Work of Breathing During Constant- and Variable-Flow Nasal Continuous
Positive Airway Pressure in Preterm Neonates
Paresh B. Pandit, MD*‡; Sherry E. Courtney, MD‡§; Kee H. Pyon, PhD‡§; Judy G. Saslow, MD‡§; and Robert H. Habib, PhD储
ABSTRACT. Background. Constant-flow nasal con-tinuous positive airway pressure (NCPAP) often is used in preterm neonates to recruit and maintain lung volume. Physical model studies indicate that a variable-flow NC-PAP device provides more stable volume recruitment with less imposed work of breathing (WOB). Although superior lung recruitment with variable-flow NCPAP has been demonstrated in preterm neonates, corroborating WOB data are lacking.
Objective. To measure and compare WOB associated with the use of variable-flow versus constant-flow NCPAP in preterm neonates.
Methods. Twenty-four preterm infants who were re-ceiving constant-flow NCPAP (means, SD) and had birth weight of 1024ⴞ253 g, gestational age of 28ⴞ1.7 weeks, age of 14ⴞ13 days, and FIO2of 0.3ⴞ0.1 were studied. Variable-flow and constant-flow NCPAP were applied in random order. We measured changes in lung volume and tidal ventilation (VT) by DC-coupled/calibrated respira-tory inductance plethysmography as well as esophageal pressures at NCPAP of 8, 6, 4, and 0 cm H2O. Inspiratory WOB (WOBI) and lung compliance were calculated from the esophageal pressure and VTdata using standard meth-ods. WOB was divided by VTto standardize the results. Results. WOBI decreased at all CPAP levels with variable-flow NCPAP, with a maximal decrease at 4 cm H2O. WOBIincreased at all CPAP levels with constant-flow CPAP. Lung compliance increased at all NCPAP levels with variable-flow, with a relative decrease at 8 cm H2O, whereas it increased only at 8 cm H2O with constant-flow NCPAP. Compared with constant-flow NCPAP, WOBIwas 13% to 29% lower with variable-flow NCPAP.
Conclusion. WOBI is decreased with variable-flow NCPAP compared with constant-flow NCPAP. The in-crease in WOBIwith constant-flow NCPAP indicates the presence of appreciable imposed WOB with this device. Our study, performed in neonates with little lung dis-ease, indicates the possibility of lung overdistention at CPAP of 6 to 8 cm H2O with the variable-flow device. Further study is necessary to determine the efficacy of variable-flow NCPAP in neonates with significant lung
disease and its use over extended periods of time. Pediatrics 2001;108:682– 685; continuous-flow and vari-able-flow NCPAP, work of breathing, premature neonates, lung compliance.
ABBREVIATIONS. NCPAP, nasal continuous positive airway pressure; VL, lung volume; WOB, work of breathing; RIP,
respi-ratory inductance plethysmography; Pes, esophageal pressure; VT,
tidal ventilation;⌬VL, change in lung volume; CL, lung
compli-ance; DC, direct current; RR, respiratory rate; SE, standard error.
N
asal continuous positive airway pressure (NCPAP) often is used in preterm neonates to recruit and maintain lung volume (VL).NCPAP usually is provided by varying the resis-tance to exhalation while constant gas flow is deliv-ered by a neonatal ventilator through nasal prongs (constant-flow NCPAP).
An NCPAP device that uses demand or variable gas flow (variable-flow NCPAP) is available.1,2
Phys-ical model studies comparing constant-flow and variable-flow NCPAP report a relative decrease in airway pressure variability during breathing with variable-flow NCPAP. This indicates a potential for superior lung recruitment and maintenance of VL.1,2
Moreover, Klausner et al2 found that the imposed
work of breathing (WOB) with the variable-flow NC-PAP prongs was one fourth that of conventional constant-flow NCPAP prongs, ascribing this to dif-ferences in prong design. Infant data to support these findings are scarce. In particular, we are unaware of any published data on WOB during variable-flow NCPAP support.
We recently demonstrated that variable-flow NC-PAP provides superior lung recruitment for similar CPAP levels in preterm neonates.3However, the gas
flows required to generate an equivalent CPAP with the variable-flow device generally are greater than with the constant-flow device. Although the design of the variable-flow NCPAP prongs allows for excess gas flow to be diverted away from the patient, it is unclear whether WOB is affected. Thus, our objective was to measure and compare WOB associated with the use of variable-flow versus constant-flow NC-PAP in preterm neonates.
