EVALUATION AND ACCURACY OF THREE DIFFERENT APEX
LOCATORS IN WORKING LENGTH ESTIMATION OF VITAL FIRST
MANDIBULAR MOLARS – AN INVIVO STUDY
Dissertation submitted to
THE TAMIL NADU Dr.M.G.R. MEDICAL UNIVERSITY
In partial fulfillment for the degree of
MASTER OF DENTAL SURGERY
BRANCH IV
ACKNOWLEDGEMENTS
First of all, I am grateful to
The Almighty God
who gave me the inner
strength and confidence to understand, learn and complete this research and blessing
me with all the goodness and wonderful people in my life.
My sincere heartfelt thanks to my post graduate teacher and my guide Dr.
I.ANAND SHERWOOD, M.D.S., PhD., Professor & Head
, Department of
Conservative Dentistry and Endodontics, CSI college of Dental Sciences and
Research, who have helped me with his guidance, support, care and constant
encouragement throughout my study period wherever and whenever needed. His
guidance with patience and motivation helped me in all the time of research. I like
to give my deep gratitude for being my advisor and mentor during my
post-graduation period. I am indeed blessed to be under his supervision and assistance
with his words of appreciation.
I convey my sincere thanks to
Dr. Thanvir Mohamed Niazi, M.D.S.
,
I also wish to thank the management of CSI College of Dental Sciences and
Research, Madurai for their help and support.
My sincere thanks to
Mrs. Aishwarya Mani M.Sc., Biostatistics,
for her
guidance in statistics.
I remain ever grateful to
my supportive batch mates, ever motivating
juniors and friends
for their immense help throughout the study.
Special thanks to
my parents
for their love, understanding, support and
encouragement throughout these years without which, I would not have reached so
far. I would really like to appreciate and thank
my sister
for her soul support
throughout the thesis works.
CONTENTS
S. NO. INDEX PAGE.NO
1. INTRODUCTION 1 - 5
2. AIMS AND OBJECTIVES 6
3. REVIEW OF LITERATURE 7 - 20
4. MATERIALS 21 – 22
5. METHODOLOGY 23 – 32
6. RESULTS 33 – 52
7. DISCUSSION 53 – 59
8. SUMMARY 60
9. CONCLUSION 61 - 62
10. REFERENCES -
LIST OF FIGURES
FIGURE.NO TITLE PAGE NO.
FIGURE I ARMAMENTARIUM FOR ROOT CANAL THERAPY 28
FIGURE II ARMAMENTARIUM FOR ISOLATION 28
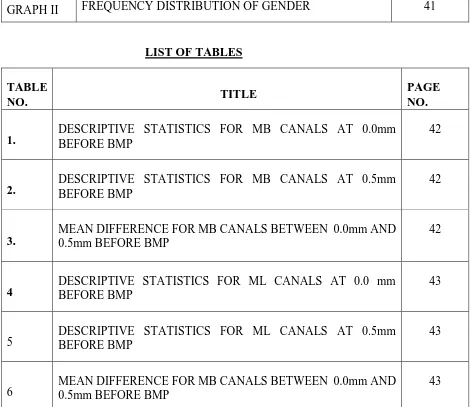
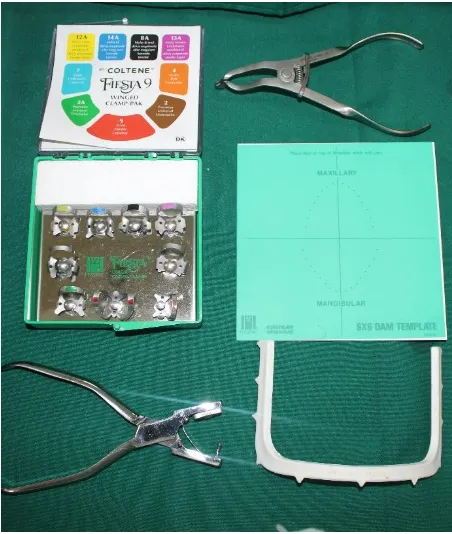
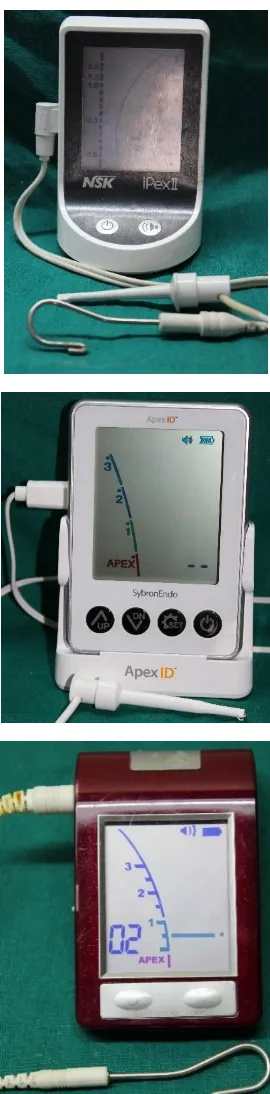
FIGURE III iPex II , Apex ID , Root ZX APEX LOCATORS 29
FIGURE IV
WORKING LENGTH ASSESSMENT USING DIFFERENT APEX LOCATORS
30
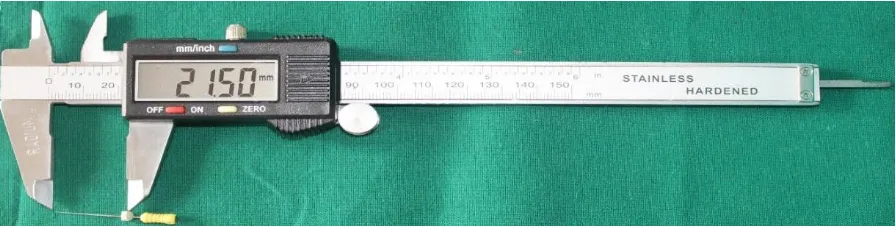
FIGURE V
MEASUREMENT OF WORKING LENGTH USING VERNIER CALIPER
31
FIGURE VI
ARMAMENTARIUM FOR RADIOGRAPHS
(PARALLELING DEVICE, PSP SENSOR AND
VISTASCAN)
31
FIGURE VII
RADIOGRAPHS TAKEN AT 0.0mm AND 0.5mm READINGS FOR THREE DIFFERENT APEX LOCATORS BEFORE BMP
32
FIGURE VIII
RADIOGRAPHS TAKEN AT 0.0mm AND 0.5mm READINGS FOR THREE DIFFERENT APEX LOCATORS AFTER BMP
32
TABLES AND GRAPHS
LIST OF GRAPHS
GRAPH.NO. TITLE PAGE NO.
GRAPH I
FREQUENCY DISTRIBUTION OF DIFFERENT AGE GROUPS IN THE SIXTY PATIENTS
41
GRAPH II FREQUENCY DISTRIBUTION OF GENDER 41
LIST OF TABLES TABLE
NO. TITLE
PAGE NO. 1.
DESCRIPTIVE STATISTICS FOR MB CANALS AT 0.0mm BEFORE BMP
42
2.
DESCRIPTIVE STATISTICS FOR MB CANALS AT 0.5mm BEFORE BMP
42
3.
