ARTICLE
Oral Probiotics Prevent Necrotizing Enterocolitis in
Very Low Birth Weight Preterm Infants: A
Multicenter, Randomized, Controlled Trial
Hung-Chih Lin, MDa, Chyong-Hsin Hsu, MDb, Hsiu-Lin Chen, MDc, Mei-Yung Chung, MDd, Jen-Fu Hsu, MDe, Rey-in Lien, MDe, Lon-Yen Tsao, MDf, Chao-Huei Chen, MDg, Bai-Horng Su, MD, PhDa
aDepartment of Pediatrics and School of Chinese Medicine, China Medical University Hospital, Taichung, Taiwan;bDepartment of Pediatrics, Mackay Memorial Hospital,
Taipei, Taiwan;cDepartment of Pediatrics, Chung-Ho Memorial Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan;dDepartment of Pediatrics, Chang Gung
Memorial Hospital at Kaohsiung, Kaohsiung, Taiwan;eDepartment of Pediatrics, Chang Gung Children’s Hospital, Taoyuan, Taiwan;fDepartment of Pediatrics, Changhua
Christian Hospital, Changhua, Taiwan;gDepartment of Pediatrics, Taichung Veterans General Hospital, Taichung, Taiwan
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
Orally administered probiotics reduce the incidence of NEC in VLBW preterm infants. However, optimal strains, timing, dosage, and duration of probiotic administration to VLBW preterm infants need to be further evaluated in large trials.
What This Study Adds
Bifidobacteriummay be the most appropriate strain for the prevention of NEC. Probiotics containingBifidobacterium bifidumandLactobacillus acidophilus, administered orally for 6 weeks, reduced the incidence of death or NEC for VLBW preterm infants.
ABSTRACT
OBJECTIVE.The goal was to investigate the efficacy of orally administered probiotics in preventing necrotizing enterocolitis for very low birth weight preterm infants.
METHODS.A prospective, blinded, randomized, multicenter controlled trial was con-ducted at 7 NICUs in Taiwan, to evaluate the beneficial effects of probiotics in necrotizing enterocolitis among very low birth weight infants (birth weight:⬍1500 g). Very low birth weight infants who survived to start enteral feeding were eligible and were assigned randomly to 2 groups after parental informed consent was obtained. Infants in the study group were givenBifidobacterium bifidumand Lactoba-cillus acidophilus, added to breast milk or mixed feeding (breast milk and formula), twice daily for 6 weeks. Infants in the control group were fed with breast milk or mixed feeding. The clinicians caring for the infants were blinded to the group assignment. The primary outcome measurement was death or necrotizing enteroco-litis (Bell’s stageⱖ2).
RESULTS.Four hundred thirty-four infants were enrolled, 217 in the study group and 217 in the control group. The incidence of death or necrotizing enterocolitis (stage
ⱖ2) was significantly lower in the study group (4 of 217 infants vs 20 of 217 infants). The incidence of necrotizing enterocolitis (stageⱖ2) was lower in the study group, compared with the control group (4 of 217 infants vs 14 of 217 infants). No adverse effect, such as sepsis, flatulence, or diarrhea, was noted.
CONCLUSION.Probiotics, in the form ofBifidobacteriumandLactobacillus, fed enterally to very low birth weight preterm infants for 6 weeks reduced the incidence of death or necrotizing enterocolitis.Pediatrics2008;122:693–700
N
ECROTIZING ENTEROCOLITIS (NEC)is one of the most catastrophic gastrointestinal emergencies in very low birthweight (VLBW) preterm infants, affecting 7% to 14% of these infants.1NEC is a leading cause of death and
morbidity in NICUs,2,3and the incidence of NEC has not changed in the past 20 years.2Recent reports suggested the
increasing occurrence of NEC and estimated up to 9000 cases of NEC in the United States every year, with a case fatality rate of 15% to 30%.4
The pathogenesis of NEC remains an enigma, but it is widely considered a multifactorial disease; prematurity, enteral feeding, intestinal hypoxia-ischemia, and bacterial colonization are considered major risk factors. Most likely, NEC is the clinical culmination of multiple risk factors that result in bowel injury through a final, common, inflammatory pathway.5–8
It has been suggested that an inappropriate, accentuated, inflammatory response to colonizing pathogenic florae in the premature gastrointestinal tract plays a major role in the initiation of NEC.9 The inflammatory cascade
promotes the spread of bacteria or toxin, resulting in ischemia, necrosis, and, in some cases, perforation.10 In vitro
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-3007
doi:10.1542/peds.2007-3007
This trial has been registered at www.clinicaltrials.gov (identifier NCT00540033).
Drs Lin and Hsu contributed equally to this report.
Key Words
probiotics, necrotizing enterocolitis, very low birth weight infants
Abbreviations
NEC—necrotizing enterocolitis VLBW—very low birth weight PVL—periventricular leukomalacia CLD— chronic lung disease IVH—intraventricular hemorrhage
Accepted for publication Feb 13, 2008
Address correspondence to Hung-Chih Lin, MD, Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan, No. 2 Yu-Der Road, Taichung, 404, Taiwan. E-mail: [email protected]
evidence showed that pathogenic florae attach to the epi-thelial cells of preterm infants much more easily than to those of term infants,11,12and studies indicated that
com-mensal bacteria could inhibit or reduce inflammatory sig-naling in intestinal epithelia through inhibition of the NF-B pathway.13,14These data suggest that probiotics, by
modifying the occurrence of these cascades of events, may play a major role in reducing the incidence of NEC.
Bin-Nun et al15 and we16 showed that orally
admin-istered probiotics reduce the incidence of NEC in VLBW preterm infants. Two meta-analyses arrived at the same conclusion; however, the limited number of clinical tri-als results in lack of definition of optimal strains, timing, dosage, and duration of probiotics administered to VLBW preterm infants, and these issues need to be eval-uated in large trials.17,18Furthermore, it has been
spec-ulated that the microbes of the developing intestinal tract of premature infants affect the maturation and optimal functioning of the intestinal innate and adaptive immune systems. Therefore, intestinal microbes may be involved in the pathogenesis of systemic inflammation-related diseases such as chronic lung disease (CLD), in-traventricular hemorrhage (IVH), and periventricular leukomalacia (PVL).19,20 However, no clinical trial has
examined this hypothesis.
