June 2015
2015-2016
Service Agreement
Performance Framework
Contents
1 Background 4
Overview of the Department’s Performance Framework 4
2 Purpose of the Service Agreement Performance Framework 6 3 Service Agreement Performance Monitoring and Reporting Process 7
Service Agreement Performance Monitoring 7
Exceptional Events 7
Service Agreement Performance Reporting 7
Service Agreement Quarterly Performance Review Meetings 8
4 2015-2016 Changes to KPIs 9
New KPIs 9
Changes to Existing KPIs 9
Removal of KPIs 9
5 Service Agreement Performance Management Process 10
Principles of the Service Agreement Performance Management Process 10
Elements of Service Agreement Performance Management 11
Performance Intervention Levels 11
6 2015-2016 Key Performance Indicators Data Summary 15 7 Service Agreement Key Performance Indicator Definitions 19
Finance and Activity 19
Variation from budget – full year projected – FA1 19
THS cash liquidity – FA2 19
Acute admitted raw separations – FA3 20
Acute admitted inlier weighted units (same day and multi day) – FA4 20
Admitted patient episode coding (clinical coding) including contracted care – timeliness –
FA5 21
Admitted patient episode coding (clinical coding) including contracted care – accuracy –
FA6 22
Safety and Quality 23
Hand Hygiene compliance – SQ1 23
Healthcare associated staphylococcus aureus (including MRSA) bacteraemia infection rate –
SQ2 23
Access to Care (Emergency Care and Elective Surgery) 24 Percentage of Triage 1 emergency department presentations seen within the recommended
time – AEC1 24
Percentage of Triage 2 emergency department presentations seen within the recommended
Percentage of emergency department did not wait presentations – AEC3 26
Time until most admitted patients (90%) departed emergency department – AEC4 27
Ambulance offload delay part 1 – AEC5 28
Ambulance offload delay part 2 – AEC6 28
Access to Elective Surgery 29
Baseline elective surgery admissions – AES1a 29
Rebuilding Health Services – AES1b 30
Tasmanian Health Assistant Package admissions – AES1c 30
Average overdue days – AES2 30
Maximum wait time – AES3 31
Category 1 admitted within the recommended time – AES4 31
Category 2 admitted within the recommended time – AES5 32
Category 3 admitted within the recommended time – AES6 32
Category 2 treat in turn rates – AES7 33
Category 3 treat in turn rates – AES8 33
Hospital initiated postponements (HIPs) – AES9 34
Mental Health 34
28 Day re-admission rate – MH1 34
Acute 7 day post discharge community care – MH2 35
Seclusion rates – MH3 36
Primary Health 37
Priority category one Aged Care Assessment Team (ACAT) clients seen ‘on time’ in all
settings – PH1 37
Priority category two Aged Care Assessment Team (ACAT) clients seen ‘on time’ in all
settings – PH2 37
Priority category three Aged Care Assessment Team (ACAT) clients seen ‘on time’ in all
settings – PH3 38
Oral Health 38
Number of Dental Weighted Activity Units (DWAUs) delivered between 1 July 2015 and
30 June 2016 – OH1 38
Proportion of ‘Emergency’ clients managed on the same day as they are triaged – OH2 39
Cancer Screening and Control Services 40
Percentage of clients assessed within 28 days of screening mammogram – CSCS1 40
1
Background
Overview of the Department’s Performance Framework
Under the Tasmanian Health Organisations Act 2011 (the Act),the Minster for Health (the Minister) enters into annual Service Agreements with THO Governing Councils. The development of, and advice regarding these Agreements originates from the Department (acting on behalf of the Minister as the Purchaser). The Department’s purchasing function is supported by a number of governing instruments, including the
2015-2016 Purchasing Framework, which outlines the process followed in purchasing services, and this document, the 2015-2016 Service Agreement Performance Framework, which codifies the process of monitoring THS performance against the requirements of the Service Agreement.
In addition to its role as the Purchaser, the Department has a broader responsibility as System Manager to undertake such strategic, planning and monitoring functions and activities as necessary to enable it to provide assurance to the responsible Ministers (the Minister for Health and the Treasurer have joint responsibilities under the Act) that the Tasmanian health system is being managed effectively and efficiently. There are many activities that occur in the Tasmanian health system, outside of those that are purchased directly from the THS through the Service Agreement that should be subject to ongoing monitoring. The Monitoring Suite, governed by the Monitoring Suite Operational Guidelines, enables the System Manager to gain an understanding of the state of Tasmania’s publicly funded health services, supplementing the quasi contractual arrangements of the Service Agreement. Should there be a patient safety issue that requires an urgent response, it will be guided by the Clinical Governance Framework.
The functions of Purchaser and System Manager cannot be viewed in isolation of each other - the nature and volume of services purchased will impact on the effectiveness and efficiency of the Tasmanian health system and the primary mechanism for effective system management is through informed, appropriate purchasing. Purchasing is a necessarily transactional process, and so must be contextualised to be effective as a mechanism to enact Government policy in health and to ensure that purchasing decisions reflect the longer term application of strategy.
An annual (rolling) Statement of Purchaser Intent (currently under review as part of the One Health System
reform programme), which signals purchaser intentions over the coming five years, will act as the bridge between the functions of the Purchaser and System Manager. This will be the translational implement linking the activities of the Purchaser to the priorities of the System Manager and will be released in the first quarter of every calendar year.
The dual role of the Department as both Purchaser and System Manager is represented graphically in Figure1.
Background
2
Purpose of the Service Agreement Performance
Framework
Annual Service Agreements between the Minister and THS Governing Council sets out the expectations of the volume and quality of services to be delivered and the funding provided in relation to the delivery of those services.
It is the responsibility of the Governing Council to ensure that the THS deliver the requirements of the Service Agreement once established. It is the responsibility of the Department to ensure that THS performance against those requirements is monitored and managed to ensure that where necessary, the performance intervention options available to the Minister under the Actare effectively implemented. The 2015-2016 Service Agreement Performance Framework explains the process of monitoring THS performance against the requirements of the Service Agreement to ensure that where determined necessary, the performance management options available to the Minister under the Act are effectively implemented.
It describes an integrated process for the monitoring and assessment of THS performance against the requirements of the Service Agreement and provides both the Department and the THS with a clear delineation of roles, responsibilities and expectations in response to identified Service Agreement performance issues.
It should be read in conjunction with the following key documents:
2015-2016 THS Service Agreement
State-wide Clinical Governance Framework
2015-2016 THS Purchasing & Funding Guidelines.