MEAN DIFFERENCE FOR MB CANALS BETWEEN 0.0mm AND 0.5mm BEFORE BMP
42
4
DESCRIPTIVE STATISTICS FOR ML CANALS AT 0.0 mm BEFORE BMP
43
5
DESCRIPTIVE STATISTICS FOR ML CANALS AT 0.5mm BEFORE BMP
43
6
MEAN DIFFERENCE FOR MB CANALS BETWEEN 0.0mm AND 0.5mm BEFORE BMP
[image:9.612.71.541.269.676.2]7
DESCRIPTIVE STATISTICS FOR DISTAL CANALS AT 0.0 mm BEFORE BMP
44
8
DESCRIPTIVE STATISTICS FOR DISTAL CANALS AT 0.5mm BEFORE BMP
44
9
MEAN DIFFERENCE FOR DISTAL CANALS BETWEEN 0.0mm AND 0.5mm BEFORE BMP
44
10
DESCRIPTIVE STATISTICS FOR MB CANALS AT 0.0mm AFTER BMP
45
11
DESCRIPTIVE STATISTICS FOR MB CANALS AT 0.5mm AFTER BMP
45
12
MEAN DIFFERENCE FOR MB CANALS BETWEEN 0.0mm AND 0.5mm AFTER BMP
45
13
DESCRIPTIVE STATISTICS FOR ML CANALS AT 0.0 mm AFTER BMP
46
14
DESCRIPTIVE STATISTICS FOR ML CANALS AT 0.5mm AFTER BMP
46
15 MEAN DIFFERENCE FOR MB CANALS BETWEEN 0.0mm AND 0.5mm AFTER BMP 46
16
DESCRIPTIVE STATISTICS FOR DISTAL CANALS AT 0.0 mm AFTER BMP
47
17 DESCRIPTIVE STATISTICS FOR DISTAL CANALS AT 0.5mm AFTER BMP 47
18
MEAN DIFFERENCE FOR DISTAL CANALS BETWEEN 0.0mm AND 0.5mm AFTER BMP
19
COMPARISON OF MEAN DIFFERENCE ANALYSIS FOR APEX LOCATORS BEFORE AND AFTER BMP AT 0.5mm USING PAIRED t-TEST FOR MB CANALS
48
20
COMPARISON OF MEAN DIFFERENCE ANALYSIS FOR APEX LOCATORS BEFORE AND AFTER BMP AT 0.5mm USING PAIRED t-TEST FOR ML CANALS
48
21
COMPARISON OF MEAN DIFFERENCE ANALYSIS FOR APEX LOCATORS BEFORE AND AFTER BMP AT 0.5mm USING PAIRED t-TEST FOR DISTAL CANALS
49
22
COMPARISON OF MEAN DIFFERENCE ANALYSIS BETWEEN 0.5mm MARK READINGS AND RADIOGRAPHIC WORKING LENGTH BEFORE CANAL PREPARATION FOR THREE DIFFERENT APEX LOCATORS USING PAIRED t-TEST FOR MB CANALS
50
23
COMPARISON OF MEAN DIFFERENCE ANALYSIS BETWEEN 0.5mm MARK READINGS AND RADIOGRAPHIC WORKING LENGTH BEFORE CANAL PREPARATION FOR THREE DIFFERENT APEX LOCATORS USING PAIRED t-TEST FOR ML CANALS
50
24
COMPARISON OF MEAN DIFFERENCE ANALYSIS BETWEEN 0.5mm MARK READINGS AND RADIOGRAPHIC WORKING LENGTH BEFORE CANAL PREPARATION FOR THREE DIFFERENT APEX LOCATORS USING PAIRED t-TEST FOR DISTAL CANALS
50
25
COMPARISON OF MEAN DIFFERENCE OF 0.5mm MARK READINGS BEFORE CANAL PREPARATION WITHIN THE THREE DIFFERENT APEX LOCATORS (in mm) USING REPEATED MEASURES ANOVA TEST
51
S.NO ABBREVATIONS DESCRIPTIONS
1. CDJ CEMENTODENTINAL JUNCTION
2. AF APICAL FORAMEN
3. AC APICAL CONSTRICTION
4. EPT ELECTRONIC PULP TESTER
5. EALs ELECTRONIC APEX LOCATORS
6. RVG RADIOVISIOGRAPHY
7. NAOCL SODIUM HYPOCHLORITE
8. CHX CHLORHEXIDINE
9. EDTA ETHYLENE DIAMINE TETRACETIC ACID
10. BMP BIOMECHANICAL PREPARATION
11. µm MICROMETER
12. Mm MILLIMETER
13. MB MESIOBUCCAL
15. IOPA INTRAORAL PERIAPICAL RADIOGRAPH
16. PSP PHOTOSTIMULABLE PHOSPHOR
INTRODUCTION
The complete removal of all the pulp tissue, necrotic material and the microorganisms from the root canal system is a mandatory and essential process for the success of root canal treatment1. The root canal preparation and the filling always must terminate within the root canal and must not extend beyond the apex and also no uninstrumented areas should be left inside the root canal system1.
The Glossary of endodontic terminology of the American Association of Endodontists defines the working length as “the distance from a coronal reference point to the point at which canal preparation and obturation must terminate”5. Reference point is the site
on the occlusal or incisal surface from which measurements are made6. The apical
limit is a controversial topic that have been discussed extensively in root canal therapy7.
For decades, this topic just remains as a topic of discussion among the endodontists. So knowledge about the anatomy and histological composition of the apical third of the tooth in determining the ideal apical limit for instrumentation and filling of the root canal is of vital importance7.
Classic concept of the apical root anatomy is based on three anatomic and histologic landmarks in the apical region of the root:
Apical constriction
Pa
ge
2
Apical foramen is an aperture at or near the apex of the root, through which the nerve and blood vessels of the pulp pass, represents the junction of the pulp and periodontal tissue and is not always located in the centre of the root apex. Usually, the apical foramen opens 0.5-1.0mm from the anatomic apex.
Apical portion of the root canal having narrowest diameter is called apical constriction. The location of the apical constriction is considered to be 0.5-1.0 mm short of the anatomical apex. It has otherwise been called minor apical foramen7.
Cementodentinal junction is the region where the dentin and cementum gets united. It is a histological barrier formed and cannot be determined or located clinically or radiographically. It doesnot always coincide with apical constriction and is located 0.5-3.00 mm short of the anatomic apex7.
The European Society of Endodontology recommend that working length determination should be as close as possible to the apical constriction. Postoperative discomfort is generally expected to be a complaint when this area is violated by instruments or filling materials leading to compromised healing7.
Establishing accurate working length and maintaining it throughout the biomechanical preparation is an essential step which aids in the success of root canal treatment2. However, the end-point at which the instrumentation and filling must terminate is still a controversy. It is generally accepted that the root canal preparation be pertained within the sound dentin but never beyond the root apex2.
coronal reference point to the cement-dentinal junction (CDJ) is considered as the ideal working length for the root canal treatment10.
Grove (1930) stated that ‘the proper point to which root canals should be filled is the junction of the dentin and the cementum and that the pulp should be severed at the point of its union with the periodontal membrane’4. The cementodentinal junction
(CDJ) is generally considered the area or a junction where the pulp tissue ends and the periodontal tissues begins4.
The aim of the root canal treatment is to create a potential barrier that is present between the contents of the canal and the apical tissues (Schilder 1967)4.And it is believed and accepted that the preparation as well the obturation be at the apex or even short of the apical constriction4. Working length determination is a preliminary
step where the clinician or the operator gets a chance to decide and locate the level of apical barrier prior to biomechanical preparation. Hence it must be accurate for the entire procedure to end at the right finish point.
Different methods have been used for locating the position of the canal terminus and measuring the working length of root canals. These includes radiographic methods, electronic methods, tactile method and other adjunctive methods8.
The tactile perception is a simple and virtually effective method but is inaccurate in cases with immature apex, excessive curvatures and if the canal is constricted throughout its length11.
Pa
ge
4
Though it has a number of disadvantages like radiation hazard both to the patient and the personnel, image distortion and observer’s bias in radiographic interpretation which may lead to errors11.The introduction of radiovisiography (RVG) involving the
use of sensor instead of conventional X-ray have substantially reduced the radiation dose and duration of endodontic procedures because it effectively eliminated the film processing time. Other advantages includes zoom function that helps in the diagnostic performance by magnifying areas such as the apical zone11.
The first reported use of current to measure the root canal working length was in 1918 by Custer. An investigation by Suzuki in 1942, reported that the electrical resistance between the periodontal ligament and the oral mucosa in-vivo was a constant value of 6.5 kΩ. In 1962, Sunada constructed the first EALs4. He noted a marked increase in
the conductivity of a tooth at the apical foramen when the canal was dry or filled with a non-conductive medium. From then, there was gradual research made about this electric current, which gave first, second, third, fourth generation of apex locators for the past 60 years4. The electronic apex locators are equal or higher in accuracy compared with radiographic methods and this has been shown by various in-vivo, and in-vitro studies4.
Shabahang et al. (1996) found that the Root ZX could locate the apical foramen with a tolerance of +/- 0.5 mm in a vital teeth, in 96.2% cases. Its advantage includes locating the apical constriction rather than the radiographic apex3. They also reduce the treatment time, radiation dose, which may be higher with conventional radiographic measurements3.
cannot be used in patients with, perforations, fractures of root and their accuracy in cases of immature apex, root resorption, hemorrhage and swelling are also questionable3. Thus there is no single best working length determination method or
100% accurate apex locators stated in the literature3.
