Krzysztof Woźniak
1, A–F, Hubert Teichert
2, A–F, Dagmara Piątkowska
1, A, D–F,
Mariusz Lipski
3, A, D–FAn Assessment of Relationships Between the Five-Factor
Personality Model and the Morphology and Function
of the Stomathognatic System
Ocena zależności między pięcioczynnikowym modelem osobowości
a morfologią i czynnością układu stomatognatycznego
1 Department of Orthodontics, Pomeranian Medical University, Szczecin, Poland 2 Teichert & Partners: Psychology and Business, Szczecin, Poland
3 Department of Preclinical Conservative Dentistry and Preclinical Endodontics, Pomeranian Medical University,
Szczecin, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. The personality as a system of genetically predetermined features is responsible for modifying rela-tions between an individual’s genotype and phenotype. The key element linking personality with facial morphology is the muscular system.
Objectives. The aim of this study was to investigate the association between facets of the five-factor personality model (FFM) domains and both the morphology and function of the stomathognatic system.
Material and Methods. Two hundred volunteers (100 female and 100 male) aged 20 to 25 (mean age: 23.4) under-went anthropometric measurements to calculate the anterior face height ratio N-Sn/Sn-Gn. For cephalometric analysis, standard right-profile images of the face were used. Calibration was performed with a 100-mm metal ruler placed next to each photographed individual. The Revised NEO Personality Inventory (NEO-PI-R), which includes 240 statements, was used for personality assessment in order to investigate the five main personality domains: neuroticism, extraversion, openness to experience, agreeableness, conscientiousness and six facets within each domain.
Results. The results show significant correlations between factors of the personality such as neuroticism (r = 0.3488; p = 0.0000) and extraversion (r = –0.3405; p = 0.0000) and the inclination angle (FH/HOR) as the predictor of the function of the stomathognatic system. Additionally, the correlation analysis revealed a significant positive associa-tion between the anterior face height ratio and anxiety (r = 0.3952; p = 0.0000).
Conclusions. The results of this study indicate a selective association between personality and both the morphol-ogy and function of the stomathognatic system (Adv Clin Exp Med 2012, 21, 5, 637–643).
Key words: personality, anxiety, NEO-PI-R, face morphology.
Streszczenie
Wprowadzenie. Osobowość jako zespół cech zdeterminowanych genetycznie, jest odpowiedzialna za modyfiko-wanie relacji zachodzących między genotypem człowieka a jego fenotypem. W obrębie głowy elementem łączącym osobowość z morfologią twarzy jest układ mięśniowy.
Cel pracy. Określenie związku między aspektami pięcioczynnikowego modelu osobowości (PMO) a morfologią i czynnością układu stomatognatycznego.
Materiał i metody. Dwustu ochotnikom (100 kobiet i 100 mężczyzn) w przedziale wiekowym 20–25 lat (średnia 23,4) wykonano pomiary antropometryczne w celu obliczenia indeksu przedniej wysokości twarzy (N-Sn/Sn-Gn). Pomiary cefalometryczne wykonano na standardowych zdjęciach prawego profilu twarzy. Do kalibracji zdjęć
wyko-Adv Clin Exp Med 2012, 21, 5, 637–643 ISSN 1899–5276
ORIGINAL PAPERS
Numerous long-term studies on the five-fac-tor personality model (FFM), implementing mul-tivariate analysis, have resulted in the creation of the five-factor theory of personality (the “big five”) [1–3]. In this model, the personality is described by certain unique traits. A primary stipulation of this theory is that features of the personality are endogenous basic qualities of the inheritable type with little environmental influence [4]. These qualities tend to develop from early childhood up to adulthood, when their ultimate shape is ac-quired. The features are organized hierarchically, from strictly determined and specific ones to gen-eral ones.
The topmost part of this hierarchy is shaped by the traits constituting the “big five”: neuroti-cism, extraversion, openness, agreeableness, and conscientiousness. The validity of the five-factor personality model has been ascertained by the intercultural convergence of its principles with roots in lexical hypotheses [5]; by the associa-tion between self-descripassocia-tions and descripassocia-tions of studied individuals by their relatives and friends; by internal correlations between indicators related to personality traits and indicators of motivation, emotion and interpersonal contact; by diagnoses of personality disturbance related to the dimen-sions and facets of personality factors rather than categories [6]; and by genetic evidence and evolu-tion theory [7].
