jo u r n al h o m e p a g e :w w w . i j m i j o u r n a l . c o m
A
comparison
between
the
VIPS
model
and
the
ICF
for
expressing
nursing
content
in
the
health
care
record
Jan
Florin
a,∗,
Anna
Ehrenberg
a,
Margareta
Ehnfors
b,
Catrin
Björvell
c,daSchoolofHealthandSocialStudies,DalarnaUniversity,79188Falun,Sweden bSchoolofHealthandMedicalSciences,ÖrebroUniversity,71082Örebro,Sweden cManagerofNursingQuality,KarolinskaUniversityHospital,17176Stockholm,Sweden dDepartmentofNeurobiologyCareSciencesandSociety,KarolinskaInstitutet,Stockholm,Sweden
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16February2012
Receivedinrevisedform
22May2012 Accepted28May2012 Availableonlinexxx Keywords: Documentation Classification ICF Mapping Nursing VIPS
a
b
s
t
r
a
c
t
Background:Multi-professionalstandardizedterminologiesareneededthatcovercommon
aswellasprofession-specificcarecontentinordertoobtainafullcoverageanddescription
ofthecontributionsfromdifferenthealthprofessionals’perspectivesinhealthcare.
Imple-mentationofterminologiesinclinicalpracticethatdonotcoverprofessionals’needsfor
communicationmightjeopardizethequalityofcare.
Purpose:TheaimofthestudywastocomparethestructureandcontentoftheSwedishVIPS
modelfornursingdocumentationandtheinternationalclassificationoffunction,disability
andhealth(ICF).
Method:Mappingwasperformedbetweenkeywordsandprototypicalexamplesforpatient
status in the VIPS modeland terms in the ICFand its framework of domains,
chap-tersandspecific terms.Thestudyhadtwophases.Inthefirstphase13keywordsfor
patient statusintheVIPS modeland the289terms(prototypicalexamples) describing
related contentweremappedtocomparabletermsintheICF.Inphasetwo,1424terms
on levels2–4 inthe ICFweremappedto thekey wordsforpatient statusin theVIPS
model.
Results:Differencesinclassificationstructuresandcontentwerefound,withamore
elab-orated levelofdetaildisplayed intheICFthanintheVIPSmodel.Amajorityofterms
couldbemapped,butseveralessentialnursingcareconceptsandperspectivesidentified
in theVIPSmodelweremissinginthe ICF.Two-thirdsofthe contentinthe ICFcould
bemapped totheVIPS’keywordsforpatient status;however, theremainingtermsin
the ICF, describingbodystructure andenvironmental factors,are not partofthe VIPS
model.
Conclusion: Despitethata majority ofthe nursing contentin the VIPSmodelcould be
expressedbytermsintheICF,theICFneedstobedevelopedandexpandedtobefunctional
fornursingpractice.Theresultshaveinternationalrelevanceforglobaleffortsto
imple-mentunifyingmulti-professionalterminologies.Inaddition,ourresultsunderlinetheneed
forsufficientcoverageandlevelofdetailtosupportdifferentprofessionalperspectivesin
healthcareterminologies.
©2012ElsevierIrelandLtd.Allrightsreserved.
∗ Correspondingauthorat:SchoolofHealthandSocialStudies,DalarnaUniversity,79188Falun,Sweden.Tel.:+4623778446.
E-mailaddress:jfl@du.se(J.Florin).
1386-5056/$–seefrontmatter©2012ElsevierIrelandLtd.Allrightsreserved.
Pleasecitethisarticleinpressas:J.Florin,etal.,AcomparisonbetweentheVIPSmodelandtheICFforexpressingnursingcontentinthehealth
ARTICLE IN PRESS
IJB-2881; No.ofPages10
2
international journal of medical informatics xxx (2012)xxx–xxx1.
Introduction
Communication betweenhealth professionals, both within
aprofession andbetweenprofessionalgroups,isimportant
for the delivery of high quality care with respect to
con-tinuity of care, patient safety and patient participation in
healthcare.Professionalcontributionstopatientcareneed
to berepresented inthe patient’s electronic health record
(EHR)inordertosupportplanning,deliveryand evaluation
of comprehensive and safe patient care. The need to use
standardized terminologies in health care and to develop
multi-professionalEHR systems haslong been recognized.
Standardizedterminologies are not onlyneeded to reduce
theriskforcommunicationbreakdownbutarealsonecessary
toenablethe extractionofrelevant informationfrom
elec-tronicinformationsystemsthatcouldbeusedforknowledge
development,benchmarking,qualityimprovement,resource
allocation and research. In general, the use of
standard-izednursingterminologieshasbeenratherscarceinhealth
care. Traditionally,registered nurses (RNs) have used local
documentation methods, often in the form of narrative
descriptions.Thereis,however,arangeofstandardized
nurs-ingterminologiesavailablethatdescribenursingdiagnoses,
interventions and outcomes (either separate or in various
combinations). One example is the NANDA International
NursingDiagnosesandClassifications[1].Anotherexample
istheInternationalClassificationforNursingPractice(ICNP),
whichwasestablishedbytheInternationalCouncilofNurses
(ICN)[2].TheICNP,whichcomprisestermsfornursing
phe-nomena and activities, is a comprehensive summation of
severalterminologies.
Currently, no multi-professional terminology for health
careinpracticaluseexiststoday,butamajorefforthasbeen
directedtowardthistarget.Suchaterminologyisneededto
capturealltypesanddimensionsofhealthcaredatatoensure
better health care practiceand more appropriateresource
allocation. The work of multiple professional groups (e.g.,
nurses,physiotherapistsandoccupationaltherapists)needs
representationsinEHRsinawaythatmakestheinformation
retrievable for multiple purposes. Standardized
Nomencla-tureofMedicine–Clinicalterms(SNOMED-CT)[3]hasbeen
translated into several languages and its development for
practical use has been initiated. Medicine has a long
tra-ditionof using standardizedterminologies (e.g., the World
Health Organization (WHO) approved International
Classi-fication of Diseases (ICD)) [4]. Further, part of the current
WHOfamilyofclassificationsistheinternational
classifica-tionoffunction,disabilityandhealth(ICF)[5],whichprovides
a complementary functional perspective to ICD based on
theknowledgeareasofother healthdomains.TheICFwas
developedprimarilybyphysio-andoccupationaltherapists.
Currently, the VIPSmodel hasbeen widelyused sincethe
early 1990s by RNs in Sweden [6] and other Nordic
coun-triesfornursingdocumentation. TheICFhasrecentlybeen
introducedformulti-professionaluseinsomefieldsofhealth
care in Sweden. However, there has not been any critical
analysis of the coherence of the two. This study
there-forefocuses onmapping termsin theVIPSmodeland the
ICF.