Knowledge of apical anatomy, prudent use of radiographs and the correct use of an electronic apex locator will assist practitioners to achieve predictable results in determining the working length of any root canal system. But with the advent of electronic apex locators and the operator getting to know their accuracy in locating the working length, radiation exposure could be brought down and minimized.
It is important to know the accuracy of apex locators in determining the working length from a clinical point of view.
AIM AND OBJECTIVES
AIM AND OBJECTIVES
Evaluation and accuracy of three different apex locators in working length estimation of vital first mandibular molars – An invivo study.
AIM:
The aim of this invivo study is to evaluate the accuracy of three different apex locators in identifying the apical constriction in vital mandibular first molars
OBJECTIVES:
To compare the difference in readings between the three different apex locators (iPex II, Apex ID and Root ZX) at “APEX” mark readings with the radiographic observation at “APEX”.
To know the accuracy of the three different apex locators used in this study
REVIEW OF LITERATURE
REVIEW OF LITERATURE
The primary objective of root canal treatment is a thorough cleaning and shaping of the entire root canal system and to seal the root canal system for which determining the working length is mandatory. Anatomically the apical constriction is a logical location for working length, since this is that part of the root canal that coincides with the narrowest diameter of the entire root canal system. Grove in 1931 suggested that the cementodentinal Junction (CDJ) as the location for working length because it represents the transition between pulpal and periodontal tissue 1, 4.
Dummer et al. (1984) mentioned this as the clinically very difficult part to locate, due to its
8
Various techniques are used to determine working length and its maintenance during cleaningand shaping procedure, which is a key factor for a successful endodontic therapy. The tactile perception is the simple and the virtual effective method, but it was said to be inaccurate in root canal systems which was different from that of the routine cases like, immature apex, excessively curved roots, and if the canal is constricted throughout its length20.
This was later followed by the development and production of electronic devices for locating the canal terminus. This is been considered the revolutionizing invention in RCT. There are many advantages which includes comparable or better accuracy compared to conventional radiographs, constant monitoring of working length when the apex locators are being integrated with advanced rotary systems. These all decreases the total radiographs needed and thereby the radiation exposures 18, 19.
There are no studies clearly reporting the superiority of one method over the other. Each have its own advantages and disadvantages22. Czeerw et al. (1995) mentioned that in vivo studies are the best representative of the true accuracy of a given apex locator in function compared to invitro studies.
The cementodentinal junction or the apical constriction as mentioned before have been the narrowest portal of entry of pulpal vasculature from the periapical tissue that have been recommended as an ideal termination for root canal preparation. Hence prior to root canal treatment, it is mandatory we take an undistorted preoperative radiograph to assess the root canal morphology4. The success of any endodontic treatment depends on the apical extend of
10
A brief review of previous studies presented, on the various aspects of apex locators in workinglength determination which helps in understanding and planning the present study.
Martinez-Lozano MA et al. (2001) studied in vitro, the methodological considerations in determining the working length in 28 root canals of twenty mandibular teeth. Here they compared the working length measurements obtained by two radiolographical methods (conventional film and digital radiograph) and apex locator (Apit EM-S3 Locator). Here the measurements were recorded for the apical foramen as reference but measurements within ±0.5mm of the apical foramen were also considered acceptable. It was concluded that none of the techniques were totally satisfactory in establishing the true working length. Electronic method being 67.8% followed by 61.4% for digital radiograph and 50.6% for conventional radiograph 22.
However, their results again insists the fact that Electronic devices does not precisely determine the apical constriction and hence can be used as an adjunct just to reduce the number of radiographs taken 19.
Wrbas KT et al. (2006) conducted an in vivo study for comparing the working length determination with two electronic apex locators (Root ZX and Raypex 5) in twenty single canal teeth. The working length was determined in vivo followed by extraction of the teeth for exvivo analysis. It was found that the minor foramen was located within the limits of ±0.5mm in 75% of cases with Root ZX and in 80% of the cases for Raypex 5. There was no statistical significance between the two electronic apex locators regarding the determination of apical constriction. Hence it was concluded that electronic apex locators is a reliable method for determining working length25.
12
length (AC) needs histological analysis which was the limitation of this study. Hence EALs asan adjunct vital tool20.
Hassanien EE et al. (2008) did an invitro histomorphometric study of the root apex of mandibular premolar teeth. This study attempted to correlate working length measured with electronic (Root ZX) and radiograph methods (0.5mm short of the radiographic apex) to various positions in the apical portion of the root canal. Later the teeth were extracted from both groups and trimmed with fine diamond stones and sof-lex discs for 4-5mm apically to expose the inserted files. This was done with care so as to not disturb the apical anatomy. These results indicated that the use of an electronic device consistently brought the file tip closer to the apical foramen and CDJ while remaining within the confines of the root. Also the narrowest diameter of canal was most commonly located at 1.5mm from apical foramen and begins to start wider as it approaches the apical foramen. On the existence of Apical Constriction in relation to arbitrary points measured at 0.5, 1.0mm and 1.5mm from the apical foramen. It was found to be 1.5mm from the apical foramen and was weak at the most commonly chose 0.5mm distance. So unlike the apical constriction the cementodentinal junctional width was most closely related to 0.5mm point. Hence it was concluded that:
Cementodentinal junction and apical constriction are not same points.
Apical constriction is always coronal to the cementodentinal junction.
ElAyouti A et al. (2009) in their clinical study on consistency of apex locator function in five hundred and seven patients , 1001 root canals (261 women and 246 males; 394 teeth for endodontic treatment and 113 teeth for retreatment) in an age group of 19-62 years (average age: 43.2yrs). The apex locators used were Root ZX, Raypex 5 which was chosen because of their repeatedly proven reliability and precision. Various factors such as tooth type, pulp status (vital/nonvital), treatment type (initial/retreatment), sex and age of the patient were considered with regard to consistency of apex locators checked. It was found that the function of apex locators was consistent in 85% of the patients (429/507). Also teeth with obliterated canals were resulting in inconsistent functioning of the apex locators. Statistically Root ZX was significantly higher than Raypex 5. It was also stated that tooth isolation with rubber dam and drying the pulp chamber are adequate means to obtain a stable electronic working length (EWL) measurement in teeth with metallic restorations. Other factors did not play a role in electronic apex locators readings. Radiographically, 97% of consistent measurements were acceptable14.
14
different, which proves that the minor foramen’s morphology and major foramen’s locationwere both influencing factors in the performance of Electronic Apex Locators5.
Nayale G and Shetty S (2010) compared the conventional radiography and radiovisiography with Raypex 5 Apex Locator for imaging root canal length in 40 single rooted anterior teeth. Here if the file tip was 0.5mm beyond the apex it was designated as “+” and if the file tip was 0.5mm short of the apex it was designated as “-’’. Measurements that are within ±o.5mm of the apical foramen were considered acceptable. The study concluded that electronic method (90%) was more accurate compared to conventional radiograph (72.5%) and RVG (85%). The results were similar to other studies which reported for Raypex 5 performance in vivo 21.
Gomez G et al. (2012) evaluated in vitro the effects of six apex locators (Mini Apex Locator, DentaPort ZX, Novapex, Raypex 5, Root ZX mini, Justy II) on pacemaker function. The pacemaker used was MerlinTM Patient Care System programmer model 3650 (Saint Jude Medical). It was concluded that Electromagnetic Interference (EMI) was only observed when the Electronic Apex Locators were positioned close to the electrode tip or sometimes when they were positioned close to the generator, and the EMI only interfered with pacemaker function a when the lead of the EALs was less than 2cm from the tip of the electrode. No permanent changes was produced in the functioning of pacemaker were detected, which gives a clue that EALs can be used in cardiac patients also 10.
1
6
Mull JP et al. (2012) made an invitro study on the comparison of accuracy of two EALs (Root ZX and Sybron mini) in the presence of various irrigants (1% NaOCl, 2% CHX, 17% EDTA, and saline) for determining the apical constriction. The irrigants were used to check the accuracy of any apex locator which is an electronic device can be easily influenced by the positive and negatively charged particles in the irrigant used. The file was introduced inside the canal until the screen of the apex locators blinked with a flashing bar between APEX and (0.5 reading) and “0.5” blue LED was “on” for Sybron Mini. It was concluded that with 2% CHX in the canals the accuracy of Root ZX aand Sybron Mini was 86.7% and 93.3% respectively, and for 17% EDTA solution this was 81.6% and 75 % respectively. The overall accuracy of measurements within ± 0.5mm of actual length (at minor constriction) by Root ZX and Sybron Mini was 88.3% and 87.5% respectively with 1% NaOCl being highly conductive and 2% CHX low conductive6.
