Ectopic calcification and bone: a comparison
of the effect of dietary carbohydrates, sugars
and protein
Rachel Nicoll BSc MA
1, John McLaren Howard PhD
2and Michael Y Henein MD PhD
11 Department of Public Health and Clinical Medicine and Heart Centre
Umea University, Umea, Sweden
2 Acumen Lab, Tiverton, Devon, UK
Introduction
Cardiovascular (CV) calcification presence, extent and
progression has been shown in several studies to correlate
with fracture or low bone mineral density (BMD), particularly in
older men and women
1-3. CV calcification shares some similar
properties with cortical bone
4and, when severe, can manifest as
bone formation in both arteries and valves
5,6. CV calcification and
impaired bone metabolism are particularly prevalent in chronic
kidney disease (CKD), where the condition has become known as
mineral-bone disorder (MBD)
7. The association between bone and
ectopic calcification is further strengthened by studies showing
that renal calcification can be prevented by ibandronate, which
inhibits bone resorption
8. Although calcification can be associated
with atherosclerosis (i.e. intimal calcification), the deposition of
hydroxyapatite is primarily medial; its pathophysiology is complex,
involving not only physicochemical factors but also biological
actions in smooth muscle
9. Although a number of studies have
been carried out on the influence of dietary carbohydrates, sugars
and protein on bone, those relating diet to ectopic calcification are
considerably fewer and the comparison is necessarily restricted.
Carbohydrates and sugars
Ectopic calcification
In a prospective study of premenopausal women, carbohydrate
intake was inversely associated with coronary artery
calcification (CAC) five years after menopause but was not
associated with aortic calcification or carotid artery plaque
10and a large cross-sectional study showed that whole grain
intake was not associated with two measures of subclinical
atherosclerosis: carotid intima-media thickness (CIMT) and
CAC
11. Although there are no studies considering dietary intake
of sugars, diabetes mellitus, metabolic syndrome, insulin
resistance and high blood glucose, HbA1C and triglycerides
are known risk factors for the presence of aortic
12, breast
13,
carotid
14and coronary artery calcification
15,16and may also
correlate with the aortic calcification score
17or CAC score
18.
The relationship between CAC presence and blood glucose
levels was found particularly among men
19and may be
non-linear
20, with low insulin levels, as well as hyperinsulinaemia,
independently predicting CAC presence
21. Similarly in animals, a
high carbohydrate diet appears to facilitate nephrocalcinosis
22,
while starch or any form of sugar can result in increased
incidence of CV or renal calcification, particularly in magnesium
deficiency
23,24. Galactooligosaccharides or a high phytate diet,
however, can reduce CV and renal calcification
25,26. Likewise,
in vitro studies have shown that a high glucose medium
enhances calcification of vascular smooth muscle cells (VSMCs)
and increased expression of markers of bone formation,
confirming a cell-mediation process characterized by the
trans-differentiation of VSMCs to osteoblast-like cells
27.
Bone
Studies of carbohydrate intake and bone parameters
show mixed results
28,29, with several comparison studies
of carbohydrates, proteins or fats showing no difference in
markers of bone formation or resorption
30,31. Nevertheless, a
12 month study found that BMD was significantly lower with
a high carbohydrate diet compared to a high protein diet
32.
Abstract
Dietary fibre is generally inversely associated with BMD
33. Type
2 diabetes and insulin resistance are strongly associated with
impaired bone strength and quality
34, although there may be
less correlation with BMD
35and bone formation
36or resorption
37;
some have suggested that it may be hyperinsulinaemia, rather
than hyperglycaemia, that underlies the relationship
34. The effect
of sugar intake depends upon the type, with sucrose or fructose
intake correlated with increased bone resorption markers
38,
adversely affecting mineral homeostasis
39, while higher glucose
intake decreased bone resorption markers
37. Low lactose intake
reduced calcium absorption and BMD
40and increased fracture
risk
41. Prebiotics, such as inulin or fructans, increased mineral
absorption in humans but results on bone parameters were not
always positive
42,43.
In animals, both high
44and low
45carbohydrate intake can
have a detrimental effect on bone formation, while higher
dietary fibre from legumes can increase calcium absorption,
bone calcium content and BMD
46. High glucose, sucrose
and fructose generally result in lower BMD, particularly in
magnesium deficiency, probably through reduced calcium
absorption
47. Lactose again appears to be beneficial for bone
48,
while xylitol can slow bone resorption, increasing BMD, BMC
and biomechanical properties
49. Mannitol and prebiotics
can improve bone mineral absorption by increasing gut
fermentation, resulting in greater mineral uptake in bone and
improved BMD and bone strength
50.