1.1. TheVIPSmodel
In Sweden, RNs’ recording in the health record has been
mandatorybylawsince1986andnowadaysaddressedinthe
revisedSwedishpatientrecordact[7].TheVIPSmodelisthe
SwedishacronymforWell-being,Integrity,PreventionandSafety,
which reflectsfour basicvaluesunderpinningnursingcare
[6,8].Themodelwasfirstpublishedin1991[6]withtheaimof
providingaconceptualizationofessentialelementsin
nurs-ingandastructureofkeywordstoorganizenursingcontentin
thepatientrecordinaccordancewiththenursingprocess.To
facilitateapatient-centeredapproach,theVIPSmodelfocuses
ontheindividualpatient’sfunctioningindailylifeactivities
ratherthanonpathophysiologicalproblemsororgansystems.
Themodel wasthe resultofa structuredresearch process
thatincludedanextensiveliteraturereview,reviewofrecords,
empiricaltestinginclinicalpracticeandvalidationwith
exist-ingtheoreticalmodelsinnursing[6].TheVIPSmodelprovides
aframeworkfornursingdocumentationtosupportnursesto
acknowledgeandverbalizeessentialdatathatreflects
nurs-ingpractice.InthiswaytheVIPSmodelhelpstofacilitatethe
structuringofinformationandknowledgereflectingnursing
practice,aswellassupportteachingandresearchactivitiesin
nursing.
TheVIPSmodelpresentskeywordsontwolevels[6,8,9].
Level oneconcerns thenursingprocess model:assessment
(nursinghistory, nursingstatus),nursingdiagnosis,nursing
goal,nursinginterventionandnursingoutcome(Fig.1).Level
twoconsistsofasubdivisionofkeywordsundernursing
his-tory,nursing statusand nursinginterventions. Prototypical
examplesareprovidedforeverykeywordonleveltwo.
Nursingstatuscomprisesdescriptionsofsignsand
symp-toms regardinga patient’s healthsituation and conditions
influencing nursing care, as assessed from different
per-spectives (e.g.,nurseand patient).Thedocumentationofa
patient’shealthstatusshouldaddressthefollowing
dimen-sions: function, including alterations, risks and resources;
comfort, both from a physical and psychosocial point of
view; influencing factors/circumstances (e.g., environment,
resources–demands,internal–external,positive–negativeand
expectations–values);aids/devicesused bythe patient(e.g.,
pharmacological,technicalorpsychosocial)[6,8,9].
TheVIPSmodelhasshowngoodcontentvalidityinmany
areas of nursing care, including acute surgical and
medi-cal,stroke,dementia,geriatric,pediatric,peri-operativeand
psychiatric care[8,10]. The VIPSmodel is usedfor
record-ingnursingandindividualcareplanningthroughoutSweden,
aswellasinDenmark,Norway,Estonia andLatvia.Several
softwareapplicationsfortheEHRhaveincludedthemodel.
Moreover, it is taughtin mostnursing undergraduate
pro-gramsinSwedenandSwedishtextbooksinnursinghavebeen
organizedaccordingtotheVIPSmodel.
1.2. Theinternationalclassificationoffunctioning, disabilityandhealth
WHOhasdevelopedseveralclassificationssupportinghealth
care practice,including the ICF [5]. It was first releasedin
2001and laterpresented(in 2007)inaversion forchildren
Fig.1–OverviewoftheVIPSmodel.
Fig.2–Theinternationalclassificationoffunctioning,disabilityandhealth[5].
describebodystructure,functioninganddisabilitybutalsoto
captureconceptionsofadynamicinteractionbetweenhealth
conditionsandcontextualfactors[5].TheICFisbasedona
bio-psycho-socialmodel, which combinesprevious models
forfunctioninganddisability[12],andconsistsoftwo
sepa-ratepartswithtwocomponentseach:functioninganddisability
withthecomponentsbody structuresandbody functionsand
activitiesandparticipationandcontextualfactorswiththe
compo-nentsenvironmentalfactorsandapersonalfactor,whichhasbeen
identifiedbutnotyetdeveloped.Thestructureispresentedin
Fig.2withthecomponentbodystructuresandbodyfunctions
presentedastwoseparateentitiesforclarificationofthe
num-berofterms.
Eachcomponentismadeupofdifferentchapters
contain-ingterms(levels2–4)thataretheunitsoftheclassification.
Intotal,thereare30chaptersand1424terms.Themaximum
numberoftermsavailabletodescribeaperson’shealthand
ahealth-relatedconditionis30onthefirstlevel,362onthe
secondlevel,926onthethirdleveland136onthefourthlevel.
A hierarchicalcodingsystem isused inwhichthe
compo-nents are designated byletters:b forbody functions,sfor
Pleasecitethisarticleinpressas:J.Florin,etal.,AcomparisonbetweentheVIPSmodelandtheICFforexpressingnursingcontentinthehealth
ARTICLE IN PRESS
IJB-2881; No.ofPages10
4
international journal of medical informatics xxx (2012)xxx–xxxTable1–ExamplesoftermsandcodesonfourlevelsintheICFconceptualframe.
Component Level1 Level2 Level3 Level4
bBodyfunctions b2Sensoryfunctionsandpain b280Sensationofpain b2801Paininbodypart b28013Paininback
environmentalfactors.The letter isfollowed byanumeric codedisplayingthelevelandpositionoftheterminthe hier-archy(Table1).Further,twofigurescanbeaddedtothecode
thatdisplayqualifiersrepresentingtheperspectivesof
capac-ityandperformance.
The ICF has gained increased attention internationally
asaunifyingclassificationsystemapplicabletothe
knowl-edgeareasandresponsibilitiesforvarioushealthprofessions,
includingnursing.Ithasbeensuggestedasameanstoexpand
nurses’thinkingandclinicalpracticebyaddinganincreased
awarenessofsocial,culturalandpoliticaldimensionsof
dis-ability[13].Further,itisregardedasausefulframeworkand
foundationinsettinggoalsfornursinginterventions
regard-ingacute and earlypost-acuterehabilitation[14]. However,
theICFisnotsuitableforformulatingnursingdiagnosesto
thesameextentastheNANDA[1]andtheICNP[2]that
con-tainstandardizeddiagnosisexpressions,orconsideringthe
InternationalStandardreferenceterminologymodel(RTM)for
nursingdiagnosis[15]ortheuseofcurrentlyestablished
cri-teriafordiagnosesaccordingtothePES(problem-etiology–
signsandsymptoms)format[16].However,elementsin
nurs-ingdiagnosesretrievedfromapatient’sEHRcouldbeclassified
usingtheICF,butwithratherlowinterrateragreementfrom
61to75%onahigherleveland42to60%onamoredetailed
levelintheclassificationhierarchy[17].Theapplicationofcore
setsfromtheICFfornursinghasbeentestedwithacceptable
results[18].SeveralauthorshaveconcludedthattheICFhas
relevancetonursingcare,butthatnursesoughttotakeamore
activepartinthefurtherdevelopmentoftheICF[13,14,17,19].
