in Children With Perthes Disease
WHAT’S KNOWN ON THIS SUBJECT: The causes of Perthes disease are unknown. There is considerable evidence that the disease has a vascular mechanism, although the nature of this is unknown. There is some suggestion that affected individuals may have a heightened cardiovascular risk in adulthood.
WHAT THIS STUDY ADDS: Children with Perthes disease have reduced vascular caliber, which is independent of body height, and abnormal functional vascular measures. Thesefindings may be important in the mechanism of disease and may have implications on long-term vascular morbidity.
abstract
BACKGROUND AND OBJECTIVES:Perthes disease is a childhood pre-cipitant to osteoarthritis of the hip, for which the etiology and mech-anism are unknown. There is mounting evidence to suggest a vascular insult is responsible for disease, and it is suggested that this may have long-term implications for the vascular health of affected individuals. This study sought to use ultrasound measures to investigate vascular structure and function in children affected by Perthes disease.
METHODS: This case control study encompassed 149 cases and 146 controls, frequency matched for age and gender. Endothelial function was measured by using the technique offlow-mediated dilation of the brachial artery, and alterations in arterial flow were recorded in response to an ischemic stimulus.
RESULTS:There was a significant structural alteration in the vascula-ture among individuals with Perthes disease (resting brachial artery diameter (cases 2.97 mm versus controls 3.11 mm;P = .01), which remained even after adjusting for height. In addition, there was a no-table reduction in blood velocity (cases 33.84 cm/s versus controls 37.83 cm/s; P = .01) and blood flow (cases 149.82 mL/min versus controls 184.67 mL/min; P = .001), which was independent of baseline arterial size. There was no evidence to suggest that fl ow-mediated dilation of the brachial artery was impaired among affected individuals (P= .71).
CONCLUSIONS:Children with Perthes disease exhibit small artery cal-iber and reduced function, which is independent of body composition. These data imply that that Perthes disease may reflect a wider vascular phenomenon that could have long-term implications for the vascular health of affected individuals.Pediatrics2012;130:e126–e131
AUTHORS:Daniel C. Perry, MB, ChB(Hons), MRCS(Eng), PhD,a,b
Daniel J. Green, BSc, MSc, PhD,c,dColin E. Bruce, MB, ChB,
FRCS (Orth),bDaniel Pope, BSc, MSc, PhD,aPeter Dangerfield,
MD, FHEA,eMary Jane Platt, MD, MPH, FRCPH,fAndrew J. Hall,
MB, BS, MSc, PhD, FRCP, FFPH, FMedSci,gand Helen Jones,
BSc, PhDc
aDepartment of Public Health and Policy, University of Liverpool,
Liverpool, United Kingdom;bDepartment of Children’s
Orthopaedic Surgery, Alder Hey Hospital, Liverpool, United Kingdom;cResearch Institute for Sport and Exercise Sciences,
Liverpool John Moores University, Liverpool, United Kingdom;
dSchool of Sport Science, Exercise and Health, The University of
Western Australia, Crawley, Australia;eSchool of Medicine,
University of Liverpool, Liverpool, United Kingdom;fNorwich
Medical School, University of East Anglia, Norwich, United Kingdom; andgFaculty of Epidemiology and Population Health,
London School of Hygiene and Tropical Medicine, London, United Kingdom
KEY WORDS
Legg-Perthes disease, etiology, risk factors
ABBREVIATIONS
FMD—flow-mediated dilation MED—multiple epiphyseal dysplasia ROI—region of interest
All authors were involved in the design, data interpretation, drafting, andfinal approval of this paper. The data analysis was conducted by Drs Perry and Jones.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-3269
doi:10.1542/peds.2011-3269
Accepted for publication Mar 8, 2012
Address correspondence to Daniel C. Perry, MB, ChB (Hons), MRCS (Eng), PhD, Honorary Lecturer in Child Health, Department of Children’s Orthopaedic Surgery, Alder Hey Children’s Hospital, Liverpool, L12 2AP, United Kingdom. E-mail: danperry@doctors. org.uk
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURES:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
Perthes disease (juvenile idiopathic osteonecrosis of the femoral head) affects∼1 in 850 children in Northern Europe and the United States.1The
dis-ease manifests through hip pain with lim-ited movements and presents a marked physical and psychological burden in childhood. The disease often alters the shape of the hip, which may accelerate osteoarthritic changes,2and is a
com-mon precipitant for joint replacement in early adult life.