Bifidobacteria and lactobacilli are commonly found in breastfed infants,21 and most cases of NEC in VLBW
infants occur before 6 weeks of age.22We hypothesized
that orally administered probiotics, in the form of bi-fidobacteria and lactobacilli, fed to VLBW preterm in-fants for 6 weeks would reduce the incidence and sever-ity of NEC.
METHODS
We performed a pilot study from January 1, 2005, to March 31, 2005, to verify the viability of probiotic bac-teria in the stool when Infloran (National Collection of Dairy Organisms, Reading, United Kingdom and Labo-ratorio, Farmaceutico, Mede, Italy)(containing Lactoba-cillus acidophilus and Bifidobacterium bifidum) was fed to VLBW preterm infants. Stool was collected for the first week of life from VLBW preterm infants (gestational age:
⬍34 weeks; birth weight:⬍1500 g) who were fed Inflo-ran in the NICU of China Medical University Hospital, after informed parental consent was obtained. Fecal samples were analyzed by using the methods reported by Lee et al23; we confirmed that B bifidum and L
aci-dophilus colonized the intestines of preterm infants fed Infloran.
From April 1, 2005, to May 30, 2007, a prospective, masked, randomized, controlled trial was conducted in 7 level III NICUs in Taiwan. The study protocol was ap-proved by the institutional review board of each hospi-tal. VLBW preterm infants (gestational age:⬍34 weeks; birth weight: ⬍1500 g) who survived to feed enterally were eligible for the trial. They were assigned randomly to the study or control group by the principal investiga-tor at each center after informed parental consent was obtained. Randomization was performed by using se-quential numbers generated at the computer center of China Medical University Hospital and sent to the
prin-cipal investigator at each center when an infant was eligible for enrollment. VLBW preterm infants who had severe asphyxia (stage III), fetal chromosomal anoma-lies, cyanotic congenital heart disease, congenital intes-tinal atresia, gastroschisis, or omphalocele, those who were fed exclusively with formula, and those who were fasted for⬎3 weeks were excluded.
The study group was given Infloran (L acidophilus[109 colony-forming units, NCDO 1748; National Collection of Dairy Organisms] andB bifidum[109colony-forming units, NCDO 1453; National Collection of Dairy Organ-isms, Reading, United Kingdom]; Laboratorio Farmaceu-tico, Italy) at 125 mg/kg per dose twice daily, through addition to breast milk or mixed feeding (breast milk and formula), for 6 weeks; the control group was fed breast milk or mixed feeding. Infloran was sent to each center and stored in a refrigerator at 2°C to 8°C. Infloran was added to breast milk (the infant’s own mother’s milk) or formula by the breast milk team before feeding. Both breast milk and formula for the study and control groups were prepared by the breast milk team, who did not know the colony counts of probiotics and were not involved in the care of the infants. The team members followed the orders from a sealed envelope. Therefore, the only personnel who knew of the infants’ group assignments were the investigators at each center and those on the breast milk team, who were not involved in the care of the study infants.
The indications for feeding and a strict feeding proto-col were followed for all study infants, as described in a previous study.16 Depending on the birth weight and
gestational age, a certain amount of breast milk was initiated after the infant tolerated 1 trial of distilled wa-ter. On the first day, 1 mL/kg distilled water was given twice, followed by breast milk. The amount of feeding was increased slowly if tolerated, with increments of no more than 20 mL/kg per day per feeding. An oral intake of 100 mL/kg per day was defined as complete enteral feeding. Feeding was stopped if there was any sign of feeding intolerance, defined as the presence of gastric aspirate in an amount that was more than one half of the previous feeding, twice, with abdominal distension. In-fants who weighed ⬍1000 g received total parenteral nutrition until one half of their energy was supplied through the oral route. The same attending physician was in charge of the care of the infants during their hospital stay. The residents who rotated through the NICU provided care by following established protocols in the unit. Definitions of prenatal steroid use, small for gestational age, prolonged rupture of amniotic mem-branes, chorioamnionitis, asphyxia, respiratory distress syndrome, patent ductus arteriosus, IVH, PVL, and sepsis and indications for surfactant and indomethacin were as described in our previous study.15The management
trans-mitted to the office of the principal investigator (Dr Lin) at China Medical University Hospital.
NEC was diagnosed and classified according to a mod-ification of the classmod-ification described by Bell et al.24The
final determination of the diagnosis of NEC of stageⱖ2 was made by 2 independent attending physicians who did not know the group assignment of the infant. If there was disagreement, then the senior neonatologist in each center was consulted to make the final diagnosis. Spon-taneous intestinal perforation was diagnosed on the ba-sis of clinical, radiologic, and histologic findings25 by 2
independent attending physicians who did not know the group assignment of the infant.
Demographic and clinical variables that were poten-tial risk factors for NEC were recorded in the protocol once the infants completed the 6-week study period. The primary outcome was death or stage ⱖ2 NEC that oc-curred during the study period. Secondary outcomes were culture-proven sepsis without NEC, CLD, IVH, PVL, feeding amount per week, days to full enteral feed-ing, and weight gain per week. Adverse effects, including culture-proven sepsis attributable to L acidophilus or B bifidum, flatulence, and diarrhea, also were recorded.