Dietary protein
Ectopic calcification
There have been no human studies investigating protein
intake and CV calcification and in animals they focus almost
exclusively on nephrocalcinosis, with the majority showing that
increased dietary protein reduced renal calcification in rats
with or without CKD with frequent reduction in urinary calcium
excretion
51,52. Likewise, a low protein intake induced more
severe renal calcification, with decreased glomerular filtration
rate and enhanced urinary albumin loss, suggesting kidney
damage
53. In a study which considered both nephrocalcinosis
and bone health, krill protein produced lower renal tubular
calcium deposition than casein, but had no effect on BMC
or bone strength
54; although this shows a positive benefit of
krill protein, this may in part be due to the omega-3 fatty acid
content. A high calcium, high phosphorus or low magnesium
intake can enhance the detrimental effect of low protein intake
on renal calcification
51,53, while a calcium deficiency combined
with high protein intake also enhanced the rate of ectopic
calcification
54.
Bone
Bone is 50% protein and 50% mineral
56and consequently
dietary protein is essential for bone formation
57but it has
nevertheless been considered detrimental to bone since
protein induces urinary calcium excretion thought to derive
from bone resorption
58,59. Some recent studies, however,
suggest that increased calcium excretion may derive from
increased absorption, possibly through elevated gastric acid
production
58,60, higher glomerular filtration rate or decreased
renal calcium reabsorption
61. This is born out in a 2009
systematic review and meta-analysis of protein intake studies
and protein supplementation trials, which found a small
positive association with BMD and no detrimental association
with fracture risk
62. Recent studies have generally shown that,
although there may be little short term effect
63, long term high
protein intake is positively associated with BMD, BMC and
decreased fracture risk
64and slowed bone turnover
65. Similarly,
animal studies have generally shown that while high protein
diets certainly increase urinary calcium excretion, they either
have no effect on bone
66or bone calcium content and bone
mass is improved
67. In fact, it is generally low protein diets that
are harmful to bone, particularly after ovariectomy
68,69. There has
been concern that a high animal/vegetable protein ratio may
be detrimental to bone
70. Despite this, a 2009 meta-analysis
showed that BMD was around 4% lower in vegetarians than
in omnivores
71, although it was noted that key confounding
variables had not been taken into account
72. Since then a
large study found no association between hip fracture and the
animal/plant protein ratio
73, while animal protein was found
to increase calcium absorption to a greater extent than soy
protein
74.
There may be an interaction with calcium status in humans.
Sahni et al found that when calcium intake was <800 mg/d,
there was a three-fold increase in fracture risk with a high
animal protein intake, while in those consuming ≥800 mg/d
calcium those with a high animal protein intake had an 85%
reduced risk of hip fracture
73. Nevertheless, the body is clearly
attempting to compensate since among postmenopausal
women, a high protein intake increased calcium retention
only in those with a low calcium intake
75. Supplementing both
protein and calcium significantly reduced bone loss in elderly
hip fracture patients
76, while protein intake was associated
with BMD increase over three years in subjects aged ≥65
receiving calcium and vitamin D
76,77. A high protein diet in
calcium repletion can also protect against the bone loss of
weight reduction
78. Age may also play a role; a large study
showed that increased protein intake was associated with a
decreased risk of osteoporotic hip fracture in subjects aged
50-69 years but not in those aged 70-89, regardless of calcium
intake
79. Nevertheless, other prospective studies of the elderly
have shown a clear relationship between low protein intake and
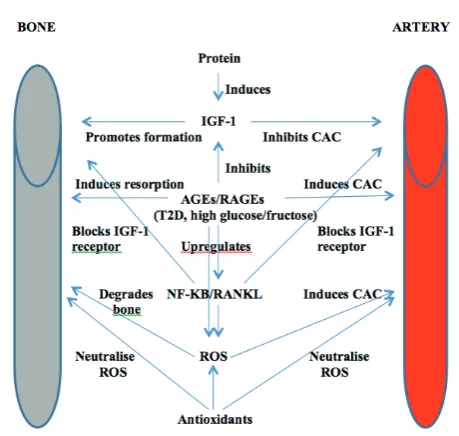
Figure 3
: Action of protein and sugars on bone and arteries
Key
IGF-1
Insulin-like growth factor 1
AGEs
Advanced glycation end products
RAGEs Receptor for AGEs
decreased BMD
[80].
Potential mechanisms
There may be several shared mechanisms of action between
the effect of protein and sugars on ectopic calcification and
bone but one of the best studied is insulin-like growth factor
(IGF) 1, which is known to stimulate bone formation and,
together with its receptor, has a protective effect against arterial
calcification
81,82. Protein is known to increase production of
IGF-1
83, while blood glucose and insulin levels are important
regulators
84. In vitro studies show that human VSMCs cultured
in advanced glycation end products (AGEs), which are
significantly increased in diabetes mellitus, induce enhanced
calcification due to both decreased expression of IGF-1 and
upregulation of NF-
κ
B, which blocks the IGF-1 receptor.