The mechanism by which the avascular necrosis develops is unknown. It is hy-pothesized that there is diminished blood supply via the lateral ascending vessel to the epiphysis.3Many observers
have suggested that this may arise through a thrombophilic process, but a systematic review of coagulopathies among 475 cases concluded that there were no significant differences in an-tithrombin activity, protein S or C ac-tivity, or antiphospholipid antibodies.4
The relationship with the Factor V Leiden mutation is uncertain; however, it appears unlikely that there is a major thrombophilic association.
More recently, it has been suggested that abnormalities in vascular struc-ture and function may be the mecha-nism by which the disease develops, with particular interest focused toward the possibility of endothelial dysfunc-tion.5–7The endothelium forms a large
endocrine organ, the function of which is to regulate vascular tone, platelet aggregation, coagulation, and fi bri-nolysis. Endothelial dysfunction may precipitate inflammation, thrombosis, vasoconstriction, and atherosclerotic plaque formation.8 Endothelial
dys-function in children and young adults has been demonstrated in relation to passive smoking, short stature, and low birth weight.9,10Each of these has
similarly been associated with Perthes disease.5,11–13
The dilator response of a conduit artery to increased flow after a period of
imposed distal limb ischemia is a com-mon measure of endothelial function, which is termedflow-mediated dilation (FMD).14 FMD is a noninvasive and
widely accepted measure that is com-monly used in research as an inde-pendent predictor of cardiovascular events.15–17Adults who were affected
by Perthes disease in childhood are demonstrated to have a greater risk of premature cardiovascular disease in adulthood, therefore adding support to an abnormality of vascular function.18
Recently, it has been proposed that hy-peremic blood flow responses to a period of ischemia also predict cardio-vascular outcomes.19,20These
respon-ses reflect small-artery dilator function, rather than that of the larger conduit arteries.21
Despite previous suggestions that the mechanism responsible for Perthes may be related to vascular dysfunction, no previous study has investigated large- or small-artery functional respon-ses in children with Perthes disease. We hypothesized that FMD and hyperemic responses to an ischemic stimulus would be abnormal in children with Perthes disease.
METHODS
Participants
A case-control study was undertaken at Alder Hey Children’s Hospital, Liverpool. Cases comprised patients drawn from the Merseyside Perthes register and recruited at a routine hospital atten-dance. All patients were aged 5 to 16 years with a confirmed diagnosis of Perthes disease. In each case the di-agnosis was verified by a consultant pediatric radiologist and consultant pediatric orthopedic surgeon based upon the radiographic appearance and clinical features. Bilateral synchro-nous disease necessitated a skeletal survey to exclude a multiple epiphyseal dysplasia (MED). Cases of MED, cerebral palsy, and developmental hip dysplasia
were excluded owing to their known independent association with avascu-lar necrosis of the hip. No cases were actively immobilized, and all were at least 4 months after the last surgical intervention.
Controls were an age- and gender-stratified sample of the orthopedic out-patient population, frequency matched on a 1:1 basis. Age matching occurred within 2 groups: 5 to 10 years old, 11 to 16 years old. Controls were similarly at-tending Alder Hey Hospital and were drawn from a number of children’s or-thopedic outpatient clinics. The clinics sampled were knee clinic, general or-thopedic clinic, normal variants clinic, and trauma clinic. Any controls with a restriction in hip movement, unless a clear alternative diagnosis was apparent, were excluded. On each sampling day, all eligible controls were approached for inclusion. Controls with MED, cere-bral palsy, and developmental hip dys-plasia were excluded, as were patients actively immobilized (irrespective of site of pathology) and those within 4 months of surgery.
