PRENATAL EXPOSURE TO ORGANOPHOSPHATE ESTERS AND COGNITIVE AND BEHAVIORAL DEVELOPMENT IN YOUNG CHILDREN
Brett Thomas Doherty
A dissertation submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of
Epidemiology in the Gillings School of Global Public Health.
Chapel Hill 2018
© 2018
ABSTRACT
Brett Thomas Doherty: Prenatal Exposure to Organophosphate Esters and Cognitive and Behavioral Development in Young Children
(Under the direction of Julie L. Daniels)
Organophosphate esters (OPEs) are chemical additives applied to a variety of consumer products as flame retardants and for other purposes. OPEs volatilize from products and are prevalent in the environment and in humans. OPEs are potentially developmentally toxic, but epidemiologic evidence is limited.
We investigated developmental effects of prenatal OPE exposure with data from the Pregnancy, Infection, and Nutrition (PIN3), PIN Postpartum, and PIN Kids studies. The PIN3 Study is a prospective birth cohort study of pregnant women in North Carolina between 2001 and 2005. We measured OPE metabolite concentrations in prenatal urine, including diphenyl phosphate (DPHP), bis(1,3-dichloro-2-propyl phosphate) (BDCIPP), isopropyl-phenyl phenyl phosphate (ip-PPP), and 1-hydroxyl-2-propyl bis(1-chloro-2-propyl) phosphate (BCIPHIPP). The PIN studies assessed children’s cognitive and behavioral development using the Mullen Scales of Early Learning (MSEL) at 12 and 36 months, the MacArthur-Bates Communicative
Development Inventories (MB-CDI) at 12 and 30 months, the Infant-Toddler Social-Emotional Assessment at 24 months, and the Behavioral Assessment Scale for Children (2nd Edition, BASC-2) at 36 months. We estimated the covariate-adjusted change in performance on these developmental assessments per interquartile range (IQR) increase in specific gravity-corrected, log-transformed OPE metabolite concentrations, and investigated effect measure modification of these associations by child’s sex.
Higher ip-PPP concentrations were associated with poorer overall cognitive
-0.32), primarily driven by the Fine Motor and Expressive Language subscales. Conversely, ip-PPP was associated with fewer internalizing symptoms on the BASC-2 (β: -1.77; 95% CI: -3.24, -0.29). BDCIPP concentrations were associated with more externalizing behaviors on the BASC-2 (β: 2.32; 95% CI: 0.85, 3.79) and ITSEA (β: 2.07; 95% CI: 0.29, 3.85). Other OPE metabolites were not strongly associated with developmental scores. We did not observe strong evidence of effect measure modification by child’s sex.
ACKNOWLEDGEMENTS
There are many people I’d like to acknowledge for the assistance and support they provided me in the completion of this dissertation.
First, I’d like to acknowledge my committee members, without whom this project would not have been possible and who provided thoughtful input at every step. I’d also like to thank them for accommodating my tight timeline, which I am sure was burdensome at times, and to especially thank Julie and Stephanie for encouraging me to set a shorter timeline that would allow me to pursue postdoctoral training.
First, thank you, Julie, for everything: your availability to meet and work with me through the many aspects of the project, your general patience with me, your openness that allowed me to be comfortable in my ignorance and curiosity, your encouragement, your keeping me on task, and much more. It is very difficult for me to imagine this whole process working out as well as it did with any other advisor. Thank you.
Thank you, Kate, for working with me through some tricky issues and always being timely and thoughtful, plus being an all-around great person to work with and be around.
Thank you, Stephanie, for challenging me to think more critically and grow as an epidemiologist. Much of my training I can attribute to you, and I’m very proud to say that I’ve been one of your trainees.
Thank you, Andy, for your thoughtful reviews that forced me think more critically about important aspects of the project, and for being an overall great person to work with.
looked forward to receiving your comments, as I knew there would always be something new for me to learn that would improve my writing.
I would also like to thank Alex Keil, whom I consider an honorary committee member due to his significant contributions to the statistical analysis, epidemiologic integrity, and writing of the manuscripts. Alex, it was an absolute privilege to work with you. I very much enjoyed our conversations and would often learn far more than I bargained for in our meetings (I mean that in the best way possible). You were incredibly helpful to me in working through the analyses, and also in thinking through some of the foundational epidemiologic concepts. I really can’t thank you enough.
I would next like to thank the wonderful community of UNC Epidemiology, with its many kind, intelligent, and cooperative students and faculty members that made for an excellent learning environment. In particular, thanks to my MSPH Cohort, who graciously tolerated me and were always great people to work with and learn from. I’d also like to acknowledge the UNC Epidemiology students more broadly, particularly the ENVR/OCC and RPPE groups, who were always a warm and welcoming group; it was a real privilege to be a part of this community. I’d like to give a special acknowledgement to Alberto Vargas, who helped to keep me sane, but also made a great tennis opponent, jam partner, and friend. I’d like to thank Valerie and
Jennifer, who were always extremely helpful, always available, and always a pleasure to talk to. I’d like to thank the other many faculty members who contributed to my training and education, with particular thanks to Charlie Poole, Larry Engel, David Richardson, and Steve Cole.
my sister, Jennifer, for always being there for me. And lastly, I’d like to thank the Hopkinton crew, for obvious reasons – where would I be without you guys? I shudder to think.
Although less personal, I would like to acknowledge all the artists who created the great and beautiful music that got me through this process – its significance cannot be overstated. Additionally, I’d like to thank the town of Carrboro for being its utopian self – I cannot imagine a more peaceful and accommodating environment and will miss it dearly.
