Systematic Review of Design and Effects of Splints
and Exercise Programs in Hand Osteoarthritis
INGVILD KJEKEN, GEIR SMEDSLUND, RIKKE H. MOE, BARBARA SLATKOWSKY-CHRISTENSEN,
TILL UHLIG,
ANDKÅRE BIRGER HAGEN
Objective. To describe and evaluate the design and effects of splints and exercise programs in hand osteoarthritis. Methods. Controlled trials identified through systematic literature reviews were included. Design of splints and exercise programs were evaluated according to existing recommendations and classification systems. The risk of bias was assessed by 2 independent reviewers and effects were summarized descriptively or by meta-analyses.
Results. Twelve trials were included in the review: 7 assessed the effect of splints, 3 the effect of exercises, and 2 a combination of splints and exercises. The results revealed a great variety in the design of splint and exercise programs. A meta-analysis of the 2 randomized trials with low risk of bias demonstrated that splints significantly reduced hand pain at short-term (<3 months) and long-term (>3 months) followup, with a standardized mean difference of 0.37 (95% confidence interval [95% CI] 0.03, 0.71) and 0.80 (95% CI 0.45, 1.15), respectively. Further, results from single trials indicated that hand exercises may reduce pain and increase range of motion and strength, while a combination of splints and daily exercises may reduce pain and stiffness and improve function.
Conclusion. There is consistent evidence that splints reduce hand pain, but limited evidence for the effects of hand exercises and a combination of hand exercises and splints in hand osteoarthritis.
INTRODUCTION
Hand osteoarthritis (OA) is one of the most common joint disorders, affecting as many as 26% of women and 13% of men agesⱖ70 years. As the disease is strongly associated with aging, the prevalence is expected to rise dramatically in the coming decades (1). Manifestations of hand OA are soft tissue swelling, bony enlargements, and bone ero-sions, most frequently within the distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints of the sec-ond through fifth fingers, and the carpometacarpal thumb joint (CMC1) (2). This in turn has functional consequences such as pain and reduced mobility and grip force, and activity limitations and participation restrictions (3–5). Studies further indicate that levels of pain and disability are significantly higher among patients with CMC1 in-volvement compared to those without symptoms in the CMC1 (6,7).
Currently, there is no cure for hand OA. Pharmacologic treatment is mostly confined to symptomatic treatment, and surgical treatment is limited to severe OA of the CMC1. The European League Against Rheumatism (EULAR) states that optimal management of hand OA re-quires a combination of nonpharmacologic and pharmaco-logic treatment, which should be tailored according to the patient’s wishes and expectations and his or her level of pain, disability, and restriction of quality of life (8). They further recommend that all patients should be provided with education concerning joint protection and an exer-cise regimen involving both range of motion (ROM) and strengthening exercises. Patients with OA of the CMC1 should be provided with splints to prevent and/or correct subluxation and deformity of the thumb.
In a previous overview of systematic reviews, we iden-tified 3 that addressed splints and exercises (9). One was the EULAR recommendations (8). The second reviewed the evidence for splinting of the CMC1. The authors con-cluded that even if there was fair evidence for the effec-tiveness of splinting to relieve pain and improve function, there was no clear evidence of the superiority of one type of splint over another, and patients’ preferences regarding the type of splint varied (10). The third review summed up the evidence for nonsurgical interventions for hand OA, stating that “there is at least some evidence from a pub-lished RCT for the efficacy for”. . .“splints for first CMC OA,”. . .“yoga” and “strength training exercise and spa Ingvild Kjeken, PhD, Geir Smedslund, PhD, Rikke H. Moe,
MSc, Barbara Slatkowsky-Christensen, MD, Till Uhlig, PhD, Kåre Birger Hagen, PhD: Diakonhjemmet Hospital, Oslo, Norway.
Address correspondence to Ingvild Kjeken, PhD, National Resource Center for Rehabilitation in Rheumatology, Dia-konhjemmet Hospital, PO Box 23, Vinderen, 0319 Oslo, Nor-way. E-mail: [email protected].
Submitted for publication October 6, 2010; accepted in revised form December 22, 2010.
DOI 10.1002/acr.20427
© 2011, American College of Rheumatology
ORIGINAL ARTICLE
therapy” (11). That systematic review was updated in 2009 (12). Since then, another systematic review of conservative interventions for hand OA (13) and 4 relevant single stud-ies (14 –17) have been published. However, none of the 4 systematic reviews included any systematic description of the design of splints or exercise programs. Therefore, based on the knowledge gap identified in our previous overview, the aim of this study was to describe and eval-uate the design and effect of splints and exercise programs in hand OA.
MATERIALS AND METHODS
Literature search. We performed a broad systematic lit-erature search and included randomized controlled trials (RCTs), controlled clinical trials using inadequate genera-tion of sequence allocagenera-tion, controlled before and after studies, and interrupted time series examining the effec-tiveness of splints and/or exercise programs in patients with hand OA. We used all relevant synonyms for study designs and hand OA and excluded pharmacologic and surgical interventions (18) (see Supplementary Appendix A, available in the online version of this article at http:// onlinelibrary.wiley.com/journal/10.1002/(ISSN) 2151-4658). Furthermore, we performed a search with terms for hand OA and synonyms for exercise and splints. The following databases were searched until May 2010: Cochrane Central Register of Controlled Trials, Allied and Complementary Medicine Database, Medline, EMBase, Cumulative Index to Nursing and Allied Health Literature, OTseeker, and Physiotherapy Evidence Database. In addi-tion, reference lists in relevant studies and reviews were examined.
As it was important for us not only to assess the effect of splints and exercises, but also the design, we chose a pragmatic strategy concerning the diagnosis of hand OA. The study group therefore was composed of people ages
ⱖ18 years who were diagnosed with hand OA by a phy-sician. Studies combining participants with a variety of diseases were included if data could be extracted for the hand OA group separately. Only publications available in English, German, French, or a Scandinavian language were included.
Data collection. The first author (IK) together with one of the coauthors (RHM, BS-C, or TU) independently screened titles and abstracts against the inclusion criteria and extracted data using a data collection form. Uncer-tainty or disagreement was resolved by discussion with a third author (KBH). If data were missing or unclear, the authors of the article were contacted for clarification.
Statistical analysis. Internal validity. Two authors (IK, KBH) assessed internal validity by investigating the fol-lowing criteria: concealment of allocation, cointervention, intent-to-treat analysis and losses to followup, outcome assessment, and blinding of patients. The criteria were rated as met, unclear, or not met. An overall assessment of internal validity was based on a summary of the 5 criteria,
with low risk of bias (⬎3 met), moderate risk of bias (3 met), or high risk of bias (⬍3 met) (Table 1). Details con-cerning operationalization of the criteria have been re-ported elsewhere (19).
Design of splints. Splints in hand OA are designed to support, protect, or immobilize joints in order to reduce pain and allow healing of inflamed joints or tissue, to prevent deformity, and/or to correct existing deformities (20). The design of the splints was described according to the Splint Classification System (SCS) (20). In the SCS, splints are classified according to location (articular or nonarticular), primary anatomic part(s) included, direc-tion (the primary kinematic funcdirec-tion of the splint), pur-pose (immobilization, mobilization, or restriction), and total number of joints included in the splint (Table 2). In addition, we reported material (rigid, semirigid, or soft), if the splint was prefabricated or custom made, and instruc-tions for splint use.
Design of hand exercise programs. Hand exercises in OA are aimed at maximizing pain-free functional ROM, increasing functional strength, maintaining joint stability, and avoiding fixed deformities (21,22). To our knowledge, no specific recommendations regarding design of hand exercise programs have been published. Therefore, we evaluated each program according to the American College of Sports Medicine (ACSM) recommendations for devel-oping muscular strength and flexibility in older frail adults. It was stated in these recommendations that to increase strength and endurance, resistance training should be individualized and progressive (23). For persons agesⱖ50 to 60 years, 1 set of 10 –15 repetitions that con-ditions the major muscle groups 2–3 days per week was recommended, while exercises to develop and maintain ROM should be performed 2–3 days per week with at least 4 repetitions per muscle group. The minimum exercise session should be 20 minutes preceded by a warm-up period, and older people should be allowed a minimum recovery period of 48 hours between exercise sessions. A minimum training period of 12–15 weeks was recom-mended to reach an optimal effect.
Methods for summarizing the evidence of effectiveness. We sought controlled studies with reported group sizes and between-group differences postintervention and at different followup times. We used Comprehensive Meta-Analysis 2.0 (CMA) for computing pooled effects (24). If the means and SDs were not available, CMA was able to accept data in approximately 100 different formats and converted the data into a standardized mean difference (SMD). We regarded the effect as small, moderate, or large if the SMD was 0.2– 0.5,⬎0.5 to⬍0.7, andⱖ0.7; respec-tively (25). When 2 or more studies had similar interven-tions, populainterven-tions, comparisons, and outcomes, we per-formed fixed-effect meta-analyses. Otherwise, we reported the effect sizes. If it was not possible to compute an effect size, we summarized the effects descriptively.
