Purpose: Critical Access Hospitals (CAH) utilize swing beds for inpatient and post-acute care. For services provided in swing beds, CAHs are reimbursed by Medicare based on
reasonable costs incurred while providing care. Post-acute care that occurs outside of CAHs is reimbursed based on the Skilled Nursing Facility Prospective Payment System (SNF PPS), which pays less than cost-based reimbursement. Policymakers have considered changing CAH swing bed reimbursement to the SNF PPS in recent years to decrease Medicare spending. This study aims to measure the impact of this change in reimbursement on CAHs.
Methods: This study uses cost report data from 2015-2017 to estimate the change in operating margin that CAHs would have experienced if this change in reimbursement occurred. Multivariate regression analysis is conducted to determine if certain CAHs are disproportionately impacted based on certain characteristics. Lastly, community characteristics were analyzed for the CAHs most and least affected by the change.
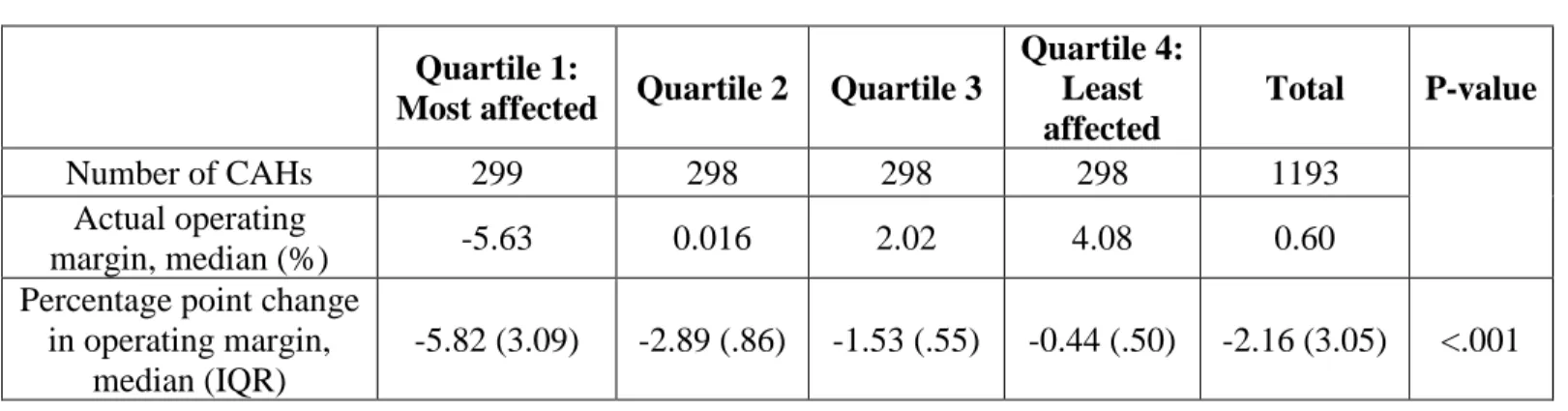
Results: The median change in operating margin for all CAHs in 2016 is estimated to be -2.16 percentage points. The vast majority of CAHs would experience a negative change in operating margin. The change would disproportionately impact CAHs that are smaller, more rural, located in the South, and rely more heavily on swing beds. Additionally, the CAHs more adversely impacted serve communities with higher percentages of racial/ethnic minorities and poorer overall health outcomes.
Discussion: Changing Medicare CAH swing bed reimbursement would have a significant impact on CAH financial viability. Considering the rising number of rural hospital closures in the past decade, this change could put more financial stress on hospitals that are already
1 Introduction and Background:
Approximately sixty percent of community hospitals in the United States are located in rural areas.1 Many rural hospitals are struggling financially because of declining revenue and patient volume,2 which can be seen in the increasing number of rural hospital closures over the last 10 years.3 Hospital financial instability and closures can create significant access barriers for rural residents,4 who already have higher levels of chronic disease, worse health outcomes, and lower per capita income.5 Additionally, rural hospitals are often a major player in the local economy, contributing jobs and attracting other
industries to the area.6 For this reason, Congress has created several programs to preserve access to health care in rural areas.
