COMPARISON OF DIMENSIONAL ACCURACY OF OPEN
TRAY AND CLOSED TRAY IMPRESSION TECHNIQUES
WHILE USING MULTI -UNIT ABUTMENTS
IN DENTAL IMPLANTS
A Dissertation submitted
in partial fulfil lment of the requirements
for the degree of
MASTER OF DENTAL SURGERY
BRANCH –I
PROSTHODONTICS
THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY
CHENNAI- 600032
ADHIPARASAKTHI DENTAL COLLEGE & HOSPITAL
MELMARUVATHUR- 603319
DEPARTMENT OF PROSTHODONTICS
CERTIFICATE
This i s to cert if y that Dr. A. T. GANAGAMANI, Post Graduat e student (2016 -2019) from the Depart ment of Prost hodont ics, Adhi paras akt hi Dent al C oll ege and Hospi tal, M elm aruvathur – 603319, has done this dissertation titled “COMPARISO N O F DI ME NSIONAL ACCURACY O F O PE N TRAY AND CLOSED TRAY I MPRESSION TECHNIQUES WHILE US ING MULTI -UNIT AB UT MENTS I N DENT AL I MPL ANTS” under our direct guidance and supervision in
parti al ful fill ment of the regul ati ons l ai d down b y the Tam i lnadu Dr. M.G.R M edi cal Uni versit y, Chennai – 600032 for M DS., (Branch - I) Departm ent of P rost hodonti cs Degree Examinati on.
Guide & Head of the Departm ent
Dr.N.VE NKATES AN, MDS
Professor and Head Departm ent of P rost hodonti cs
Principal
Dr. S. THILL AINAYAGAM., MDS
Professor and Head,
ACKNOWLEDGEMENT
I t hank AL MI GHT Y GO D for all his bles sings and for being with m e t hroughout and leads m e to prepare and complet e thi s diss ert ati on.
I t hank our C orrespondent Dr. T. Ramesh, MD., for his vital encouragem ent and s upport.
I am thankful t o Dr. Thill ainayag am, MDS., our bel oved princi pal , Adhiparas akt hi Dent al Coll ege and Hos pital, M elm aruvathur for providing m e wi th the opport unit y t o utiliz e t he faciliti es of the coll ege.
I avail t his opport unit y to expres s m y gr atitude and reverence to m y bel oved t eacher and guide Dr. N. VE NKATES AN , MDS., Profess or and Head, Depart ment of P rosthodontics, Adhi paras akt hi Dent al College and Hospit al, M elm aruvathur. His purs uit for perfection and immense support were a source of constant inspi ration t o me and without whi ch such an endeavour would never have m at erial ized.
I am t hankful and express m y gratitude to m y t eachers
I al so wish t o thank m y s eniors, Dr.S.Elakk iya, Dr.S.Vinothku mar, and m y post graduat e colleagues Dr. Nithyapri ya, Dr.Vidhu An tony and I warml y acknowledge m y juniors Dr.Jeevith a Mani, Dr.Kabil an, Dr.Mi thra, Dr. Pravin Thars an, Dr. Pazh ani Prasan th and Dr. Muthu Ann amalai .
I am i nfinit el y obli ged t o m y ever l oving parents
Mr. A. Thiyagarajan, m y mother Mrs . T. Poomariammal , m y wife
Dr. M. Preethi and m y daught er T.G. T haara without whos e s upport and underst anding, an ythi ng of these would have been not pos sibl e.
I t hank Dr. Dipayan Datta for hel ping me wit h the stat isti cs in the stud y. I thank Mr. Maveeran, B.com.,MLIS ., Li brari an and the librar y st aff Mr.K.SelvaKu mar,B.A., Adhi paras akt hi Dent al Coll e ge and Hospit al , M elm aruvathur , for t he favours the y have rendered.
DECL ARATIO N
TIT LE OF THE DIS SERTATION
COMPARISON OF DIMENSIONAL ACCURACYOF OPEN TRAY AND CLOSED
TRAY IMPRESSION TECHNIQUES WHILE USING MULTI-UNIT ABUTMENTS IN DENTAL
IMPLANTS
P LACE OF THE S TUDY
Adhi paras akt hi Dent al Coll ege and Hospital, Melm aruvathur -603319.
DUR AT ION OF THE COURSE 3 Years
NAME OF THE GUIDE Dr. N. VENKATESAN , M DS., NAM E OF HOD Dr. N. VENKATESAN, M DS.,
I hereb y decl are that no part of the di ss ert ati on will be uti li zed for gai ning financial assist ance or an y promoti on wit hout obt aining prior permis sion of the P rinci pal , Adhi paras akthi Dent al col lege and Hospital, M elm aruvathur -603319. In addition, I decl are that no part of this work will be publi shed eit her in print or in elect ronic medi a without the guides knowledge who have been acti vel y involved i n diss ert ati on. The aut hor has the ri ght to res erve for publ ish work s olel y with the permissi on of the Pri nci pal, Adhiparas akthi Dent al college and Hospital, M elm aruvathur -603319.
Guid e & H ead of Departmen t
ABSTRACT BACKGRO UND:
A dental impl ant i s a prostheti c devi ce m ade of all opl astic mat eri al im plant ed into the oral ti ssue beneath the mucos a and or perios teal l a yer and or wit hin the bone t o provi de retention and support for a fixed or removable dent al pros thesis. M aking a superstruct ure with pas sive fitness is one of the m ain objectiv es during implant -bas ed prosthesis . Preparati on of a precis e moul d with st able di mens ions prior to casting is neces sar y to achi eve t his passive fitnes s fai ling whi ch can lead to fract ure of t he impl ant components. The impression techni ques that are us ed i n impl ants are open tra y and cl os ed t ra y t echni ques . Bot h can result in dim ensi onal inaccurac y that can l ead to failure of the final abutment.
AI M AND OBJE CT IVE:
To compare the dim ensi onal accurac y and the bett er impres sion techni que between open tra y and cl os e tra y im pres sion t echni ques whil e using mul tiuni t abutm ent s in dent al impl ants .
MATE RI AL AND METHO DS:
units of the compound coping were pl aced deep in the impressi on b y appl ying press ure with com pl ete or partial clockwis e rot ati on till a resist ance agai nst rotation was felt . The i mpress ion was examined and it was repeat ed when an y kind of defi ci enc y was obs erved i ncl uding trapped ai r bubbl es and l eft overs of im pressi on mat eri al between the coping connection and the anal ogue. Dental stone, hi gh strength (t ype IV) cast was then prepa red that were trimmed and coded after being cured for one hour. The casts were anal ys ed b y CMM (coordi nating measuring m achine, GMT German y). S tatist ical anal ys is adopt ed i n this s tud y was Student t -test.
RESULTS:
Statist icall y si gni fi cant p val ue was ach i eved onl y for im plant 1 of the open tra y and clos ed t ra y im pressi on techniques. When implant 1 was compared for difference in m ean from the cont rol, open tra y method s howed less er devi ation from t he st andard, and hence bett er accurac y i n im press i on
CONCLUS ION:
The res ults of the present st ud y show t hat open t ra y im press ion techni que produces bett er di mensional accurac y when compared t o clos ed t ra y impressi on t echni que when used for mul ti -unit abutment implants
KE Y WORDS:
CONTENTS
S.NO
TITLE
PAGE NO
1.
INTRODUCTION
1
2.
AIM AND OBJECTIVES
9
3.
REVIEW OF LITERATURE
10
4.
MATERIALS AND METHOD
22
5.
RESULTS
30
6.
DISCUSSION
39
7.
CONCLUSION
54
LIST OF TABLES
S.No Titl e Page-No
1. Descript ive st ati sti cs 30
2.
Independent t t est t o com pare the mean values of t he vari abl e with the control values
31
3.
Independent t t est t o com pare the mean values of t he vari abl e with the control values
31
4.
Independent t t est t o com pare the mean values of t he vari abl e with the control values
32
5.
Independent t t est t o com pare the mean values of t he vari abl e with the control values
32
6.
Independent t t est t o com pare the mean values of t he vari abl e with the control values
33
7.