Neuroticism is one of the best investigated traits among the “big five”. It is also known as emotional sensitivity, or emotional instability/ reactivity. It reflects emotional adaptation as op-posed to emotional instability. It refers directly to the tendency to experience negative emotions such as anger, sadness, fear, embarrassment, guilt and disgust. These emotions commonly impair the process of adaptation, therefore neurotic individu-als may be more prone to accept irrational ideas and fantasies, and may tend to present worse im-pulse control and difficulty to cope with stress ef-fectively. It is also related to nervousness, excessive emotional reactions, a feeling of endangerment and an inclination to be hypochondriac. Other
facets of this domain include excessive unneces-sary worrying and low self-esteem [8].
Neuroticism is comprised of angry hostility, depressiveness, overt criticism, impulsiveness and hypersensitivity to anxiety. Anxiety is often con-fused with fear, which occurs only in the situation of natural, immediate and real danger. Anxiety is experienced in the context of imaginary situations, which might or might not appear, and in most cas-es is not linked with any observable reason [9].
In dentistry, fear as a psychological factor is addressed as a basic feature influencing the shape and function of the stomatoghathic system, along with psychiatric illnesses, disturbances of occlu-sion, orthopedic dysfunctions, isometric muscle work, the influence of physical factors (cold, hu-midity, the climate), hormonal and metabolic in-fluences, the proprioceptive reflex from dysfunc-tional and improperly or overly loaded joints, or joint microinjuries.
Difficulties with controlling aggression and fear lead to functional body changes – for exam-ple, excessive muscular tension and hyperactivity cause a long-term, non-physiological load on the supportive tissues [10]. This process may result in morphological changes of the face.
The aim of this study was to investigate the as-sociation between the facets of the five-factor per-sonality model domains and the morphology and function of the stomathognatic system.
Material and Methods
Two hundred volunteers (100 female and 100 male) aged 20 to 25 (mean age: 23.4) partici-pated in this study. Cephalometric measurements were done on the basis of standard right-profile images of the face, stored in Adobe Photoshop software. Prior to conducting the vertical linear measurements, verification and calibration of the true image size was performed, using a 100-mm metal ruler placed near each of the photographed individuals. Each picture was taken at a distance of one meter from the photographed individual,
rzystano 100 mm metalową linijkę umieszczoną w pobliżu twarzy każdej fotografowanej osoby. Oceny osobowości dokonano, używając inwentarza osobowości NEO-PI-R. Inwentarz ten składa się z 240 twierdzeń umożliwiających pomiar 5 głównych obszarów osobowości: neurotyzmu, ekstrawersji, otwartości na doświadczenia, sumienności, ugodowości oraz 6 składników w obrębie każdego z nich.
Wyniki. Uzyskane wyniki wskazują na statystycznie istotną korelację czynników osobowości i kąta inklinacji (FH/ HOR) jako predykatora czynności układu stomatognatycznego w aspekcie Neurotyczności (r = 0.3488; p = 0.0000) i Ekstrawertyczności (r = –0,3405; p = 0,0000). Ponadto analiza korelacji wykazała pozytywną zależność między indeksem przedniej wysokości twarzy a lękiem (r = 0,3952; p = 0,0000).
Wnioski. Wyniki badań wskazują na wybiórczy związek osobowości z morfologią i czynnością układu stomatogna-tycznego (Adv Clin Exp Med 2012, 21, 5, 637–643).
using a Canon IXY Digital 800 IS camera in the same lighting conditions. Study participants were seated on a chair in an upright position with the head in its natural position (NHP), with teeth in maximum intercuspidation and lips in repose.
First, two anthropometric linear measure-ments – nasion to subnasale (N-Sn) and subnasale to gnathion (Sn-Gn) were measured on each of the lateral photographs, and were used to estimate the anterior face height ratio N-Sn/Sn-Gn (in %). One angular measurement was also made: the inclina-tion angle (FH/HOR), between the Frankfort hor-izontal (FH) line and the extracranial horhor-izontal (HOR) line with the head in the NHP. If the Frank-fort horizontal line is formed over the extracranial horizontal line passing through the Tragus point, the angle is read in positive degrees. If the Frank-fort horizontal is formed below the extracranial horizontal line passing through the Tragus point, the angle is read in negative degrees [11].
