S U P P L E M E N T A R T I C L E
Update on Vaccine Liability in the United States:
Presentation at the National Vaccine Program Office
Workshop on Strengthening the Supply of Routinely
Recommended Vaccines in the United States,
12 February 2002
Geoffrey EvansNational Vaccine Injury Compensation Program, Health Resources and Services Administration, Department of Health and Human Services, Rockville, Maryland
Two decades ago, a liability crisis brought on by concerns about the safety of diphtheria and tetanus toxoids and pertussis vaccine led to supply shortages and calls for rationing of the vaccine. Vaccine prices skyrocketed, and research on new products was threatened. In response, Congress created the National Vaccine Injury Com-pensation Program, which is tort reform legislation designed to compensate individuals quickly, easily, and generously. Since 1988, the Vaccine Injury Compensation Program has stabilized the marketplace, as evidenced by high immunization rates, stable pricing, and an increasing number of vaccine candidates in development. Although current vaccine shortages do not appear to be related to issues of liability, a new wave of tort litigation alleging that some vaccines cause autism has led to speculation that history could repeat itself.
In the 1980s, shortages of diphtheria and tetanus tox-oids and pertussis (DTP) vaccine supplies occurred af-ter hundreds of lawsuits alleging that the vaccine caused injury and death were filed against vaccine manufac-turers and administrators [1]. The costs of defending against and potentially providing compensation to hun-dreds of claimants led many companies to cease pro-duction of the vaccine. By 1984, calls for the rationing of DTP vaccine were further proof of a deteriorating marketplace. In addition, exponential increases in vac-cine prices, the uncertainty of vacvac-cine research and de-velopment, and the real possibility of disease outbreaks all made it clear that something had to be done quickly.
Viewpoints expressed in this article do not necessarily represent the views of the Department of Health and Human Services.
Reprints or correspondence: Dr. Geoffrey Evans, National Vaccine Injury Compensation Program, Health Resources and Services Administration, Department of Health and Human Services, 5600 Fishers Ln., Rm. 11C-26, Rockville, MD 20857 ([email protected]).
Clinical Infectious Diseases 2006; 42:S130–7
This article is in the public domain, and no copyright is claimed. 1058-4838/2006/4205S3-0007
An informal coalition of parents, physicians, attorneys, and representatives of the vaccine industry convinced Congress to pass compromise legislation known as the National Childhood Vaccine Injury Act of 1986 (NCVIA). A key component of the act, the National Vaccine Injury Compensation Program (VICP), be-came operational 2 years later.
The controversy regarding injuries and illnesses caused by vaccines weighed heavily in creating the VICP’s framework and the NCVIA’s sweeping vaccine safety provisions. The US federal government was es-sentially brought into a full-time vaccine safety role. The NCVIA included a mandate for reporting adverse events listed on a newly created table of medical ditions (“Vaccine Injury Table”), as well as any con-traindicating reaction to a vaccine that is specified in the manufacturer’s package insert. These reports are made to the Vaccine Adverse Event Reporting System. Other vaccine safety mandates included office record-keeping (i.e., documenting the date of vaccine admin-istration, the manufacturer and lot number, and the name and address of the administrator), development
by guest on July 17, 2016
http://cid.oxfordjournals.org/
of risk-benefit information materials (“Vaccine Information Statements”), and Institute of Medicine (IOM) studies of ad-verse events associated with covered vaccines.
The NCVIA also provided for 2 advisory panels, the Advisory Commission on Childhood Vaccines and the National Vaccine Advisory Committee. Mirroring the forces underlying passage of the NCVIA, the Advisory Commission on Childhood Vac-cines comprises parents, physicians, and attorneys (bringing petitioner and industry perspectives), whose charge it is to monitor the VICP. The Advisory Commission on Childhood Vaccines makes recommendations to the Secretary of the US Department of Health and Human Services (DHHS) by ad-vising on changes to the Vaccine Injury Table and by moni-toring vaccine safety.
The National Vaccine Advisory Committee has much broader responsibilities of reviewing and making recommen-dations concerning research on and production, delivery, safety, and efficacy of vaccines. Recommendations are forwarded to the DHHS Assistant Secretary for Health and have included ad hoc committee reviews of the risks associated with each of the vaccines listed in the Vaccine Injury Table.
