R E S E A R C H
Open Access
The impact of internal displacement on
child mortality in post-earthquake Haiti: a
difference-in-differences analysis
Bradley Chen
1, Timothy J. Halliday
2,3,4and Victoria Y. Fan
5,6,7*Abstract
Background:The Haiti earthquake in 2010 resulted in 1.5 million internally displaced people (IDP), yet little is known about the impact of displacement on health. In this study, we estimate the impact of displacement on infant and child mortality and key health-behavior mechanisms.
Methods:We employ a difference-in-differences (DID) design with coarsened exact matching (CEM) to ensure
comparability among groups with different displacement status using the 2012 Haiti Demographic and Health Survey (DHS). The participants are 21,417 births reported by a nationally representative sample of 14,287 women aged 15–49. The main independent variables are household displacement status which includes households living in camps, IDP households (not in camps), and households not displaced. The main outcomes are infant and child mortality; health status (height-for-age, anemia); uptake of public health interventions (bed net use, spraying against mosquitoes, and vaccinations); and other conditions (hunger; cholera).
Results:Births from the camp households have higher infant mortality (OR = 2.34, 95 % CI 1.15 to 4.75) and
child mortality (OR = 2.34, 95 % CI 1.10 to 5.00) than those in non-camp IDP households following the earthquake. These odds are higher despite better access to food, water, bed net use, mosquito spraying, and vaccines among camp households.
Conclusions: IDP populations are heterogeneous and households that are displaced outside of camps may
be self-selected or self-insured. Meanwhile, even households not displaced by a disaster may face challenges in access to basic necessities and health services. Efforts are needed to identify vulnerable populations to provide targeted assistance in post-disaster relief.
Keywords: Infant mortality, Child mortality, Internally displaced people, Earthquake, Haiti
Background
On January 12, 2010, an earthquake of magnitude 7.0 struck Haiti near its capital. The earthquake killed a total of 222,600 people and displaced 1.5 million people (IDP) [1–3]. Poor physical infrastructure in Haiti has been cited as a primary cause of the excess number of deaths from injuries in the disaster’s immediate aftermath [4]. In the medium to long-term aftermath, however, poor public health infrastructure has been cited as a primary
cause of excess mortality [5], exacerbated by weak gov-ernance of the Haitian state [6]. Many IDP relocated to camps where anecdotal accounts described inadequate sanitation and security [3, 7]. Other IDP relocated to other areas in Haiti.
A few studies based on surveys have shown that the earthquakes had detrimental effects on household wel-fare. For example, Saint-Macary and Zanuso showed that households that were disproportionately impacted by the earthquakes had lower participation in labor markets [8]. They also found that households that received material assistance and/or moved to camps saw larger reductions in their assets. Similarly, Novella and Zanuso showed that households that were most affected by the * Correspondence:[email protected]
5
Department of Public Health Sciences & Epidemiology, University of Hawaii at Manoa, 1960 East–west Road, Biomed D204, Honolulu, HI, USA 6François-Xavier Bagnoud Center for Health and Human Rights, Harvard T.H.
Chan School of Public Health, 651 Huntington Ave, Boston, MA, USA Full list of author information is available at the end of the article
earthquakes were less likely to invest in the human cap-ital of their children [9].
In this paper, we contribute to this literature by estimat-ing the impact of displacement on mortality and key mechanisms explaining health status. We utilize the Demographic and Health Survey from Haiti for 2012. Spe-cifically, we estimate the causal impact of internal dis-placement to a camp or to a non-camp setting in another location within Haiti on child mortality. To address con-founding variables that are related to both our outcomes and displacement, we employ matching methods in con-junction with a difference-in-differences (DID) research design. We also examine associations of key mechanisms explaining health status such as anemia and stunting and utilization such as immunization and bed net use.
Methods
Data and research design
Our primary data source to evaluate the impact of in-ternal displacement on health is the fifth Demographic and Health Survey in Haiti [10]. The survey was con-ducted two years after the Haiti earthquake from January to June 2012. The information on children and birth his-tory came from a nationally representative sample of 14,287 women aged 15–49. The standard core DHS questionnaire collects rich information regarding hous-ing and socioeconomic status of households, health care utilization, and a number of maternal and child health outcomes including child mortality and biometric indicators.
As households and individuals that were internally dis-placed by the earthquake may be inherently different from those who were not, a simple comparison of health outcomes between the displaced and non-displaced would yield biased results which reflect the underlying drivers of their displacement. Therefore, we adopt a two-stage research design to enhance inter-group com-parability. First, using coarsened exact matching, we match individuals on a number of household character-istics that would affect their likelihood of being dis-placed by the earthquake. Second, we assess the impact of internal displacement on infant and child mortality among those coming from similar households. This min-imizes the effects from uncontrolled factors that affect both displacement and child health.