Independent t t est t o com pare the mean values of t he vari abl e with the control values
33
LIST OF FIGURES
S.No Titl e Page-n o
1. Arm am ent arium 24
2. Met al m odel 24
3. Im pl ant s pl aced at angul ations of 00,170,280 25 4. Mast er M odel placed on surve yor 25 5. Closed t ra y t rans fer checked for parall eli sm 26 6. Closed t ra y i mpres si on 26 7. Open t ra y transfer checked for parall elism 27 8. Open t ra y impression 27 9. Att achment of impl ant analogues 28 10. Die stone cast prepared from cl osed t ra y i mpressi on 28 11. Die stone cast prepared from open tra y im pressi on 29
12.
Angulations m easured usi ng co -ordinate measuring machine(GMT, Germ an y)
LIST OF GRAPHS
S.No Titl e Page. No
1
Compari son of open tra y i mpression m ethod wit h control
35
2
Compari son of clos ed tra y impressi on m ethod wit h control
Introduction
Page 1
A Dent al impl ant i s a prostheti c devi ce made of alloplastic mat eri al im plant ed into the oral ti ssue beneath the mucos a and or perios teal l a yer and or wit hin the bone t o provi de retention and support for a fixed or removable dental prosthesis; a s ubst ance that is placed into and or on the jaw bone to support a fixed or removable dent al prosthes es.[1] It i s a surgical component that interfaces wi th the bone of t he jaw or skul l to support a dent al prosthesi s s uch as a crown, bridge , denture , faci al prosthesi s or t o act as an ort hodonti c anchor .
Introduction
Page 2
Toot h loss is ver y comm on and it can happen as a result of diseas e and t raum a; therefore, the use of dental implants t o provi de support for replacement of mi ssing t eeth has a long and m ultifaceted histor y. St atis tics provided b y t he American As soci ation of Oral and Maxillofaci al S urgeons show that 69% of adults ages 35 to 44 have lost at least one permanent tooth to an accident, gum dis eas e, a failed root canal or tooth deca y. Furthermore, b y age 74, 26% of adul ts have lost all of t heir perm anent t eeth. Therefore, the us e of dent al impl ants reveal s that about 100,000 -300,000 dental impl ants are placed per year, whi ch approximates the numbers of art ifi ci al hip and knee joi nts pl aced per year. [2]
The basis for modern dental impl ant s is a biologi c process called oss eoint egration . The genesis of oss eoi ntegration as a concept was introduced b y P er - Ingvar Branemark (1969), profes sor at t he Instit ut e of Appli ed Biot echnology, Universit y of Got eb org. He call ed it as “A direct s truct ural and functi onal connection bet ween ordered li ving bone and the surface of t he load – coveri ng implant.” Os seoint egration is defined as “The apparent direct att achment or connection of oss eous tissue to an inert, all oplasti c mat eri al without interveni ng connecti ve
tissue”.[1] The American Academ y of impl ant dentist ry in 1989
defines oss eoint egration as “Contact established without interposition
of nonbone tissue betw een normal remodel ed bone and an impl ant
ent ailing a sustai ned transf er and di stri bution of load from the impl ant
Introduction
Page 3
minim al am ount of bone should be rem oved, the bas ic t opograph y of the region s houl d not be changed, t he ret enti on of the ori gi nal or transiti onal denture s hould be m ai ntai ned duri ng the healing period.[3] Maki ng a superst ructure with pas sive fitness is one of the m ain obj ecti ves duri ng im plant -based prost hes is. Passive fitnes s is the t erm used to addres s fitt ing status of the i mplant in whi ch im plant bod y shows adequat e fitti ng of its superst ruct ure for simul taneous adapt ati on when one or more number of im pl ants a re us ed or connected. Preparation of a precis e mould wit h st able di mensions pri or t o casti n g is necess ar y to achi eve thi s passive fi tnes s. However, failing t o achi eve this passi ve fit ness will incur st ress on i mplants whi ch can fi nall y lead to fract ure of the im plant components and failure of t he treat ment . The forces created i n t he impl ant due to non -pas sive nat ure of the superstruct ure i s abl e to resorb t he bone surroundi ng the im plant and caus e is chemi a withi n peri -implant tissue and subsequent heal ing w ith non- mineral tis sue around the impl ant, mechani cal fracture, loosening of t he implant com ponents and fracture of the rest oration.
Introduction
Page 4
have been regarded more t han other issues. Som e degrees of error and inaccurac y have also been noti ced in the precis e transfer of t he implant positi ons for all im pr essi on methods. Dimensional changes occur due to the contraction i n the im pression m at eri al due t o pol ymerizati on reaction with form at ion of vol atil e mat erials and b y -product s and als o from t he pressure applied duri ng the im pressi on t echnique.
Dental impressi on can be defined as “a negative im pri nt or a positi ve di git al im age dis pla y of int raoral anatom y us ed to cast o r produce a 3D repli ca of the anatomical st ructure that is t o be used as a perm anent record or for the production of a dent al rest oration or a prostheses” – GPT-9. Dental impression of implants placed in mouth form a criti cal aspect in fi nal prosthesi s and ever y effort s hould be made to ensure that the int raoral fit i s accurat el y reproduced in the impress ion made.
Introduction
Page 5
abutments are not neces sar y. Open tra y techni que us es a custom or stock t ra y wit h access to t he i mpres sion coping s crews , which expos es the coronal end s of the im pression coping. Im press ion mat eri al is s yri nged around the impress ion coping and fil led tra y i s then ins ert ed into t he mouth, ens uring t hat gui de pi n of the im pres sion coping is visibl e and prot rudes through the hol e i n the tra y. Impressi on cop i ngs are uns crewed and t he y are removed from the m out h together with the set im press ion. The implant anal ogues are connect ed t o the copings using the same screw. Som e precauti ons to be t aken are radiographicall y confirmed seati ng of im pressi on copi ng to t he impl ant and us e vi n yl gloves when el ast omeri c impres sion m at eri al is us ed. This technique can be us ed for singl e tooth rest orati ons, multi -unit restorations and im plant over dentures for eit her cem ent ret ained or screw ret ained prost hesi s. An advant ag e of this t echnique is t he dentis t can confirm t he l aborator y preparati on and contour of the provi sional prosthesis to achi eve the desi red heali ng and soft t issue contour before final crown fabricati on.
Introduction
Page 6
techni que depends upon its resist ance to deformation under t he forces of impressi on m aterial; hence t he use of ri gid splint m at eri al is essent ial for accurat e master cast. Mat erials used to spl int i mpressi on copings incl ude patt ern resin, li ght -curing composit e resi n, i mpressi on plas ter and autopol ymerizing acr yli c resi n.
In closed t ra y i mpres sion t echnique, the copings are connected to the im pl ant and aft er the rem oval of im pressi ons t he y are ret ained on the impl ant s. Thes e copings are t hen removed from the impl ant , att ached to the implant analogues and rei ns erted in the impressi on. Clinical situati ons which indicat e the use of the closed t ra y techni que are lim ited int erarch space, a t endenc y t o gag, or if i t is too difficult to access an im pl ant i n the pos terior regi on of t he mouth.
Introduction
Page 7
rel iable impression t echni que b ut it cannot be us ed i n mos t s ituat ions where t he abutm ents are modi fi ed, angulated impl ant s are pl ace d.
When restori ng a full arch, screw -retained implant prostheti c case, even a mini m al disparit y in the draw of the impl ant int erface access caus es restorative chall enges. The us e of multi -unit abutments can overcom e restorative chall enges and is hi ghl y recomm ended (i f not requi red) when creati ng a f ull arch s crew -ret ained impl ant restoration . M ulti -unit abutm ent s (MUA), are desi gn ed with a range of angle correct ion and are availabl e for vi rtuall y all im plant plat forms. Multi -uni t abutments provi de a passive draw and posi tive uni form seat for all abutm ent sit es. The y are indi cat ed i n s crew ret ained full arch prosthes es, to correct angul ations, to correct for implant hei ght disparities. The advantage of usi ng multi -uni t abutm ents far outwei ghs an y of the dis advantages such as much easi er and more predi ct abl e seating of the final restoration, reduced st ress trans lat ed into the restorative s ys t em due t o t he passi ve nature of t he s eating process of multi-unit abutm ents and easi er to remove and repl ace the prost hesis duri ng recall appoint ment s.
