Association Between Clinically Meaningful Behavior Problems and
Overweight in Children
Julie C. Lumeng, MD*; Kate Gannon, MPH‡; Howard J. Cabral, PhD‡; Deborah A. Frank, MD*; and Barry Zuckerman, MD*
ABSTRACT. Objective. To determine whether there is a relationship between clinically meaningful behavior problems and concurrent and future overweight in 8- to 11-year-old children.
Methods. 1998 National Longitudinal Survey of Youth
interview data for 8- to 11-year-old children and their moth-ers were analyzed. A Behavior Problems Index score>90th percentile was considered clinically meaningful. Child overweight was defined as a body mass index (BMI)>95th percentile for age and sex. Multiple logistic regression was used to control for potential confounders (selected a priori): child’s sex, race, use of behavior-modifying medication, history of academic retention, and hours of television per day; maternal obesity, smoking status, marital status, edu-cation, and depressive symptoms; family poverty status; and Home Observation for Measurement of the Environ-ment-Short Form (HOME-SF) cognitive stimulation score. In an attempt to elucidate temporal sequence, a second analysis was conducted with a subsample of normal-weight children who became overnormal-weight between 1996 and 1998 while controlling for BMIzscore in 1996.
Results. The sample included 755 mother-child pairs.
Of the potential confounding variables, race, maternal obesity, academic grade retention, maternal education, poverty status, and HOME-SF cognitive stimulation score acted as joint confounders, altering the relationship between behavior problems and overweight in the mul-tiple logistic regression model. With these covariates in the final model, behavior problems were independently associated with concurrent child overweight (adjusted odds ratio: 2.95; 95% confidence interval: 1.34 – 6.49). The relationship was strengthened in the subsample of pre-viously normal-weight children, with race, maternal obe-sity, HOME-SF cognitive stimulation score, and 1996 BMIzscore acting as confounders (adjusted odds ratio: 5.23; 95% confidence interval: 1.37–19.9).
Conclusions. Clinically meaningful behavior
prob-lems in 8- to 11-year-old children were independently associated with an increased risk of concurrent over-weight and becoming overover-weight in previously normal-weight children. Pediatrics 2003;112:1138 –1145;obesity, overweight, child behavior, child behavior disorders, Na-tional Longitudinal Survey of Youth.
ABBREVIATIONS. BMI, body mass index; NLSY, National Lon-gitudinal Survey of Youth; HOME-SF, Home Observation for Measurement of the Environment-Short Form; BPI, Behavior Problems Index; OR, odds ratio; CI, confidence interval.
C
hildhood overweight is a growing public health problem. More than 20% of children between the ages of 6 and 11 years are over-weight,1 and the severity of overweight hasin-creased in the past 10 years.2 Well-described risk
factors for childhood overweight include race,2
ele-vated maternal body mass index (BMI),3,4 and
amount of television viewing.5 The literature
di-verges on whether low socioeconomic status is a risk factor.4,6,7
Several risk factors for childhood overweight, in-cluding television viewing8 and low socioeconomic
status,9 –12are also associated with increased rates of
behavior problems. However, the relationship of be-havior problems and childhood overweight has not been explored thoroughly. Previous studies have shown an association between behavior problems and childhood overweight.13–20 Interpretation of
these data has been limited, however, by method-ologic constraints, including small and homoge-neous samples, limited use of standardized behavior rating scales, and bias as a result of samples’ being drawn only from weight-loss clinics. Individuals who attend weight-loss clinics have higher rates of psychological problems than overweight individuals who do not attend such a clinic.21,22Furthermore, the
previous studies have focused on statistical differ-ences in behavior rating scales, as opposed to clini-cally meaningful behavioral differences. No study has controlled adequately for potentially confound-ing variables such as television viewconfound-ing, socioeco-nomic status, or quality of the home environment. Finally, recent data are lacking; the most pertinent studies were conducted at least 10 years ago.13–16
To address issues raised by previous research, the current analysis investigates the relationship be-tween clinically meaningful behavior problems in 8-to 11-year-old children and childhood overweight in a nationally representative, nonreferred population. In addition, in an attempt to explore the temporal sequence of this association, we conducted a second analysis investigating the relationship between clin-ically meaningful behavior problems in normal-weight children and becoming overnormal-weight 2 years later.
From the *Division of Behavioral and Developmental Pediatrics, Depart-ment of Pediatrics, Boston University School of Medicine and Boston Med-ical Center, Boston, Massachusetts; and ‡Boston University School of Public Health, Boston, Massachusetts.
Received for publication Apr 1, 2002; accepted Jul 7, 2003.