In addition, a number of key “system management frameworks” have been committed to under the ‘One State, One Health System; Better Outcomes’ reform programme. These include:
Statement of Purchaser Intent
Monitoring Suite of Indicators
Service Agreement Performance Monitoring and Reporting Process
3
Service Agreement Performance Monitoring and
Reporting Process
Service Agreement Performance Monitoring
The Annual Service Agreement between the Minister and THS Governing Council includes specific KPIs and associated targets.
KPIs and targets are systematically considered and adopted in the following order of preference where practical:
existing national policy based targets
existing Tasmanian health policy based targets
new targets based on previous performance baselines.
KPI targets establish the levels of performance that determine whether any action is required regarding the identification and management of Service Agreement performance issues.
Not all national or state based targets form part of the Service Agreement. Some have been determined as better placed within the Monitoring Suite as broader markers of the effective and efficient management of the Tasmanian health system.
Further information regarding the target source is provided in section 6.
Exceptional Events
There may be circumstances beyond the reasonable control of the THS which may prevent the achievement of KPI targets and it is important that such circumstances are recognised.
At its discretion, and on a case-by-case basis, the Department will consider requests from the THS to consider such circumstances as part of the ongoing performance monitoring process. The intention is to recognise extraordinary and generally unforseen events beyond the reasonable control of the THS, but not planned service interruptions such as capital works or ad hoc operational difficulties.
The THS is expected to provide the Department with timely advice of such circumstances and to actively mitigate any risk(s) to achieving KPI targets.
Service Agreement Performance Reporting
At the end of each quarter, the Department provides the responsible Ministers with the THS Quarterly Service Agreement Performance Report, outlining Service Agreement performance against all KPIs over the preceding quarter and, where necessary, recommended performance interventions. The report is compiled by the System Purchasing and Performance (SPP) Unit of the Department following completion of quarterly Service Agreement performance review meetings with the THS.
Service Agreement Quarterly Performance Review Meetings
Quarterly performance review meetings are co-ordinated by SPP. Meetings are characterised by:
a common standard agenda for all meetings, varied for specific local performance issues and the escalation status
THS led discussion that enables THS representatives to describe their proactive performance management from an operational-level perspective
aiming to reduce the need for further escalation of the performance response
clear recording and communication of actions and requirements of the THS and the Department. Core attendance is kept to a minimum to facilitate smooth and efficient conduct of business ensuring coverage of each performance domain. Additional attendees may be included where attention to specific areas of performance requires the involvement of staff with specialist expertise and knowledge.
Each meeting will have the following core attendees:
The Department:
SPP Deputy Secretary will attend all meetings
other Departmental Directors or their representatives will attend as required
generally, representatives of SPP will also attend and provide secretariat support if required.
THS:
the attendance of the THS Chair is required
attendance by other members of the Governing Council and/or senior executives is at the discretion of the Chair, unless attendance of a specified executive is requested by the Secretary or delegate. It is anticipated that the THS Chief Executive Officer will attend.
The Secretary of the Department may attend if and when a performance issue has been escalated and is unsatisfactory.
2015-2016 Changes to KPIs
4
2015-2016 Changes to KPIs
New KPIs
Access to Care (Emergency Care and Elective)
Baseline elective surgery admissions - (Assessment level based on whole of THS)
Average overdue days
Maximum wait time
Category 2 admitted within the recommended time
Category 3 admitted within the recommended time
Category 2 treat in turn rates
Category 3 treat in turn rates
Hospital initiated postponements (HIPs)
Cancer Screening and Control Services
Percentage of clients assessed within 28 days of screening mammogram
Eligible women screened for breast cancer
Changes to Existing KPIs
Finance and Activity
Variation from budget – full year projected – (Assessment level based on whole of THS)
THS cash liquidity – (Assessment level based on whole of THS)
Mental Health Service
28 Day Re-admission rate (Target reduced to </= 13.9%)
Seclusion Rates (Target reduced to <8 per 1 000 patient days)
Oral Health
Proportion of ‘Emergency’ clients managed on the same day that they are triaged (Target increased to 80%)
Primary Health
Priority category one Aged Care Assessment Team (ACAT) clients seen ‘on time’ in all settings (Assessment level based on whole of THS)
Priority category two Aged Care Assessment Team (ACAT) clients seen ‘on time’ in all settings (Assessment level based on whole of THS)
Priority category three Aged Care Assessment Team (ACAT) clients seen ‘on time’ in all settings (Assessment level based on whole of THS)
Removal of KPIs
Access to Care (Emergency Care and Elective)
Percentage of all emergency department presentations seen within recommended triage time (removed from Service Agreement – to be included in Monitoring Suite)
5
Service Agreement Performance Management
Process
Principles of the Service Agreement Performance Management
Process
The Department’s approach to performance monitoring, assessment and response is shaped by the principles outlined in Table 1 below.
Table 1: Principles of the Performance Framework
Realistic Performance and funding expectations will be balanced with the resources and capacity of the health system and the current fiscal environment.
Consistency and Transparency
The Department will apply a consistent and transparent method for assessing performance against clear, agreed KPI targets, and responding where appropriate. The default response to the non-achievement of performance targets will be escalation, with the Minister (or delegate) maintaining discretion to waive such escalations.
Accountability The Department and THS have distinct and separate roles and accountabilities as Purchaser and Provider respectively. The Department, on behalf of the Minister, will negotiate an annual Service Agreement with the THS and monitor performance against the requirements of the Agreement. The THS is accountable for delivering services to the agreed standards outlined in the Service Agreement and ensuring that an effective internal performance framework is in place that demonstrates processes to actively monitor the requirements of the Agreement.
Informed Purchasing
The Department’s System Manager role will inform the establishment of purchasing priorities and KPIs, in turn shaping negotiation of the Service Agreement.
Integration The Department recognises change or variation in a particular aspect of performance may require changes to other, interdependent, elements of the system. The Department acknowledges that influences outside the control of the THS may affect performance and such factors will be considered when performance is assessed.
Recognition Superior performance will be recognised and reviewed by the Department for lessons to be shared across the THS.
Service Agreement Performance Management Process
Elements of Service Agreement Performance Management
Service Agreement performance management will involve:
on-going monitoring and review of THS performance against the requirements of the Service Agreement
identifying a performance concern and determining the appropriate response
determining when a performance intervention is necessary and the level of intervention required
determining when the performance intervention needs to be escalated or can be de-escalated.
Performance Intervention Levels
There are four performance levels in the 2015-2016Service Agreement Performance Framework.