Research Design
Parents and children were invited to attend a research clinic, at which vascular parameters and basic anthropometrics (height/ weight) were measured and demographic details recorded. Endo-thelial function was measured by using the technique of FMD. This is a non-invasive measure of endothelial func-tion that sonographically measures the degree of brachial artery dilation in response to a shear stimulus. The technique has widespread acceptance throughout the literature10,22and is
in-creasingly being used in childhood epi-demiologic studies.23
Measurement Procedures
FMD was recorded by using a stan-dardized technique.24 All scans were
recorded by a single trained observer
least 6 hours, with .8 hours absti-nence from caffeine. This occurred in a quiet room at room temperature with the child supine.
After 10 minutes of rest, a 10-MHz mul-tifrequency linear array probe attached to a high-resolution ultrasound ma-chine (Terason 3000) was used to image the brachial artery on the right arm. The artery was scanned in longitudinal section above the elbow. Depth and gain settings were adjusted to optimize the lumen/ arterial wall interface. Once a satisfactory transducer position was established, the position was main-tained for the duration of the study. Continuous Doppler velocity assess-ment was similarly obtained at the lowest possible insonation angle. Base-line scans for the assessment of resting vessel diameter andflow were recor-ded. An occluding cuff was then infl a-ted to 200 mm Hg for 5 minutes around the forearm. Diameter andflow record-ings were resumed 30 seconds before cuff deflation and continued for 3 minutes thereafter.
Custom-designed edge-detection and wall-tracking software (LabVIEW 6.02, National Instruments) was used to determine the vascular parameters, which is largely independent of any investigator bias.25The initial phase of
the image analysis involved the iden-tification of regions of interest (ROIs). These ROIs allowed automated cali-bration of diameters on the vascular image and velocities on the Doppler strip. A ROI was drawn around the op-timal area of the vascular image, within this ROI a pixel-density algorithm auto-matically identified the angle-corrected near and far wall e-lines for every pixel column within the ROI. Typical vessel ROIs contain∼200–300 diameter meas-urements per frame, the average of which was calculated and stored. This process occurs at 30 frames per second.
siderably more repeatable (coefficient of variation = 6.7%) than manual meth-ods and are associated with less ob-server error.25The resultant graphical
output automatically calculates the FMD, after indicating the point of cuff deflation whereby the arterialflow and shear rise rapidly.
Statistical Analysis
Analysis was conducted by using uni-variate and biuni-variate analyses, and then a multivariate model. Logistic re-gression was conducted universally adjusting for age (continuous variable) and gender (categorical variable). Ad-ditional adjustments were made for each of the confounding variables that arose, and confounders were retained within the model if their inclusion pro-duced a 10% measured change in effect size. All analyses were conducted by using Stata 10.0 (StataCorp, College Station, TX). P values of ,.05 were considered significant.
RESULTS
One hundred forty-nine patients and 146 controls were recruited to take part. Thirty-two children (17 patients and 15 controls) were unable to tolerate the examination or scans were of insuffi -cient quality to allow vascular measures
Table 1. There was no difference in the age or gender of either group.
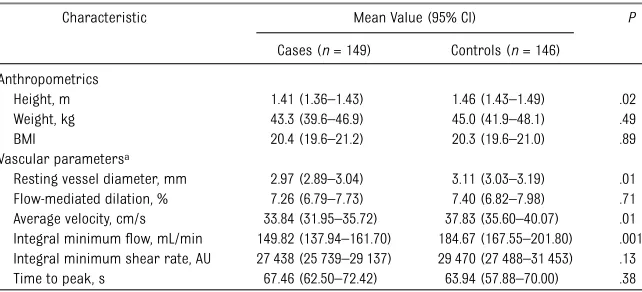
Bivariate analyses revealed that the mean height of individuals with Perthes disease was 5 cm less than controls (P= .02), although weight and BMI were not different between groups (Table 1). The vascular parameters demonstrated a reduced brachial diameter (cases 2.97 mm versus controls 3.11 mm;P= .01), reduced blood velocity (cases 33.84 cm/s versus controls 37.83 cm/s;P= .01) and reduced blood flow (cases 149.82 mL/min versus controls 184.67 mL/min; P = .001). There was no dif-ference in the FMD response (P= .71). After adjusting for age and gender, each of these associations remained (Table 2, adjustment 1).