Reprint requests to (J.C.L.) Center for Human Growth and Development, 300 Ingalls Bldg, 10th Floor, Ann Arbor, MI 48109-0406. E-mail: [email protected]
METHODS
The National Longitudinal Survey of Youth (NLSY) is a multi-purpose survey sponsored by the US Department of Labor. It originally included⬎12 600 individuals, ages 14 to 21 years, who have been interviewed annually since 1979. Since 1986, biennial assessments have been administered to the children of women in the original cohort. We included children who were between 8 years, 0 months and 11 years, 0 months at the 1998 survey. This age range was selected because overweight prevalence signifi-cantly increases between ages 6 and 11 years compared with ages 5 years and younger.7,23 Given the underlying hypothesis that behavior problems precede the onset of overweight, we elected to assess the association beginning at 8 years of age so that the potential effect of behavior problems having their onset during the grade-school years could be measured. Of the original NLSY cohort, 4944 women were eligible to be surveyed in 1998. Of these, 87% (4301) were interviewed. Approximately 82% (3533) of the women interviewed were mothers. Response rates differed by ⬍5% among major racial groups for both the mother and the child assessments.24The eligible age range included 1416 children, and 90% (1268) of this group had weight and height data. We limited the sample to children with complete data for all covariates. The final sample, therefore, consisted of 755 children. This study was approved by the Institutional Review Board at Boston University School of Medicine.
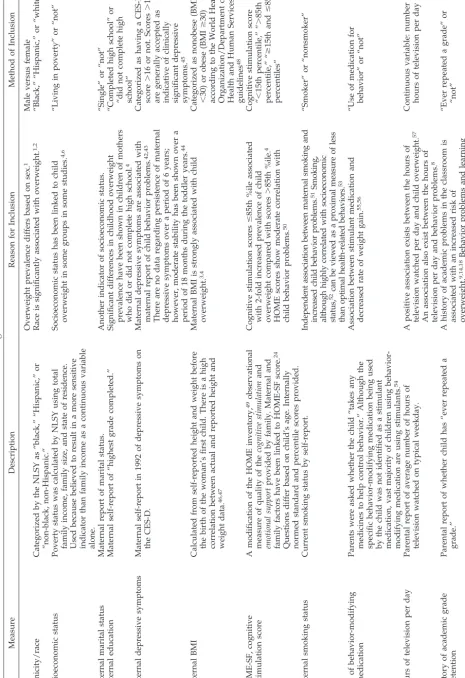
Demographic data consisted of child’s sex, race, mother’s mar-ital status, mother’s education, and family poverty status (Table 1). Additional characteristics that may modify an association between behavior problems and overweight were identified from the liter-ature and included as potential covariates (Table 1). These were mother’s obesity, mother’s depressive symptoms, Home Observa-tion for Measurement of the Environment-Short Form (HOME-SF) cognitive stimulation score, mother’s smoking status, use of be-havior-modifying medication, hours of television per day, and history of academic grade retention.
Overweight
Height and weight were measured by an in-home interviewer in 81% and 78% of subjects, respectively. For the remainder of subjects, parental report was used. There was no statistically sig-nificant difference between measured and reported height and weight data (data available on request). Child overweight was defined as a BMIⱖ95th percentile for age and sex based on the newest norms from the National Center for Health Statistics.25
Behavior Problems
Mothers answered questions regarding their child’s behaviors in the previous 3 months using the Behavior Problems Index (BPI). The BPI was created by Zill and Peterson26to measure the fre-quency, range, and type of childhood behavior problems for chil-dren ages 4 years and older. Many items were derived from the Achenbach Child Behavior Checklist.27 Mothers could answer “often,” “sometimes true,” or “not true” to each item. Responses were dichotomized into “often or sometimes true” or “not true” by the NLSY. These dichotomized scores are the basis for the age-and sex-based normed total stage-andard scores provided by the NLSY. Externalizing and internalizing standard scores were cre-ated by the NLSY on the basis of the trichotomous “often,” “some-times true,” or “not true” rating. Norms for externalizing and internalizing standard scores are age based but not sex based. Some questions in the BPI contribute to both the internalizing subscore and the externalizing subscore. The BPI is also divided into 6 subscales: antisocial, anxious/depressed, dependent, head-strong, hyperactive, and peer conflicts/withdrawn. The specific questions included in the BPI are provided in Table 2. Higher scores represent more behavior problems. The overall completion rate of the BPI was approximately 93%, with Hispanic children having slightly lower levels of completion.24We categorized total BPI standard scores as clinically meaningful when they were ⬎90th percentile for the entire cohort of 8- to 11-year-old children in the NLSY in 1996 and in 1998. We selected this cutoff on the basis of previous data indicating that BPI scores at this level are associated with higher rates of referrals for mental health servic-es.9The⬎90th percentile cutoff was also used to categorize inter-nalizing and exterinter-nalizing standard scores as clinically meaning-ful.
Statistical Analysis
All data analysis was done using SAS (SAS Institute Inc, Cary, NC). The survey oversampled children who were born to poor and minority women. Therefore, we weighted the data by using the sampling weights given for 1998 so that the sample is nation-ally representative of children among the same age cohort. De-scriptive statistics are provided as unweighted frequencies to demonstrate the actual composition of the sample. Clustering caused by the presence of siblings was accounted for by using generalized linear models fit via generalized estimating equa-tions.28
We performed multiple logistic regression accounting for clus-tering with children’s overweight status as the dependent vari-able. We computed both unadjusted and adjusted odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) from the logistic regression models. AllPvalues presented are 2-tailed. An ␣ level of 0.05 was used to determine statistical significance. The covariates described in Table 1 were included in a model. Each of these candidate covariates was tested in a model with behavior problems and overweight by excluding them one by one while keeping all others in the model. Covariates that altered the relationship of clinically meaningful behavior prob-lems to child overweight in these models by⬎10% were retained in the final model.29To determine whether internalizing or exter-nalizing behaviors were specifically accounting for the relation-ship of behavior problems to childhood overweight, internalizing and externalizing BPI scores⬎90th percentile were each tested individually in the model. In an attempt to elucidate temporal sequence, the analysis was repeated using a subsample of children who were not overweight in 1996, using 1996 BPI scores, 1996 BMI
zscores, and 1998 data for the remaining covariates.