The level of performance response and intervention dictates the action required by the THS and/or the Department. The Minister approved delegation of certain Ministerial powers and functions that enables the Secretary to escalate or de-escalate concerns for:
Level 1 (unsatisfactory performance), requesting a Performance Improvement Plan
Level 2 (sustained unsatisfactory performance), ability to appoint a Performance Improvement Team. The Minister retains the power to appoint a Ministerial Representative to assist the Governing Council, if considered necessary, as part of a Level 2 Performance Escalation. The Minister also retains the power to approve a Level 3 Performance Escalation.
The non-achievement of any individual Service Agreement KPI target will lead to the immediate identification of a performance concern and application of the performance intervention process outlined below. Service Agreement KPIs require compliance and the achievement of assigned targets within the specified assessment period. Generally, a performance escalation will only be recommended in circumstances where the THS is unable to demonstrate to the Department that:
the performance concern is being actively managed and monitored by the THS
a robust and transparent plan for sustainable performance improvement is in place within the THS
the THS possesses the necessary skills to achieve sustainable performance improvement in the area of concern.
The Minister may waive any recommendation received from the Department to proceed with a performance escalation.
Based on the response provided by the THS to performance concerns, an issue may be escalated or de-escalated in a non-sequential fashion.
Service Agreement KPIs are viewed independently of each other - that is, escalation or de-escalation is managed on the basis of each KPI, without mitigation by performance in other KPIs.
Performance Escalation Level 0 (Satisfactory Performance)
If a Service Agreement KPI target is achieved, the KPI will be assigned Level 0 (satisfactory performance). Satisfactory performance will be noted in the THS Quarterly Service Agreement Performance Report provided to the Minister.
Performance Escalation Level 1(Unsatisfactory Performance)
The non-achievement of a Service Agreement KPI target will lead to the immediate identification of a performance concern and the application of the performance intervention process. In the event of
non-achievement, the Secretary will consider escalating the performance issue to Level 1 (unsatisfactory performance).
Before taking this action, the Chair and CEO will be advised of the intention to escalate and be provided with an opportunity to provide more information to the Department in relation to the performance issue. In such circumstances the Chair or CEO must provide supporting information within 7 days from receipt of the request.
Performance Escalation Level 2 (Sustained Unsatisfactory Performance)
At Level 2, direct intervention will occur due to sustained unsatisfactory performance. Formal notification of the intention to escalate to Level 2 will be provided by the Secretary to the Chair and the CEO. Depending on the nature of the performance concern, at Level 2, the Secretary may appoint a Performance Improvement Team or the Minister may appoint a Ministerial Representative to assist the Governing Council in its oversight of the THS’s functions.
Performance Escalation Level 3 (Challenged and Failing)
For sustained performance concerns that have not been resolved, the Secretary may recommend to the Minister that a higher level of response be initiated (Level 3 – challenged and failing). Formal notification of the intention to recommend to the Minister that escalation to Level 3 should occur will be provided by the Secretary to the Chair and the CEO.
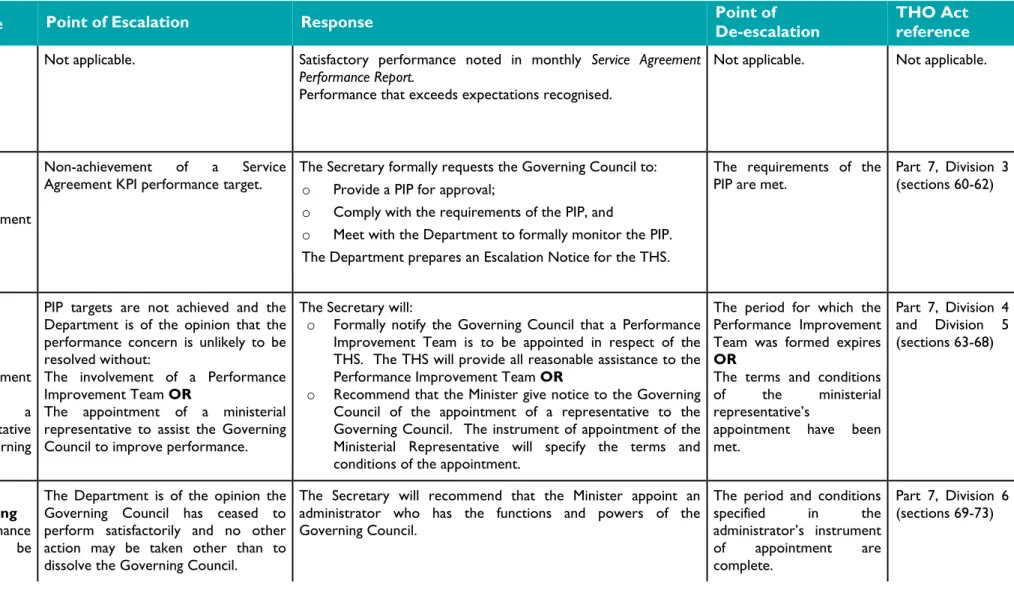
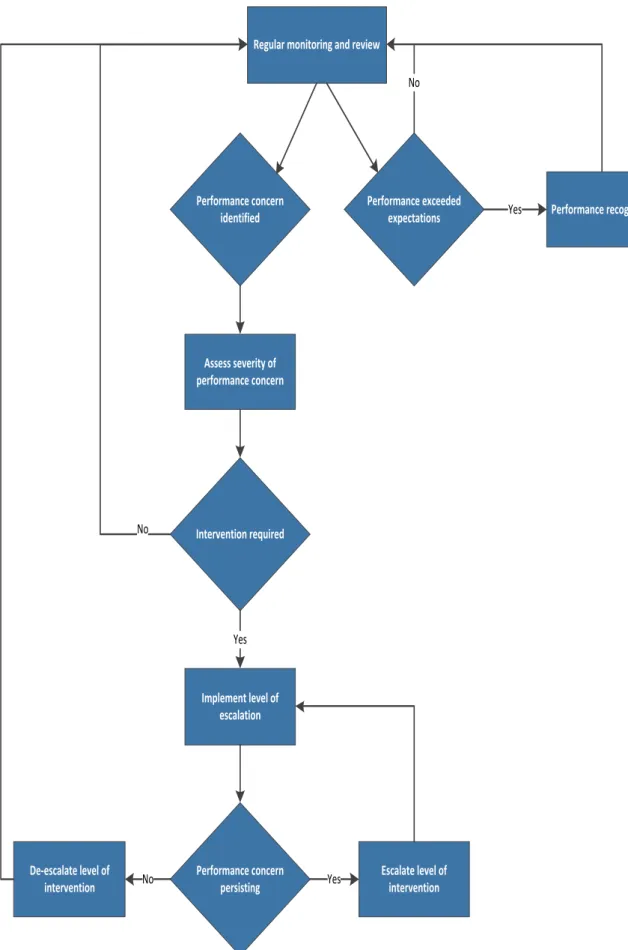
Table 2 summarises the escalation/de-escalation response process. Figure 2 demonstrates the escalation/de-escalation decision process.