BACKGROUND, STRUCTURE, AND PROCESS The VICP was designed to address a variety of public policy needs [2–4]. First, and most important, it is only simple justice that individuals who are inadvertently injured by properly pro-duced vaccines that are administered through public health programs should receive compensation. Because society man-dates the use of vaccines, through state laws for school en-rollment, it is reasonable and appropriate that society take re-sponsibility for unavoidable adverse outcomes associated with the use of vaccines. Second, the delays and uncertainties of the tort system warranted a more reasonable and fair approach. Third, disruptions of vaccine production and supply would inevitably lead to serious outbreaks of otherwise preventable disease. Fourth, the unprecedented vaccine price increases were caused largely by the projected costs of litigation, as calculated by the manufacturers. Fifth, the increasing scientific capability for the production of new and improved vaccines obviously required considerable interest and investment on the part of biologics manufacturers. The litigious climate surrounding the use of vaccines was detrimental to such efforts. Finally, there was no evidence that the problem of vaccine liability was going to disappear, particularly in view of the attention devoted to it by the media.
Congress addressed these needs by creating a federal no-fault system under which awards can be made to individuals who are injured by vaccines quickly, easily, and generously. Persons injured through the receipt of a vaccine are required to file claims with the VICP before they are allowed to bring a civil
lawsuit. Rules of evidence, discovery, and other legal procedures are relaxed, to accelerate the compensation process. Negligence on the part of the manufacturer or health care provider is removed from proceedings—thus, the “no-fault” designation. Judgments (whether dismissing the claim or awarding com-pensation) must be expressly rejected by the petitioner before a civil lawsuit can be filed. Once a judgment is rejected, a person essentially forfeits any right to compensation under the pro-gram and can seek remedies only through other channels.
Additional protections for manufacturers were provided for lawsuits filed outside the VICP. These protections in-cluded the elimination of plaintiff allegations of vaccine mis-design or inadequate warning of risk, which were 2 common tort theories pursued in the 1980s, and the elimination of punitive damages, unless it could be proven that production of the vaccine was marred by fraud, intentional wrongdoing, or criminal activity [5].
A unique feature of the Act was creation of the Vaccine Injury Table and its definitional counterpart, the Qualifications and Aids to its Interpretation (“Aids to Interpretation”) [6, 7]. In-dividuals may receive compensation if they can prove, by a preponderance of the evidence (i.e., more likely than not) that an injury listed in the Vaccine Injury Table occurred within the prescribed time frame. The government may successfully counter this allegation with greater evidence of an alternate cause. However, this “factor unrelated to the vaccine” cannot include “any idiopathic, unexplained, unknown, hypothetical, or undocumentable injury, illness or condition.” It can include “infection, toxins, trauma, or metabolic disturbances” [8]. This simplified approach greatly reduces the burden of proving cau-sation, which is necessary in civil courts to prove the occurrence of medical malpractice.
The VICP involves 3 governmental entities: the DHHS, the Department of Justice (DOJ), and the US Court of Federal Claims. Petitioners, either through an attorney or on their own, file a petition with the DHHS and the Court, which begin the review and adjudication process. A physician or nurse in the DHHS Health Resources and Services Administration’s Divi-sion of Vaccine Injury Compensation has 90 days to review the documents The medical staff develops a recommendation for or against entitlement to compensation, which is then for-warded to the Court through the DOJ attorney assigned to the case. A distinguished group of pediatric and adult medical sub-specialists may, at times, assist VICP staff in reaching a decision on eligibility, and they routinely testify on behalf of the Sec-retary in hearings.
As an initial matter, eligibility for receiving compensation is based on proving 1 of 3 elements: (1) an injury listed on the Vaccine Injury Table occurred during the prescribed interval; or (2) the vaccine actually caused the injury, if it is listed in
by guest on July 17, 2016
http://cid.oxfordjournals.org/
the Table, but the injury either occurred after the specified interval or is not listed; or (3) the vaccine significantly aggra-vated a preexisting medical condition. Petitioners are not eli-gible to receive compensation, however, if the Court determines that there is greater evidence of a non–vaccine-related cause for the injury.
In addition to satisfying one of these elements, petitioners
must also show that there were continued effects for16 months,
except in the case of a related death or if the vaccine-related injury necessitated “inpatient hospitalization and sur-gical intervention.” This latter exception was added by Congress in 2000, because infants who experience intussusception (an adverse event causally related to some rotavirus vaccines) usu-ally recover completely and, therefore, would not satisfy the “continued effects” provision. Language was passed providing eligibility for compensation for those infants who were hos-pitalized and underwent surgery [9].
Final decisions are made by special masters, court-appointed lawyers with expertise in the legal and medical issues associated with adverse reactions to vaccines. Eligibility for compensation is recommended if the VICP and DOJ staff find that the records fulfill the requirements of the Act. The court nearly always concurs with an entitlement recommendation, thereby obvi-ating the need for a hearing.
When entitlement to compensation is conceded, the DOJ and the petitioner try to reach agreement on the amount of compensation (damages). The level of compensation is often based on lifelong care plans that evaluate the health of the injured person and the person’s future needs. The government and petitioner often use informal negotiations under the guid-ance of a special master to resolve entitlement and damages issues. Alternative dispute resolution is increasingly being used to avoid having to hold a formal hearing.