One such program, the Medicare Rural Hospital Flexibility Program (Flex Program), was created in 1997 as part of the Balanced Budget Act (BBA). The Flex Program aimed to address rural hospital financial viability following a wave of closures after implementation of the Inpatient Prospective Payment System. The program created the Critical Access Hospital (CAH) designation for rural hospitals, which qualifies certain hospitals for cost-based reimbursement from Medicare based on reasonable costs for inpatient and outpatient services.7i The Social Security Act created the swing bed
agreement, which allows qualifying small rural hospitals to have beds that “swing” between
2 Swing beds are an important source of post‐acute care, benefiting both rural
residents and providers.10,11 For 4.1% of the rural population residing in a non‐core based statistical area, swing beds provide the only available access to post‐acute care.10 Moreover, rural hospitals – particularly Critical Access Hospitals (CAHs) – rely on swing beds to help them better manage patients and staffing and to help ensure financial stability of their organizations.11 While the number of swing bed days has been growing since the early 2000’s,10,11 swing beds currently represent only 1 to 2 percent of total Medicare
fee-for-service skilled care days in rural areas.10
Despite being a small portion of Medicare’s total spending on skilled nursing care,
swing beds have received a disproportionately large share of attention. Several reports from the Medicare Payment Advisory Commission (MedPAC) have raised concerns that the current reimbursement formula results in relatively higher payment for swing bed care provided in CAHs, and thus greater use and cost to Medicare.12,13 Similarly, a March 2015 report by the Office of Inspector General (OIG) estimated potential savings to Medicare if swing bed reimbursement were changed to reflect that of other facilities offering similar SNF-type services.14
In November 2017, the House Ways and Means Committee announced a bipartisan Medicare extenders package.15 The package included several offset policies including “Modification of payments for critical access hospital swing beds, including the
U.S. Department of Health and Human Services (HHS) Office of Inspector General (OIG) recommendations and regulatory relief.” The proposed policy would change swing-bed
3 heavily criticized by the Critical Access Hospital Coalition,17 the American Hospital
Association,18 and the National Rural Health Association,19 and ultimately was not implemented.20 However, the controversy surrounding Medicare reimbursement of swing beds in CAHs continues.
Despite this controversy, no research has been conducted to determine the average net effect a change from cost-based reimbursement to the SNF-PPS would have on CAH profitability. This study aims to fill that gap and determine whether certain CAHs would be more affected by the change than others. Additionally, this study will analyze the
community characteristics of the CAHs that are most and least affected by the change in reimbursement.
Methods
Study Design
This retrospective, observational study is conducted in two stages. The first stage is descriptive and uses cross-sectional data from each of the years 2015, 2016 and 2017. The second stage uses descriptive analysis and multivariate regression analysis on unbalanced panel data from 2015 to 2017.
Study Sample and Data
The study sample includes all U.S. Critical Access Hospitals (CAHs) that have annual Medicare cost reports covering at least 360 days and report at least one day of patient care in a swing bed in any of the years 2015, 2016 or 2017. Certain observations were dropped due to inconsistent or missing data. Rural is defined as micropolitan or noncore-based statistical areas as determined by the Office of Management and Budget, and areas with Rural Urban
4 CAHs in 2015, 1193 CAHs in 2016 and 1055 CAHs in 2017. Study data are drawn from
multiple secondary sources. Medicare cost report data come from the Centers for Medicare and Medicaid Services’ (CMS) Hospital Cost Reporting Information System (HCRIS). Information
on hospital location is obtained from the CMS Provider of Services (POS) Current File. Data to construct hospital markets are drawn from the Hospital Service Area File. Demographic and health status data used to study hospital community characteristics come from the Neilsen Claritas PopFacts File and County Health Rankings, respectively.