Over-expression of IGF-1 inhibited calcification in VSMCs, while
absence of the IGF-1 receptor negated the effect of AGEs on
calcification.
85Interestingly, the addition of moderate calcium
to the medium induced the IGF-1 receptor and inhibited
calcification in VSMCs, although high calcium led to inhibition
of the IGF-1 receptor, which increased calcification
86. This may
help to explain why an imbalance between protein and calcium
is detrimental.
A number of studies have been carried out on AGEs
independently of their effect on IGF-1. When AGEs come into
contact with their receptor (RAGE), intracellular reactive oxygen
species (ROS) are generated and mitogen-activated protein
kinase (MAPK) and nuclear factor kappa-B (NF-kB) signalling
is initiated
[87]. VSMCs cultured with AGEs showed enhanced
production of ROS, upregulated expression of RAGEs and
increased phosphorylation of p38 MAPK, as well as increased
activity of markers of bone formation: alkaline phosphatase,
osteopontin and osteocalcin
88,89. When an antioxidant or
anti-RAGE antibody was added to the medium, ROS expression,
p38 MAPK phosphorylation and calcification were reduced
and endogenous antioxidant expression increased, suggesting
that calcification of VSMCs occurs through a RAGE/oxidative
stress pathway via osteoblast-like differentiation of smooth
muscle cells
88,89. A high glucose medium has a similar effect on
VSMCs
90.
The AGE-RAGE interaction is additionally seen in bone
cells, resulting in increased expression of cytokines, growth
factors and adhesion molecules, which influence osteoclasts
and osteoblasts
91and affect the structural and mechanical
properties of bone
92. In mouse bone cells, AGEs resulted in an
increased number of resorption pits formed by osteoclasts,
while rat bone particles incubated with glucose were resorbed
to a much greater extent than control bone particles, suggesting
that AGEs enhance osteoclast-induced bone resorption
93.
Similarly, the fructose-induced stimulation of receptor activator
of NF-kB ligand (RANKL) significantly increased the number of
osteoclasts and pit formation in rat bone, accompanied by an
increase in ROS, an effect which could be completely abolished
by the antioxidant N-acetylcysteine
94. Among the elderly,
AGE-modified proteins stimulated monocytes/macrophages to
secrete bone-resorbing cytokines such as interleukin-1 beta,
interleukin-6 and tumour necrosis factor- alpha, with enhanced
net calcium efflux from bone
95.
Conclusion
A diet high in carbohydrates appears to increase ectopic
calcification, particularly in magnesium deficiency, although the
effect of carbohydrate and fibre on bone in humans is unclear
but appears to be consistently more detrimental than a high
protein diet. Although there are no human studies of the effect
of intake of sugars on ectopic calcification, diabetes mellitus,
insulin resistance and high blood glucose are risk factors
for both ectopic calcification and bone loss. Dietary sugars
generally increase ectopic calcification in animals, while in vitro
studies show that a high glucose medium significantly enhances
calcification of VSMCs, with increased local markers of bone
formation through action of AGEs which generate ROS. Sugars
generally reduce BMD in humans, although lactose appears
beneficial for bone in calcium deficiency but may increase renal
and CV calcification in animals. Prebiotics can increase mineral
absorption and improve BMD in animals, while also inhibiting
ectopic calcification, but the results on bone in humans are
inconsistent.
Whereas a high carbohydrate diet can increase ectopic
calcification, a diet high in protein may inhibit it, possibly
through induction of IGF-1. Dietary protein intake was generally
inversely correlated with renal calcification in animals with
and without CKD, although there were no human studies of
protein intake and ectopic calcification. In both animals and
humans, there is a modest positive association between protein
intake and BMD and an inverse association with fracture risk;
there appears to be little difference between animal and plant
proteins. There may be a strong synergistic interaction with
calcium, with low calcium and high protein intake significantly
increasing fracture risk and enhancing renal calcification,
while a high protein and calcium intake significantly reduced
fracture risk and inhibited ectopic calcification. Increased
protein is known to increase urinary calcium excretion but
rather than being taken from bone, this seems more likely to
be due to increased intestinal absorption and/or decreased
renal reabsorption, although this may only occur in calcium
deficiency. In general, therefore, a diet high in carbohydrate
and sugars and low in protein is detrimental to both arteries
and bone. This finding accords with our previous review, which
concluded that the dietary fats which are beneficial or harmful
for arteries are also beneficial or harmful for bone.