Sindreu FD et al. (2013) in their in vivo study for evaluating the accuracy of iPex and Root ZX electronic apex locators using various irrigants (2.5% NaOCl and 2% CHX) in 32 single rooted human teeth. The file was said to be positioned 0.5mm short of the major apical foramen for Root ZX when the file withdrawn from APEX leads to a flashing bar between the APEX and 1mm. For iPex the display shows a “0.5” mark in LCD screen when the file is withdrawn slowly after the “APEX” signal. It was concluded that there was significant differences between the readings of iPex and Root ZX irrespective of whether 2.5% NaOCl or 2% CHX was used as irrigant. Here iPex (42.8%) was less accurate compared to Root ZX (46.4%) in determining the root working length both for 2.5% NaOCl and 2% CHX8.
18
Milanovoic I et al. (2015) evaluated the accuracy of three Electronic Apex Locators indetermining the apical foramen in multirooted teeth which was a randomized clinical and laboratory study, with a sample size of 30 multirooted teeth which includes premolars and molars. Here the authors evaluated the accuracy of EALs in determining the Apical Foramen rather than Apical Constriction. The working length is estimated in vivo, which is confirmed with ex-vivo extraction measurements. The microscopic measurements after extraction was done by axially grounding the lateral side of the root curvature using a high speed, water-cooled, hand piece diamond bur 018 until the Flexofile became transparent through the thin layer of the residual wet dentine. The last layer of thin dentin is removed with the help of scalpel blade (#15). It was concluded that Raypex 5, Apex NRG and ProPex II was accurate to within ±0.5 mm in 84.6%, 78.6% and 66.7% of cases respectively2.
Lakshmy DS et al. (2016) made a clinical in vivo study on the correlation of working length determined using three EALs ( Root ZX, iPex and Apex ID) with radiographic working length in nineteen maxillary incisors and data analyzed using correlation coefficient test. The apex locators displayed “0.5” on their display screen when the file was withdrawn after reaching the “0.0” reading on display for iPex and Root ZX and as “APEX” for Apex ID. Radiographically the 0.5mm was detected from the working length. The results showed the maximum correlation with radiographic working length for Root ZX (R=0.9881) followed by Apex ID (R=0.9731) and iPex (R=0.9508). But their results did not suggest that EALs are replacing radiographs, but they are ideal tools for complementing radiographic methods of working length determination. Hence can help reducing the number of radiographs taken in this regard18.
20
Cruz ATG et al.(2017) compared the accuracy of two endodontic rotary motors with integratedapex locators (MM Control, Root ZX II) with auto apical reverse function for locating the apical limit in 36 single rooted teeth at apex reading and 0.5mm readings. Here the green labelled “0.5” is said to correspond with the apical constriction. The authors concluded that the EAL function of MM control (77.8%) was less accurate than Root ZX II (83.3%) which resulted in a higher percentage of readings even beyond the apical foramen13.
Oliveira TN et al. (2017) determined the accuracy of five electronic apex locators (Root ZX II, Raypex 6, Apex ID, Propex II, Propex Pixi) in function of different employment protocols. The protocols are:
-1.0, insertion up to 1.0mm below the apical foramen
0.0/-1.0, insertion until the AF and withdrawn 1.0 mm short of the AF;
0.0, insertion until the AF; and
Over / 0.0, insertion until ‘‘over’’ and withdrawal to AF, in eighty human lower premolar teeth in vitro.
21
MATERIALS
ARMAMENTARIUM USED:
Endo-Frost cold spray (Coltene, Whaledent Pvt., Germany)
Local anesthesia – 2% Lignocaine with 1:80,000 adrenaline (LIGNOX 2% A, Warren, Indoco Remedies Ltd.)
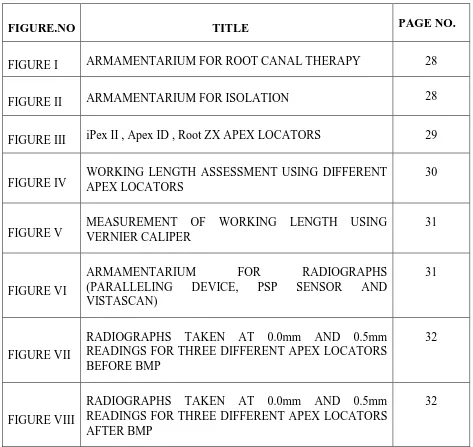
Rubber Dam kit (HYGENIC® Rubber Dam Kit, Coltene, Whaledent Ltd.)
Flat cylindrical bur (SF-11, Mani Co., Japan)
Endo Access bur (Dentsply ENDO-Z bur)
High speed Air Rotor hand piece ( PANA AIR, NSK)
K file (10/15 size, Mani Co., Japan)
6% taper 20 and 25 size RaCe files (FKG Dentaire,, Germany)
NSK ENDOMATE DT Endomotor (Dentsply)
3% Sodium Hypochlorite (Parcan, Septodont Healthcare India Pvt. Ltd.)
Saline [(NS 500ml, sodium chloride 0.9%) Fresenius Kabi, India Pvt. Ltd.)]
X-Ray holder (Paralleling technique, Densmart X Ray film holder, India)
PSP Sensor ( Durr Dental, Germany)
Zinc Oxide Eugenol Sealer (Deepak Enterprise, Mumbai)
Paper points (DiaDent, India)
Ball burnisher (GDC restorative instrument kit)
DEVICES USED :
PSP Scanner ( Vistascan Mini Plus, Durr Dental, Germany)
Three different electronic apex locators:
iPex II (NSK, Tochigi, Japan)
Root ZX (J Morita, MFG Corp., Kyoto, Japan)
Apex ID (Kerr Dental, USA)
METHODOLOGY
METHODOLOGY
This was a single-blinded, block randomized clinical study done in mandibular first molars of 60 patients with the age group of 13 - 60 years which included 36 males and 24 males, who were reported to the Department Of Conservative Dentistry and Endodontics, during the period of October 2017 to January 2018.
Sample size of 60 patients was calculated to be sufficient to detect statistical difference using G Power Version 3.1.9.2 (Universitiät Kiel, Germany). Total number of root canals for the 60 mandibular molars were 180 root canals (1 mesiobuccal, 1 mesiolingual, and 1 distal root canal for 60 teeth).
Institutional ethical committee clearance was obtained for the study (attached as annexure I). The patients were explained about the operative procedure, after which the patients signed in the written informed consent prior to the clinical treatment (attached as annexure II). Either symptomatic or asymptomatic teeth with a diagnosis of irreversible pulpitis were taken for the study.
24
The exclusion criteria included patients who were having any systemic ailments, sincethis would not allow the operator to complete the root canal treatment in a single appointment. Tooth which were having calcifications, periapical radiolucency and evidence of root resorption in the radiograph, the presence of extra roots or root canals, curved roots or root canals. Periodontally compromised teeth was also excluded from the study.
Once when the patient have been chosen properly according to the set inclusion criteria, Local anesthesia with a composition of 2% Lignocaine with 1:80,000 adrenaline (LIGNOX® 2% A, Warren, Indoco Remedies Ltd.) was administered by inferior alveolar nerve block technique. The patient is then clinically checked at the anesthetized region for numbness. The region is later isolated with rubber dam (HYGENIC® Rubber Dam Kit, Coltene, Whaledent Ltd). Access cavity preparation was done using an Endo Access bur (Densply ENDO-Z bur) for access opening using high speed handpiece with copious water irrigation. Pulpal and root canal orifice bleeding was confirmed and the crown of the teeth was adjusted by flattening the occlusal surface with a flat-end cylindrical bur for 2mm [(SF-11 Mani Co., Japan) diameter of the bur head] to achieve a stabilized coronal reference point (all as shown in Figures I and II). A homogenous block randomization was used for the three different apex locators (Figure III): every patient or teeth was allocated using the following six electronic apex locator sequences:
A indicates : iPex II (NSK, Tochigi, Japan)
B indicates : Root ZX (J Morita, MFG Corp., Kyoto, Japan)
C indicates : Apex ID (Kerr Dental, USA)
Each consecutive sequence was used in 60 patients. Electronic apex locator readings were measured by a single operator.
