City, University of London Institutional Repository
Citation
: Sethu, S., Seelam, B., Nukella, P. B., Modi, A., Ali, R. and Keay, L. (2018).
Prevalence of refractive errors in children in India: a systematic review. Clinical and Experimental Optometry, 101(4), pp. 495-503. doi: 10.1111/cxo.12689This is the accepted version of the paper.
This version of the publication may differ from the final published
version.
Permanent repository link:
http://openaccess.city.ac.uk/20118/Link to published version
: http://dx.doi.org/10.1111/cxo.12689
Copyright and reuse:
City Research Online aims to make research
outputs of City, University of London available to a wider audience.
Copyright and Moral Rights remain with the author(s) and/or copyright
holders. URLs from City Research Online may be freely distributed and
linked to.
City Research Online: http://openaccess.city.ac.uk/ [email protected]
REVIEW
Prevalence of Refractive errors in children in India – A systematic review. *Sethu Sheeladevi PhD
Ϯ
Bharani Seelam BSc Optom,
§
Phanindra B NukellaPhD,
¶
Aditi ModiBDS, M.Phil,
¶
Rahul Ali MD, MPH
Ϯ
Lisa KeayPhD
*School of Health Sciences, City, University of London
Ϯ The George Institute for Global Health, India
§ VISION 2020: The Right to Sight-INDIA
¶ Orbis International, India
Running Title: Prevalence of refractive errors in children
Background, Uncorrected refractive error is an avoidable cause of visual impairment which affects children in India. The objective of this review is to estimate the prevalence of
refractive errors in children ≤ 15 years.
Methods, The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed in this review. A detailed literature search was
performed to include all population and school-based studies published from India from the year 1990 using the Cochrane Library, Medline and Embase up to Jan 2017. The quality of the included studies were assessed based on a critical appraisal tool developed for systematic reviews of prevalence studies.
Results, Four population and eight school based studies were included. The overall
prevalence of refractive error per 100 children was 8.0 (CI: 7.4 – 8.1) and in schools it was 10.8 (CI: 10.5 – 11.2). The population based prevalence of myopia, hyperopia (≥+2.0D) and astigmatism was 5.3%, 4.0% and 5.4% respectively. Combined Refractive error and myopia alone were higher in urban areas compared to rural areas (OR: 2.27(CI: 2.09 – 2.45) and (OR: 2.12(CI: 1.79 – 2.50) respectively. The prevalence of combined refractive errors and myopia alone in schools was higher among girls than boys (OR: 1.2(CI: 1.1 – 1.3) and (OR: 1.1(CI: 1.1 – 1.2) respectively. However, hyperopia was more prevalent among boys than girls in schools (OR: 2.1(CI: 1.8 – 2.4).
Uncorrected Refractive error (URE) is the most common cause of visual impairment around the world 1 and in children URE and its consequences have a profound effect on their overall development most importantly on educational and psychosocial development 2, 3.
In India, varied prevalence rates of myopia and hyperopia have been reported in children 4-6. These studies have confirmed that many children are in need of spectacle correction and in rural India around 86% of children presented without correction for RE 4.
Children often do not complain of defective vision and may not even be aware of their problem. They may adjust to poor vision by strategies such as changing position in the classroom and moving objects closer and tending to avoid tasks that require more visual concentration. It is recommended to screen children for early detection and intervention to provide them with the best opportunities to learn and develop 7.
In India as of January 2017,( http://www.indiaonlinepages.com/population/india-current-population.html) there are 365 million children aged < 15 years (29% of the population are children aged less than 15 years (National Health Profile 2015, published by Government of India), and providing vision screening for all children is a daunting task. The availability of eye care services in the country varies between and within regions. Given these disparities, school based vision screening services are considered cost effective in detecting correctable causes of decreased vision8 and as part of the National Program for Control of Blindness, school vision screening is widely practised at present in the country 9. Hence, it is necessary to estimate the prevalence both at the community and at the school level to aid planning and implementation of refractive error services in children.