Data Analysis
The key dependent variable of interest is the change in a hospital’s operating margin that
would result if Medicare swing bed reimbursement to CAHs is changed from the current cost-based method to the Medicare Skilled Nursing Facility (SNF) prospective payment system (PPS). Operating margin measures the profitability of a hospital’s core operations and is defined
as [(operating revenue minus operating expenses) / operating revenue].22 The first stage of the analysis estimates the median net effect on operating margin of switching Medicare CAH swing bed reimbursement. The second stage of the analysis utilizes multivariate ordinary least squares regression to determine if hospitals with certain characteristics are disproportionately affected by the change in reimbursement. Additionally, the second stage assesses whether community demographic or health status characteristics are associated with the change in operating margin. Stage 1: Determining the Net Average Effect on Operating Margin
Medicare currently reimburses CAHs for routine care provided in either an acute
inpatient bed or a swing bed based on the average daily costs to the hospital of providing acute, swing bed, and observation care. The formula for this reimbursement is shown in Equation (1):
5 In Equation (1), Reimbursement is the total payment from Medicare for the routine cost portion of Medicare-covered acute and swing bed days. Total Routine Inpatient Cost reflects total routine inpatient operating costs reported on the Medicare Cost Report. The cost of nonskilled post–acute swing bed days is represented by Swing NF Medicaid Cost. Since nonskilled swing bed days are reimbursed by Medicaid, this cost is subtracted from total inpatient cost. The remaining inpatient routine cost is divided by the sum of all Acute Days, skilled swing bed days (Swing SNF Days), and Observation Days to arrive at the inpatient routine cost per diem. The resulting per diem is then multiplied by the numbers of Medicare acute days and Medicare skilled swing days to calculate the hospital’s Medicare reimbursement for inpatient routine care.23
The SNF PPS reimburses skilled nursing facilities by first providing a base rate per day. From there, Medicare adjusts the base rate based on geographic factors such as labor costs. This rate is then further adjusted to account for case mix. A day of patient care is assigned to one of 66 resource utilization groups (RUGS) that are weighted based on how resource intensive the care is expected to be (See Appendix 1).24
This study uses the Medicare cost report formula outlined in Appendix 2 to estimate each hospital’s total Medicare reimbursement for routine inpatient care assuming reimbursement of
6 compared to the operating margin under cost-based reimbursement (See Appendix 3). The
median across all CAHs is used to determine the net change in operating margin caused by changing the reimbursement model.
Stage 2: Regression Analysis and Community Characteristics
7 Next, CAHs are categorized as “most affected” and “least affected” based on quartiles of the simulated change in operating margin. CAHs in quartile 1 are considered most affected and those in quartile 4 are considered least affected. For the CAHs in each of these categories, average demographic and health status characteristics in the hospital communities are analyzed to determine whether there are statistically significant differences between the two groups. Statistical significance is measured using one-way analysis of variance tests (ANOVA). Demographic characteristics including population, population greater than 65 years of age, sex, unemployment, per capita income, unemployment rate, and race are measured at the hospital market level. Health status, including percent in fair/poor health, percent with inadequate social/emotional support, and years of potential life lost, are measured at the county level. Results
8 operating margin declined from an already negative value to a more negative one, while an additional ten percent of CAHs moved from a positive to a negative operating margin.
Table 1. Sample Summary Statistics and Change in Operating Margin for the Year 2016
Quartile 1:
Most affected Quartile 2 Quartile 3
Quartile 4: Least affected
Total P-value
Number of CAHs 299 298 298 298 1193
Actual operating
margin, median (%) -5.63 0.016 2.02 4.08 0.60
Percentage point change in operating margin,
median (IQR)
-5.82 (3.09) -2.89 (.86) -1.53 (.55) -0.44 (.50) -2.16 (3.05) <.001
Table 2. Characteristics of Change in Operating Margin in 2016
Change in operating margin
(2016) # of CAHs
Negative to more negative 561
Positive to negative 122
Positive to less positive 510
Table 3 presents the results of the multivariate regression analysis, showing the
relationship between the hospital characteristics (independent variables) and change in operating margin for the years 2015 through 2017. Among the measures of rurality, miles to nearest SNF and being in an isolated rural area relative to a small rural area both showed statistically
9 million dollar increase in net patient revenue, all else equal, there is a 0.3 and 0.014 percentage point change in operating margin, respectively. Among the geographic location variables, the dummy variable of being located in the South relative to the Midwest was statistically significant and was associated with a -0.54 percentage point change in operating margin, all else equal. The presence of long term care at a hospital was associated with a 1.1 percentage point change in operating margin, all else equal. For every 1 percentage point increase in Medicare share and 1 day increase in swing bed ADC, all else equal, there is a 1.5 and -0.71 percentage point change in operating margin, respectively.
