Risk Factors for the Development of
Bladder and Bowel Dysfunction
Thomas W. Gaither, BS, a Christopher S. Cooper, MD, FAAP, FACS, b Zachary Kornberg, BS, a
Laurence S. Baskin, MD, a Hillary L. Copp, MD, MSa
BACKGROUND: Patients with vesicoureteral reflux and concomitant bladder and bowel
dysfunction (BBD) are at high risk for febrile urinary tract infections. Risk factors for BBD have been identified in retrospective studies without validated measures.
METHODS: We conducted a secondary analysis of the Randomized Intervention for Children
with Vesicoureteral Reflux and Careful Urinary Tract Infection Evaluation trials. The outcome of interest in the analysis of these children was the development of BBD, defined by using the dysfunctional voiding questionnaire, during any time point in the studies. We used multivariable logistic regression to determine the independent effects of sex, baseline percentile BMI, cohort status (Randomized Intervention for Children with Vesicoureteral Reflux versus Careful Urinary Tract Infection Evaluation), continuous antibiotic prophylaxis (yes or no), and reflux status (dilating versus nondilating) on the development of BBD.
RESULTS: Three hundred and eighteen patients met inclusion criteria. The majority of
patients (244 patients, 77%) were not toilet trained at baseline visit. The median baseline age (interquartile range) was 21 months (11–35 months), and 299 (94%) patients were girls. During the study period, 111 (35%) developed BBD. Baseline BMI percentile was not associated with BBD development (adjusted odds ratio [aOR] = 1.0; 95% confidence interval [CI]: 0.9–1.1), whereas female sex was highly associated with BBD development (aOR = 12.7; 95% CI: 1.6–98). Patients with dilating reflux at baseline were 2.1 times more likely to develop BBD (95% CI: 1.2–3.7). Antibiotic prophylaxis was not associated with BBD development (aOR = 0.8; 95% CI: 0.4–1.4).
CONCLUSIONS: Dilating reflux and female sex were identified as risk factors for development of
BBD, but neither BMI nor prophylactic antibiotics was associated with the development of BBD.
abstract
aDepartment of Urology, University of California, San Francisco, San Francisco, California; and bDepartment of Urology, University of Iowa, Iowa City, Iowa
Mr Gaither performed the statistical analysis and drafted initial manuscript; Mr Kornberg performed some statistical analysis and critically reviewed the manuscript; Drs Cooper and Baskin critically reviewed and revised the manuscript and interpreted statistical analysis; Dr Copp initiated the study idea, obtained the study data, critically reviewed statistical analysis, and revised the manuscript; and all authors approved the final manuscript as submitted.
DOI: https:// doi. org/ 10. 1542/ peds. 2017- 2797 Accepted for publication Oct 20, 2017
Address correspondence to Hillary L. Copp, Department of Urology, University of California, San Francisco, 1825 4th St, 5th Floor, Mission Hall Pediatric Urology, San Francisco, CA 94143. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2018 by the American Academy of Pediatrics
What’s KnOWn On thIs subject: Bladder and bowel dysfunction (BBD) is common in patients with and without vesicoureteral reflux. The combination of BBD and vesicoureteral reflux places patients at significant risk for urinary tract infections. BBD risk factors have been identified in retrospective studies without validated measurements.
What thIs stuDy aDDs: We identify female sex and dilating reflux as independent risk factors for the development of BBD. Although obesity has been linked to voiding dysfunction in children, we did not find a relationship between BMI and BBD.