96References
1. El Maghraoui A, Rezqi A, Mounach A, Achemlal L, Bezza A, Dehhaoui M, Ghozlani I. Vertebral fractures and abdominal aortic calcification in postmenopausal women. A cohort study. Bone. 2013 Sep;56(1):213-9 2. Raggi P, Kleerekoper M. Contribution of bone and mineral abnormalities
to cardiovascular disease in patients with chronic kidney disease. Clin J Am Soc Nephrol. 2008 May;3(3):836-43
3. Choi SH, An JH, Lim S, Koo BK, Park SE, Chang HJ, Choi SI, Park YJ, Park KS, Jang HC, Shin CS. Lower bone mineral density is associated with higher coronary calcification and coronary plaque burdens by multidetector row coronary computed tomography in pre- and postmenopausal women. Clin Endocrinol (Oxf). 2009 Nov;71(5):644-51 4. Du J, Peterson M, Kansal N, Bydder GM, Kahn A. Mineralization in
calcified plaque is like that of cortical bone--further evidence from ultrashort echo time (UTE) magnetic resonance imaging of carotid plaque calcification and cortical bone. Med Phys. 2013; 40(10): 102301 5. Schmid K, McSharry WO, Pameijer CH et al. ‘Chemical and
physicochemical studies on the mineral deposits of the human atherosclerotic aorta’. Atherosclerosis. 1980; 37: 199-210 6. Nicoll R, Henein M. Extensive coronary calcification: a clinically
unrecognised condition. Curr Vasc Pharmacol. 2010 Sep;8(5):701-5 7. Nemcsik J, Kiss I, Tislér A. Arterial stiffness, vascular calcification and
bone metabolism in chronic kidney disease. World J Nephrol. 2012 Feb 6;1(1):25-34
8. Price PA, Roublick AM, Williamson MK. ‘Artery calcification in uremic rats is increased by a low protein diet and prevented by treatment with ibandronate’. Kidney Int. 2006; 70(9): 1577-83
9. Lomashvili K, Garg P, O’Neill WC. Chemical and hormonal determinants of vascular calcification in vitro. Kidney Int. 2006 Apr;69(8):1464-70. 10. Park HA, Lee JS, Kuller LH. Relationship between premenopausal dietary
11. Lutsey PL, Jacobs DR Jr, Kori S, Mayer-Davis E, Shea S, Steffen LM, Szklo M, Tracy R. Whole grain intake and its cross-sectional association with obesity, insulin resistance, inflammation, diabetes and subclinical CVD: The MESA Study. Br J Nutr. 2007; 98(2): 397-405
12. Danielsen R, Sigvaldason H, Thorgeirsson G, Sigfússon N. Predominance of aortic calcification as an atherosclerotic manifestation in women: the Reykjavik study. J Clin Epidemiol. 1996 Mar;49(3):383-7
13. Baum JK, Comstock CH, Joseph L. Intramammary arterial calcifications associated with diabetes. Radiology. 1980 Jul;136(1):61-2
14. van Gils MJ, Bodde MC, Cremers LG, Dippel DW, van der Lugt A. Determinants of calcification growth in atherosclerotic carotid arteries; a serial multi-detector CT angiography study. Atherosclerosis. 2013; 227(1): 95-9
15. Meigs JB, Larson MG, D’Agostino RB, Levy D, Clouse ME, Nathan DM, Wilson PW, O’Donnell CJ. Coronary artery calcification in type 2 diabetes and insulin resistance: the framingham offspring study. Diabetes Care. 2002 Aug;25(8):1313-9
16. Kronmal RA, McClelland RL, Detrano R, Shea S, Lima JA, Cushman M, Bild DE, Burke GL. Risk factors for the progression of coronary artery calcification in asymptomatic subjects: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2007; 115(21): 2722-30
17. Barascuk N, Ganz M, Nielsen M, Register TC, Rasmussen LM, Karsdal MA, Christiansen C. Abdominal aortic calcification quantified by the Morphological Atherosclerotic Calcification Distribution (MACD) index is associated with features of the metabolic syndrome. BMC Cardiovasc Disord. 2011 Dec 20;11:75
18. Schauer IE, Snell-Bergeon JK, Bergman BC, Maahs DM, Kretowski A, Eckel RH, Rewers M. Insulin resistance, defective insulin-mediated fatty acid suppression, and coronary artery calcification in subjects with and without type 1 diabetes: The CACTI study. Diabetes. 2011; 60(1): 306-14. 19. Moebus S, Stang A, Möhlenkamp S, Dragano N, Schmermund A,
Slomiany U, Hoffmann B, Bauer M, Broecker-Preuss M, Mann K, Siegrist J, Erbel R, Jöckel KH; Heinz Nixdorf Recall Study Group. Association of impaired fasting glucose and coronary artery calcification as a marker of subclinical atherosclerosis in a population-based cohort--results of the Heinz Nixdorf Recall Study. Diabetologia. 2009 Jan;52(1):81-9 20. Rutter MK, Massaro JM, Hoffmann U, O’Donnell CJ, Fox CS. Fasting
glucose, obesity, and coronary artery calcification in community-based people without diabetes. Diabetes Care. 2012 Sep;35(9):1944-50 21. Tanaka M, Fukui M, Tomiyasu K, Akabame S, Nakano K, Hasegawa G,