TABLE OF CONTENTS
LIST OF TABLES ... xiii
LIST OF FIGURES ... xvii
LIST OF ABBREVIATIONS ... xviii
CHAPTER 1: INTRODUCTION AND SPECIFIC AIMS ... 1
CHAPTER 2: BACKGROUND AND REVIEW OF LITERATURE ... 7
2.1 Modern Uses of Organophosphate Flame Retardants and Plasticizers ... 7
2.2 Environmental Presence and Human Exposure... 8
2.3 Exposure among Pregnant Women and Vulnerability of the Developing Fetus ...12
2.4 Direct Fetal Exposure and Potential Toxicity ...13
2.5 Indirect Fetal Exposure and Potential Toxicity ...15
2.6 Experimental Evidence of Behavioral Effects in Animal Models ...16
2.7 Epidemiologic Evidence of Cognitive and Behavioral Effects ...16
2.8 Endocrine-Disrupting Compounds and Sex-Specific Associations ...17
2.9 Significance of Potential Cognitive and Behavioral Effects of OPEs ...18
CHAPTER 3: INNOVATION ...19
CHAPTER 4: APPROACH ...23
4.1 Overview ...23
4.2 Study Design and Study Population...24
4.3 Assessment of Maternal Exposure to OPEs during Pregnancy ...28
4.4 Assessment of Children’s Cognitive and Behavioral Development ...34
4.4.2 MacArthur-Bates Communicative Development Inventories
(MB-CDI) ...37
4.4.3 Behavioral Assessment for Children, 2nd Edition (BASC-2) ...38
4.4.4 Infant-Toddler Social Emotional Assessment (ITSEA) ...40
4.5 Supporting Covariate Information ...42
4.6 Statistical Analyses ...44
4.6.1 Diagnostic Analyses: Descriptive Analyses ...46
4.6.2 Diagnostic Analyses: Specification of Covariates ...46
4.6.3 Diagnostic Analyses: Specification of Exposure ...49
4.6.4 Diagnostic Analyses: Specification of Outcomes ...51
4.6.5 Primary Analyses: Main Effects ...52
4.6.6 Primary Analyses: Effect Measure Modification by Sex of the Child ...52
4.6.7 Sensitivity Analyses ...53
4.7 Statistical Power ...53
4.8 Strengths and Limitations ...55
CHAPTER 5: PROTECTION OF HUMAN SUBJECTS ...58
CHAPTER 6: PRENATAL EXPOSURE TO ORGANOPHOSPHATE ESTERS AND BEHAVIORAL DEVELOPMENT IN YOUNG CHILDREN IN THE PREGNANCY, INFECTION, AND NUTRITION STUDY ...59
6.1 Overview ...59
6.2 Introduction ...60
6.3 Materials and Methods ...62
6.3.1 Study Population ...62
6.3.2 Measurement of OPE Metabolite Concentrations ...63
6.3.3 Behavioral Assessments ...64
6.3.4 Covariates ...66
6.4 Results ...67
6.4.1 Study Population ...67
6.4.2 OPE Metabolite Concentrations ...68
6.4.3 Behavioral Assessments ...68
6.4.4 Associations between OPE Metabolite Concentrations and Behavioral Assessments ...68
6.4.5 Sensitivity Analyses ...69
6.5 Discussion ...70
6.6 Conclusions ...76
CHAPTER 7: PRENATAL EXPOSURE TO ORGANOPHOSPHATE ESTERS AND COGNITIVE DEVELOPMENT IN YOUNG CHILDREN IN THE PREGNANCY, INFECTION, AND NUTRITION STUDY ...91
7.1 Overview ...91
7.2 Introduction ...92
7.3 Materials and Methods ...93
7.3.1 Study Population ...93
7.3.2 Assessment of Prenatal OPE Exposure ...94
7.3.3 Assessment of Cognitive Function ...95
7.3.4 Covariates ...97
7.3.5 Statistical Analyses ...97
7.3.6 Sensitivity Analyses ...98
7.4 Results ...98
7.4.1 Study Population ...98
7.4.2 OPE Metabolite Concentrations ...99
7.4.3 Cognitive Assessments...99
7.4.4 Associations between OPE Metabolite Concentrations and Cognitive Assessments ...99
7.5 Discussion ... 101
7.6 Conclusions ... 106
CHAPTER 8: CONCLUSIONS ... 118
8.1 Overview of Study ... 118
8.2 Results ... 119
8.2.1 Results: Associations between ip-PPP and Cognitive Development ... 119
8.2.2 Results: Associations between BDCIPP and Behavioral Development ... 120
8.2.3 Results: Effect Measure Modification by Sex of the Child ... 121
8.2.4 Results: Supplementary Analyses ... 122
8.3 Strengths and Limitations ... 124
8.3.1 Strengths and Limitations: Study Population ... 124
8.3.2 Strengths and Limitations: Exposure Assessment ... 125
8.3.2.1 Intra-individual Variability and Exposure Misclassification ... 125
8.3.2.2 Imperfect Sensitivity and Specificity of Metabolites ... 127
8.3.2.3 Variability from Laboratory Assays ... 128
8.3.3 Strengths and Limitations: Outcome Assessment ... 130
8.4 Summary ... 132
8.5 Concluding Remarks on OPEs and the Management of Toxicological Risks and the Role of Epidemiology ... 133
APPENDIX A. SUPPLEMENTAL TABLES ... 139
LIST OF TABLES
Table 1. Urinary OPE metabolite concentrations (ng/mL) measured in the PIN
Study and select comparison populations. ...11
Table 2. Relevant study population characteristics. ...27
Table 3. Characteristics of participants for whom both OPE measurements and developmental assessments are available. ...28
Table 4. OPE metabolites, abbreviations, and parent compounds. ...31
Table 5. Descriptive statistics of Standard Reference Materials, batch-specific CVs, and average of batch-specific CVs. ...33
Table 6. Distributions of concentrations of OPE metabolites measured in maternal urine samples collected in the PIN Study (n=349). ...33
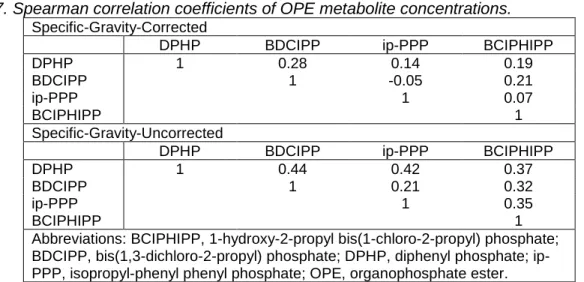
Table 7. Spearman correlation coefficients of OPE metabolite concentrations. ...34
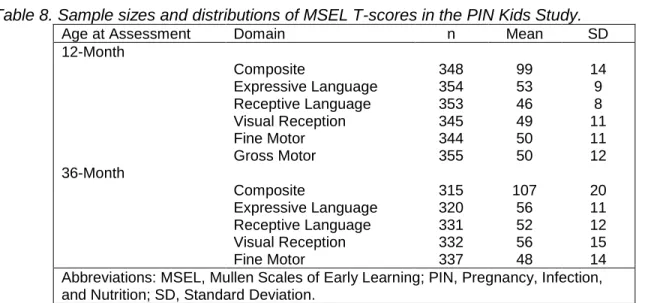
Table 8. Sample sizes and distributions of MSEL T-scores in the PIN Kids Study. ...36
Table 9. Pearson correlation coefficients between MSEL T-scores at 12 and 36 months. ...36
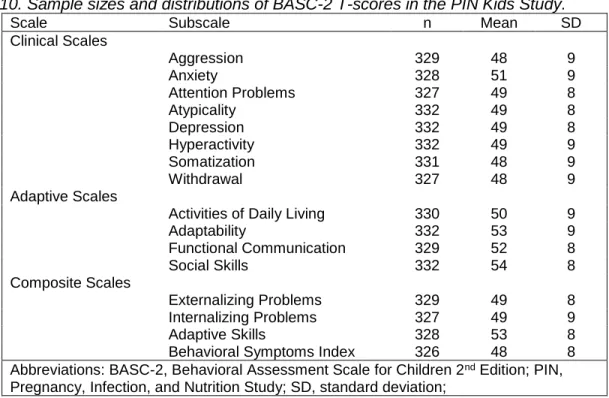
Table 10. Sample sizes and distributions of BASC-2 T-scores in the PIN Kids Study. ...40
Table 11. Sample sizes and distributions of ITSEA T-scores in the PIN Kids Study. ...41
Table 12. Percentages of children above and below age- and sex-specific cutpoints on ITSEA subscales. ...42
Table 13. Relevant covariate information collected in the PIN Studies. ...43
Table 14. Statistical analyses. ...45