The event rate for sample size calculation was based on unpublished data of the Premature Infant Founda-tion of Taiwan and the Bravura NaFounda-tional Health Insur-ance database (2003–2004). Their recent event rate for death or NEC (stageⱖ2) for VLBW preterm infants was
⬃25% for level III neonatal centers in Taiwan. With the
␣error set at .05 and theerror at .1 and an absolute reduction in the incidence of NEC or death of 50%, the number needed to verify our hypothesis was 203 infants for each arm. Student’s 2-tailedttest and the2test or Fisher’s exact test were used to explore the differences in continuous and categorical variables, respectively. Uni-variate and multiUni-variate logistic regression models were used to estimate odds ratios and 95% confidence inter-vals. Multivariate logistic regression analysis was used to assess the relationship between different outcome mea-sures and the effect of probiotics, after adjustment for the potentially confounding effects of demographic fac-tors, clinical characteristics, and possible bias attributable to the multicenter design. All statistical tests were 2-sided, and aPvalue of⬍.05 was considered to indicate statistical significance. Analyses were performed with SAS 9.1 (SAS Institute, Cary, NC).
RESULTS
Figure 1 shows the flow of study subjects through the phases of the study. There were 580 VLBW infants ad-mitted to the 7 NICUs during the study period. One hundred thirty-seven infants were excluded; either they died (n⫽98), they met the exclusion criteria (n⫽14), or family members declined consent for the study (n⫽ 25). A total of 443 infants were enrolled in the trial; 3 infants in the study group and 1 in the control group dropped out of the program because of parental wishes to withdraw the infants from the trial. Two infants in the study group and 3 in the control group underwent spon-taneous intestinal perforation and were excluded. There were 217 infants in the study arm and 217 in the control
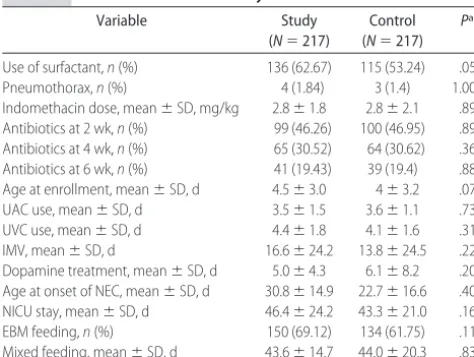
arm. The mothers’ clinical and infants’ demographic and clinical characteristics did not differ between the 2 groups, except for lower birth weight and first arterial blood pH values in the study group (Table 1). The in-fants’ clinical variables also did not differ between the 2 groups, except for more frequent use of surfactant re-placement therapy in the study group (Table 2).
Table 3 shows the primary outcomes of the study. The incidence of death or stageⱖ2 NEC (4 of 217 infants vs 20 of 217 infants; P⫽.002) was significantly lower in the study group, compared with the control group. Two infants in the study group and 9 infants in the control group developed stage 2 NEC; 2 infants in the study group and 5 infants in the control group developed stage 3 NEC. Four and 14 infants developed stageⱖ2 NEC in the study and control groups, respectively (P ⬍ .02). There was no difference between the study group and control group in the incidence of death attributable to
TABLE 1 Perinatal Variables for Study Infants
Variable Study
(N⫽217)
Control (N⫽217)
Pa
PROM,n(%) 59 (21.2) 64 (29.8) .55
Preeclampsia,n(%) 37 (17.0) 37 (17.2) .97 Prenatal steroid treatment,n(%) 107 (49.3) 96 (44.7) .33 Amnionitis,n(%) 16 (7.4) 14 (6.5) .72 Cesarean section,n(%) 149 (69.6) 136 (63.3) .16
Male,n(%) 122 (56.2) 115 (53) .50
SGA,n(%) 47 (21.7) 46 (21.2) .91
Apgar score of⬍6 at 5 min,n(%) 61 (28.5) 50 (23.5) .24
Asphyxia,n(%) 8 (3.7) 5 (2.3) .58b
Birth weight, mean⫾SD, g 1028.9⫾246.0 1077.3⫾214.4 .03 First arterial pH, mean⫾SD 7.26⫾0.13 7.29⫾0.11 .01
PROM indicates prolonged rupture of membrane; SGA, small for gestational age.
aByttest or2test. bBy Fisher’s exact test.
Assessed for eligibility (n = 580)
Randomly assigned (n = 443)
Enr
ol
lment
Al
lo
cation
Follow-up
Allocated to intervention (n = 221) Received allocated intervention (n = 221)
Excluded (n = 137): died (n = 98), did not meet inclusion
criteria (n = 14), refused to participate (n = 25)
Final number analyzed: 217 Discontinued intervention Family withdraw (n = 1) SIP
(n = 3)
Final number analyzed: 217 Allocated to intervention (n = 222) Received allocated intervention (n = 222)
Discontinued intervention Family withdraw (n = 3) SIP
(n = 2)
A
nalysi
s
FIGURE 1
NEC. The incidence of death not attributable to NEC (0 of 217 infants vs 6 of 217 infants;P⫽.04) was signifi-cantly lower in the study group, compared with the control group.
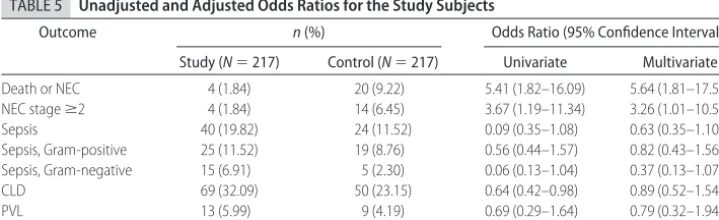
The outcomes of infants enrolled in each center are shown in Table 4. Table 5 shows the unadjusted and adjusted odds ratios for primary (death or NEC) and secondary outcome variables. The incidence of death or stageⱖ2 NEC was significantly lower in the probiotic-treated group in both unadjusted and adjusted analyses; the latter was performed by entering potential con-founding variables (birth weight, surfactant use, pH, ges-tational age, and center) into the multivariate logistic regression model. Similar results were found in the anal-ysis of NEC alone. For the secondary outcomes, there were no differences between the 2 groups with respect to PVL and severe IVH; although sepsis was more fre-quent among infants in the study group, there was no difference in the univariate analysis or with adjustment for various confounding variables, such as birth weight, umbilical venous catheter use, intermittent mandatory ventilation, NICU stay, and center. The pathogens were most often related to catheter-related infections in both groups. None of the positive blood cultures yielded Lac-tobacillus or Bifidobacterium spp. The incidence of CLD
was higher in the study group according to the univar-iate analysis, but no difference was observed in the logistic regression analysis. No other adverse effect, such as flatulence or diarrhea, was noted.