Region specific prevalence estimates are necessary for policy decisions and evidence based allocation of resources. However, cost and logistics limits make population based studies from each region prohibitive. In such a scenario, a systematic review provides pooled
‘METHODS’ This review included data collected in India and published between January 1, 1990 and January 1, 2017. OVID, Embase, EbscoHost and Cochrane library databases were searched using a strategy with terms based on medical subject headings using (MeSH) in the title and abstract. Broad search strategy combined terms related to epidemiology (including MeSH search using exp prevalence * and exp epidemiology * and keyword search using the words prevalence, epidemiology, incidence, rates and proportions), terms related to disease (including MeSH search using exp refractive error *, exp myopia*, exp hypermetropia*, exp astigmatism*, exp presbyopia*and keyword search using the term refractive error, myopia, hypermetropia and astigmatism ), and terms related to population (including MeSH search using exp India * and keyword search using the words India) see Appendix for full search strategy . Also, manual search was done based on the reference lists of the eligible articles and reviews for any additional articles. A manual search was conducted for all age groups and this report includes only data related to refractive errors in children aged less than 15 years. And an additional search was conducted to include any studies which reported the prevalence of refractive errors among school going children in India. The systematic review met the criteria outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 guidelines. The protocol for this review was not published.
Inclusion and exclusion criteria:
All epidemiological studies that reported prevalence of any refractive errors from an Indian population were considered for full text review. Studies that used only qualitative methods, all review papers and all those studies published only as an abstract or presented in
conferences and duplicate publications from the same study were excluded.
technique, screening tools, cycloplegia, screening personnel, location (urban or rural), total sample size, number of children with refractive error and number of children with different types of refractive error.
For analysis both MetaXL and Open Meta (Analyst)
(http://www.cebm.brown.edu/openmeta/) were used to calculate the pooled estimate of refractive errors in children which is the primary aim of this review. For this calculation, Freeman-Tukey double arcsine transformation 11 was used with a random effects model, separately for population and school based data .
As part of the secondary aim of this review, sub-group analysis was performed to estimate the pooled prevalence by type of refractive errors (myopia, hyperopia and astigmatism), by gender and geographic location (rural versus urban). We calculated Cochran Q statistic testing for heterogeneity across studies and reported I squared 12, 13.
‘RESULTS’ Of 178 potentially relevant titles and abstracts, 26 full text articles were considered eligible. The review strategy is summarised in Figure 1 and the details of 14 excluded studies with the reasons are presented as Table 1. Twelve studies, including four population based cross sectional studies 4-6, 14 and eight school based studies were included in this review 15-22.
Of the four population based studies, three were from South India 4, 6, 14 and one from North India 5. All the eight school based studies were spread across seven different states.
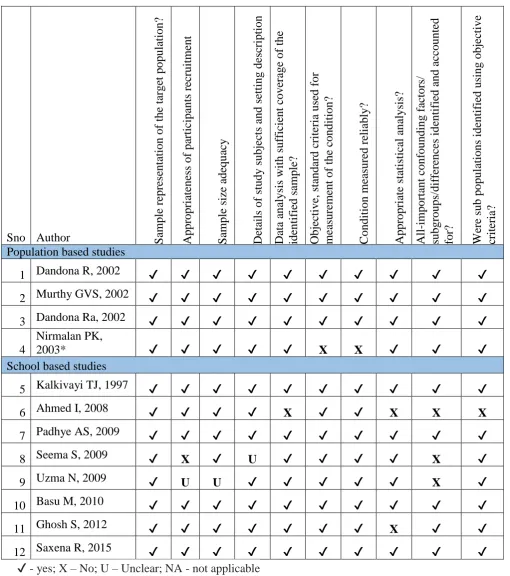
However, sample size, age group and the definition of refractive errors varied significantly in the included studies. The characteristics of population based and school based studies are presented in Table 2 and 3 respectively and the results of the quality assessment summarised in Table 4. Publication bias was assessed and the distribution of studies in population and school based plots were asymmetrical (LFK index: 2.31: Major asymmetry and LFK index: 123: Minor asymmetry respectively). Very high heterogeneity was found between the included studies reporting prevalence of refractive errors in children (Cochran’s Q-test, p<0.001; I2= 100%; see Figure 2 & 3).
and myopia alone was higher in urban areas compared to rural areas (OR: 2.27 (CI: 2.09 – 2.45) and (OR: 2.12(CI: 1.79 – 2.50) respectively.
The prevalence of combined refractive errors, myopia and hyperopia was higher in urban schools compared to schools in rural areas (OR: 4.9, (CI: 4.46 – 5.507), (OR: 3.4 (CI: 3.03 – 3.92) and (OR: 14.1(CI: 10.6 – 18.9) respectively. The prevalence of combined refractive errors and myopia alone in schools was higher among girls than boys (OR: 1.2(CI: 1.1 – 1.3) and (OR: 1.1(CI: 1.1 – 1.2) respectively however, hyperopia was more prevalent among boys compared to girls in schools (OR: 2.1(CI: 1.8 – 2.4). The prevalence of refractive errors in various sub groups is presented in Table 5 & 6.