Table 3. Multivariate Regression Analysis of Change in Operating Margin for the years 2015-2017
Coefficient (β) 95% Confidence Interval Measures of rurality
Miles to nearest SNF -0.00021 *** [-0.00033 , -0.00093]
Urbana -0.0097 [-0.023 , 0.0033)
Large rural area -0.0041 [-0.0092 , 0.00092]
Isolated rural area -0.011 *** [-0.015 , -0.0073] Measures of size
Acute average daily
census 0.0030 *** [0.0023 , 0.0037]
Net patient revenue
(millions) 0.00014 *** [0.00005 , 0.00023]
Measures of geographic location
Northeastb 0.0035 [-0.0018 , 0.0088]
South -0.0054 ** [-0.010 , -0.00040]
West -0.0015 [-0.0063 , 0.0034]
Other measures Presence of long term
care 0.011 *** [0.0074 , 0.015]
Medicare share of patient
population 0.015 ** [0.00021 , 0.031]
Swing bed average daily
census -0.0071 *** [-0.0092 , -0.0050]
***p<.001 **p<.05
10 and Metro CBSA. Large rural area: RUCA<7 and non-urban. Small rural area:
7<RUCA<10 and non-Metro CBSA (omitted in the regression analysis). Isolated rural area: RUCA=10.
b. Northeast, South, and West are based on census region classifications from the US Census Bureau. The Midwest region was omitted in the regression analysis.
11 Table 4. Characteristics of the Communities Served by the CAHs that are Most and Least Affected by the Change in Reimbursement
Characteristics Quartile 1: Most affected Quartile 2 Quartile 3 Quartile 4: Least affected
Total
P-value
Demographic, mean
Total population 22637 25505 25639 43088 29200 <.001
Percent white 81.0 86.8 88.7 87.0 85.9 <.001
Percent black 8.4 3.9 3.4 3.8 4.9 <.001
Percent Hispanic 10.0 7.9 6.7 8.1 8.2 0.01
Percent age 65 or older 19.1 19.8 20.2 19.5 19.7 0.10
Percent female 49.6 49.4 49.6 49.7 49.6 0.27
Health, mean
Percent in poor or fair
health 16.8 15.2 14.9 15.5 15.6 <.001
Years of potential life lost 8479 7674 7451 7590 7787 <.001 Percent with no social or
emotional support 18.1 17.8 16.7 14.7 16.8 <.001
Economic, mean
Poverty rate 12.3 11.3 11.0 11.4 11.5 0.01
Per-capita income 24581 24906 24970 24752 24802 0.73
Unemployment rate 7.2 7.2 7.7 8.5 7.7 <.001
Limitations
There are several limitations to this study’s design. First, CMS issued a final rule in July
12 swing bed reimbursement. Any changes in hospitals’ use of swing beds could have an impact on
the results; however, the direction of the effect is not known because it would depend on the behavior of each hospital. Finally, the analysis assumes that the Medicare cost report formulas used to determine hospital reimbursement, including the swing bed carve-out, would remain unchanged.
Discussion and Implications
The purpose of this study was to estimate the financial impact on CAHs of changing the Medicare reimbursement method for swing bed days from cost-based to the SNF PPS. Results showed that this change would have a negative profitability impact on virtually all CAHs, with a median change in operating margin of -2.16 percentage points. Approximately 60% of CAHs in the sample would have a negative operating margin following this change. Since operating margin is an important indicator of financial health for hospitals,22 this could have significant consequences for CAH viability. The loss in profitability is due to the SNF PPS having lower reimbursement rates than cost-based reimbursement.
13 source for the CAH. Medicare share likely resulted in larger transfers of fixed costs back to acute inpatient days, therefore counteracting the effect of the reduction in swing bed reimbursement.
Lastly, this study found statistically significant differences in community and
demographic characteristics between the most and least affected CAHs. The quartile 1 hospitals served communities with a higher percent of racial and ethnic minorities, poorer overall health outcomes, and a higher poverty rate. Additionally, quartile 1 CAHs serve communities with smaller total populations, which is in agreement with regression results for rurality. The
unemployment rate in quartile 4 communities was higher than in quartile 1 CAHs. More research is needed to understand this relationship.