The ICF is currently implemented in some areas in
Sweden(primarily withinresidentialcarefacilities)to
sup-port multi-professionaldocumentation practice concerning
patient status and communication between health
profes-sionsand theirrespective knowledgedomains. InSweden,
theICFisintroducedasaninterfaceterminologyreplacing,
orimplementedincombinationwith,previousstructuresof
standardizedterms,oftenbasedonthe VIPSmodel,which
presentsanewstructuretotheEHR.Comprehensivecoverage
isaqualityfactorofterminologycontentthatneedsexternal
referencestandardstobeestablished(e.g.,userrequirements
anddomain-specificneedsofcontent)[20]. Thetwo
termi-nologies have different purposes. The ICF was developed
primarilyfromaparamedicalandrehabilitationperspective.
Thus,studies investigatingthe coherence betweennursing
knowledgeand theICF onagenerallevel are lacking. Itis
thereforeimportanttoascertainthattheICFprovidesa
com-prehensivecontentcoverageinwhichtermsareonasufficient
levelofdetail tosupportand representspecific knowledge
domainsand professionalclinicalpracticeswithinnursing.
ItisimportantthattheICFprovidecomprehensivecoverage
inordertoacquiresensitivedataonallaspectsofapatient’s
problemsandneedsunderpinningcaredecisions.Becausethe
VIPSmodelwasdevelopedspecificallyfor(andiscurrently
usedsuccessfullywithin)nursingpractice,oneapproachto
evaluatethenursingsensitivityoftheICFistomapthecontent
oftheICFandVIPSmodel.
2.
Aim
Theaimofthestudywastocomparethestructureand
con-tentoftheSwedishVIPSmodelfornursingdocumentation
withtheICF.Thiscanbedonebymappingthekeywordsand
prototypicalexamplesofsuggestedcontentforpatientstatus
intheVIPSmodeltotheframeworkofdomains,chaptersand
termsintheICF.
Threeresearchquestionsguidedthestudy:
1. Towhatextentcanthekeywordsinthe VIPSmodelon
levels1and2forpatientstatusbemappedtotheICF?
2. Towhatextentcannursingdatadescribedasprototypical
examplesforpatientstatusintheVIPSmodelbemapped
tothetermsonlevels1–4intheICF?
3. Towhatextentcanthetermsonlevels1–4intheICFbe
mappedtopatientstatusintheVIPSmodel?
3.
Methods
Thestudyusedadescriptivedesignbyperformingmapping
ofcontentintwoclassifications.
3.1. Material
The Swedish versions ofthe VIPSmodel [6,8] and the ICF
[21] were used in this study. Thirteen of 14 key words in
the VIPS model for patient status were used for
compari-son, alongwiththe prototypicalexamplesprovided(thisis
because theICFcategorizesterms limitedtopatient status).
Subsequently, thekey wordsin theVIPS fornursinghistory
and nursing interventions were not used formapping. The
selectedkeywordsintheVIPSforpatientstatuswere
com-munication,cognition/development,breathing/circulation,nutrition,
elimination,skin/integument,activity,sleep,pain/perception, sexu-ality/reproduction,psychosocial,spiritual/culturalandwell-being. Thekeywordcompositeassessmentwasexcludedbecausethe
content reflectspatientstatusbasedonassessment
instru-mentsorscalesnotnaturallylinkedtoothersinglekeywords.
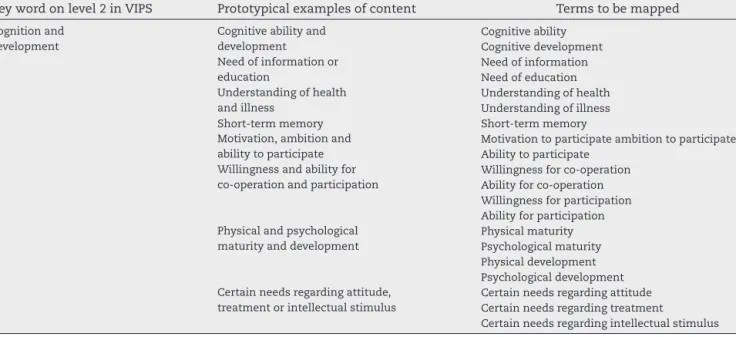
Additionally, 289 terms were identifiedfrom the
prototypi-calexamplesprovidedforthe13keywords.Forexample,the
keywordcognition/developmentconsistedofeightprototypical
examples ofcontent thatcouldbedividedinto 15separate
termstobemapped(Table2).Intotal,1424termsonlevels
2–4oftheICFwereusedinthemappingprocess,aswellas30
Table2–Examplesofextractedmappingtermsfromlevel2keywordsandprototypicalexamplesintheVIPSmodel
(Englishversion2002).
Keywordonlevel2inVIPS Prototypicalexamplesofcontent Termstobemapped
Cognitionand development
Cognitiveabilityand development Cognitiveability Cognitivedevelopment Needofinformationor education Needofinformation Needofeducation Understandingofhealth andillness Understandingofhealth Understandingofillness Short-termmemory Short-termmemory Motivation,ambitionand
abilitytoparticipate
Motivationtoparticipateambitiontoparticipate Abilitytoparticipate
Willingnessandabilityfor co-operationandparticipation
Willingnessforco-operation Abilityforco-operation Willingnessforparticipation Abilityforparticipation Physicalandpsychological
maturityanddevelopment
Physicalmaturity Psychologicalmaturity Physicaldevelopment Psychologicaldevelopment Certainneedsregardingattitude,
treatmentorintellectualstimulus
Certainneedsregardingattitude Certainneedsregardingtreatment
Certainneedsregardingintellectualstimulus
3.2. Mappingprocedure
Themappingprocedureconsistedoftwoparts.Inthefirstpart thetermsweremappedtograspthecomprehensivenessand completenessofterms[22]inthe ICFrepresentingnursing
sensitiveinformationdescribedintheVIPS.Atotalof13key
wordsand289termsderivedfromprototypicalexamplesin
patientstatusintheVIPSmodelweremappedtotermsonlevels
1–4intheICFbytwooftheauthors(JFandCB).
Inthe second part, terms on levels 2–4 inthe ICF were
mappedaccordingtothekeywordsforpatientstatus inthe
VIPSmodelbytwootherauthors(MEandAE).Themapping
procedureswereperformedpartlyindependentlywithinthe
pairofauthors,withfinalagreementreachedafterdiscussion.
Excelspreadsheetswereusedtoorganizethedatafor
com-parisonanddescriptivestatisticswereappliedtopresentthe
data.
4.
Results
4.1. ComparisonbetweentheVIPSmodelandtheICF
Thekey wordsonlevel 1intheVIPSmodel,whichdisplay
thestepsofthenursingprocess,wereabsentintheICF.The
ICFisaclassificationtodescribevarioushealthconditionsfor
functionandactivity,whichwouldcorrespondtopatient
sta-tusbutdoesnotsupportprocesses,andsubsequently,notthe
nursingprocessasawhole.