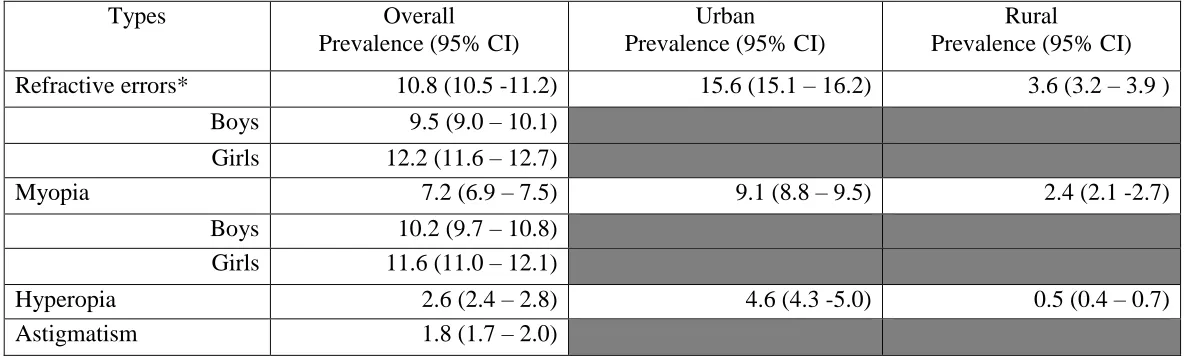
‘DISCUSSION’ The overall population based estimates of prevalence of refractive errors, myopia, hyperopia (≥ +2.0D) and astigmatism in children were 8.0%, 5.3%, 4.0% and 5.4% respectively, while the corresponding figures from the school based data were 10.8%, 7.2%, 2.6% and 1.8%.
The Odds of having combined refractive errors and myopia alone was twice as high among urban children compared to rural children. This is similar to earlier findings 23on the epidemiology of RE in other parts of the world and this meta-analysis provides further support for this pattern across India. This may be due to the increased educational demands leading to more near vision activities 20. Also, the greater use of electronic gadgets such as tablets, smart phones and computer games may be the contributing factor for increased prevalence rates in urban areas. Though near work is considered as a risk factor for increased myopia, the association between myopia and near work remains elusive 24.
Comparison between the included studies was complicated by the inherent variability in the methodology adopted in each study resulting in significant heterogeneity. The Refractive Error in School Children (RESC) protocol has been considered as a standard methodology for estimating refractive errors in children 25. However, in India two population based studies 4, 5 adopted the RESC protocol but unfortunately the age group enrolled in these two studies were different making it difficult for direct comparison. Adoption of standard methods including RE definition, standardised age group sampling across studies will enable comparisons between studies.
way of assessing ametropias in children 26 and 11 out of 12 included studies met these criteria. Moving forward, it will be key to ensure that cycloplegia is integral to any studies of refractive error in children in India.
School based data showed that, myopia was higher among girls than boys, perhaps reflecting different environmental factors as the tendency of girls to spend a greater number of hours reading and writing at home and significantly lesser hours outdoors as compared to boys 20. Estimating prevalence by gender was not possible from the population based studies due to inadequate information.
Considering the progressive nature of myopia in young children and the risk associated with high levels of myopia, vision screening programs should include follow up services.
Furthermore, eye health messages highlighting and encouraging children to increase outdoor activities may reduce this risk factor for myopia in Indian children 27.
The range of refractive errors is quite high in very young children, particularly hyperopia. It is unclear whether correction of refractive error affects emmetropisation 28. One population based study included in the present review used a cut off of ≥ +0.5D as hyperopia, which escalated the overall prevalence of refractive error in children 6. Most of these children will not require spectacle correction, hence, for estimating the spectacle need a clinically
significant level hyperopia of ≥+2.0 D cut off was used and is recommended for future studies of prevalence. However symptoms and binocular visual function should also be taken into consideration and there are clear guidelines available for prescribing spectacles in different age groups in children 29. Studies in other settings have demonstrated a link between hyperopia and lower educational attainment 30.
Although it is ideal to screen every single child for refractive errors, considering the number of children to be screened and the given resource constraints, a population based screening for childhood refractive errors may not be feasible in India. A pragmatic approach is
In India, as part of the National Program for Control of Blindness, School Eye Health Screening Program has been in place for more than two decades 9. Millions of children have been screened every year and this program is found to be cost effective in screening for refractive errors in children in India with volunteer support from school teachers reducing associated costs 8.