The survey comprised the second part of the research. The Revised NEO Personality Inventory (NEO-PI-R), which included 240 statements, was used. The inventory allows the five main person-ality domains to be investigated: neuroticism, ex-traversion, openness to experience, agreeableness and conscientiousness, with six facets within each of them. The analyzed facets include:
– for neuroticism: anxiety, angry hostility, de-pression, self-consciousness, impulsiveness and vulnerability;
– for extraversion: warmth, gregariousness, assertiveness, activity, excitement seeking and ex-perience of positive emotions;
– for openness to experience: fantasy, esthet-ics, feelings, actions, ideas and values;
– for agreeableness: trust, straightforwardness, altruism, compliance, modesty and tenderness;
– for conscientiousness: competence, order, dutifulness, achievement striving, self-discipline and deliberation.
To complete the NEO-PI-R study, the partici-pants recorded their responses using the five-point Likert scale, ranging from “strongly disagree” (0) to “strongly agree” (4). The time allowed for com-pleting the inventory was from 35 to 45 minutes [12, 13].
Linear regression analysis was used to check the association between the dependent variable of the anterior face height ratio and the independent variables of the facets. The significance level for all statistical comparisons was predetermined at the threshold of p ≤ 0.05. The data analysis was per-formed with Statistica 7.0 software (Stat Soft. Inc.).
Results
Table 1 presents results of the anterior face height ratio N-Sn/Sn-Gn (in %). The anterior face height ratio varied from 65.91% to 119.60% (mean: 80.70%). Female participants tended to present a larger inclination (mean: 81.02%) than the males (meanL 80.38%). There were no significant differ-ences between the male and female subjects (p = 0.8679).
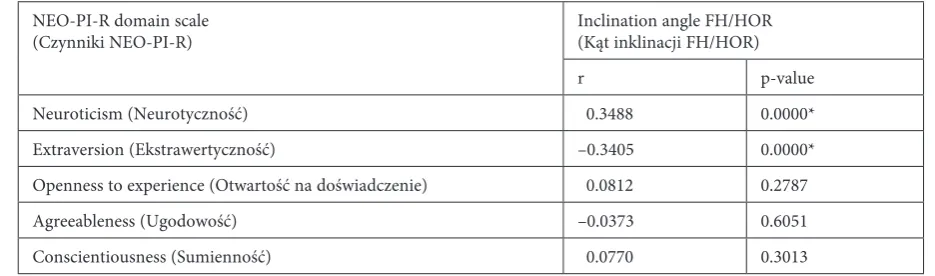
The results in Table 2 show significant correla-tions between the factors of the personality such as neuroticism (r = 0.3488; p = 0.0000) and extraver-sion (r = –0.3405; p = 0.0000) and the inclination angle (FH/HOR) assesed in NHP as a predictor of the function of the stomathognatic system.
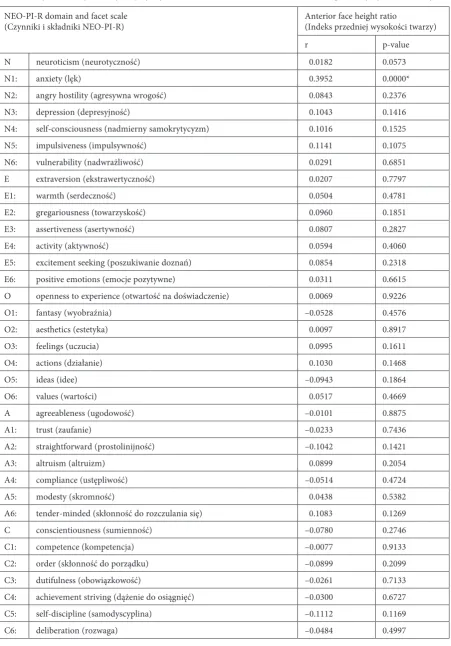
Table 3 presents the Pearson correlation coef-ficients of the anterior face height ratio at each of the personality domains. Among the volunteers, modestly significant positive correlations were found between the anterior face height ratio and anxiety (r = 0.3952; p = 0.0000).
Table 1. The anterior face height ratio (N-Sn/Sn-Gn). Mean, median and standard deviations as well as min-max values are presented in percentages
Tabela 1. Indeks przedniej wysokości twarzy (N-Sn/Sn-Gn). Wartości średniej, mediany, odchylenia standardowego i warto-ści min-max zostały wyrażone w procentach
N-Sn/Sn-Gn N Mean
(Średnia) Median(Mediana) SD Minimum Maximum p-value Female
(Kobiety) 100 81.02 79.46 8.98 65.91 119.6 0.8679
Male
(Mężczyźni) 100 80.38 80.08 5.99 68.75 100.00
Total
Discussion
Alongside Sheldon’s theory, the most popular classification based on constitutional personality types was created by Kretschmer, who associated the body type with temperament and psyche. Each of the constitutional types was described by char-acteristic features. The leptosomic type (thin and weak) was associated with a schizothymic temper-ament and a tendency to develop schizophrenia in adult life, and to suffer more frequently from tuberculosis and gastritis. Pyknic people were supposed to present a cyclothymic temperament, a tendency for depression, cardiovascular disease, arteriosclerosis, arthritis, cholelithiasis, pancreati-tis and diabetes. People of athletic type tended to be predisposed to epilepsy, vasomotor head dis-turbance (migraine) and asthma. Further studies on personality traits as a factor influencing human functioning have confirmed these relationships [14–16].