Table 15. Covariates and functional forms. ...49
Table 16. Statistical power to detect statistically significant associations at a fixed Type-I error rate of 0.05 for various sample sizes. ...55
Table 17. Characteristics of the study population. ...78
Table 18. SG-corrected OPE metabolite concentrations (ng/mL) measured in maternal urine samples collected in PIN3 (n=349). ...80
Table 19. Behavioral assessment scores in the PIN3 Study...81
Supplemental Table 1. Behavioral assessments in the PIN3 Study. ...83 Supplemental Table 2. SG-uncorrected OPE metabolite concentrations (ng/mL)
measured in maternal urine samples collected in the PIN Study (n=349). ...84 Supplemental Table 3. Effect measure modification of primary associations by
child's sex. Covariate-adjusted change in behavioral assessment score per IQR change in log transformed, SG-corrected OPE metabolite concentration (ng/mL)
estimated using the ...85 Supplemental Table 4. Covariate-adjusted change in behavioral assessment
score by tertile of SG-corrected OPE metabolite concentration (ng/mL). ...87 Supplemental Table 5. Covariate-adjusted change in behavioral assessment
score per IQR change in log transformed, SG-corrected OPE metabolite
concentration (ng/mL), with all OPE metabolites included in a single model. ...89 Supplemental Table 6. Covariate-adjusted change in behavioral assessment
score per IQR change in log transformed, SG-uncorrected OPE metabolite
concentration (ng/mL). ...90 Table 21. Characteristics of the study population. ... 108 Table 22. OPE metabolite concentrations measured in maternal urine samples
collected in PIN3 (n=349) (specific gravity-corrected). ... 110 Table 23. Cognitive assessment scores in PIN3. ... 111 Table 24. Covariate-adjusted change in cognitive assessment scores per IQR
change in log transformed, SG-corrected OPE metabolite concentration (ng/mL). ... 112 Supplemental Table 7. OPE metabolite concentrations measured in maternal
urine samples collected in the PIN Study (n=349) (not corrected for specific
gravity content). ... 113 Supplemental Table 8. Effect measure modification of primary associations by
child's sex. Covariate-adjusted change in cogntive assessment scores per IQR change in log transformed, SG-corrected OPE metabolite concentration (ng/mL)
estimated using the ... 114 Supplemental Table 9. Covariate-adjusted change in behavioral assessment
score by tertile of SG-corrected OPE metabolite concentration (ng/mL). ... 115 Supplemental Table 10. Covariate-adjusted change in cognitive assessment
scores per IQR change in log transformed, SG-corrected OPE metabolite
concentration (ng/mL), with all OPE metabolites included in a single model. ... 116 Supplemental Table 11. Covariate-adjusted change in cognitive assessment
score per IQR change in log transformed, SG-uncorrected OPE metabolite
Table 25. Distributions of season of collection and delivery date of child among
analytic batches. ... 129 Appendix Table 1. Characteristics of the study population. ... 139 Appendix Table 2. OPE metabolite concentrations measured in maternal urine
samples collected in PIN3 (n=349) (specific gravity-corrected). ... 141 Appendix Table 3. OPE metabolite concentrations measured in maternal urine
samples collected in the PIN Study (n=349) (not corrected for specific gravity
content). ... 141 Appendix Table 4. Developmental assessment scores in the PIN3 Study. ... 142 Appendix Table 5. Covariate-adjusted associations between an IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
scores. ... 143 Appendix Table 6. Effect measure modification of primary associations by child's
sex. ... 145 Appendix Table 7. Categorical specifications of OPE metabolite concentrations. ... 149 Appendix Table 8. Covariate-adjusted associations between an IQR increase in
SG-corrected OPE metabolite concentrations and change in developmental
assessment scores, mutually adjusted for all OPE metabolites. ... 152 Appendix Table 9. Covariate-adjusted associations between IQR increase in
SG-uncorrected OPE metabolite concentrations and developmental assessment
scores. ... 154 Appendix Table 10. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment scores (alternative adjustment set: original adjustment set with addition of parity
and cigarette smoke)... 156 Appendix Table 11. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
scores (alternative adjustment set: crude). ... 158 Appendix Table 12. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
scores (alternative adjustment set: marital status, parity, and cigarette smoke). ... 160 Appendix Table 13. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
scores (alternative adjustment set: education only). ... 162 Appendix Table 14. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
Appendix Table 15. Covariate-adjusted associations between IQR increase in SG-corrected OPE metabolite concentrations and developmental assessment
scores (alternative adjustment set: original covariate set, plus delivery date). ... 166 Appendix Table 16. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
scores, restricted to participants with OPE metabolites below the 99th percentile. ... 168 Appendix Table 17. Covariate-adjusted associations between IQR increase in
SG-corrected OPE metabolite concentrations and developmental assessment
scores, with adjustment for PBDE-47, PCB-153, and DDE. ... 170 Appendix Table 18. Odds of "Of Concern" score on ITSEA subdomains per IQR
increase in SG-corrected OPE metabolite concentrations. ... 172 Appendix Table 19. Effect measure modification of primary associations by