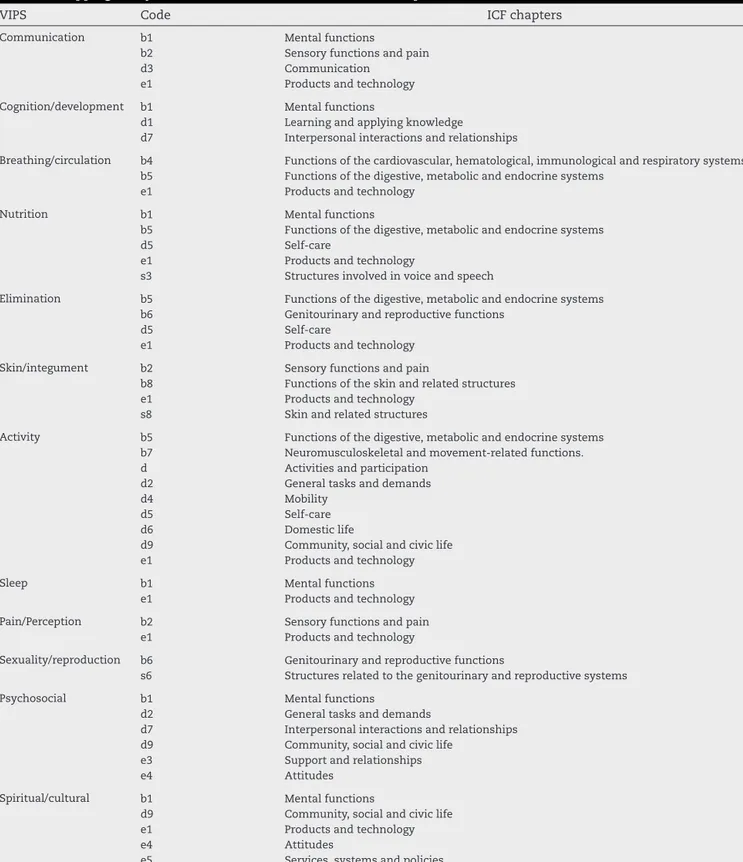
Inall,12keywordsonlevel2intheVIPSmodelforpatient
statuscouldbestatedusingtermsonlevel1(chapters)inthe
ICF,mostoftenfoundaspartofabroadertermorasasimilar,
butdifferentlyworded,term(Table3).However,theVIPSkey
wordwell-being,asenseofone’sownperceivedhealthanda
summaryofanindividual’slifesituationcouldnotbemapped
totheICF.Well-beingoccursintheICFaspartoflookingafter
one’shealth(d570)orassistingothers(d660).Further,asanaim
descriptionforhealthservices(e5800),healthsystems(e5801)and
health policies(e5802),butnotasadescription ofthehealth
conditionofthepatient.
A semantically perfect match tothe ICF could oftenbe
foundforthekeywordsintheVIPSmodel.However,the
hierar-chicalplacementandscopeofthetermswereoftensomewhat
different, which meant that several terms in the ICFwere
neededtocoverthesuggestedcontentforaspecifiedkeyword
intheVIPSmodel.Forexample,therewasaperfectmatch
inwordingbetweenchapterd3intheICFandthekeyword
communicationintheVIPSmodel,butthedescribed content
withintheICFwasnarrower,leadingtotheneedtouse
sev-eralchaptersintheICFtocoverthecontentforcommunication
intheVIPSmodel.Therelevantcontentwasrepresentedin
theICFchaptersb1,b2,d3ande1,reflectingthreedomainsat
thesametime.Onereasonforthatisthedivisioninfunction
andactivity(i.e.,apatient’sactivityoractivities,notnursing
activities)(chapterbandd)intheICFthathasnoparallelin
theVIPSmodel,whereahigherlevelofabstractionisused.
Ontheotherhand,termsforproductsandtechnologywere
presentundereightofthekeywordsintheVIPSmodelbut
gatheredunderonechapter(e1)intheICF.
Content described asprototypical examples for the key
wordnutritioncouldbemappedtotheareasoffivechaptersin theICF:functionsofthedigestivemetabolicandendocrinesystems
(b5),mentalfunctions(b1),self-care(d5),productsandtechnology
(e1)andstructuresinvolvedinvoiceandspeech(s3)(Table3).The keywordsleepintheVIPSmodelcouldbemappedtotheICF
aspartofthebroadertermmentalfunctions(b1),whichwasalso
thecasewithseveralofthekeywordsintheVIPSmodel.
4.2. ContentoftheVIPSmodelmappedtotheICF
Ofthe289termsdescribingprototypicalexamplesintheVIPS
model,179(62%)couldbemappedtothe ICF.However,the
termsintheVIPSmodelaredescribedonamoreaggregated
andlessdetailedlevelthantheICFterms.Someofthe
Pleasecitethisarticleinpressas:J.Florin,etal.,AcomparisonbetweentheVIPSmodelandtheICFforexpressingnursingcontentinthehealth
ARTICLE IN PRESS
IJB-2881; No.ofPages10
6
international journal of medical informatics xxx (2012)xxx–xxxTable3–Mappingofkeywordsonlevel2intheVIPSmodeltochaptersintheICF.
VIPS Code ICFchapters
Communication b1 Mentalfunctions
b2 Sensoryfunctionsandpain
d3 Communication
e1 Productsandtechnology Cognition/development b1 Mentalfunctions
d1 Learningandapplyingknowledge
d7 Interpersonalinteractionsandrelationships
Breathing/circulation b4 Functionsofthecardiovascular,hematological,immunologicalandrespiratorysystems b5 Functionsofthedigestive,metabolicandendocrinesystems
e1 Productsandtechnology Nutrition b1 Mentalfunctions
b5 Functionsofthedigestive,metabolicandendocrinesystems
d5 Self-care
e1 Productsandtechnology
s3 Structuresinvolvedinvoiceandspeech
Elimination b5 Functionsofthedigestive,metabolicandendocrinesystems b6 Genitourinaryandreproductivefunctions
d5 Self-care
e1 Productsandtechnology Skin/integument b2 Sensoryfunctionsandpain
b8 Functionsoftheskinandrelatedstructures e1 Productsandtechnology
s8 Skinandrelatedstructures
Activity b5 Functionsofthedigestive,metabolicandendocrinesystems b7 Neuromusculoskeletalandmovement-relatedfunctions. d Activitiesandparticipation
d2 Generaltasksanddemands
d4 Mobility
d5 Self-care
d6 Domesticlife
d9 Community,socialandciviclife e1 Productsandtechnology
Sleep b1 Mentalfunctions
e1 Productsandtechnology Pain/Perception b2 Sensoryfunctionsandpain
e1 Productsandtechnology
Sexuality/reproduction b6 Genitourinaryandreproductivefunctions
s6 Structuresrelatedtothegenitourinaryandreproductivesystems Psychosocial b1 Mentalfunctions
d2 Generaltasksanddemands
d7 Interpersonalinteractionsandrelationships d9 Community,socialandciviclife
e3 Supportandrelationships
e4 Attitudes
Spiritual/cultural b1 Mentalfunctions
d9 Community,socialandciviclife e1 Productsandtechnology
e4 Attitudes
e5 Services,systemsandpolicies
whichwasmostcommonintheareasofthepatient’sown per-spectiveandperceptionsrelatedtopsychosocialorexistential matters(e.g.,termsrelatedtofeelings,experiences, percep-tions,habits, skills,intentions, meaningsor preferencesof thepatientorfamily).Further,somephysicalmattersanda senseofwell-beingasaglobalestimationofapatient’shealth conditionandtermsdescribingpersonalfactorsintheVIPS modelcouldnotbeexpressedbytheICF.Thereisalackof
termsinexpressinggender,ethnicity,ageandother health-relatedfactors(e.g.,fitnesslevel,lifestyle,habits,upbringing, socialbackground,education,professionandcommon behav-iorpatternsandcharacteristics).