To account for missing data, we created a model to determine whether selection bias altered the relationship between significant behavior problems and being overweight. We examined the influ-ence of potential selection bias by adding a propensity score to model the probability of inclusion in the sample with complete data.30Our estimation of the association between behavior prob-lems and child overweight was not altered by the inclusion of this variable.
RESULTS
The 1998 sample included 755 mother-child pairs. The ages of the children included in the analysis were 8 years, 0 months to 11 years, 0 months. Ap-proximately half of the sample was male, 12% were overweight, and 10% had a BPI score⬎90th percen-tile (Table 3). The average unweighted standard scores for the BPI subscales in overweight versus not overweight children were similar although consis-tently slightly greater in the overweight children (Ta-ble 4).
Behavior Problems and Concurrent Overweight
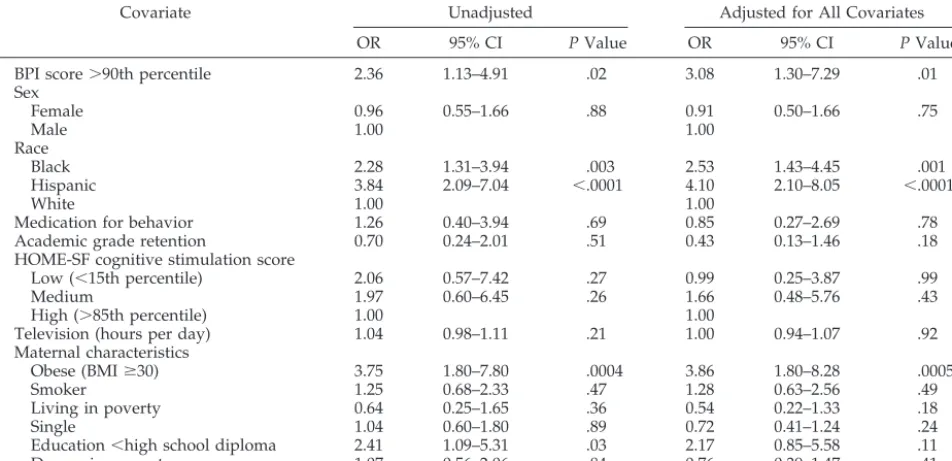
A relationship between clinically meaningful be-havior problems and overweight was present in the bivariate analysis (OR: 2.36; 95% CI: 1.13– 4.91). Other variables found to be associated with over-weight in the bivariate analysis were race, maternal obesity, and maternal education (Table 5).
control of 2 or more variables gives different results from those obtained by controlling for each variable separately. Therefore, race, maternal obesity, aca-demic grade retention, maternal education, poverty status, and HOME-SF cognitive stimulation score all were retained in the model. In this final model, clin-ically meaningful behavior problems were indepen-dently associated with concurrent child overweight (adjusted OR: 2.95; 95% CI: 1.34 – 6.49; Table 6).
We tested for the presence of interactions between the covariates by adding terms to the multiple logis-tic regression model. We examined interactions of race by significant behavior problems, by maternal obesity, by academic grade retention, by maternal education, by poverty status, by maternal depressive symptoms, and by HOME-SF cognitive stimulation score; maternal obesity by significant behavior prob-lems, by academic grade retention, by maternal ed-ucation, by poverty status, by maternal depressive symptoms, and by HOME-SF cognitive stimulation score; academic grade retention by significant behav-ior problems, by maternal education, by poverty sta-tus, by maternal depressive symptoms, and by HOME-SF cognitive stimulation score; maternal ed-ucation by significant behavior problems, by poverty status, by maternal depressive symptoms, and by HOME-SF cognitive stimulation score; family pov-erty status by significant behavior problems, by ma-ternal depressive symptoms, and by HOME-SF cog-nitive stimulation score; and maternal depressive symptoms by significant behavior problems and HOME-SF cognitive stimulation score. We could not evaluate HOME-SF cognitive stimulation score by significant behavior problems as we did not have the
power to do so. None of the interactions evaluated was statistically significant. Although a total BPI score ⬎90th percentile was related to overweight, neither an externalizing nor an internalizing subscale score ⬎90th percentile was significantly related to overweight.
Unlike previous research with the NLSY,4,31there
was no independent relationship between the num-ber of hours of television watched per day or cogni-tive stimulation in the home environment and child-hood overweight. To determine whether the absence of a relationship was attributable to controlling for behavior problems, we removed the clinically mean-ingful behavior problems variable from the model adjusted for all covariates that is listed in Table 5. There was no significant change in the relationship of either number of hours of television per day (OR: 1.00; 95% CI: 0.93–1.07) or low cognitive stimulation in the home environment (OR: 1.13; 95% CI: 0.28 – 4.60) with childhood overweight.