Service Agreement Performance Management Process
Table 2: Performance Escalation/De-escalation Response Framework
Level of Response Point of Escalation Response Point of De-escalation THO Act reference
Level 0 Satisfactory Performance
No action required
Not applicable. Satisfactory performance noted in monthly Service Agreement Performance Report.
Performance that exceeds expectations recognised.
Not applicable. Not applicable.
Level 1 Unsatisfactory Performance
Performance Improvement Plan (PIP) required
Non-achievement of a Service
Agreement KPI performance target. The Secretary formally requests the Governing Council to: o Provide a PIP for approval;
o Comply with the requirements of the PIP, and
o Meet with the Department to formally monitor the PIP. The Department prepares an Escalation Notice for the THS.
The requirements of the
PIP are met. Part 7, Division 3 (sections 60-62)
Level 2 Sustained Unsatisfactory Performance Performance Improvement Team OR Appointment of a Ministerial Representative to assist the Governing Council.
PIP targets are not achieved and the Department is of the opinion that the performance concern is unlikely to be resolved without:
The involvement of a Performance Improvement Team OR
The appointment of a ministerial representative to assist the Governing Council to improve performance.
The Secretary will:
o Formally notify the Governing Council that a Performance Improvement Team is to be appointed in respect of the THS. The THS will provide all reasonable assistance to the Performance Improvement Team OR
o Recommend that the Minister give notice to the Governing Council of the appointment of a representative to the Governing Council. The instrument of appointment of the Ministerial Representative will specify the terms and conditions of the appointment.
The period for which the Performance Improvement Team was formed expires
OR
The terms and conditions of the ministerial representative’s
appointment have been met.
Part 7, Division 4 and Division 5 (sections 63-68)
Level 3
Challenged and failing
Changes to the governance of the THS may be required
The Department is of the opinion the Governing Council has ceased to perform satisfactorily and no other action may be taken other than to dissolve the Governing Council.
The Secretary will recommend that the Minister appoint an administrator who has the functions and powers of the Governing Council.
The period and conditions specified in the administrator’s instrument of appointment are complete. Part 7, Division 6 (sections 69-73)
Figure 2: Performance Intervention Decision Process
Performance concern identified
Performance exceeded expectations Regular monitoring and review
Assess severity of performance concern Performance recognition No Yes Intervention required No Implement level of escalation Performance concern persisting De-escalate level of intervention Escalate level of intervention Yes No Yes
2015-2016 Key Performance Indicators Data Summary
6
2015-2016 Key Performance Indicators Data
Summary
Domain Code
Finance and Activity (FA) Source of KPI
Target
FA1 Variation from budget - full year projected DHHS-Budget
and Finance
Balanced budget
FA2 Cash liquidity DHHS-Budget
and Finance
THS Operating Account has a favourable balance
FA3 Acute admitted raw separations Tasmanian
Activity Based Funding Model (DHHS SPP). Negotiated with THS. Recognises prevailing State Government policy directions 93 542
FA4 Acute admitted inlier weighted units (same
day and multi day)
Tasmanian Activity Based Funding Model (DHHS SPP). Negotiated with THS. Recognises prevailing State Government policy directions 92 636
FA5 Admitted patient episode coding (clinical
coding) including contracted care - timeliness
DHHS (SPP) 100% within 42
days of separation
FA6 Admitted patient episode coding (clinical
coding) including contracted care - accuracy DHHS (SPP) 100% within 30 days of advice from SPP Domain Code
Safety and Quality (SQ) Source of KPI
SQ1 Hand Hygiene compliance ACSQHC ≥70% (all specified facilities)
SQ2 Healthcare associated staphylococcus
aureus (including MRSA) bacteraemia infection rate
National Standard
≤2.0 per 10 000 patient days (all specified facilities)
Domain Code
Access to Care (Emergency Care and Elective Surgery)
Source of KPI
Target
Access to Emergency Care
AEC1 Percentage of Triage 1 emergency
department presentations seen within recommended time Australasian College for Emergency Medicine 100% (all specified facilities)
AEC2 Percentage of Triage 2 emergency
department presentations seen within recommended time Australasian College for Emergency Medicine 80% (all specified facilities)
AEC3 Percentage of emergency department did
not wait presentations
DHHS (SPP) ≤5% (all
specified facilities)
AEC4 Time until most admitted patients (90%)
departed emergency department
National Health Performance Authority ≤8 hours (all specified facilities)
AEC5 Ambulance offload delay part 1 Australasian
College for Emergency Medicine 85% within 15 minutes (all specified facilities)
AEC6 Ambulance offload delay part 2 Australasian
College for Emergency Medicine 100% within 30 minutes (all specified facilities) Access to Elective Surgery
AES 1a Baseline elective surgery admissions DHHS - SPP 14 126
AES 1b Rebuilding Health Services DHHS - SPP 2 260
AES 1c Tasmanian Health Assistance Package
admissions
2015-2016 Key Performance Indicators Data Summary
AES 2 Average overdue days DHHS – SPP Dec 15: 177
Jun 16: 137
AES 3 Maximum wait time DHHS – SPP Dec 15: 730
Jun 16: 600
AES 4 Category 1 admitted within the
recommended time
DHHS – SPP Dec 15: 80%
Jun 16: 90%
AES 5 Category 2 admitted within the
recommended time
DHHS – SPP Dec 15: 60%
Jun 16: 70%
AES 6 Category 3 admitted within the
recommended time
DHHS – SPP Dec 15: 40%
Jun 16: 45%
AES 7 Category 2 treat in turn rates DHHS – SPP Dec 15: 40%
Jun 16: 45%
AES 8 Category 3 treat in turn rates DHHS – SPP Dec 15: 40%
Jun 16: 45%
AES 9 Hospital initiated postponements (HIPs) DHHS – SPP Dec 15: 14.7%
Jun 16: 12.6%
Domain Code
Mental Health (MH) Source of KPI
Target
MH1 28 Day re-admission rate NMDS ≤13.9% (all
specified regions)
MH2 Acute 7 day post discharge community care NMDS 75% (all
specified regions)
MH3 Seclusion rates To be included
in NMDS
< 8 per 1 000 patient days (all specified regions)
Domain Code
Primary Health (PH) Source of KPI
Target
PH1 Aged Care Assessment Team (ACAT) -
Priority Category one clients seen ‘on time’ in all settings
ACAP
Minimum Data Set
85%
PH2 Aged Care Assessment Team (ACAT) -
Priority Category two clients seen ‘on time’ in all settings
ACAP
Minimum Data Set
85%
PH3 Aged Care Assessment Team (ACAT) -
Priority Category three clients seen ‘on time’ in all settings
ACAP Minimum Data Set 85% Domain Code
Oral Health (OH) Source of KPI
OH1 Number of Dental Weighted Activity Units (DWAUs) delivered between 20 December 2012 and 30 June 2015 NPA on Treating More Public Dental Patients Sep15: 13 125 Dec15: 24 954 Mar16: 35 451 Jun16: 45 883
OH2 Proportion of 'Emergency' clients managed
on the same day that they are triaged
THO South (OHST)
80%
Domain Code
Cancer Screening and Control Services (CSCS)
Source of KPI
Target
CSCS1 Percentage of clients assessed within 28
days of screening mammogram
TBC >90%
CSCS2 Eligible women screened for breast cancer TBC Number of
women screened YTD is more than same time two years ago
The timeframes for data collection are specified against each KPI in the following section (Service Agreement Key Performance Indicator Definitions).