Bladder and bowel dysfunction (BBD) is defined as the combination of functional constipation and lower urinary tract symptoms.1 BBD has
become more widely recognized as an entity that negatively impacts urinary tract health.2 Not only
does BBD decrease the likelihood for spontaneous vesicoureteral reflux (VUR) resolution but also is a known risk factor for urinary tract infections (UTIs) and potential renal scarring.3–5 In fact, children with
BBD and any grade of VUR have the highest risk of recurrent febrile or symptomatic UTIs, even when compared with children with high-grade VUR (56% vs 30%).4
Risk factors for the development of BBD are not well defined. A large multivariable analysis of >2500 patients at risk for UTI revealed that female sex was highly associated with BBD and found no association between BBD and reflux.6
However, this study was limited by its retrospective nature and the use of nonvalidated measures of BBD. Additionally, the authors of previous studies have demonstrated that overweight children are less responsive to treatment of BBD, but it is unclear if overweight children are at risk for developing BBD.7
To overcome these limitations, we sought to identify risk factors for the development of BBD by performing a secondary data analysis of 2 studies that prospectively measured BBD status by using validated questionnaires.
MethODs study Population
We used data available from the National Institute of Diabetes and Digestive and Kidney Disease from 2 prospective trials: the Careful Urinary Tract Infection Evaluation (CUTIE) trial and the Randomized Intervention for Children with Vesicoureteral Reflux (RIVUR) trial.4, 8 The RIVUR trial is a double-blinded,
randomized, placebo-controlled trial in which antibiotic prophylaxis to prevent recurrent UTI in patients with grade 1 to 4 VUR is studied. The CUTIE trial is a prospective study of patients who were screened for inclusion in the RIVUR trial but found to not have VUR. Both studies included children after an index febrile or symptomatic UTI between the ages of 2 to 72 months and were managed for 2 years. In the current study, patients with baseline BBD (n = 97) or unknown BBD status (n = 11) were removed. Patients whose BBD status was unavailable during follow-up, either because of not being toilet trained (n = 298) or missing BBD status (n = 78), were removed. Thus, 318 patients were included in the study and were at risk for BBD development during the 2-year period.
Possible Risk Factors
We examined the independent effects of sex, percentile BMI at baseline, VUR at baseline (dilating versus nondilating or no reflux), and treatment and/or study arm on BBD development. BMI percentiles were based on the World Health Organization’s nomograms for children ≥12 months and the Centers for Disease Control and Prevention’s nomograms for children <12 months. In cases in which percentile BMI was missing from the initial visit (n = 28), we used the earliest next visit to estimate baseline percentile BMI. Dilating reflux was defined as grades III to V on the International Classification of Vesicoureteral Reflux. In addition, we also tested whether being assigned to prophylactic antibiotics was associated with BBD development.
Main Outcome
BBD was assessed by using the dysfunctional voiding questionnaire score.9 The exact form used in
the study can be found in the supplemental material in the original
RIVUR publication.8 BBD was defined
as a score ≥6 in female subjects and defined as a score ≥9 for male subjects, as per the developers of the study.10 Patients were considered
to develop BBD if these scores met criteria at either the 12-month or the 24-month visits, which were the follow-up visits with BBD data available.
statistical analysis
All analyses were performed in Stata version 13 (StataCorp, College Station, TX). We used descriptive statistics to describe the population. We compared risk factors in a univariable and multivariable analysis. In the univariable analysis, we used Student’s t tests for continuous variables and the Pearson χ2 test for categorical
variables. All continuous data were assessed for normality. We then used multivariable logistic regression to determine independent effects of our risk factors on the development of BBD during the study period. Because BBD status was missing in a proportion of patients, we performed a sensitivity analysis with imputed outcomes. We developed 2 multivariate models in which we imputed all missing patients to have BBD versus all missing to not have BBD. Because we expected the true proportion of missing patients to be somewhere in the middle, this gave a range of possible estimates. All tests were 2-sided, and P values <.05 were considered statistically significant. The institutional review board provided exempt status for the secondary data analysis.
Post hoc analyses
entry if their child had a history of constipation that was assessed regardless of toilet training status. We then added constipation history to our multivariate model to assess the possibility of confounding. Because the number of boys who developed BBD was small (n = 1), we also lowered the cutoff for the BBD definition to the same cutoff as girls (≥6). We then repeated our models with this less stringent definition.