Introduction
Page 8
of us e and surgi cal effi ci enc y. Multi -unit abutments are avail abl e in different angl es s uch as 17o,28oand 40o. The angl ed Multi -uni t abutments al low for the tilti ng of the two post eri or implants, meaning longer impl ant s can be positi oned i n the ant erior bone, rat her than i n the post erior where t he bone is oft en res orbed. This increas es bone to -implant contact and reduces the need for verti cal bone augm entati on.
Aim and Objectives
Page 9
Aim of th e stu dy
To com pare t he di mensional accurac y and i denti f y a better impress ion t echnique bet ween the open t ra y and cl os e d t ra y i mpressi on techni ques when usi ng multiunit abutments i n dent al impl ant s .
Obj ectives of th e s tudy
To find the dim ensional accurac y of open t ra y impres sion techni que using mul t iunit abutm ent
To find the dimens ional accurac y of clos ed t ra y impress ion techni que using mul t iunit abutm ent .
Review of Literature
Page 10
Im plant failur e
Im pl ant therap y, while hi ghl y effective, does have the potential for both techni cal and bi ological compl ications. A. G. Wee et al in 1999 [5] report ed that the com pli cations include bone loss , fract ure of the impl ant or the fracture at th e i mpl ant abutm ent int erface.
M. Karl et al i n 2004[6] told that t here are s everal cli ni cal and laborator y variables that can affect t he accurac y of t he im plant cast. These have a di rect effect on the fi nal fi t of t he prost hesis and include impress ion t echnique, pouring m ethods, im pres sion mat eri al s, properti es of the di e st one us ed, m achi ning t ol erance of the implant mat eri al us ed and i m plant dept h and angulation.
Passi ve fit of im plan ts
Review of Literature
Page 11
superstruct ure especi all y with m ulti -unit implant support ed prosthes es. Although there is no act ual definiti on to hi ghli ght t he m eani ng of pas sive fi t cli ni cal l y , the superst ructure of the s crew ret ained impl ant -support ed prosthesi s can be consi dered pas sive if it does not generate stati c loads and strai ns withi n the prosthesis or i n t he surrounding bone mat rix. J emt et al[8] defi ned the passive fit as a level of fit which will not produce or caus e an y l ong -t erm clini cal probl em.
Im plant m isfit
Review of Literature
Page 12
Machinin g t oleran ce
Lee et al in 2008 [10] stat es mechanical or m achi ning tol erance is defi ned as t he di fference i n res t positi ons (horizontal shift ) bet ween the components when t hese component s are held in place b y t hei r respective fast ening screws. This can be considered as a source of misfit , whi ch ca n range from 22 to 100 mi crons .
Biologi cal toler ance
Lee et al in 2008 [10] stat es biologi cal tolerance i s the capabi lit y of t he bone surrounding t he impl ant s t o wit hst and and t ol erat e t he stress es dist ribut ed along t he impl ant -bone int erface, wi thout an y further clini cal com plications.
V.A.Chi a et al i n 2017[11] evaluat ed several studies that att empt ed to define the mi sfi t num eri cal l y, but there was no definit e agreem ent to quanti f y the accept able l evel of the mis fit . The fi rst person to quantif y the passi ve fit of impl ant fram ework was Branemark who st at ed t hat the misfit should be not more t han 10 mi crons.
Fact ors affecting passive fit
Review of Literature
Page 13
whi ch i ncl udes i mpressi on m at erial , impression t echnique, the implant angul ations and the number of impl ant s. The impression techni que itsel f depends on whether it is a di rect or indi rect method, s plint ed or non-spli nt ed, and on the desi gn of t he impression coping.
Im pressi on m a ter ial
Carr AB in 1992 [13] concluded t hat there is an i nevit able, inherent dis crepanc y in t he impl ant im pression, whi ch was quot ed in the range of 50 μ m. One of the factors rel at ed to thi s inherent discrepanc y i s the shrinkage and cont ract ion of the impression m at erial due to t he cross -li nking and rearrangement of the pol ym er chai ns. Further shrinkage can occur due to los s of vol atil e consti tuent s and b y -products. The expansion wi ll als o occur if there is wat er sorpti on. Several impression mat eri al s have been use d for mult i -uni t impl ant impress ion; t he mos t comm onl y described were addition sil icone and pol yether im press ion m ateri als . This can be correlated to t hei r improved accurac y.
Im pressi on tr ay
Review of Literature
Page 14
and at the s ame tim e, the im press ion material was uniform l y di stribut ed withi n t he customi zed t ra y unli ke the s tock tra y. The impl ant impress ion can be at the abutm ent or im pl ant level.
Im plant level im pr es sion an d copin g
The impl ant l evel i mpressi on i s preferred i n the aestheti c z ones and reduces the num ber of treatm ent vi si ts. The im press ion copings are mainl y s uppl ied in tapered or squared shapes . Muai yed Mahmoud Buz a yan et al i n 2013[15] report ed that m odi fi cat ion of t he coping surface could enhance the accurac y of t he im press ions , modifi cations such as airborne part icl e abrasion of the copi ngs and coating t he copings wi th t he compati bl e adhesi ve.
Num ber of im plants and an gulati on
Review of Literature
Page 15
Im plant im pres sion pr ocedures
Pande y K et al i n 2013[17] Two m ain impl ant impressi on techni ques are used for transferri ng t he intra -oral spati al rel ationshi p of the im pl ants t o t he working cas t. One impressi on t echni que is the direct open t ra y t echnique uses an open t ra y, a custom tra y t hat contai ns wi ndows exposing the im pressi on copings . The other impress ion t echni que is the indi rect t echnique that us es closed t ra y. The most common t echni ques are closed -t ra y, open - tra y whi ch has been cit ed al most si milarl y in t he lit erat ure, although angul ation of th e implants pl a ys a key rol e in the accurac y of impressi on. The t rans fer techni que us es t apered copings and a cl os ed t ra y to make an impress ion.
Open tr ay/ pi ck up i m pression
Review of Literature
Page 16
Rubber bas e impress ion m at eri al i s loaded, and t he impression is taken on the open tra y. Impressi on coping is felt below t he wax sealed window area of t he t ra y. After the com pl et e s et, the i mpressi on copings are uns crewed t hrough t he wi ndow on the t ra y. As copings are ti ght ened t ogether, t hes e will com e out together wit hout any m om ent and with great er accurac y from the m out h. The copings are eas il y rem oved wit h proper support of impressi on m at erial . Gingival form er/ healing abutments are repl aced on impl ant fixture.
Advant ages of open tra y i mpres sion t echniques as told b y S parsh Garg i n 2013[18] are reduces the effect of i mpl ant angulat ions, reduces deform ation of t he impressi on m at eri al, removes the concern for repl aci ng back the coping int o the respective s pace of t he i mpressi on. Dis advantages of open tra y t echnique are the movem ent of impressi on copings insi de the i mpres si on during the clini cal and laborat or y phas es ma y cause inaccuracy in transferri ng the spati al posit ions of impl ant s from t he oral cavit y to the m as ter cast.
Closed t ray im pressi on techni que
Review of Literature
Page 17
coping and impress ion m at eri al whi ch is ensured before final t ra y sel ection.
Review of Literature
Page 18
the fat e of impl ant support ed prosthesi s . Gingival form er is tightened on im plant fixture after rem oval of the cl osed t ra y t rans fer.
Accordi ng to C onrad et al[16] and Lee et al[10], in some situations, the indi rect clos ed t ra y is preferred to di rect open t ra y techni ques, such as i n cas es of gaggi ng, l imited int er -arch space and i n cases where access t o the post erior region is limit ed. The advant ages of this t echni que; it is easi er as it resem bles the conventional i mpressi on techni que and t he repli ca t o copings fast eni ng would be visualized directl y, suit abl e for short i nter arch space and speci al tra y is not requi red. However, the impression m at eri al recovering f rom angl ed implants will b e diffi cult, and t here will be a hi gh chance of impress ion deform ation. Im pression copings need to be carefull y reposi tioned and correctl y ori ent ed back at t hei r respective sit es.