The personality as a system of genetically pre-determined features is responsible for modifying relations between an individual’s genotype, which provides background developmental capabilities, and the external environmental factors that influ-ence phenotypic variability. For the head, the key element linking genetically determined personal-ity with facial morphology is the muscular system. If it is assumed that function is superior to shape, changes in the muscular part of the stomatogha-thic system during the developmental stages of life induce alterations in morphology.
Individuals with a strong element of anxiety presenting in the personality structure experience strong and overwhelming feelings of tension and concern. They are filled with insecurity, timidity, feelings of misadaptation, personal unattractive-ness and low self-esteem [8]. At a somatic level, this
results in a constant state of overload, manifesting as an increase in muscular tension not only within the stomathoghatic system but also within the in-dividual’s whole motor system. Moreover, a crav-ing for acceptance and recognition with increased sensitivity to criticism and rejection enhances the tendency to withdraw from social contacts, with fear of being criticized resulting in additional feel-ings of self-worthlessness.
Importantly, restraint from verbal expres-sion (“teeth clenching”) is intensified, for fear of being judged by the social sphere when express-ing unpopular personal opinions or feelexpress-ings (e.g. of discontentment). Other reason for an increase in muscular tension is constant anticipation of an imaginary attack from the people around one. Continuous control over one’s personal reactions and analysis of behavior are other reasons for muscle tensing, along with the raising of a psycho-logical barrier preventing the expression of natural and spontaneous reactions. A permanent increase in muscular tension results in impairment of verti-cal facial growth, manifesting morphologiverti-cally in lower face height.
The influence of psychological factors on the stomathonathic system is also present after growth has concluded. This is especially important for pa-tients with temporomandibular disorders (TMDs) – a group of conditions characterized by pain or dysfunction in the temporomandibular joint (TMJ) and/or the muscles of mastication. TMD can include myofascial pain, internal derangement and/or degenerative changes of the temporoman-diblular joint. TMD pain is a common and costly problem affecting approximately to 15% of the adult population [17, 18]. These patients also have a lower pain threshold and increased response to experimental pain stimuli. There are many theo-ries attempting to explain the cause of these
dif-Table 2. Correlations between the five-factor model and the inclination angle FH/HOR in NHP
Tabela 2. Wyniki analizy korelacji między pięcioma głównymi czynnikami osobowości a kątem inklinacji FH/HOR w NHP
NEO-PI-R domain scale
(Czynniki NEO-PI-R) Inclination angle FH/HOR(Kąt inklinacji FH/HOR)
r p-value
Neuroticism (Neurotyczność) 0.3488 0.0000*
Extraversion (Ekstrawertyczność) –0.3405 0.0000*
Openness to experience (Otwartość na doświadczenie) 0.0812 0.2787
Agreeableness (Ugodowość) –0.0373 0.6051
Conscientiousness (Sumienność) 0.0770 0.3013
* p-value ≤ 0.05.