Theconceptofqualityoflifecouldnotbemappedtothe ICFthoughtherearetermsintheICFreflectingqualityrelated tospecificareas,suchasconsciousness(b1102),sleep(b1343), psychomotor functions(b1471),vision(b2102),voice (b3101)
94
59 51 53
24 32
299
8
92
29
187
6
0 50 100 150 200 250 300 350Number of ICF terms
Key words in
VIPS
Fig.3–NumberofICFtermsthatcouldbemappedtokeywordsforpatientstatusintheVIPSmodel(n=934).
andqualityofenvironmentalfactors.TermsintheICFcould
beusedtodescribecurrenthealthconditionsbutdidnot
per-mitthedescriptionofrisksorpotentialproblemsofpatients.
Forinstance,sensationoffalling(b2402)couldbedescribedbut
notincreasedriskoffalling.Alackofsomethingoraneedof
somethingaspartofthedescriptionofapatient’sstatus(e.g.,
knowledgedeficitregardingtreatmentandself-care
manage-mentasdescribedintheVIPSmodel)couldnotbeexpressed
bytheICF.Apatient’slackofknowledgeandneedsof
infor-mationweremissingintheICF,whereastherewereICFterms
todescribelearningneeds(mostlybasicskillssuchaswriting
andreading)andapatient’sabilitytoapplyknowledge.
Suchfeelingsasanxiety,fear,anger,hate,tension,sadness,
sorrow,emotionalinstabilityorjoy,happinessandlovethat
arepresentintheVIPSmodelcouldnotbeexplicitlymapped
tothe ICF.However, these feelingscould bemapped on a
moregenerallevelasemotionalfunctions(b152)orfromthe
per-spectiveofchildren:functionsofappropriatenessofemotion
(b1520),regulationofemotion(b1521)andrangeofemotion
(b1522).Termstodescribecopingstrategies,lossofcontrol,
dependenceand helplessnessin theVIPSmodel could not
bemappedtotheICF,althoughsomefeaturesof
psycholog-icalcharacteristicsweredescribedundergeneralinterpersonal
interactions(d710–d729)intheICF.Thewillingnessofapatient
tocooperateorparticipate,asdescribedintheVIPSmodel,
could notbemappedto theICF.Further,psychosocial
fac-tors(such asfeelingsofsecurityor insecurityand trustor
mistrust)couldnotbemappedtotheICF.Itispossible,
how-ever,todescribeaperson’scharacterintheICF:forexample,
trustworthiness(b1267)isdefinedas“amentalfunctionthat
producesapersonaldispositionthatisdependableand
prin-cipled,ascontrastedtobeingdeceitfulandanti-social”.Hence,
anassessmentbyanobservercouldbedescribed,whereasa
patient’sownfeelingoftrust,aspresentintheVIPSmodel,
couldnotbemappedtoICFterms.Spiritualandcultural
fac-tors(e.g.,meaningoflifeandperspectiveondeath,sickness
experiences,senseofbelongingandsenseofcoherence),as
presentintheVIPSmodel,couldnotbemappedtotheICF.
CoherenceispresentintheICFinrelationtoorganizinga
log-icalthinkingprocess,butdescriptionofamoreholisticsense
ofapatient’ssenseofcoherencecouldnotbemappedtothe
ICF.
ThereweretermsintheICFforsleepfunctions(b134)
regard-ing amount, onset, maintenanceand quality of sleep, but
termscoveringfeelingsoftiredness,exhaustionorfatigue,as
presentintheVIPSmodel,couldnotbemappedtotheICF.
TheICFfocusesonfunctionsthatshouldleadtopersonal
feel-ingsandexperiences,buttheactualresult(e.g.,thefeelingof
beingrestedorrelaxed)couldnotbeexpressed.Restis
men-tionedinthe ICFasanendgoalinrelationtothefunction
qualityofsleep(b1343),whichisdescribedas“mentalfunctions
thatproducethenaturalsleepleadingtooptimalphysicaland
mentalrestandrelaxation”.Thereisatermforexpressing
fati-gability(b4552),afunctionrelatedtosusceptibilitytofatigue
atanylevelofexertion.Thistermisconsideredamore
pre-cisedescriptionofexercisetolerancefunctions(b455).However,
fatigueinitself,asdescribedintheVIPSmodel,couldnotbe
mappedtotheICF.
Atermforsensationofpain(b280)doesexistintheICF,with
someexamplesofdifferentfeaturesofpain,butanelaborated
descriptionofthecharacterofpain(e.g.,terms forpattern,
durabilityandintensity)thatisdescribedintheVIPSmodel
couldnotbemappedtotheICF.TermsintheVIPSmodelfor
givingbirth,orrelatedtoaperson’sowndeath,couldnotbe
mappedtotheICF.
4.3. ICFtermsmappedintotheVIPSmodel
In all, 934 terms (66%) on levels 2–4 in the ICF could be
mappedtothekeywordsforpatientstatusintheVIPSmodel
(Fig. 3). Thekey wordactivity in the VIPSmodel was
suit-able for the largest amount of mapped terms in the ICF
(n=299),followedbythekeywordpsychosocial(n=187).The
keywordsspiritual/culturalandsleepwereleastfrequentlyused
formappedtermsfrom theICF,coveringonlysixandeight
ICFterms,respectively.TherewerenotermsintheICFthat
mappedintothekeywordwell-beingintheVIPSmodel.
Alto-gether,490ICFterms(34%)couldnotbemappedintotheVIPS
model,including280termsrelatedtobodystructuresand210
termsrelatedtootherissuesthatarenotintendedtobepart
oftheVIPSpatientstatuskeywords.Someanatomicalterms
intheICFfortheskincouldbemappedtotheVIPSkeyword
skin/integument,whereas therest ofthe anatomicalterms
Pleasecitethisarticleinpressas:J.Florin,etal.,AcomparisonbetweentheVIPSmodelandtheICFforexpressingnursingcontentinthehealth
ARTICLE IN PRESS
IJB-2881; No.ofPages10
8
international journal of medical informatics xxx (2012)xxx–xxxcoversarangeofareasnotrelevantfornursingandtherefore
notpossibletomaptotheVIPSmodel(e.g.,thelevel2category
intheICFforservices,systemsandpolicies)(e5).