Snap fit im pr essi on techniqu e
Review of Literature
Page 19
Advant ages are it helps to overcom e the movement of impres sion coping inside the im pressi on m ateri al, ti me s a ving, has the advantage of both the open and cl os ed t ra y i mpl ant impression t echniques , more com fort abl e for both the cl ini ci an and the pati ent and eas y t o mani pul at e, helps t o overcom e t he m ovem ent of im pres si on coping inside the impression mat eri al , time saving. The s nap -fit t echnique is the most reli abl e i m pressi on t echnique but it cannot be us ed in most situations where the abutm ent s are m odifi ed, angulated implant s are placed.[4]
Digit al im pr essi on t echni ques
Review of Literature
Page 20
tools to t each toot h anatom y and tooth preparati ons i n teaching institutions.
Di git al im press ion procedures have been recentl y in t roduced in fixed and im plant prosthodontics, as b y thei r nat ure, thes e procedures ma y elimi nat e the errors wit h convent ional impressi ons and st one casts (Ender & Mehl 2015; Chochli dakis et al. 2016). Di git al i mpressi ons using an int ra-oral optical scanner (IOS) eliminat e tra y selecti on, dispensi ng and pol ym eriz ation of impress ion m at erials, and disinfecti on and shi pping to the laborat ory, whil e pati ent com fort is an additional advantage (P apasp yri dakos et al. 2014). The di gital impress ions are s ent and sto red elect ronicall y, improvi ng effi ci enc y (Lee et al . 2015; Li n et al. 2015; Gi menez Gonzal ez et al. 2016; Papasp yri dakos et al. 2016). C urrentl y, the most popul ar video acquisition IOS s ys t ems on t he market are t he TR IOS (3shape), the Omni cam (CEREC b y Si r ona), and the True Definiti on s canner (3M ESPE)[65]. Though t he us e of di git al impressions for implant dentist r y has not been full y established, accurac y of di git al im pres sions has not been wi del y studied till toda y. Verifi cation of accurac y of a di git al impress ion i n the im plant fi eld should be a prerequi sit e for t he cl ini cal applicati on of an y new t echnology.[19]
The A ccuracy of the Dir ect and th e Indi rect Techniqu es
Review of Literature
Page 21
accurat e than the indirect one. Others demonst rat ed t hat the indirect techni que was m ore accurat e t han t he di rect ones. W hile the rest found no statisti call y si gnifi cant di fference bet ween both t echniques. A s yst em atic review by Lee et al [10] concluded t hat, in situati ons where there are th ree im plants or fewer, no si gnifi cant di fference bet ween t he direct and the indi rect techniques were observed, whi le in cas e of m ore than three i mpl ants , the di rect techni que was fo und t o be m ore accurat e.
Materials and Method
Page 22
Material s and M eth od
The res earch was done through an experim ent al laborat or y method on 10 s ampl es in each group and a mast er sam ple formi ng a total number of 21 s ampl es . A steel model, havi ng 8 cm di am et er and 3 cm hei ght, was m ade. Ever y two angulated im pl ants were 4 cm apart with 3.5 cm dist ance from central im pl ant . The positi on of impl ants was anal ys ed b y the surve yor so that the cent ral impl ant (Im plant -1 00) was pl aced perpendicular t o t he cast ing s urface while the other implants had divergence or convergence of 17°( Implant 2) and 28o (Im pl ant 3) respecti vel y from t he cent ral component. T he implants were fixed usi ng c ya noacr yl at e. Even though we know cust om tra ys are best s uit ed for m aki ng impl ant impressi ons, in a cli nical perspective the use of stock t ra ys out wei ghs t he use of cust om t ra ys . Therefore in this s tud y st ock t ra ys were us ed i ns tead of custom tra ys . All operations were impl em ent ed by one operator. Stock t ra ys m ade of m et al wit h cust omis ed tra y handles to be at tached t o the s urve yor were used. The tra ys were then tri mmed and perforat ed to enhance gri ppi ng of t he impress ion mat er i al . The t ra ys were fill ed b y pol yvinyl s iloxane mat eri al and s eparat e impressions were made. The im pres sion mat erial was allowed t o be pol ym eriz ed for 3 minutes before det achm ent.
Materials and Method
Page 23
trans fer copings. Im pressi on copings of t he cl os ed tra y rem ai ned on t he main cast aft er pol ym eriz ation of the impressi on m at eri al. These copings were removed from the mai n cas t and connected to the analogue when the t ra y was removed. Anal ogue uni ts o f t he copi ngs were pl aced deep in the im pres sion b y appl ying pres sure with complet e or parti al clockwis e rot ation till a resist ance against rotati on was felt. This contact feel ing i mpli es t hat posi tion of the im pl ant has been correctl y transferred.
Materials and Method
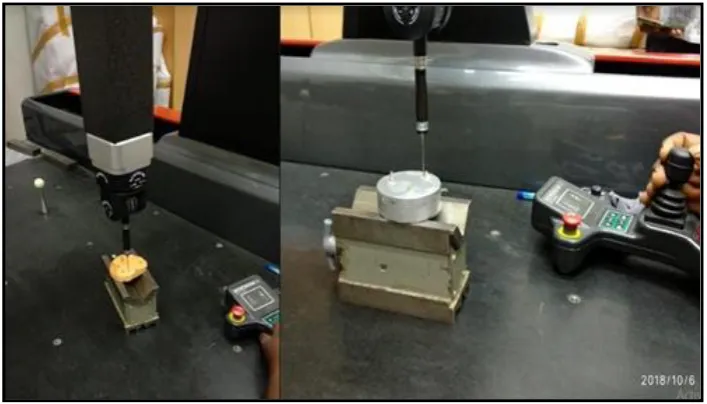
Page 24 Figu re 1: Armamen tariu m
[image:35.595.109.486.98.349.2] [image:35.595.168.427.443.731.2]Materials and Method
Page 25 Figu re 3: I mplan ts placed at angulati ons
[image:36.595.169.427.126.356.2] [image:36.595.204.391.423.744.2]Materials and Method
Page 26 Figu re 5: Clos ed tray transfer ch eck ed for p arall elis m
[image:37.595.212.383.102.385.2] [image:37.595.217.379.456.739.2]Materials and Method
Page 27 Figu re 7: Op en tray transf er ch ecked for parallel is m
[image:38.595.216.381.99.386.2] [image:38.595.207.384.452.755.2]Materials and Method
Page 28 Figu re 9: Attach ment of Impl ant anal ogues
[image:39.595.172.425.126.356.2] [image:39.595.174.424.452.714.2]Materials and Method
Page 29 Figu re 11 : Di e s ton e cas t p repared from op en tray i mp res sion
[image:40.595.128.473.126.422.2] [image:40.595.121.475.518.720.2]Results
[image:41.595.86.514.126.328.2]Page 30 Table 1: Descrip tive s tatis ti cs