Those cases not conceded by the DHHS usually proceed to a hearing before a special master, at which point, testimony from both sides is presented, including testimony from medical expert witnesses for each party. After hearing testimony from both sides, the Court engages in an evaluation of the weight and credibility of the evidence. This may or may not result in an award of compensation.
Compensation for minors or incompetent persons is usually in the form of a lump-sum payment and an annuity designed to provide a lifetime stream of benefits. Elements of compen-sation include medical care, lost wages, and pain and suffering. Compensation for death claims is awarded in a lump-sum pay-ment capped at $250,000. “Reasonable” attorneys’ fees and costs are paid whether or not petitioners are successful in ob-taining compensation, if the claim is brought in good faith and on a reasonable basis. Punitive damages and awards to others in the family for loss of companionship are not allowed.
Decisions of the special masters may be appealed by either
party to a judge of the Court of Federal Claims and then to the US Court of Appeals for the Federal Circuit. One VICP case decided by the Federal Circuit was reviewed by the Su-preme Court.
One provision omitted from the 1986 legislation was a mech-anism for adding new vaccines to the VICP. The Omnibus Budget Reconciliation Act of 1993 corrected this omission by mandating that vaccines recommended by the Centers for Disease Control and Prevention (usually on the basis of a vote by the Advisory Committee on Immunization Practices) for routine administra-tion to children be added to the VICP [10]. However, it is only after enactment of an excise tax by Congress that the vaccine is officially covered by the program. Once the vaccine is added, there are 8 years of retroactive coverage (based on the effective date of the excise tax) for individuals alleging that injury resulted from administration of vaccines before the start of coverage, with a 2-year window in which to file these “older” claims. For newly added vaccines, adverse events occurring during prelicensure clinical trails may be eligible for compensation, although the VICP has yet to receive such a claim.
IMPLEMENTATION AND PROGRAM EXPERIENCE
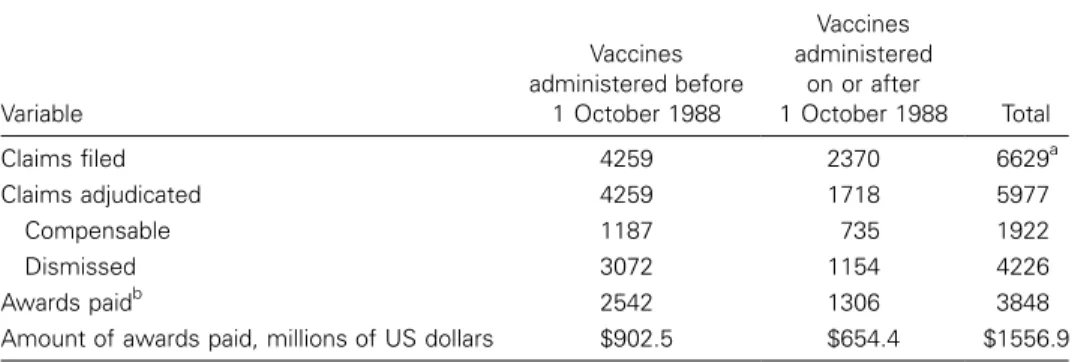
The VICP began receiving claims on 1 October 1988, which is the date of enactment and differentiates 2 categories of peti-tioners. Retrospective claims, which are for vaccines adminis-tered before 1 October 1988, had to be filed by 31 January 1991. Thousands of claims, nearly one-third of which involved vaccines administered during the 1950s and 1960s, were filed by the deadline (table 1). Compensation was paid from the appropriations from the Treasury authorized by Congress each year. As of September 2004, all retrospective claims had been adjudicated.
Prospective claims are for vaccines administered on or after 1 October 1988. These claims must be filed either within 36 months after the first postvaccination symptom appears or, in the case of a death, within 24 months of the death and within 48 months after the onset of the vaccine-related injury that resulted in death.
Funding is provided through a tax of $0.75 placed on each dose (or disease prevented) of designated childhood vaccine. For example, the excise tax on diphtheria and tetanus toxoids and acellular pertussis vaccine is $2.25, whereas the tax on inactivated poliovirus vaccine is $0.75 [11]. (Initially, the tax was determined on the basis of estimates of awards related to each vaccine.) As of July 2005, the Vaccine Injury
Compen-sation Trust Fund contained1$2.1 billion, compared with
av-erage outlays of∼$61 million annually over the previous 6 years.