Table 3. Correlations between the domains and facets of the personality and the anterior face height ratio
Tabela 3. Wyniki analizy korelacji między czynnikami i składnikami osobowości a indeksem przedniej wysokości twarzy
NEO-PI-R domain and facet scale
(Czynniki i składniki NEO-PI-R) Anterior face height ratio(Indeks przedniej wysokości twarzy)
r p-value
N neuroticism (neurotyczność) 0.0182 0.0573
N1: anxiety (lęk) 0.3952 0.0000*
N2: angry hostility (agresywna wrogość) 0.0843 0.2376
N3: depression (depresyjność) 0.1043 0.1416
N4: self-consciousness (nadmierny samokrytycyzm) 0.1016 0.1525
N5: impulsiveness (impulsywność) 0.1141 0.1075
N6: vulnerability (nadwrażliwość) 0.0291 0.6851
E extraversion (ekstrawertyczność) 0.0207 0.7797
E1: warmth (serdeczność) 0.0504 0.4781
E2: gregariousness (towarzyskość) 0.0960 0.1851
E3: assertiveness (asertywność) 0.0807 0.2827
E4: activity (aktywność) 0.0594 0.4060
E5: excitement seeking (poszukiwanie doznań) 0.0854 0.2318
E6: positive emotions (emocje pozytywne) 0.0311 0.6615
O openness to experience (otwartość na doświadczenie) 0.0069 0.9226
O1: fantasy (wyobraźnia) –0.0528 0.4576
O2: aesthetics (estetyka) 0.0097 0.8917
O3: feelings (uczucia) 0.0995 0.1611
O4: actions (działanie) 0.1030 0.1468
O5: ideas (idee) –0.0943 0.1864
O6: values (wartości) 0.0517 0.4669
A agreeableness (ugodowość) –0.0101 0.8875
A1: trust (zaufanie) –0.0233 0.7436
A2: straightforward (prostolinijność) –0.1042 0.1421
A3: altruism (altruizm) 0.0899 0.2054
A4: compliance (ustępliwość) –0.0514 0.4724
A5: modesty (skromność) 0.0438 0.5382
A6: tender-minded (skłonność do rozczulania się) 0.1083 0.1269
C conscientiousness (sumienność) –0.0780 0.2746
C1: competence (kompetencja) –0.0077 0.9133
C2: order (skłonność do porządku) –0.0899 0.2099
C3: dutifulness (obowiązkowość) –0.0261 0.7133
C4: achievement striving (dążenie do osiągnięć) –0.0300 0.6727
C5: self-discipline (samodyscyplina) –0.1112 0.1169
C6: deliberation (rozwaga) –0.0484 0.4997
* p-value ≤ 0.05.
ferences, but psychological theories are among the most credible [17, 18].
The current authors’ review of papers by Turner and Dworkin [19] related to TMD and psychological factors, published from1995 to 2002, provided some interesting insights. There was substantial empirical evidence that psychosocial factors play an important role in the symptoms, symptom impact and treatment response of pa-tients with TMD. Depression, somatization and anxiety are prevalent among patients with TMD. These factors in particular have been indicated to influence the expression of the signs and symp-toms of TMD.
Anxiety is a negative emotional condition linked to the expectation of external or internal danger, often reflected as uneasiness, a feeling of tension, embarrassment or a sense of being threat-ened. In contrast to fear, it is an internal pro-cess, not directly linked to any immediate threat or pain. Anxiety becomes pathological, when it dominates personal behavior, restricts freedom and in consequence leads to various disturbances. Anxiety reactions lose their adaptative function and become inadequate to the stimuli, often exac-erbated by situations in which there is no threat. It is often accompanied by vegetative components of various types, such as tremors, increased muscular tension, tingling, heart pain, breathing problems, diarrhea and/or nycturia. Anxiety is associated with a number of psychopathological reactions, especially when it is perceived as a cognitive risk factor for panic disorders [9].
Somatization has been defined by Sherman et al. as “the tendency to experience numerous physical symptoms for which no apparent organic cause can be determined. Alternatively, if a medi-cal cause is present, somatization is said to occur when complaints about the bodily disturbance and dysfunction are in excess of the pathology. Barsky suggests that somatization is related to an amplifi-cation of bodily signals” [20, 21]. It is necessary to refer patients to an appropriately trained psychol-ogist or psychiatrist if one or more of the following
symptoms is noted in their history: disability (in daily work, household maintenance, recreational and social activities) out of proportion to objec-tive findings; symptoms of psychological disor-ders (most commonly depression, anxiety or so-matization); prolonged or excessive use of opiates, benzodiazepines, alcohol or other drugs. It must also be emphasized here that patients qualified as moderately or severely disabled should undergo multidisciplinary treatment, aiming at reducing the psychological factor in TMD etiology.
The relationship between mood and somatic ailments requires a thorough assessment of the psychometric point of view. The axis that best describes the character of the symptoms is neu-roticism. It may be assumed that complaints are more related to a real ailment and symptoms in people with a low level of neurotism, in compari-son to individuals with a higher level of this factor. Generally, neurotism is of such importance in the research on the psychological aspects of health, es-pecially stress-related aspects, that it should always be measured and controlled [4].