The 2012 Haiti survey asked questions especially per-taining to the earthquake. For instance, it asked individ-uals whether they “live in current housing during the earthquake,” based upon which we determined whether the individual had been displaced. In addition to stand-ard household covariates, questions on earthquake-related housing damage and mortality were also used to match and enhance the comparability of households.
The key health outcomes in our study are infant mortal-ity and under-five child mortalmortal-ity. The information is cap-tured through the full birth history recalled by the interviewed women and recorded in the survey. To pro-vide a more comprehensive picture of health status, health interventions and behaviors and to explore potential mechanisms affecting mortality, we further examined the relationship of displacement on key indicators of health status such as anthropometric growth (height for age) and anemia level (ordinal indicating severity), uptake of public health interventions of bed net use, spraying against mos-quitoes, and vaccination for BCG, measles, and DPT, as well as conditions of experiencing hunger in the last 4 weeks, and infection with cholera after October 2010.
Statistical analysis Matching
Our analyses begin by matching individuals on house-hold characteristics which delivers a similar likelihood of displacement across groups. We employ coarsened exact matching (CEM) for this purpose. Conceptually, CEM is similar to exact matching, but rather than requiring matched pairs to have exactly the same covariate values, they are matched by meaningful groups of covariate values [11]. We choose CEM over some “approximate matching” methods including propensity score matching (PSM) for several reasons. First, PSM may lead to a poorer imbalance on matched covariates, which in cer-tain circumstances may compromise the validity of the research design, perhaps, more so than non-matching [12, 13]. In contrast, CEM belongs to monotonic imbal-ance bounding matching methods, which bound the maximal imbalance by ex ante choice [14]. Second, for approximate matching methods such as PSM, in addition to the iterative process of estimation, matching and balance checking, its application also requires ana-lyses to be limited to“common support”so as to remove extrapolations beyond data limits and model depend-ency. CEM, on the other hand, limits the analyses to common empirical support automatically. There are a number of other benefits, described extensively in the literature [11, 13, 14].
We perform a logit regression to explore potential pre-dictors of camp residence and displacement. Based on the results, we match households on their likelihood of being displaced based upon the following characteristics: location of residence (region, urban/rural), household size, gender of household head, wealth index, and
whether the housing was damaged during the
earthquake.
Difference-in-differences (DID)
This allows us to employ a DID design to identify the births prior to the earthquake as controls. We use a logit model to analyze the impact of IDP on infant and child mortality, with the following specification:
Mit ¼αþβLociþγPostiþδðLociPosttÞ þθXi þηZiþεit
where, Mit refers to the logit of the probability of the
binary dependent variable indicating whether the live birth i born in year t died or not prior to 1 year of age (infant mortality), and whether a live birth died prior to reaching 5 years of age (child mortality). The variable Loci indicates the location of the household.
Households belong to one of the following three groups: camp resident, displaced but not residing in a camp, and non-displaced (in the same housing after earthquake). The variable Postt is a dummy variable indicating whether the birth was born after the earth-quake. The DID interaction term between Loc and
Post in our model and its coefficient, δ, captures the impact of displacement on infant and child mortality controlling for inherent mortality differences prior to the earthquake. The vector Xi is a set of household
characteristics, such as geographical location, house-hold size, househouse-hold head characteristics, wealth and land ownership, and damage by the earthquake. We
also control for a number of birth characteristics, Zi,
which include indicators for a twin birth, gender, birth order, and preceding interval in months. The household and birth characteristics adjust for any remaining imbalance resulting from the coarseness in our matching procedure.
We next explore the key mechanisms explaining child mortality by estimating a logit model in the cross section. All the dependent variables are binary except for the time to water source (continuous), and the severity of anemia (ordinal—non-anemic, mild, moderate and severe), for which an ordinary least squares model and an ordered logit model are estimated respectively. Once again, we control for household and child characteristics.