season of OPE measurement (summer vs. non-summer). ... 173 Appendix Table 20. Covariate-adjusted associations between BCIPP
concentrations and performance on cognitive and behavioral developmental
LIST OF FIGURES
Figure 1. OPEs and metabolites of interest in the PIN Study. ... 8 Figure 2. Direct and indirect pathways through which maternal OPE exposure
during pregnancy could influence offspring's cognition and behavior. ...13 Figure 3. Directed Acyclic Graph depicting hypothesized causal relations
between Maternal OPE Metabolite Concentrations in Urine and Child's Score on
Developmental Assessments. ...48 Figure 4. Estimated change in children's score on BASC-2 composites per IQR
increase in log-transformed, specific gravity corrected OPE metabolite
concentration measured in maternal prenatal urine. ...77 Figure 5. Estimated change in children’s score on Mullen Scales of Early
Learning (Composite Score and Scales) per IQR increase in log transformed, specific-gravity-corrected OPE metabolite concentration measured in maternal
LIST OF ABBREVIATIONS ADHD Attention-Deficit/Hyperactivity Disorder AIC Aikake Information Criterion
BASC-2 Behavioral Assessment Scale for Children, 2nd Edition BCIPHIPP 1-hydroxyl-2-propyl bis(1-chloro-2-propyl) phosphate BCIPP bis(1-chloro-2-propyl phosphate)
BDCIPP bis(1,3-dichloro-2-propyl phosphate)
BMI Body Mass Index
CADS Conner’s ADHD/DSM-IV Scales
CD Conduct Disorder
CHAMACOS Center for the Health Assessment of Mothers and Children of Salinas CV coefficient of variation
DAG directed acyclic graph
DDE dichlorodiphenyldichloroethylene DPHP diphenyl phosphate
EMM effect measure modification ESI electrospray ionization FM550 Firemaster™ 550
GAM Generalized Additive Models
GM geometric mean
ICC Intraclass Correlation Coefficient ip-PPP isopropyl-phenyl phenyl phosphate IQR interquartile range
IRB Institutional Review Board
ITSEA Infant-Toddler Social Emotional Assessment LC-MS/MS liquid chromatography tandem mass spectrometry
MB-CDI MacArthur-Bates Communicative Development Inventories MDL method detection limit
MLE Maximum Likelihood Estimation MSEL Mullen Scales of Early Learning
NHANES National Health and Nutrition Examination Survey
NR not reported
ODD Oppositional Defiant Disorder OPE organophosphate ester
PBDE polybrominated diphenyl ethers PCB polychlorinated biphenyl
PIN Study Pregnancy, Infection, and Nutrition Study
PIN3 Study Pregnancy, Infection, and Nutrition Study, 3rd Phase PRS-P parent rating scale for preschool-age children
SD standard deviation
SE standard error
SG specific gravity
SPE solid phase extraction SRM standard reference material
T3 triiodothyronine
T4 thyroxine
TDCIPP tris(1,3-dichloro-2-propyl) phosphate TPHP triphenyl phosphate
UNC-CH University of North Carolina at Chapel Hill
CHAPTER 1: INTRODUCTION AND SPECIFIC AIMS
Certain organophosphate esters (OPEs) possess physicochemical properties that support their use as flame retardants, plasticizers, lubricants, and in other applications [1-3]. Production of these compounds has increased in recent years [1, 3-5] as manufacturers have sought alternative flame retardant compounds amid increasing concerns of the environmental fate and toxicity of previously-used flame retardant compounds (specifically, polybrominated diphenyl ethers, or PBDEs) [4-8]. OPEs are applied to products as chemical “additives”, meaning they are applied post-polymerization and are not chemically bound to products, and are therefore vulnerable to volatilization and leaching into nearby media and the environment [1-3]. OPEs are applied to a variety of common consumer products, including polyurethane foam (e.g., in sofas or furniture cushions) [1, 3], electronic devices [9, 10], baby products [11], recreational equipment [12, 13], and nail polishes [14].
In accordance with their application to a variety of consumer products and their capacity to volatilize and leach from materials, OPE compounds are present at detectable concentrations in many human environments [1-3, 15-20], including residential housing [15, 17, 20-26], office spaces [15, 17, 19, 20, 27, 28], and child care environments [15, 19, 20, 29, 30]. These
compounds can enter the human body through inhalation, ingestion, and dermal absorption [3, 31]; inhalation and/or ingestion of indoor dust is a well-documented source of exposure among the general population [3, 17, 19, 21, 23, 24, 26, 31-34], though absorption following dermal contact [12, 13, 35-37], respiration of contaminated air [20, 28, 38], ingestion of contaminated food [33, 39], consumption of contaminated water [40], and other pathways can also contribute to exposure [3, 31]. Inside the human body, these compounds are metabolized to their
other metabolic and excretion pathways also exist [31, 45, 48]. Biological half-lives of OPEs in humans are likely on the order of hours to days [42, 43, 47, 49], though frequent exposure ensures constant presence in the body. Biological markers of OPE exposure are consequently detected with high frequency in biomonitoring surveys and observational studies [20, 21, 24, 25, 33, 34, 50-60]. Consistent with these findings, exposure among pregnant women and women of reproductive age occurs with similar high frequency [21, 52, 53, 55, 56].
indirectly affect fetal development. In summary, exposure to OPEs is largely unavoidable in the modern human environment, and pregnant women and their developing children, who are especially vulnerable to potential toxic effects of exogenous pollutants, are among the exposed.