Service Agreement Key Performance Indicator Definitions
7
Service Agreement Key Performance
Indicator Definitions
Finance and Activity
Variation from budget – full year projected – FA1
Definition This KPI measures the variance between full year budget and full year projected actual on a cash basis for all funding types.
Calculating
performance Calculated by subtracting the full year projected cash forecast from the full year cash budget on an all funds basis including carry forwards.
KPI target Balanced budget projected.
KPI target source DHHS – Budget and Finance. Assessment level Whole of THS.
Assessment
period Performance is assessed quarterly.
Frequency of data
collection Monthly.
Data Source Finance 1.
THS cash liquidity – FA2
Definition This KPI is a measure of the THS’s capacity to meet its financial commitments when they fall due. If the THS is unable to meet its financial commitments within a given month, an advance of future funding is required to ensure the THS complies with Treasurer’s Instruction (TI) 402. This KPI is an early KPI that there is the potential for a liquidity problem impacting on the THS’s capacity to meet its financial
commitments within the current financial year. Calculating
performance Calculated by subtracting the total of the advance from the closing balance of the THS Operating Account at the end of the month to demonstrate what the unadjusted position would have been.
KPI target THS Operating Account has a favourable balance. KPI target source DHHS – Budget and Finance.
Assessment level Whole of THS. Assessment
period Performance is assessed quarterly.
Frequency of data
collection Monthly. In instances where the THS requires an advance of funds in one month, it will enable the THS to take corrective action in the following month(s) to return the THS Operating Account to a favourable balance.
Data Source Finance 1.
Acute admitted raw separations – FA3
Definition This KPI measures the volume of raw separations. A raw separation is an episode of admitted patient care. Raw separations are not adjusted for the complexity of the episode of care and represent each individual episode of care in a given period. Calculating
performance The total number of raw separations (admitted acute inc. qualified newborns and mental health) as defined in the DHHS Admission and Discharge Policy Manual effective as from 1 July 2015.
This KPI measures baseline activity only. It excludes “above baseline” activity associated with, and funded under, separate Commonwealth or State programs.
KPI target 93 542
KPI target source Tasmanian Funding Model - DHHS SPP. Assessment level Whole of THS.
Assessment
period Performance is assessed quarterly on a year to date basis. Frequency of data
collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source iPM.
Acute admitted inlier weighted units (same day and multi day) – FA4
Definition This KPI measures the volume of inlier weighted units. Inlier weighted units are rawseparations adjusted for the complexity of each individual episode of care. Previously measured as weighted separations, inlier weighted units are now a specified output of the Tasmanian Funding Model.
Service Agreement Key Performance Indicator Definitions
Calculating
performance The total number of inlier weighted units (admitted acute inc. qualified newborns and mental health) as defined in the DHHS Admission and Discharge Policy Manual effective as from 1 July 2015.
The average cost weight used to construct this KPI is calculated from the National Hospital Morbidity Database, using AR-DRG public cost weights published by the Commonwealth Department of Health and Ageing. However, the following costs are excluded as the Tasmanian Funding Model funds these separately (with the exception of depreciation which is not funded):
Depreciation
ICU
Mechanical ventilation
ED
This KPI measures baseline activity only. It excludes “above baseline” activity associated with, and funded under, separate Commonwealth or State programs.
KPI target 92 636
KPI target source Tasmanian Funding Model - DHHS SPP. Assessment level Whole of THS.
Assessment
period Performance is assessed quarterly on a year to date basis. Frequency of data
collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source iPM.
Admitted patient episode coding (clinical coding) including contracted
care – timeliness – FA5
Definition This KPI measures the percentage of admitted patient episodes coded within 42 days of the episode separation.
Calculating
performance All admitted patient episode separations within the specified assessment period are within scope. The coding date (considered to be the date recorded against the principal diagnosis field in iPM) will be compared with the separation date. All records not coded within 42 days of the separation date will be considered to fail. KPI target 100% within 42 days of separation.
KPI target source DHHS –SPP. Assessment level Whole of THS. Assessment
period Quarterly, based on performance over the most recent quarter against which the 42 day period can be applied (e.g. the December 2015 quarterly assessment will be based on the percentage of admitted patient episodes coded within 42 days of the episode separation for all episode separations dated between 1 July 2015 and 30 September 2015).
Frequency of data
collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month (e.g. the December 2015 quarterly assessment for all episode separations dated between 1 July 2015 and 30 September 2015 will be based on data collected from Health Central through iPM on the sixth working day in January 2016).
Admitted patient episode coding (clinical coding) including contracted
care – accuracy – FA6
Definition This KPI measures the percentage of fatal data errors (as specified in the schedule below) that are corrected within 30 days of being reported by DHHS to the THS. Calculating
performance At the end of each month, DHHS will provide THSs with a list of fatal data errors detected over the previous month. Errors not corrected by the THS within 30 days of receipt of the list will be considered to fail. The date of receipt will be
considered to be the date upon which the list of fatal data errors is e-mailed to THS CEO’s by SPP. The list will clearly indicate the date by which the correction of fatal data errors is to occur.
KPI target 100% within 30 days of advice.
KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Quarterly, based on performance over the most recent quarter against which the 30 day period can be applied (e.g. the December 2015 quarterly assessment will be based on the percentage of fatal data errors corrected within 30 days of receipt of the monthly list of fatal data errors for the months of July 2015, August 2015 and September 2015).
Frequency of data
collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month (e.g. the December 2015 quarterly assessment for the months of July 2015, August 2015 and September 2015 will be based on data collected from Health Central through iPM on the sixth working day in January 2016).