Results
Descriptive statistics
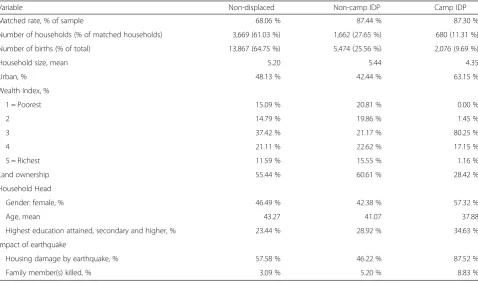
Our investigation is based upon the matched sample of 21,417 births from 6011 households. Descriptive statistics on these matched births by displacement status are presented in Table 1. Approximately one-third of the matched births were from displaced households, with 9.69 % residing in camps and the rest living elsewhere. Prior to matching, the three groups were different (descriptive statistics of the pre-matched sample are presented in Appendix 1); CEM
Table 1Descriptive statistics of household characteristics and earthquake damage among matched birth
Variable Non-displaced Non-camp IDP Camp IDP
Matched rate, % of sample 68.06 % 87.44 % 87.30 %
Number of households (% of matched households) 3,669 (61.03 %) 1,662 (27.65 %) 680 (11.31 %)
Number of births (% of total) 13,867 (64.75 %) 5,474 (25.56 %) 2,076 (9.69 %)
Household size, mean 5.20 5.44 4.35
Urban, % 48.13 % 42.44 % 63.15 %
Wealth Index, %
1 = Poorest 15.09 % 20.81 % 0.00 %
2 14.79 % 19.86 % 1.45 %
3 37.42 % 21.17 % 80.25 %
4 21.11 % 22.62 % 17.15 %
5 = Richest 11.59 % 15.55 % 1.16 %
Land ownership 55.44 % 60.61 % 28.42 %
Household Head
Gender: female, % 46.49 % 42.38 % 57.32 %
Age, mean 43.27 41.07 37.88
Highest education attained, secondary and higher, % 23.44 % 28.92 % 34.63 %
Impact of earthquake
Housing damage by earthquake, % 57.58 % 46.22 % 87.52 %
matching reduced this imbalance among households of different displacement statuses.
Model analyses
Point estimates from our model showed that households residing in camps experienced increased infant and child mortality relative to households that were not displaced, whereas households that were displaced but not re-located to camps saw reductions. We also found that in-fant and child mortality was the highest in the camps, despite higher access to key mechanisms of health status compared to households elsewhere.
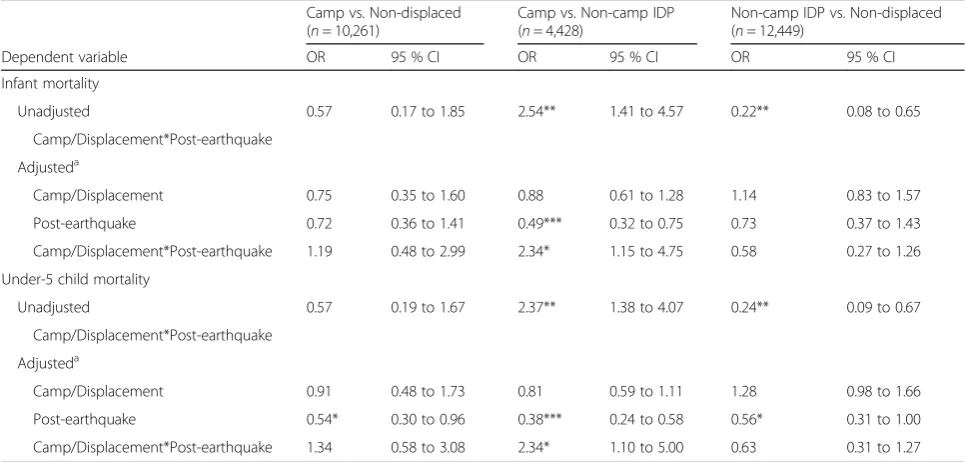
Impact of displacement on infant and child mortality
The results of the DID analyses are shown in Table 2. Across the three models, post-earthquake births were as-sociated with lower mortality compared to those pre-earthquake, e.g. the OR of post-earthquake was 0.49 (95 % CI 0.32 to 0.75) for infant mortality and 0.38 (95 % CI 0.24 to 0.58) for child mortality among IDP, in-dicating that child survival improved over time.
Our DID captured differential trends in mortality. The estimates of the interaction term between displace-ment and post-earthquake in the fully adjusted model showed that births in camp households had higher in-fant and child mortality than the two other groups. After the earthquake, the camp IDP births compared to non-camp IDP births had a high OR = 2.34 (95 % CI 1.15 to 4.75) of infant mortality and OR = 2.34 (95 % CI
1.10 to 5.00) of child mortality. Odds ratios of camp births compared to births in non-displaced households were 1.19 (95 % CI 0.48 to 2.99) in infant mortality and 1.34 (95 % CI 0.58 to 3.08) in child mortality. This is consistent with the finding that the births from non-camp IDP households had lower infant and child mor-tality than the non-displaced births. Among these two groups, displacement was associated with odds ratios of 0.58 (95 % CI 0.27 to 1.26) and 0.63 (95 % CI 0.31 to 1.27), for infant and child mortality, respectively. Simi-larly, the unadjusted model also shows that non-camp IDP births had the lowest infant and child mortality among the three groups and that there is no statistically significant difference in mortality between births from camp and non-displacement households.