Considering the increasing rate of rural hospital closures in the last decade3 and the increasing risk of financial distress among rural hospitals,28 this change could have a significant impact on CAH financial viability. If policymakers choose to make this change in reimbursement, it would be important to consider potential ways to offset the significant losses that some CAHs would face. This study also demonstrates that many of the hospitals adversely impacted by this change serve disadvantaged communities and vulnerable
populations. A hospital closure in these communities could exacerbate already existing socioeconomic and health disparities.
Acknowledgements
Randy Randolph, MRP, Ann Howard, and Roger Thompson, CPA provided assistance with data and methods.
Funding
16 Appendix 2. Formula for Stage 1 Analysis
Calculation
Acute care days -
Medicare
Total Swing-bed SNF -
Medicare Total Observation days Observation cost Observation charges
Medicare observation charges
Inpatient days, excluding swing-bed and newborn = Total acute care days + observation
days Swing-bed SNF days through Dec. 31st
Swing bed SNF days after Dec. 31st
Medicare rate for swing-bed SNF services through Dec. 31st Medicare rate for swing-bed SNF services after Dec. 31st Total general inpatient routine costs
Swing-bed costs applicable to NF-type services through Dec. 31st Swing-bed costs applicable to NF-type services after Dec. 31st Total swing-bed costs
General inpatient routine costs
Program general inpatient routine costs Total Medicare swing-bed routine costs Inpatient routine services - swing-bed SNF Ancillary services - swing-bed SNF
Subtotal
= Inpatient routine services swing-bed SNF + ancillary services swing-bed
SNF Inpatient services
Average State Rural RUGS rate
Change in CAH Medicare swing-bed SNF reimbursement -
If Swing-bed SNF services are paid using applicable RUGs rate If no carve out of swing-bed SNF routine costs on wkst D-1
Medicare swing bed days = Medicare swing bed SNF days
Average state rural RUGS rate = Average state rural RUGS rate
Rugs reimbursement = Medicare swing bed SNF days *
Average state rural RUGS rate
Current CAH swing-bed SNF reimbursement
= Inpatient routine services swing-bed SNF + ancillary services swing-bed SNF
Loss of CAH Medicare swing-bed SNF reimbursement (A)
17 Change in CAH Medicare inpatient acute reimbursement -
If swing-bed SNF routine costs are carved out on wkst D-1 Swing-bed SNF days -
Through December 31st = Swing-bed SNF days through
December 31st
After December 31st = Swing bed SNF days after December
31st Medicare rate for swing-bed SNF days -
Through December 31st = Medicare rate for swing-bed SNF
services thru December 31st
After December 31st = Medicare rate for swing-bed SNF
services after December 31st
Swing-bed services carve out
= [Swing-bed SNF days through December 31st * Medicare rate for
swing-bed SNF services thru December 31st] + [Swing bed SNF days after
December 31st * Medicare rate for
swing-bed SNF services after December 31st]
Swing-bed NF services carve out -
Through December 31st = Swing-bed costs applicable to NF
type services thru December 31st
After December 31st = Swing-bed costs applicable to NF
type services after December 31st
Total carve out
= Swing-bed services carve-out + swing-bed NF services carve out through Dec. 31st + swing-bed NF
services carve out after Dec. 31st
Total general inpatient routine costs = Total general inpatient routine costs
Net general inpatient routine costs = Total general inpatient routine costs –
total carve out
Inpatient days, excluding swing-bed and newborn = Inpatient days, excluding swing-bed and newborn
Adjusted general inpatient cost per day
= Net general inpatient routine costs/inpatient days, excluding swing-bed and newborn
Medicare acute care days = Medicare acute care days