Table 6 presents outcome variables for different weight groups in the study and control groups. The number of infants was limited for infants weighing⬍750 g, and results are difficult to interpret because of type II error. Incidence of death or NEC ⱖstage 2 was signifi-cantly lower in infants weighted 500 –750 g (p ⫽0.02) and 1001–1500g (p ⫽ 0.02), but approach to nearly significant in infants weighted 751–1000 g (p ⫽ 0.07). Incidence of NEC ⱖstage 2 was significantly lower in infants weighted 1001–1500 g (p ⫽0.02), but not sig-nificant in infants weighted 500 –750 g and 751–1000 g. There was a trend that incidence NEC ⱖ stage 2 was lower in infants weighted 500 –750 g and 751–1000 g (1 vs 2 and 3 vs 5). Occurrence of sepsis was most often in the infants weighted ⬍1000 g. The incidence of Gram-positive and Gram-negative sepsis did not differ between study and control groups for infants in the different weight groups.
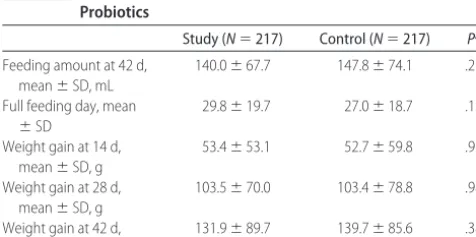
Table 7 shows that the age of attainment of full feed-ing and weight gain at various ages were similar between the 2 groups.
DISCUSSION
This is the first multicenter, randomized, controlled trial that showed efficacy of probiotics containing B bifidum and L acidophilus in reducing the incidence of NEC among VLBW preterm infants. We also found that the study group had a lower incidence of death or NEC. According to our data, the number needed to treat to prevent 1 case of NEC was 20 patients, and the number needed to treat to prevent 1 death or case of NEC was 14 patients.
Many variables have been suggested to be associated with the development of NEC; however, only prematu-rity and low birth weight have been consistently identi-fied in case-control studies.26,27 The current study was
designed as a multicenter, randomized, controlled trial. During the randomization process, we neglected to strat-ify according to birth weight, which resulted in an im-balance of patient assignment to the study and control groups, with the birth weight being lower in the former group. The lower birth weight also accounts for the greater acuity of the infants’ illness, as evidenced by lower first arterial pH and more frequent use of surfac-tant therapy. The difference in birth weight was because there were 33 infants in the study group but only 18 infants in the control group who weighed⬍750 g. How-ever, in the study group, there was lower incidence of death or NEC in different weight groups; incidence NEC tended to be lower in each weight group and no infants died with NEC. We addressed this methodologic defi-ciency by performing posthoc, multivariate, logistic re-gression analysis, entering potential risk factors that could bias the results (eg, birth weight and first arterial pH). Additional support for the validity of our data was the demonstration that the incidence of the primary study outcome (death or NEC) remained lower in the TABLE 2 Clinical Variables for Study Infants
Variable Study
(N⫽217)
Control (N⫽217)
Pa
Use of surfactant,n(%) 136 (62.67) 115 (53.24) .05 Pneumothorax,n(%) 4 (1.84) 3 (1.4) 1.00b
Indomethacin dose, mean⫾SD, mg/kg 2.8⫾1.8 2.8⫾2.1 .89 Antibiotics at 2 wk,n(%) 99 (46.26) 100 (46.95) .89 Antibiotics at 4 wk,n(%) 65 (30.52) 64 (30.62) .36 Antibiotics at 6 wk,n(%) 41 (19.43) 39 (19.4) .88 Age at enrollment, mean⫾SD, d 4.5⫾3.0 4⫾3.2 .07 UAC use, mean⫾SD, d 3.5⫾1.5 3.6⫾1.1 .73 UVC use, mean⫾SD, d 4.4⫾1.8 4.1⫾1.6 .31 IMV, mean⫾SD, d 16.6⫾24.2 13.8⫾24.5 .22 Dopamine treatment, mean⫾SD, d 5.0⫾4.3 6.1⫾8.2 .20 Age at onset of NEC, mean⫾SD, d 30.8⫾14.9 22.7⫾16.6 .40 NICU stay, mean⫾SD, d 46.4⫾24.2 43.3⫾21.0 .16 EBM feeding,n(%) 150 (69.12) 134 (61.75) .11 Mixed feeding, mean⫾SD, d 43.6⫾14.7 44.0⫾20.3 .83
UAC indicates umbilical artery catheter; UVC, umbilical venous catheter; IMV, intermittent man-datory ventilation; EBM, exclusive breast milk.
aByttest or2test. bBy Fisher’s exact test.
TABLE 3 Primary Outcomes of Study
Outcome n Pa
Study (N⫽217)
Control (N⫽217)
Death or NEC 4 20 .002
NEC, stage 2 2 9 .27
NEC, stage 3 2 5 .13
NEC, stageⱖ2 4 14 .02
Death attributable to NEC 2 3 .98
Death not attributable to NEC 0 6 .04
probiotic-treated group. Because center variation can play an important role in outcome, we included center outcomes in the model.
Because of the methodologic misstep that caused un-even distribution of the weight groups and resulted in fewer infants weighing⬍750 g in the control group, it is difficult to interpret the results for infants weighing
⬍750 g because of type II error. In the study group, however, there were significantly lower incidences of death or NEC in different weight groups; the incidence of NEC tended to be lower in each weight group, and no infants died as a result of causes other than NEC. Addi-tional research with an adequate number of weight-stratified infants is urgently needed to help define the beneficial effects of probiotics in each group.