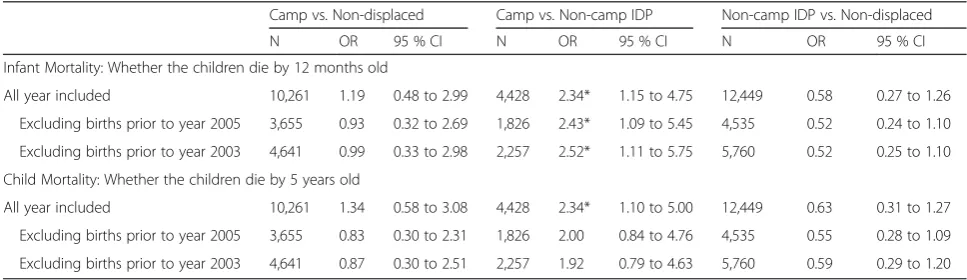
As a sensitivity analysis, we restricted the pre-earthquake control sample to those within 5 and 7 years before 2010 earthquake, respectively (Appendix 2). Estimates are consistent and showed that camp births had higher infant and child mortality than non-camp IDP births while their mortalities were not statistically different than those of the non-displaced ones.
Health status and utilization
To explore mechanisms through which displacement status affects infant and child mortality, we examined the associations between displacement status and indica-tors of health status and uptake of public health inter-ventions. Results are presented in Table 3.
Table 2Impact of displacement status on infant and child mortality
Camp vs. Non-displaced (n= 10,261)
Camp vs. Non-camp IDP (n= 4,428)
Non-camp IDP vs. Non-displaced (n= 12,449)
Dependent variable OR 95 % CI OR 95 % CI OR 95 % CI
Infant mortality
Unadjusted 0.57 0.17 to 1.85 2.54** 1.41 to 4.57 0.22** 0.08 to 0.65
Camp/Displacement*Post-earthquake
Adjusteda
Camp/Displacement 0.75 0.35 to 1.60 0.88 0.61 to 1.28 1.14 0.83 to 1.57
Post-earthquake 0.72 0.36 to 1.41 0.49*** 0.32 to 0.75 0.73 0.37 to 1.43
Camp/Displacement*Post-earthquake 1.19 0.48 to 2.99 2.34* 1.15 to 4.75 0.58 0.27 to 1.26
Under-5 child mortality
Unadjusted 0.57 0.19 to 1.67 2.37** 1.38 to 4.07 0.24** 0.09 to 0.67
Camp/Displacement*Post-earthquake
Adjusteda
Camp/Displacement 0.91 0.48 to 1.73 0.81 0.59 to 1.11 1.28 0.98 to 1.66
Post-earthquake 0.54* 0.30 to 0.96 0.38*** 0.24 to 0.58 0.56* 0.31 to 1.00
Camp/Displacement*Post-earthquake 1.34 0.58 to 3.08 2.34* 1.10 to 5.00 0.63 0.31 to 1.27
***p< 0.001, **p< 0.01, *p< 0.05 a
We assessed two non-mortality biomarker-based health measures: growth for age and level of anemia. Our analyses detected a significantly higher likelihood of having severe anemia among children in camp households than those in the non-camp IDP house-holds (OR = 1.57, 95 % CI 1.07 to 2.30). There was no significant difference among household of different displacement status in anthropometric growth, an in-dicator of long-term household stresses and chronic food insecurity.
Across the indicators on uptake of public health inter-ventions, camp households consistently had relatively better access to basic necessities. Compared to non-displaced households, camp households were more likely to use a bed net for sleeping (OR = 3.23, 95 % CI 2.03 to 5.17) and to spray their households against mosquitoes (OR = 22.53, 95 % CI 11.08 to 45.80). Moreover, camp households also had better access to water, with a regression coefficient for displacement at−5.37 (95 % CI
−9.41 to−1.32) (OLS results not shown). Non-camp IDP households also had significantly higher use of a bed net (OR = 1.39, 95 % CI 1.13 to 1.69) compared to the non-displaced households.
We further investigated differences in having re-ceived vaccines recommended during early childhood (specifically BCG, measles, and DPT). Compared to non-displaced children, children in camps were sig-nificantly more likely to have been vaccinated against
measles by 1 year of age (OR = 2.33, 95 % CI 1.16 to 4.65) and, among children born after the earthquake, to have been given the BCG vaccine (OR = 2.62, 95 % CI 1.18 to 5.81). Children in non-camp IDP house-holds were also more likely to have received the BCG vaccination than their counterparts in non-displaced households (OR = 1.56, 95 % CI 1.01 to 2.40).
Other dependent variables assessed were the experi-ence of hunger in the last four weeks and cholera in-fection of any family member since October 2010. Compared to non-displaced households, camp house-holds were less likely to have experienced hunger (OR = 0.58, 95 % CI 0.38 to 0.88) and were also less likely to have any family member that suffered from cholera since the inception of the cholera outbreak (OR = 0.55, 95 % CI 0.30 to 1.01). In contrast, non-camp IDP households were less likely to go hungry (OR = 0.72, 95 % CI 0.59 to 0.87) compared to non-displaced households.