RESULTS
Description of included studies. The searches resulted in 1,619 potentially relevant articles, of which 1,590 were
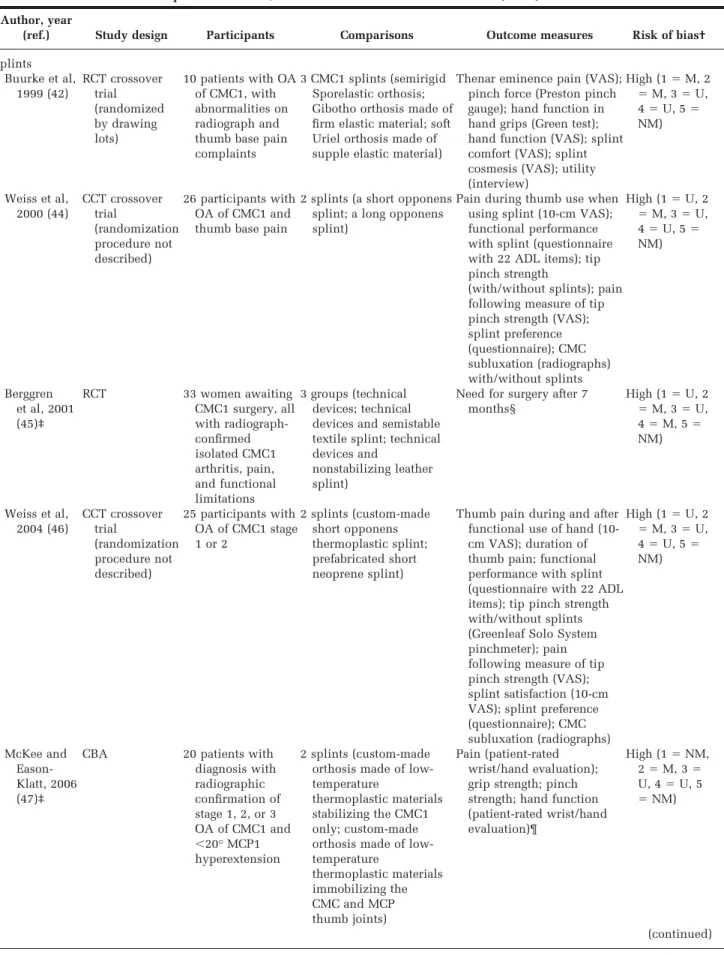
Table 1. Included randomized controlled trials (RCTs), controlled clinical trials (CCTs) using inadequate generation of sequence allocation, and controlled before and after studies (CBAs)*
Author, year
(ref.) Study design Participants Comparisons Outcome measures Risk of bias†
Splints Buurke et al, 1999 (42) RCT crossover trial (randomized by drawing lots) 10 patients with OA of CMC1, with abnormalities on radiograph and thumb base pain complaints
3 CMC1 splints (semirigid Sporelastic orthosis; Gibotho orthosis made of firm elastic material; soft Uriel orthosis made of supple elastic material)
Thenar eminence pain (VAS); pinch force (Preston pinch gauge); hand function in hand grips (Green test); hand function (VAS); splint comfort (VAS); splint cosmesis (VAS); utility (interview) High (1⫽M, 2 ⫽M, 3⫽U, 4⫽U, 5⫽ NM) Weiss et al, 2000 (44) CCT crossover trial (randomization procedure not described) 26 participants with OA of CMC1 and thumb base pain
2 splints (a short opponens splint; a long opponens splint)
Pain during thumb use when using splint (10-cm VAS); functional performance with splint (questionnaire with 22 ADL items); tip pinch strength
(with/without splints); pain following measure of tip pinch strength (VAS); splint preference (questionnaire); CMC subluxation (radiographs) with/without splints High (1⫽U, 2 ⫽M, 3⫽U, 4⫽U, 5⫽ NM) Berggren et al, 2001 (45)‡ RCT 33 women awaiting CMC1 surgery, all with radiograph-confirmed isolated CMC1 arthritis, pain, and functional limitations 3 groups (technical devices; technical devices and semistable textile splint; technical devices and
nonstabilizing leather splint)
Need for surgery after 7 months§ High (1⫽U, 2 ⫽M, 3⫽U, 4⫽M, 5⫽ NM) Weiss et al, 2004 (46) CCT crossover trial (randomization procedure not described) 25 participants with OA of CMC1 stage 1 or 2 2 splints (custom-made short opponens thermoplastic splint; prefabricated short neoprene splint)
Thumb pain during and after functional use of hand (10-cm VAS); duration of thumb pain; functional performance with splint (questionnaire with 22 ADL items); tip pinch strength with/without splints (Greenleaf Solo System pinchmeter); pain following measure of tip pinch strength (VAS); splint satisfaction (10-cm VAS); splint preference (questionnaire); CMC subluxation (radiographs) High (1⫽U, 2 ⫽M, 3⫽U, 4⫽U, 5⫽ NM) McKee and Eason-Klatt, 2006 (47)‡
CBA 20 patients with diagnosis with radiographic confirmation of stage 1, 2, or 3 OA of CMC1 and ⬍20° MCP1 hyperextension 2 splints (custom-made orthosis made of low-temperature
thermoplastic materials stabilizing the CMC1 only; custom-made orthosis made of low-temperature thermoplastic materials immobilizing the CMC and MCP thumb joints) Pain (patient-rated wrist/hand evaluation); grip strength; pinch strength; hand function (patient-rated wrist/hand evaluation)¶ High (1⫽NM, 2⫽M, 3⫽ U, 4⫽U, 5 ⫽NM) (continued)
excluded according to the predefined selection criteria for full-text review. Four reviewers (IK together with RHM, BS-C, or TU) performed a full-text review of the remaining 29 articles, resulting in exclusion of an additional 17 (22,26 – 41). The most common reasons for exclusion were study design (37–39,41), mixed patient populations (26,27,34,38,40), or that studies were treatment recom-mendations without any effect evaluation (22,30 –32).
A total of 12 studies were included, of which all but 2 (42,43) were published in 2000 or later. An overview of the included studies is shown in Table 1, according to study design, number of participants, comparisons, outcome measures, and risk of bias in the study. Seven studies assessed the effectiveness of splints (14,17,42,44 – 47), 3
assessed the effectiveness of exercises (16,43,48), and 2 assessed the effectiveness of a combination of splints and exercises (15,49). Six studies compared splints of different design (42,44 – 47,49), and 3 studies included a control group that did not use any splint (14,17,45). Two of the exercise studies compared exercise versus treatment as usual (43,48), while the third exercise study compared exercise with a sham hand cream (16). Of the 2 studies combining splints and exercises, 1 compared 1 splint and exercise program with another splint and exercise program (49), while the other compared different doses of splints and exercises (15). Participants in all but 3 studies (43,44,48) had radiograph-documented OA of the CMC1, and in 4 studies, participants with stage 4 OA were ex-Table 1. (Cont’d)
Author, year
(ref.) Study design Participants Comparisons Outcome measures Risk of bias†
Rannou et al, 2009 (14) RCT 112 participants with radiographic evidence of OA of CMC1, 1 of 2 clinical features of OA of the CMC1, and thumb base pain⬎30 mm on VAS Custom-made neoprene splint worn at night compared to treatment as usual (no splint)
Pain (VAS); hand disability (Cochin Hand Functional Scale); patient global perceived disability (VAS); patient global assessment (6-point scale); pinch strength (electronic dynamometer); thumb mobility (Kapandji index); thumb abduction (angle in degrees measured from picture) Low (1⫽M, 2 ⫽M, 3⫽M, 4⫽M, 5⫽ NM) Gomes Carreira et al, 2010 (17) RCT 40 patients with diagnosis of painful OA of CMC1 in dominant hand and radiographic confirmation of stage 2 or 3 in CMC1 and no severe hand deformities Custom-made functional thermoplastic splint compared to treatment as usual (no splint)#
Thumb base pain (VAS) with/without the splint; function (DASH); grip strength (Jamar dynamometer); pinch strength (pinch gauge dynamometer); upper limb dexterity (O’Connor test equipment) Low (1⫽M, 2 ⫽M, 3⫽M, 4⫽M, 5⫽ NM)** Exercises Garfinkel et al, 1994 (43) CCT with different participants in different phases (randomization procedure not described) 26 participants with OA of DIP or PIP joints of the finger(s)†† Exercise-based program compared to treatment as usual (drug treatment)
Finger joints ROM
(goniometer); grip strength (Jamar dynamometer); finger tenderness (dolorimeter); finger circumference (jeweler’s ring sizer); hand pain (VAS); hand function (HAQ) High (1⫽U, 2 ⫽M, 3⫽U, 4⫽U, 5⫽ NM) Lefler and Armstrong, 2004 (48) CCT (randomization procedure not described) 19 subjects with hand OA determined by physician and some hand/finger OA pain impairment 3 strength training exercises compared to treatment as usual
Grip strength (Jamar dynamometer); tip pinch strength (Jamar pinch gauge); lateral pinch strength (Jamar pinch gauge); Palmar pinch strength (Jamar pinch gauge); finger ROM (goniometer); pain (6-point scale) High (1⫽U, 2 ⫽M, 3⫽U, 4⫽U, 5⫽ NM) (continued)
cluded (17,46,47,49). Of the included studies, 9 had a high risk of bias (15,42– 49), 1 had a moderate risk (16), while 2 had a low risk of bias (14,17). Additional information was provided by the authors in 3 studies (15,45,47).