VARIABLES N MI NI MUM MAXI MUM MEAN SD
OPEN 1 10 87°46'8" 88°46'8" 88°4'12" 0°28'48" OPEN 2 10 86°42'28" 88°42'28" 87°36'36" 0°43'48" OPEN 3 10 87°31'59" 89°31'59" 88°37'48" 0°48'36" C LOSED 1 10 86°46'8" 88°46'8" 87°52'12" 0°33'36" C LOSED 2 10 83°42'28" 88°42'28" 86°6'36" 1°57'18" C LOSED 3 10 87°31'59" 89°31'59" 89°13'48" 0°57'36"
Valu es in degrees converted in d eci mal
VARIABLES N MI NI MUM MAXI MUM MEAN SD
OPEN 1 10 87.77 88.77 88.0700 .48305 OPEN 2 10 86.71 88.71 87.6100 .73786 OPEN 3 10 87.63 89.63 88.6300 .81650 C LOSED 1 10 86.77 88.77 87.8700 .56765 C LOSED 2 10 83.71 88.71 86.1100 1.95505 C LOSED 3 10 87.63 89.63 89.2300 .69921
Note: N: number of s ampl es
Open 1: Open t ra y i mpressi on of Im pl ant 1 ;Clos ed 1: Clos ed tra y impress ion of Impl ant 1
Open 2: Open t ra y impres sion of Implant 2 ;Cl os ed 2: Cl osed t ra y impress ion of Impl ant 2
Results
Page 31 Table 2: Indep end ent t test to com p are th e mean valu es of th e variabl e with th e con trol valu es [St ati sticall y si gni fi cant difference exists bet ween the m ean of the variabl e and the cont rol (p<0.05) ]
Vari abl e Independent t t est t df Sig. Mean
Difference
Std. Error Differ ence
95% Confidence Int erval of t he
Difference Lower Upper Open Implant 1 3.395 9 .008 1.72000 .50662 .57394 2.86606
Table 3: Indep end ent t test to comp are th e mean valu es of th e variabl e with th e control valu es [St ati sticall y si gni ficant difference exists bet ween the m ean of the variabl e and the cont rol (p<0.05) ]
Vari abl e Independent t t est t df Sig. Mean
Difference
Std. Error Difference
95% Confidence Int erval of t he
Difference Lower Upper Open Implant 2 2.972 9 .016 2.30000 .77388 .54936 4.05064
[image:42.595.54.546.153.290.2] [image:42.595.54.547.396.543.2]Results
Page 32 Table 4: Indep end ent t test to comp are th e mean valu es of th e variabl e with th e control valu es [St ati sticall y si gni ficant difference does not exist bet ween t he m ean of the variable and the cont rol (p>0.05)]
Vari abl e Independent t t est t df Sig. Mean
Difference
Std. Error Difference
95% Confidence Int erval of t he
Difference Lower Upper Open Implant 3 1.553 9 .155 1.33000 .85635 .60720 3.26720
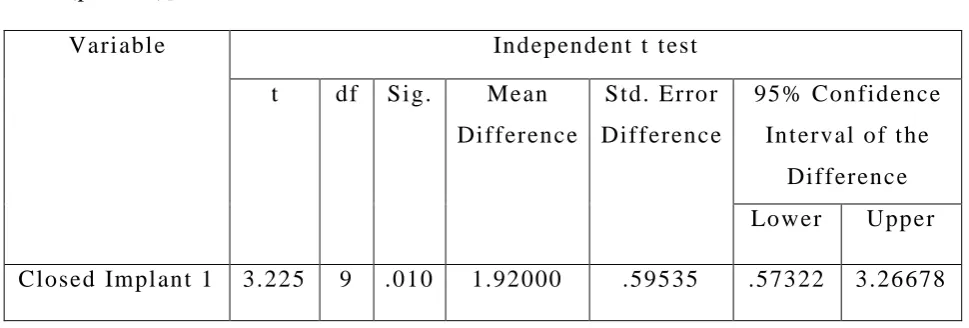
Table 5: Indep end ent t test to comp are th e mean valu es of th e variabl e with th e control valu es [St ati sticall y si gni ficant difference does not exist bet ween t he m ean of the variable and the cont rol (p>0.05)]
Vari abl e Independent t t est t df Sig. Mean
Difference
Std. Error Difference
95% Confidence Int erval of t he
Difference Lower Upper Closed Impl ant 1 3.225 9 .010 1.92000 .59535 .57322 3.26678
[image:43.595.61.538.180.325.2] [image:43.595.56.541.446.610.2]Results
Page 33 Table 6: Indep end ent t test to comp are th e mean valu es of th e variabl e with th e control valu es [St ati sticall y si gni ficant difference does not exist bet ween t he m ean of the variable and the cont rol (p>0.05)]
Vari abl e Independent t t est t df Sig. Mean
Difference
Std. Error Difference
95% Confidence Int erval of t he
Difference Lower Upper Closed Impl ant 2 1.853 9 .097 3.80000 2.05047 .83849 8.43849
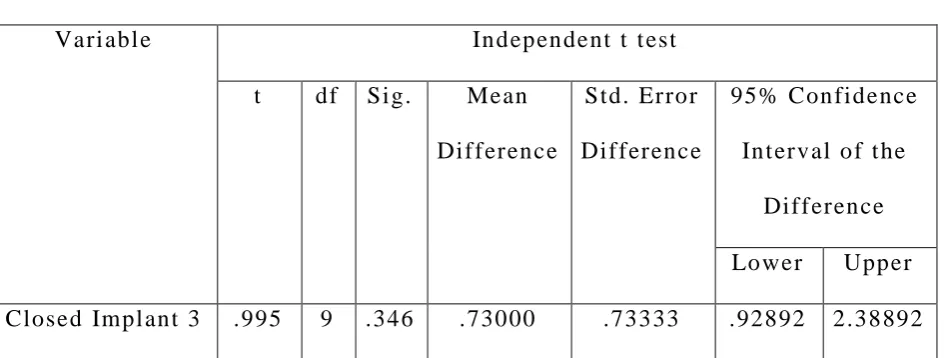
Table 7: Indep end ent t test to comp are th e mean valu es of th e variabl e with th e control valu es [St ati sticall y si gni ficant difference does not exist bet ween t he m ean of the variable and the cont rol (p>0.05)]
Vari abl e Independent t t est t df Sig. Mean
Difference
Std. Error Difference
95% Confidence Int erval of t he
Difference Lower Upper Closed Impl ant 3 .995 9 .346 .73000 .73333 .92892 2.38892
[image:44.595.56.540.179.322.2] [image:44.595.65.539.446.625.2]Results
[image:45.595.99.495.150.390.2]Page 34 Table 8: Fin al chart with the p values of independ en t t tests
[* Mean difference between case and control i s st atist icall y si gnificant (p<0.05)]
TECHNIQUES VARIABLES MEAN ± SD P VALUE O F T TEST
O PEN
IM P LANT 1 88.07 ± .48 .008* IM P LANT 2 87.61 ± .73 .016* IM P LANT 3 88.63 ± .81 .155
CLOSED
IM P LANT 1 87.87 ± .56 .010* IM P LANT 2 86.11 ± 1.95 .097 IM P LANT 3 89.23 ± .69 .346
Table 9: Mean differen ce of op en and cl osed method
Open tray meth od Clos ed tray method
Im pl ant 1 1.72000 1.92000 Im pl ant 2 2.30000 3.80000 Im pl ant 3 1.33000 0.73000
Note:
Open: Open tra y impression Im pl ant 1: 0o implant Closed: Cl os ed tra y i mpressi on Im pl ant 2: 17o implant
[image:45.595.97.497.438.552.2]Results
Page 35 Graph 1: Comp ari s on of op en tray i mp ression method wi th con trol
Graph 2: Comp ari s on of clos ed tray i mpression method wi th con trol
Note:
Open 1: Open t ra y i mpressi on of Impl ant 1(0o) Clos ed 1: Cl osed tra y impress ion of Impl ant 1(0o)
Open 2: Open tra y i mpressi on of Im plant 2(17o) Clos ed 2: C losed tra y impression of Impl ant 2(17o)
Open 3: Open tra y i mpressi on of Im plant 3(28o) Closed 3: C losed tra y impression of Impl ant 3(28o)
86 86.5 87 87.5 88 88.5 89 89.5 90
OPEN 1 OPEN 2 OPEN 3
88.07
87.61
88.63 89.79 89.91 89.96
COMPARISON OF OPEN TRAY METHOD WITH CONTROL
CASE CONTROL 84 85 86 87 88 89 90
CLOSED 1 CLOSED 2 CLOSED 3
87.87
86.11
89.23 89.79 89.91 89.96
COMPARISON OF CLOSED TRAY METHOD WITH CONTROL
Results
Page 36
A total of 10 s am ples each cont ai ning three implants were assess ed b y open and closed tra y i mpression t echni ques, m aking a t ot al of t went y s ampl es . The three impl ants i n each cast was divi ded int o open impl ant -1, open implant -2 and open implant -3 each containing t en val ues i n open t ra y impressi on t echnique. Simil arl y cl osed -t ra y impress ion t echni que values were divided into cl os ed implant -1, cl os ed implant -2 and clos ed impl ant -3 each cont ai ni ng t en values .