Discussion
The increasing frequency and intensity of natural di-sasters has wrought significant economic toll on pop-ulations around the world [15]. When coupled with poor infrastructure, these disasters become particu-larly devastating by displacing numerous people and producing complex social and health situations. In this study, we examined the impact of household
Table 3Association between displacement status and child health status and health behaviors in post-earthquake Haitia
Camp vs. Non-displaced Camp vs. Non-camp IDP Non-camp IDP vs. Non-displaced
Dependent variable N OR 95 CI N OR 95 CI N OR 95 CI
Child health status
Stunting 1,910 1.06 0.41 to 2.72 1,077 1.44 0.85 to 2.45 2,503 1.40 0.99 to 1.98
Anemia level 1,718 1.03 0.59 to 1.81 938 1.57* 1.07 to 2.30 2,248 0.94 0.76 to 1.17
Malaria
Bed net use 4,083 3.23*** 2.03 to 5.17 2,152 1.76*** 1.29 to 2.42 5,051 1.39** 1.13 to 1.69
Indoor spraying 4,072 22.53*** 11.08 to 45.80 2,138 11.07*** 4.64 to 26.42 5,036 1.27 0.82 to 1.97
Vaccinationb
BCG vaccination 1,971 2.62* 1.18 to 5.81 1,157 0.90 0.56 to 1.43 2,534 1.56* 1.01 to 2.40
Measles vaccination 2,472 2.33* 1.16 to 4.65 1,407 0.91 0.61 to 1.37 3,179 1,23 0.91 to 1.67
DPT vaccination (3 shots) 2,478 1.43 0.77 to 2.65 1,406 0.86 0.56 to 1.32 3,184 0.96 0.71 to 1.30
Other conditions
Hunger 4,084 0.58* 0.38 to 0.88 2,151 1.06 0.76 to 1.49 5,051 0.72*** 0.59 to 0.87
Cholera after Oct 2010 4,084 0.55 0.30 to 1.01 2,152 0.64* 0.42 to 0.97 5,052 0.98 0.78 to 1.24
***p< 0.001, **p< 0.01, *p< 0.05 a
All models are adjusted for region, location (rural/town/city), altitude, household size, sex, age and education level of the household head, wealth index, land ownership, whether housing was destroyed and family members killed by earthquake. Stunting refers to height-for-age <−2SD
b
displacement as a result of the 2010 Haiti earthquake on child health and explore potential underlying mechanisms. To our knowledge, our study is the only study which has used nationally representative data to quantitatively assess the impact of internal displace-ment by natural disasters on health.
There are several limitations to our study. Similar to all studies based upon surveys, our results are suscep-tible to recall bias by the interviewed mothers. This is true for birth histories that are further away from the time of the interview. Recall bias also likely occurred in the documentation of health behaviors and uptake of public health interventions (but not biomarker-based in-dicators). Unlike our analyses on infant and child mor-tality, our analyses on health behavior mechanisms used a cross-sectional design, preventing definitive conclu-sions about the directionality of potential causal rela-tionships. For instance, our observation that camp households were less likely to have experienced hunger recently and yet their children were more likely to have severe anemia, could be due to households with poor food intake previously being drawn to camps since camps were thought to have adequate food supply from aid agencies and organizations.
Our record of the displacement status was limited to three categories (moved to a camp, moved elsewhere, or did not move) and lacks variability and precision of the intensity of displacement from one place to another. Hence, the variable did not allow us to assess the dose– response relationship of displacement on health, because the displacement status is determined by the informa-tion of residence at the time of the interview. We lack data on how long a household had been displaced or has been living in a camp, or how the housing quality chan-ged from one location to another. Households reporting to reside in camps could have been displaced and lived in camps since the immediate aftermath of the earth-quake or some time afterward. Likewise, non-camp IDP households may have never lived in a camp, or may have moved out of a camp by the time of the survey. Thus, the identified differences between the two displaced pop-ulations in our models may be under-estimated.
After accounting for socioeconomic factors that shape the susceptibility of households being displaced by the earthquake, we find that survival of children in camp households was most adversely affected by the earthquake, followed by those in households that were not displaced.