The most frequent outcomes in the studies were hand strength and pain (assessed in all but 1 study [45]), and function (assessed in all but 2 studies [45,48]) (Table 1). ROM was assessed in 3 studies, dexterity was assessed in 2 studies (16,17), and CMC1 subluxation, splint satisfaction, and splint preference were assessed in 2 studies (44,46).
Design of splints. The 9 studies addressing the effect of splints involved testing of 18 different splints for OA of the CMC1. The common features for all splints were that they were articular and included the CMC1 (Table 2). Only 1 study included a detailed description of the purpose of the splint (49), and none of the studies included a def-inition of the primary kinematic function of the splint or a hypothesis of why and how the design of the splint would be
effective to reduce symptoms and/or enhance function in hand OA.
Three of the splints were designed to support the CMC1 only. All of these were custom made from a rigid material, thereby immobilizing the joint (44,46,47). Seven of the splints supported or immobilized the wrist, CMC1, and metacarpophalangeal thumb joint (MCP1); 3 of these were custom made in a rigid material and prescribed for day and night use (44) or night use only (14,15). Only one of the rigid splints was prefabricated (42), and of the 3 splints tested in this study by Buurke et al, the rigid one was the least preferred because of pressure sores and reports that it was too stiff. Three studies lacked information (42,45) or gave incomplete information (15) concerning instructions for use, but additional information was provided by the authors of 2 of these (15,45). Participants were either in-structed to wear the splints full time (49), whenever they had symptoms in their thumb (44,46,47), during the day Table 1. (Cont’d)
Author, year
(ref.) Study design Participants Comparisons Outcome measures Risk of bias†
Rogers and Wilder, 2009 (16) RCT crossover trial 76 participants with OA gradeⱖ2 in 1 hand joint and minimum score of 225 on AUSCAN function subscale‡‡
9 hand exercises compared to sham hand cream
Hand function, stiffness, and pain (AUSCAN); grip strength (Jamar dynamometer); pinch strength (Jamar
dynamometer); dexterity (Purdue Pegboard Model)
Moderate (1⫽ M, 2⫽M, 3 ⫽NM, 4⫽ M, 5⫽NM) Splints and exercises Wajon and Ada, 2005 (49) CCT (randomization procedure not described) 40 participants with thumb base pain and stage 1, 2, or 3 OA of CMC1
Thumb strap splint and abduction exercise compared to short opponens splint and pinch grip exercise
Pain at rest (10-cm VAS); tip pinch strength (pinch gauge); hand function (Sollermann hand function test) High (1⫽U, 2 ⫽M, 3⫽U, 4⫽M, 5⫽ NM) Boustedt et al, 2009 (15)‡
CBA 42 women with clinically and/or radiograph-diagnosed hand OA, and pain in CMC1 joint(s)
Joint protection program with patient education, provision of assistive technology, elastic thumb splints, paraffin wax treatment, and exercises compared to same program with addition of splints for every affected joint and home exercises
Pain (100-mm VAS); stiffness (100-mm VAS); grip force (Grippit electronic instrument); pinch grip (Grippit electronic instrument); arm and hand function (DASH)
High (1⫽NM, 2⫽M, 3⫽ U, 4⫽M, 5 ⫽NM)
* OA⫽osteoarthritis; CMC1⫽carpometacarpal thumb joint (thumb base); VAS⫽visual analog scale; M⫽met; U⫽unclear; NM⫽not met; ADL⫽ activities of daily living; MCP1⫽metacarpophalangeal thumb joint; DASH⫽Disabilities of the Arm, Shoulder, and Hand; DIP⫽distal interpha-langeal; PIP⫽proximal interphalangeal; ROM⫽range of motion; HAQ⫽Health Assessment Questionnaire; AUSCAN⫽Australian/Canadian Osteoarthritis Hand Index.
† Internal validity was assessed using the following criteria (18): 1⫽concealment of allocation; 2⫽cointervention; 3⫽intent-to-treat analysis and losses to followup; 4⫽outcome assessment; 5⫽blinding of patients. An overall assessment of internal validity was based on a summary of the 5 criteria, with low risk of bias (⬎3 met), moderate risk of bias (3 met), or high risk of bias (⬍3 met).
‡ Additional information was provided by the authors.
§ Outcomes in the study are need for surgery after 7 months and 7 years. However, as all participants could use both splints after 7 months, only results after the initial 7-month period were included in the review.
¶ The method of assessment is not stated for grip strength and pinch strength.
# Outcomes were measured at 45, 90, and 180 days. After 90 days, the control group received the same splint as the study group. Therefore, only results at 45 and 90 days were included in the review.
** For results after the first 45 and 90 days of the study.
†† Exact number of participants in trial unclear because of unclear description.
only (15,17,45), or at night only (15,50). Splint adherence was recorded in 2 studies (14,46). The study period lasted from 2 weeks (42) to 7 years (45), with 2 of the most recent studies having a followup period of 1 year (14,15).
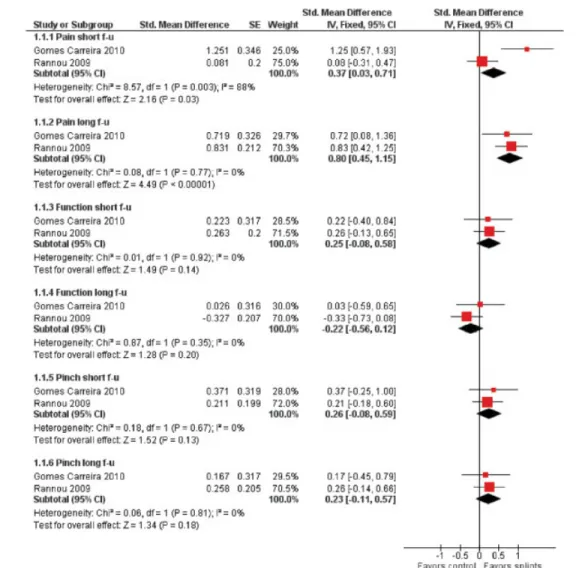
Effects of splint use. Studies with low risk of bias. Only 2 of the 9 splint studies had low risk of bias (14,17). Figure 1 shows meta-analyses of pain, function, and pinch grip at short-term (ⱕ45 days) and long-term (ⱖ3 months) fol-Table 2. Design of splints, described according to the Splint Classification System (20)*
Author, year (ref.) No. of splints/ purpose Splints Location Joints, no. CM or PF
Splint material Splint use
Wrist CMC1 MCP1 Soft
Semi-rigid Rigid Instructions
Study period for controlled intervention Buurke et al, 1999 (42) 3 splints used in random order/ to stabilize thumb Splint 1 X X X 3 PF — X — ND 12 weeks; each splint was used for 4 weeks Splint 2 X X X 3 PF — — X ND Splint 3 X X — 2 PF X — — ND Weiss et al, 2000 (44) 2 splints used in random order/ splint 1 immobilized CMC1, splint 2 supported CMC1 and MCP1
Splint 1 — X — 1 CM — — X Both splints: wear whenever symptoms in thumb are felt, day or night 2 weeks; each splint was used for 1 week Splint 2 X X X 3 CM — — X Berggren et al, 2001 (45)† 2 splints, 1 in each group/ ND for both splints
Splint 1 — X X 2 CM X — — Both splints: wear as much as possible during daytime, especially during straining activities 7 months; thereafter, participants had access to both splints Splint 2 X X X 2 PF† — X — Weiss et al, 2004 (46) 2 splints used in random order/ splint 1 immobilized CMC1, splint 2 immobilized wrist, CMC1, and MCP1
Splint 1 — X — 1 CM — — X Both splints: wear whenever symptoms in thumb are felt, day or night 2 weeks; each splint was used for 1 week Splint 2 X X X 3 PF — X — McKee et al, 2006 (47)† 2 splints, 1 in each group/to stabilize thumb
Splint 1 — X — 1 CM — — X Both splints: wear whenever pain is felt in thumb, day or night, during activity or rest 4 weeks (2 weeks for each splint) Splint 2 — X X 2 CM — — X Wajon and Ada, 2005 (49) 2 splints, 1 in each group/ ND for splint 1, splint 2 prevented flexion and adduction of metacarpal, dorso-radial subluxation of base of first metacarpal, and subsequent MCP hyperextention
Splint 1 — X X 2 CM — — X Both splints: wear full time Both splints: 6 weeks Splint 2 — X X 2 CM — — X (continued)
lowup. The analyses were homogeneous, except for pain at short followup (I2 ⫽ 88%). Splints showed a significant
effect on pain both at short-term and long-term followup, but there was uncertainty regarding the heterogeneous ef-fects for the short-term followup, and the confidence in-terval was large for the long-term followup.