Oda Y, Nakamura N. U-shaped relationship between insulin level and coronary artery calcification (CAC). J Atheroscler Thromb. 2010 Oct 27;17(10):1033-40
22. Schwille PO, Brandt G, Brunner P, Ulbrich D, Kömpf W. Pancreatic islets, plasma glucagon and renal calcification in rats fed various diets. Results of a pilot study (author’s transl). Urologe A. 1975 Nov;14(6):306-14 23. [23] Koh ET, Min KW, Scholfield DJ, Sarkarcadeh A. Comparison of renal
calcium concentration in obese, lean, diabetic, and non-diabetic Zucker rats fed a magnesium-deficient fructose diet. Magnes Res. 1991 Sep-Dec;4(3-4):163-9
24. Zhou YB, Zhang J, Cai Y, Teng X, Duan XH, Song JQ, Du J, Tang CS, Qi YF. Insulin resistance induces medial artery calcification in fructose-fed rats. Exp Biol Med (Maywood). 2012 Jan;237(1):50-7
25. Chonan O, Takahashi R, Yasui H, Watanuki M. ‘Effects of beta-1-4 linked galactooligosaccharides on use of magnesium and calcification of the kidney and heart in rats fed excess dietary phosphorus and calcium’. Biosci Biotechnol Biochem. 1996; 60(10): 1735-7
26. Grases F, Sanchis P, Perello J, Isern B, Prieto RM, Fernandez-Palomeque C, Saus C. ‘Phytate reduces age-related cardiovascular calcification’. Front Biosci. 2008; 13: 7115-22
27. Liu F, Zhong H, Liang JY, Fu P, Luo ZJ, Zhou L, Gou R, Huang J. Effect of high glucose levels on the calcification of vascular smooth muscle cells by inducing osteoblastic differentiation and intracellular calcium deposition via BMP-2/Cbfβ-1 pathway. J Zhejiang Univ Sci B. 2010; 11(12): 905-11 28. Reddy ST, Wang CY, Sakhaee K, Brinkley L, Pak CY. Effect of
low-carbohydrate high-protein diets on acid-base balance, stone-forming propensity, and calcium metabolism. Am J Kidney Dis. 2002 Aug;40(2):265-74
29. Carter JD, Vasey FB, Valeriano J. The effect of a low-carbohydrate diet on bone turnover. Osteoporos Int. 2006;17(9):1398-403
30. Foster GD, Wyatt HR, Hill JO, Makris AP, Rosenbaum DL, Brill C, Stein RI, Mohammed BS, Miller B, Rader DJ, B, Wadden TA, Tenhave T, Newcomb CW, Klein S. Weight and metabolic outcomes after 2 years on a low-carbohydrate versus low-fat diet: a randomized trial. Ann Intern Med. 2010; 153(3): 147-57
31. Noakes M, Keogh JB, Foster PR, Clifton PM. Effect of an energy-restricted, protein, low-fat diet relative to a conventional high-carbohydrate, low-fat diet on weight loss, body composition, nutritional status, and markers of cardiovascular health in obese women. Am J Clin Nutr. 2005 Jun;81(6):1298-306
32. Thorpe MP, Jacobson EH, Layman DK, He X, Kris-Etherton PM, Evans EM. A diet high in protein, dairy, and calcium attenuates bone loss over twelve months of weight loss and maintenance relative to a conventional high-carbohydrate diet in adults. J Nutr. 2008 Jun;138(6):1096-100
33. O’Brien KO, Allen LH, Quatromoni P, Siu-Caldera ML, Vieira NE, Perez A, Holick MF, Yergey AL. High fiber diets slow bone turnover in young men but have no effect on efficiency of intestinal calcium absorption. J Nutr. 1993 Dec;123(12):2122-8
34. Srikanthan P, Crandall CJ, Miller-Martinez D, Seeman TE, Greendale GA, Binkley N, Karlamangla AS. Insulin resistance and bone strength. Findings from the study of midlife in the United States. J Bone Miner Res. 2013 Aug 26. Epub ahead of print
35. Kao CH, Tsou CT, Chen CC, Wang SJ. Bone mineral density in patients with noninsulin-dependent diabetes mellitus by dual photon absorptiometry. Nucl Med Commun. 1993; 14(5): 373-7
36. Kemink SA, Hermus AR, Swinkels LM, Lutterman JA, Smals AG. Osteopenia in insulin-dependent diabetes mellitus; prevalence and aspects of pathophysiology. J Endocrinol Invest. 2000; 23(5): 295-303 37. Chailurkit LO, Chanprasertyothin S, Rajatanavin R, Ongphiphadhanakul
B. Reduced attenuation of bone resorption after oral glucose in type 2 diabetes. Clin Endocrinol (Oxf). 2008 Jun;68(6):858-62
38. Elgán C, Dykes AK, Samsioe G. Bone mineral density and lifestyle among female students aged 16-24 years. Gynecol Endocrinol. 2002 Apr;16(2):91-8
39. [39] Milne DB, Nielsen FH. The interaction between dietary fructose and magnesium adversely affects macromineral homeostasis in men. J Am Coll Nutr. 2000 Feb;19(1):31-7
40. Goulding A, Taylor RW, Keil D, Gold E, Lewis-Barned NJ, Williams SM. Lactose malabsorption and rate of bone loss in older women. Age Ageing. 1999 Mar;28(2):175-80
41. Honkanen R, Kröger H, Alhava E, Turpeinen P, Tuppurainen M, Saarikoski S. Lactose intolerance associated with fractures of weight-bearing bones in Finnish women aged 38-57 years. Bone. 1997 Dec;21(6):473-7 42. Scholz-Ahrens KE, Ade P, Marten B, Weber P, Timm W, Acil Y et al.