Results
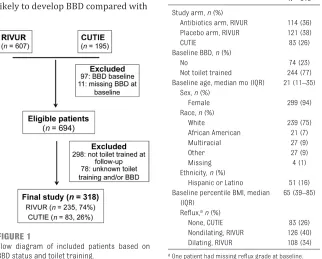
Figure 1 shows the patients who met inclusion criteria. In total, 318 patients were included in the study; 74% of patients were from the RIVUR trial, and 26% of patients were from the CUTIE trial. Table 1 shows baseline characteristics of patients in our study. The majority of patients (244 patients, 77%) were not toilet trained at baseline visit. The median baseline age (interquartile range [IQR]) was 21 months (11–35 months), and 299 (94%) of patients were girls. The median (IQR) baseline percentile BMI was 64 (39–85), and 108 out of 234 (48%) had dilating reflux at baseline.
univariable analysis
One hundred and eleven patients (35%) developed BBD throughout the study period, which occurred in 5% of boys (1 out of 19) and 37% of girls (110 out of 299). A small minority of patients (21, 7%) had BBD at the 1-year visit that was resolved by the 2-year visit. Table 2 shows the results of the univariable analysis. There were no statistical differences in the proportion of patients who developed BBD by study cohort or by study arm. Ninety-nine percent of patients who developed BBD were girls compared with only 91% of girls in the group who did not develop BBD, P < .01. Patients who developed BBD were
also significantly more likely to have dilating reflux at baseline compared with those who did not develop BBD (42% vs 29%, P = .04). Baseline and follow-up median BMI did not differ between these 2 groups (61 vs 66, P = .76 and 63 vs 66, P = .68, respectively).
Multivariable analysis
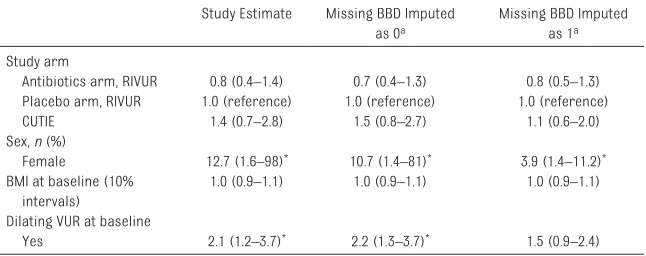
Table 3 shows the multivariable analyses of patients included in the study and the imputed analysis. Seventy-eight patients with unknown toilet training and BBD status had their BBD status imputed for the sensitivity analysis. Girls were more likely to develop BBD compared with
boys (adjusted odds ratio [aOR] = 12.7; 95% confidence interval [CI]: 1.6–98). Patients with dilating reflux at baseline were 2 times as likely to develop BBD during the study period (aOR = 2.1; 95% CI: 1.2–3.7). Baseline BMI did not affect the risk of developing BBD (aOR = 1.0; 95% CI: 0.9–1.1). The results remained robust in the sensitivity analysis. If
FIGuRe 1
Flow diagram of included patients based on BBD status and toilet training.
table 1 Clinical Characteristics of Patients With Baseline and Follow-up BBD Status in the CUTIE and RIVUR Studies (N = 318)
N = 318 Study arm, n (%)
Antibiotics arm, RIVUR 114 (36)
Placebo arm, RIVUR 121 (38)
CUTIE 83 (26)
Baseline BBD, n (%)
No 74 (23)
Not toilet trained 244 (77)
Baseline age, median mo (IQR) 21 (11–35) Sex, n (%)
Female 299 (94)
Race, n (%)
White 239 (75)
African American 21 (7)
Multiracial 27 (9)
Other 27 (9)
Missing 4 (1)
Ethnicity, n (%)
Hispanic or Latino 51 (16) Baseline percentile BMI, median
(IQR)
65 (39–85) Reflux, an (%)
None, CUTIE 83 (26)
Nondilating, RIVUR 126 (40)
Dilating, RIVUR 108 (34)
a One patient had missing reflux grade at baseline.