Behavior Problems in Normal-Weight Children and Future Overweight
Of the 755 children in the 1998 sample, 746 were interviewed in 1996 and 700 had height and weight data. Of these 700 children, 90% were not overweight in 1996, resulting in a final sample size of 629. Six percent of the 629 children who were not overweight in 1996 became overweight by 1998. This subsample of 629 children was similar to the original sample: 9% had clinically meaningful behavior problems, 7% of the mothers were obese, 10% of the families were living in poverty, 4% of the children were taking medication to modify behavior, and 9% had repeated a grade (additional data available on request).
When this subsample was entered into the model, a relationship of significant behavior problems in normal-weight children in 1996 to becoming over-weight 2 years later was present in the unadjusted analysis (OR: 2.87; 95% CI: 1.06 –7.80). We again en-tered the same candidate covariates (1998 data) and the BMIzscore from 1996 into the model one by one and retained those that altered the relationship be-tween behavior problems and future overweight by
⬎10%. The only covariates that altered the relation-ship in this manner were race, maternal obesity, HOME-SF cognitive stimulation score, and BMI z
score in 1996. After adjustment for these covariates, clinically significant behavior problems in normal-weight children in 1996 were independently associ-ated with becoming overweight 2 years later (ad-justed OR: 5.23; 95% CI: 1.37–19.93; Table 7).
CONCLUSIONS
We found in a nationally representative sample that clinically meaningful behavior problems in 8- to 11-year-old children were independently associated with concurrent child overweight and, in a separate analysis, with an increased risk of becoming over-weight 2 years later in normal-over-weight children. The magnitude of the relationship was similar to that of several previously recognized risk factors, including maternal obesity and race.
To our knowledge, our study is the first to inves-TABLE 2. Composition of BPI and Subscales
1. Sudden changes in mood/feeling (I, X) 2. Feels/complains no one loves him/her (I, X) 3. High strung, tense, nervous (E, H)
4. Cheats or tells lies (E, A) 5. Too fearful or anxious (E, I, X) 6. Argues too much (E, H)
7. Difficulty concentrating/paying attention (E, R) 8. Easily confused/in a fog (E, I, R)
9. Bullies or is cruel/mean to others (E, A) 10. Disobedient at home (E, H)
11. Does not feel sorry for misbehaving (A) 12. Trouble getting along with others (E, P) 13. Impulsive—acts without thinking (E, R) 14. Restless, overly active, etc (E, R) 15. Not liked by other children (E, P) 16. Trouble with obsessions, etc (E, R) 17. Is secretive, keeps to self
18. Stubborn, sullen, or irritable (E, H) 19. Strong temper, loses it easily (E, H) 20. Unhappy, sad, or depressed (E, I, X) 21. Withdrawn, not involved with others (I, P) 22. Breaks things deliberately (E, A)
23. Clings to adults (I, D) 24. Cries too much (I, D)
25. Demands a lot of attention (I, D) 26. Too dependent on others (I, D) 27. Worries too much
28. Feels worthless or inferior (I, X)
tigate systematically the relationship of a clinically meaningful level of behavior problems and child-hood overweight in a nationally representative sam-ple while analytically controlling for a large number of potentially confounding factors. Three previous studies demonstrated marginally increased scores on the Child Behavior Checklist in overweight children
in non– clinic-referred populations.15,18,19 The
num-ber of overweight children in these studies, however, varied from 25 to 30, and the samples were over-whelmingly minority (83%–100%) and of low socio-economic status. The only study that used a large sample that we are aware of demonstrated an in-creased teacher report of “behavioral problems” in association with an increased rate of weight gain in 5399 Swedish schoolchildren in the 1970s.14
Demo-graphic characteristics of this sample were neither described nor controlled for in the analysis.