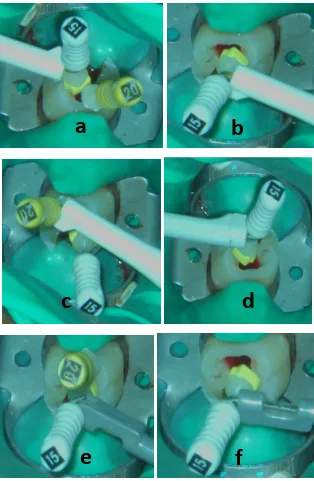
The largest size K file (either 10/15 size) (Mani Co., Japan) was inserted into the root canal till it was able to achieve a snug fit at the root apex as with tactile sensation. Then the buccal clip of the electronic apex locator was applied to the patient’s lip corner and first measurement was taken (as shown in Figure IV).
26
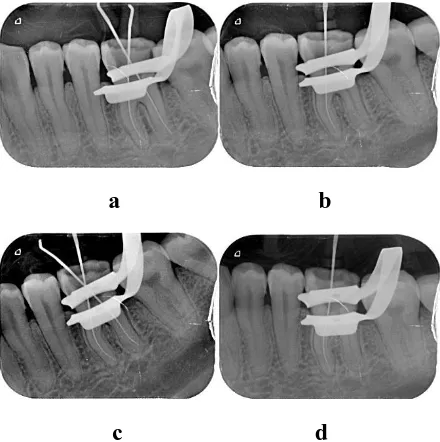
figures VIIa and VIIc) and another with file placed only in the mesiolingual root canal (asshown in figures VIIb and VIId).
Radiographic working length was estimated by subtracting 0.5mm from the length when the file tip was positioned at the root canal exit.
Next, inorder to check the accuracy of electronic apex locators reading at “0.5” mark another same size K file (Mani Co., Japan) was chosen and inserted into the root canal. File insertion was stopped once the display of the electronic apex locator showed “0.5” mark and the rubber stopper in the file was fixed using a cyanoacrylate resin when the display was stable for 5 seconds. The length of the file was measured using electronic digital caliper, and was recorded as “0.5” mark readings of the electronic apex locator display. iPex II (NSK, Tochigi, Japan)electronic apex locators had a display that shows “0.5” mark which was taken as the apical constriction or minor constriction zone. According to the manufacturer recommendations Root ZX and Apex ID devices recommends midway point between “APEX” and “1” mark as the apical constriction or minor diameter zone.
“APEX” and at “0.5” marks were checked as described previously with the help of K size file (Mani Co., Japan) and radiographs (as shown in Figures VIIIa to VIIId). So from each tooth 18 readings were recorded in 60 patients. Hence a total of 1080 readings were obtained.
Root canal obturation was completed in the same appointment using the guttapercha (DiaDent, India) and zinc oxide eugenol sealers (Deepak Enterprises, Mumbai). After completing the procedure, the occlusion was checked and relieved whenever necessary.
[image:47.612.149.468.131.364.2] [image:47.612.202.428.395.662.2]
29
[image:49.612.187.501.150.631.2]
FIGURE IV: WORKING LENGTH ASSESSMENT USING THREE DIFFERENT
a
b
c
d
31
[image:50.612.155.527.129.295.2]
FIGURE VI: ARMAMEMTARIUM FOR RADIOGRAPHY (PARALLELING DEVICE, RVG SENSOR AND VISTA SCAN)
[image:50.612.112.560.408.522.2]a b
[image:51.612.214.434.82.303.2]c d
FIGURE VII: RADIOGRAPHS TAKEN AT “0.0mm and 0.5mm” READINGS FOR THREE DIFFERENT APEX LOCATORS BEFORE BIOMECHANICAL
PREPARATION (BMP)
a b
c d
FIGURE VIII: RADIOGRAPHS TAKEN AT “0.0mm and 0.5mm” READINGS FOR THREE DIFFERENT APEX LOCATORS AFTER BIOMECHANICAL
[image:51.612.214.434.390.611.2]RESULTS
Differences among readings from apex locators and radiographic readings and for each of the devices were compared using the paired t- test. Repeated measures ANOVA with a Greenhouse-Geisser correction and post hoc test using the Bonferroni correction was used to compare the differences within three apex locators.
Descriptive data:
Graph I illustrates the frequency distribution of different age groups in the 60 patients included for the study, 28 (46%), 19(31.67%) , 9 (15%), were belonging to 18-25 years, 26-35 years and 36-40 years groups respectively with 1 (1.67%) in each group of 13-17 years, 41-45 years, 46-50 years and 50-60 years groups.
Graph II represents the frequency distribution of gender with females 24 (40%) and males 36 (60%) patients participating in the study.
Table 1 shows the descriptive data presentation for MB canals of the three different apex locators and radiographs at length “0.0 (APEX)” mark before BMP. Mean length with standard deviation was 19.8mm ± 1.84 for all the four techniques with no difference between the values obtained with apex locators and the radiograph.
34
was found to be 19.37mm ± 1.84 for iPex II, Apex ID and radiographs. It was 19.17mm ±1.83 for Root ZX.
Table 3 exhibits the mean difference in length for MB canals before BMP at 0.0mm (APEX) and the apical constriction mark (0.5mm short of the apex) for all three different apex locators. For iPex II the mean difference was 0.43mm ± 0.07, Root ZX the mean difference was 0.63mm ± 0.02, Apex ID the mean the difference was 0.43mm ± 0.01 Table 4 shows the descriptive data presentation for ML canals of the three different apex locators and radiographs at 0.0 (APEX) mark before BMP. The mean length with standard deviation was found to be 19.8mm ± 1.84 for all the four techniques with no difference between the values obtained with apex locators and the radiograph.
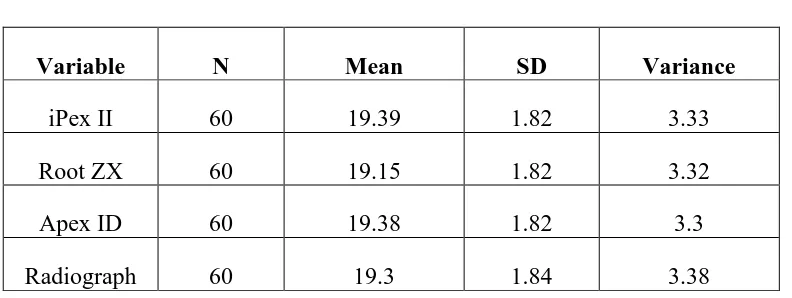
Table 5 depicts the descriptive data presentation for the ML canals of all the three different apex locators at the working length taken at designated apical constriction mark and radiographs at 0.5mm short of the apex before BMP. The mean with standard deviation was found to be 19.39mm ± 1.82 for iPex II, 19.15mm ± 1.82 for Root ZX, 19.38mm ± 1.82 for Apex ID.
radiographs. The mean with standard deviation for Root ZX was 19.67mm ± 1.90. There was no difference between the values obtained with apex locators and the radiograph.
Table 8 depicts the descriptive data presentation for all the three different apex locators at the working length taken at designated apical constriction mark and radiographs at 0.5mm short of the apex before BMP. The mean with standard deviation was found to be 19.22mm ± 1.92 for iPex II and Apex ID, 19.08mm ± 1.90 for Root ZX.
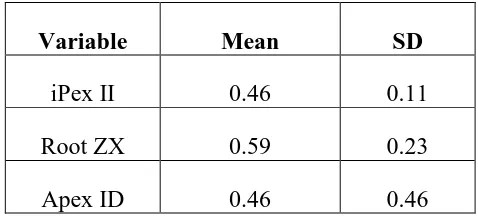
Table 9 explains the mean with standard deviation for the distal canals before BMP at “0.0 (APEX)”mark and the designated apical constriction mark 0.5mm short of the radiograph apex) as 0.46mm ± 0.11 for iPex II and Apex ID, 0.59mm ± 0.23 for Root ZX.
Table 10 depicts the descriptive data presentation for MB canals at “0.0 (APEX)” after BMP and it was found to have the mean with standard deviation for iPex II was 19.8mm ± 18.4. The mean with standard deviation for Root ZX and Apex ID was 19.8mm ± 18.5. Table 11 denotes the descriptive data presentation for MB canals at the designated apical constriction mark for the three different apex locators and apical constriction mark (0.5mm short of the apex)for the radiographs after BMP. The mean with standard deviation was found to be 19.39mm ± 1.85 for iPex II, 19.21mm ± 1.85 for Root ZX, 19.4mm ± 1.82 for Apex ID and 19.3mm ± 1.84 for radiographs.