table 2 Univariable Associations of Clinical Characteristics and Developing BBD
Developed BBD (n = 111) No BBD (n = 207) P
Study, n (%)
Antibiotics arm, RIVUR 36 (32) 78 (38) .59
Placebo arm, RIVUR 46 (41) 75 (38) —
CUTIE 29 (26) 54 (26) —
Median age in mo (IQR) at baseline 19 (11–32) 22 (11–37) .57 Sex, n (%)
Female 110 (99) 189 (91) <.01
Median baseline BMI percentile (IQR) 61 (39–85) 66 (36–85) .76 Median follow-up BMI percentile (IQR) 63 (37–87) 66 (28–85) .68 VUR at baseline
No 29 (26) 54 (26) .04
Nondilating 35 (32) 91 (44) —
Dilating 47 (42) 61 (29) —
all missing patients had developed BBD, patients with dilating reflux at baseline had similar odds of developing BBD, although the results did not reach formal statistical significance (aOR = 1.5; 95% CI: 0.9–2.4).
Post hoc analysis
Patients who developed BBD were more likely to report a history of constipation at baseline compared with those who did not develop BBD (37, 33% vs 46, 22%; P = .03). No differences in constipation history were observed between patients with dilating reflux (29, 27%) compared with patients without dilating reflux (54, 26%), P = .85, nor were there differences in constipation treatment history between patients with dilating reflux (16, 15%) compared with patients without dilating reflux (29, 14%), P = .82. After adding constipation to the model, the aOR for dilating reflux is unchanged (aOR = 2.2; 95% CI: 1.2–3.8). The aOR for constipation was 1.8 (95% CI: 1.1–3.2).
An additional 3 boys would have developed BBD if we had lowered the dysfunctional voiding questionnaire score definition. The overall
interpretation of the model estimates did not change. The aOR for girls and dilating reflux were 3.7 (95% CI: 1.0–13.2) and 2.1 (95% CI: 1.2–3.6), respectively. The other possible risk factors remained nonsignificant.
DIscussIOn
BBD recognition and treatment is an important aspect of overall UTI prevention and VUR management. In fact, the American Urological Association VUR guidelines recommend treatment of BBD before any surgical intervention of VUR is undertaken.5 BBD is an
underdiagnosed entity that merits further awareness.11 Patients with
BBD and any grade of VUR are at highest risk for recurrent UTI, which was demonstrated via a secondary analysis of the RIVUR and/or CUTIE data sets.4 To improve the
management of this population, we need to have a better understanding of which children with a history of UTI are at risk for developing BBD to better target screening and intervention. Our objective in the current study was to define risk factors for BBD development in children with a history of UTI. This is a secondary, combined analysis of 2 robust studies of patients at risk for recurrent UTIs. The strengths of these studies include prospective data collection using validated questionnaires, similar inclusion criteria, and a large number of patients. To our knowledge, this is the first study to perform a secondary analysis with the RIVUR and/or CUTIE data sets to determine risk factors for BBD development. Several findings were noteworthy. First, we confirm previous findings
that girls are more likely to develop BBD than boys.6 Second, our results
revealed that patients with dilating reflux were twice as likely to develop BBD within a 2-year time frame. These findings were consistent in all sensitivity analyses. Although not statistically significant in the second imputation model, the chance that all missing patients developed BBD is unlikely. Third, baseline BMI and antibiotic prophylaxis were not associated with BBD development. The incidence of UTI is sixfold greater in young girls compared with boys in the first 6 years of life.12 For this
reason, the majority of those eligible for the RIVUR and/or CUTIE trials were girls (729 out of 802, or 91%). Although the vast majority of study participants were girls, among the enrolled and eligible boys (n = 19), only 1 boy (5%) developed BBD compared with 110 out of 299 (37%) girls. The reasons as to why girls develop BBD overwhelmingly more than boys are not well understood. Others have observed increased dysfunctional voiding in girls versus boys in this age group.6, 9 In