METHODS
This study was approved by the Institutional Review Board of Cooper Hospital/University Medical Center. Premature infants who weighed⬍1800 g at birth and were receiving constant-flow NCPAP for apnea or mild respiratory distress were eligible for enrollment, provided that they were otherwise medically stable. Informed parental consent was obtained before testing.
From the *University of Medicine and Dentistry of New Jersey/Robert Wood Johnson Medical School, Camden, New Jersey; ‡Virtua-West Jersey Hospital, Voorhees, New Jersey; §Department of Pediatrics, Division of Neonatology, The Children’s Regional Hospital at Cooper Hospital/UMC, Camden, New Jersey; and储Mercy Children’s Hospital at St. Vincent Mercy Medical Center and Department of Pediatrics, Medical College of Ohio, Toledo, Ohio.
This work was presented in part at the Pediatric Academic Societies’ An-nual Meeting; May 1– 4, 1999; San Francisco, CA.
Received for publication Dec 7, 2000; accepted Feb 8, 2001.
Reprint requests to (R.H.H.) Mercy Children’s Hospital, 2213 Cherry St, ACC 309, Toledo, OH 43608. E-mail: robert㛭[email protected]
Data Acquisition and Analysis
The study design and data acquisition have been described in detail elsewhere.3Briefly, NCPAP was provided to each infant
with each of 3 devices applied in random order: 1) a modified nasal canula, 2) a standard nasal CPAP prongs (constant-flow), and 3) the new variable-flow NCPAP generator with prongs (vari-able-flow). Because a nasal canula is not used commonly to pro-vide NCPAP, our WOB analysis was restricted to the 2 NCPAP delivery systems using prongs:
1. Constant-flow NCPAP was delivered by connecting Inca nasal prongs (Ackrad Laboratories, Cranford, NJ) to an infant venti-lator set in CPAP mode. Adjusting the CPAP setting on the ventilator varied the amount of airway pressure applied. A continuous gas flow of 6 L/min was used. The largest prongs that fit the infant’s nares without blanching the surrounding tissue were used.
2. Variable-flow NCPAP was delivered by the Aladdin/Infant-Flow system (Hamilton Medical, Reno, NV; manufactured by EME, Ltd, Brighton, UK; and currently distributed as the In-fant-Flow Nasal CPAP system by SensorMedics Corp, Yorba Linda, CA). Changing the amount of gas flow varied the amount of CPAP. The largest prongs that fit easily into the nares were used for each infant.
Measurements were performed after a feeding to facilitate quiet sleep. Sedation was not used in any infant. Infants were instru-mented and placed in the supine position. Instrumentation con-sisted of the following: 1) respiratory inductance plethysmogra-phy (RIP) bands that were fitted around the chest and the abdomen (Respiband Plus, SensorMedics Corp, Yorba Linda, CA; and Nims Inc, Miami Beach, FL); 2) insertion of a neonatal esoph-ageal balloon catheter (Ackrad Laboratories, Cranford, NJ) at the level of the lower third of the trachea to estimate intrapleural pressure from the esophageal pressure (Pes); and 3) placement of a thermistor (BreathSensor, Nellcor Puritan Bennett, Eden Prairie, MN) to detect and continuously record (EdenTrace II Plus, Eden-Tec, Eden Prairie, MN) air leaks from the mouth.
RIP was used to measure lung volume changes (⌬VL) and tidal
ventilation (VT) from its direct current (DC) and alternating
cur-rent components, respectively (Somnostar, SensorMedics Corp., Yorba Linda, CA).4,5After the RIP bands were placed, RIP was
calibrated by direct comparison6,7to leak-free flow and volume
data measured by face mask pneumotachography (Neonatal Flow Sensor #7218 [dead space 0.8 mL], Novametrix, Wallingford, CT). Before measurements began, proper placement of the Pes balloon catheter was checked by continuous on-line monitoring of Pes and adjusted until a high correlation (r2⬎0.90) was obtained between
airway opening pressure and Pes during spontaneous breathing by the infant against an occluded airway.8When necessary, the
infant’s mouth was closed gently during data collection to stop any air leak, and data with air leak at the mouth were not used. Airway flow and Pes from a series of 10 to 15 leak-free breaths were integrated to calculate VT. All signals were sampled at 100
Hz, monitored on-line, and stored on a computer for later analysis. Patients initially were placed on NCPAP of 8 cm H2O to allow
similar lung recruitment. With each device,⌬VL, VT, and Pes were
measured at NCPAP of 8, 6, 4, and 0 cm H2O. Infants were kept for
3 to 5 minutes at each CPAP level. The leak-free breaths spanning the last 20 to 30 seconds at each setting were selected for subse-quent analysis.