Monies from the trust fund can be used only for VICP com-pensation and for administrative expenses of the DHHS, the DOJ, and the Court.
by guest on July 17, 2016
http://cid.oxfordjournals.org/
Table 1. Status of the National Vaccine Injury Compensation Program, as of 31 May 2005. Variable Vaccines administered before 1 October 1988 Vaccines administered on or after 1 October 1988 Total Claims filed 4259 2370 6629a Claims adjudicated 4259 1718 5977 Compensable 1187 735 1922 Dismissed 3072 1154 4226 Awards paidb 2542 1306 3848
Amount of awards paid, millions of US dollars $902.5 $654.4 $1556.9
a
Does not include 4744 claims in the Omnibus Autism Proceeding, for a total of 11,373 claims filed. b
Includes attorney fee awards. Some adjudicated claims for which data are shown above have not yet been processed for payment.
As of July 2005, the VICP covered Haemophilus influenzae
type b (Hib); diphtheria, tetanus, and pertussis (e.g., DTP, DTaP, DT, TD, and TT); measles, mumps, and rubella (MMR, MR, M, and R); poliovirus (both inactivated poliovirus and oral poliovirus); hepatitis B virus (HBV); varicella-zoster virus (VZV); rotavirus (RV); pneumococcal conjugate (PCV); and trivalent influenza virus (TIV and LAIV). Over the history of the program, the majority (61%) of claims alleged the
occur-rence of DTP-related effects. In contrast,!200 claims alleging
injuries related to receipt of diphtheria and tetanus toxoids and acellular pertussis vaccine had been filed by mid-2005.
The breakdown of the remaining cases is as follows: 14% involved MMR vaccine, given alone or in any combination (approximately one-fifth of these cases involve adults alleging rubella vaccine–related injury), 7% involved HBV vaccine, 5% involved oral poliovirus vaccine, 4% involved inactivated po-liovirus vaccine (except for 3 claims, all for vaccines admin-istered before 1970), and 3% involved tetanus-containing vac-cines. Other than for HBV vaccine, only small numbers of claims have been filed for the newly added vaccines. (Not
in-cluded in these percentages are 14700 “unspecified” claims,
which allege injury resulting from multiple vaccines as part of the MMR, thimerosal, and autism litigation (see Public Policy Outcomes). Overall, injuries account for 86% of claims, and deaths account for 14% of claims.
MODIFYING THE VACCINE INJURY TABLE By law, the Vaccine Injury Table and Aids to Interpretation can be modified or amended by DHHS regulation in consultation with the Advisory Commission on Childhood Vaccines, after the public has had opportunity to comment. Separate efforts by the VICP to modify the Vaccine Injury Table and Aids to Interpretation began with publication of the 2 Congressionally mandated IOM reviews in 1991 and 1994, respectively [12–15]. The first set of changes, effective 10 March 1995, added the injury of chronic arthritis for rubella-containing vaccines and
removed shock-collapse and residual seizure disorder for the DTP vaccine [16]. Clarifications were also made in the defi-nitions of residual seizure disorder and encephalopathy in the Aids to Interpretation. The changes to the Vaccine Injury Table and Aids to Interpretation for DTP vaccine generated contro-versy and eventually drew the attention of Congress.
The second set of changes to the Vaccine Injury Table was far less controversial and was based on the 1994 IOM report covering the 5 remaining VICP vaccines, as well as Hib and HBV vaccines [17]. As mandated by the Omnibus Budget Rec-onciliation Act of 1993, Hib, HBV, and varicella-zoster virus vaccines were added to the VICP, because all of them were recommended by Centers for Disease Control and Prevention for routine administration to children. The other modifications, effective 24 March 1997, included the addition of thrombo-cytopenia to the Vaccine Injury Table, for measles virus–con-taining vaccines, and brachial neuritis, for tetanus toxoids– containing vaccines. Coverage of the 3 new vaccines, however, did not begin until Congress established an excise tax effective 7 August 1997 [11].
Since then, the Vaccine Injury Table has been modified fur-ther, with the general category of rotavirus vaccine added, ef-fective 21 October 1998 [18], and pneumococcal conjugate vaccines added, effective 19 December 1999 [19, 20]. In a final rule published in July 2002, intussusception was added as a listed injury to the Vaccine Injury Table, under a second cat-egory of rotavirus vaccines (i.e., live, oral, and rhesus based); other technical changes were also added. Notices of coverage for hepatitis A virus vaccines and trivalent influenza virus
vac-cines were published in theFederal Registerin December 2004
and April 2005, respectively (see Current and Future Direc-tions) [21, 22].