To optimise the benefit from the existing school eye health program, a few changes are suggested. Standard protocols across the program would increase comparability of data across the country. Comparable data are important to assess the impact of the program and to develop strategies aimed at increasing screening coverage and compliance. Also, this review could not determine the appropriate age for vision screening in children and suggests that future studies should determine this factor and develop strategies for achieving higher screening coverage in schools 32, 33.
To our knowledge this is the first systematic review on prevalence of refractive errors in children in India. Most of the population based estimates are from the southern region and this limits extrapolation to the entire country as the disparities within the country are well known, with some of the states in the Southern and Western regions having better health indices compared to the Northern region 34. Also, these estimates are based on data published from 1997 to 2015 and therefore quite old. Since myopia is an emerging public health issue contemporary data are required for reliable estimation across the country. Providing
refractive services for children imposes major logistical challenges considering that the population of India is the second highest population in the world, with 1.34 billion people (http://www.indiaonlinepages.com/population/india-current-population.html) and 29% of the population are children aged less than 15 years (National Health Profile 2015, published by Government of India). The population based estimates on refractive error in children in India indicate that 33.4 million children in the country are in need of spectacles to correct their vision. Similarly, if we screen 100 school students aged more than 7 years, 14 of them are likely to need spectacles, of which about 70% would require correction for myopia and follow-up screening on an annual basis, and correction if necessary.
country to deal with and massive efforts are required to scale up the refractive error services in children.
Based on this review, there is a need for up to date population based data on the prevalence of refractive errors in children with greater representation across India. Also, it is important that future studies adopt a standard protocol such as RESC and report data on different types of RE with clinically meaningful cut off points. For example, along with the data on overall RE in children, it is recommended to report separately on clinically significant RE with ≥-1.0D and ≥+2.0D for calculating the exact need for spectacle correction.
The major limitation of this review was the data included in this review are out of date. Also, the variation in refractive error definition, particularly in reporting hyperopia, contributing to the wide range of estimated prevalence. Moreover, few school based studies in this review included relatively low amounts of RE eg: +0.50D which is not clinically significant for spectacle correction in most children.
APPENDIX
Complete Search strategy used in EBSCOHOST:
S10 S3 AND S6 AND S9 Search modes - Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S9 S7 OR S8 Search modes -
Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S8
AB prevalen* OR AB incidence OR AB epidemiology
Search modes - Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S7
(MH "Prevalence") OR (MH "Incidence") OR (MH "Epidemiology")
Search modes - Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S6 S4 OR S5 Search modes -
Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S5 AB India OR AB Indian Search modes - Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S4 (MH "India") Search modes - Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S3 S1 OR S2 Search modes -
Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
S2
AB "refractive errors" OR AB myopia OR AB
hypermetropia OR AB astigmatism OR AB presbyopia
Search modes - Boolean/Phrase
Interface - EBSCOhost Research Databases
Search Screen - Advanced Search Database - CINAHL Plus with Full Text
REFERENCES
1. Dandona L, Dandona R. Estimation of global visual impairment due to uncorrected refractive error. Bulletin of the World Health Organization. 2008;86(8):B-C; author reply C.
2. Pratt C, Bryant P. Young children understanding that looking leads to knowing (so long as they are looking into a single barrel). Child development. 1990;61(4):973-82.
3. Packwood EA, Cruz OA, Rychwalski PJ et al. The psychosocial effects of amblyopia study. J aapos. 1999;3(1):15-7.
4. Dandona R, Dandona L, Srinivas M, Sahare P, Narsaiah S, Muñoz SR, et al. Refractive error in children in a rural population in India. Investigative Ophthalmology & Visual Science.
2002;43(3):615-22.
5. Murthy GVS, Gupta SK, Ellwein LB, Muñoz SR, Pokharel GP, Sanga L, et al. Refractive error in children in an urban population in New Delhi. Investigative Ophthalmology & Visual Science. 2002;43(3):623-31.
6. Dandona R, Dandona L, Srinivas M et al. Population-based assessment of refractive error in India: the Andhra Pradesh eye disease study. Clinical & Experimental Ophthalmology.
2002;30(2):84-93.
7. Baltussen R, Naus J, Limburg H. Cost-effectiveness of screening and correcting refractive errors in school children in Africa, Asia, America and Europe. Health policy (Amsterdam,
Netherlands). 2009;89(2):201-15.
8. Limburg H, Vaidyanathan K, Dalal HP. Cost-effective screening of schoolchildren for refractive errors. World Health Forum. 1995;16(2):173-8.
9. Jose R, Sachdeva S. School eye screening and the National Program for Control of Blindness. Indian Pediatrics. 2009;46(3):205-8.