5.
Discussion
Themainfindingsinthisstudywerethatthetwomodels
stud-ieddevelopedfordifferencepurposes,haddifferentstructures
andcontent;thecontentforeachofthekeywords
represent-ingpatientstatusintheVIPSmodelcouldnotbemappedto
onesinglecategoryintheICFandthusseveralcategoriesinthe
ICFhadtobeusedtocoverthecontent;amajorityofpatient
statustermsintheVIPSmodelcouldbemappedtotheICF
(andoftenonamorespecificlevel).Further,important
con-tentofrelevancefornursing,accordingtotheVIPSmodel,was
missingintheICF;whilethemajorityoftheICFtermscouldbe
mappedtothekeywordsforpatientstatusintheVIPSmodel.
IntheICF,66%ofthelevels2–4termscouldbemappedtothe
12patientstatuskeywordsintheVIPSmodel,indicatingthat
thosetermsarerelevantfordescribingnursingcare.
ThecategoriesintheVIPSmodelandtheICFdidnot
cor-respond fully,revealing structural differences between the
two,presumablyduetodifferencesinpurposeandtheoretical
frameworkunderpinningtheclassifications.TheVIPSmodel
isprocess-oriented,focusingonprovidingadocumentation
structureand content to reflectthe complete nursing
pro-cess.TheICF,incontrast,focusessolelyondescriptionsofthe
healthconditionsofpatientsanddoesnotclaimtocoverthe
entirecareprocess.ThefindingsindicatethattheICFcould
onlycorrespond to parts of a patient’s health status from
anursingperspective.Inthisstudy 62%oftheprototypical
examplesprovidedintheVIPSmodelcouldbemappedtothe
ICFand66%oftheICFtermscouldbemappedtothekeyword
structureintheVIPSmodel.Despitedifferencesinmapping
procedures,thereareresemblanceswithpreviousreportsin
which46%ofthetermsintheICFcouldbemappedtotheICNP
withanexactor partialmatch[23].Ourfindingsshowthat
asubstantial portionofrelevantnursingcontent described
intheVIPSmodelisnotcoveredbythecurrentlyavailable
termsintheICF.Otherstudiesregardingcomprehensiveness
intheICFinrelatedknowledgedomainshavereporteda
bet-ter matchbetween thecontent inassessmentinstruments
forspecifichealthareaswiththeICFterms.Thus,reported
lowerfigures formissingtermsintheICFwerefound,e.g.,
for5%ofthecontentinhealthrelatedqualityoflife
instru-ments[24],20%inoutcomemeasuresforburninjuries[25],
and 23%forpatient reportedoutcome measuresrelated to
hemophilia,ofwhich10%wereconceptsonamoregeneral
andunspecificlevel [26]. Comparisonmadebetweenterms
inthehomecareassessmentinstrumentInterRAI(Resident
AssessmentInstrument)homecareandtheICFclassification
showedthat25%oftheassessmenttermscouldnotbecoded
withICFcodes,ofwhich15%wereonagenerallevelandnot
preciselydefined[27].
Further,thecontentforpatientstatusintheVIPSmodel
covers moreareas than solely descriptions of health
con-ditionsinthat self-careactivities andassistingdevices are
alsoincorporated.Ontheotherhand,environmentalfactors
andbodystructuresareincludedintheframeworkoftheICF
togetherwithfunctionsandactivities.Thedifferencebetween
functionandactivityisemphasizedintheICF,whereasthe
VIPSmodelfocusesonactivitiesindailylifeandthus
sub-sumessomedegreeoffunctioning.Forexample,thedegree
andqualityofmusclepowercanbecategorizedintheICFas
musclepowerfunction(b730).Incontrast,intheVIPSmodel
it iscategorized aspartofthekeywordactivityand
there-forefocusesmoreonuseandconsequencesofimpairment
inactivitiesindailylifewherethefunctionisneeded.Inthis
casetheICFprovidesacleardistinctionbetweenfunctionand
activity,whichcouldbeusefulinnursing.
Onebasicpresumptionunderpinningthenursingprocess
istheindividualizationofnursingcareandpatients’active
engagementintheirowncare.Innursingitisimportantto
acknowledgethepatientsintheirlifecontext,whichincludes
thefamily,buttheICFhasastrongfocusontheindividualand
doesnotincludeafamilyperspective.Thisfindinglimitsthe
use-fulnessofICFforrepresentingfamily,orgroup-baseddescriptionsof healthstatus,and,asaconsequence,hindersthecomparisonand crossreference offamily-based conceptsfromnursing, e.g. Nurs-ingMinimumDataSets[28].Surprisingly,patientparticipation
isdifficulttoexpressusingspecifictermsintheICF.Patient
participationismerelyusedasanoverarchingconceptinthe
ICFandthusmoreprecisetermsdescribingactual
participa-tionarelackingintheICF.ThetermsintheICFreflectmore
ofanassumingly objectiveassessmentofaperson’shealth
asdescribedbyhealthprofessionalsandnotbythepatients
themselves asactiveparticipantsincare.Asubjective
per-spective(e.g.,regardingfeelingsemanatingfromapatient’s
perceptionsandpreferences)isnotpossibletodescribeusing
theICF.Further,aperson’ssenseofqualityoflifeand
well-beingassubjectivedescriptions,presentintheVIPSmodel,is
notpossibletostateusingtheICF,butthedescriptions
pro-videdbytheICFtermscanbeseenasoperationalizationsof
amoreobjectivewell-being[12].TheICFneedstoexpandin
theseareastoincludeconceptsofqualityoflife,andthismight
alsoinvolveexpandingtheconceptualmodelofICFwith
qual-ity oflifeandhumandevelopment,as hasbeensuggested
intheliterature[29].Suggestionshavepreviouslybeenmade
regardingtheneedtoexpandtheICFclassification,toconduct
amultidisciplinaryclinicalmodificationtograsptheneedsof
allprofessionalsgroups[30],andthefindingsfromthisstudy
supportthissuggestion.IntheICFthereisaneedformore
specificterms(e.g.,skincondition,self-careandnutrition)in
severalareasofcentralimportancefornursing.Informationof
apatient’sskinconditionisanimportantpartofnurse
assess-ment, regardlessof clinical specialty. In the ICFprotective
functionsoftheskin(b810)coverarangeofhealthconditions
(e.g.,callusformation,hardeningandimpairments,suchas
skinlesions,ulcers,bedsoresandthinningofskin).More
spe-cifictermsareneededintheICFtodescribeskinconditions
regardingcolor,cleanness, injuries,dryness,rashandstate
ofhealingthatcannotbeexpressedinthecurrentversionof
theICF.Anotherareaofvitalconcernfornursingisself-care.