The ability of bacteria to cross epithelial cell layers is thought to be a crucial first step in the cascade of events leading to the development of NEC.28,29Bacterial
inter-actions with the premature gut might play a major role in the proposed pathogenesis of NEC; many studies sug-gest a strong relationship between delay and low colo-nization of commensal florae and proliferation of patho-genic florae in the immature gut, predisposing preterm infants to develop NEC.28–32Using animal models, Caplan
et al33and Butel et al34showed that bifidobacterial
sup-plementation in rat pup and quail models resulted in intestinal colonization and subsequent reduction in NEC-like lesions. Our findings of a beneficial effect of oral probiotic supplementation may be based on this mechanism. Bifidobacteria and lactobacilli have been shown to inhibit intestinal colonization of pathogenic
microorganisms, to produce protective nutrients, and to prevent translocation of other bacteria.35These
charac-teristics support the use ofBifidobacteriumand Lactobacil-lusas appropriate species of probiotics for the prevention of NEC.
The probiotics we used in the current study were different from those in our previous study, because the supplier of the probiotics altered the formula by chang-ingBifidobacterium infantis(used in our previous trial) to B bifidum (used in current study). In the study by Bin-Nun et al,15the probiotics containedB infantis,
Streptococ-cus thermophilus, and B bifidum. Molecular studies have indicated that Bifidobacterium spp in the intestinal tract can range from 60% to 90% of the total fecal microbiota in breastfed infants, and lactic acid-producing bacteria may account for⬍1% of the total microbiota, indicating the significant dominance of Bifidobacterium.36 Studies
also indicated thatB bifidum,Bifidobacterium longum, and Bifidobacterium breve are the most common strains in healthy breastfeeding infants.37,38A recent study showed
that B bifidum is a promising candidate for probiotic intervention in inflammatory disorders of the gastroin-testinal tract.39On the basis of these clinical trials and in
vitro studies, it is reasonable to speculate that probiotics that contain Bifidobacterium might be most appropriate for the prevention of NEC.
Human milk feeding has been shown to reduce the incidence of NEC but cannot eradicate NEC, as in this study. Three of 4 infants in the study group and 6 of 14 infants in the control group were receiving exclusive breast milk feeding but still developed NEC. It has been TABLE 4 Outcome Variables at Each Center
Outcome n
A (N⫽63) B (N⫽56) C (N⫽70) D (N⫽59) E (N⫽71) F (N⫽61) G (N⫽54)
Death or NEC 4 2 4 3 5 4 2
NEC, stageⱖ2 3 2 3 2 3 3 2
Death not attributable to NEC 1 0 1 1 2 1 0
Death attributable to NEC 0 1 1 0 1 1. 1
Sepsis 9 7 11 9 12 7 9
CLD 18 14 20 16 21 17 13
PVL 3 2 4 2 5 4 2
IVH, gradeⱖ3 2 1 3 2 4 2 2
A to G represent the neonatal centers.
TABLE 5 Unadjusted and Adjusted Odds Ratios for the Study Subjects
Outcome n(%) Odds Ratio (95% Confidence Interval)
Study (N⫽217) Control (N⫽217) Univariate Multivariate
Death or NEC 4 (1.84) 20 (9.22) 5.41 (1.82–16.09) 5.64 (1.81–17.58) NEC stageⱖ2 4 (1.84) 14 (6.45) 3.67 (1.19–11.34) 3.26 (1.01–10.57) Sepsis 40 (19.82) 24 (11.52) 0.09 (0.35–1.08) 0.63 (0.35–1.10) Sepsis, Gram-positive 25 (11.52) 19 (8.76) 0.56 (0.44–1.57) 0.82 (0.43–1.56) Sepsis, Gram-negative 15 (6.91) 5 (2.30) 0.06 (0.13–1.04) 0.37 (0.13–1.07) CLD 69 (32.09) 50 (23.15) 0.64 (0.42–0.98) 0.89 (0.52–1.54)
PVL 13 (5.99) 9 (4.19) 0.69 (0.29–1.64) 0.79 (0.32–1.94)
IVH, gradeⱖ3 6 (2.78) 10 (4.69) 1.72 (0.62–4.83) 2.01 (0.67–6.01)
shown that human milk feeding may not eliminate NEC because of interleukin 10 deficiency.40 Both
Bifidobacte-rial and Lactobacillus has been shown to induce IL10 production.41,42 Breastfeeding promotes a strong
bi-fidobacterial presence in the infant gut by providing oligosaccharides that act as favorable substrates for bi-fidobacteria. Oral administration of specific strains of Lactobacillusspecies stimulate the Bifidobacterium micro-biota.43Probiotics and human milk may have synergistic
effects with bifidobacteria and lactobacilli to inhibit the inflammatory response in NEC. In the current study and as in most NICUs, a large majority of infants were fed human milk; therefore, it was difficult to demonstrate potential synergistic effects of probiotics and human milk.
Our previous study16 and other studies44,45 showed
that probiotics may reduce the incidence of sepsis; how-ever, meta-analysis did not confirm this association.17,18
The current study did not show that probiotics reduced the incidence of sepsis in VLBW infants as in our previ-ous study, and occurrences of sepsis even seemed more frequent in the study group. Our previous study did not examine sepsis in detail. We analyzed the frequency of sepsis according to Gram-positive, Gram-negative, and fungal infections and found that the pathogens were most often related to catheter-related infections in both groups. Theoretically, changing the intestinal ecosystem could not prevent Gram-positive sepsis. The incidence of
Gram-negative sepsis was higher in the study group, but no difference was observed in either univariate analysis or logistic regression analysis with risk factors. It is well known that risk factors for late-onset sepsis include young gestational age, use of a central line, total paren-teral nutrition, and prolonged use of mechanical venti-lation, among others.45 We speculate that probiotics
would not prevent late-onset sepsis because of the com-plexity of this disorder. Probiotics alone could not over-come the invasive procedures inducing infection. The same speculation can be made regarding the nonsignif-icant effects on CLD, IVH, and PVL. The primary effect of orally administered probiotics is in the gastrointestinal tract. It is not surprising to see the lack of beneficial effects on other organs, such as the lung and central nervous system.