addition, girls with dysfunctional voiding are more likely to develop UTIs compared with boys, and thus girls with dysfunctional voiding were more likely to be enrolled in the RIVUR and/or CUTIE trials.13
However, we purposefully excluded girls who had documented BBD at the time of study enrollment to investigate factors associated with the subsequent development of BBD. Patients with dilating reflux at baseline were twice as likely to develop BBD throughout the study period, which was a consistent finding in all models. It is possible that reflux and BBD share a common etiology. Such a common etiology could stem from a shared nerve supply between the bladder and bowel, which could be affected by a common defect.14 Another
possible explanation is inherent abnormal urine volume and cycling
table 3 Multivariable Analysis of the Development of BBD by Baseline Clinical Factors Study Estimate Missing BBD Imputed
as 0a
Missing BBD Imputed as 1a
Study arm
Antibiotics arm, RIVUR 0.8 (0.4–1.4) 0.7 (0.4–1.3) 0.8 (0.5–1.3) Placebo arm, RIVUR 1.0 (reference) 1.0 (reference) 1.0 (reference)
CUTIE 1.4 (0.7–2.8) 1.5 (0.8–2.7) 1.1 (0.6–2.0)
Sex, n (%)
Female 12.7 (1.6–98)* 10.7 (1.4–81)* 3.9 (1.4–11.2)*
BMI at baseline (10% intervals)
1.0 (0.9–1.1) 1.0 (0.9–1.1) 1.0 (0.9–1.1) Dilating VUR at baseline
Yes 2.1 (1.2–3.7)* 2.2 (1.3–3.7)* 1.5 (0.9–2.4)
of urine associated with dilating VUR that may impact bladder and bowel function. Although surgical treatment of reflux does not always resolve BBD symptoms, 15 the
refluxing ureter could impact the normal development of the bladder and bowel function. Tanagho and Nguyen16 postulate an alternative
mechanism in which they describe reflux as a result of trigonal abnormalities that not only lead to reflux but also to dysfunctional voiding after toilet training. Because of the prospective nature of these studies, we document that the reflux is present before BBD development, although many included children were not toilet trained at enrollment and could have had BBD that was not detectable by the questionnaire before toilet training. However, we found no differences in constipation history and treatment between those with and without dilating reflux. It also appears that constipation is not confounding the relationship between dilating reflux and BBD development. Prospective data collection in children with BBD and reflux is essential to further investigate a common etiology to develop the best management strategies.
It is likely that not all BBD diagnosed by the questionnaire, which covers both bladder and bowel symptoms, share a common etiology. In fact, Shaikh et al10
report that BBD is often present in patients without VUR, and they suggest BBD and VUR are not causally related. Patients with BBD without VUR may have a different subtype or etiology of BBD than patients with VUR. Certainly, the range of symptoms experienced by children with BBD is varied.17
The subtypes of symptoms, such as bladder overactivity versus dysfunctional voiding, affect VUR resolution rates15 and provide
evidence of differing subtypes of
BBD. Continued efforts are needed to better define types of BBD that go beyond parental subjection and may include objective measures such as urodynamics.18
Obesity in children correlates with nocturnal enuresis and dysfunctional voiding.19, 20 Children
with higher BMIs also have
increased constipation and soiling.21
We did not find a relationship between BMI and the development of BBD. This is consistent with findings by Borch et al.22 In this
study of 73 patients with BBD, the authors found no relationship between BMI and urinary versus bowel symptoms. Although obese patients with BBD are less responsive to treatment, 7, 19 the
etiology of the BBD in patients with reflux does not seem to be related to baseline BMI.