Adjusted program general inpatient routine costs = Adjusted general inpatient costs per day * Medicare acute care days
Original program general inpatient routine costs = Program general inpatient routine costs
Difference
= Adjusted program general inpatient routine costs - Original program general inpatient routine costs
Cost-based reimbursement rate = Cost-based reimbursement rate
Additional CAH Medicare inpatient reimbursement (B) = Difference * cost-based reimbursement rate
18
If swing-bed SNF routine costs are carved out on wkst D-1
General inpatient routine costs = General inpatient routine costs
Inpatient days, excluding swing-bed and newborn = Inpatient days, excluding swing-bed and newborn
General inpatient cost per day
= General inpatient routine
costs/Inpatient days, excluding swing-bed and newborn
Adjusted general inpatient cost per day = Adjusted general inpatient cost per
day
Difference = Adjusted general inpatient cost per
day-general inpatient cost per day
Observation days = Observation days
Additional observation costs = Difference * observation days
Observation charges = Observation charges
Medicare observation charges = Medicare observation charges
Additional Medicare observation cost
= (Additional observation
costs/observation charges) * Medicare observation charges
Cost-based reimbursement rate = Cost-based reimbursement rate
Additional CAH Medicare outpatient reimbursement (C) = Additional Medicare observation cost * cost-based reimbursement rate
Change in CAH Medicare reimbursement -
If Swing-bed SNF services are paid using applicable RUGs rate If carve out of swing-bed SNF routine costs on wkst D-1
Loss of CAH Medicare swing-bed SNF reimbursement (A) = Loss of CAH Medicare swing-bed SNF reimbursement
Additional CAH Medicare inpatient reimbursement (B) = Additional CAH Medicare inpatient reimbursement
Additional CAH Medicare outpatient reimbursement (C) = Additional CAH Medicare outpatient reimbursement
19 Appendix 3. Actual and Simulated Operating Margin
𝐴𝑐𝑡𝑢𝑎𝑙 𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 𝑚𝑎𝑟𝑔𝑖𝑛 (𝑂𝑀) =𝑂𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 𝑅𝑒𝑣𝑒𝑛𝑢𝑒 − 𝑂𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 𝑒𝑥𝑝𝑒𝑛𝑠𝑒𝑠 𝑂𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 𝑟𝑒𝑣𝑒𝑛𝑢𝑒
𝑆𝑖𝑚𝑢𝑙𝑎𝑡𝑒𝑑 𝑂𝑀 = (𝑂𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 𝑟𝑒𝑣𝑒𝑛𝑢𝑒+𝑇𝑜𝑡𝑎𝑙 𝑐ℎ𝑎𝑛𝑔𝑒 𝑖𝑛 𝐶𝐴𝐻 𝑀𝑒𝑑𝑖𝑐𝑎𝑟𝑒 𝑟𝑒𝑖𝑚𝑏𝑢𝑟𝑠𝑒𝑚𝑒𝑛𝑡)−𝑜𝑝𝑒𝑟𝑎𝑡𝑖𝑛𝑔 𝑒𝑥𝑝𝑒𝑛𝑠𝑒𝑠
20 References
1. Fast Facts on U.S. Hospitals, 2018. American Hospital Association. https://www.aha.org/statistics/fast-facts-us-hospitals. Published 2018.
2. Connie Tai W-T, Porell FW, Kathleen Adams E. Hospital Choice of Rural Medicare Beneficiaries: Patient, Hospital Attributes, and the Patient–Physician Relationship. Health
Serv Res. 2004;39(6):1903-1922. doi:10.1111/j.1475-6773.2004.00324.x
3. 102 Rural Hospital Closures: January 2010 – Present. NC Rural Health Research Program. https://www.shepscenter.unc.edu/programs-projects/rural-health/rural-hospital-closures/. 4. Wishner J, Solleveld P. A Look at Rural Hospital Closures and Implications for Access to
Care: Three Case Studies. Kaiser Family Foundation. https://www.kff.org/report- section/a-look-at-rural-hospital-closures-and-implications-for-access-to-care-three-case-studies-issue-brief/. Published 2016.
5. Jones C, Ahearn M, Parker T, Mishra AK, Variyam J. Health Status and Health Care
Access of Farm and Rural Populations.; 2009.
https://www.ers.usda.gov/publications/pub-details/?pubid=44427.
6. Doeksen G, Schott V. Economic Importance of the Health-Care Sector in a Rural Economy. Rural Remote Heal. 2002;3(1):135.
7. Flex Program. National Rural Health Research Center. https://www.ruralcenter.org/tasc/flex.
8. Swing Bed Providers. Centers for Medicare and Medicaid Services.
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SNFPPS/SwingBed.html.