Inthisrespect,theICFistoogeneral,i.e.,itdoesnotprovide
termsatasufficientlevelofdetail.ByusingtheICF,a
descrip-tioncanbemadeofapatienthavingproblemswithself-care
(d5),e.g.,withwashingoneself(d510)(moreprecisely,washing
wholebody,d5101).Inadditiontothis,nursesneedtoconvey
assistapatient(e.g.,ifthereisaproblemforthepatientin
reachingvariouspartsofhisorherbody,usingtheshoweror
thesoap,orknowingtheproperorderinperformingpersonal
hygiene).
TheICFisusefulindescribingapatient’shealthstatuson
adetailedlevel. However,previous reportshaveshownthe
limitedusefulnessoftheICFindocumentingnursing
diag-noses[17]ortocrossreferencenursingdiagnosticconcepts
[28].ThislimitationisbecausetheICFdoesnotmeetcurrently
establishedqualitycriteriafornursingdiagnosis[16].
To reach a domain-specific (e.g., nursing) analysis of a
patient’s situation,asuitable theoretical framework
under-pinningtheprofessionalperspectiveinquestionisrequired.
Suchaframeworkwould alsohelpintheguidanceofwhat
dataandinformationareimportantinassessingthecurrent
situationand formaking interpretationsofthe assessment
findings.
5.1. Methodologicalconsiderations
TheuseoftheVIPSmodeltodepictcorenursingcontentfor
mappingwiththeICFstrengthenedthestudysinceitisawell
researchedand validated modeltodocument nursing
con-tentinpatienthealthrecordswhichiswidelyusedinvarious
clinicalareasofnursingcare,bothnationallyand
internation-allyinEurope.Inthisstudywechoosetoperformamapping
procedurebetweentheICFtermsandhealthstatuscontent
describedintheVIPSmodel.Nursingdiagnosesconceptswere
notincludedinthemappingastheICFtermsarenotcoherent
withthecurrentwayofstructuringandstatingnursing
diag-noses[1,2,16,17].Themappingprocedurehasbeenconducted
byresearcherswellacquaintedwithboththeVIPSmodeland
theICF,andrepeateddiscussionsamongtheauthorsyielded
consensusregardingthemappingofspecificterms.Initially
anattemptwasdonetoutilizemoreexplicitjudgment
cat-egoriesinthemapping:perfectmatch,broaderornarrower
concept.However,thatstrategywasabandonedsincethetwo
conceptualmodelscomprisetermsonquitedifferentlevels,
anditwasanticipatedthatthetermsintheICFweregenerally
describedonamoredetailedlevel.Atthesametimeabroader
conceptcouldalsobefoundhighupintheclassification
hier-archyoftheICF.Adecisionwasmadetoidentifyconceptual
comprehensivenessandcompletenessbetweenthetwo
mod-els.TheoriginalICFclassificationwasusedinthisstudyand
possiblysomeoftheareasthatweremissing(e.g.,relatedto
termsforchildren)mighthavebeenidentifiediftheICF-CY
classificationhadalsobeenused.
6.
Conclusion
and
clinical
implication
Thisstudy addressedthe content coverage ofthe ICFas a
standardizedclassificationfromanursingpointofview.The
findings indicated some problems in using a classification
developedfromacertainprofessionalperspectivethataimsto
coverthatfieldofknowledgeandhealthcareactivityasa
uni-fyingclassificationforanotherprofessionalgroupinhealth
care– in this case nursing. The VIPS and the ICF operate
ondifferentlevels:hence,withsomedegreeofoverlapping
ofthe twoclassificationsystems, theycouldco-exist inan
EHR.TheICFclassificationprovidesdetailsonfourlevelsthat
willbenecessary forcomprehensivedocumentation inthe
healthrecord.However,theICFdoesnotprovideenough
cov-erageanddetailinsomeareasandaspectsofvitalimportance
innursingcare.Further,thetheoretical frameworks
under-pinningthe VIPSmodelandthe ICF,aswell asdifferences
in structure, level of detail and degree of process
orienta-tionneedtobeacknowledged.IftheICFistobeusedinits
currentformandcontent,withouttheuseofadditional
sup-plementingnursing-specificcontent,thereisahighriskof
missingimportantdataandperspectivesonapatients
situ-ation,whichultimatelymayaffectthequalityandsafetyof
nursingcare.TheICFhasthepotentialformulti-professional
use,anddespiteitselaborateddetails,itneedstobedeveloped
andexpandedtoprovideacomprehensiveaccountfor
nurs-ingknowledgeinhealthcare.Furtherstudiesareneededto
addressthecontentoftheICFinrelationtonursingand
espe-ciallytheeffectofusingtheICFonpatientcareandnurses’
abilitytorecordandcommunicatenursing-specific
informa-tion.
Authors’
contribution
JF,AE,MEandCBdesignedandplannedthestudy,andwere
all activeinthemappingprocessandanalysesofthedata.
JFwasresponsiblefordraftingthemanuscriptwhileAE,ME
andCBmadecriticalrevisionsofthemanuscriptforimportant
intellectualcontent.
Conflict
of
interest
statement
Twooftheauthors(AEandME)aredevelopersandcopyright
holdersoftheVIPSmodel.
Summarytable
“Whatwasalreadyknownonthetopic?”
• TheVIPSmodelhasbeenwidelyusedandtestedin variousnursingcontexts.
• A multi-professional standardized terminology is neededinhealthcare.
• The ICF is suggested to provide a common frame-workandlanguageforallhealthprofessions,including nurses.
“Whatthisstudyaddedtoourknowledge?”
• ThisstudyinvestigatedthecontentvalidityoftheICF fromanursingperspective.
• TheICFcoversamostofthenursingcontentinthe VIPSmodelandoftenwithasufficientlevelofdetails.
• Corenursingtermsandnursingperspectivesare miss-ingintheICF.
• TheICFtermscanlargelybemappedtothekeywords forpatientstatusintheVIPSmodel.
Pleasecitethisarticleinpressas:J.Florin,etal.,AcomparisonbetweentheVIPSmodelandtheICFforexpressingnursingcontentinthehealth
ARTICLE IN PRESS
IJB-2881; No.ofPages10
10
international journal of medical informatics xxx (2012)xxx–xxxr
e
f
e
r
e
n
c
e
s
[1] NANDA,NursingDiagnoses.DefinitionsandClassification
2009–2011,WileyBlackwell,2009.
[2] ICN,InternationalClassificationforNursingPractice,2011,
Availablefrom:
http://www.icn.ch/pillarsprograms/international-classification-for-nursing-practice-icnpr/.
[3] InternationalHealthTerminologyStandardsDevelopment
Organisation,SNOMEDCT,2011,Availablefrom:
http://www.ihtsdo.org/snomed-ct/.
[4] WorldHealthOrganization,InternationalClassificationof
Diseases,2011,Availablefrom:
http://apps.who.int/classifications/icd10/browse/2010/en.