PUBLIC POLICY OUTCOMES
Congress expected that the Act would, once and for all, address the liability and public health problems surrounding
by guest on July 17, 2016
http://cid.oxfordjournals.org/
Figure 1. Claims filed against US manufacturers of diphtheria and tetanus toxoids and pertussis vaccine and diphtheria and tetanus toxoids and acellular pertussis vaccine. **Denotes lawsuits alleging the development of autism (or other neurodevelopmental disorders) as a result of administration of vaccines, as of December 2004. Data are from the Division of Vaccine Injury Compensation, Health Resources and Services Administration, US Department of Health and Human Services.
nization. It would appear that the VICP has done so, in large
measure. First, compensation awards have been made to11900
families and individuals (apart from attorneys’ fees and costs in numerous other cases). Second, the marketplace is much more stable, with immunization rates at an all-time high and several new, recently licensed vaccines [23]. Annual Investi-gational New Drug requests to the Food and Drug Adminis-tration, a necessary step in beginning testing in human subjects, initially increased and have remained steady from 1986 to the present, signaling renewed confidence in vaccine research and development (data from the Center for Biologics Evaluation and Research, Food and Drug Administration). The dramatic increases in the prices of childhood vaccines of the past, which manufacturers associated with liability, have stopped. Today, vaccine prices reflect public- and private-sector purchase trends and the effects of inflation, rather than concerns about liability or repercussions. Although the supply shortages of childhood vaccines from 2000 to 2003 brought back memories of the vaccine shortages of 1980s, there is no evidence that liability concerns were responsible.
Another benefit of the NCVIA was the tort reform measures. The limited rules of discovery and the short, informal hearings that apply in VICP cases have eliminated or ameliorated many of the problems inherent in the tort system. Adjudication times for VICP cases are much shorter than those for the civil system,
averaging 3.0 years for vaccines administered after 1988. More-over, many of the hearings before the special masters are con-cluded within a day and are less adversarial than they were under the tort system. Program awards are generally structured to ensure petitioners a lifetime stream of benefits.
Perhaps the most important barometer of success of the NCVIA is civil litigation. The number of DTP vaccine–related claims against US companies had remained low for more than a decade (figure 1). Some recent lawsuits involving cases already adjudicated by the VICP have already been dismissed, whereas others are still pending adjudication. Although claims against health care providers are more difficult to track, there is no indication that the liability experience of these providers is any different from that of manufacturers. However, a new trend in civil litigation appears to have the potential to adversely affect future vaccine supplies.
Starting in 2001, individual and class action lawsuits were filed in state and Federal courts alleging that the MMR vaccine or vaccines containing thimerosal, an ethylmercury compound used as a preservative for decades in the formulation of many routine childhood vaccines, caused autism (or other
neuro-developmental disorders). By the end of 2004,1350 lawsuits
against vaccine manufacturers and administrators were pending
in120 states [24], despite the fact that IOM reports in 2001
found no proven evidence of a causal relationship between
by guest on July 17, 2016
http://cid.oxfordjournals.org/
receipt of childhood vaccines and the development of autism (or other neurodevelopmental disorders) [25, 26]. More sig-nificantly, in a follow-up report, the IOM concluded that there is proven evidence against a causal relationship between both MMR vaccines and thimerosal-containing vaccines and autism, on the basis of controlled epidemiological studies published in the interim [27].
Although the NCVIA requires individuals alleging vaccine-related injuries for covered vaccines to first file with the VICP before pursuing civil actions, many plaintiffs adopted several strategies to circumvent this requirement. Plaintiffs argue that their actions are not governed by the VICP, because they allege that thimerosal is an “adulterant” to, and not a part of, vaccines. This argument hinges on the Act’s definition of a “vaccine-related injury or death,” which excludes any injury or death associated with an adulterant or contaminant intentionally added to a cov-ered vaccine [28]. Over time, courts are rejecting this argument dismissing “individual lawsuits” filed on behalf of an injured party, usually a child, who is alleged to be developmentally im-paired. Others, so-called “derivative claims,” filed on behalf of parents or other family members seeking damages for certain losses (e.g., companionship, consortium, or services) are often allowed to continue, because these types of damages are not covered under the Act. Plaintiffs are also filing “medical moni-toring” class action lawsuits that do not allege specific injuries, but, instead, demand the costs of medical monitoring to deter-mine whether thimerosal-related injuries will develop in the fu-ture. Individuals numbering in the thousands to millions are each seeking $999.00 in damages, a strategy based on the Act’s prohibiting individuals from suing a vaccine company of
ad-ministrator for damages1$1000.00 [29]. Most of these lawsuits
were being dismissed by early 2005 [24].
In late 2001, in addition to civil litigation, the VICP began receiving claims alleging vaccine-related autism, first for MMR vaccine (which is an attenuated live, viral vaccine and has never contained thimerosal), and then for a variety of other childhood vaccines. More recently, claims have been filed alleging thi-merosal-related injury associated with several different vaccines (e.g., DTP, Hib, and HBV vaccines). Some of these filings in-clude individuals who had pursued an adulterant theory in civil courts and were subsequently dismissed in pretrial motions.