Mounting experimental and observational evidence suggests that OPEs are capable of interfering with physiologic processes related to cognitive and behavioral development [25, 79-93]. For instance, it is well established that disruption of maternal or fetal endocrine function during pregnancy can adversely affect development of physiologic structures and properties related to cognition and behavior [94-102], and substantial evidence indicates that OPEs can interfere with the endocrine system through multiple pathways [25, 80, 81, 84-89, 91, 92, 103]. For example, several in vivo experimental studies have reported associations between OPE exposure and sex and thyroid hormone expression in model organisms [80, 81, 84-86, 88, 91, 92], and similar associations have been reported in a small number of observational studies in human populations [25, 87]. Additionally, both in vivo and in vitro experimental evidence indicates OPEs (or their metabolites) are potentially neurotoxic [79, 82, 88, 90, 104-107]. For example, Wang et al. [90] reported that TDCIPP exposure decreased concentrations of the neurotransmitters serotonin and dopamine in zebrafish. Additionally, Dishaw et al. [79] reported TDCIPP increased oxidative stress, decreased cell number, and increased differentiation into both dopaminergic and cholinergic neurophenotypes in exposed PC12 cells (rat adrenal cells), and that TDCIPP displayed greater potential neurotoxicity than chlorpyrifos (a known
neurotoxin). Other pathways through which OPEs could influence cognition and behavior are also plausible (e.g., interference with nuclear receptors) [85, 108-111]. Additionally, recent in vivo studies have reported behavioral changes in model organisms exposed to OPEs [112-116]. Some of these studies reported sex-specific effects of OPE exposure [84-89], which are
exposure. In the first, Lipscomb et al. [83] performed a cross-sectional study to evaluate associations between ∑OPE concentrations measured in passive silicone samplers worn by children and the children’s scores on the Social Skills Improvement Rating Scale, a teacher-rated social behavior assessment, in a population of children ages three to five years (n=72). The investigators reported that greater ∑OPE concentrations in the passive samplers were associated with poorer scores on the Responsibility subscale and greater scores on the Externalizing subscale, both reflecting adverse effects. Key limitations of this study include its modest sample size, cross-sectional study design, and utilization of a summary measure of OPEs. In a second investigation, Castorina et al. [118] used data from the Center for the Health Assessment of Mothers and Children of Salinas (CHAMACOS) in California to investigate associations between concentrations of three OPE metabolites (diphenyl phosphate or DPHP, bis(1,3-dichloroisopropyl) phosphate or BDCIPP, and isopropylphenyl phenyl phosphate or ip-PPP) measured in urine collected from mothers during pregnancy and offspring’s performance on three psychometric assessments administered at 7 years of age (n’s from 248 to 282): the Wechsler Intelligence Scale for Children 4th edition (WISC-IV), the Behavior Assessment
in other study populations is necessary to make stronger inference about the potential developmental effects of early life OPE exposures.
Data collected from the third phase of the Pregnancy, Infection, and Nutrition Study (PIN3 Study) and subsequent follow-ups (including PIN Postpartum and PIN Kids; hereafter collectively referred to as “PIN Study” or “PIN Studies”) provide an efficient opportunity to investigate developmental effects of prenatal exposure to OPEs [55, 56, 119]. Briefly, the PIN Studies constitute a prospective birth cohort study of pregnant women living in central North Carolina who delivered between 2001 and 2006 (n=2006) and were followed-up repeatedly post-pregnancy, during which their children’s cognition and behavior were assessed using multiple developmental assessments. To estimate prenatal exposure to OPEs, we used
concentrations of metabolites of TPHP, TDCIPP, ip-DPHP, and TCIPP measured in a spot urine sample collected from pregnant mothers between 24 and 30 week’s gestation. For measures of cognitive development, we used children’s scores on the Mullen Scale of Early Learning (MSEL) [120] administered at 12 and 36 months (n of 358 and 341, respectively), as well as the
MacArthur-Bates Communicative Development Index (MB-CDI) administered at 12 and 36 months (n of 401 and 380, respectively). For measures of behavioral development, we used children’s scores on the Infant Toddler Social Emotional Assessment (ITSEA) [121] and Behavior Assessment System for Children-2 (BASC-2) [122], which are available for
In summary, our investigation will seek to improve the understanding of developmental toxicity of prenatal exposure to OPEs, with emphasis on cognitive and behavioral development and sex-specific effects. This information will contribute to decision making pertaining to the use and regulation of these compounds.
We therefore used data collected in the PIN Study to investigate the following specific aims: Aim 1. Investigate the association between prenatal exposure to triphenyl phosphate
(TPHP), isopropylated triarylphosphate isomers (ITPs), tris(1,3-dichloro-2-propyl) phosphate (TDCIPP), and tris(1-chloro-2-propyl) phosphate (TCIPP) and cognitive development.
Sub Aim 1a. Investigate effect measure modification of the above relationship by sex of the child.
Aim 2. Investigate the association between prenatal exposure to triphenyl phosphate (TPHP), isopropylated triarylphosphate isomers (ITPs), tris(1,3-dichloro-2-propyl) phosphate (TDCIPP), and tris(1-chloro-2-propyl) phosphate (TCIPP) and behavioral development.
CHAPTER 2: BACKGROUND AND REVIEW OF LITERATURE 2.1 Modern Uses of Organophosphate Flame Retardants and Plasticizers
In order to comply with regulations pertaining to flammability standards of consumer products, manufacturers of consumer goods, including furniture and electronic devices, routinely apply chemical flame retardants to their products [5, 22, 123]. Until the mid-2000s,
polybrominated diphenyl ethers (PBDEs) were among the most commonly used commercial chemical flame retardants [5, 22, 123]. Amid concerns of their environmental fate and potential toxicity, however, PBDEs were phased out of production and a new class of flame retardants, organophosphate flame retardants (OPEs), has emerged as an alternative to PBDEs among manufacturers [5, 22, 123]. As a result, recent years have witnessed increased production of these compounds [1-5, 18]. Some OPEs (including triphenyl phosphate (TPHP) and arylated analogs (e.g., isopropylated triarylphosphate isomers, ITPs) are components of FireMaster™ 550 (FM550) [5, 112, 124], a flame retardant mixture commonly applied to polyurethane foam [1, 5, 124]. Other OPEs, including tris(1,3-dichloro-2-propyl) phosphate (TDCIPP), and tris(1-chloro-2-propyl) phosphate (TCIPP), are also used as flame retardants [1, 4]. Additionally, OPEs are sometimes mixed with other chemicals to produce flame retardant mixtures, such as FireMaster 550™ [112]. OPEs are applied as “additive” flame retardants (as opposed to
2.2 Environmental Presence and Human Exposure
In accordance with their application to a variety of ubiquitous consumer products and their capacity to volatilize and leach from their materials, OPEs are present at detectable concentrations in many human environments [1-3, 15-20], including residential housing [15, 17, 20-26], office spaces [15, 17, 19, 20, 27, 28], and child care environments [15, 19, 20, 29, 30]. In particular, OPEs can accumulate in the dust of indoor environments, which, following disruption, can lead to their suspension as air particles [30]; consequently, inhalation and/or ingestion of indoor dust are significant and well-documented sources of exposure [3, 17, 19, 21, 23, 24, 26, 31-34], though absorption following dermal contact [12, 13, 35-37], respiration of contaminated air [20, 28, 38], ingestion of contaminated food [33, 39], consumption of contaminated water [40], and other pathways can also contribute to exposure [3, 31].