Maternal obesity and race have strong indepen-dent associations with child overweight, both in our analyses and in others.3,4,7Controlling for these
fac-tors did not explain or diminish the independent relationship between behavior problems and over-weight. We hypothesized that poverty would be a significant confounding factor, given the relationship of socioeconomic status to behavior problems.9
Al-though poverty did conjointly modify the relation-ship between behavior problems and overweight in combination with race, maternal obesity, maternal education, academic grade retention, and HOME-SF TABLE 3. Demographic Characteristics of Unweighted Sample of Children With and Without BPI
Score⬎90th Percentile in 1998
Behavior Problems (n⫽73)
No Behavior Problems (n⫽682)
Total (N⫽755)
Child characteristics Sex (%)
Male 55 53 53
Female 45 47 47
Race (%)
Black 26 28 27
Hispanic 22 19 20
White 52 53 53
Overweight (BMIⱖ95th percentile; %)
Yes 21 11 12
No 79 89 88
Medication for behavior (%)
Yes 21 3 4
No 79 97 96
Repeated a grade (%)
Yes 21 7 9
No 79 93 91
HOME-SF cognitive stimulation score (%)
Low (⬍15th percentile) 37 15 18
Medium 56 73 71
High (⬎85th percentile) 7 12 11
Television (hours per day) 3.6⫾2.6 3.7⫾3.2 3.7⫾3.1 Maternal characteristics
Obese (BMI⬎30; %)
Yes 12 8 8
No 88 92 92
Smoker (%)
Yes 36 22 23
No 64 78 77
Living in poverty (%)
Yes 16 9 9
No 84 91 91
Single (%)
Yes 58 32 35
No 42 68 65
Education (%)
⬍High school diploma 21 8 9
ⱖHigh school diploma 79 92 91
Depressive symptoms (%)
Yes 48 20 22
No 52 80 78
TABLE 4. Unweighted Means With Standard Deviations for BPI Subscale Standard Scores, Overweight Versus Normal-Weight Children (n⫽755)
Subscale Overweight Not
Overweight
Mean SD Mean SD
Antisocial 109.2 16.2 105.4 13.8
Anxious/depressed 105.2 12.1 101.8 13.1
Headstrong 105.1 14.2 102.5 13.2
Hyperactive 104.3 14.3 101.8 13.8
Dependent 107.1 14.2 104.0 13.4
Peer
conflicts/withdrawn
105.1 13.3 103.1 11.6
cognitive stimulation score, the effect was relatively small. Unlike previous work with the NLSY data set,31the amount of television viewing did not
inde-pendently predict child overweight in our analysis or
act as a confounder. Controlling for behavior prob-lems also did not explain the absence of an associa-tion. This may reflect that the children in our sample are slightly younger than those in the previous study, and the association between television view-ing and overweight is less clear in younger chil-dren.5,32 The discrepancy may also reflect different
definitions of outcome. We used the definition for “overweight” (BMIⱖ95th percentile) compared with the previous study, which used the less stringent definition of “at risk for overweight” (BMI ⱖ85th percentile).
We also did not replicate the findings of a previous study demonstrating that low cognitive stimulation in the home is independently associated with child-hood overweight,4and this was also not explained
by controlling for behavior problems. The absence of an independent association may be because the pre-vious study included children initially ages birth to 8 years and evaluated the cumulative incidence of overweight 6 years later. The age range in our study was older, and the follow-up was not as long. Low cognitive stimulation in the home did, however, act as a joint confounder in our analysis, slightly dimin-ishing the relationship between behavior problems and overweight. This observation supports the pre-vious data indicating a significant role of the home environment in mediating the child’s weight status and speaks to the complexity of the association. The differences in findings in both the case of television viewing and cognitive stimulation in the home may also reflect different confounders controlled for in each analysis.
Although a relationship between a BPI score
⬎90th percentile and overweight was present, when we attempted to disaggregate internalizing and ex-ternalizing behavior problems, neither was related to overweight. These results suggest that of the children with clinically significant behavior problems, there was not a large proportion with either an internaliz-TABLE 5. Unadjusted and Adjusted ORs for Concurrent Overweight for Covariates in 1998 (n⫽755)
Covariate Unadjusted Adjusted for All Covariates
OR 95% CI PValue OR 95% CI PValue
BPI score⬎90th percentile 2.36 1.13–4.91 .02 3.08 1.30–7.29 .01
Sex
Female 0.96 0.55–1.66 .88 0.91 0.50–1.66 .75
Male 1.00 1.00
Race
Black 2.28 1.31–3.94 .003 2.53 1.43–4.45 .001
Hispanic 3.84 2.09–7.04 ⬍.0001 4.10 2.10–8.05 ⬍.0001
White 1.00 1.00
Medication for behavior 1.26 0.40–3.94 .69 0.85 0.27–2.69 .78
Academic grade retention 0.70 0.24–2.01 .51 0.43 0.13–1.46 .18
HOME-SF cognitive stimulation score
Low (⬍15th percentile) 2.06 0.57–7.42 .27 0.99 0.25–3.87 .99
Medium 1.97 0.60–6.45 .26 1.66 0.48–5.76 .43
High (⬎85th percentile) 1.00 1.00
Television (hours per day) 1.04 0.98–1.11 .21 1.00 0.94–1.07 .92
Maternal characteristics
Obese (BMIⱖ30) 3.75 1.80–7.80 .0004 3.86 1.80–8.28 .0005
Smoker 1.25 0.68–2.33 .47 1.28 0.63–2.56 .49
Living in poverty 0.64 0.25–1.65 .36 0.54 0.22–1.33 .18
Single 1.04 0.60–1.80 .89 0.72 0.41–1.24 .24
Education⬍high school diploma 2.41 1.09–5.31 .03 2.17 0.85–5.58 .11