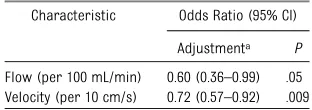
FMD was negatively correlated with age, height, and resting brachial artery di-ameter. Bloodflow was positively cor-related with age, height, weight, BMI, and resting brachial diameter. Blood velocity was positively correlated with age and height. Adjusting for each of the confounding variables revealed that only the adjustment for height had any notable effect on any of the vascular predictor variables (Table 2, adjust-ment 2). Even after adjusting for rest-ing brachial artery size, a reduction in velocity andflow persisted (Table 3).
TABLE 1 Anthropometric and Vascular Measures in the Study Group
Characteristic Mean Value (95% CI) P
Cases (n= 149) Controls (n= 146) Anthropometrics
Height, m 1.41 (1.36–1.43) 1.46 (1.43–1.49) .02 Weight, kg 43.3 (39.6–46.9) 45.0 (41.9–48.1) .49 BMI 20.4 (19.6–21.2) 20.3 (19.6–21.0) .89 Vascular parametersa
Resting vessel diameter, mm 2.97 (2.89–3.04) 3.11 (3.03–3.19) .01 Flow-mediated dilation, % 7.26 (6.79–7.73) 7.40 (6.82–7.98) .71 Average velocity, cm/s 33.84 (31.95–35.72) 37.83 (35.60–40.07) .01 Integral minimumflow, mL/min 149.82 (137.94–161.70) 184.67 (167.55–201.80) .001 Integral minimum shear rate, AU 27 438 (25 739–29 137) 29 470 (27 488–31 453) .13 Time to peak, s 67.46 (62.50–72.42) 63.94 (57.88–70.00) .38
CI, confidence interval.
DISCUSSION
The principalfindings of this study are that children with Perthes disease ex-hibit smaller conduit arterial caliber and impaired hyperemic responses to an ischemic stimulus, a surrogate marker of small-artery function, in comparison with controls. Furthermore, we observed no apparent difference in the conduit artery FMD response. It is well established that a growth abnor-mality exists in Perthes disease, with distal anatomic structures (ie, the hands and feet) small relative to trunk size; a growth pattern described as rostral sparing.12,26 It therefore appears that
this is reflected in the vasculature, be-cause the arterial caliber was dispro-portionately small after correcting for height. Nevertheless, even after adjust-ing for arterial size, affected children had a significant reduction in bloodflow, suggesting that a functional impairment occurs in addition to any phenomena pertaining to arterial size.
This is thefirst study that has exam-ined arterial function in children with Perthes disease. It has been suggested that the mechanism for Perthes dis-ease is vascular in origin, based upon pathologic and clinical evidence, along with the unusual anatomy of the vas-culature to the infant femoral epiph-ysis.3,27It has been demonstrated that
between 3 and 7 years, the blood supply to the epiphysis is almost universally dependent on a single artery, the lateral ascending artery.3,27Pathologic studies
of femoral heads affected by Perthes disease have demonstrated changes that are consistent with an avascular process.28–30 Likewise, the clinical
ap-pearance of disease supports a vascu-lar mechanism, because the anterior aspect of the head, which is the furthest point from the vascular origin, is uni-versally affected.31Ourfindings support
this mechanism by demonstrating de-creased vasodilator capacity in small arteries that control bloodflow respon-ses, after a period of ischemia. Such arteries are likely to be of similar caliber to those implicated in Perthes disease.