10. Munn Z, Moola S, Riitano D et al. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. 2014;3(3):123-8. 11. Barendregt JJ, Doi SA, Lee YY et al. Meta-analysis of prevalence. J Epidemiol Community Health. 2013;67(11):974-8.
12. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539-58.
13. Higgins JP, Thompson SG, Deeks JJ et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-60.
14. Nirmalan PK, Vijayalakshmi P, Sheeladevi S et al. The Kariapatti pediatric eye evaluation project: baseline ophthalmic data of children aged 15 years or younger in Southern India. American journal of ophthalmology. 2003;136(4):703-9.
15. Ahmed I, Mian S, Mudasir S et al. Prevalence of myopia in students of Srinagar city of Kashmir, India. International Journal Of Health Sciences. 2008;2(1):77-81.
16. Basu M, Das P, Pal R et al. Spectrum of visual impairment among urban female school students of Surat. Indian Journal Of Ophthalmology. 2011;59(6):475-9.
17. Ghosh S, Mukhopadhyay U, Maji D et al. Visual impairment in urban school children of low-income families in Kolkata, India. Indian Journal Of Public Health. 2012;56(2):163-7.
18. Kalikivayi V, Naduvilath TJ, Bansal AK et al. Visual impairment in school children in southern India. Indian journal of ophthalmology. 1997;45(2):129-34.
19. Padhye AS, Khandekar R, Dharmadhikari S et al. Prevalence of uncorrected refractive error and other eye problems among urban and rural school children. Middle East African Journal Of Ophthalmology. 2009;16(2):69-74.
20. Saxena R, Vashist P, Tandon R et al. Prevalence of myopia and its risk factors in urban school children in Delhi: the North India Myopia Study (NIM Study). Plos One.
2015;10(2):e0117349-e.
21. Seema S, Vashisht BM, Meenakshi K et al. Magnitude of refractive errors among school children in a rural block of Haryana. Internet Journal of Epidemiology. 2009;6(2):6p-p 1p.
23. Wu PC, Huang HM, Yu HJ et al. Epidemiology of Myopia. Asia-Pacific journal of ophthalmology (Philadelphia, Pa). 2016;5(6):386-93.
24. Ramamurthy D, Lin Chua SY, Saw SM. A review of environmental risk factors for myopia during early life, childhood and adolescence. Clin Exp Optom. 2015;98(6):497-506.
25. Negrel AD, Maul E, Pokharel GP et al. Refractive Error Study in Children: sampling and measurement methods for a multi-country survey. Am J Ophthalmol. 2000;129(4):421-6.
26. Manny RE, Fern KD, Zervas HJ et al. 1% Cyclopentolate hydrochloride: another look at the time course of cycloplegia using an objective measure of the accommodative response. Optometry and vision science. 1993;70(8):651-65.
27. Rose KA, Morgan IG, Ip J et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279-85.
28. Mutti DO, Mitchell GL, Jones LA et al. Accommodation, acuity, and their relationship to emmetropization in infants. Optometry and vision science. 2009;86(6):666-76.
29. Leat SJ. To prescribe or not to prescribe? Guidelines for spectacle prescribing in infants and children. Clin Exp Optom. 2011;94(6):514-27.
30. Williams WR, Latif AH, Hannington L et al. Hyperopia and educational attainment in a primary school cohort. Archives of disease in childhood. 2005;90(2):150-3.
31. WHO. Elimination of avoidable visual disability due to refractive error. Report of an Informal Planning Meeting.6-10.
32. Limburg H, Kansara HT, d'Souza S. Results of school eye screening of 5.4 million children in India--a five-year follow-up study. Acta Ophthalmologica Scandinavica. 1999;77(3):310-4.
33. Murthy G. Vision Testing for Refractive Errors in Schools. ‘Screening’ Programmes in Schools. Community Eye Health. 2000;13(33):3-5.
34. Bhandari P. Refining State Level Comparisons in India. Planning Commission, Government of India, Working Paper Series. 2012.
35. Bandrakalli P, Ganekal S, Jhanji V et al. Prevalence and causes of monocular childhood blindness in a rural population in southern India. Journal of Pediatric Ophthalmology and Strabismus. 2012;49(5):303-7.
36. Singh MM, Murthy GV, Venkatraman R et al. A study of ocular morbidity among elderly population in a rural area of central India. Indian Journal Of Ophthalmology. 1997;45(1):61-5. 37. Ganekal S, Jhanji V, Liang Y et al. Prevalence and etiology of amblyopia in Southern India: results from screening of school children aged 5-15 years. Ophthalmic Epidemiology.
2013;20(4):228-31.