‘Prebiotics, probiotics and synbiotics affect mineral absorption, bone mineral content and bone structure’. J Nutr. 2007; 137 (3 Suppl 2): 838S-46S
43. Abrams SA, Griffin IJ, Hawthorne KM, Liang L, Gunn SK, Darlington G, Ellis KJ. ‘A combination of prebiotic short- and long-chain inulin-type fructans enhances calcium absorption and bone mineralisation in young adolescents’. Am J Clin Nutr. 2005; 82(2): 471-6
44. de Tessieres C, Saffar JL. Spontaneous recovery from growth disturbances and osteopenia induced by a high carbohydrate diet in hamsters. J Biol Buccale. 1992 Jun;20(2):117-20.
45. Bielohuby M, Matsuura M, Herbach N, Kienzle E, Slawik M, Hoeflich A, Bidlingmaier M. Short-term exposure to low-carbohydrate, high-fat diets induces low bone mineral density and reduces bone formation in rats. J Bone Miner Res. 2010 Feb;25(2):275-84
46. Shiga K, Hara H, Takahashi T, Aoyama Y, Furuta H, Maeda H. Ingestion of water-soluble soybean fiber improves gastrectomy-induced calcium malabsorption and osteopenia in rats. Nutrition. 2002 Jul-Aug;18(7-8):636-42
47. Tsanzi E, Light HR, Tou JC. The effect of feeding different sugar-sweetened beverages to growing female Sprague-Dawley rats on bone mass and strength. Bone. 2008; 42(5): 960-8.
48. Hämäläinen MM, Knuuttila M, Svanberg M, Koskinen T. Comparison of the effect of gluconate, lactose, and xylitol on bone recalcification in calcium-deficient rats. Bone. 1990;11(6):429-38
49. Mattila PT, Svanberg MJ, Knuuttila ML. Increased bone volume and bone mineral content in xylitol-fed aged rats. Gerontology. 2001 Nov-Dec;47(6):300-5
50. Weaver CM, Martin BR, Nakatsu CH, Armstrong AP, Clavijo A, McCabe LD et al. ‘Galactooligosaccharides improve mineral absorption and bone properties in growing rats through gut fermentation’. J Agric Food Chem. 2011; 59(12): 6501-10
51. Sterck JG, Ritskes-Hoitinga J, Beynen AC. ‘Inhibitory effect of high protein intake on nephrocalcinosis in female rats’. Br J Nutr. 1992; 67(2): 223-33
52. Ohtsuka S, Kitano T, Maeda Y, Azami S. ‘Effect of the protein and oil contents on calcium utilization in the diets of female Fischer rats that were fed by three different feeding methods’. J Nutr Sci Vitaminol (Tokyo). 2006; 52(5): 316-26
53. Wen SF, Huang TP, Moorthy AV. ‘Effects of low-protein diet on
experimental diabetic neuropathy in the rat’. J Lab Clin Med. 1985; 106(5): 589-97
54. Gigliotti JC, Smith AL, Jaczynski J, Tou JC. Consumption of krill protein concentrate prevents early renal injury and nephrocalcinosis in female Sprague-Dawley rats. Urol Res. 2011 Feb;39(1):59-67.