Depressive symptoms 1.07 0.56–2.06 .84 0.76 0.39–1.47 .41
TABLE 6. Adjusted OR for Concurrent Overweight by BPI Score⬎90th Percentile and Factors Altering the Relationship by ⬎10%, 1998 Data (n⫽755)
OR 95% CI PValue
BPI score⬎90th percentile 2.95 1.34–6.49 .007 Race
Black 2.24 1.28–3.94 .005
Hispanic 3.83 1.97–7.46 ⬍.0001
White 1.00
Maternal obesity (BMIⱖ30) 3.89 1.83–8.26 .0004 Academic grade retention 0.44 0.13–1.46 .18 Maternal education⬍high
school diploma
2.23 0.85–5.83 .10
Living in poverty 0.49 0.20–1.20 .12 Maternal depressive symptoms 0.71 0.36–1.39 .31 HOME-SF cognitive
stimulation score
Low (⬍15th percentile) 0.96 0.25–3.71 .95
Medium 1.65 0.48–5.67 .42
High (⬎85th percentile) 1.00
TABLE 7. Adjusted OR for Future Overweight by 1996 BPI Score⬎90th Percentile and Factors Altering the Relationship by ⬎10% in Subsample of Children Who Were Not Overweight in 1996 (n⫽629)
OR 95% CI PValue
BPI score⬎90th percentile 5.23 1.37–19.93 .015 Race
Black 1.82 0.79–4.24 .17
Hispanic 5.47 2.18–13.7 .0003
White 1.00
Maternal obesity (BMIⱖ30) 5.95 1.67–21.2 .006 HOME-SF cognitive
stimulation score
Low (⬍15th percentile) 2.43 0.31–18.7 .39
Medium 4.10 0.52–32.4 .18
High (⬎85th percentile) 1.00
ing standard score⬎90th percentile or a large pro-portion with an externalizing score⬎90th percentile. Rather, it seems that the majority of children with BPI scores⬎90th percentile had subthreshold inter-nalizing and exterinter-nalizing BPI scores. This is consis-tent with our clinical experience and with the data presented in Table 4. The overweight children had slightly higher scores on all subscales; there were not particular subscales that seemed to be accounting for the relationship.
The results of our analysis of the temporal rela-tionship between child behavior problems and over-weight suggest that behavior problems may precede the onset of overweight at least in some children. Controlling for the child’s previous weight status only strengthened the association between behavior problems and subsequent overweight, which sup-ports our underlying hypothesis. Given that it seems that behavior problems sometimes precede becom-ing overweight, the higher prevalence of behavior problems in overweight children may not then sim-ply be a response to stigmatization.
Previous research has demonstrated a relationship between childhood depression and adult over-weight33in addition to a relationship between
ado-lescent depression and an increased risk of over-weight 1 year later.34Although the BPI cannot make
mental health diagnoses, behavior problems are sometimes indicative of underlying mental health diagnoses.9A significant change in weight is a
diag-nostic criterion for depression,35 and food binging
behavior has been reported as comorbid with psy-chiatric diagnoses in adults.36 – 40Thus, just as a
men-tal health diagnosis in childhood may be a risk factor for adult obesity, extreme behavior problems in childhood may be a more proximal indicator of over-weight risk in childhood.
There are potential limitations to the study reflect-ing residual confoundreflect-ing and study design. Our measure of maternal mental health was available only in 1992. There are no data, to our knowledge, regarding the stability of maternal depressive symp-toms over a period of 6 years. It is possible that a more proximal measure of maternal depressive symptoms would have slightly altered our results. We also were unable to control for paternal obesity, which is a risk factor for child overweight of similar magnitude to the risk of maternal obesity.3 There
may also be other confounding variables for which we were unable to control. Finally, our sample size of overweight children was limited. Unlike other stud-ies with limited sample size, however, our sample was nationally representative.
Implication
These data strongly suggest a significant relation-ship of behavior problems to childhood overweight. On the basis of our second analysis, it seems that children with behavior problems may be at increased risk of becoming overweight, suggesting that the clinical evaluation of children with significant behav-ioral problems should include an assessment of over-weight risk based on physical activity and nutrition. It should be emphasized that most overweight
chil-dren in our study did not have behavior problems. However, a better understanding of a child’s behav-ioral profile may be helpful in addressing the moti-vational issues that pediatricians perceive to be a major barrier to treatment41 of childhood
over-weight. Additional research is needed to understand how a child’s behavioral profile may be associated with physical activity and eating patterns leading to overweight.
ACKNOWLEDGMENTS
This study was supported by HRSA MCHB 5T77 MC00015 09, the American Heart Association Fellow-to-Faculty Transition Award, and the Joel and Barbara Alpert Endowment for Children of the City.
We thank Howard Bauchner, MD, for thoughtful review of the manuscript.
REFERENCES
1. Troiano R, Flegal K, Kuczmarski R, Campbell S, Johnson C. Overweight prevalence and trends for children and adolescents: The National Health and Nutrition Examination Surveys, 1963 to 1991.Arch Pediatr Adolesc Med. 1995;149:1085–1091
