HUMAN PAPILLOMA VIRUS GENOTYPING IN A GROUP OF IRAQI WOMEN BY USING REPRODUCIBLE DNA EXTRACTION FROM FORMALIN FIXED PARAFFIN EMBEDDED SECTIONS
Full text
Figure
Related documents
DEG: Differentially expressed gene; FC: Fold change; FFPE: Formalin fixed paraffin embedded; FPKM: Fragments per kilobase of exon per million; HRCT: High-resolution computed
As the successful labelling of sarcolemmal membrane-associated proteins in formalin-fixed and paraffin-embedded (FFPE) muscle sections using IHC staining has rarely been described,
Gene expression analysis of normal and colorectal cancer tissue samples from fresh frozen and matched formalin-fixed, paraffin-embedded (FFPE) specimens after manual and automated
The present study was designed to evaluate a chip-based digital PCR (dPCR) system for assessing HER2 amplification from formalin-fixed paraffin-embedded breast carcinoma tissue and
By applying the four PCR assays to the 11 formalin-fixed, paraffin-embedded autopsy samples from patients with a clin- ical history of tuberculosis, a Ziehl-Neelsen-positive
Detection of Mycobacterium bovis in formalin-fixed, paraffin-embedded tissues of cattle and elk by PCR amplification of an IS6110 sequence specific for Mycobac- terium
ELISA: Enzyme-linked immunosorbent assays; FFPE: Formalin-fixed and paraffin-embedded; GAPDH: Glyceraldehyde-3-phospate dehydrogenase; IHC: Immunohistochemistry; RPPA: Reverse
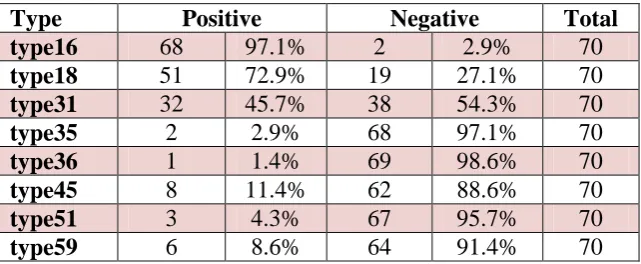
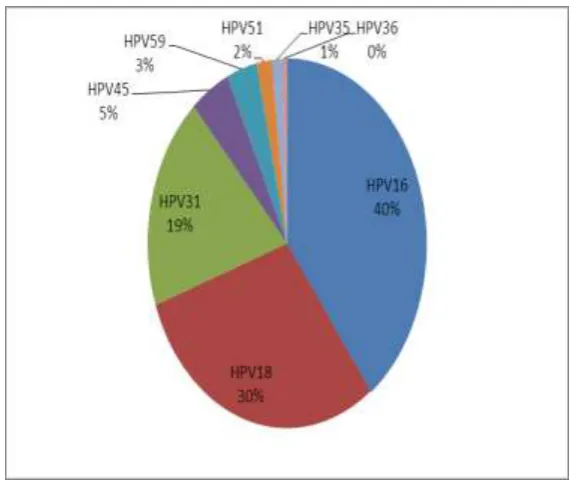
A total of 112 archived formalin- fixed and paraffin-embedded cervical tissue blocks dated 2009-2015, with histological diagnosis of invasive cervical cancer were