Additionally, Rannou et al found a significant and mod-erate increased disability for splints versus care as usual at 1-year followup (14), while Gomes Carreira et al (17) found that the splint group had significant and moderate im-proved grip strength at 45 days of followup compared to the control subjects (Table 3).
Studies with high risk of bias and computable effect sizes. In the study by Berggren et al, there were no signif-icant effects of any of the 2 splints compared to technical devices regarding need for surgery after 7 months (45).
Studies with high risk of bias without computable effect sizes. In 1999, Buurke et al reported that the soft orthosis scored significantly better than the more rigid types on comfort, function, and hand function in hand grips, while the semirigid orthosis scored best on cosmesis (42). There were no significant differences in pain reduction among the 3 types of orthoses. Weiss et al reported in 2000 that “both splints appear to reduce subluxation at the first CMC joint in patients with grades 1 and 2 osteoarthritis.” The majority of the patients preferred the short splint (44). Weiss et al reported in 2004 that both the rigid and the
semirigid splint reduced subluxation in the CMC1, but the effect was greater when wearing the rigid splint (46). Par-ticipants rated the semirigid splint significantly higher than the custom-made rigid splint.
Both pain and function were improved with splinting, but the effect was amplified with the prefabricated semi-rigid splint. McKee and Eason-Klatt reported that both the long and short orthoses “reduced pain and improved hand function. However, the [short] carpometacarpal-stabilizing orthosis was preferred by participants because only 1 joint was restricted rather than 2” (47).
Design of exercise programs. The purpose of the exer-cise programs was to increase grip and/or pinch strength (15,16,43,48), ROM (15,16,43), and stability of the CMC1 (15,30,48). However, the number and types of exercises varied largely in the 6 programs (1 study included 2 dif-ferent programs), ranging from a program with 1 thumb exercise (49), to 2 programs with 9 exercises (Table 4) (15,16). Four programs contained an exercise to increase pinch strength (15,16,48,49), 3 included a resistance exer-cise to increase grip strength (gripping) (15,16,48), and 1 had exercises to increase key pinch (16). A device or material to give resistance was used in 4 programs (15,16,48,49). Three programs included exercises to in-crease finger flexion and opposition of the thumb (large Table 2. (Cont’d) Author, year (ref.) No. of splints/ purpose Splints Location Joints, no. CM or PF
Splint material Splint use
Wrist CMC1 MCP1 Soft
Semi-rigid Rigid Instructions
Study period for controlled intervention Boustedt et al, 2009 (15)† 1 splint in group 1, up to 3 splints in group 2/ND for all splints
Splint 1, group 1 X X — 2 PF X — — Splint 1, group 1: wear if pain at daytime. Splint 1 and 2, group 2: wear at all times during day. Splint 3, group 2: wear at night Each splint: 1 year Splint 1, group 2 X X — 2 PF X — — Splint 2, group 2 X X X 3 CM — — X Splint 3, group 2 X X — 2 CM — — X Rannou et al, 2009 (14) 1 splint in the intervention group/used as a rest splint
Splint 1 X X X 3 CM — — X Wear at night 1 year
Gomes Carreira et al, 2010 (17) 1 splint in the intervention group/stabilize the CMC1
Splint 1 — X X 2 CM — — X Use during activities of daily living; remove during rest and sleep, bathing and heat activities 90 days; thereafter, both groups wore splint
* All splints are articular. CMC1⫽carpometacarpal thumb joint (thumb base); MCP1⫽metacarpophalangeal thumb joint; CM⫽custom made; PF⫽ prefabricated; ND⫽no description available.
fist, okay signs, and thumb reach) (15,16,48). Of the 2 programs including thumb abduction and extension exer-cises (15,49), 1 used resistance, thereby having a greater potential to strengthen these muscles (15). Design of the program was justified in 1 study (49).
As shown in Table 5, none of the 6 exercise programs met all of the ACSM recommendations concerning warm up, combination of exercises, intensity, progression, and length of exercise period (23). Of the described programs, 3 included the recommended combination of exercises addressing strength and ROM (15,16,48), but only 2 of these also had the recommended number of repetitions (16,48). While all programs probably had the potential to reach a recommended minimum daily session dose of 20 minutes, participants were instructed to exercise every day in 4 of the programs (15,16,49) and only 1 program had the recommended 2–3 exercise days per week (48). There was a progression in the intensity in 4 of the programs (16,48,49), but only 2 programs lasted for the recom-mended minimum of 12 weeks (15,16), only 1 included a
warm-up period (15), and none of the programs contained any stretching exercises. Two programs fulfilled 6 and 7 of 9 criteria, respectively (16,48), of which 1 also recorded proto-col adherence and had a moderate risk of bias (16).
Effect of exercises. The studies that reported comput-able effects of exercises all had a high risk of bias, and we did not conduct meta-analyses. We were able to compute effect sizes in 1 of the 3 studies. This study tested the effect of yoga, and reported a significant and large effect on pain during activity (43) (Table 3). In the other 2 studies, Lefler and Armstrong reported that “compared with the nontreat-ment control group, grip strength and range of motion im-proved significantly (P ⬍ 0.05). No significant changes in pain levels or pinch strength occurred (P⬎0.05)” (48). Rog-ers and Wilder reported that “changes in AUSCAN [Austra-lian/Canadian Hand Osteoarthritis Index] sub-scales did not differ between exercise and sham treatments. No changes in dexterity were seen. Grip and pinch measures modestly improved after exercise but not after sham” (16).
Figure 1. Meta-analysis of effects of splints on pain, function, and pinch grip at short-term (ⱕ45 days) and long-term (ⱖ3 months) followup
(f-u). Function is measured by the Disabilities of the Arm, Shoulder, and Hand questionnaire or the Cochin Hand Functional Scale. Std. ⫽standard; SE⫽standard error; IV⫽inverse variance method; 95% CI⫽95% confidence interval.
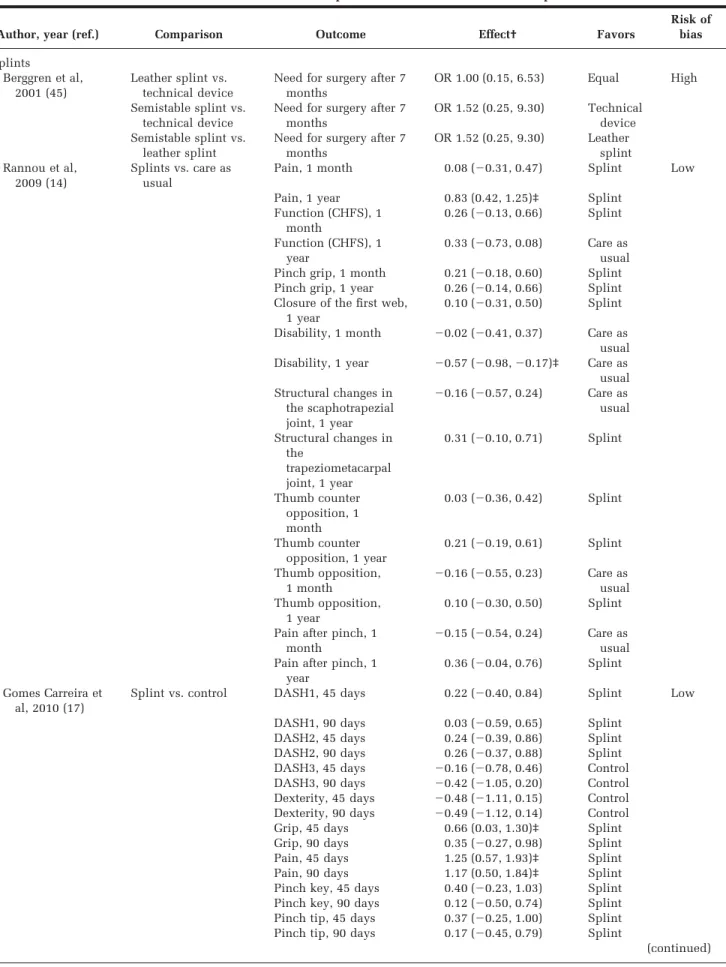
Table 3. Results of the 6 included studies that provided data for calculation of computable effects* Author, year (ref.) Comparison Outcome Effect† Favors
Risk of bias Splints Berggren et al, 2001 (45) Leather splint vs. technical device
Need for surgery after 7 months
OR 1.00 (0.15, 6.53) Equal High Semistable splint vs.