55. Kelly O, Cusack S, Cashman KD. ‘The effect of bovine whey protein on ectopic bone formation in young growing rats’. Br J Nutr. 2003; 90(3): 557-64
56. Heaney RP. ‘Protein and calcium: antagonists or synergists?’. Am J Clin Nutr. 2002; 75: 609-10
58. Cao JJ, Johnson LK, Hunt JR. A diet high in meat protein and potential renal acid load increases fractional calcium absorption and urinary calcium excretion without affecting markers of bone resorption or formation in postmenopausal women. J Nutr. 2011; 141(3): 391-7 59. Pannemans DL, Schaafsma G, Westerterp KR. Calcium excretion,
apparent calcium absorption and calcium balance in young and elderly subjects: influence of protein intake. Br J Nutr. 1997 May;77(5):721-9 60. Kerstetter JE, O’Brien KO, Caseria DM, Wall DE, Insogna KL. The impact
of dietary protein on calcium absorption and kinetic measures of bone turnover in women. J Clin Endocrinol Metab. 2005 Jan;90(1):26-31 61. Wagner EA, Falciglia GA, Amlal H, Levin L, Soleimani M. Short-term
exposure to a high-protein diet differentially affects glomerular filtration rate but not Acid-base balance in older compared to younger adults. J Am Diet Assoc. 2007 Aug;107(8):1404-8
62. Darling AL, Millward DJ, Torgerson DJ, Hewitt CE, Lanham-New SA. ‘Dietary protein and bone health: a systematic review and meta-analysis’. Am J Clin Nutr. 2009; 90(6): 1674-92
63. Cao JJ, Pasiakos SM, Margolis LM, Sauter ER, Whigham LD, McClung JP, Young AJ, Combs GF Jr. Calcium homeostasis and bone metabolic responses to high-protein diets during energy deficit in healthy young adults: a randomized control trial. Am J Clin Nutr. 2013 Epub ahead of print
64. Kerstetter JE, Kenny AM, Insogna KL. ‘Dietary protein and skeletal health: a review of recent human research’. Curr Opin Lipidol. 2011; 22(1): 16-20 65. Jesudason D, Nordin BC, Keogh J, Clifton P. Comparison of 2 weight-loss
diets of different protein content on bone health: a randomized trial. Am J Clin Nutr. 2013 Nov;98(5):1343-52
66. [66] Mardon J, Habauzit V, Trzeciakiewicz A, Davicco MJ, Lebecque P, Mercier S, Tressol JC, Horcajada MN, Demigné C, Coxam V. Long-term intake of a high-protein diet with or without potassium citrate modulates acid-base metabolism, but not bone status, in male rats. J Nutr. 2008 Apr;138(4):718-24.
67. Zhao Y, Martin BR, Wastney ME, Schollum L, Weaver CM. ‘Acute versus chronic effects of whey proteins on calcium absorption in growing rats’. Exp Biol Med (Maywood). 2005; 230(8): 536-42
68. Marotte C, Gonzales Chavez MM, Pellegrini GG, Friedman SM, Lifshitz F, Mandalunis P, Zeni SN. ‘Low protein intake magnifies detrimental effects of ovariectomy and vitamin D on bone’. Calcif Tissue Int. 2013; Epub ahead of print.
69. Bourrin S, Toromanoff A, Ammann P, Bonjour JP, Rizzoli R. ‘Dietary protein deficiency induces osteoporosis in aged male rats’. J Bone Miner Res. 2000;1 5(8): 1555-63.
70. Sellmeyer DE, Stone KL, Sebastian A, Cummings SR. ‘A high ratio of dietary animal to vegetable protein increases the rate of bone loss and the risk of fracture in postmenopausal women. Study of Osteoporosis Fractures Research Group’. Am J Clin Nutr. 2001; 73(1): 118-22 71. Ho-Pham LT, Nguyen ND, Nguyen TV. ‘Effect of vegetarian diets on bone
mineral density: a Bayesian meta-analysis’. Am J Clin Nutr. 2009; 90: 943-50
72. Lanham-New SA. ‘Is ‘vegetarianism’ a serious risk factor for osteoporotic fracture?’. Am J Clin Nutr. 2009; 90: 910-1
73. Sahni S, Cupples LA, McLean RR, Tucker KL, Broe KE, Kiel DP, Hannan MT. ‘Protective effect of high protein and calcium intake on the risk of hip fracture in the Framingham offspring cohort’. J Bone Miner Res. 2010; 25(12): 2770-6
74. Kerstetter JE, Wall DE, O’Brien KO, Caseria DM, Insogna KL. Meat and soy protein affect calcium homeostasis in healthy women. J Nutr. 2006 Jul;136(7):1890-5
75. Hunt JR, Johnson LK, Roughead ZK. ‘Dietary protein and calcium interact to influence calcium retention: a controlled feeding study’. Am J Clin Nutr. 2009; 89(5): 1357-65
76. Dawson-Hughes B. Interaction of dietary calcium and protein in bone health in humans. J Nutr. 2003; Mar;133(3):852S-854S
77. Dawson-Hughes B, Harris SS. ‘Calcium intake influences the association of protein intake with rates of bone loss in elderly men and women’. Am J Clin Nutr. 2002; 75(4): 773-9
78. Bowen J, Noakes M, Clifton PM. A high dairy protein, high-calcium diet minimizes bone turnover in overweight adults during weight loss. J Nutr. 2004 Mar;134(3):568-73
79. Wengreen HJ, Munger RG, West NA, Cutler DR, Corcoran CD, Zhang J, Sassano NE. Dietary protein intake and risk of osteoporotic hip fracture in elderly residents of Utah. J Bone Miner Res. 2004 Apr;19(4):537-45 80. Hannan MT, Tucker KL, Dawson-Hughes B, Cupples LA, Felson DT,
Kiel DP. Effect of dietary protein on bone loss in elderly men and women: the Framingham Osteoporosis Study. J Bone Miner Res. 2000 Dec;15(12):2504-12
81. Siddals KW, Allen J, Sinha S, Canfield AE, Kalra PA, Gibson JM. Apposite insulin-like growth factor (IGF) receptor glycosylation is critical to the maintenance of vascular smooth muscle phenotype in the presence of factors promoting osteogenic differentiation and mineralization. J Biol Chem. 2011 May 13;286(19):16623-30.