The results of this study should be interpreted within a clinical context. We believe that inquiring about a child’s bladder and bowel symptoms should take place for all patients with a previous UTI. Prompt medical management should be considered before any surgical treatment in patients with BBD. In female patients and/or patients with dilating reflux in particular, we recommend using a formal BBD questionnaire to monitor symptoms. General practitioners should have a low threshold for initiation of BBD treatment (including timed voiding and a bowel regimen) and for referral to subspecialists who commonly manage BBD if additional assistance with treatment is
necessary.
A limitation of this study is that it is a secondary data analysis of studies not designed specifically for this purpose. As such, outcome ascertainment was not collected as rigorously as the studies’
primary outcomes. Nevertheless, the prospective collection of these data via validated questionnaires at designated study time points were
decided a priori. We also addressed this issue with our sensitivity analyses, but missing data are challenging to predict. These results may not generalize to populations outside of the inclusion criteria, including patients without a previous symptomatic UTI or patients with grade 5 reflux. Because the study only contained 19 boys (6%) that met inclusion criteria, the risk factors identified may only apply to girls. As noted, we cannot completely rule out the possibility that BBD was present in patients who were not toilet trained. Unmeasured confounding factors, such as increased parental awareness, could also drive the relationship between VUR and BBD. Although identified as a risk factor, we cannot conclude dilating VUR causes BBD, and the pathophysiology behind this relationship merits future investigation.
cOnclusIOns
BBD is common in patients at risk for UTIs. Dilating reflux and female sex were identified as risk factors for the development of BBD, but neither being overweight or the use of prophylactic antibiotics was associated with the development of BBD. The risk of developing BBD should be considered when tailoring a comprehensive management plan for children with VUR.
abbRevIatIOns
aOR: adjusted odds ratio BBD: bladder and bowel
dysfunction CI: confidence interval CUTIE: Careful Urinary Tract
Infection Evaluation IQR: interquartile range
ReFeRences
1. Burgers RE, Mugie SM, Chase J, et al. Management of functional constipation in children with lower urinary tract symptoms: report from the Standardization Committee of the International Children’s Continence Society. J Urol. 2013;190(1):29–36 2. Elder JS, Diaz M. Vesicoureteral
reflux–the role of bladder and bowel dysfunction. Nat Rev Urol. 2013;10(11):640–648
3. Naseer SR, Steinhardt GF. New renal scars in children with urinary tract infections, vesicoureteral reflux and voiding dysfunction: a prospective evaluation. J Urol. 1997;158(2):566–568 4. Keren R, Shaikh N, Pohl H, et al.
Risk factors for recurrent urinary tract infection and renal scarring. Pediatrics. 2015;136(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 136/ 1/ e13
5. Skoog SJ, Peters CA, Arant BS Jr, et al. Pediatric Vesicoureteral Reflux Guidelines Panel summary report: clinical practice guidelines for screening siblings of children with vesicoureteral reflux and neonates/ infants with prenatal hydronephrosis. J Urol. 2010;184(3):1145–1151 6. Chen JJ, Mao W, Homayoon K, Steinhardt GF. A multivariate analysis of dysfunctional elimination syndrome, and its relationships with gender, urinary tract infection and vesicoureteral reflux in children. J Urol. 2004;171(5):1907–1910 7. Arlen AM, Cooper CS, Leong T. Role
of body mass index in school-aged children with lower urinary tract
dysfunction: does weight classification predict treatment outcome? J Pediatr Urol. 2017;13(5):454.e1–454.e5 8. Hoberman A, Greenfield SP, Mattoo