[5] WorldHealthOrganization,InternationalClassificationof
Functioning,DisabilityandHealth,2011,Availablefrom:
http://www.who.int/classifications/icf/en/.
[6] M.Ehnfors,I.Thorell-Ekstrand,A.Ehrenberg,Towardsbasic
nursinginformationinpatientrecords,VårdiNorden21
(3–4)(1991)12–31.
[7] SFS,Patientdatalag2008:355(SwedishforPatientDataAct
2008:355),2008,Availablefrom:
http://www.notisum.se/rnp/sls/lag/20080355.htm.
[8] A.Ehrenberg,M.Ehnfors,I.Thorell-Ekstrand,Nursing
documentationinpatientrecords:experienceoftheuseof
theVIPS-model,J.Adv.Nurs.24(1996)853–867.
[9] M.Ehnfors,A.Ehrenberg,I.Thorell-Ekstrand,The
developmentanduseoftheVIPS-modelintheNordic
countries,in:N.Oud(Ed.),ACENDIO2002.Proceedingsofthe
specialconferenceoftheAssociationofCommonEuropean
NursingDiagnoses,InterventionsandOutcomesinVienna,
VerlagHansHuber,Bern,2002,pp.139–168.
[10] C.Björvell,R.Wredling,I.Thorell-Ekstrand,Long-term
increaseinqualityofnursingdocumentation:effectsofa
comprehensiveintervention,Scand.J.CaringSci.16(2002)
34–42.
[11] WHO,InternationalClassificationofFunctioning,Disability
andHealthforChildrenandYouth,2011,Availablefrom:
http://www.who.int/mediacentre/news/releases/2007/pr59/en/.
[12] A.Cieza,G.Stucki,Theinternationalclassificationof
functioningdisabilityandhealth:itsdevelopmentprocess
andcontentvalidity,Eur.J.Phys.Rehabil.Med.44(2008)
303–313.
[13] P.M.Kearney,J.Pryor,Theinternationalclassificationof
functioning,disabilityandhealth(ICF)andnursing,J.Adv.
Nurs.46(2)(2004)162–170.
[14] M.Mueller,C.Boldt,E.Grill,R.Strobl,G.Stucki,
IdentificationofICFcategoriesrelevantfornursinginthe
situationofacuteandearlypost-acuterehabilitation,BMC
Nurs.3(2008)7,http://dx.doi.org/10.1186/1472-6955-7-3.
[15] ISO/TC215/WG3/CD18104,IntegrationofaReference
TerminologyModelforNursing,InternationalStandards
Organization,Geneva,Switzerland,2002,
http://www.tc215.wg3.nhs.uk/docs/wg3148.pdf.
[16] M.Muller-Staub,M.-A.Lavin,I.Needham,T.VanAchterberg,
Meetingthecriteriaofanursingdiagnosisclassification:
evaluationofICNPs,ICF,NANDAandZEFP,Int.J.Nurs.Stud.
44(2007)702–713.
[17] M.M.Heinen,T.VanAchterberg,G.Roodbol,M.A.Frederiks,
ApplyingICFinnursingpractice:classifyingelementsof
nursingdiagnoses,Int.Nurs.Rev.52(2005)304–312.
[18] A.Rauch,I.Kirchberger,C.Boldt,A.Cieza,G.Stucki,Does
thecomprehensiveinternationalclassificationof
functioning,disabilityandhealth(ICF)coresetfor
rheumatoidarthritiscapturenursingpractice?ADelphi
survey,Int.J.Nurs.Stud.46(2009)1320–1334.
[19] J.Pryor,R.Forbes,L.Hall-Pullin,Isthereevidenceofthe
internationalclassificationoffunctioning,disabilityand
healthinundergraduatenursingstudents’patient
assessments?Int.J.Nurs.Pract.10(2004)134–141.
[20] X.Zhu,J.-W.Fan,D.M.Baorto,C.Weng,J.J.Cimino,Areview
ofauditingmethodsappliedtothecontentofcontrolled
biomedicalterminologies,J.Biomed.Inform.42(3)(2009)
413–425.
[21] Socialstyrelsen.Klassifikationavfunktionstillstånd,
funktionshinderochhälsa(SwedishversionofInternational
ClassificationofFunctioning,DisabilityandHealth),
Socialstyrelsen,2003,Availableat
http://www.socialstyrelsen.se/publikationer2003/2003-4-1.
[22] T.Y.Kim,A.Coenen,N.Hardiker,Aqualityimprovement
modelforhealthcareterminologies,J.Biomed.Inform.43
(2010)1036–1043.
[23] T.Y.Kim,A.Coenen,TowardharmonizingWHO
internationalclassifications:anursingperspective,Inform.
HealthSoc.Care36(1)(2011)35–49.
[24] A.Cieza,G.Stucki,Contentcomparisonofhealth-related
qualityoflife(HRQOL)instrumentsbasedonthe
internationalclassificationoffunctioning,disabilityand
health(ICF),Qual.LifeRes.14(5)(2005)1225–1237.
[25] J.Wasiak,M.McMahon,S.Danilla,A.Spinks,H.Cleland,B.
Gabbe,Measuringcommonoutcomemeasuresandtheir
conceptsusingtheinternationalclassificationof
functioning,disabilityandhealth(ICF)inadultswithburn
injury:asystematicreview,Burns37(2011)913–924.
[26] S.Riva,M.Bullinger,E.Amann,S.vonMackensen,Content
comparisonofhaemophiliaspecificpatient-ratedoutcome
measureswiththeinternationalclassificationof
functioning,disabilityandhealth(ICF,ICF-CY),HealthQual.
LifeOut.8(2010)129,http://www.hqlo.com/content/8/1/
139.
[27] K.Berg,H.Finne-Soveri,L.Gray,J.C.Henrard,J.Hirdes,N.
Ikegami,G.Ljunggren,J.N.Morris,L.Paquay,L.Resnik,G.
GaryTeare,RelationshipbetweeninterRAIHCandtheICF:
opportunityforoperationalizingtheICF,Brit.HealthServ.
Res.47(2009),http://dx.doi.org/10.1186/1472-6963-9-47.
[28] W.Goossen,Cross-mappingbetweenthreeterminologies
withtheInternationalStandardNursingReference
TerminologyModel,Int.J.Nurs.Terminol.Classif.17(4)
(2006)153–164.
[29] J.McDougall,V.Wright,P.Rosenbaum,TheICFmodelof
functioninganddisability:incorporatingqualityoflifeand
humandevelopment,Dev.Neurorehabil.13(3)(2010)
204–211.
[30] Y.Heerkens,Y.VanderBrug,H.T.Napel,D.VanRavensberg,
PastandfutureuseoftheICF(formerICIDH)bynursingand
alliedhealthprofessionals,Disabil.Rehabil.25(11–12)(2003)
![Fig. 2 – The international classification of functioning, disability and health [5].](https://thumb-us.123doks.com/thumbv2/123dok_us/1733769.2743598/3.918.86.837.111.781/fig-international-classification-functioning-disability-health.webp)