2. Strauss R, Pollack H. Epidemic increase in childhood overweight.
JAMA. 2001;286:2845–2848
3. Whitaker R, Wright J, Pepe M, Seidel K, Dietz W. Predicting obesity in young adulthood from childhood and parental obesity.N Engl J Med. 1997;337:869 – 873
4. Strauss R, Knight J. Influence of the home environment on the devel-opment of obesity in children. Pediatrics. 1999;103(6). Available at: http://www.pediatrics.org/cgi/content/full/103/6/e85
5. Dietz W, Gortmaker S. Do we fatten our children at the television set? Obesity and television viewing in children and adolescents.Pediatrics. 1985;75:807– 812
6. Sobal J, Stunkard A. Socioeconomic status and obesity: a review of the literature.Psychol Bull. 1989;105:260 –275
7. Troiano R, Flegal K. Overweight children and adolescents: description, epidemiology, and demographics.Pediatrics. 1998;101(suppl 3):497–504 8. Singer M, Slovak K, Frierson T, York P. Viewing preferences, symptoms of psychological trauma, and violent behaviors among children who watch television.J Am Acad Child Adolesc Psychiatry. 1998;37:1041–1048 9. Gortmaker S, Walker D, Weitzman M, Sobol A. Chronic conditions, socioeconomic risks, and behavioral problems in children and adoles-cents.Pediatrics. 1990;85:267–276
10. Yeates K, MacPhee D, Campbell F, Ramey C. Maternal IQ and home environment as determinants of early childhood intellectual competence: a developmental analysis.Dev Psychol. 1983;19:731–739 11. Fergusson D, Horwood L, Shannon F. Relationship of family life events,
maternal depression, and child-rearing problems.Pediatrics. 1984;73: 773–776
12. Clarizo H, McCoy G.Behavior Disorders in School-Aged Children. Scran-ton, PA: Chandler; 1970
13. Carey W, Hegvik R, McDevitt S. Temperamental factors associated with rapid weight gain and obesity in middle childhood.J Dev Behav Pediatr. 1988;9:194 –198
14. Mellbin T, Vuille J. Further evidence of an association between psycho-social problems and increase in relative weight between 7 and 10 years of age.Acta Paediatr Scand. 1989;78:574 –580
15. Banis H, Varni J, Wallander J, Korsch B. Psychological and social adjustment of obese children and their families.Child Care Health Dev. 1988;14:157–173
16. Israel A, Shapiro L. Behavior problems of obese children enrolling in a weight reduction program.J Pediatr Psychol. 1985;10:449 – 460 17. Epstein L, Klein K, Wisniewski L, Weng R. Child and parent
psycho-logical problems influence child weight control.Obes Res. 1994;2:509 18. Tershakovec A, Weller S, Gallagher P. Obesity, school performance and
behaviour of black, urban elementary school children.Int J Obes Relat Metab Disord. 1994;18:323–327
19. Pine D, Wasserman G, Coplan J, Staghezza-Jaramillo B. Cardiac profile and disruptive behavior in boys at risk for delinquency.Psychosom Med. 1996;58:342–353
20. Strauss C, Smith K, Frame C, Forehand R. Personal and interpersonal characteristics associated with childhood obesity.J Pediatr Psychol. 1985; 10:337–343
morbidly obese bariatric clinic patients. Am J Psychiatry. 1992;149: 227–334
22. Goldsmith S, Anger-Friedfeld K, Beren S, Rudolph D, Boeck M, Aronne L. Psychiatric illness in patients presenting for obesity treatment.Int J Eat Disord. 1992;12:63–71
23. Ogden C, Troiano R, Briefel R, Kuczmarski R, Flegal K, Johnson C. Prevalence of overweight among preschool children in the United States, 1971 through 1994.Pediatrics. 1997;99(4). Available at: http:// www.pediatrics.org/cgi/content/full/99/4/e1
24. Center for Human Resource Research.NLSY79: 1998 Child and Young Adult Data Users Guide, Columbus, OH: The Ohio State University; 2002 25. Kuczmarski R, Ogden C, Grummer-Strawn L, Flegal K, Guo S, Wei R.
CDC Growth Charts.Adv Data. 2000;314:1–28
26. Zill N, Peterson J.Behavior Problems Index. Washington, DC: Child Trends, Inc; 1986
27. Achenbach T, Edelbrock C.Manual for the Child Behavior Checklist and Revised Child Behavior Profile.Burlington, VT: University of Vermont, Department of Psychology; 1983
28. Diggle P, Liang K, Zeger S.Analysis of Longitudinal Data. Oxford, UK: Clarendon Press; 1994
29. Rothman K, Greenland S. Modern Epidemiology. Philadelphia, PA: Lippincott-Raven; 1998
30. Heckman J. Sample selection bias as a specification error.Econometrica. 1979;47:153–161
31. Gortmaker S, Must A, Sobol A, Peterson K, Colditz G, Dietz W. Tele-vision viewing as a cause of increasing obesity among children in the United States, 1986 –90.Arch Pediatr Adolesc Med. 1996;150:356 –362 32. DuRant R, Baranowski T, Johnson M, Thompson W. The relationship
among television watching, physical activity, and body composition of young children.Pediatrics. 1994;94:449 – 454
33. Pine D, Goldstein B, Wolk S, Weissman M. The association between childhood depression and adulthood body mass index.Pediatrics. 2001; 107:1049 –1056
34. Goodman E, Whitaker R. A prospective study of the role of depression in the development and persistence of adolescent obesity.Pediatrics. 2002;110:497–504
35. First M.Diagnostic and Statistical Manual of Mental Disorders.4th ed. Washington, DC: American Psychiatric Association; 1994