A few case reports have raised concerns regarding infections with probiotic microorganisms in patients who are immunocompromised or have underlying med-ical conditions predisposing them to infection.47,48
How-ever, it was noted by Presterl et al48 that some
Lactoba-cillusstrains can be found in the intestinal microbiota of healthy humans, and the source of infection in those cases cannot be conclusively proven.49In a review of the
literature, there were no reports of bifidobacterial sepsis related to probiotic use; this is in keeping with animal studies that suggest low pathogenicity.50Although Kunz
et al51 described 2 premature infants who developed
Lactobacillusbacteremia while takingLactobacillus rhamo-sus GG (LGG) supplements, both of those preterm in-fants had short-gut syndrome; other authors and we did not observe sepsis attributable to probiotic organisms during the studies.15–18The number of patients
accumu-lated from all clinical trials may yield enough power to state that treatment is relatively safe, comparing the possible sepsis attributable to probiotics (0 of 940 pa-tients; sum of all clinical trials including ours)17,18with
the higher incidence (7%–14%) and disastrous effects of NEC for VLBW infants.
The incidence of NEC or death was lower than the expected effect size we used in the sample size calcula-tion. This may be partly a result of improvements in the quality of care for VLBW infants in Taiwan. It may also TABLE 6 Outcome Variables for Different Weight Groups
Outcome 500–750 g 751–1000 g 1001–1500 g
Study (N⫽33)
Control (N⫽18)
Pa Study
(N⫽69)
Control (N⫽61)
Pa Study
(N⫽115)
Control (N⫽138)
Pa
Weight, mean⫾SD, g 665.7⫾69.6 677.9⫾49.7 .52 873.5⫾73.5 886.3⫾76.0 .33 1227.8⫾127.1 1213.8⫾117.1 .36
Death without NEC,n(%) 0 3 (16.66) .04 0 3 (4.91) .11 0 0
Death or NEC,n(%) 1 (3.03) 5 (27.77) .02 3 (4.34) 8 (13.11) .07 0 7 (5.07) .02 NEC stageⱖ2,n(%) 1 (3.03) 2 (11.11) .29 3 (4.34) 5 (8.19) .47 0 7 (5.07) .02 Sepsis, Gram-positive,n(%) 9 (27.3) 1 (5.6) .08b 8 (11.6) 9 (14.8) .59 8 (7.0) 9 (6.5) .89
Sepsis, Gram-negative,n(%) 3 (9.1) 0 (0) .54b 8 (13.0) 4 (6.6) .22 4 (5.2) 1 (1.5) .15b
CLD,n(%) 24 (72.72) 11 (61.11) .22 34 (4.92) 24 (39.34) .26 11 (9.57) 15 (10.86) .73
PVL,n(%) 6 (18.18) 0 .08 3 (4.34) 4 (6.56) .70 4 (3.48) 5 (3.62) 1.00
IVH,n(%) 3 (9.09) 0 .54 2 (2.89) 6 (9.83) .14 1 (0.87) 4 (2.89) .38
aBy 2-samplettest. bBy Fisher’s exact test.
TABLE 7 Feeding Amount and Weight Gain Outcomes With Probiotics
Study (N⫽217) Control (N⫽217) Pa Feeding amount at 42 d,
mean⫾SD, mL
140.0⫾67.7 147.8⫾74.1 .27
Full feeding day, mean
⫾SD
29.8⫾19.7 27.0⫾18.7 .13
Weight gain at 14 d, mean⫾SD, g
53.4⫾53.1 52.7⫾59.8 .91
Weight gain at 28 d, mean⫾SD, g
103.5⫾70.0 103.4⫾78.8 .98
Weight gain at 42 d, mean⫾SD, g
131.9⫾89.7 139.7⫾85.6 .38
be attributable to the fact that the sickest infants were not enrolled in the study, because they either died before feeding or were not fed before 3 weeks of age. We conclude that probiotics containingB bifidumandL aci-dophilus, administered orally for 6 weeks, reduce the incidence of death or NEC for VLBW preterm infants.
ACKNOWLEDGMENTS
This study was supported by the National Science Coun-cil of Taiwan (grant NSC 94-2314-B-039-007) and was approved by the institutional review board of China Medical University Hospital (proposal DMR94-IRB-14). We thank our wonderful team members; this work would not have been possible without their active co-operation. We express sincere gratitude to Prof Wen-Miin Liang and Li-Na Liao in the Biostatistics Center, China Medical University, for their outstanding work on the statistical analyses. We also acknowledge the edito-rial assistance of Dr William Oh in the preparation of the manuscript.
REFERENCES
1. Hintz SR, Kendrick DE, Stoll BJ, et al. Neurodevelopmental and growth outcomes of extremely low birth weight infants after necrotizing enterocolitis.Pediatrics.2005;115(3):696 –703 2. Fanaroff AA, Hack M, Walsh MC. The NICHD Neonatal Re-search Network: changes in practice and outcomes during the first 15 years.Semin Perinatol.2003;27(4):281–287
3. Holman RC, Stoll BJ, Curns AT, Yorita KL, Steiner CA, Schon-berger LB. Necrotising enterocolitis hospitalisations among ne-onates in the United States.Paediatr Perinat Epidemiol. 2006; 20(6):498 –506
4. Lin PW, Stoll BJ. Necrotising enterocolitis. Lancet. 2006; 368(9543):1271–1283
5. Caplan MS, Simon D, Jilling T. The role of PAF, TLR, and the inflammatory response in neonatal necrotizing enterocolitis.