Results
Page 37
clos ed impl ant -3 had a m ean val ue of 89.23 wit h a minim um of 87.63 and a m aximum val ue of 89.23 wit h a st andard devi ati on of 0.66921.
Independent t test s were performed to compare the mean values of the vari ables with thei r control values. Tabl e 2 shows i ndependent t test with a mean difference of 1.7200 for open im pl ant -1 when com pared t o cont rol . The result was st atisti call y si gnificant with p val ue at 0.008. Table 3 shows independent t test wit h a mean difference of 2.300 for open -im plant 2 when com pared to cont rol. The result was stati sti cal l y si gni fi cant with p value at 0.016. Tabl e 4 shows independent t test wi th a m ean difference of 1.3300 for open -i mplant 3 when com pared to control. The res ul t was not st atisti call y s igni ficant with p val ue at 0.155.
Table 5 shows independent t t est wit h a m ean di fference of 1.9200 for clos ed -im plant 1 when compared t o cont rol . The result was stati sti cal l y si gni fi cant with p value at 0.001. Tabl e 6 shows independent t t est wi th a mean di fference of 3.8000 for cl os ed -im plant 2 when com pared to control. The result was not st atisti call y si gnificant with p val ue at 0.097. Tabl e 7 s hows independent t t est wit h a m ean difference of 0.7300 for closed -im pl ant 3 wh en compared to cont rol . The res ult was not st atisti call y si gni ficant wit h p value at 0.346.
Results
Page 38
p val ue at 0.008 and 0.016, whereas cl os ed implant -1 showed stati sti cal l y si gni fi cant value with p value at 0.001. Table 8 s hows th e mean di fference for open impl ant -1 and open impl ant -2 i mpl yi ng l ess er deviati on from the st andard when compared to closed im plant.
Since the s tud y i n volves assessm ent of bett er impres sion techni que b y com paring close values from the cont rol, l es ser mean difference was cons idered to be a bett er i mpres sion technique and clini call y s i gni fi cant. P values < 0.05 show s tat isti call y si gnificant result .
Discussion
Page 39
Dental impression of impl ant s placed in mouth form a criti cal aspect in final prost hesi s and ever y effort s houl d be made to ensure that t he i nt raoral fit is accurat el y reproduced in the i mpressi on produced. This enables t he perfect fit for the final abutm e nt placed i n the mout h. Hi gh precisi on i n t ransfer of cli nical conditi ons to dent al laborator y is one of the most import ant factors in fabri cati on of the prosthesis with excell ent fi t for ei ther nat ural t eeth or imp lants. Therefore the ess ential fi rst st ep for fabri cat ion of a success ful implant -support ed prosthesis is accurat e trans fer of three -di mens ional implant posi tion and angul ati on from the mout h t o t he m ast er cast vi a impress ion [5,6]. Inaccurat e posit ion of the impl ant in the m ast er cast makes it i m pos sibl e to fabri cat e a well -fit ting pr osthesi s , and the result ant mi sfi t can l ead to biom echani cal compl icati ons such as screw looseni ng[7],bone loss[8],and cerami c veneer fract ure as a result of increasing stres s wit hin the prosthesi s or at t he int erfac e of t he im pl ant and bone.
Discussion
Page 40
As dis cuss ed earlier impl ant l evel i mpression t echniques ar e of two t ypes – the open tra y and the closed tra y t echnique. The open tra y techni que involves fast eni ng an im press i on copi ng to t he im plant wit h a screw that proj ect s above t he hei ght of the coping and t hrough an opening cut i n a cus tom impression tra y. T he s crew is loosened when the m at eri al is s et and the tra y is removed from the mout h with the impress ion coping retained wit hin t he im pressi on. An impl ant analog is fastened to the impressi on copi ng usi ng the s am e screw. The open t ra y techni que allows for the impression coping to rem ain in the im pressi on. This reduces the effect of t he im plant angul ation, the de formation of the im press ion m at erial upon recover y from the mouth, and rem oves the concern for repl acing the coping back int o its res pecti ve space i n the im pressi on. Dis advant ages of this t echnique are that there are more parts t o control when fast ening, there m a y be som e rotati onal movement of the im pressi on coping when s ecuring the impl ant analog, and blind att achm ent of the implant analog to the im press ion coping ma y result in a mis fit of components.[12,13] Our st ud y has concluded that open tra y impressi on technique has bett er dimensional accurac y when com pared to cl osed t ra y im pression technique.
Discussion
Page 41
and 30 degrees ) and impressi ons were m ade wit h pol yet her i mpressi on mat eri al s and concluded t hat metal -splinted di rect technique produced the most accurate casts.
Michael Stimm elm ayr et al 2012[21] studi ed open and cl osed tra y im pres sion techniques for four impl ant ins erted nearl y bilat eral i n ten edentulous j aws . The y found that the dis crepanc y bet ween the splint ed pi ck -up im pression t echnique and the transfer t echni que were in a range wit h cli nical influence and for bett er accurac y of impl ant -support ed prosthodontics, the spli nted pick -up technique s hould be used. [22] Simil ar st ud y b y t he sam e aut hors to eval uate t he accurac y of three di fferent impressi on techniques di git all y and concluded that for bet ter accurac y of impl an t-supported prosthodont ics, the spli nted pick-up t echni que s hould be used for impress ions of four implants evenl y s pread i n edentulous j aws.
Discussion
Page 42
bet ween impl ants were m easured using a traveling m icros cope and found that t here was no st atisti call y si gnifi cant di fference between t he direct uns plint ed and splint ed t echni ques whil e the i ndi rect techni que was st atis ticall y si gnifi cantl y di fferent from the other two t ech niques .
Naconec y M M et al in 2004[25] evaluat ed the deformat ion of a met alli c fram ework connected to 15 s tone cas ts fabricat ed usi ng 3 trans fer t echniques to det erm ine the most accurat e i mpressi on procedure. The y concluded t hat the di rect splinted t echni que was t he most accu rat e trans fer m ethod for mul tiple abutm ent s compared to direct nonspli nt ed and indirect t echniques. [26] A stud y b y Assi f D et al i n 1993 st udi ed four im pression procedures for accurac y i n a laborator y model t hat simul at ed cl ini cal practi ce. The accurac y of stone casts with bras s impl ant analogs was meas ured agai nst a standard fram ework us ing a di git al mi cros cope and concluded t hat when impress ions were made b y removing an i mpres sion from smoot h trans fer copings and repl acing the copings in the impres sion, the majorit y of casts were unaccept abl e.
Discussion
Page 43
Rutkunas Vet al 2012[27] eval uat ed t he effects of 5 - and 25-degree im pl ant angul ations i n si mulat ed cli nical cast s on an impress ion 's accurac y when using di fferent impressi on mat eri al s and tra y s el ections and concl uded t hat increas ed angul ation tended to decreas e im pres sion accurac y wit h the open -t ra y technique was mo re accurat e wit h hi ghl y non axi all y ori ent ed implants. [28] Si-Hoon J o et al 2010 com pared t he accurac y of the im plant mast er cast accordi ng t o the t ype (pi ck -up, trans fer) and the length (l ong, short) of the impress ion copi ngs and concl uded that pick -up t ype im pres si on coping exhibit ed a si gnifi cantl y l ower error rate than the t rans fer t yp e.
Lee YJ et al 2009[29] eval uated the accurac y of four i mpl ant-level i mpression t echniques wi th opti cal micros cop y on two angul ated conical int ernal connection im pl ants . A mast er cast with t wo int ernal -connecti on impl ant anal ogs angul ated 10 degrees from each ot he r and a mast er fram ework were fabri cat ed and concluded that the cast s produced from nonoct agonal pi ckup impression t echni ques were more accurat e than thos e produced usi ng transfer impressi on t echni ques.