Service Agreement Key Performance Indicator Definitions
Safety and Quality
Hand Hygiene compliance – SQ1
Definition This KPI measures the compliance rate as the percentage of correct hand hygiene performed by hospital staff.
Calculating
performance Data is collected by authorised Hand Hygiene auditors in accordance with the Hand Hygiene Australia, Hand Hygiene Manual.
Numerator: Number of times hand hygiene was performed correctly at the correct time.
Denominator: Number of hand hygiene opportunities that were observed.
KPI target 70%.
KPI target
source An interim national benchmark of 70% for hand hygiene reporting on MyHospitals has been advised by the Australian Commission on Safety and Quality in Health Care.
Assessment
level Facility specific: RHH, LGH, NWRH and MCH.
Assessment
period
Performance is assessed quarterly based on the most recent published
TIPCU data.
Frequency ofdata collection Data is submitted to Hand Hygiene Australia three times per annum:
March 31st
June 30th
October 31st.
Data source TIPCU.
Healthcare associated staphylococcus aureus (including MRSA)
bacteraemia infection rate – SQ2
Definition This KPI measures the rate of Healthcare Associated Staphylococcus aureus
bacteraemia infection. This KPI is concerned with cases of this infection which are associated with a patient receiving healthcare.
Calculating
performance The definitions applied are consistent with national definitions which are published by the Australian Commission on Safety and Quality in Healthcare Data set specification – Surveillance of Healthcare Associated Infections: Staphylococcus aureus
bacteraemia and Clostridium difficile infection (Version 4.0).
Numerator: Number of cases of healthcare associated Staphylococcus aureus bacteraemia.
Denominator: Number of patient days for the given period (matching the numerator period).
KPI target No more than 2.0 cases per 10,000 patient days. KPI target
source The national benchmark for states and territories (public hospitals) according to the Australian Commission on Safety and Quality in Health Care. Assessment
level Facility specific: RHH, LGH, NWRH and MCH.
Assessment
period Performance is assessed quarterly based on the most recent published TIPCU data. Frequency of
data collection In line with the TIPCU 2011 data is collected and reported on as per the following process: Staphylococcus aureus Bacteraemia Surveillance Protocol V3,
TIPCU receive notification of a SAB from the Communicable Diseases Prevention Unit (CDPU).
Participating hospitals will receive notification of a SAB from TIPCU and are requested to provide additional information via a SAB Surveillance Form.
All SAB which were collected before the end of the month should have completed surveillance information submitted to TIPCU by the 10th calendar day of the following month or nearest work day.
The TIPCU obtain a monthly summary report detailing all SABs from the participating laboratories. This data is used by TIPCU to validate that all forms received by the IC Teams and GPs correspond with the individual reports of SABs provided by the laboratories.
Publically identified hospital data is published quarterly by the Tasmanian Infection & Control Unit and is available on the TIPCU DHHS website and used in SPP Quarterly Performance Reporting.
Data source TIPCU.
Access to Care (Emergency Care and Elective Surgery)
Percentage of Triage 1 emergency department presentations seen
within the recommended time – AEC1
Definition This KPI measures the percentage of patients that are treated within the national recommended benchmark for waiting times for triage category 1 in public hospital emergency departments.
Calculating
performance The definitions applied are consistent with the national definitions used for reporting against the National Partnership Agreement on Hospital and Health Workforce Reform. The definitions include presentations that have been assigned a triage category between 1 and 5. Presentations that are ‘did not wait’, ‘dead on arrival’ or the waiting time to service delivery is invalid are excluded for the purpose of calculating this KPI. See Australasian Triage Scale from the Australasian College for Emergency Medicine for a description of each triage category, including indicative clinical descriptors.
Time to treatment is calculated by subtracting the date and time the patient presented to the emergency department from the date and time treatment
Service Agreement Key Performance Indicator Definitions
commenced. The time to treatment is then compared to the recommended treatment time for the allocated initial triage category.
The KPI is calculated for triage category 1 and presented as a percentage. Computation: 100 x (Numerator ÷ Denominator)
Numerator: Total number of presentations to emergency departments that were treated within benchmarks for triage category 1:
Triage category 1: seen within seconds, calculated as less than 2 minutes (being a waiting time of 2 or below, which allows for 2:59 seconds*).
* This is in line with the national reporting standards.
Denominator: Total number of triage 1 presentations to emergency departments.
KPI target 100%.
KPI target
source Australasian College for Emergency Medicine.
Assessment
level Facility specific. RHH, LGH, NWRH and MCH.
Assessment
period Performance is assessed quarterly. A new performance assessment period commences at the beginning of each quarter (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source EDIS.
Percentage of Triage 2 emergency department presentations seen
within the recommended time – AEC2
Definition This KPI measures the percentage of patients that are treated within the national recommended benchmark for waiting times for triage category 2 in public hospital emergency departments.
Calculating
performance The definitions applied are consistent with the national definitions used for reporting against the National Partnership Agreement on Hospital and Health Workforce Reform. The definitions include presentations that have been assigned a triage category between 1 and 5. Presentations that are ‘did not wait’, ‘dead on arrival’ or the waiting time to service delivery is invalid are excluded for the purpose of calculating this KPI. See Australasian Triage Scale from the Australasian College for Emergency Medicine for a description of each triage category, including indicative clinical descriptors.
Time to treatment is calculated by subtracting the date and time the patient presented to the emergency department from the date and time treatment commenced. The time to treatment is then compared to the recommended treatment time for the allocated initial triage category.
Computation: 100 x (Numerator ÷ Denominator)
Numerator: Total number of presentations to emergency departments that were treated within benchmarks for triage category 2:
Triage category 2: seen within 10 minutes (being a waiting time of 10 or below, which allows for 10:59 seconds*).
* This is in line with the national reporting standards.
Denominator: Total number of triage 2 presentations to emergency departments.
KPI target 80%.
KPI target
source Australasian College for Emergency Medicine.
Assessment
level Facility specific. RHH, LGH, NWRH and MCH.
Assessment
period Performance is assessed quarterly. A new performance assessment period commences at the beginning of each quarter (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source EDIS.
Percentage of emergency department did not wait presentations –
AEC3
Definition This KPI measures the percentage of emergency department presentations that concluded with the patient leaving the emergency department before being attended by a health care professional.
Calculating
performance The definitions applied were set by the Emergency Care Network Steering Committee. The definitions include presentations that have been assigned a triage category between 1 and 5. Presentations that are ‘dead on arrival’ or the waiting time to service delivery is invalid are excluded for the purpose of calculating this KPI. See Australasian Triage Scale from the Australasian College for Emergency Medicine for a description of each triage category, including indicative clinical descriptors.