Lung compliance (CL) was calculated from VTand Pes data
using standard methods.8Inspiratory WOB (WOB
I) was
calcu-lated from the area subtended by the inspiratory limb of the Pes–VTcurve, according to Campbell’s diagram.9Resistive WOB
(RWOB) was calculated as the area between the inspiratory and expiratory loops of the Pes–VTcurve. For standardizing the results
from different infants and for varying breathing amplitudes, WOB was divided by VT.
Sample Size Calculation/Statistical Analysis
Sample size was based on finding a clinically significant⌬VL
between any 2 NCPAP devices as previously reported by us.3A
sample size of 28 to 32 patients is required to attain a statistical power of 0.8 to 0.85 when one assumes a 20% difference to be significant with a 0.05 significance criterion.10 Dependent
vari-ables were analyzed as mixed linear models in a randomized block factorial design.11Devices and CPAP levels were considered
fixed effects, and patients were treated as random blocks. Differ-ences between devices, within NCPAP levels, and devices-within-NCPAP levels were tested using least square, pair-wise mean comparisons. The effects of missing cells were adjusted for by using Satterthwaite approximations.11P⬍.05 was considered to
be significant.
RESULTS
Thirty-five infants were recruited for study. Of these, Pes monitoring and RIP data that allowed accurate calculations of WOB were obtained in 24 infants. The patient characteristics of these 24 infants including baseline CLare shown in Table 1.
Changes (means, SD) in respiratory rate (RR; min⫺1) and V
T with NCPAP are shown in Table 2.
RR was similarly decreased as NCPAP increased for the 2 devices. VTwas not changed with NCPAP for
either device but was greater for the variable-flow device at all CPAP levels (P⬍ .001).
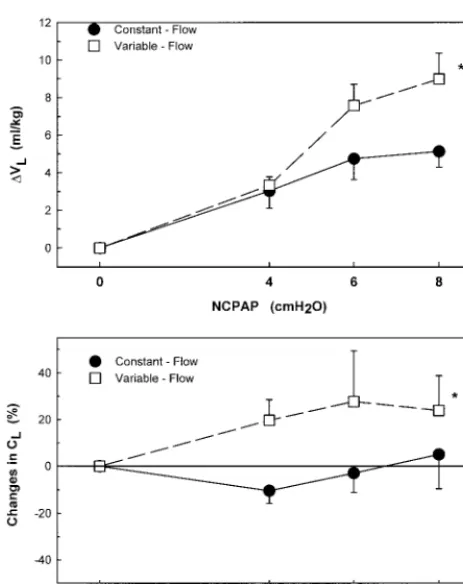
⌬VL as a function of NCPAP for each device are
shown in Fig 1, top. Although ⌬VL increased with
NCPAP with both systems, ⌬VL was significantly
greater overall with the variable-flow device (P ⬍
.001). The corresponding CLcomparison is shown in
Fig 1, bottom. CL essentially was unchanged with
constant-flow NCPAP but was slightly increased at CPAP of 4 and 6 cm H2O, relative to 0 cm H2O, for
the variable-flow device. At CPAP of 8 cm H2O, this
tendency was reversed and CLwas slightly (not
sig-nificantly) lower with variable flow.
Changes in WOBI and its component RWOB per
milliliter of delivered VTare shown in Fig 2. Overall,
both WOBIand RWOB were significantly lower with
the variable-flow device compared with the con-stant-flow system (P ⬍ .001). WOBI with
variable-flow NCPAP was lower by 28.8%, 29.0%, and 13.6% at CPAP of 4, 6, and 8 cm H2O, respectively. At
CPAP of 0 cm H2O, RWOB was significantly greater
with constant-flow NCPAP (P⬍.05), possibly indi-cating the effects of the larger mechanical impedance of the Inca nasal prongs. This difference, however, did not affect WOBIat 0 cm H2O.