9. Reiter KL, Holmes GM, Broyles IH. Medicare, swing beds, and Critical Access Hospitals.
Med Care Res Rev. 2013. doi:10.1177/1077558712463247
10. Reiter K, Freeman V. Trends in Skilled Nursing Facility and Swing Bed Use in Rural
Areas Following the Medicare Modernization Act of 2003.; 2011.
http://www.shepscenter.unc.edu/rural/pubs/report/FR101.pdf.
11. Freeman V, Radford A. Why Use Swing Beds? Conversations with Hospital
Administrators and Staff.
12. Report to the Congress: Medicare and the Health Care Delivery System. Washington, DC; 2012.
13. Report to the Congress: Issues in a Modernized Medicare Program. Washington, DC; 2005.
14. General O of I. Medicare Could Have Saved Billions at Critical Access Hospitals If Swing Bed Services Were Reimbursed Using the Skilled Nursing Facility Prospective Payment
System Rates.; 2015.
15. Ways & Means Leaders Announce Bipartisan Medicare Extenders Package.; 2017. https://waysandmeans.house.gov/ways-means-committee-leaders-announce-bipartisan-medicare-extenders-package/.
16. Reiter KL, Holmes GM. A Critique of the Office of the Inspector General’s Report on Swing Beds in Critical Access Hospitals. North Carolina Rural Heal Res Progr. 2015;(March).
17. Tell Congress to Oppose Changes to Swing-Bed Reimbursements. CAH Coalition.
https://www.cahcoalition.com/congress-proposes-changes-to-swing-bed-reimbursements/. 18. Ways & Means Leaders Announce Medicare Extenders Package. American Hospital
https://www.aha.org/news/headline/2017-11-15-ways-and-means-leaders-21 announce-medicare-extender-plan. Published 2017.
19. Seigel J. Rural Advocates Stand Up for CAHs in Letter to Ways and Means Committee. National Rural Health Association.
https://www.ruralhealthweb.org/blogs/ruralhealthvoices/december-2017/rural-advocates-stand-up-for-cahs-in-letter-to-way. Published 2017.
20. Critical Access Hospitals Successfully Stop Cuts to Swing Bed Reimbursement. CAH Coalition. https://www.cahcoalition.com/critical-access-hospitals-successfully-stop-cuts-to-swing-bed-reimbursement/.
21. Defining Rural Population. Health Resources & Services Administration.
https://www.hrsa.gov/rural-health/about-us/definition/index.html. Published 2017. 22. A Primer on Interpreting Hospital Margins.; 2003.
http://www.shepscenter.unc.edu/rural/pubs/other/Primer.pdf.
23. Reiter KL, Holmes GM, Broyles I. Medicare, swing beds, and Critical Access Hospitals.
Med Care Res Rev. 2013;70(2):206-217.
24. Skilled Nursing Facility Services Payment System.; 2017. http://medpac.gov/docs/default-
source/payment-basics/medpac_payment_basics_17_snf_finalb4a411adfa9c665e80adff00009edf9c.pdf?sf vrsn=0.
25. Schmidheiny K. Short Guides to Microeconometrics.; 2018. https://www.schmidheiny.name/teaching/ols2up.pdf.
26. Baltagi B. Unbalanced Panel Data Models. In: Econometric Analysis of Panel Data. John Wiley & Sons; 2005:165.
27. Healthcare Finance: An Introduction to Accounting and Financial Management. https://www.ache.org/pubs/hap_companion/gapenski_finance/online appendix b.pdf. 28. Holmes GM, Kaufman BG, Pink GH. Predicting Financial Distress and Closure in Rural
Hospitals. J Rural Heal. 2017. doi:10.1111/jrh.12187
29. Patient Driven Payment Model. Centers for Medicare and Medicaid Services.
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SNFPPS/PDPM.html. Published 2018.
i The following are the requirements for Critical Access Hospital designation:
• Participate in Medicare
• Be located in a rural area in a state with an established State Flex Program
• Offer emergency services 24 hours a day 7 days a week
• Have an average annual length of stay of 96 hours or less per patient for acute care
• Be located at least 35 miles away from the nearest hospital or 15 miles if the terrain is mountainous or
there are only secondary roads
ii To provide swing bed services, a CAH cannot have more than 25 inpatient beds