Cabral LM et al in 2007 [30] invest i gated 4 impression techni ques t o determ ine thei r dim ensi onal accurac y in comparison wit h a st andard t echni que and concl uded that the direct i mpressi on techni que with squared transfer copings with acr yl i c res in spl ints
Discussion
Page 44
impress ion procedures usi ng t wo impression t echniques and t wo different mat eri als and c oncluded that the repositioning i mpressi on techni que at t he im plant l evel produced less predi ct abl e results t han the pi ckup technique at the abutment l evel. The choi ce of i mpression m at eri al m ade no si gnificant di fference. The y also com pared the effect of impression t echnique al ong wi th i mpressi on mat eri al t o ass ess di mens ional accurac y i n 40 l ab produced casts. The y concl uded that t he open t ra y technique produced bett er di mens ional accurac y with l ess er rot ational errors than cl os ed tra y technique due t o greater errors in anal ogue positi on when compared to i mpressi ons.
Discussion
Page 45
Sabour y A et al [34] compared the accurac y of four impressi on -maki ng t echni ques i n angul at ed im plant s based on verti cal gap and anal ys ed four groups of fi ve s ampl es were - cl os ed -tray s nap -fi t trans fer, open -t ra y non spli nted i mpression copi ng, m etal spli nted impress ion coping, and fabri cated acr yl ic resi n transfer cap. A gol d -pall adi um fram ework was fabri cat ed over the angul at ed implant abutments, the fi t of which was used as reference. The gaps bet ween the m et al fram ework and the impl ant analogs were m easured in sam ple groups . The y concl uded that m et al s pl inted impressi on coping and fabri cat ed acr yli c resin transfer cap techniques produced quite more accurat e im press ions than closed -t ra y snap-fit t rans fer.
Özçelik[35] TB compared the Dim ensi onal Accurac y of Four Different Impl ant Im pression Techniques in parall el m andibul ar implants di gitall y wi th a l as er opti cal s canner and ali gned b y obs erving the superpositi ons of the anat omical landmarks using a software progr am. The groups were closed tra y impress ions with and without plas tic caps, open tra y impressions with a direct s plint ed t echnique and an im proved direct splint ed technique. The results showed l es ser dimensional accuracy in cl os ed t ra y impressi on t echnique group.
Discussion
Page 46
tapered copi ngs not splint ed (custom clos ed tra y) and t en square copings spli nted with acr yl ic - resi n (cust om open t ra y) with pol ys ulfide im pres si on m at erial s and concl uded t hat the cus tom open tra y t echni que was t he m ost accurat e im pressi on for multi pl e impl ants com pared with clos ed custom t ra y.
Hakim eh Siadet et al[37] com pared the two im press ion techni ques for all on four protocol. The y concl uded that open t ra y techni ques were more accurate and caus ed l ess er di mens ional inst abilit y.
Discussion
Page 47
splinti ng is mai nl y emplo yed whil e t aki ng open -tra y impressi ons onl y. In our stud y, we compared the effi ci ency of the open and cl osed -t ra y impress ion t echniques. Hence the factor of s plinti ng i s not i ncluded in our stud y. The open t ra y t echni que is more accurat e when done properl y becaus e the coping locks into t he impression m at erial and is not removed b efore fabri cati ng a model . However closed t ra y techni que are i deal for s ingl e unit im pl ant restorat ions. This t echnique can be used for multi pl e units, provided t he y are paral lel . St ock im pressi on tra ys are us ed for the closed tra y technique. If impl ant s are not parallel , the cl osed t ra y t echnique can cause the impressi on to lock int o the patient’s mouth. Closed tray can be inaccurate if the impression coping i s not placed back int o the impress ion properl y before fabri cating m odels for t he case.[38]
Ver y few s tudi es have found the clos ed t ra y i mpres sion techni que t o be superi or to open t ra y i mpressi on technique. Contrar y to much favoured open t ra y impressi on t echni ques stud y b y Balouch F et al [39] on comparing dim ensional Accurac y between Open -Tra y and Closed-Tra y Impl ant Im pres sion Technique in 15° Angl ed Im plants and concl uded that closed i mpression technique had less di mens ional changes in comparis on with open tra y m ethod.
Discussion
Page 48
existing im pl ants for fixed parti al dent ures were i ncluded. Group I (cl os ed -t ra y) and group II (open -tra y) were com pared u si ng microcomput ed t om ograph y scanning. No st atisti call y si gni fi cant differences were found bet ween the cl os ed - and open-tra y techniques . Na yereh R ashidanet 2012 [41] compared the accurac y of t wo different impress ion t echniques with t wo di fferent impressi on coping s hapes using pol yet her impression m at eri al t o obt ain precis e defini tive cast s. Two reference acr ylic resi n wit h fi ve internal connection impl ants having different shapes of im pres sion copings were fabri cat ed. Twent y medi um‐consist enc y pol yether i mpres sions of these models were made with s quare and conical impressi on copings of each s ys t em usi ng open‐t ra y and clos e‐tra y techniques . M at ching impl ant repl icas were screwed into the im pressi on copings in the im pres sions. Impressi ons were poured wit h t y pe IV st one, and t he positi onal accurac y of t he implant repli ca heads in x‐, y‐, and z‐axes and als o rot ational displ acem ent were evaluat ed usi ng a coordinat e m easuring machi ne. The y found no si gnificant di fference bet ween di rect and indi rect impress ion techniques.
Discussion
Page 49
vitro of clos ed and open t ra y impressi on techniques for Nobel Active implants pl aced at vari ous angulat ions. Twel ve open t ra y and 12 clos ed tra y impressi ons were m ade. Occlusal , lat eral , and frontal vi ew photographs of the resul ting cast s were used to meas ure t he linear and angul ar displ acement of implant analogs and no si gni fi cant di fference was found in the im pressi ons m ade of Nobel Active im plants with the open or clos ed tra y t echni ques. The y concluded both t echni ques had no effect on Nobel i m plant s ystem s. Also studi es b y Hami dreza R aj ati Haghi et al [44] conc l uded that both i mpres si on t echni ques produce sam e dimensi onal accurac y wi th no statis tical s i gni fi cance.
Discussion
Page 50
Chang WG et al 2012[46] com pared the ac curac y of cast s m ade using three di fferent impressi on techniques to obt ain an accurate definit ive cast for fabri cati on of m ultiple -impl ant prosthes es. Twel ve experim ent al groups were form ed com bi ning t he foll owi ng conditi ons: three impression t echniques , t wo impres sion m at eri al s, and two cast mat eri al s. The m ai n effects of the t hree factors were anal yz ed b y three -wa y anal ys is of vari ance using the ful l factorial general linear m odel bet ween factors. The res ults showed that there were no si gnificant differen ces in m ean val ues for the transferred dim ensions bet ween the control and experim ent al groups. None of the meas urem ents in the horizont al plane of the definiti ve casts dem onst rated s igni ficant differences am ong t he impressi on t echni ques wit h different impr essi on and cas t m at eri als .
Discussion
Page 51
coping/l aborat or y analog positi oned in t he impression using a touch -probe coordi nate m easuring m achi ne. Within the limit ations of the in vitro stud y t he y concluded that t he open - and cl os ed -tra y t echni ques had no effect on t he accurac y of multi ple impl ant im press ions. The interact ion between impress ion technique and impl ant angul ation was also not si gni fi cant.
Discussion
Page 52
Herbst D et al in 2000 [50] eval uated and com pared 4 impressi on techni ques in t erms of thei r dim ens ional accurac y to reproduce impl ant positi ons on worki ng casts and concluded t hat the di mens ional accurac y of all t he techniques was excepti onal and t he obs erved differences can be regarded as cli ni cal l y negli gible. [51] Spector MR et al 1990 creat ed an experiment al model was devel oped to test the accurac y of open and closed t ra y i m pressi on techniques and the com ponent s us ed t o make the t ransfer records . St atisti call y, no si gni fi cant difference was found between the t hree m ethods t ested. [52] Al-Abdull ah K et al 2013 eval uated the accurac y of the Robocasts and com pare them t o those defi nitive casts fabricat ed with conventional implant impressi on techni ques (open tra y wit h spl int ed impress ion copings t echnique) and concl uded that accurac y of fit was not infl uenced b y t he im plant angul ation or positi on for either i mpressi on techni que or b y the Encode heal ing abutment hei ght for t h e Encode impress ion technique.