38. Ambika K, Nair NP. A study on awareness of primary school teachers regarding refractive errors and its early identification among primary school children. International Journal of Nursing Education. 2013;5(1):6-9.
39. Saxena R, Vashist P, Tandon R et al. Accuracy of visual assessment by school teachers in school eye screening program in Delhi. Indian Journal of Community Medicine. 2015;40(1):38-42. 40. Rewri P, Kakkar M, Raghav D. Self-vision testing and intervention seeking behavior among school children: a pilot study. Ophthalmic Epidemiology. 2013;20(5):315-20.
41. Priya A, Veena K, Thulasiraj R et al. Vision screening by teachers in southern Indian schools: testing a new "all class teacher" model. Ophthalmic Epidemiology. 2015;22(1):60-5.
42. Gupta Y, Sukul RR, Gupta M et al. School eye survey in rural population in UP, India. Nepalese Journal Of Ophthalmology. 2011;3(1):78-9.
43. Rustagi N, Uppal Y, Taneja DK. Screening for visual impairment: outcome among schoolchildren in a rural area of Delhi. Indian Journal Of Ophthalmology. 2012;60(3):203-6.
44. Gupta M, Gupta BP, Chauhan A et al. Ocular morbidity prevalence among school children in Shimla, Himachal, North India. Indian Journal Of Ophthalmology. 2009;57(2):133-8.
Corresponding author contact details
Name: Sethu Sheeladevi
Table1: Characteristics of Excluded studies S.
No
Author/ Journal name/ Year Reason for exclusion
1. Bandrakalli P et al. Journal of Pediatric Ophthalmology and Strabismus.
2012;49(5):303-7.
Data on refractive errors leading to
amblyopia is only presented in this article. (35)
2 Singh MM et al. Indian Journal Of Ophthalmology. 1997;45(1):61-5.
Data focused on elderly population and not on children. (36)
3 Jose, R et al. Indian Pediatrics 46(3): 205-208.
No prevalence data reported in this article. (9)
4 Ganekal, S et al. Ophthalmic Epidemiology. 2013; 20(4): 228-231.
Main focus of the article was on amblyopia(37)
5 Ambika, Ketal. (2013). International Journal of Nursing Education 5(1): 6-9.
Primary focus was on awareness of refractive errors among teachers.(38) 6 Saxena, R., et al. (2015).Indian Journal of
Community Medicine 40(1): 38-42.
No prevalence data reported in this article(39)
7 Rewri, P., et al. (2013). Ophthalmic Epidemiology 20(5): 315-320.
No prevalence data reported in this article(40)
8 Priya, A., et al. (2015). Ophthalmic Epidemiology 22(1): 60-65.
Main focus of the article was on screening sensitivity by all class teacher and there was no data on prevalence (41)
9 Limburg, H., et al. (1995). World Health Forum 16(2): 173-178.
No data on the prevalence of refractive errors(8)
10 Limburg, H., et al. (1999). Acta
Ophthalmologica Scandinavica 77(3): 310-314.
Results were analysed based on the
summary report prepared from the districts. No clear information on the refraction procedures(32)
11 Gupta Y, et al. Nepalese journal of
ophthalmology : a biannual peer-reviewed academic journal of the Nepal Ophthalmic Society : NEPJOPH. 2011;3(1):78-9.
No information on schools’ selection and the total number of children enrolled in each school. (42)
12 Rustagi N eta l. Indian Journal Of Ophthalmology. 2012;60(3):203-6.
Poor coverage for refraction (41.5%) among the children identified with the vision problem. (43)
13 Gupta M, et al. Indian Journal Of Ophthalmology. 2009;57(2):133-8.
No definition given on how refractive error was assessed(44)
14 Ajith S et al. Research Journal of
Pharmaceutical, Biological and Chemical Sciences. 2015;6(4):2024-7.