The primary objective of this study was to assess FMD responses and investi-gate the hypothesis that endothelial dysfunction may be apparent in sub-jects with Perthes disease. Previous researchers have suggested abnor-malities in endothelial function based
on the presence of biochemical param-eters and risk factors in Perthes disease that are known to impair endothelial function,5–7yet no studies to date have
sought to assess endothelial function directly. Our finding, that blood flow was impaired, despite normal conduit artery dilator function, suggests that vascular dysfunction in smaller arteries may precede that in larger vessels. This abnormality of the distal vascular bed increases peripheral resistance and thus reduces blood velocity and flow. This is thefirst study, to our knowledge, to demonstrate decreased arterial cali-ber and reduced bloodflow in Perthes disease.
We acknowledge that the findings of the current study require cautious in-terpretation; nevertheless, ourfindings raise the hypothesis that Perthes dis-ease may reflect a wider vascular phenomenon that may manifest as cardiovascular disease in later life. In support of our findings, a recent study using the common animal model of Perthes disease (the stroke-prone spontaneously hypertensive rate) has demonstrated arterial narrowing, and arthrosclerotic-like hypertrophy of the vasculature to the immature hip among these rats.32The stroke prone
spontaneously hypertensive rate rat is also a common animal model of arte-riosclerosis, hypertension, and cere-brovascular disease and is known to develop spontaneous femoral head is-chemia in infancy in∼50% of cases.33
Furthermore, abnormal hyperemic re-sponses, such as those observed in the current study, have recently been shown to be associated with cardiovascular disease in adults.19,20Likewise, reduced
arterial size is believed to be a key fac-tor contributing to the higher cardio-vascular risk in individuals of short stature.34
Long-term cardiovascular consequences of Perthes disease have been identified by 1 study that demonstrated greater TABLE 2 Multivariable Adjustment of Each of the Parameters
Characteristic Odds Ratio (95% CI)
Adjustment 1a P Adjustment 2b P Anthropometrics
Height, cm 0.95 (0.92–0.98) .001 — —
Weight, kg 1.00 (0.98–1.02) .80 — —
BMI 1.02 (0.97–1.08) .43 — —
Vascular parametersc
Flow-mediated dilation (%) 0.98 (0.91–1.06) .65 0.97 (0.89–1.05) .46 Resting vessel diameter (mm) 0.30 (0.14–0.66) .003 0.38 (0.17–0.86) .02 Flow (per 100 mL/min) 0.51 (0.34–0.76) .001 0.53 (0.35–0.81) .003 Velocity (per 10 cm/s) 0.72 (0.57–0.91) .005 0.71 (0.56–0.90) .005
CI, confidence interval.
aAdjustment 1: adjusted for age and gender. bAdjustment 2: adjusted for age, gender, and height. cVascular measures available in 132 cases and 129 controls.
TABLE 3 Vascular Parameters Adjusted for Arterial Size
Characteristic Odds Ratio (95% CI)
Adjustmenta P Flow (per 100 mL/min) 0.60 (0.36–0.99) .05 Velocity (per 10 cm/s) 0.72 (0.57–0.92) .009
CI, confidence interval.
aAdjusted for age, gender, height, and resting vessel
di-ameter (millimeters).
based on the Swedish inpatient regis-ter, demonstrated a higher frequency of ischemic heart disease (hazard ratio 2.69 [95% confidence interval 1.20– 6.03]) and hypertension (hazard ratio 2.97 [95% confidence interval 1.87– 4.72]), after adjusting for socioeco-nomic deprivation. The study, published in 2010, recruited individuals diag-nosed between 1965 and 2005, and, therefore, the majority of individuals are relatively young to consider car-diovascular disease. There are no studies to date that detail the cause
historic cohort were identified addi-tional research in this area would be invaluable.
In the current study the control group was formed from a hospital population. The advantage of this group was that it overcomes selection bias related to access to health care. Yet, at the same time, it introduces the assumption that a group of hospital patients are rep-resentative of the population at large. To help overcome this, a number of hospital clinics formed the control group, therefore attempting to prevent
variable. Any bias attributable to hospital populations would be likely to move the odds ratio toward the null; there-fore, the observed differences may be underestimates.
In summary, the novel finding of this study was the reduction in small artery caliber and function in children with Perthes disease, which appeared inde-pendent of body size. This may be an im-portant finding both in terms of the etiology of Perthes disease and may have long term consequences for vascular health.