In recognition of the likelihood of large numbers of claims, the Court set up a unique proceeding allowing the filing of simple petitions without accompanying medical records or other supporting documents (e.g., affidavits). General Autism Order I, which was issued on 2 July 2002, outlined a 2-step process of discovery followed by an evidentiary hearing on the merits of causation generally [30]. A decision on injuries and illnesses caused by vaccines, expected by 2 July 2004, would
then be applied to individual claims. As of July 2005, 14700
claims had been filed for inclusion in the Omnibus Autism
Proceeding, and discovery was ongoing. Petitioners may opt out of the autism proceeding, either to pursue their case in-dividually within the VICP or to withdraw in order to seek remedies in the tort system if the NCVIA’s requirements are satisfied. Several dozen petitioners had withdrawn their claims as of July 2005. The Court is expected to issue a new hearing date on causation once the discovery process nears completion. CONGRESSIONAL OVERSIGHT
In recent years, Congress has increased its oversight of the VICP. Criticism has focused on the adversarial nature of the program, the time required for adjudication, the changes to the Vaccine Injury Table, the huge surplus in the trust fund, and the fact that the public is not well informed about the existence of the VICP. In reports issued in December 1999 and March 2000, the General Accounting Office found the VICP adjudication process to be easier than the traditional tort system but not as streamlined as Congress had originally intended [31, 32]. More-over, although there appeared to be a scientific basis for the changes to the Vaccine Injury Table made by the DHHS, the General Accounting Office found some inconsistencies in ap-plying results of the IOM studies. As for the trust fund, so-lutions varied depending on stakeholder perspective, with pe-titioners wanting more claims compensated by decreasing the burden of proof, vaccine manufacturers wanting the tax re-duced to reduce costs, and researchers calling for a portion of incoming revenues annually to pay for vaccine safety research and surveillance.
In the end, the only recommendation of the General Ac-counting Office was that the DHHS publish a clear methodology for future changes to the Vaccine Injury Table, to help ensure that the changes are perceived as being fair. The second report, which focused only on the trust fund, had no recommendation. In September 1999, the Subcommittee on Drugs and Crim-inal Justice, which is part of the House Government Reform Committee, held the first of 3 hearings on the VICP. Two more hearings by the full committee followed in November and De-cember 2001. The parents of injured children, petitioners’ at-torneys, medical experts, and representatives of the program testified. In October 2000, a bipartisan report released by the Subcommittee made the following recommendations: (1) a re-view of the Vaccine Injury Table to ensure the inclusion of current science; (2) the increased use of speedy informal dispute resolution; and (3) the development of an alternative standard for cases not related to the Vaccine Injury Table. The last rec-ommendation is proving to be the most challenging [33].
In contrast to the beginning of the VICP, when most claims alleged an injury listed on the Vaccine Injury Table, the majority of claims filed today allege conditions not listed in the Vaccine Injury Table. Admittedly, the 1995 modifications to the Vaccine Injury Table and Aids to Interpretation forced some claimants
by guest on July 17, 2016
http://cid.oxfordjournals.org/
to pursue their claims on a causation basis. Probably more significant has been the addition of new vaccines for which few injuries are listed in the Vaccine Injury Table. Since 1997, only 2 injuries have been added for the 7 new vaccines. Moreover, of nearly 450 claims related to HBV vaccine, none involve anaphylaxis or anaphylactic shock, the only condition listed for this vaccine on the Vaccine Injury Table. Having to pursue such claims on the basis of causation is more difficult, because pe-titioners are not afforded the presumption of causation given to petitioners bringing claims of injuries listed in the Vaccine Injury Table. It is also likely that a greater number of hearings on entitlement will be required.
The Subcommittee’s call for the development of an alternate standard reflects this reality and has led to developments in 2 areas. In December 2000, a proposal by the American Academy of Pediatrics to use a more relaxed standard for adjudicating injuries not listed in the Vaccine Injury Table was presented to the Advisory Commission on Childhood Vaccines [34]. Fur-thermore, 2 decisions by the Chief Special Master highlighted the complex challenge of determining causation in vaccine in-jury cases [35, 36]. As in the past, the US Court of Appeals for the Federal Circuit may rule on these interpretations of the NCVIA and render additional guidance on making causation in fact decisions.
By the spring of 2005, legislation introduced in the House contained various process improvements to the VICP, including increased compensation for death claims and an increase in the statute of limitations to 6 years for both injury and death claims [37]. A Senate bill introduced in the previous Congressional session was similar but also included additional language aimed at tightening the restrictions on filing of lawsuits in the civil system without first filing with the VICP [38]. Neither bill has been acted upon by the time of publication.