Inside the body, OPEs are metabolized to their respective mono- or diesters [6, 31, 41-46], which are primarily excreted in urine [42, 43, 47], though other metabolic and excretion pathways also exist [31, 45, 48]. Biological half-lives of mono- and diester metabolites are likely on the order of hours to days [42, 43, 47, 49]. A consequence of relatively short biological half-lives is that spot assessments are vulnerable to exposure misclassification due to intra-individual variability in exposure over time. Studies of intra-individual variability in OPE
metabolite concentrations have reported intraclass correlation coefficients (ICCs) for OPEs typically ranging between 0.3 and 0.8, indicating low to moderate reproducibility, depending on the metabolite, study population, and time period of interest [55, 126-128]. Despite these short
OPE diester metabolites (and other biological markers of OPE exposure) are consistently detected with high frequencies in biomonitoring surveys and observational studies [20, 21, 24, 25, 33, 34, 50-60].
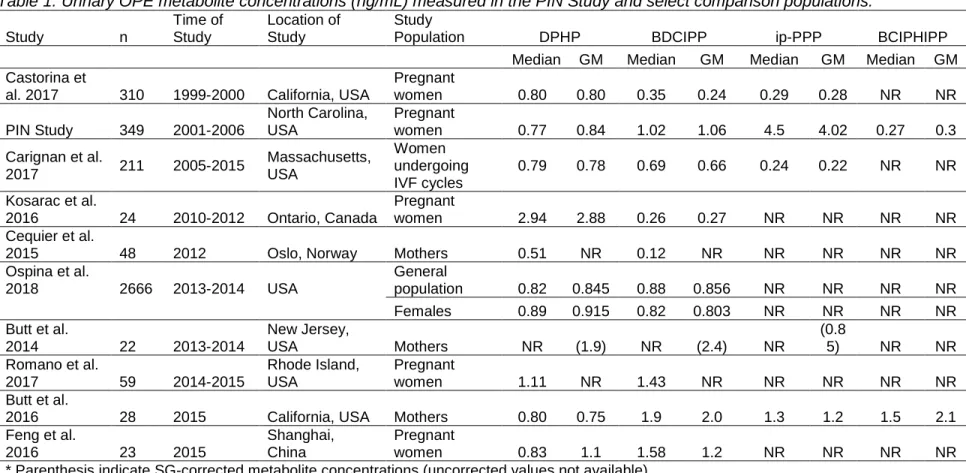
A summary of previously reported urinary OPE metabolite concentrations measured in the PIN Study and select comparison populations is presented in Table 1. Relative to Castorina et al. [21], the only previous epidemiologic investigation of prenatal OPE exposure, our study population possessed comparable levels of DPHP, but notably higher levels of both BDCIPP and ip-PPP. We suspect this to be due to our study enrollment period occurring between 2001 and 2006, after the PBDE phase-out and subsequent increase in OPE usage that occurred in 2003-04, whereas Castorina et al. enrolled participants between 1999 and 2000, prior to the PBDE phase-out. Evidence suggests that OPE exposures have increased substantially since the PBDE phase-out [54]. In light of this, it is interesting to note that the levels of DPHP and BDCIPP in our study population were comparable to those reported in the
11
Table 1. Urinary OPE metabolite concentrations (ng/mL) measured in the PIN Study and select comparison populations.
Study n
Time of Study
Location of Study
Study
Population DPHP BDCIPP ip-PPP BCIPHIPP
Median GM Median GM Median GM Median GM
Castorina et
al. 2017 310 1999-2000 California, USA
Pregnant
women 0.80 0.80 0.35 0.24 0.29 0.28 NR NR
PIN Study 349 2001-2006
North Carolina, USA
Pregnant
women 0.77 0.84 1.02 1.06 4.5 4.02 0.27 0.3
Carignan et al.
2017 211 2005-2015
Massachusetts, USA
Women undergoing IVF cycles
0.79 0.78 0.69 0.66 0.24 0.22 NR NR
Kosarac et al.
2016 24 2010-2012 Ontario, Canada
Pregnant
women 2.94 2.88 0.26 0.27 NR NR NR NR
Cequier et al.
2015 48 2012 Oslo, Norway Mothers 0.51 NR 0.12 NR NR NR NR NR
Ospina et al.
2018 2666 2013-2014 USA
General
population 0.82 0.845 0.88 0.856 NR NR NR NR
Females 0.89 0.915 0.82 0.803 NR NR NR NR
Butt et al.
2014 22 2013-2014
New Jersey,
USA Mothers NR (1.9) NR (2.4) NR
(0.8
5) NR NR
Romano et al.
2017 59 2014-2015
Rhode Island, USA
Pregnant
women 1.11 NR 1.43 NR NR NR NR NR
Butt et al.
2016 28 2015 California, USA Mothers 0.80 0.75 1.9 2.0 1.3 1.2 1.5 2.1
Feng et al.
2016 23 2015
Shanghai, China
Pregnant
women 0.83 1.1 1.58 1.2 NR NR NR NR
* Parenthesis indicate SG-corrected metabolite concentrations (uncorrected values not available).
2.3 Exposure among Pregnant Women and Vulnerability of the Developing Fetus Consistent with findings among the general population, exposure to OPEs among pregnant women occurs with similar high frequency [21, 52, 53, 55, 56]. Exposure among pregnant women is of particular concern as it introduces the possibility of affected fetal
development through both direct and indirect pathways; here, direct pathways of exposure refer to an exogenous agent directly interacting with tissues and organs of the developing fetus, whereas indirect pathways of exposure originate from alternations in maternal physiology that subsequently affect fetal development. Fetal exposure through any pathway is concerning as the prenatal period is a particularly sensitive period of development [61-65] because it is during this time that tissues and organs are developing and undergoing foundational time-sensitive structural changes, and physiological insults that occur during this period produce more significant and longer-lasting changes, relative to perturbations that occur after tissues and organs have more fully formed [61, 62, 64, 131]. Consequently, even apparently mild
perturbations of maternal or fetal physiology that occur during the sensitive prenatal period can meaningfully impact adult physiology [65, 67-69, 132].