36
Table 13 depicts the descriptive data presentation for the three different apex locators andradiographs at “0.0 (APEX)” for the ML canals after BMP. The data shows a mean with standard deviation of 19.8mm ± 1.84 for all the three different apex locators and radiographs.
Table 14 denotes the descriptive data presentation for the three different apex locators at designated apical constriction mark and radiograph at the apical constriction mark (0.5mm short of the apex) after BMP for the ML canals. The mean with standard deviation was 19.43mm ± 1.85 for iPex II, 19.23mm ± 1.86 for Root ZX, 19.42 mm ± 1.83 for Apex ID and 19.32mm ± 1.84 for radiograph.
Table 15 exhibits the mean with standard deviation for ML canals after BMP at “0.0 (APEX)” and the apical constriction mark (0.5mm short of the apex) as 0.37mm ± 0.10 for iPex II, 0.57mm ± 0.50 for Root ZX. 0.38mm ± 0.10 for Apex ID and 0.48mm ± 0.00 for radiographs.
Table 16 depicts the descriptive data presentation for distal canals after BMP at “0.0 (APEX)” for radiographs and the three different apex locators. It was found to have a mean difference of 19.7mm ± 1.91 for iPex II and radiograph, 19.72mm ± 1.92 for Root ZX and 19.72 mm ± 1.93 for Apex ID.
Table 18 exhibits the mean difference with standard deviation for distal canals after BMP at “0.0(APEX)” and apical constriction mark (0.5mm short of the apex) was found to be 0.44mm ± 0.11 for iPexII, 0.59mm ± 0.16 for Root ZX, 0.43mm ± 0.11 for Apex ID and 0.49mm ± 0.06 for radiographs.
Paired t test analysis:
Table 19 depicts the comparison of before and after BMP mean values obtained at designated apical constriction mark from three different apex locators for MB canals. The mean with standard deviation was 0.02mm ± 0.21 for iPex II, 0.04mm ± 0.23 for Root ZX, 0.03mm ± 0.22 for Apex ID. The results were not statistically significant.
Table 20 denotes the comparison of apex locators values measured at a designated apical constriction mark before and after BMP for ML canals. The mean with standard deviation was statistically significant with 0.04mm ± 0.27 for iPex II, 0.08mm ± 0.27 for Root ZX, 0.04mm ± 0.23 for Apex ID at p<0.05. In the ML canals, Root ZX readings had the highest difference of 0.08 mm (p<0.05) between the lengths taken before and after BMP.
Table 21 denotes the comparison of three different apex locators values measured at a designated apical constriction mark before and after BMP for distal canals using the paired t-test. The mean difference was 0.04mm ± 0.31 for iPex II, 0.05mm ± 0.29 for Root ZX, 0.07mm ± 0.35 for Apex ID. Mean difference was not statistically significant.
38
Table 22 denotes the comparison of the designated apical constriction mark of the threedifferent apex locators with that of the radiographs at working length 0.5mm short of the apex before BMP for MB canals. The mean difference with standard deviation was 0.07±0.78 for iPex II, 0.13±0.16 for Root ZX and 0.06±0.10 for Apex ID (p< 0.05).
Table 23represents the comparison of the designated apical constriction mark of the three different apex locators with that of the radiographs at working length 0.5mm short of the apex before BMP for ML canals. The mean difference with standard deviation was 0.93mm±0.98 for iPex II, 0.15mm±0.16 for Root ZX and 0.08mm±0.09 for Apex ID. Table 24shows the comparison of the designated apical constriction mark of the three different apex locators with that of the radiographs at working length 0.5mm short of the apex before BMP for distal canals. The mean with standard deviation was 0.04±0.11 for iPex II, 0.09mm±0.24 for Root ZX and 0.04mm ±0.10 for Apex ID.
Tables 22 to 24highlights that for iPex II and Apex ID readings had increased length estimation in all the three canals when compared with radiograph working length but within 0.1mm at p<0.05. It also shows that the Root ZX “0.5” readings were showing the highest difference of 0.13mm, 0.15mm and 0.09mm (P<0.05) for mesiobuccal, mesiolingual and distal canals respectively before BMP.
Repeated measures ANOVA test:
Pag
e
41
GRAPH II : FREQUENCY DISTRIBUTION OF GENDER
1 (1.67%)
28 (46.67%)
19 (31.67 %)
9 (15%)
1 (1.67%) 1(1.67%) 1 (1.67%)
0 5 10 15 20 25 30
13 - 17 18 - 25 26 - 35 36 - 40 41 - 45 46 - 50 50 - 60
A G E ( in ye ars ) Axis Title frequency (%)
24
(40%)
36 (60%)
Gender Frequency (%)
Female Male
42
[image:61.612.100.496.168.312.2]I. Descriptive statistics before and after BMP BEFORE BIOMECHANICAL PREPARATION (BMP):
TABLE 1: DESCRIPTIVE STATISTICS FOR MB CANAL AT “00” in mm:
Variable N Mean SD Variance
iPex II 60 19.8 1.84 3.38
Root ZX 60 19.8 1.84 3.38
Apex ID 60 19.8 1.84 3.38
[image:61.612.102.496.383.521.2]Radiograph 60 19.8 1.84 3.38
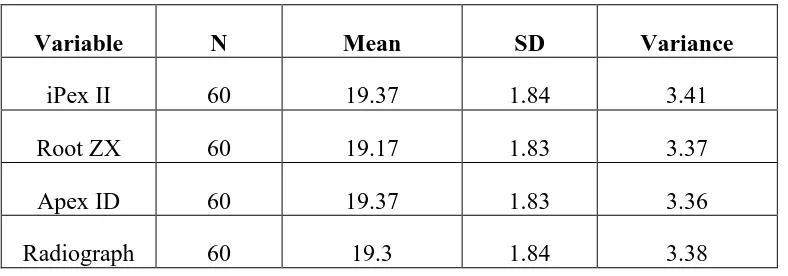
TABLE 2: DESCRIPTIVE STATISTICS FOR MB CANAL AT “0.5” in mm:
Variable N Mean SD Variance
iPex II 60 19.37 1.84 3.41
Root ZX 60 19.17 1.83 3.37
Apex ID 60 19.37 1.83 3.36
Radiograph 60 19.3 1.84 3.38
TABLE 3: MEAN DIFFERENCE FOR MB CANALS BETWEEN “0.0” AND “0.5” in mm
Variable Mean SD
[image:61.612.198.452.609.719.2]Pag
e
43
TABEL 4: DESCRIPTIVE STATISTICS FOR ML CANAL AT “00” in mm:
Variable N Mean SD Variance
iPex II 60 19.8 1.84 3.38
Root ZX 60 19.8 1.84 3.38
Apex ID 60 19.8 1.84 3.4
[image:62.612.101.497.320.469.2]Radiograph 60 19.8 1.84 3.38
TABLE 5: DESCRIPTIVE STATISTICS FOR ML CANAL AT “0.5” in mm:
Variable N Mean SD Variance
iPex II 60 19.39 1.82 3.33
Root ZX 60 19.15 1.82 3.32
Apex ID 60 19.38 1.82 3.3
[image:62.612.213.435.564.672.2]Radiograph 60 19.3 1.84 3.38
TABLE 6: MEAN DIFFERENCE FOR ML CANALS BETWEEN “0.0” AND “0.5” in mm:
Variable Mean SD
iPex II 0.41 0.98
Root ZX 0.65 0.16
44
TABLE 7: DESCRIPTIVE STATISTICS FOR DISTAL CANAL AT “0.0” in mm:
Variable N Mean SD Variance
iPex II 60 19.68 1.91 3.64
Root ZX 60 19.67 1.9 3.61
Apex ID 60 19.68 1.92 3.67
Radiograph 60 19.68 1.91 3.64
TABLE 8: DESCRIPTIVE STATISTICS FOR DISTAL CANAL AT “0.5” in mm:
Variable N Mean SD Variance
iPex II 60 19.22 1.92 3.7