In contrast to our expectations, the households that were displaced but did not reside in camps seem to be least impacted in terms of children’s health. Al-though intuition might be that the displaced popula-tion was more vulnerable than the non-displaced one [3], the IDP was in fact heterogeneous. Households
displaced other than to camps had greater reductions in infant and child mortality compared to those dis-placed to camps. These findings may partially be ex-plained by selective migration. That is, people who moved in response to the earthquake could be self-selected as unobserved health problems may com-promise mobility [16]. Alternatively, the migration of households could be a manifestation of self-insurance strategies with extended families or friends who can provide shelter in hardship, a common informal risk-coping strategy in developing countries [17]. This is consistent with our observation that the non-camp IDP households enjoy better access to resources which improve health. These findings highlight the importance of migration as a strategy to reduce the impact of a disaster [18].
There was no significant difference in child mortal-ity between those displaced to camps and those not displaced. Compared to IDP groups, children in non-displaced households had poorer access to resources which can improve health. This implies that, for some households with the same likelihood of displacement, staying behind results in poorer living conditions and access to health services; they might live in a dam-aged house in a disaster-prone area but simply cannot afford or lack the networks to migrate. Future studies and investigations are required to understand the challenges and difficulties confronting these vulner-able households. Although they are not internally displaced, they are frequently overlooked. For govern-ments and agencies working in post-disaster relief, beyond the displaced population, efforts need to be dedicated to identify and reach out to households that could be “left behind” in damaged areas.
Households in camps experienced higher infant and child mortality than households not displaced to camps, and our investigation into household condi-tions and health practices yielded additional insights into possible mechanisms. On one hand, households in camps seem to have good access to resources which can improve health such as food and water ac-cess. On the other hand, children in camps do suffer from a higher likelihood of severe anemia, which is consistent with their higher infant and child mortality. This raises the issue of the quality of food to enhance their physical well-being.
(including protein energy malnutrition) resulting from food insecurity and limited access to nutritious food in camps can lead to compromised immunity and in-creased susceptibility to infections, resulting in further energy loss, and triggering a vicious cycle of deteriorat-ing nutritional status and illness. We found higher rates of hunger and anemia of children in camps compared to those displaced elsewhere, despite higher rates of vaccination coverage.
A third explanatory factor may be the risks associated with heightened security risks of living in camps. News reports suggested an increased incidence of both sexual and other physical violence in camps, which in turn could lead to higher mortality and morbidity from phys-ical injury, mental health, and challenges to caretakers and mothers in their ability to care for their children. In-deed, according to the 2012 Haiti DHS report, 36 % of women aged 15–49 living in camps reported to have ex-perienced physical violence, and 16 % having experi-enced sexual violence, both higher than the population averages at 28 % and 13 %, respectively [10]. Prevalence of domestic violence in camps was also a notable issue in camps at 29 %.
Finally, our study’s emphasis on physical health should not de-emphasize the importance of mental health as an essential dimension of human health, especially in a complex emergency context.
Conclusions
Our use of a DID design to evaluate the impact of dis-placement on infant and child mortality, as well as a series of examinations into the association between dis-placement status and access to resources which can improve health, underline complexities in post-disaster relief. Not only is it the case that there is much work to be done to improve the health of those living in camps and that these households are likely to face a wide range of short and long-term challenges in the years to come, the displacement population itself is heterogeneous. Moreover, even individuals that are not displaced by di-sasters are not well-protected and risk-free. Evidence-based and better-targeted interventions require greater knowledge and better systematic evaluations of what works and who is at risk. Given the extensive impact of the earthquake on Haiti, all public health interventions including those that tackle water treatment, vaccination, and vector control [19–21] should consider the post-earthquake housing context. Despite the US$6 billion in aid to Haiti, there are few evaluations of services deliv-ered and lives saved [22]. Scholars, governments and international agencies should begin to systematically col-lect and analyze information on disaster impact, so that we can make progress to establish resilient and respon-sive health systems that can truly be the safety nets of our populations.
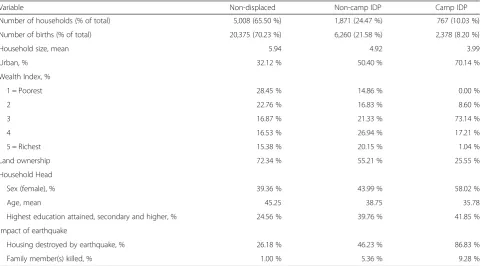
Table 4Descriptive statistics of the pre-matched sample
Variable Non-displaced Non-camp IDP Camp IDP
Number of households (% of total) 5,008 (65.50 %) 1,871 (24.47 %) 767 (10.03 %)
Number of births (% of total) 20,375 (70.23 %) 6,260 (21.58 %) 2,378 (8.20 %)
Household size, mean 5.94 4.92 3.99
Urban, % 32.12 % 50.40 % 70.14 %
Wealth Index, %
1 = Poorest 28.45 % 14.86 % 0.00 %
2 22.76 % 16.83 % 8.60 %
3 16.87 % 21.33 % 73.14 %
4 16.53 % 26.94 % 17.21 %
5 = Richest 15.38 % 20.15 % 1.04 %
Land ownership 72.34 % 55.21 % 25.55 %
Household Head
Sex (female), % 39.36 % 43.99 % 58.02 %
Age, mean 45.25 38.75 35.78
Highest education attained, secondary and higher, % 24.56 % 39.76 % 41.85 %
Impact of earthquake
Housing destroyed by earthquake, % 26.18 % 46.23 % 86.83 %
Family member(s) killed, % 1.00 % 5.36 % 9.28 %
Appendix 2
Abbreviations
CEM, coarsened exact matching; DHS, Demographic and Health Survey; DID, difference-in-differences; IDP, internally displaced people; PSM, propensity score matching
Acknowledgements
The authors would like to thank Chun-Wing Tse for helpful comments and Pamela Krueger for excellent research assistance.