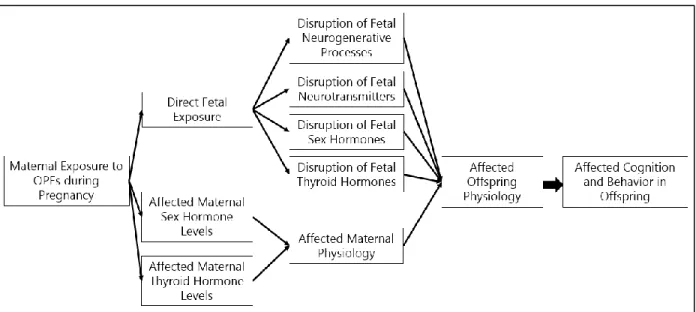
pregnancy, both directly and indirectly; these pathways are described in greater detail below with supporting evidence from experimental and observational studies.
Figure 2. Direct and indirect pathways through which maternal OPE exposure during pregnancy could influence offspring's cognition and behavior.
2.4 Direct Fetal Exposure and Potential Toxicity
Direct evidence of fetal exposure to OPEs is currently limited, though available evidence indicates it is likely that significant maternal-fetal transfer of OPEs occurs. For example, Zhao et al. [70] measured several OPEs and their metabolites in human chorionic villi and deciduae, indicating potential maternal-fetal transfer in early gestation, prior to the development of a mature placenta. Other evidence suggests that placental accumulation and transplacental transfer of OPEs may occur. For example, Ding et al. measured TPHP and TDCIPP in 86% and 44% (respectively) of placental tissue samples obtained from 50 pregnant women living in China [52]. Interestingly, an experimental study by Baldwin et al. [71] observed sex-specific
accumulation of TPHP in rat placentas (a potential mechanism for sex-specific effects), but did not observe transfer to pups; a similar study also did not observe gestational transfer of OPEs to rat pups [148]. Beyond OPEs, related exogenous pollutants, such as organophosphorus
similarly capable of such trans-placental transfer. Ultimately, degree of maternal-fetal transfer of a xenobiotic is influenced by a variety of factors, including molecular weight [75], protein binding capacity [76], degree of active transport [76, 77], actions of placental metabolizing enzymes [77], and other physicochemical properties of the compounds, such as degree of halogenation [78]. Given the low molecular weight of many OPE compounds (all compounds of interest in this study < 500 Da), a significant degree of maternal-fetal transfer, including transplacental transfer, is likely to occur. Because it is plausible that maternal exposure to OPEs during pregnancy results in direct fetal exposure, it is necessary to consider the pathways through which such direct exposure might influence offspring’s cognition and behavior.
One such pathway is through disruption of neurogenerative processes (e.g.,
proliferation, migration, differentiation, synaptogenesis, myelination, apoptosis, cytotoxicity to neuronal cells, altered neuronal cell transcription), which are foundational to the formation of the brain [65, 149], and for which there exists suggestive experimental evidence that OPEs are capable of interfering with these neurogenerative processes [79, 82, 88, 90, 104-107]. For example, Dishaw et al. [79] reported TDCIPP increased oxidative stress, decreased cell
number, and increased differentiation into both dopaminergic and cholinergic neurophenotypes in rat adrenal cells, and that TDCIPP displayed greater potential neurotoxicity than chlorpyrifos (an established neurotoxin). Relatedly, prenatal neurotransmitter levels also play a significant role in the development of structures related to cognition and behavior [150-155], and there exists limited experimental evidence that OPEs may influence expression and levels of these essential compounds [88, 90]. For example, in two related studies, Wang et al. [88, 90] reported that exposure to TDCIPP decreased concentrations of the neurotransmitters serotonin and dopamine in zebrafish, and potentially in a sex-specific fashion.
and behavioral development is well-documented [94, 96, 97, 99-102]. There exists both experimental and observational evidence that OPEs can interfere with functioning of the endocrine system, specifically by modifying the expression and action of sex [25, 84-86, 89, 103, 156] and thyroid hormones [25, 80, 81, 87, 91, 92]. For example, in one in vivo study of zebrafish larvae exposure to TPHP, Kim et al. reported that TPHP exposure increased concentrations of both triiodothyronine (T3) and thyroxine (T4). More recently, in an
observational study of OPE exposure and thyroid hormone concentrations, Preston et al. [87] reported that urinary TPHP metabolite concentrations were associated with increased total T4, and that this association was stronger among women than men.
Taken together, although evidence that maternal exposure to OPEs during pregnancy results in direct fetal exposure is limited, it remains a plausibility given recent evidence
indicating maternal-fetal transfer [52, 70] and that related compounds are known to cross the placental barrier; if direct fetal exposure does occur, it could potentially perturb fetal cognitive and behavioral development through the pathways described above.
2.5 Indirect Fetal Exposure and Potential Toxicity
As previously established, pregnant women are frequently exposed to OPEs from their environments [21, 52, 53, 55, 56]. As maternal physiology is intimately linked to fetal physiology and development, physiologic effects of OPE exposure experienced by a pregnant woman during pregnancy can indirectly affect the development of her offspring. Of particular concern are alterations in maternal endocrine function, including thyroid function [95, 98, 157-161] and sex hormone concentrations [97], as these hormones perform critical functions in the
development of anatomical structures and physiological systems related to cognitive and behavioral development in the fetus [162-167]. As outlined above, there is substantial evidence that OPEs can interfere with both sex hormone [25, 84-86, 89, 103, 156] and thyroid hormone [25, 80, 81, 87, 91, 92] activity, including limited evidence from human studies [25, 87].
affecting the hormonal environment in utero, and ultimately affecting development of organs and tissues related to cognitive and behavioral development in the fetus.
2.6 Experimental Evidence of Behavioral Effects in Animal Models
Beyond evidence of pathway-specific toxicity, there also exists a growing body of experimental evidence relating OPE exposures to behavioral changes in model organisms [88, 113-115, 168, 169]. In one such study, Oliveri et al. [115] reported that zebrafish exposed to TDCIPP in early life exhibited elevated locomotor activity and reduced predator escape behavior in adulthood, relative to controls. Although evidence of behavioral effects in model organisms is valuable and suggestive of potential behavioral effects of OPE exposure in humans, it is
important to recognize that extrapolation of evidence from experimental animal models to humans is challenging; most importantly, animal physiologies may meaningfully differ from humans, and the exposures experienced by model organisms in experimental settings (doses, pathways, mixtures) may not adequately emulate exposures experienced by human
populations. Therefore, it is necessary to determine whether behavioral abnormalities are also observed in human populations.