CURRENT AND FUTURE DIRECTIONS
During the 1990s, some experts suggested adding more selec-tive-use vaccines (e.g., influenza virus and pneumococcal poly-saccharide vaccines, which are used primarily for adults) to the VICP. A National Vaccine Advisory Committee review in 1996 found little evidence to support the need, on the basis of liability concerns expressed by manufacturers and health care providers [39]. However, with studies showing increased morbidity due to influenza among preschool-aged children, the Centers for Disease Control and Prevention formally recommended influ-enza virus vaccine for routine use in 6–23-month-old children, commencing with the 2004–2005 influenza season [40]. Passage of the American Jobs Protection Act of 2004 led to imposition of excise taxes on trivalent influenza virus vaccines administered during each influenza season (both the injectable and nasal spray products) and on hepatitis A vaccines [41]. Notices of
Coverage were published in the Federal Register announcing
that 1 December 2004 and 1 July 2005 would be the effective dates of coverage for hepatitis A virus and trivalent influenza virus vaccines, respectively [21, 22]. By specifying trivalent in-fluenza virus vaccines for coverage, Congress chose to distin-guish between adding to the VICP routine trivalent vaccines administered annually in seasonal influenza campaigns and a future licensed monovalent product that would be used in a influenza pandemic. Legislation signed into law at the end of 2005 addressed liability protection for industry and limited compensation for individuals harmed by a vaccine, in the event of a future pandemic [42].
Another category of vaccines for possible inclusion are those for which development may be impeded by liability concerns. Vaccines against group B streptococci, cytomegalovirus, and respiratory syncytial virus disease, all of which cause significant morbidity and mortality among infants, are currently in de-velopment. Vaccination of pregnant women against these dis-eases holds great promise for protecting very young infants. Even though infants would receive the benefit of vaccination, the fact that the vaccines would not be administered directly to infants or children prevents their inclusion in the VICP, on the basis of current law. Adding this category of vaccine, how-ever, would require Congressional action [43].
In conclusion, the VICP appears to have satisfied the critical public policy concerns that brought about passage of the pro-gram nearly 20 years ago. The instability of the past is long gone, replaced by a more stable marketplace with the expec-tation of new, innovative products and technology. Although there is uncertainty over the autism litigation, there is reason to believe the VICP will continue to serve as a successful al-ternative to the tort system.
Acknowledgments
I thank Ward Sorensen, Tamara Overby, and Linda Rozzelle (Division of Vaccine Injury Compensation, Healthcare Systems Bureau, Health Re-sources and Services Administration, US Department of Health and Human Services) and Elizabeth H. Saindon, Emily Marcus Levine, and David E. Benor (Office of General Counsel, US Department of Health and Human Services) for their assistance in preparing the manuscript.
Potential conflicts of interest. G.E. is an employee of the US Depart-ment of Health and Human Services; he receives no financial support nor does he have financial interest in domestic or international vaccine companies.
References
1. Evans G, Harris D, Levine E. US law. In Plotkin SA, Orenstein WA, eds. Vaccines. 4th ed. Philadelphia: WB Saunders,2003:1591–617. 2. Public Law 99–660 § 311 et seq., US Statutes at Large 100: 3755, codified
at US Code 42 (1986), § 300aa-1, et seq.
3. Public Law 100–203, § 4301 et seq. US Statutes at Large 101: 1330–221, codified atUS Code42 (1987), § 300aa-1 et seq.
4. Smith MH. National Childhood Vaccine Injury Compensation Act. Pediatrics1988; 82:264–9.
5. US Code 42 § 300aa-23(d).
6. Code of Federal Regulations 42: 100.3.
7. US Department of Health and Human Services. National Childhood
by guest on July 17, 2016
http://cid.oxfordjournals.org/
Vaccine Injury Act: Vaccine Injury Table. Rockville, MD: US Depart-ment of Health and Human Services, 2005. Available at: http:// www.hrsa.gov/osp/vicp/table.htm. Accessed 8 November 2005. 8. US Code 42 § 300aa-13(a)(2).
9. Public Law 106–310 § 1701, US Statutes at Large 114 (2000): 1101. 10. Public Law 103–66, § 13632, US Statutes at Large 107 (1993): 565,
codified at US Code 42, § 300aa-14(e).
11. Taxpayer Relief Act of 1997, Public Law 105–34, § 904, US Statutes at Large 111 (1997): 251.
12. Institute of Medicine. Howson CP, Howe CJ, Fineberg HV, eds. Adverse effects of pertussis and rubella vaccines. Washington, DC: National Academy Press,1991.
13. Howson CP, Fineberg HV. The ricochet of magic bullets: summary of the Institute of Medicine report: adverse effects of pertussis and rubella vaccines. Pediatrics1992; 89:318–24.