Funding
University of Hawaii at Manoa RTRF Start-Up Funds.
Availability of data and materials
DHS data are available from the DHS Program upon request at dhsprogram.com. The code to replicate these results is available upon request from the authors and will be posted to a public data repository.
Authors’contributions
VF conceived of the study and methods. BC led the data analysis in cooperation with VF. TH contributed to literature review. BC wrote the first draft. All authors contributed to the writing and analysis. All authors read and approved the final manuscript.
Authors’information
BC is an assistant professor in the Institute of Public Health at the National Yang-Ming University. TH is an associate professor in the Department of Economics and VF is an assistant professor in the Department of Public Health Sciences at the University of Hawaii at Manoa.
Competing interests
The authors declare that they have no competing interests.
Consent for publication Not applicable.
Ethics approval and consent to participate
Procedures and questionnaires for standard DHS surveys have been reviewed and approved by the ICF International Institutional Review Board (IRB). The ICF International IRB ensures that the survey complies with the U.S. Department of Health and Human Services regulations for the protection of human subjects (45 CFR 46).
Author details 1
Institute of Public Health, National Yang-Ming University, 155 Linong Street, Sec. 2, Taipei, Taiwan112.2Department of Economics, University of Hawaii at Manoa, 2424 Maile Way, 533 Saunders Hall, Honolulu, HI 96822, USA.3IZA, Bonn, Germany.4University of Hawaii Economic Research Organization,
Honolulu, HI, USA.5Department of Public Health Sciences & Epidemiology, University of Hawaii at Manoa, 1960 East–west Road, Biomed D204, Honolulu, HI, USA.6François-Xavier Bagnoud Center for Health and Human Rights, Harvard T.H. Chan School of Public Health, 651 Huntington Ave, Boston, MA, USA.7Center for Global Development, Washington, D.C., USA.
Received: 6 April 2016 Accepted: 11 July 2016
References
1. Domercant JW, Guillaume FD, Marston BJ, Lowrance DW. Haiti health systems recovery team, Ministry of Health, Republic of Haiti. Update on progress in selected public health programs after the 2010 earthquake and cholera epidemic—Haiti, 2014. Morb Mortal Wkly Rep MMWR. 2015;64(6):137–40.
2. EM-DAT. The OFDA/CRED international disaster database [Internet]. Brussels, Belgium: Université Catholique de Louvain; 2015 [cited 2015 Dec 8]. Available from: http://www.emdat.be/database. Accessed 8 December 2015. 3. Sherwood A, Bradley M, Rossi L, Gitau R, Mellicker B. Supporting Durable
Solutions to Urban, Post-Disaster Displacement [Internet]. The Brookings Institution. 2014. Available from: http://www.brookings.edu/research/ reports/2014/02/07-haiti-earthquake-displacement-bradley. Accessed 23 December 2015.
4. Bilham R. Lessons from the Haiti earthquake. Nature. 2010;463(7283):878–9. 5. Garfield R. Priorities for mortality reduction in Haiti. Disaster Med Public
Health Prep. 2010;4(01):18–20.
6. Rice SE, Patrick S. Index of State Weakness in the Developing World [Internet]. Washington, DC: The Brookings Institution; 2008. Available from: http://www.brookings.edu/research/reports/2008/02/weak-states-index. Accessed 8 December 2015
7. Pape JW, Deschamps MM, Ford H, Joseph P, Johnson WD, Fitzgerald DW. The GHESKIO refugee camp after the earthquake in Haiti—dispatch 2 from Port-au-Prince. N Engl J Med. 2010;362(9):e27.
8. Saint-Macary C, Zanuso C. Build back better? Long-lasting impact of the 2010 Earthquake in Haiti. 2015.
9. Novella R, Zanuso C. Reallocating Children’s Time: Coping Strategies after the 2010 Haiti Earthquake [Internet]. DIAL (Développement, Institutions et Mondialisation); 2015 Sep. Available from: http://EconPapers.repec.org/ RePEc:dia:wpaper:dt201513. Accessed 8 December 2015.