The KPI is presented as a percentage.
Numerator: Total number of presentations who have been identified as ‘did not wait’.
Denominator: Total number of presentations to emergency departments. KPI target </= 5%.
KPI target
source Emergency Care Network Steering Committee.
Assessment
Service Agreement Key Performance Indicator Definitions
Assessment
period Performance is assessed quarterly. A new performance assessment period commences at the beginning of each quarter (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source EDIS.
Time until most admitted patients (90%) departed emergency
department – AEC4
Definition This KPI measures the time within which 90% of patients were admitted and physically left the emergency department.
Calculating
performance Numerator: • include records with the triage categories from 1 to 5. • exclude records if the Waiting time to service is invalid, i.e.
- Length of stay < 0.
- Presentation date or time is missing.
- Physical departure date or time is missing.
The 90th percentile (the ninetieth percentage value in a group of data arranged from lowest to highest value for time waited) represents the time within which 90% of patients were admitted and physically left the emergency department.
For example, if there were 100 observations admitted to the hospital, the 90th percentile will correspond to the average time for the 90th and 91st observations. If there were 101 observations, the 90th percentile will correspond to the time for the 91st observation.
Emergency department stay time is calculated by subtracting the date and time the patient presented to the emergency department from the date and time the patient physically left the emergency department.
Denominator: Not applicable. KPI target </= 8 hours.
KPI target
source National Health Performance Authority.
Assessment
Level Facility specific. RHH, LGH, NWRH and MCH.
Assessment
period Performance is assessed quarterly. A new performance assessment period commences at the beginning of each quarter (i.e. performance is not measured on a year to date basis).
Frequency of data collection and
performance assessment
Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source EDIS.
Ambulance offload delay part 1 – AEC5
Definition This KPI measures the percentage of Ambulance Tasmania presentations to an emergency department for which transfer of clinical care to the emergency department occurs within the Australasian College for Emergency Medicine recommended target times (see below).
Calculating
performance This KPI is measured as a percentage. The definitions applied were recommended by the Australasian College for
Emergency Medicine. The definitions include presentations that have been assigned a triage category between 1 and 5. Presentations that are 'dead on arrival' are
excluded for the purpose of calculating this KPI. The definition includes
presentations that arrive by Ambulance Tasmania (arrival modes such as police, non-emergency patient transport are out of scope).
Numerator: Total number of Ambulance Tasmania presentations to an
emergency department where transfer of clinical care to the emergency department occurred within the following target times:
85% of presentations transferred within 15 minutes.
100% of presentations transferred within 30 minutes.
Denominator:
Total number of Ambulance Tasmania presentations to the emergency department.
KPI target 85% within 15 minutes.
KPI target
source Australasian College for Emergency Medicine.
Assessment
Level Facility specific. RHH, LGH, NWRH and MCH.
Assessment
period Performance is assessed quarterly. A new performance assessment period commences at the beginning of each quarter (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source EDIS.
Ambulance offload delay part 2 – AEC6
Definition This KPI measures the percentage of Ambulance Tasmania presentations to an emergency department for which transfer of clinical care to the emergency department occurs within the Australasian College for Emergency Medicine recommended target times (see below).
Calculating
performance This KPI is measured as a percentage. The definitions applied were recommended by the Australasian College for
Service Agreement Key Performance Indicator Definitions
triage category between 1 and 5. Presentations that are 'dead on arrival' are excluded for the purpose of calculating this KPI. The definition includes
presentations that arrive by Ambulance Tasmania (arrival modes such as police, non-emergency patient transport are out of scope).
Numerator: Total number of Ambulance Tasmania presentations to an
emergency department where transfer of clinical care to the emergency department occurred within the following target times:
85% of presentations transferred within 15 minutes.
100% of presentations transferred within 30 minutes.
Denominator:
Total number of Ambulance Tasmania presentations to the emergency department.
KPI target 100% within 30 minutes.
KPI target
source Australasian College for Emergency Medicine.
Assessment
level Facility specific. RHH, LGH, NWRH and MCH.
Assessment
period Performance is assessed quarterly. A new performance assessment period commences at the beginning of each quarter (i.e. performance is not measured on a year to date basis).
Frequency of data collection
Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source EDIS.
Access to Elective Surgery
Baseline elective surgery admissions – AES1a
Definition This KPI measures the total number of admissions for elective surgery from the elective surgery wait list, excluding activity funded under the Rebuilding Health Services (RHS) program, and the Tasmanian Health Assistance Package (THAP). Calculating
performance Count of admissions for surgery where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’, and the funding source is ‘Regular’. KPI target Baseline elective surgery admissions: 14 126.
KPI target
source DHHS – SPP.
Assessment
level Whole of THS.
Assessment
period Performance is assessed quarterly on a year-to-date basis. Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Rebuilding Health Services – AES1b
Definition This KPI measures elective surgery which is funded under the Rebuilding Health Services (RHS) program.
Calculating
performance Count of admissions for surgery where the funding source is ‘RHS’ and where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
KPI target Number of admissions: 2 260.
KPI target
source DHHS – SPP.
Assessment
level Whole of THS.
Assessment
period Performance is assessed quarterly on a year-to-date basis. Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Tasmanian Health Assistant Package admissions – AES1c
Definition This KPI measure activity funded under the Tasmanian Health Assistance Package (THAP).
Calculating
performance Count of admissions for elective surgery where the funding source is ‘THAP’ and where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
KPI target Number of THAP funded admissions: 2 190.
KPI target
source DHHS – SPP.
Assessment
level Whole of THS.
Assessment
period Performance is assessed quarterly on a year-to-date basis. Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Average overdue days – AES2
Definition This KPI measures the average number of overdue days waiting of patients who have waited beyond the clinically recommended time.
Calculating
performance Numerator: Denominatorcount of the total number of overdue days waiting for all patients. : the number of patients who have waited beyond the clinically recommended time.
KPI target December 2015: 177.
Service Agreement Key Performance Indicator Definitions KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly as at the end of the period. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Maximum wait time – AES3
Definition This KPI measures the maximum waiting time for patients who are on the elective surgery list waiting for a surgical procedure.
Calculating
performance The number of days waiting for the longest waiting patient on the elective surgery waiting list.
KPI target December 2015: 730.
June 2016: 600. KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly as at the end of the period. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Category 1 admitted within the recommended time – AES4
Definition This KPI measures the number of Category 1 patients who are admitted for surgery within the clinically recommended timeframe of 30 days.
Calculating
performance This KPI is expressed as a percentage. Numerator: Total number of Category 1 patients admitted within the clinically recommended time of 30 days or less, where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
Denominator:
Total number admissions for Category 1 patients where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
KPI target December 2015: 80%.