14. Institute of Medicine. Stratton KR, Howe DJ, Johnston RB, eds. Ad-verse events associated with childhood vaccines: evidence bearing on causality. Washington, DC: National Academy Press,1994.
15. Stratton KR, Howe CJ, Johnston RB. Adverse events associated with childhood vaccine other than pertussis and rubella: summary of a report from the Institute of Medicine. JAMA1994; 271:1602–5. 16. Health Resources and Services Administration. “National Vaccine
In-jury Compensation Program: revision of the Vaccine InIn-jury Table,” Federal Register 60 (1995): 7678.
17. Health Resources and Services Administration. “National Vaccine In-jury Compensation Program: revisions and additions to the Vaccine Injury Table—II,” Federal Register 62 (1997): 7685.
18. Health Resources and Services Administration. “National Vaccine In-jury Compensation Program: addition of vaccines against rotavirus to the program,” Federal Register 64 (1999): 40517.
19. Health Resources and Services Administration. “National Vaccine In-jury Compensation Program: revisions and additions to the Vaccine Injury Table,” Federal Register 66 (2001): 36735.
20. Health Resources and Services Administration. “National Vaccine In-jury Compensation Program: revisions and additions to the Vaccine Injury Table,” Federal Register 67 (2002): 48558.
21. Health Resources and Services Administration. “National Vaccine In-jury Compensation Program: inclusion of hepatitis A vaccines in the Vaccine Injury Table,” Federal Register 69 (2004): 69945–6. 22. Health Resources and Services Administration. “National Vaccine
In-jury Compensation Program: addition of trivalent influenza vaccines to the Vaccine Injury Table,” Federal Register 70 (2005): 19092–3. 23. Centers for Disease Control and Prevention (CDC). National, state
and urban area vaccination coverage among children aged 19–35 months—United States, 2002. MMWR Morb Mortal Wkly Rep 2003; 53:728–32.
24. Moss R. Presentation at the 2nd Workshop on Vaccine Supply. Wash-ington, DC: 24 January2005.
25. Institute of Medicine. Measles-mumps-rubella vaccines and autism. Washington, DC: National Academy Press,2001.
26. Institute of Medicine. Thimerosal-containing vaccines and neurode-velopmental disorders. Washington, DC: National Academy Press, 2001.
27. Institute of Medicine. Vaccines and autism. Washington, DC: National Academy Press,2004.
28. US Code 42 § 300aa-33(5). 29. US Code 42 § 300aa-11(a)(2).
30. US Court of Federal Claims. Office of Special Masters: Omnibus autism proceeding. Washington, DC: US Court of Federal Claims,2005. Avail-able at: http://www.uscfc.uscourts.gov/OSM/OSMAutism.htm. Ac-cessed 28 June 2005.
31. General Accounting Office. Report to Congressional Requesters. Vac-cine Injury Compensation: program challenged to settle claims quickly and easily. Washington, DC: General Accounting Office,1999. 32. General Accounting Office. Report to Congressional Requesters.
Vac-cine Injury Trust Fund: revenue exceeds current need for paying claims. Washington, DC: General Accounting Office,2000.
33. US House of Representatives, Committee on Government Reform, Subcommittee on Criminal Justice, Drug Policy and Human Resources. The Vaccine Injury Compensation Program: addressing needs and im-proving practices. Washington, DC: US Government Printing Office, 2000.
34. Peter G. Proposed revisions to the Vaccine Injury Compensation Pro-gram. Presentation before the Advisory Commission on Childhood Vaccines. Washington, DC: 5 December2001.
35. Capizzano v. Sec. of HHS,00-729V Ct. Fed. Cl. (2004). 36. Althen v. Sec. of HHS,00–170 Ct. Fed. Cl. (2003).
37. National Vaccine Injury Compensation Program Improvement Act of 2005, HR 1297, 109th Congress (2005).
38. Improved Vaccine Affordability and Availability Act, S 754, 108th Con-gress (2003).
39. Lloyd-Puryear MA, Ball LK, Benor D. Should the Vaccine Injury Com-pensation Program be expanded to cover adults? Public Health Rep 1998; 113:236–42.
40. Centers for Disease Control and Prevention. Prevention and control of influenza: recommendations of the Advisory Committee on Im-munization Practices (ACIP). MMWR Recomm Rep2004; 53(RR-6): 1–40 [erratum: MMWR Recomm Rep 2004; 53:743].
41. American Jobs Creation Act of 2004, Public Law 108–357, §§ 889–890 (2004).
42. Public Law 109-148, Division C (2005).
43. Moss R. Presentation at the Barriers to Immunization Workshop. Washington, DC: 29 April2005.
by guest on July 17, 2016
http://cid.oxfordjournals.org/