DISCUSSION
NCPAP is increasingly being used as the primary method of ventilatory support in preterm infants with respiratory distress syndrome. This trend is based on the perceived advantages of this relatively noninvasive approach, including avoiding the risks and complications of intubation and mechanical ven-tilation. More important, compared with intubation and mechanical ventilation, NCPAP is believed to
TABLE 1. Patient Characteristics (n⫽24)
Characteristic Median (Range)
Birth weight (g) 945 (606–1488)
Weight at testing (g) 1151 (664–1461)
Male:female 16:8
Gestational age (wk) 29 (25–31)
Age (days) 8 (2–48)
Corrected gestational age (wk) 30.5 (26–33)
Days ventilated (n⫽18) 5 (1–42)
CPAP, cm H2O 5 (4–8)
CL(ml/cm H2O)* 2.30⫾0.48
Fraction of inspired oxygen 0.26 (0.21–0.55)
* CLis provided as mean⫾SE.
ARTICLES 683
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news
decrease the likelihood of pulmonary barotrauma and volutrauma in infants and consequently the de-velopment of chronic lung disease.12
The conventional method used to provide NCPAP uses constant-flow CPAP delivered via nasal prongs connected to a neonatal ventilator. In a newer system that provides variable-flow NCPAP, a flow driver delivers gas via specially designed nasal prongs.1
Studies comparing the efficacy of these 2 approaches remain scarce and are limited mostly to mechanical models.2Furthermore, no studies have compared the
possible effects of constant- versus variable-flow NC-PAP on WOB and lung mechanics in infants. This
perhaps is due to the difficulty of obtaining the rel-evant WOB measurements in neonates, particularly without altering the delivery of NCPAP.
In mechanical model studies, constant-flow NC-PAP has been associated with increased WOB com-pared with both mask CPAP13 and variable-flow
NCPAP.2 The design of the variable-flow NCPAP
system offers several advantages during both inspi-ration and expiinspi-ration. During inspiinspi-ration, the design of the variable-flow nasal prongs results in high-velocity jet flows, allowing gas entrainment. This assists inspiration on demand, which, in turn, keeps the CPAP level constant.1,2 A less variable CPAP
would be expected to improve and maintain VL
re-cruitment with CPAP.
We recently reported that variable-flow NCPAP led to superior ⌬VL compared with constant-flow NCPAP.3Such increased V
Lwill improve lung
me-chanics and, hence, may decrease WOB, provided that parenchymal overdistention is avoided. Note that, on exhalation, the variable-flow nasal prongs allows any excess gas flow from the CPAP driver to be shunted away from the patient to ambient air, through an expiratory outlet. This is in contrast to constant-flow NCPAP whereby gas flow continues toward the nares during exhalation.1,2,14 With
con-stant-flow NCPAP, the patient’s expiratory effort then must overcome this excess flow, leading to in-creased expiratory work.
Arguably, these advantages of variable-flow NC-PAP should translate into superior clinical perfor-mance, including an improved success rate of extu-bation. Data supporting this were presented recently for ventilated preterm infants who were extubated prophylactically to CPAP. Here, investigators found that the rate of successful extubation was greater with the Infant-Flow system compared with con-Fig 1. Changes in VL(top) and CL(bottom) with NCPAP. *The
overall⌬VL(mean⫾standard error [SE]) was significantly greater
with variable-flow compared with constant-flow NCPAP (P ⬍ .001) and was associated with increased CL (mean ⫾ SE). CL
essentially was unchanged with constant-flow NCPAP. *CL
gen-erally was greater with variable-flow NCPAP (P⬍.05). Note the relative decrease in CLat 8 cm H2O with the variable-flow device,
indicating the possibility of lung overdistension.
Fig 2. Changes in WOBI(mean⫾SE) and its component RWOB
(mean⫾SE). Overall, both WOBIand RWOB were significantly
lower with the variable-flow device compared with constant-flow NCPAP (P⬍.001). Note that RWOB was greater at 0 cm H2O with
constant-flow NCPAP (P⬍.05), possibly due to a larger mechan-ical impedance of the constant-flow nasal prongs.