technical device
Need for surgery after 7 months
OR 1.52 (0.25, 9.30) Technical device Semistable splint vs.
leather splint
Need for surgery after 7 months OR 1.52 (0.25, 9.30) Leather splint Rannou et al, 2009 (14) Splints vs. care as usual
Pain, 1 month 0.08 (⫺0.31, 0.47) Splint Low Pain, 1 year 0.83 (0.42, 1.25)‡ Splint
Function (CHFS), 1 month 0.26 (⫺0.13, 0.66) Splint Function (CHFS), 1 year 0.33 (⫺0.73, 0.08) Care as usual Pinch grip, 1 month 0.21 (⫺0.18, 0.60) Splint Pinch grip, 1 year 0.26 (⫺0.14, 0.66) Splint Closure of the first web,
1 year
0.10 (⫺0.31, 0.50) Splint Disability, 1 month ⫺0.02 (⫺0.41, 0.37) Care as
usual Disability, 1 year ⫺0.57 (⫺0.98,⫺0.17)‡ Care as usual Structural changes in the scaphotrapezial joint, 1 year ⫺0.16 (⫺0.57, 0.24) Care as usual Structural changes in the trapeziometacarpal joint, 1 year 0.31 (⫺0.10, 0.71) Splint Thumb counter opposition, 1 month 0.03 (⫺0.36, 0.42) Splint Thumb counter opposition, 1 year 0.21 (⫺0.19, 0.61) Splint Thumb opposition, 1 month ⫺0.16 (⫺0.55, 0.23) Care as usual Thumb opposition, 1 year 0.10 (⫺0.30, 0.50) Splint Pain after pinch, 1
month
⫺0.15 (⫺0.54, 0.24) Care as usual Pain after pinch, 1
year
0.36 (⫺0.04, 0.76) Splint Gomes Carreira et
al, 2010 (17)
Splint vs. control DASH1, 45 days 0.22 (⫺0.40, 0.84) Splint Low DASH1, 90 days 0.03 (⫺0.59, 0.65) Splint
DASH2, 45 days 0.24 (⫺0.39, 0.86) Splint DASH2, 90 days 0.26 (⫺0.37, 0.88) Splint DASH3, 45 days ⫺0.16 (⫺0.78, 0.46) Control DASH3, 90 days ⫺0.42 (⫺1.05, 0.20) Control Dexterity, 45 days ⫺0.48 (⫺1.11, 0.15) Control Dexterity, 90 days ⫺0.49 (⫺1.12, 0.14) Control Grip, 45 days 0.66 (0.03, 1.30)‡ Splint Grip, 90 days 0.35 (⫺0.27, 0.98) Splint Pain, 45 days 1.25 (0.57, 1.93)‡ Splint Pain, 90 days 1.17 (0.50, 1.84)‡ Splint Pinch key, 45 days 0.40 (⫺0.23, 1.03) Splint Pinch key, 90 days 0.12 (⫺0.50, 0.74) Splint Pinch tip, 45 days 0.37 (⫺0.25, 1.00) Splint Pinch tip, 90 days 0.17 (⫺0.45, 0.79) Splint
Effect of splints and exercises. Even if both studies of splints and exercises reported computable effects, they had a high risk of bias, and we did not conduct meta-analyses (15,49). No significant differences between the 2 treatment regimens were demonstrated in the study by Wajon and Ada (49). Boustedt et al found significant and large positive effects of more exercises and splints as mea-sured by the Disabilities of the Arm, Shoulder, and Hand Outcome Measure, pain during motion and stiffness both after the intervention and at the 1-year followup, and reduced night pain at the 1-year followup (15) (Table 3).
DISCUSSION
To our knowledge, this is the first review that includes both a meta-analysis of the effects of splints and a thor-ough analysis of design of splints and exercise programs for hand OA. The meta-analysis demonstrates that splints significantly reduce hand pain. Concerning exercises, there is limited evidence from a single trial with high risk
of bias that hand exercises may reduce pain and increase ROM and strength, and that a combination of splints and daily exercises may reduce pain and stiffness and improve function. The results further demonstrate that there cur-rently is no consensus concerning the design of splints and exercise programs.
The literature defines 4 main purposes for splints for hand OA (22,51–53). Still, there was a general lack of definition of the primary function of the splint(s) tested in the reviewed studies, and no hypotheses regarding effect mechanisms of the splint were suggested. Further, even if all splints included the CMC1, the design varied from supporting this joint only to additionally including the wrist and/or MCP1 joint. There was also a great variation in the materials used. Therefore, to build an evidence-based practice for the use and effect of splints in hand OA, future studies should link design to purpose and hypoth-esized working mechanisms.
One such hypothesis is that splints may provide support of inflamed joints, thereby reducing inflammation and de-Table 3. (Cont’d)
Author, year (ref.) Comparison Outcome Effect† Favors
Risk of bias
Exercises Garfinkel et al,
1994 (43)
Yoga vs. control Hand function, 10 weeks
0.75 (⫺0.23, 1.74) Yoga High Pain during activity, 10
weeks
1.38 (0.34, 2.43)‡ Yoga Pain at rest, 10 weeks 0.35 (⫺0.61, 1.32) Yoga Splints and exercises
Wajon and Ada, 2005 (49)
Splint 1 and exercise 1 vs. splint 2 and exercise 2
VAS pain, 2 weeks 0.16 (⫺0.47, 0.79) Control High VAS pain, 6 weeks 0.21 (⫺0.46, 0.89) Control
Pinch tip, 2 weeks 0.23 (⫺0.40, 0.86) Splint Pinch tip, 6 weeks 0.34 (⫺0.33, 1.02) Splint Sollerman, 2 weeks§ 0.07 (⫺0.56, 0.70) Splint Sollerman, 6 weeks§ ⫺0.16 (⫺0.83, 0.52) Control Boustedt et al,
2009 (15)
More exercising and splint use vs. less exercising and splint use
DASH after treatment 0.98 (0.27, 1.68)‡ Exercise High DASH, 1 year 1.09 (0.38, 1.80)‡ Exercise
Grip force after treatment
0.34 (⫺0.33, 1.01) Exercise Grip force, 1 year 0.34 (⫺0.33, 1.01) Exercise Pain during motion
after treatment
0.75 (0.06, 1.44)‡ Exercise Pain during motion, 1
year
0.90 (0.20, 1.60)‡ Exercise Night pain after
treatment
0.75 (0.06, 1.44)‡ Exercise Night pain, 1 year 0.90 (0.20, 1.60)‡ Exercise Pinch grip after
treatment
0.26 (⫺0.41, 0.92) Exercise Pinch grip, 1 year 0.62 (⫺0.06, 1.31) Exercise Stiffness after treatment 0.88 (0.18, 1.58)‡ Exercise Stiffness, 1 year 0.72 (0.04, 1.41)‡ Exercise
* OR⫽odds ratio; CHFS⫽Cochin Hand Function Scale; DASH⫽Disabilities of the Arm, Shoulder, and Hand questionnaire; DASH1⫽optional subscale for athletes and musicians; DASH2⫽optional subscale for workers; DASH3⫽3 subscales concerning physical function, symptoms, and social aspects; VAS⫽visual analog scale.
† Values are the standardized mean difference (95% confidence interval) unless otherwise indicated. ‡ Statistically significant effects.
creasing pain. In a recent study, a significant positive correlation between pain and ultrasound-assessed inflam-mation in hand OA was demonstrated (54). In future stud-ies, a baseline ultrasound assessment of the joints would allow testing of a hypothesis of splints being (more) effec-tive to reduce pain in joints with synovitis.
Another hypothesis is that splints can prevent or decel-erate development of deformities, especially in the early stages without fixed deformities (stage 1 and 2) (30,32,44,47,51). Subluxation of the CMC1 with and with-out splints was measured in 2 studies (44,46). The results indicate that subluxation was reduced when wearing splints, and reduced further with a rigid splint than a soft splint (46), and with a longer splint versus a splint sup-porting the CMC1 only (44). In the 2 splint studies with low risk of bias, a long and rigid splint was found to be pain relieving and well tolerated for longtime night use (14), while a shorter splint used during activities of daily living significantly reduced pain (17). A regimen with a
small splint for pain relief during the day and a longer and rigid night splint for prevention of deformities may be worth testing in future studies. Further, rigid splints should be custom made to ensure optimal comfort, and in order to obtain a maximal effect, patients should probably start using deformity-preventing splints soon after diag-nosing since splints in later stages of OA may mainly have a pain-relieving effect.
All studies in this review evaluated the effect of splints designed to support thumb joints. In a recent cohort study, splint treatment for OA of the DIP joints significantly re-duced hand pain (41). Therefore, further investigation of splint treatment for the DIP and PIP joints is warranted.