10. Ministry of Public Health and Population (MSPP), Haitian Chilhood Institute (IHE), ICF International. 2012 Haiti Mortality, Morbidity, and Service Utilization Survey: Key Findings [Internet]. Calverton, Maryland, USA: MSPP, IHE, and ICF International; 2013. Available from: http://dhsprogram.com/ pubs/pdf/SR199/SR199.eng.pdf. Accessed 26 November 2015. 11. Blackwell M, Iacus S, King G, Porro G. cem: Coarsened exact matching in
Stata. Stata J. 2009;9(4):524–46.
Table 5Sensitivity analyses limiting pre-earthquake control births within 5 and 7 years before the 2010 earthquake
Camp vs. Non-displaced Camp vs. Non-camp IDP Non-camp IDP vs. Non-displaced
N OR 95 % CI N OR 95 % CI N OR 95 % CI
Infant Mortality: Whether the children die by 12 months old
All year included 10,261 1.19 0.48 to 2.99 4,428 2.34* 1.15 to 4.75 12,449 0.58 0.27 to 1.26
Excluding births prior to year 2005 3,655 0.93 0.32 to 2.69 1,826 2.43* 1.09 to 5.45 4,535 0.52 0.24 to 1.10
Excluding births prior to year 2003 4,641 0.99 0.33 to 2.98 2,257 2.52* 1.11 to 5.75 5,760 0.52 0.25 to 1.10
Child Mortality: Whether the children die by 5 years old
All year included 10,261 1.34 0.58 to 3.08 4,428 2.34* 1.10 to 5.00 12,449 0.63 0.31 to 1.27
Excluding births prior to year 2005 3,655 0.83 0.30 to 2.31 1,826 2.00 0.84 to 4.76 4,535 0.55 0.28 to 1.09
Excluding births prior to year 2003 4,641 0.87 0.30 to 2.51 2,257 1.92 0.79 to 4.63 5,760 0.59 0.29 to 1.20
12. Fan VY-M, Mahal A. What prevents child diarrhoea? The impacts of water supply, toilets, and hand-washing in rural India. J Dev Eff. 2011;3(3):340–70. 13. King G, Nielsen R, Coberley C, Pope JE, Wells A. Comparative Effectiveness
of Matching Methods for Causal Inference. 2011.
14. Iacus, Stefano M., Gary King, and Giuseppe Porro. Causal inference without balance checking: Coarsened exact matching. Polit Anal. 2011;mpr013. URL is available here: http://pan.oxfordjournals.org/content/early/2011/08/23/ pan.mpr013.short.
15. Guha-Sapir D, Hargitt D, Hoyois P. Thirty years of natural disasters 1974– 2003: The numbers. Presses univ. de Louvain. 2004.
16. Halliday TJ, Kimmitt MC. Selective migration and health in the USA, 1984– 93. Popul Stud. 2008;62(3):321–34.
17. Dercon S. Income risk, coping strategies, and safety nets. World Bank Res Obs. 2002;17(2):141–66.
18. Cooper M. Migration and Disaster-Induced Displacement: European Policy, Practice, and Perspective [Internet]. Washington, DC: Center For Global Development Working Paper Series; 2012. Available from: http://www. cgdev.org/publication/migration-and-disaster-induced-displacement-european-policy-practice-and-perspective. Accessed 2 February 2016. 19. Lenhart A, Orelus N, Maskill R, Alexander N, Streit T, McCall PJ.
Insecticide-treated bednets to control dengue vectors: preliminary evidence from a controlled trial in Haiti. Trop Med Int Health. 2008;13(1):56–67.
20. Tohme RA, François J, Wannemuehler K, Magloire R, Danovaro-Holliday MC, Flannery B, et al. Measles and rubella vaccination coverage in Haiti, 2012: progress towards verifying and challenges to maintaining measles and rubella elimination. Trop Med Int Health. 2014;19(9):1105–15.
21. Murray A, Pierre-Louis J, Joseph F, Sylvain G, Patrick M, Lantagne D. Need for certification of household water treatment products: examples from Haiti. Trop Med Int Health. 2015;20(4):462–70.
22. Ramachandran V, Walz J. Haiti: where has all the money gone? J Haitian Stud. 2015;21(1):26–65.
23. World Health Organization (WHO). WHO recommendations for routine immunization - summary tables [Internet]. WHO. 2015. Available from: http://www.who.int/immunization/policy/immunization_tables/en/. Accessed 23 December 2015.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal • We provide round the clock customer support
• Convenient online submission • Thorough peer review
• Inclusion in PubMed and all major indexing services • Maximum visibility for your research
Submit your manuscript at www.biomedcentral.com/submit