Semin Pediatr Surg.2005;14(3):145–151
6. Viscardi RM, Lyon NH, Sun CC, Hebel JR, Hasday JD. Inflam-matory cytokine mRNAs in surgical specimens of necrotizing enterocolitis and normal newborn intestine.Pediatr Pathol Lab Med.1997;17(4):547–559
7. Sharma R, Tepas JJ III, Hudak ML, et al. Neonatal gut barrier and multiple organ failure: role of endotoxin and proinflam-matory cytokines in sepsis and necrotizing enterocolitis.J Pe-diatr Surg.2007;42(3):454 – 461
8. Halpern MD, Holubec H, Dominguez JA, et al. Up-regulation of IL-18 and IL-12 in the ileum of neonatal rats with necrotizing enterocolitis.Pediatr Res.2002;51(6):733–739
9. Claud EC, Walker WA. Hypothesis: inappropriate colonization of the premature intestine can cause neonatal necrotizing en-terocolitis.FASEB J.2001;15(8):1398 –1403
10. Markel TA, Crisostomo PR, Wairiuko GM, et al. Cytokines in necrotizing enterocolitis.Shock.2006;25(4):329 –337
11. Walker WA. Development of the intestinal mucosal barrier.
J Pediatr Gastroenterol Nutr.2002;34(suppl 1):S33–S39 12. Forchielli ML, Walker WA. The effect of protective nutrients on
mucosal defense in the immature intestine.Acta Paediatr Suppl.
2005;94(449):74 – 83
13. Neish AS, Gewirtz AT, Zeng H, et al. Prokaryotic regulation of epithelial responses by inhibition of IB-␣ubiquitination. Sci-ence.2000;289(5484):1560 –1563
14. Collier-Hyams LS, Sloane V, Batten BC, Neish AS. Cutting edge: bacterial modulation of epithelial signaling via changes in neddylation of cullin-1.J Immunol.2005;175(7):4194 – 4198
15. Bin-Nun A, Bromiker R, Wilschanski M, et al. Oral probiotics prevent necrotizing enterocolitis in very low birth weight ne-onates.J Pediatr.2005;147(2):192–196
16. Lin CH, Su BH, Chen AC, et al. Oral probiotics reduce the incidence and severity of necrotizing enterocolitis in very low birth weight infants.Pediatrics.2005;115(1):1– 4
17. Schanler RJ. Probiotics and necrotising enterocolitis in prema-ture infants. Arch Dis Child Fetal Neonatal Ed. 2006;91(6): F395–F397
18. Deshpande G, Rao S, Patole S. Probiotics for prevention of necrotising enterocolitis in preterm neonates with very low birthweight: a systematic review of randomised controlled tri-als.Lancet.2007;369(9573):1614 –1620
19. Caicedo RA, Schanler RJ, Li N, et al. The developing intestinal ecosystem: implications for the neonate. Pediatr Res. 2005; 58(4):625– 628
20. Neu J, Douglas-Escobar M, Lopez M. Microbes and the devel-oping gastrointestinal tract. Nutr Clin Pract. 2007;22(2): 174 –182
21. Pietzak M. Bacterial colonization of the neonatal gut.J Pediatr Gastroenterol Nutr.2004;38(4):389 –391
22. Wilson R, Kanto WP Jr, McCarthy BJ, Burton A, Lewin P, Feldman RA. Age at onset of necrotizing enterocolitis: an epi-demiologic analysis.Pediatr Res.1982;16(1):82– 85
23. Lee YJ, Yu WK, Heo TR. Identification and screening for anti-microbial activity againstClostridium difficileof Bifidobacterium
andLactobacillusspecies isolated from healthy infant faeces.Int J Antimicrob Agents.2003;21(4):340 –346
24. Bell MJ, Ternberg JL, Feigin RD, et al. Neonatal necrotizing enterocolitis: therapeutic decisions based upon clinical staging.
Ann Surg.1978;187(1):1–7
25. Cass DL, Wesson DE. Advances in fetal and neonatal surgery for gastrointestinal anomalies and disease.Clin Perinatol.2002; 29(1):1–21
26. Vaughan EE, de Vries MC, Zoetendal EG, Ben-Amor K, Ak-kermans AD, de Vos WM. The intestinal LABs.Antonie Van Leeuwenhoek. 2002;82:341–352
27. Favier CF, Vaughan EE, De Vos WM, Akkermans AD. Molec-ular monitoring of succession of bacterial communities in hu-man neonates.Appl Environ Microbiol.2002;68:219 –226. 28. Schell MA, Karmirantzou M, Snel B, Vilanova D, Berger B,
Pessi G. The genome sequence of Bifidobacterium longum reflects its adaptation to the human gastrointestinal tract.Proc Natl Acad Sci USA.2002;99:14422–14427
29. Benno Y, He F, Hosoda M, Hashimoto H, Kojima T, Yamazaki K. Effects of Lactobacillus GG yogurt on human intestinal microecology in Japanese subjects.Nutrition Today. 1996;31: 9 –11
30. Gewolb IH, Schwalbe RS, Taciak VL, Harrison TS, Panigrahi P. Stool microflora in extremely low birthweight infants.Arch Dis Child Fetal Neonatal Ed.1999;80(3):F167–F173
31. Shah U, Walker WA. Adverse host responses to bacterial toxins in human infants.J Nutr.2000;130(2S suppl):420S– 425S 32. Dai D, Walker WA. Role of bacterial colonization in neonatal
necrotizing enterocolitis and its prevention. Acta Paeditr Sin.
1998;39(6):357–365
33. Caplan MS, Miller-Catchpole R, Kaup S, et al. Bifidobacterial supplementation reduces the incidence of necrotizing entero-colitis in a neonatal rat model.Gastroenterology.1999;117(3): 577–583
34. Butel MJ, Roland N, Hibert A, et al. Clostridial pathogenicity in experimental necrotising enterocolitis in gnotobiotic quails and protective role of bifidobacteria.J Med Microbiol.1998;47(5): 391–399
of intestinal flora development in breast-fed and formula-fed infants by using molecular identification and detection meth-ods.J Pediatr Gastroenterol Nutr.2000;30(1):61– 67
37. Butel MJ, Suau A, Campeotto F, et al. Conditions of bifidobac-terial colonization in preterm infants: a prospective analysis.