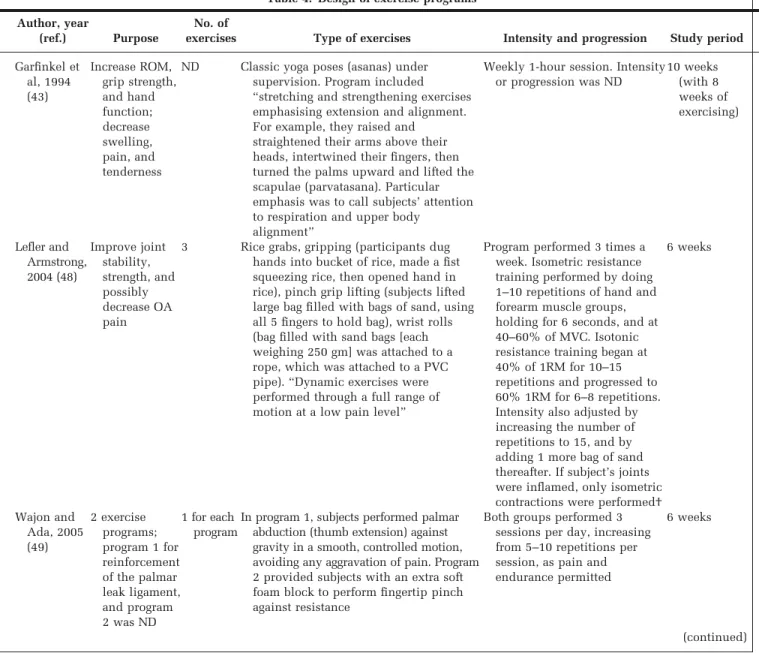
As in the splint studies, there was a great variety in the design of programs in the exercise studies, and justifica-tion of choices and/or hypothesis for working mechanisms were provided only in 1 study (49). Further, no programs fulfilled the ACSM recommendations for developing mus-cular strength and flexibility in older frail adults (23). Table 4. Design of exercise programs*
Author, year
(ref.) Purpose
No. of
exercises Type of exercises Intensity and progression Study period
Garfinkel et al, 1994 (43) Increase ROM, grip strength, and hand function; decrease swelling, pain, and tenderness
ND Classic yoga poses (asanas) under supervision. Program included “stretching and strengthening exercises emphasising extension and alignment. For example, they raised and
straightened their arms above their heads, intertwined their fingers, then turned the palms upward and lifted the scapulae (parvatasana). Particular emphasis was to call subjects’ attention to respiration and upper body
alignment”
Weekly 1-hour session. Intensity or progression was ND 10 weeks (with 8 weeks of exercising) Lefler and Armstrong, 2004 (48) Improve joint stability, strength, and possibly decrease OA pain
3 Rice grabs, gripping (participants dug hands into bucket of rice, made a fist squeezing rice, then opened hand in rice), pinch grip lifting (subjects lifted large bag filled with bags of sand, using all 5 fingers to hold bag), wrist rolls (bag filled with sand bags [each weighing 250 gm] was attached to a rope, which was attached to a PVC pipe). “Dynamic exercises were performed through a full range of motion at a low pain level”
Program performed 3 times a week. Isometric resistance training performed by doing 1–10 repetitions of hand and forearm muscle groups, holding for 6 seconds, and at 40–60% of MVC. Isotonic resistance training began at 40% of 1RM for 10–15 repetitions and progressed to 60% 1RM for 6–8 repetitions. Intensity also adjusted by increasing the number of repetitions to 15, and by adding 1 more bag of sand thereafter. If subject’s joints were inflamed, only isometric contractions were performed†
6 weeks Wajon and Ada, 2005 (49) 2 exercise programs; program 1 for reinforcement of the palmar leak ligament, and program 2 was ND 1 for each program
In program 1, subjects performed palmar abduction (thumb extension) against gravity in a smooth, controlled motion, avoiding any aggravation of pain. Program 2 provided subjects with an extra soft foam block to perform fingertip pinch against resistance
Both groups performed 3 sessions per day, increasing from 5–10 repetitions per session, as pain and endurance permitted
6 weeks
Table 4. (Cont’d)
Author, year
(ref.) Purpose
No. of
exercises Type of exercises Intensity and progression Study period
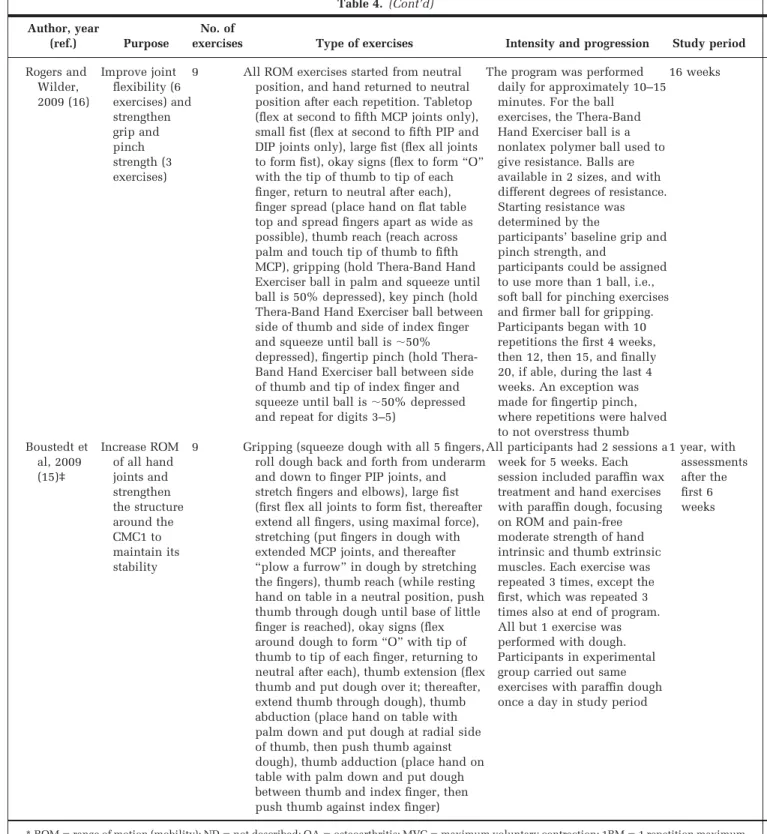
Rogers and Wilder, 2009 (16) Improve joint flexibility (6 exercises) and strengthen grip and pinch strength (3 exercises)
9 All ROM exercises started from neutral position, and hand returned to neutral position after each repetition. Tabletop (flex at second to fifth MCP joints only), small fist (flex at second to fifth PIP and DIP joints only), large fist (flex all joints to form fist), okay signs (flex to form “O” with the tip of thumb to tip of each finger, return to neutral after each), finger spread (place hand on flat table top and spread fingers apart as wide as possible), thumb reach (reach across palm and touch tip of thumb to fifth MCP), gripping (hold Thera-Band Hand Exerciser ball in palm and squeeze until ball is 50% depressed), key pinch (hold Thera-Band Hand Exerciser ball between side of thumb and side of index finger and squeeze until ball is⬃50% depressed), fingertip pinch (hold Thera-Band Hand Exerciser ball between side of thumb and tip of index finger and squeeze until ball is⬃50% depressed and repeat for digits 3–5)
The program was performed daily for approximately 10–15 minutes. For the ball
exercises, the Thera-Band Hand Exerciser ball is a nonlatex polymer ball used to give resistance. Balls are available in 2 sizes, and with different degrees of resistance. Starting resistance was determined by the
participants’ baseline grip and pinch strength, and
participants could be assigned to use more than 1 ball, i.e., soft ball for pinching exercises and firmer ball for gripping. Participants began with 10 repetitions the first 4 weeks, then 12, then 15, and finally 20, if able, during the last 4 weeks. An exception was made for fingertip pinch, where repetitions were halved to not overstress thumb
16 weeks Boustedt et al, 2009 (15)‡ Increase ROM of all hand joints and strengthen the structure around the CMC1 to maintain its stability
9 Gripping (squeeze dough with all 5 fingers, roll dough back and forth from underarm and down to finger PIP joints, and stretch fingers and elbows), large fist (first flex all joints to form fist, thereafter extend all fingers, using maximal force), stretching (put fingers in dough with extended MCP joints, and thereafter “plow a furrow” in dough by stretching the fingers), thumb reach (while resting hand on table in a neutral position, push thumb through dough until base of little finger is reached), okay signs (flex around dough to form “O” with tip of thumb to tip of each finger, returning to neutral after each), thumb extension (flex thumb and put dough over it; thereafter, extend thumb through dough), thumb abduction (place hand on table with palm down and put dough at radial side of thumb, then push thumb against dough), thumb adduction (place hand on table with palm down and put dough between thumb and index finger, then push thumb against index finger)
All participants had 2 sessions a week for 5 weeks. Each session included paraffin wax treatment and hand exercises with paraffin dough, focusing on ROM and pain-free moderate strength of hand intrinsic and thumb extrinsic muscles. Each exercise was repeated 3 times, except the first, which was repeated 3 times also at end of program. All but 1 exercise was performed with dough. Participants in experimental group carried out same exercises with paraffin dough once a day in study period
1 year, with assessments after the first 6 weeks
* ROM⫽range of motion (mobility); ND⫽not described; OA⫽osteoarthritis; MVC⫽maximum voluntary contraction; 1RM⫽1 repetition maximum (the maximum amount of weight a person can lift in a single repetition for a given exercise); MCP ⫽metacarpophalangeal; PIP⫽proximal interphalangeal; DIP⫽distal interphalangeal; CMC1⫽carpometacarpal thumb joint (thumb base).