TK, et al; RIVUR Trial Investigators. Antimicrobial prophylaxis for children with vesicoureteral reflux. N Engl J Med. 2014;370(25):2367–2376
9. Farhat W, Bägli DJ, Capolicchio G, et al. The dysfunctional voiding scoring system: quantitative standardization of dysfunctional voiding symptoms in children. J Urol. 2000;164(3 pt 2): 1011–1015
10. Shaikh N, Hoberman A, Keren R, et al. Recurrent urinary tract infections in children with bladder and bowel dysfunction. Pediatrics. 2016;137(1):e20152982
11. Santos JD, Lopes RI, Koyle MA. Bladder and bowel dysfunction in children: an update on the diagnosis and treatment of a common, but underdiagnosed pediatric problem. Can Urol Assoc J. 2017;11(1–2 suppl 1):S64–S72 12. Mårild S, Jodal U. Incidence rate of
first-time symptomatic urinary tract infection in children under 6 years of age. Acta Paediatr. 1998;87(5):549–552 13. Van Batavia JP, Ahn JJ, Fast AM,
Combs AJ, Glassberg KI. Prevalence of urinary tract infection and vesicoureteral reflux in children with lower urinary tract dysfunction. J Urol. 2013;190(suppl 4):1495–1499
14. Bauer SB. Special considerations of the overactive bladder in children. Urology. 2002;60(5 suppl 1):43–48; discussion 49
15. Sillén U. Bladder dysfunction and vesicoureteral reflux. Adv Urol. 2008;2008:815472
16. Tanagho EA, Nguyen HT. Vesicoureteral reflux. In: Tanagho EA, McAninch JW, eds. Smith’s General Urology. 17th ed. New York, NY: McGraw-Hill; 2008:179–192
17. Koff SA, Wagner TT, Jayanthi VR. The relationship among dysfunctional elimination syndromes, primary vesicoureteral reflux and urinary tract infections in children. J Urol. 1998;160(3 pt 2):1019–1022
18. Greenfield SP, Wan J. The relationship between dysfunctional voiding and congenital vesicoureteral reflux. Curr Opin Urol. 2000;10(6):607–610 19. Guven A, Giramonti K, Kogan BA. The
effect of obesity on treatment efficacy in children with nocturnal enuresis and voiding dysfunction. J Urol. 2007;178(4, pt 1):1458–1462 20. Erdem E, Lin A, Kogan BA, Feustel PJ.
Association of elimination dysfunction and body mass index. J Pediatr Urol. 2006;2(4):364–367
21. Fishman L, Lenders C, Fortunato C, Noonan C, Nurko S. Increased prevalence of constipation and fecal soiling in a population of obese children. J Pediatr. 2004;145(2):253–254
22. Borch L, Hagstroem S, Bower WF, Siggaard Rittig C, Rittig S. Bladder and bowel dysfunction and the resolution of urinary incontinence with successful management of bowel symptoms in children. Acta Paediatr. 2013;102(5):e215–e220
FInancIal DIsclOsuRe: The authors have indicated they have no financial relationships relevant to this article to disclose.
FunDInG: No external funding.
DOI: 10.1542/peds.2017-2797 originally published online December 27, 2017;
2018;141;
Pediatrics
and Hillary L. Copp
Thomas W. Gaither, Christopher S. Cooper, Zachary Kornberg, Laurence S. Baskin
Risk Factors for the Development of Bladder and Bowel Dysfunction
Services
Updated Information &
http://pediatrics.aappublications.org/content/141/1/e20172797
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/141/1/e20172797#BIBL
This article cites 21 articles, 2 of which you can access for free at:
Subspecialty Collections
s_sub
http://www.aappublications.org/cgi/collection/genitourinary_disorder
Genitourinary Disorders
http://www.aappublications.org/cgi/collection/urology_sub
Urology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2017-2797 originally published online December 27, 2017;
2018;141;
Pediatrics
and Hillary L. Copp
Thomas W. Gaither, Christopher S. Cooper, Zachary Kornberg, Laurence S. Baskin
Risk Factors for the Development of Bladder and Bowel Dysfunction
http://pediatrics.aappublications.org/content/141/1/e20172797
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.