Root ZX 60 19.08 1.9 3.58
Apex ID 60 19.22 1.9 3.61
Radiograph 60 19.18 1.91 3.64
TABLE 9: MEAN DIFFERENCE FOR DISTAL CANALS BETWEEN “0.0” AND “0.5” in mm:
Variable Mean SD
iPex II 0.46 0.11
Root ZX 0.59 0.23
Apex ID 0.46 0.46
[image:63.612.180.419.532.640.2]Pag
e
45
[image:64.612.100.499.138.287.2]AFTER BIOMECHANICAL PREPARATION (BMP):
TABLE 10: DESCRIPTIVE STATISTICS FOR MB CANAL AT “0.0” in mm:
Variable N Mean SD Variance
iPex II 60 19.8 1.84 3.41
Root ZX 60 19.8 1.85 3.45
Apex ID 60 19.8 1.85 3.45
[image:64.612.182.419.584.692.2]Radiograph 60 19.8 1.84 3.41
TABLE 11: DESCRIPTIVE STATISTICS FOR MB CANAL AT “0.5” in mm:
Variable N Mean SD Variance
iPex II 60 19.39 1.85 3.44
Root ZX 60 19.21 1.85 3.44
Apex ID 60 19.4 1.82 3.34
Radiograph 60 19.3 1.84 3.38
TABEL 12: MEAN DIFFERENCE FOR MB CANALS BETWEEN “0.0” AND “0.5” in mm
Variable Mean SD
iPex II 0.41 0.08
Root ZX 0.59 0.13
46
TABLE 13: DESCRIPTIVE STATISTICS FOR ML CANAL AT “0.0” in mm:
Variable N Mean SD Variance
iPex II 60 19.8 1.84 3.38
Root ZX 60 19.8 1.84 3.38
Apex ID 60 19.8 1.84 3.4
Radiograph 60 19.8 1.84 3.38
[image:65.612.103.493.316.453.2]\
TABLE 14: DESCRIPTIVE STATISTICS FOR ML CANAL AT “0.5” in mm:
Variable N Mean SD Variance
iPex II 60 19.43 1.85 3.44
Root ZX 60 19.23 1.86 3.46
Apex ID 60 19.42 1.83 3.35
[image:65.612.182.420.545.652.2]Radiograph 60 19.32 1.84 3.41
TABLE 15: MEAN DIFFERENCE FOR ML CANALS BETWEEN “0.0” AND “0.5” in mm:
Variable Mean SD
iPex II 0.37 0.10
Root ZX 0.57 0.15
Pag
e
[image:66.612.101.497.93.232.2]47
TABLE 16: DESCRIPTIVE STATISTICS FOR DISTAL CANAL AT “0.0” in mm:
Variable N Mean SD Variance
iPex II 60 19.7 1.91 3.67
Root ZX 60 19.72 1.92 3.72
Apex ID 60 19.72 1.93 3.73
[image:66.612.102.499.301.443.2]Radiograph 60 19.7 1.91 3.67
TABLE 17: DESCRIPTIVE STATISTICS FOR DISTAL CANAL AT “05” in mm:
Variable N Mean SD Variance
iPex II 60 19.26 1.92 3.7
Root ZX 60 19.13 1.91 3.65
Apex ID 60 19.29 1.9 3.61
Radiograph 60 19.21 1.92 3.69
TABLE 18: MEAN DIFFERENCE FOR DISTAL CANALS BETWEEN “0.0” AND “0.5” in mm
Variable Mean SD
iPex II 0.45 0.11
Root ZX 0.59 0.16
[image:66.612.156.436.533.640.2]48
[image:67.612.100.542.180.329.2]II. COMPARISON OF MEAN DIFFERENCE ANALYSIS FOR APEX LOCATORS BEFORE AND AFTER BMP AT O.5 USING PAIRED t - TEST
TABLE 19: COMPARISON OF BEFORE AND AFTER AT “0.5” (in mm) FOR MB CANALS
MB CANAL AT “05”
Mean difference SD P value
iPex II 0.02 0.21 0.4090
Root ZX 0.04 0.23 0.1590
Apex ID 0.03 0.22 0.2835
Radiograph 0.02 0.19 0.3214
TABLE 20: COMPARISON OF BEFORE AND AFTER AT “0.5” (in mm) FOR ML CANALS
ML CANAL AT “05”
MEAN DIFFERENCE
SD P value
IPex II 0.04 0.27 0.3585
Root ZX 0.08 0.27 0.0264
Apex ID 0.04 0.23 0.1354
[image:67.612.101.540.407.556.2]Pag
e
[image:68.612.105.515.113.286.2]49
TABLE 21: COMPARISON OF BEFORE AND AFTER AT “0.5” (in mm) FOR DISTAL CANALS:
DIST CANAL AT “05”
MEAN DIFFERENCE
SD P value
iPex II 0.04 0.32 0.2776
Root ZX 0.05 0.29 0.2269
Apex ID 0.07 0.35 0.1564
50
III. COMPARISON OF MEAN DIFFERENCE ANALYSIS BETWEEN “0.5” MARK READINGS AND RADIOGRAPH WORKING LENGTH BEFORE CANAL PREPARATION FOR THREE DIFFERENT APEX LOCATORS USING
PAIRED t-TEST.
TABLE 22: COMPARISON OF THE MEAN DIFFERENCE BETWEEN “0.5” MARK READINGS AND RADIOGRAPH FOR MESIOBUCCAL CANALS (in
mm):
Apex locators Mean difference SD P value
iPex II 0.07 0.78 0.00
Root ZX 0.13 0.16 0.00
Apex ID 0.06 0.10 0.00
TABLE 23: COMPARISON OF THE MEAN DIFFERENCE BETWEEN “0.5” MARK READINGS AND RADIOGRAPH FOR MESIOLINGUAL CANALS (in mm):
Apex locators Mean difference SD P value
iPex II 0.09 0.98 0.00
Root ZX 0.15 0.16 0.00
Apex ID 0.08 0.09 0.00
TABLE 24: COMPARISON OF THE MEAN DIFFERENCE BETWEEN “0.5” MARK READINGS AND RADIOGRAPH FOR DISTAL CANALS (in mm):
Apex locators Mean difference SD P value
iPex II 0.04 0.11 0.00
[image:69.612.146.497.431.539.2]Pag
e
51
[image:70.612.90.533.229.609.2]IV.COMPARISON BEFORE BMP BETWEEN THE THREE APEX LOCATORS AT DESIGNATED MARK (0.5 mm) USING REPEATED ANOVA MEASURES TEST
TABLE 25: COMPARISON OF MEAN DIFFERENCE OF “0.5” MARK READINGS BEFORE CANAL PREPARATION WITHIN THREE DIFFERENT APEX LOCATORS
(in mm): (REPEATED MEASURES ANOVA TEST)
Apex locators
i j
MB canal readings at 0.5 designated mark(in mm)
ML canal reading at 0.5 designated mark (in mm)
Distal canal reading at 0.5 designated mark (in mm)
Mean diff.
Std.
error
Sig.b Mean
diff.
Std.
error
Sig.b Mean
diff. Std. error Sig.b 1 2 3 0.200* 0.002 0.025 0.015 0.000 1.000 0.243* 0.0133 0.022 0.011 0.000 0.230 0.137* -0.002* 0.033 0.018 0.000 0.927 2 1 3 -0.200* -0.198* 0.025 0.023 0.000 0.000 -0.243* -0.230* 0.022 0.022 0.000 0.000 -0.137* -0.138* 0.033 0.031 0.000 0.000 3 1 2 -0.002 0.198* 0.015 0.023 1.000 0.000 -0.013 0.230* 0.011 0.022 0.231 0.000 0.002 0.138* 0.018 0.031 0.927 0.000
52
Based on estimated marginal means
DISCUSSION
The objective of this study was to evaluate the accuracy of three different electronic apex locators (EALs) Root ZX, Apex ID and iPex II in determining the apex as well as apical constriction of mandibular first molars compared to radiographs. Clinically in this study, all the three different apex locators properly functioned 98% of the cases which in a clinical practice translates to 2 in 100 patients with regard to dysfunction of the apex locators.
Historically, radiographs are considered one of the primary means for determining the working length though there are inherent limitations, of being two-dimensional images of a three-dimensional object1. An in-vivo study by Milanovoic et al. has shown that the “APEX” readings of the three different apex locators (Raypex 5, APEX NRG, Propex II) had a high correlation with the observations of the exit of canals (apical foramen)17. In this study it was considered that apical foramen is as an appropriate termination17. Anantomic working length when obtained radiographically is obtained by presenting the tip of the file 1.0mm short of the radiographic apex rather than at the end of the canal i.e., apical foramen17.
