception of Bhutan, Iran, and the Republic of
Korea, the occurrence of vasectomy has gradually declined over the past 15 years.(38)
Finer L.(2006) opined that for achieving “Healthy people 2020 goal” it is
necessary to "improve pregnancy planning and spacing. Unintended pregnancies
occur among women of all income groups, educational levels and ages. However,
are highest among the women ages 18 to 24, women whose income is below the
poverty line and women possessing less than a high school diploma.(39)
Chandra A. et.al., (2005) reported that women with lower levels of education
and income, uninsured women and non-Hispanic black women are less likely to
have access to family planning services.(40)
According to Guttmacher Institute’s publication, men are less likely to have
access to family planning services and also in the act of receiving the services, when
compared to women.(41)
Engender Health Organization (2000) report grouped female sterilization
procedures into two broad categories namely procedures for reaching the fallopian
tubes (primarily abdominal approaches such as mini laparotomy, laparoscopy and
laparotomy) and methods for occluding the fallopian tubes (mainly ligation and
excision, mechanical devices such as clips or rings and electro coagulation). The
timing of the sterilization procedure is an important consideration in the choice of
approach. Female sterilization procedures can be performed in conjunction with a
term delivery i.e., soon after a vaginal delivery or immediately following an
uncomplicated first- trimester abortion during interval period. Postpartum
procedures are usually performed during the first 48 hours following vaginal delivery
or with special care 3-7 days after delivery. Interval sterilization is performed at six or
more weeks after delivery. Several factors affect the decision to have a postpartum
sterilization, including a sterilization procedure performed within the 42-days period
following delivery, an interval sterilization or a sterilization procedure performed at
any other time. Interval procedures tend to outweigh postpartum sterilizations among
sterilizations, however, are considerably more common than interval procedures
among countries in Latin America. The Caribbean countries with high levels of
interval procedures, consider to introduce postpartum sterilization, since it is generally
more convenient for the client and is less costly to the programme. Country
programmes that emphasize postpartum procedures, however, must ensure clients’
informed choice and consent before they experience the stress of labour.(42)
Blayo Y.(1993) elaborated the nature of the changing family planning and
population control policies in China and their impact on fertility. During the 1950s,
the Marriage Law was implemented and communes, brigades, teams in rural areas and
work units in districts and residents' committees effectively administered the means of
population control. The legal minimum age for males to marry was 20 years and 18
years for females. However, it was strongly urged that females not marry until 23
years in rural areas and until 25 years in urban areas. The urged age limit for males
from rural area were 25 and 28 years respectively. Rural areas stipulated a birth
interval of 3 years and urban areas required 4-5 years. The limit on births was 2 in
urban areas. In rural areas it was 3 until 1977 when the number was reduced to 2.
Unplanned pregnancies should be terminated according to the law. By 1975-76, the
program was universally applied, but fertility decline still did not meet the goals. The
single-child campaign was then established in 1979. Incentives and bonuses were
offered to those bearing only 1 child and disincentives and penalties were applied to
those who had additional children. The new mobilization of 1983 attempted to restrict
births to ‘one’ more vigorously; abortions became compulsory and sterilizations were
Ringheim K. 1993. reported that globally, men have not shared equally with
women the responsibility for fertility regulation. While family planning efforts have
been directed almost exclusively toward women, the lack of male involvement may
also reflect the limited options available to men. Current methods for men are either
coitus-dependent, such as the condom or withdrawal or permanent, such as
vasectomy. The 20-year history of social science research on male contraceptive
methods is examined here in terms of the human factor and method factors related to
the acceptability of hypothetical methods. New male methods, particularly if
reversible, may alter men's willingness to accept or share responsibility for the control
of fertility. Research opportunities in the areas of gender, decision-making,
communication, health education, and service delivery will be enhanced when
methods for women and men are comparable.
Most men believe that men should share fertility regulation responsibilities
with their partners, but only a small proportion do so. Most family planning (FP)
programmes are designed to serve only women. Limited contraceptive choices may
also explain this inconsistency. Vasectomy is the only new male method in 25 years,
the other methods being condoms and periodic abstinence. Before men or even
women use a method, they must have already thought about fertility regulation. They
must also consider their life style and stage of reproductive life. Men are more likely
to accept a non-coitus dependent and long-acting contraceptive method. In developing
countries, the number of children men have indicates their social status and wealth, so
men's demand for contraception is low. Further, couples do not often use the
traditional methods of spacing births such as postpartum abstinence and prolonged
breast feeding. Long-acting, non-coitus dependent, and reversible male contraceptive
methods are currently being researched and include injectable o