Table 2: Characteristics of the population based studies included in this review S . n o First author & Year of public ation Loca tion Regio n Study period Age group screening tools used Cyclopl egic screening
personnel definitions used
Subject locations (%) total no of childre n examin ed no of Children with RE # with myopia #with hypero pia # with Astigm atism Rur
al urban
1 Dando na R 2002( 4)** And hra Prad esh South April 2000 -Feb 2001 7 to 15 Retroilluminated logMAR E chart, lensometer, streak retinoscopy and auto refraction Yes in all childre n ophthalmic technicians and ophthalmologi st
Myopia -SE -0.50D and hyperopia - SE
+2.00 D or more. 100 0 4074 194 163 31 150
2 Murth y GVS, 2002( 5)** New Delh i North Dec 2000 to Mar 2001 5 to 15 LogMAR tumbling E chart, streak retinoscopy and handheld auto refractor Yes in all childre n Ophthalmic technicians and ophthalmologi st
Myopia -SE -0.50D and hyperopia –SE
+2.00 D or more. 0 100 5950 898 440 458 400
3 Dando na R, 2002* (6) And hra Prad esh
South July 1997 - Feb
2000 0-99*
Tumbling E, streak retinoscopy Yes in childre n optometrist and ophthalmologi st
Myopia - SE worse than -0.50D and hyperopia as SE
worse than +0.50D 77 23 2603 1726 81 1645 NR*
4 Nirma lan PK, 2003( 14) Tam ilnad u South July to Dec
2002 0-15
VA assessed using cambridge crowded cards, cake decorations, streak retinoscopy Yes (at the discreti on of ophthal mologi st) ophthalmic assistants and ophthalmologi st
Myopia - SE worse than -0.5 D and hypermetropia - SE
greater than + 2.0 D 100 0 10605 63 NR
NR
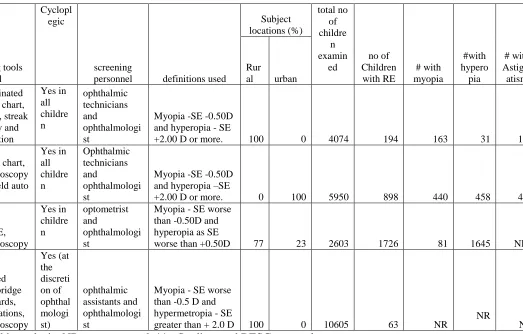
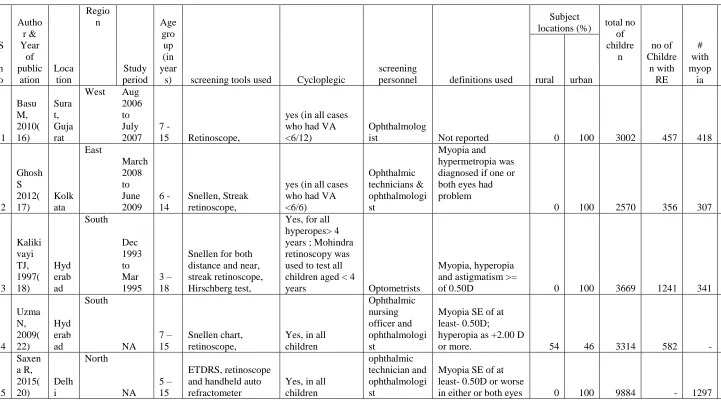
Table 3: Characteristics of the studies that reported refractive errors in school children S . n o Autho r & Year of public ation Loca tion Regio n Study period Age gro up (in year
s) screening tools used Cycloplegic
screening
personnel definitions used
Subject
locations (%) total no of childre n no of Childre n with RE # with myop ia #with hypero pia # with Astig matis m rural urban
1 Basu M, 2010( 16) Sura t, Guja rat
West Aug 2006 to July 2007
7
-15 Retinoscope,
yes (in all cases who had VA <6/12)
Ophthalmolog
ist Not reported 0 100 3002 457 418 21 18
2 Ghosh S 2012( 17) Kolk ata East March 2008 to June 2009 6 -14 Snellen, Streak retinoscope,
yes (in all cases who had VA <6/6) Ophthalmic technicians & ophthalmologi st Myopia and hypermetropia was diagnosed if one or both eyes had problem
0 100 2570 356 307 65 234
3 Kaliki vayi TJ, 1997( 18) Hyd erab ad South Dec 1993 to Mar 1995 3 – 18
Snellen for both distance and near, streak retinoscope, Hirschberg test,
Yes, for all hyperopes> 4 years ; Mohindra retinoscopy was used to test all children aged < 4
years Optometrists
Myopia, hyperopia and astigmatism >=
of 0.50D 0 100 3669 1241 341 900 410
4 Uzma N, 2009( 22) Hyd erab ad South NA 7 – 15 Snellen chart, retinoscope,
Yes, in all children Ophthalmic nursing officer and ophthalmologi st
Myopia SE of at least- 0.50D;
hyperopia as +2.00 D
or more. 54 46 3314 582 - - -
5 Saxen a R, 2015( 20) Delh i North NA 5 – 15 ETDRS, retinoscope and handheld auto refractometer
Yes, in all children
ophthalmic technician and ophthalmologi st
Myopia SE of at least- 0.50D or worse
6 Padhy e AS, 2009( 19) Mah aras htra West Aug 2004 and July 2005 6 – 15
Snellen E Chart, Hirschberg's test, streak retinoscopy