June 2016: 90%. KPI target
source
Assessment level
Whole of THS. Assessment
period
Performance is assessed 6 monthly. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of data collection
Monthly. Data collected through Health Central from iPM.
Data source iPM.
Category 2 admitted within the recommended time – AES5
Definition This KPI measures the number of Category 2 patients who are admitted for surgery within the clinically recommended time of 90 days.
Calculating
performance This KPI is expressed as a percentage. Numerator: Total number of Category 2 patients removed from the wait list within the clinically recommended time of 90 days or less, where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
Denominator:
Total number admissions for Category 2 patients where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
KPI target December 2015: 60%.
June 2016: 70%. KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Category 3 admitted within the recommended time – AES6
Definition This KPI will measure number of Category 3 patients who are admitted for surgery within the clinically recommended timeframe of 365 days.
Calculating performance
This KPI is expressed as a percentage.
Numerator: Total number of Category 3 patients removed from the wait list within the clinically recommended time of 365 days or less, where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
Denominator:
Total number admissions for Category 3 patients where the removal reason is ‘Planned Procedure Completed’ or ‘Admitted as emergency’.
Service Agreement Key Performance Indicator Definitions June 2016: 70%. KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Category 2 treat in turn rates – AES7
Definition This indicator measures the number of Category 2 patients who are treated in turn. Calculating
performance This KPI is expressed as a percentage. The ‘Treat in Turn’ report reports on activity over a rolling 12 month period, updated on a quarterly basis.
Numerator: count of the number of Category 2 patients who are admitted for surgery and who are treated within 90 days, but not before 31 days, from the time they are added to the wait list.
Denominator: count of the total number of category 2 patients admitted for surgery.
KPI target December 2015: 40%.
June 2016: 45%. KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly as at the end of the period. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Data is collected quarterly and reported over a 12 month rolling period. Performance is assessed on a quarterly basis.
Data source iPM.
Category 3 treat in turn rates – AES8
Definition This indicator measures the number of Category 2 patients who are treated in turn Calculating
performance This KPI is expressed as a percentage. The ‘Treat in Turn’ report reports on activity over a rolling 12 month period, updated on a quarterly basis.
Numerator: count of the number of Category 3 patients who are admitted for surgery and who are treated within 365 days, but not before 91 days, from the time
they are added to the wait list.
Denominator: count of the total number of category 3 patients admitted for surgery.
KPI target December 2015: 40%.
June 2016: 45%. KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly as at the end of the period. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Data is collected quarterly and reported over a 12 month rolling period. Performance is assessed on a quarterly basis.
Data source iPM.
Hospital initiated postponements (HIPs) – AES9
Definition This KPI measures the number of hospital initiated postponements. Calculating
performance Count of the total number of scheduled appointments for elective surgery that are cancelled by the hospital.
KPI target December 2015: 14.7%.
June 2016: 12.6%. KPI target source DHHS – SPP. Assessment level Whole of THS. Assessment
period Performance is assessed 6 monthly. A new performance assessment period commences at the beginning of each six month period (i.e. performance is not measured on a year to date basis).
Frequency of
data collection Monthly. Data collected through Health Central from iPM.
Data source iPM.
Mental Health
28 Day re-admission rate – MH1
Definition This KPI measures the percentage of overnight separations from an acute inpatient unit that are followed by readmission to the same or a similar type unit MHS Inpatient within 28 days of discharge.
Calculating
performance This KPI is measured as a percentage.
Service Agreement Key Performance Indicator Definitions
unit occurring within the reference period that are followed by a readmission to the same or similar type unit within 28 days.
Denominator: Number of in scope overnight separations from the acute inpatient unit in the reference period.
Coverage / scope: The following separations are excluded:
Same day separations.
Statistical and change of care type separations.
Separations that end by transfer to another acute or psychiatric hospital.
Separations that end by left against medical advice / discharge at own risk.
Separations where length of stay is one night only and procedure code for ECT is recorded.
KPI target </=13.9%. KPI target
source The target is based on the latest nationally reported average of 13.9% (the latest published Australian average (https://mhsa.aihw.gov.au/KPIs/nkpi/). Assessment
level Whole of THS.
Assessment
period Performance is assessed quarterly on a year to date basis. Frequency of
data collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source iPM.
Acute 7 day post discharge community care – MH2
Definition This KPI measures the percentage of separations from an acute psychiatric inpatient unit for which a community ambulatory or inpatient service contact, in which the consumerparticipated, was recorded in the 7 days immediately following that separation.
Inpatient service contacts must only be used for clients referred to an external provider and not clients already referred to a community ambulatory team. Clients referred to a community ambulatory service must be contacted by the community service.
Calculating
performance This KPI is measured as a percentage.
Numerator: Number of overnight separations from the acute inpatient unit occurring, within the reference period, for which a community mental health service or inpatient contact, in which the consumer participated, was recorded in the 7 days immediately following that separation.
Denominator: Number of overnight separations from the acute inpatient unit in the reference period.
KPI target 75%.
source 2013) is 60.7%.
As the national KPI is based solely on community ambulatory service contacts the inclusion of contacts from the inpatient units for clients referred to an external provider is expected to significantly increase the number of clients contacted and 75% is considered an appropriate target for 2015 – 2016.
It is expected in the medium term that the target will increase to reflect the need to contact all clients being discharged from an inpatient unit.
The latest published Australian average is available here:
https://mhsa.aihw.gov.au/KPIs/nkpi/. Assessment
level Whole of THS.
Assessment
period Performance is assessed quarterly on a year to date basis. Frequency of
data collection Monthly. Data collected through Health Central from iPM on the sixth working day of the month.
Data source iPM.
Seclusion rates – MH3
Definition This KPI measures the number of seclusion events per 1,000 patient days within an in scope unit.
Calculating performance
Unit of measurement: Count.
Numerator: Number of seclusion events occurring in the mental health service’s inpatient units during the reference period.
Denominator: Number of accrued mental health care days within the mental health services inpatient units during the reference period.
Coverage / scope:
• All public health mental health admitted patient services approved for involuntary clients.
KPI target <8 per 1000 patient days
KPI target source
The latest Nationally reported average as per the AIHW Mental Health Services in Australia website http://mhsa.aihw.gov.au/KPIs/nkpi/ in 2012-2013 of 8 events per 1,000 patient days.
Continuous improvement is expected, even in circumstances where performance is below the specified target, with the ultimate aim of 0 seclusion events
Assessment
level Whole of THS.
Assessment
period Performance is assessed quarterly on a year to date basis. Frequency of
data collection
Monthly. Data collected through Health Central from iPM on the sixth working day of the month.