36. Brody M, Walsh B, Devlin M. Binge eating disorder: reliability and validity of a new diagnostic category.J Consult Clin Psychol. 1994;62: 381–386
37. Yanovski S, Nelson J, Dubbert B, Spitzer R. Association of binge eating disorder and psychiatric comorbidity in obese subjects.Am J Psychiatry. 1993;150:1472–1479
38. Womble L, Williamson D, Martin C, et al. Psychosocial variables asso-ciated with binge eating in obese males and females.Int J Eat Disord. 2001;30:217–221
39. Zwaan MD. Binge eating disorder and obesity.Int J Obes. 2001;1: S51–S55
40. Hudson J, McElroy S, Raymond N, et al. Fluvoxamine in the treatment of binge-eating disorder: a multicenter placebo-controlled, double blind trial.Am J Psychiatry. 1998;155:1756 –1762
41. Story M, Neumark-Stzainer D, Sherwood N, et al. Management of child
and adolescent obesity: attitudes, barriers, skills, and training needs among health care professionals.Pediatrics. 2002;110:210 –214 42. Fergusson D, Horwood L, Gretton M, Shannon F. Family life events,
maternal depression, and maternal and teacher descriptions of child behavior.Pediatrics. 1985;75:30 –35
43. Friedlander S, Weiss D, Traylor J. Assessing the influence of maternal depression on the validity of the Child Behavior Checklist.J Abnorm Child Psychol. 1986;14:123–133
44. McLennan J, Kotelchuck M, Cho H. Prevalence, persistence, and corre-lates of depressive symptoms in a national sample of mothers of tod-dlers.J Am Acad Child Adolesc Psychiatry. 2001;40:1316 –1323
45. Radloff L. The CES-D Scale: a self-report depression scale for research in the general population.J Appl Psychol Measurement. 1977;1:385– 401 46. Stunkard A, Albaum J. The accuracy of self-reported weights.Am J Clin
Nutr.1981;34:1593–1599
47. Stewart A. The reliability and validity of self-reported weight and height.J Chron Dis. 1982;35:295–309
48. World Health Organization.Measuring Obesity: Classification and De-scription of Anthropometric Data. Report on a WHO consultation on the epidemiology of obesity.Copenhagen, Denmark: WHO Regional Office for Europe, Nutrition Unit; 1988
49. Caldwell B, Bradley R.Home Observation for Measurement of the Environ-ment.Little Rock, AR: University of Arkansas at Little Rock, Center for Child Development and Education; 1984
50. Bradley R, Caldwell B, Rock S, Hamrick H. Home Observation for Measurement of the Environment: development of a home inventory for use with families having children 6 to 10 years old.Contemp Educ Psychol. 1988;13:58 –71
51. Weitzman M, Gortmaker S. Maternal smoking and behavior problems of children.Pediatrics. 1992;90:342–349
52. Lantz P, House J, Lepkowski J, Williams D, Mero R, Chen J Socioeco-nomic factors, health behaviors, and mortality: results from a nationally representative prospective study of US adults. JAMA. 1998;279: 1703–1708
53. Logan S, Spencer N. Smoking and other health related behaviour in the social and environmental context.Arch Dis Child. 1996;74:176 –179 54. Jensen P, Bhatara V, Vitiello B, Hoagwood K, Feil M, Burke L.
Psycho-active medication prescribing for U.S. children: gaps between research and clinical practice.J Am Acad Child Adolesc Psychiatry. 1999;38:557–565 55. Barkley R, McMurray M, Edelbrock C, Robbins K. Side effects of meth-ylphenidate in children with attention deficit hyperactivity disorder: a systemic, placebo-controlled evaluation.Pediatrics. 1990;86:184 –192 56. Safer D, Allen R, Barr E. Depression of growth in hyperactive children
on stimulant drugs.N Engl J Med. 1972;287:217–220
57. Andersen R, Crespo C, Bartlett S, Cheskin L, Pratt M. Relationship of physical activity and television watching with body weight and level of fatness among children: results from the third National Health and Nutrition Examination Survey.JAMA. 1998;279:938 –942
58. Prior M, Smart D, Sanson A, Oberklaid F. Relationships between learn-ing difficulties and psychological problems in preadolescent children from a longitudinal sample.J Am Acad Child Adolesc Psychiatry. 1999;38: 429 – 436
IATROGENIC HYPOCHONDRIA
“For each illness that doctors cure with medicine, they provoke ten in healthy people by inoculating them with the virus that is a thousand times more powerful than any microbe: the idea that one is ill.”
DOI: 10.1542/peds.112.5.1138
2003;112;1138
Pediatrics
Zuckerman
Julie C. Lumeng, Kate Gannon, Howard J. Cabral, Deborah A. Frank and Barry
in Children
Association Between Clinically Meaningful Behavior Problems and Overweight
Services
Updated Information &
http://pediatrics.aappublications.org/content/112/5/1138 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/112/5/1138#BIBL This article cites 47 articles, 12 of which you can access for free at:
Subspecialty Collections
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.112.5.1138
2003;112;1138
Pediatrics
Zuckerman
Julie C. Lumeng, Kate Gannon, Howard J. Cabral, Deborah A. Frank and Barry
in Children
Association Between Clinically Meaningful Behavior Problems and Overweight
http://pediatrics.aappublications.org/content/112/5/1138
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.