Clinical research, health-related psychology and behavioral medicine are three branches of research where psychometric tools, including the NEO Personality Inventory (NEO-PI-R) are used. The choice of this tool is justified by the strong as-sociation between health status and lifestyle, which in turn is a sum of personality facets. It is clear that in every aspect of human life, from one’s pro-fessional and recreational interests to one’s reac-tions to stress, personality determinants play a key role, becoming a cognitive filter that enhances or reduces the interaction of environmental factors with the body. It must be emphasized that per-sonality features, as the most basic and permanent tendencies, have a wide range of influence on an individual’s acquired interactions with the envi-ronment.
The results of this study indicate that there is a selective association between the personality and both the morphology and function of the stoma-thognatic system.
References
[1] Costa PT: Clinical use of the five-factor model: An introduction. J Pers Assess 1991, 57, 393–398.
[2] Costa PT, Mcrae RR: Four ways five factors are Basic. Pers Individ Dif 1992, 13, 653–665.
[3] Deary IJ: A (latent) big five personality model in 1915? A reanalysis of Webb’s data. J Pers Soc Psychol 1996, 71, 992–1005.
[4] Mcrae RR, John OP: An introduction to the five-factor model and its applications. J Pers 1992, 60, 175–215.
[5] Goldberg LR: The structure of phenotypic personality traits. Am Psychol 1993, 48,26–34.
[6] Widiger TA: The DSM-III-R categorical personality disorder diagnoses: A critique and alternative. Psychol Inq 1993, 4, 75–90.
[7] Jang KL, Livesley JW, Angleitner A, Rieman R, Vernon PA: Genetic and environmental influences on the covari-ance of facets defining the domains of the five-factor model of personality. Pers Individ Dif 2002, 33,83–101.
[9] Cox BJ, Blager SC, Taylor S, Fuentes K, Ross LM: Anxiety sensitivity and five-factor model of personality. Behav Res Ther 1999, 37, 633–641.
[10] Raftowicz-Wójcik K, Matthews-Brzozowska T, Kawala B, Antoszewska J: The Effects of Breast Feeding on Occlusion in Primary Dentition. Adv Clin Exp Med 2011, 20, 3, 371–375.
[11] Downarowicz P, Matthews-BrzozowskaT , Kawala B , Drohomyretska M: Dynamic Changes in Morphometric Analysis in Patients Following Class III Bimaxillary Surgery. Adv Clin Exp Med 2012, 21, 1, 93–97.
[12] McRae RR, Costa PT: Discriminant validity of NEO-PI-R facet scales. Educ Psychol Meas 1992, 52, 229–237.
[13] Costa PT, McCrae RR: Stability and change in personality assessment: The revised NEO Personality Inventory in the year 2000. J Pers Assess 1997, 68, 86–94.
[14] Le Blanc J, Ducharme MB, Thompson M: Study on the correlation of the autonomic nervous system responses to stressor of high discomfort with personality traits. Physiol Behav 2004, 82, 647–652.
[15] Saito T, Nakamura T, Endo T: Big Five personality factors related to face recognition. Shinrigaku Kenkyu 2005, 75, 517–522.
[16] Podgórna P, Zawadzka A, Rymaszewska J, Szuba A: Depression and anxiety symptoms and cardiovascular dis-ease in an over-fifty rural population. Adv Clin Exp Med 2007, 16, 4, 513–518.
[17] Więckiewicz M, Paradowska A, Kawala B, Więckiewicz W: SAPHO Syndrome as a Possible Cause of Masticatory System Anomalies – a Review of the Literature. Adv Clin Exp Med 2011, 20, 4, 521–525.
[18] Kawala B, Minch L, Antoszewska J: Temporomandibular Dysfunction and Malocclusion in Young Adult Males – A Clinical Examination in a Medical Experiment. Adv Clin Exp Med 2011, 20, 5, 635–639.
[19] Turner J, Dworkin S: Screening for psychosocial risk factors in patients with chronic orofacial pain. J Am Dent Assoc 2004, 135, 1119–1125.
[20] Sherman J, LeResche L, Huggins KH, Mancl L, Sage J, Dworkin SF: The Relationship of Somatization and Depression to Experimental Pain Response in Women With Temporomandibular Disorders. Psychosom Med 2004, 66, 6, 852–860.
[21] Barsky AJ: Amplification, somatization and the somatoform disorders. Psychosomatics 1992, 33, 28–34.
Address for correspondence:
Dagmara Piątkowska Department of Orthodontics Pomeranian Medical University Al. Powstańców Wlkp. 72/6 70-111 Szczecin
Poland
Tel.: +48 504 012 262
E-mail: [email protected]
Conflict of interest: None declared