Yes in all children
optometrists, ophthalmologi st
Myopia SE ≥ - 0.75 D in one or both eyes. Hyperopia SE greater >+2.00 D in one or both eyes and astigmatism if >=
1.00D 40 60 12422 470 268 82 24
7 Ahme d I, 2008* (15) Kas hmir North NA 7 -21
Snellen E chart, pinhole, streak retinoscopy
Yes in all children (cycloplegic autorefraction) Optometrists, ophthalmologi st
Mild, moderate and severe myopia was defined as 0.25 to -2.99 D, -3.00 to 5.99 D and -6.00 D or
more respectively 0 100 3419 - 140 - -
8 Seem a S, 2009( 21) Hary ana
North Sep 2006 to July 2007 6 -15
snellen E chart,
streak retinoscope Not done
Ophthalmic assistants
Definition of RE was
not reported 100 0 1265 172 153 19 69
Table 4: Quality assessment of included studies
Sno Author Sampl
e r epr es entation of the ta rge t popul ati on? Appr opria ten
ess of pa
rtic ipants re cruitm ent S ampl e size a de qu ac y De tails o
f study subj
ec
ts and se
tt ing desc riptio n Da ta a n alysi s with suff icie nt cove ra ge of th e identifie d sample? Obje cti ve , standa rd c rite ria use d for mea sure ment of th e c ond it ion? C ondit ion m ea sure d re li ably? Appr opria te statis ti ca l an alysi s? All -im porta nt conf ounding fa ctors/ subgroups/di ff ere n ce s id enti fie d a nd a cc ounted for ? W ere sub popul ati ons i de nti fie d usi ng objec ti ve criter ia ?
Population based studies
1 Dandona R, 2002 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
2 Murthy GVS, 2002 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
3 Dandona Ra, 2002 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
4
Nirmalan PK,
2003* ✔ ✔ ✔ ✔ ✔ X X ✔ ✔ ✔
School based studies
5 Kalkivayi TJ, 1997 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
6 Ahmed I, 2008 ✔ ✔ ✔ ✔ X ✔ ✔ X X X
7 Padhye AS, 2009 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
8 Seema S, 2009 ✔ X ✔ U ✔ ✔ ✔ ✔ X ✔
9 Uzma N, 2009 ✔ U U ✔ ✔ ✔ ✔ ✔ X ✔
10 Basu M, 2010 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
11 Ghosh S, 2012 ✔ ✔ ✔ ✔ ✔ ✔ ✔ X ✔ ✔
12 Saxena R, 2015 ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
✔ - yes; X – No; U – Unclear; NA - not applicable
Table5: Results of subgroup meta-analyses for population based estimates on prevalence of refractive errors (Per 100 population) in children aged 0 -15 years
Types Overall
Prevalence (95% CI)
Urban
Prevalence (95% CI)
Rural
Prevalence (95% CI)
Refractive errors* 8.0 (7.4– 8.1) 18.7 (17.7 – 19.6) 4.8 (4.5 – 5.1 )
Myopia (≥ -0.5D) 5.3 (4.9 – 5.7) 10.8 (10.0 – 11.5) 3.5 (3.0– 4.0)
High Myopia (≥ -2.0D) 1.4 (1.2 – 1.6)
Hyperopia (≥ + 2.0D) 4.0 (3.7– 4.4)
High Hyperopia (≥ + 3.0D) 0.7 (0.6 – 0.9)
Astigmatism 5.4 (5.0 – 5.8)
Table 6: Results of subgroup meta-analyses on prevalence of refractive errors (Per 100 population) in school children aged 3 -18 years
Types Overall
Prevalence (95% CI)
Urban
Prevalence (95% CI)
Rural
Prevalence (95% CI)
Refractive errors* 10.8 (10.5 -11.2) 15.6 (15.1 – 16.2) 3.6 (3.2 – 3.9 )
Boys 9.5 (9.0 – 10.1)
Girls 12.2 (11.6 – 12.7)
Myopia 7.2 (6.9 – 7.5) 9.1 (8.8 – 9.5) 2.4 (2.1 -2.7)
Boys 10.2 (9.7 – 10.8)
Girls 11.6 (11.0 – 12.1)
Hyperopia 2.6 (2.4 – 2.8) 4.6 (4.3 -5.0) 0.5 (0.4 – 0.7)
Astigmatism 1.8 (1.7 – 2.0)
Figure 1: Summary of review strategy - PRISMA Flow Diagram
Figure 2: Forest plot on prevalence of refractive errors among children aged ≤ 15 years in India