REFERENCES
1. Perry DC, Machin DMG, Pope D, et al. Racial and geographic factors in the incidence of Legg-Calvé-Perthes’disease: a systematic review. Am J Epidemiol. 2012;175(3):159– 166
2. Stulberg SD, Cooperman DR, Wallensten R. The natural history of Legg-Calvé-Perthes disease.J Bone Joint Surg Am. 1981;63(7): 1095–1108
3. Chung SM. The arterial supply of the de-veloping proximal end of the human femur.
J Bone Joint Surg Am. 1976;58(7):961–970
4. Kenet G, Ezra E, Wientroub S, et al. Perthes’ disease and the search for genetic asso-ciations: collagen mutations, Gaucher’s disease and thrombophilia. J Bone Joint Surg Br. 2008;90(11):1507–1511
5. Bahmanyar S, Montgomery SM, Weiss RJ, Ekbom A. Maternal smoking during preg-nancy, other prenatal and perinatal factors, and the risk of Legg-Calvé-Perthes disease.
Pediatrics. 2008;122(2). Available at: www. pediatrics.org/cgi/content/full/122/2/e459
6. Séguin C, Kassis J, Busque L, Bestawros A, Theodoropoulos J, Alonso ML, Harvey EJ. Non-traumatic necrosis of bone (osteonec-rosis) is associated with endothelial cell activation but not thrombophilia. Rheuma-tology (Oxford). 2008;47(8):1151–1155
7. Aksoy MC, Aksoy DY, Haznedaroglu IC, Sayinalp N, Kirazli S, Alpaslan M. Thrombomodulin and GFC levels in Legg-Calve-Perthes dis-ease.Hematology. 2008;13(6):324–328
8. Shah PK. New insights into the pathogen-esis and prevention of acute coronary syndromes. Am J Cardiol. 1997;79(12B): 17–23
9. Kallio K, Jokinen E, Raitakari OT, et al. To-bacco smoke exposure is associated with attenuated endothelial function in 11-year-old healthy children.Circulation. 2007;115 (25):3205–3212
10. Celermajer DS, Adams MR, Clarkson P, et al. Passive smoking and impaired endothelium-dependent arterial dilatation in healthy young adults. N Engl J Med. 1996;334(3):150–154
11. Molloy MK, Macmahon B. Birth weight and Legg-Perthes disease. J Bone Joint Surg Am. 1967;49(3):498–506
12. Burwell RG, Dangerfield PH, Hall DJ, Vernon CL, Harrison MH. Perthes’disease. An an-thropometric study revealing impaired and disproportionate growth.J Bone Joint Surg Br. 1978;60-B(4):461–477
13. García Mata S, Ardanaz Aicua E, Hidalgo Ovejero A, Martinez Grande M. Legg-Calvé-Perthes disease and passive smoking.J Pediatr Orthop. 2000;20(3):326–330
14. Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis.Lancet. 1992;340(8828): 1111–1115
15. Green DJ, Jones H, Thijssen D, Cable NT, Atkinson G. Flow-mediated dilation and cardiovascular event prediction: does nitric oxide matter?Hypertension. 2011;57(3):363– 369
16. Yeboah J, Crouse JR, Hsu FC, Burke GL, Herrington DM. Brachialflow-mediated di-lation predicts incident cardiovascular events in older adults: the Cardiovascular Health Study.Circulation. 2007;115(18):2390–2397
17. Yeboah J, Folsom AR, Burke GL, et al. Pre-dictive value of brachialflow-mediated di-lation for incident cardiovascular events in a population-based study: the multi-ethnic study of atherosclerosis.Circulation. 2009; 120(6):502–509
18. Hailer YD, Montgomery SM, Ekbom A, Nilsson OS, Bahmanyar S. Legg-Calve-Perthes dis-ease and risks for cardiovascular disdis-eases and blood diseases.Pediatrics. 2010;125(6). Available at: www.pediatrics.org/cgi/content/ full/125/6/e1308
19. Lind L, Berglund L, Larsson A, Sundström J. Endothelial function in resistance and con-duit arteries and 5-year risk of cardio-vascular disease.Circulation. 2011;123(14): 1545–1551
20. Anderson TJ, Charbonneau F, Title LM, et al. Microvascular function predicts cardiovas-cular events in primary prevention: long-term results from the Firefighters and Their En-dothelium (FATE) study.Circulation. 2011;123 (2):163–169
21. Naylor LH, Weisbrod CJ, O’Driscoll G, Green DJ. Measuring peripheral resistance and conduit arterial structure in humans using Doppler ultrasound.J Appl Physiol. 2005;98 (6):2311–2315
22. Tonetti MS, D’Aiuto F, Nibali L, et al. Treat-ment of periodontitis and endothelial function.N Engl J Med. 2007;356(9):911–920
24. Thijssen DHJ, Black MA, Pyke KE, et al. As-sessment of flow-mediated dilation in hu-mans: a methodological and physiological guideline.Am J Physiol Heart Circ Physiol.