TABLE 2. Breathing Pattern Changes With NCPAP
CPAP (cm H2O)
Variable-Flow NCPAP
Constant-Flow NCPAP
RR (min⫺1)
VT
(ml/kg)*
RR (min⫺1)
VT
(ml/kg)
0 73⫾16 5.9⫾2.9 73⫾23 4.8⫾2.5
4 67⫾17 5.4⫾2.8 63⫾19 4.6⫾2.4
6 64⫾18 6.0⫾2.9 65⫾24 4.8⫾2.4
8 61⫾18 6.0⫾3.0 63⫾16 4.7⫾2.2
Changes in respiratory rate (RR, min⫺1) and V
Twith variable- and
constant-flow NCPAP at various CPAP levels. Note the trend for decreasing RR with increasing CPAP with both devices. * VTwas greater with the variable-flow device at all CPAP levels
stant-flow nasal or nasopharyngeal CPAP.15,16
How-ever, studies investigating the long-term or prophy-lactic use of variable-flow NCPAP in the treatment of preterm infants have not been reported.
Critique of Experimental Methods
Measurement of lung mechanics and WOB during NCPAP is not possible with standard methods, whereby flow and volume are measured at the air-way opening, without affecting the results. This is because placement of an in-line flow-measuring de-vice such as a pneumotachograph will interfere with CPAP delivery, will cause additional imposed WOB, and is cumbersome and impractical to use in a clin-ical setting. RIP provides an attractive alternative whereby measurements of volume changes (and hence flow) are done distally at the chest wall and therefore does not interfere with or alter how CPAP is delivered to patients. Moreover, with the use of DC-coupled RIP, careful measurements allow a si-multaneous assessment of both⌬VL(DC component)
and VT(AC component). Measurement of changes in ⌬VL is not possible from pneumotachography. A
possible disadvantage of RIP is that it relies on an incomplete sampling of the thorax (1 abdominal and 1 rib-cage band; see Methods) to infer volume changes. This may limit its accuracy, particularly in the presence of significant chest wall distortion. Al-though we cannot discount completely the possible effects of this limitation of RIP, we believe that its importance is secondary as 1) we carefully marked the location of RIP bands to ensure identical place-ment, and 2) the devices were tested in random order with each patient serving as his or her own control. In this study, performed in preterm neonates with minimal lung disease, we showed that, compared with constant-flow NCPAP, a variable-flow device is able to recruit more VL(Fig 1, top) and increase the
effective CL(Fig 1, bottom) and that it is able to do
this with relatively decreased WOB (Fig 2). The latter is due partly to the larger RWOB with the constant-flow device when no CPAP constant-flow is provided (ie, CPAP of 0 cm H2O). This indicates the presence of
additional imposed WOB due to the Inca prongs (which were used exclusively in this study with the constant-flow device). Note that other commer-cially available nasal prongs used with conventional NCPAP may lead to less (or more) imposed WOB, depending on their specific design.
As mentioned above, lung recruitment was notice-ably increased for 6 and 8 cm H2O variable-flow
NCPAP (Fig 1). Although the associated WOB at these NCPAP settings remained lower than for NC-PAP⫽0, they did not continue to decrease relative to NCPAP ⫽ 4 (Fig 2). In fact, despite greater VL,
WOB was slightly—albeit not significantly— greater than for NCPAP⫽4. Given that 1) gas compression compliance is necessarily increased at higher VLand
2) RWOB was not increased as variable-flow NCPAP increased (Fig 2), our data might point to the possi-bility that lung overdistension at the higher NCPAP levels (or equivalent VL) may have occurred in some
patients with the variable-flow system. This is per-haps an indication of the increased efficacy of
main-taining a constant airway pressure (and hence VL
recruitment) with variable-flow NCPAP.1,2
There-fore, caution is advisable when titrating toward the higher NCPAP levels with this device.
CONCLUSION
Variable-flow nasal CPAP potentially can provide superior respiratory support in neonates that is char-acterized by 1) greater and more stable volume re-cruitment, 2) improved CL, and 3) decreased WOB.
Our findings, however, are limited to its short-term use in 24 neonates with mild lung disease or apnea. Similar investigation of the use of 1) variable-flow nasal CPAP in a larger number of neonates, 2) for longer periods of time, 3) in comparison with other nasal prong designs/constant-flow NCPAP, and 4) in infants with more significant lung disease are needed for confirmation of the reported findings.
ACKNOWLEDGMENTS
This work was supported in large part by a grant from the Cooper Faculty Practice Foundation. Hamilton Medical, Inc (Reno, Nevada) provided the variable-flow nasal CPAP device, manufac-tured by EME Ltd (Brighton, England).
We thank Gerald K. Arnold, PhD, for help in statistical analysis.