J Pediatr Gastroenterol Nutr.2007;44(5):577–582
38. Favier CF, Vaughan EE, De Vos WM, Akkermans AD. Molec-ular monitoring of succession of bacterial communities in hu-man neonates.Appl Environ Microbiol.2002;68(1):219 –226 39. Riedel CU, Foata F, Philippe D, et al. Anti-inflammatory effects
of bifidobacteria by inhibition of LPS-induced NF-B activa-tion.World J Gastroenterol.2006;12(23):3729 –3735
40. Fituch CC, Palkowetz KH, Goldman AS, et al. Concentrations of IL-10 in preterm human milk and in milk from mothers of infants with necrotizing enterocolitis. Acta Paediatr. 2004; 93(11):1496 –1500
41. Timmerman HM, Niers LE, Ridwan BU, et al. Design of a multispecies probiotic mixture to prevent infectious compli-cations in critically ill patients. Clin Nutr. 2007;26(4): 450 – 459
42. Bourlioux P, Koletzko B, Guarner F. The intestine and its microflora are partners for the protection of the host: report on the Danone Symposium on “The Intelligent Intestine.”Am J Clin Nutr. 2003;78(4):675– 683
43. Rayes N, Seehofer D, Theruvath T, et al. Supply of pre- and
probiotics reduces bacterial infection rates after liver transplantation: a randomized double blind trial.Am J Trans-plant.2005;5(1):125–130
44. Matsumoto T, Ishikawa H, Tateda K, Yaeshima T, Ishibashi N, Yamaguchi K. Oral administration of Bifidobacterium longum
prevents gut-derived Pseudomonas aeruginosa sepsis in mice.
J Appl Microbiol.2008;104(3):672– 680
45. Stoll BJ, Hansen N. Infections in VLBW infants: studies from the NICHD Neonatal Research Network.Semin Perinatol.2003; 27(4):293–301
46. Salminen MK, Rautelin H, Tynkkynen S, et al. Lactobacillus
bacteremia, clinical significance, and patient outcome, with special focus on probiotic L. rhamnosus GG. Clin Infect Dis.
2004;38(1):62– 69
47. Sullivan A, Nord CE. Probiotic lactobacilli and bacteraemia in Stockholm.Scand J Infect Dis.2006;38(5):327–331
48. Presterl E, Kneifel W, Mayer HK, Zehetgruber M, Makristathis A, Graninger W. Endocarditis byLactobacillus rhamnosusdue to yogurt ingestion?Scand J Infect Dis.2001;33(9):710 –714 49. Wagner RD, Warner T, Roberts L, et al. Colonization of
con-genitally immunodeficient mice with probiotic bacteria.Infect Immun.1997;65(8):3345–3351
50. Kunz AN, Noel JM, Fairchok MP. Two cases of Lactobacillus
bacteremia during probiotic treatment of short gut syndrome.
J Pediatr Gastroenterol Nutr.2004;38(4):457– 458
TRYING TO SAVE BY INCREASING DOCTORS’ FEES
“Cutting health costs by paying doctors more? That is the premise of exper-iments underway by federal and state government agencies and many insur-ers around the country. The idea is that by paying family physicians, inter-nists and pediatricians to devote more time and attention to their patients, insurers and patients can save thousands of dollars downstream on unnec-essary tests, visits to expensive specialists and avoidable trips to the hospital. Nationally, Medicare and commercial insurers pay an average of only about $60 a visit to the office of a primary-care doctor and rarely if ever pay for telephone or e-mail consultations. Many health policy experts say the pay-ments are not enough to let the doctors spend more than a few minutes with each patient. Richard Baron is one of more than 100 physicians in metropol-itan Philadelphia taking part in the experiment, which is being conducted jointly by some of the region’s largest insurers. Dr Baron still gets a fee of only about $64 for each office visit. But his five-doctor group will also receive $200 000 to $300 000 this year beyond their regular fees to keep better track of their 8400 patients. ‘We are trying to do more e-mail care and telephone care, which we haven’t been paid for in the past,’ Dr Baron said. Insurers are conducting similar pilot projects in at least a half-dozen states, in experiments involving thousands of doctors and nearly two million patients.” Such fea-tures add up to a model of primary care that proponents refer to as providing people with a ‘medical home’—a base where doctors, staff and patients pull together as one big health-care family. Or at least that is the ideal. ‘It’s the latest new, new thing—testing whether medical homes can be a vehicle for pulling America upwards from the grossly inefficient swamp in which our health system is currently mired,’ said Dr Arnold Milstein, a senior consultant at Mercer who is also a member of the Medicare Payment Advisory Com-mission, an independent Congressional agency.
DOI: 10.1542/peds.2007-3007
2008;122;693
Pediatrics
Rey-in Lien, Lon-Yen Tsao, Chao-Huei Chen and Bai-Horng Su
Hung-Chih Lin, Chyong-Hsin Hsu, Hsiu-Lin Chen, Mei-Yung Chung, Jen-Fu Hsu,
Preterm Infants: A Multicenter, Randomized, Controlled Trial
Oral Probiotics Prevent Necrotizing Enterocolitis in Very Low Birth Weight
Services
Updated Information &
http://pediatrics.aappublications.org/content/122/4/693
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/122/4/693#BIBL
This article cites 50 articles, 11 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-3007
2008;122;693
Pediatrics
Rey-in Lien, Lon-Yen Tsao, Chao-Huei Chen and Bai-Horng Su
Hung-Chih Lin, Chyong-Hsin Hsu, Hsiu-Lin Chen, Mei-Yung Chung, Jen-Fu Hsu,
Preterm Infants: A Multicenter, Randomized, Controlled Trial
Oral Probiotics Prevent Necrotizing Enterocolitis in Very Low Birth Weight
http://pediatrics.aappublications.org/content/122/4/693
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.