† Isometric resistance training is an exercise in which the joint angle and muscle length does not change during contraction, and isotonic resistance training is an exercise in which the tension remains unchanged and the muscle length changes.
In the literature, it was suggested that the deforming force of the CMC1 is the strong pull from the adductor pollicis muscle combined with increasing weakness of the opposing thenar intrinsic musculature. Therefore, in order to maintain the first web space, avoid adduction defor-mity, and improve thumb stability, strengthening the thumb extensors and abductors as well as wrist extensor muscles was recommended (22,31,32,52,53). Some au-thors further recommended that strengthening exercises should be prescribed only in earlier stages of CMC1 insta-bility, as excessive exercises to improve pinch or key grip strength in later phases may result in increased sublux-ation and pain in instable joints (31,32,52,53). Therefore, it is interesting that all but 1 program included an exercise to increase pinch strength, 2 also had an exercise to increase key grip strength, while only 2 programs included exer-cises with a potential to strengthen the extensors and abductors of the thumb (15,49).
It is often stated that hand OA exercises should be of low intensity, be performed in periods with little pain and inflammation, and should not cause pain that persists for more than 2 hours after the activity (22,31,52). However, several studies demonstrated significant correlations be-tween poor grip strength and activity limitations (1,5,50,55,56), and reduced hand strength is described as an important functional consequence by patients with hand OA (3). Also, studies have shown that intensive programs are well tolerated and safe for patients with rheumatoid arthritis, with respect to disease activity and radiologic damage of the hands and feet (57,58). These programs proved to be more effective than low-intensity programs in improving general muscle strength, joint mo-bility, and functional ability (59,60). As there were no recommendations available for design of hand exercise programs, we used the ACSM recommendations for devel-oping muscular strength and flexibility in older frail adults to evaluate the design of programs in the included studies.
However, to what degree these recommendations are valid for hand conditions, or if hand exercise programs need to be adapted according to age, has not yet been tested. Con-sequently, examining the effect of an exercise program designed according to existing recommendations would be an important next step in the process of building research evidence.
In line with previous reviews (8,10,12,13), the results from this review demonstrate that the general evidence of the effect of splints and exercises in hand OA is still insufficient. To ensure high quality, new studies should use a randomized controlled design, i.e., including a con-trol group that receives no splint or exercise, before com-paring different splint or exercise regimens. Further, fu-ture trials should include justification of the design of the splint or program and hypotheses for working mecha-nisms, and measurements should correspond to the as-pects of function and comfort that the intervention seeks to improve or ensure. To allow for testing of dose-response relationships and feasibility, adherence of programs and splints should also be recorded.
In conclusion, there is evidence from 2 RCTs that splints reduce hand pain. Further, there is some, but limited, evidence from single trials that hand exercises may reduce pain and increase ROM and strength, and that a combina-tion of splints and daily exercises may reduce pain and stiffness and improve function. The need for high-quality studies is evident.
ACKNOWLEDGMENT
The authors would like to thank Hilde Iren Flaatten for library assistance.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors
ap-Table 5. Description of exercise programs according to American College of Sports Medicine recommendations for developing muscular strength and flexibility in older frail adults (23)*
Author, year (ref.) Warm up Strength exercises included ROM exercises included Minimum 10 repetition strength exercises Minimum 4 repetition ROM exercises Minimum total daily session of 20 minutes Exercise 2–3 days per week Progress Minimum length 12–15 weeks Garfinkel et al, 1994 (43) ND ND ND ND ND Yes No (1 day) ND No Lefler and Armstrong, 2004 (48)
No Yes Yes Yes Yes Probably Yes (3 days) Yes No
Wajon and Ada,
No† No† Yes† No† Yes† Probably† No (7 days)† Yes† No 2005 (49) No‡ Yes‡ No‡ Yes‡ No‡ Probably‡ No (7 days)‡ Yes‡ No Rogers and
Wilder, 2009 (16)
No Yes Yes Yes Yes Probably No (7 days) Yes Yes
Boustedt et al, 2009 (15)
Yes Yes Yes No No Probably No (7 days) No Yes
* ROM⫽range of motion; ND⫽not described. † Thumb abduction exercise program. ‡ Thumb pinch exercise program.
proved the final version to be submitted for publication. Dr. Kjeken had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study conception and design. Kjeken, Slatkowski-Christensen, Uhlig, Hagen.
Acquisition of data.Kjeken, Moe, Slatkowski-Christensen, Uhlig, Hagen.
Analysis and interpretation of data.Kjeken, Smedslund, Moe, Uhlig, Hagen.
REFERENCES
1. Zhang Y, Niu J, Kelly-Hayes M, Chaisson CE, Aliabadi P, Felson DT. Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The Framingham Study. Am J Epidemiol 2002;156:1021–7. 2. Botha-Scheepers S, Riyazi N, Watt I, Rosendaal FR, Slagboom
E, Bellamy N, et al. Progression of hand osteoarthritis over 2 years: a clinical and radiological follow-up study. Ann Rheum Dis 2009;68:1260 – 4.
3. Stamm T, van der Giesen F, Thorstensson CA, Steen E, Birrell F, Bauernfeind B, et al. Patient perspective of hand osteoar-thritis in relation to concepts covered by instruments measur-ing functionmeasur-ing: a qualitative European multi-centre study. Ann Rheum Dis 2009;68:1453– 60.
4. Elliott AL, Kraus VB, Fang F, Renner JB, Schwartz TA, Salazar A, et al. Joint-specific hand symptoms and self-reported and performance-based functional status in African-Americans and Caucasians: the Johnston County Osteoarthritis Project. Ann Rheum Dis 2007;66:1622– 6.
5. Kjeken I, Dagfinrud H, Slatkowsky-Christensen B, Mowinckel P, Uhlig T, Kvien TK, et al. Activity limitations and partici-pation restrictions in women with hand osteoarthritis: pa-tients’ descriptions and associations between dimensions of functioning. Ann Rheum Dis 2005;64:1633– 8.
6. Bijsterbosch J, Visser W, Kroon HM, Stamm T, Meulenbelt I, Huizinga TW, et al. Thumb base involvement in symptomatic hand osteoarthritis is associated with more pain and func-tional disability. Ann Rheum Dis 2010;69:585–7.
7. Haara MM, Heliovaara M, Kroger H, Arokoski JP, Manninen P, Karkkainen A, et al. Osteoarthritis in the carpometacarpal joint of the thumb: prevalence and associations with disabil-ity and mortaldisabil-ity. J Bone Joint Surg Am 2004;86-A:1452–7. 8. Zhang W, Doherty M, Leeb BF, Alekseeva L, Arden NK,
Bijlsma JW, et al. EULAR evidence based recommendations for the management of hand osteoarthritis: report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis 2007;66:377– 88.
9. Moe RH, Kjeken I, Uhlig T, Hagen KB. There is inadequate evidence to determine the effectiveness of nonpharmacologi-cal and nonsurginonpharmacologi-cal interventions for hand osteoarthritis: an overview of high-quality systematic reviews. Phys Ther 2009; 89:1363–70.
10. Egan MY, Brousseau L. Splinting for osteoarthritis of the carpometacarpal joint: a review of the evidence. Am J Occup Ther 2007;61:70 – 8.
11. Towheed TE. Systematic review of therapies for osteoarthritis of the hand. Osteoarthritis Cartilage 2005;13:455– 62. 12. Mahendira D, Towheed TE. Systematic review of non-surgical
therapies for osteoarthritis of the hand: an update. Osteoar-thritis Cartilage 2009;17:1263– 8.
13. Valdes K, Marik T. A systematic review of conservative inter-ventions for osteoarthritis of the hand. J Hand Ther 2010;23: 334 –50.
14. Rannou F, Dimet J, Boutron I, Baron G, Fayad F, Mace Y, et al. Splint for base-of-thumb osteoarthritis: a randomized trial. Ann Intern Med 2009;150:661–9.