82. Radcliff K, Tang TB, Lim J, Zhang Z, Abedin M, Demer LL, Tintut Y. Insulin-like growth factor-I regulates proliferation and osteoblastic
differentiation of calcifying vascular cells via extracellular signal-regulated protein kinase and phosphatidylinositol 3-kinase pathways. Circ Res. 2005 Mar 4;96(4):398-400
83. Calvez J, Poupin N, Chesneau C, Lassale C, Tome D, ‘Protein intake, calcium balance and health consequences’. Eur J Clin Nutr. 2012; 66: 281-95
84. Snyder DK, Clemmons DR. Insulin-dependent regulation of insulin-like growth factor-binding protein-1. J Clin Endocrinol Metab. 1990 Dec;71(6):1632-6
85. Wang Y, Zhang ZY, Chen XQ, Wang X, Cao H, Liu SW. Advanced glycation end products promote human aortic smooth muscle cell calcification in vitro via activating NF-βB and down-regulating IGF1R expression. Acta Pharmacol Sin. 2013 Apr;34(4):480-6
86. Di Bartolo BA, Schoppet M, Mattar MZ, Rachner TD, Shanahan CM, Kavurma MM. Calcium and osteoprotegerin regulate IGF1R expression to inhibit vascular calcification. Cardiovasc Res. 2011 Aug 1;91(3):537-45. 87. Fukami K, Yamagishi SI, Okuda S. Role of AGEs-RAGE system in
cardiovascular disease. Curr Pharm Des. 2013; [Epub ahead of print] 88. Wei Q, Ren X, Jiang Y, Jin H, Liu N, Li J. Advanced glycation end
products accelerate rat vascular calcification through RAGE/oxidative stress. BMC Cardiovasc Disord. 2013; 13: 13
89. Tanikawa T, Okada Y, Tanikawa R, Tanaka Y. Advanced glycation end products induce calcification of vascular smooth muscle cells through RAGE/p38 MAPK. J Vasc Res. 2009;46(6):572-80
90. Wang Y, Shan J, Yang W, Zheng H, Xue S. High Mobility Group Box 1 (HMGB1) Mediates High-Glucose-Induced Calcification in Vascular Smooth Muscle Cells of Saphenous Veins. Inflammation. 2013; 36(6): 1592-604.
91. Hein GE. Glycation endproducts in osteoporosis--is there a
pathophysiologic importance? Clin Chim Acta. 2006 Sep;371(1-2):32-6. 92. Valcourt U, Merle B, Gineyts E, Viguet-Carrin S, Delmas PD, Garnero P.
Non-enzymatic glycation of bone collagen modifies osteoclastic activity and differentiation. J Biol Chem. 2007 Feb 23;282(8):5691-703
93. Miyata T, Notoya K, Yoshida K, Horie K, Maeda K, Kurokawa K, Taketomi S. Advanced glycation end products enhance osteoclast-induced bone resorption in cultured mouse unfractionated bone cells and in rats implanted subcutaneously with devitalized bone particles. J Am Soc Nephrol. 1997 Feb;8(2):260-70
94. Hanayama R, Shimizu H, Nakagami H, Osako MK, Makino H, Kunugiza Y, Tomita T, Tsukamoto I, Yoshikawa H, Rakugi H, Morishita R. Fluvastatin improves osteoporosis in fructose-fed insulin resistant model rats through blockade of the classical mevalonate pathway and antioxidant action. Int J Mol Med. 2009 May;23(5):581-8
95. Miyata T, Kawai R, Taketomi S, Sprague SM. Possible involvement of advanced glycation end-products in bone resorption. Nephrol Dial Transplant. 1996;11 Suppl 5:54-7