2011;300(1):H2–H12
25. Woodman RJ, Playford DA, Watts GF, et al. Improved analysis of brachial artery ultra-sound using a novel edge-detection software system.J Appl Physiol. 2001;91(2):929–937
26. Hall AJ, Barker DJ, Dangerfield PH, Osmond C, Taylor JF. Small feet and Perthes’disease. A survey in Liverpool.J Bone Joint Surg Br. 1988;70(4):611–613
27. Trueta J. The normal vascular anatomy of
the human femoral head during growth.
J Bone Joint Surg Br. 1957;39-B(2):358– 394
28. Jensen OM, Lauritzen J. Legg-Calvé-Perthes’ disease. Morphological studies in two cases examined at necropsy.J Bone Joint Surg Br. 1976;58(3):332–338
29. McKibbin B, Rális Z. Pathological changes in a case of Perthes’disease. J Bone Joint Surg Br. 1974;56B(3):438–447
30. Catterall A, Pringle J, Byers PD, Fulford GE, Kemp HB. Perthes’disease: is the epiphysial infarction complete?J Bone Joint Surg Br. 1982;64(3):276–281
31. Catterall A. The natural history of Perthes’ disease.J Bone Joint Surg Br. 1971;53(1):37–53
32. Amemiya M, Yashiro T, Kikuchi M, Kouki T, Nakama S, Hoshino Y. Scanning and
trans-mission electron microscopic observation of femoral head feeding vessels in stroke-prone spontaneously hypertensive rats.
Med Mol Morphol. 2011;44(3):139–145
33. Naito S, Ito M, Sekine I, et al. Femoral head
necrosis and osteopenia in stroke-prone spontaneously hypertensive rats (SHRSPs).
Bone. 1993;14(5):745–753
34. Paajanen TA, Oksala NKJ, Kuukasjärvi P,
Karhunen PJ. Short stature is associated with coronary heart disease: a systematic review of the literature and a
DOI: 10.1542/peds.2011-3269 originally published online June 4, 2012;
2012;130;e126
Pediatrics
Mary Jane Platt, Andrew J. Hall and Helen Jones
Daniel C. Perry, Daniel J. Green, Colin E. Bruce, Daniel Pope, Peter Dangerfield,
Services
Updated Information &
http://pediatrics.aappublications.org/content/130/1/e126 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/130/1/e126#BIBL This article cites 34 articles, 10 of which you can access for free at:
Subspecialty Collections
oskeletal_disorders_sub
http://www.aappublications.org/cgi/collection/rheumatology:muscul
Rheumatology/Musculoskeletal Disorders following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2011-3269 originally published online June 4, 2012;
2012;130;e126
Pediatrics
Mary Jane Platt, Andrew J. Hall and Helen Jones
Daniel C. Perry, Daniel J. Green, Colin E. Bruce, Daniel Pope, Peter Dangerfield,
Disease
Abnormalities of Vascular Structure and Function in Children With Perthes
http://pediatrics.aappublications.org/content/130/1/e126
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.