54
concluded over instrumentation of the canal must be a common and unnoticed occurrenceduring root canal therapy25.
There is a general agreement in the endo community that working length to be located at the apical constriction. Hassanien et al. (2008) detected the apical constriction at an average distance of 1.2mm from the apical foramen23. Hence this study was also done in the light of these new observations to determine the efficacy of all the three different EALs in location the apical foramen as well as apical constriction.
In the present study, multirooted mandibular first molar was selected for the assessment, since these type of teeth are more challenging compared to single rooted teeth, in relation to curvatures, apical deltas, lateral anastomoses etc5... Straight and patent canals with vital pulp were selected. Radiograph exposure was made with the help of paralleling technique in-order to minimize the radiographic distortion. Block randomizations were done for the three different apex locators so that there is even distribution of apex locator usage in all the molar teeth without any bias.
Initially, the readings from “APEX” mark were assessed. In this study, more than 98% of the “APEX” readings correlated with the radiographic exit of the canal for all the three apex locators used which was in concurrence with an in-vivo study by Milanovoic et al. in multirooted molar teeth using three different apex locators (Raypex 5, APEX NRG, Propex II)17. Another in-vivo study in a single rooted teeth reported that, when the “APEX” marks readings of three difference apex locators (Dentaport ZX, Raypex 5, PropexII) compared for locating major foramen within ±0.5mm had an accuracy percentage of more than 98% in agreement with the results of this study26. An
and Apex ID showed that, using these devices at “APEX” mark readings was able to achieve lowest mean error (0.1mm-0.23mm) and highest precision (83.93%) compared to other screen markings and this observation was also in concurrence with the results of this present study24.
Recent investigations with micro-CT evaluation reveal that there was no significant difference between the two apex locators (Root ZX and Apex ID) in determining the “APEX” readings with that of the CT measurements12. This observation was also similar
with that of this study. Hence all the apex locators regardless of the operating mechanisms, were correctly interpreting the apical foramen location24.
It has been shown in few studies that, the electronic withdrawals did not provide any increase in precision regarding the position of the apical constriction (Olieviera et al.)24. This is explained by the fact that when the advancing instrument is withdrawn, it will no longer be properly adjusted to the canal walls, leading to a cause of impairment in its interpretation of the capacitance factor of the impedance determined by the device. However, these findings did not corroborate with those of Piasecki et al. who observed a similar result between the electronic withdrawal and the one performed considering the electronic root canal length measurement performed at the apical foramen24.
56
(designated apical constriction i.e., “0.5” mark) was used, it has been reported a highdegree of accuracy for identification of the apical constriction within ±0.5mm25. This
study has its results similar to the present study which observed that, apex locators “0.5” readings for the same tooth were not same. Another in-vivo study by Welk et al. showed that Root ZX was 95.7% times accurate in determining the minor constriction in single rooted teeth26. Saxena et al. in an ex-vivo study with single rooted permanent teeth using iPex II concluded that, this device was able to locate the minor constriction 86.66% of the times27.
A comparative in-vivo study by Lekshmy Devi et al. to determine working length using three different apex locators showed that Apex ID “0.5” mark readings had a correlation with radiographic working length estimation of 0.973118.Comparison of “0.5” mark readings of the three different apex locators for all three canals in the present study reveals that, the readings from Root ZX apex locators varied significantly (P< 0.05) from iPex II and Apex ID devices; whilst the readings from iPex II and Apex ID apex locators matched each other9. Wrbas et al observed that, different apex locators’ “0.5” mark
readings for the same tooth were not in agreement; this is in accordance to the results of the present study.
because of the type of the tooth evaluated in the study mentioned. There will be decreased canal morphology variation in the apical third and curvature of single rooted teeth than compared to the multirooted teeth5.
Stereomicroscopic evaluation of mandibular single rooted premolar root apex by Hassanien et al. depicts that, apical constriction was always coronal to the dentinocemental junction and the mean distance of dentinocemental junction and the apical constriction was 0.3 and 1.20 mm respectively23. This study also observes, that
file tip was closer to the dentinocemental junction than to apical constriction when used with the apex locators23.Various micro CT studies have also been done to explore the root canal anatomy in the apical region11, 12, and 32. A recent micro CT study of the root canal
anatomy in both single and multi-rooted teeth root apex reveals that, the mean distance of the apical constriction from the apical foramen measured by apex locators was 0.21 mm where the most apical position of the constriction was taken as a reference point which is in correlation with the study results of Hassanien et al23, 32.Keeping in perspective of these micro CT findings the results of the current study could be extrapolated that, the “0.5” mark readings of iPex II and Apex ID devices might be closer to most apical portion of the apical constriction and Root ZX readings closer to coronal portion of the apical constriction. But this observation needs to be proved with the help of micro-CT studies in future.
58
third generation apex locators (where alternate current based on 2 or 3 frequencies formeasurement of working length) concluded that with the evolution in the fabrication of apex locators with microprocessors and a higher ability of mathematic calculation and algorithms, it is explained that a higher success rate on measurements of the working length without much distortions can be obtained 34.
There were only negligible differences between the readings obtained before and after BMP for “0.5” mark. The present study of the three different apex locators showed the “APEX” mark readings to be stable for and coincide with the radiographs. The highest change in length (0.8 mm) after canal preparation was observed for Root ZX device in mesiolingual canal. An average 0.1mm increase in length estimation was seen after canal preparation. But these change in length estimation could be considered clinically negligible as most endodontic rulers can measure to a precision of only 0.5 mm13.
Another study by Vasconcelos et al. revealed that the RCL of the teeth presented significant reduction in extent during the chemical-mechanical preparation showing the highest variation (0.6 mm), with the extent of specimens reduced by up to 1.75 mm, making it necessary to perform electronic measurements not only after cervical preparation but also as soon as instrumentation has been completed 33. There was this
SUMMARY
Page
60
SUMMARY
The purpose of this invivo study is to compare the three different apex locators in determining the working length of mandibular first molar teeth with irreversible pulpitis in comparison with an intraoral periapical radiograph.
CONCLUSIONS
CONCLUSIONS
This clinical in-vivo study was done to assess the clinical accuracy of three different apex locators viz., iPex II, Root ZX and Apex ID before and after canal preparations in mandibular first molar with irreversible pulpitis at “APEX” and “0.5” marks.
Within the limitations of this study following conclusions can be deduced:
This study finds only negligible difference in readings between the three different apex locators at “APEX” mark readings and coincide with radiographic observation. This point was stable both before and after canal preparations.
Another finding was that “0.5” (designated apical constriction) mark readings of the three different apex locators shows that Root ZX was significantly (p < 0.05) differing from that of iPex II and Apex ID. “0.5” mark readings (designated apical constriction) using three different apex locators located the apical constriction at varied points and there is no agreement among the different devices in this study.
62
canal preparation in-order to terminate the root canal filling at minor or apicalconstriction.
REFERENCES
1. Vieyra JP and Acosta J. Comparison of working length determination with radiographs and four electronic apex locators. Int Endod J 2011; 44: 510–518. 2. Cianconi L, Angotti V, Felici R, Conte G, Mancini M. Accuracy of three electronic apex locators compared with digital radiography: An ex vivo study. J Endod 2010; 36: 2003-2007.
3. Caliskan MK, Kaval ME, Tekin U. Clinical accuracy of two electronic apex locatorsin teeth with large periapical lesions. Int Endod 2014; 47: 920–925. 4. Gordon MPJ and Chandler NP. Electronic apex locators – Review. Int Endod
J 2004; 37: 425–437.
5. Ding J,Gutmann JL, Fan B, Lu Y, Chen H.Investigation of apex locators and related morphological factors. J Endod 2010; 36:1399-1403.
6. Mull JP, Manjunath V, Manjunath MK. Comparison of accuracy of two electronic apex locators in the presence of various irrigants: An in vitro study. J Conserv Dent 2012; 15: 178–182
7. Puri N, Chadha R, Kumar P, Puri K.An in vitro comparison of root canal length determination by DentaPort ZX and iPex apex locators. J Conserv Dent 2013; 16: 555–558.
9. Duran-Sindreu F, Gomes S, Stober E, Mercade M, Jane L, Roig M. In vivo accuracy of three electronic root canal length measurement devices: Dentaport ZX, Raypex 5 and ProPex II. Int Endod J 2012; 45: 552-556. 10.Gomez, Duran-Sindreu F, Clemente FJ, Garofalo RR, G