15. Boustedt C, Nordenskiold U, Lundgren NA. Effects of a hand-joint protection programme with an addition of splinting and exercise: one year follow-up. Clin Rheumatol 2009;28:793–9. 16. Rogers MW, Wilder FV. Exercise and hand osteoarthritis
symptomatology: a controlled crossover trial. J Hand Ther 2009;22:10 – 8.
17. Gomes Carreira AC, Jones A, Natour J. Assessment of the effectiveness of a functional splint for osteoarthritis of the trapeziometacarpal joint on the dominant hand: a randomized controlled study. J Rehabil Med 2010;42:469 –74.
18. Higgins JP, Green S, editors. Cochrane handbook for system-atic reviews of interventions. Cochrane Collaboration; 2008. 19. Dagfinrud H, Kvien TK, Hagen KB. Physiotherapy
interven-tions for ankylosing spondylitis. Cochrane Database Syst Rev 2008;1:CD002822.
20. Fess E, Gettle K, Philips C, Janson R. Classifications and nomenclatures of splints and splint components. In: Fess E, editor. Hand and upper extremity splinting: principles & methods. Philadelphia: Elsevier; 2004. p. 120 – 40.
21. Kurtz PE. Concervative management of arthritis. In: Burke SL, Higgins JP, McClinton MA, Suanders RJ, Valdata L, editors. Hand and upper extremity rehabilitation. 3rd ed. St. Louis: Elsevier; 2006. p. 649 –58.
22. Poole JU, Pellegrini VD Jr. Arthritis of the thumb basal joint complex. J Hand Ther 2000;13:91–107.
23. American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc 1998;30: 975–91.
24. Borenstein M, Hegdes L, Rothenstein H. Comprehensive meta-analysis version 2. Englewood (NJ): Biostat; 2005. 25. Cohen J. Statistical power analysis for the behavioural
sciences: the effect size. 2nd ed. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988.
26. Swezey RL, Spiegel TM, Cretin S, Clements P. Arthritic hand response to pressure gradient gloves. Arch Phys Med Rehabil 1979;60:375–7.
27. Dixon AS, Harrison RA, Pocock P. Trial of isotoner gloves for morning stiffness and pain in rheumatoid arthritis. Br J Clin Pract 1986;40:271–2.
28. Li SG, Zhang SR, Bao GQ. A combined therapy of mineral spring bath and “Qi-Gong” for limbs volume sphygmogram of the patients with osteoarthrosis. Chin J Phys Ther 1991;14: 15– 6.
29. Norton CO, Hoobler K, Welding AB, Jensen GM. Effectiveness of aquatic exercise in the treatment of women with osteoar-thritis. J Aquat Phys Ther 1997;5:8 –15.
30. Wajon A. Clinical splinting successes: the thumb “strap splint” for dynamic instability of the trapeziometacarpal joint. J Hand Ther 2000;13:236 –7.
31. Lockard MA. Exercise for the patient with upper quadrant osteoarthritis. J Hand Ther 2000;13:175– 83.
32. Taylor J. Restoration of dynamic stability in early osteoarthri-tis of the carpometacarpal joint of the thumb. Br J Hand Ther 2000;5:37– 41.
33. Stamm TA, Machold KP, Smolen JS, Fischer S, Redlich K, Graninger W, et al. Joint protection and home hand exercises improve hand function in patients with hand osteoarthritis: a randomized controlled trial. Arthritis Rheum 2002;47:44 –9. 34. Suomi R, Collier D. Effects of arthritis exercise programs on
functional fitness and perceived activities of daily living mea-sures in older adults with arthritis. Arch Phys Med Rehabil 2003;85:1409 –16.
35. Horlock N, Belcher HJ. Early versus late mobilisation after simple excision of the trapezium. J Bone Joint Surg Br 2002; 84:1111–5.
36. Michlovitz S, Hun L, Erasala GN, Hengehold DA, Weingand KW. Continuous low-level heat wrap therapy is effective for treating wrist pain. Arch Phys Med Rehabil 2004;85:1409 –16. 37. Day CS, Gelberman R, Patel AA, Vogt MT, Ditsios K, Boyer MI. Basal joint osteoarthritis of the thumb: a prospective trial of steroid injection and splinting. J Hand Surg Am 2004;29: 247–51.
38. McKee P, Rivard A. Orthoses as enablers of occupation: client-centred splinting for better outcomes. Can J Occup Ther 2004;71:306 –14.
persons with hand osteoarthritis: a two-year follow-up study. J Hand Ther 2007;20:244 –9.
40. Thiele J, Nimmo R, Rowell W, Quinn S, Jones G. A random-ized single blind crossover trial comparing leather and com-mercial wrist splints for treating chronic wrist pain in adults. BMC Musculoskelet Disord 2009;10:129.
41. Ikeda M, Ishii T, Kobayashi Y, Mochida J, Saito I, Oka Y. Custom-made splint treatment for osteoarthritis of the distal interphalangeal joints. J Hand Surg Am 2010;35:589 –93. 42. Buurke JH, Grady JH, de Vries J, Baten CT. Usability of thenar
eminence orthoses: report of a comparative study. Clin Reha-bil 1999;13:288 –94.
43. Garfinkel MS, Schumacher HR Jr, Husain A, Levy M, Reshetar RA. Evaluation of a yoga based regimen for treatment of osteoarthritis of the hands. J Rheumatol 1994;21:2341–3. 44. Weiss S, LaStayo P, Mills A, Bramlet D. Prospective analysis
of splinting the first carpometacarpal joint: an objective, sub-jective, and radiographic assessment. J Hand Ther 2000;13: 218 –26.
45. Berggren M, Joost-Davidsson A, Lindstrand J, Nylander G, Povlsen B. Reduction in the need for operation after conser-vative treatment of osteoarthritis of the first carpometacarpal joint: a seven year prospective study. Scand J Plast Reconstr Surg Hand Surg 2001;35:415–7.
46. Weiss S, LaStayo P, Mills A, Bramlet D. Splinting the degen-erative basal joint: custom-made or prefabricated neoprene? J Hand Ther 2004;17:401– 6.
47. McKee P, Eason-Klatt M. A multi-center study comparing two styles of orthoses for individuals with thumb carpometacar-pal osteoarthritis: ASHT 2006 scientific and clinical paper abstracts from Atlanta meeting [abstract]. J Hand Ther 2006; 19:446 –7.
48. Lefler C, Armstrong J. Exercise in the treatment of osteoarthri-tis in the hands of the elderly. Clin Kinesiol 2004;58:13–7. 49. Wajon A, Ada L. No difference between two splint and
exer-cise regimens for people with osteoarthritis of the thumb: a randomised controlled trial. Aust J Physiother 2005;51:245–9. 50. Spacek E, Poiraudeau S, Fayad F, Lefevre-Colau MM,
Beau-dreuil J, Rannou F, et al. Disability induced by hand osteoarthritis: are patients with more symptoms at digits 2-5 interphalangeal joints different from those with more symp-toms at the base of the thumb? Osteoarthritis Cartilage 2004; 12:366 –73.
51. Colditz JC. The biomechanics of a thumb carpometacarpal immobilization splint: design and fitting. J Hand Ther 2000; 13:228 –35.
52. Neumann DA, Bielefeld T. The carpometacarpal joint of the thumb: stability, deformity, and therapeutic intervention. J Orthop Sports Phys Ther 2003;33:386 –99.
53. Moran ME. Osteoarthritis and occupational therapy interven-tion. Phys Med Rehabil 2001;15:65– 81.
54. Kortekaas MC, Kwok WY, Reijnierse M, Watt I, Huizinga TW, Kloppenburg M. Pain in hand osteoarthritis is associated with inflammation: the value of ultrasound. Ann Rheum Dis 2010; 69:1367–9.
55. Allen KD, Jordan JM, Renner JB, Kraus VB. Relationship of global assessment of change to AUSCAN and pinch and grip strength among individuals with hand osteoarthritis. Osteo-arthritis Cartilage 2006;14:1281–7.
56. Jones G, Cooley HM, Bellamy N. A cross-sectional study of the association between Heberden’s nodes, radiographic osteoar-thritis of the hands, grip strength, disability and pain. Osteo-arthritis Cartilage 2001;9:606 –11.
57. De Jong Z, Munneke M, Zwinderman AH, Kroon HM, Ronday KH, Lems WF, et al. Long term high intensity exercise and damage of small joints in rheumatoid arthritis. Ann Rheum Dis 2004;63:1399 – 405.
58. De Jong Z, Vlieland TP. Safety of exercise in patients with rheumatoid arthritis. Curr Opin Rheumatol 2005;17:177– 82. 59. Van den Ende CH, Breedveld FC, le Cessie S, Dijkmans BA, de Mug AW, Hazes JM. Effect of intensive exercise on patients with active rheumatoid arthritis: a randomised clinical trial. Ann Rheum Dis 2000;59:615–21.
60. Hakkinen A. Effectiveness and safety of strength training in rheumatoid arthritis. Curr Opin Rheumatol 2004;16:132–7.