Discussion
Page 53
com bined i nt eraction of impressi on t echnique, im pl ant angul ation, and implant num ber has on the accurac y of implant defi nitive multi -unit abutment cast s. The average angl e errors for t he closed and open tra y impress ion techniques did not di ffer si gnificant l y and there was no interpretabl e patt ern of average angl e errors in t erm s of im plant angul ation and im plant num ber. The magnitude o f distortion was similar for all combinati ons of im pressi on t echnique, impl ant angul ation, and impl ant num ber.
From the above cit ed literature we can concl ude that the open -tra y im pres sion t echnique was m ore accurat e t han t he cl osed -t ra y impress ion t echnique for compl et el y edentulous pati ent s, but there seems to be no di fference for partiall y edentulous pat ients and t he accurac y of im plant impressions is affect ed b y the impl ant angul ation when it is great er than 20 degrees for parti all y and compl etel y edent ulous pati ents . No previous studies were done t o compare the open and clos ed tra y impression t echniques whi le usi ng multi -unit abutment.
Discussion
Page 54
Conclusion
Page 54
Im pression is the most import ant st ep in impl ant ret ai ned prosthesis . The best and accurat e impression will l ead to passi ve fit and accurac y of t he prosthesi s. Di fferent techniques are availabl e till dat e to m ake impres sions for impl ants. No singl e technique is suit abl e for all cases . The s el ect ed t echni que should sui t the indivi dual cas e. However the t ype of t echnique is al so strongl y dependent on the clinician’s skill. Hence an impression technique, ideal for the selected indivi dual and the cli ni ci an’s skill must be chos en to deliver a prosthesis that pas sivel y fits the im plant and results in l ess er biological and m echani cal com pli cations and resul t i n longevit y of the implant restoration.
Bibliography
Page 55
1. The Gl oss ar y of Pros thodonti c t erms –Ni nth Edition
2. Gupt a A, Dhanraj M , Sivagami G. Status of surface t reatm ent in endoss eous impl ant: a literar y overview. Indi an j ournal of dental research. 2010 J ul 1; 21(3): 433 .
3. Jayes h RS, Dhinakars am y V. Osseointegrati on. J ournal of pharm ac y &bioalli ed sci ences . 2015 Apr; 7(Suppl 1):S 226 .
4. Ga yat hridevi S.K, HarshitaGowda, Vaishali K and Suma. Im pression t echni ques i n implants. J ournal of Dent al & Oro -faci al R es earch Vol 12 Issue 02 Aug 2016 .
5. Wee AG, Aqui l ino S A, S chnei der R L. St rat egi es t o achieve fit in implant prosthodont i cs: a revi ew of t he literature. Int ernati onal Journal of P rosthodontics. 1999 M ar 1; 12(2) .
6. Karl M, Wint er W, Ta yl or TD, Heckm ann SM . In vit ro study on pas sive fit i n im pl ant -s upport ed 5 -unit fixed parti al dentures. Int ernational J ournal of Oral & M axillofaci al Im pl ants . 2004 J an 1;19(1).
7. Al-Turki , J . Chai, E. P. Laut ens chl ager, and M. C. Hut ten, “Changes in prosthetic screw stability because of misfit of implant -support ed prostheses,” In t ernational
8. T. Jemt and K. Book, “Prosthesis misfit and marginal bone loss in edentulous implant patients,” International Journal of Oral and Maxillofaci al Implants, vol. 11, no. 5, pp. 620 –625, 1996.
Bibliography
Page 56
technology for im plants consi dering operator experience, im plant angul ation, and depth. Cli nical i mpl ant dentist r y and rel at ed research. 2015 J an;17:e54 -64 .
10. Lee H, So J S, Hochs tedl er J L, E rcoli C . The accurac y of implant impress ions : a s ys t em ati c revi ew. The J ournal of prostheti c dentist r y. 2008 Oct 1;100(4):285 -91.
11. Chia VA, Es guerra R J , Teoh KH, Teo J W, Wong KM, Tan KB. In Vitro Three -Dim ensional Accurac y of Di gital Im plant Im pressions: Th e Effect of Im pl ant Angul ation. Int ernati onal Journal of Oral & M axillofaci al Impl ants . 2017 Mar 1;32(2) . 12. Carr AB. A Comparison of Im pression Techniques for a Fi ve
-Im pl ant M andibular Model . Int ernational J ournal of Oral & Maxillofaci al Implants. 1991 Dec 1 ;6(4) .
13. Carr AB. C ompari son of impression t echniques for a two -implant 15-degree di vergent model. Int ernational J ournal of Oral and Maxillofaci al Implants. 1992 Dec 1;7:468 .
14. Burns J , Palmer R, Howe L, Wilson R . Accurac y of open t ra y implant i mpres sions : an in vit ro compari son of s tock versus cust om tra ys . The J ournal of prostheti c dentis tr y. 2003 Mar 1;89(3):250 -5.
Bibliography
Page 57
16. Conrad HJ , P esun IJ , DeLong R, Hodges J S. Accurac y of two impress ion t echni ques wit h angul at ed i mplants. The J ournal of prostheti c dentist r y. 2007 J un 1; 97(6):349 -56.
17. Pande y KK. A Begi nners Gui de for Implant Impressi on: R eview Arti cl e. Int J Oral Health Med R es 2017; 4(1):91 -93.
18. Im pression t echni ques i n dent al im plant ology. A revi ew arti cl e. Sprashgarg. TMU J dent .
19. Amin S , Weber HP , Finkelm an M, El Rafi e K, Kudara Y, Papasp yri dakos P. Digital vs. convent i onal full‐arch implant impress ions : a com parative st ud y. Clin. Oral Impl.
Res . 28, 2017, 1360– 1367 .
20. Martínez -R us F, Garcí a C, Santam arí a A, Özcan M, P radí es G. Accurac y of definit ive casts usi ng 4 i mplant -level impres sion techni ques i n a s cenari o of multi -implant s yst em wit h di fferent implant angul ations and subgi ngi val al ignm ent level s. Implant dentist r y. 2013 J un 1;22(3):268 -76.
21. Stimmelm a yr M, Güt h J F, Erde lt K, Happe A, S chl ee M , Beuer F. Clinical stud y eval uati ng the discrepanc y of t wo different impress ion t echniques of four i mpl ants in an edent ulous j aw. Clinical oral investi gations. 2013 Nov 1; 17(8):1929 -3 5.
Bibliography
Page 58
23. Al Quran FA, R ashdan BA, Abu Zom ar AA, Weiner S. Pass ive fit and accurac y of t hree dental i mpl ant impress ion t echniques. Quint es sence International. 2012 Feb 1;43(2) .
24. Most afa TM, El gendy MN, Kashef NA, Halim MM. Evaluati on of the precision of three impl ant t rans fer impress ion t echni ques using two el astom eri c im pression materi als. Int ernational J ournal of P ros thodont ics. 2010 Nov 1; 23(6) .
25. Naconec y M M, Teixeira ER , Shinkai RS, Fras ca LC, Cervi eri A. Evaluation of the accurac y of 3 t ransfer techni ques for impl ant -support ed prost hes es wit h m ult ipl e abutm ents . Int ernati onal Journal of Oral & M axillofaci al Impl ants . 2004 Mar 1;19(2) . 26. Assi f D, Fenton A , Zarb G , S chmitt A . com parative accuracy of
implant impressi on procedures. Int J Peri odonti cs R estorat ive Dent. 1992;12(2): 112 -2 1.
27. Rutkunas V, Sveikat a K, S avi ckas R. Effect s of im plant angul ation, m at eri al sel ection, and im pressi on t echni que on impress ion accurac y: a prelim inary l aborator y s tud y. Int ernational J ournal of Prosthodonti cs. 2012 S ep 1;25(5) .
28. Si-Hoon J o,, K yo ung-Il Kim, J ae-Min S eo, Kwang-Yeob Song, , J u-M i Park, Seung-Geun Ahn. Effect of im pression copings and impl ant angul ati on on the accurac y of impl ant impress ions - an invitro stud y. J Adv Prost hodont . 2010 Dec; 2(4): 128 –133.