REFERENCES
1. Moa G, Nilsson K, Zetterstrom H, Jonsson LO. A new device for the administration of nasal constant positive airway pressure in the newborn: an experimental study.Crit Care Med. 1988;16:1238 –1242 2. Klausner JF, Lee AY, Hutchison AA. Decreased imposed work with a
new nasal continuous positive airway device.Pediatr Pulmonol. 1996;22: 188 –194
3. Courtney SE, Pyon KH, Saslow JG, Arnold GK, Pandit PB, Habib RH. Lung recruitment and breathing pattern during variable versus contin-uous flow nasal contincontin-uous positive airway pressure in premature infants: an evaluation of three devices.Pediatrics. 2001;107:304 –308 4. Locke R, Greenspan JS, Shaffer TH, Rubenstein SD, Wolfson MR. Effect
of nasal CPAP on thoracoabdominal motion in neonates with respira-tory insufficiency.Pediatr Pulmonol. 1991;11:259 –264
5. Sandberg KL, Lindstrom DP, Krueger ED, Sundell H, Cotton RB. Mea-surement of tidal volume during high frequency ventilation by imped-ance plethysmography.Pediatr Res. 1988;23:253–256
6. Warren RH, Alderson SH. Face mask application for calibration of respiratory inductive plethysmography in lambs.J Dev Physiol. 1988;10: 175–178
7. Brooks LJ, DiFiore JM, Martin RJ, CHIME Study Group. Assessment of tidal volume over time in preterm infants using respiratory inductance plethysmography.Pediatr Pulmonol. 1997;23:429 – 433
8. Pandit PB, Pyon KH, Courtney SE, England SJ, Habib RH. Lung resis-tance and elasresis-tance in spontaneously breathing pre-term infants: effects of breathing pattern and demographics.J Appl Physiol. 2000;88:997–1005 9. Harris TR, Wood BR. Physiologic principles. In: Goldsmith JP, Karotkin EH, eds.Assisted Ventilation of the Neonate.3rd ed. Philadelphia, PA: WB Saunders; 1996:21– 68
10. Cohen J.Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum; 1988:48 –52, 274 –280
11. Kirk R.Experimental Design: Procedures for the Behavioral Sciences. Pacific Grove, CA: Brooks/Cole; 1995:454 – 473
12. Van Marter LJ, Allred EN, Pagano M, et al. Do clinical markers of barotrauma and oxygen toxicity explain interhospital variation in rates of chronic lung disease? The Neonatology Committee for the Develop-mental Epidemiology Network.Pediatrics. 2000;105:1194 –1201 13. Goldman SL, Brady BP, Dumpit FE. Increased work of breathing
asso-ciated with nasal prongs.Pediatrics. 1979;64:160 –164
14. Moa G, Nilsson K. Nasal continuous positive airway pressure: experi-ences with a new technical approach.Acta Pediatr. 1993;82:210 –211 15. Sun SC, Tein HC. Randomized controlled trial of two methods of nasal
CPAP (NCPAP): flow driver vs conventional NCPAP [abstract].Pediatr Res. 1999;45:322A
16. Roukema H, O’Brien K, Nesbitt K, Zaw W. A crossover trial of infant flow (IF) continuous positive airway pressure (CPAP) versus nasopha-ryngeal (NP) CPAP in the extubation of babiesⱕ1250 grams birth-weight [abstract].Pediatr Res. 1999;45:317A
ARTICLES 685
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news
DOI: 10.1542/peds.108.3.682
2001;108;682
Pediatrics
Habib
Paresh B. Pandit, Sherry E. Courtney, Kee H. Pyon, Judy G. Saslow and Robert H.
Positive Airway Pressure in Preterm Neonates
Work of Breathing During Constant- and Variable-Flow Nasal Continuous
Services
Updated Information &
http://pediatrics.aappublications.org/content/108/3/682
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/108/3/682#BIBL
This article cites 13 articles, 3 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
http://www.aappublications.org/cgi/collection/agency_abcs
Agency ABC's
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.108.3.682
2001;108;682
Pediatrics
Habib
Paresh B. Pandit, Sherry E. Courtney, Kee H. Pyon, Judy G. Saslow and Robert H.
Positive Airway Pressure in Preterm Neonates
Work of Breathing During Constant- and Variable-Flow Nasal Continuous
http://pediatrics.aappublications.org/content/108/3/682
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2001 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news