2.7 Epidemiologic Evidence of Cognitive and Behavioral Effects
In a second investigation, Castorina et al. [118] investigated associations between concentrations of three OPE metabolites measured in urine collected from mothers during pregnancy (mean: 26 weeks) and offspring’s performance on three psychometric assessments administered at 7 years of age (n’s from 248 to 282): the Wechsler Intelligence Scale for
Children 4th edition (WISC-IV), the Behavior Assessment System for Children 2nd edition (BASC-2), and the Conners’ ADHD/DSM-IV Scales (CADS). The authors reported that higher
concentrations of OPE metabolites in urine during pregnancy were associated with worse scores on the WISC-IV (particularly the Working Memory scale), and higher scores on the BASC-2 Hyperactivity scale. Strengths of this study include its prospective birth cohort design, assessment of exposure during the sensitive prenatal window, and the relatively diverse array of neurobehavioral dimensions assessed. However, mothers in this study were enrolled between 1999 and 2000, prior to the PBDE phase-out and subsequent increase in OPE usage, therefore OPE exposure levels may not reflect exposures post-PBDE phase-out, which are likely to be higher.
In summary, the limited body of available epidemiologic evidence suggests early life exposures to OPEs may be associated with cognitive and behavioral effects, though these studies are not without their limitations, and reproduction of their results in other study populations is necessary to make stronger inference about the potential cognitive and behavioral effects of early life OPE exposures.
2.8 Endocrine-Disrupting Compounds and Sex-Specific Associations
thorough investigation of cognitive and behavioral effects of OPE exposure must include evaluation of sex-specific effects.
2.9 Significance of Potential Cognitive and Behavioral Effects of OPEs
Exposure to OPEs is pervasive in the United States and elsewhere, particularly following the phase-out of PBDEs, and available evidence suggests these compounds are biologically-active in manners potentially detrimental to cognitive and behavioral development in humans. The ubiquitous presence of chemical agents potentially capable of interacting with the
CHAPTER 3: INNOVATION
Our investigation, a secondary analysis of relevant data from the PIN Studies, possesses innovative aspects.
First, available epidemiologic evidence of developmental effects of prenatal OPE exposure is limited, and our investigation will strengthen this body of evidence. More
specifically, our investigation will be the second epidemiologic study of developmental effects of OPE exposures during the sensitive prenatal period, and the third epidemiologic study relating OPE exposure to developmental qualities overall. These two studies, performed by Lipscomb et al. and Castorina et al., have been described above. Briefly, the first investigation of behavioral effects of early life exposure to OPEs was performed by Lipscomb et al. [83], who evaluated cross-sectional associations between ∑OPE concentrations measured in passive silicone samplers worn by children and scores on the Social Skills Improvement Rating Scale in a population of children (n=72) ages three to five years; the investigators reported that greater ∑OPE concentrations in the passive samplers were associated with poorer scores on the Responsibility subscale and greater scores on the Externalizing subscale, both reflecting adverse effects. While suggestive of potential behavioral effects, these findings are somewhat limited by the study’s modest sample size, cross-sectional study design, assessment of only a single exposure pathway (dust and suspended particles), and assessment of exposure during a period of potentially limited sensitivity (i.e., post-natal).
To our knowledge, the only prior epidemiologic study of developmental effects of
measured in urine collected from mothers during pregnancy and offspring’s performance on three psychometric assessments administered at 7 years of age (n’s from 248 to 282). The authors reported that higher concentrations of OPE metabolites (particularly DPHP) in urine during pregnancy were associated with poorer scores on the WISC-IV (particularly the Working Memory scale), and higher scores on the BASC-2 Hyperactivity scale. In an improvement over Lipscomb et al., this study was strengthened by its prospective birth cohort design that allowed for assessment of exposure during the sensitive prenatal period and establishment of
temporality of effects. This study also benefited from administration of a relatively diverse array of developmental instruments, which allowed for assessment of a broad array of developmental endpoints. However, mothers in this study were enrolled between 1999 and 2000, prior to the PBDE phase-out and subsequent increase in OPE usage, therefore exposure levels may not reflect exposures post-PBDE phase-out, which are likely to be higher. Data from the PIN Study indicate that mothers in this population were more highly exposed and experienced a wider distribution of exposures, which will likely support our ability to observe effects of exposure. While these two studies (Lipscomb et al. and Castorina et al.) are generally suggestive of developmental effects of early life OPE exposures, it is necessary to reproduce their findings in other populations to strengthen epidemiologic inference. Ultimately, limitations of observational epidemiology require reproduction of study results and an accumulation of evidence, and our study using data collected by the PIN Studies will contribute to this body of evidence.
measured with high frequency in our study sample (98% > MDL). Therefore, our analysis, which will include investigation of associations with BCIPHIPP, and will be the first assessment of developmental effects of TCIPP exposure in humans. This is significant, as previous studies have established that TCIPP exposure is highly prevalent [4, 7, 15, 21, 22, 27, 30, 51, 52, 125, 177-183], and experimental studies have reported associations between TCIPP exposure and endocrine-related [80, 84, 104, 156] and behavioral [114] endpoints, which supports
investigation of this compound’s potential developmental effects.
Third, our investigation will assess cognitive and behavioral dimensions that have not been previously assessed in relation to early life OPE exposure. Assessment of a broad array of developmental endpoints is valuable because, in light of limited observational evidence, it remains unclear which physiologic structures and corresponding developmental qualities are most sensitive to effects of OPE exposures in humans. Therefore, identifying sensitive
endpoints will improve our understanding of developmental effects of OPE exposures and help to guide future research. For example, our investigation will be the first to assess associations between OPE exposure and dysregulation-related qualities (i.e., problems with sleeping, problems with eating, negative emotionality, sensory sensitivity), as assessed by the Infant-Toddler Social Emotional Assessment (ITSEA). The investigation of associations between OPE exposures and the dysregulation-related qualities will be a valuable contribution to our
which have not been previously assessed. The identification of either positive or null associations with these qualities will be valuable for the reasons stated above.
Additionally, our investigation will assess associations between early life OPE exposure and domains that are related, but not identical, to those that have been previously assessed. For example, we will assess associations between OPE exposure and vocabulary production and grammatical complexity – qualities measured by the MacArthur-Bates Communicate Development Inventory (MB-CDI). Although other studies have included assessments of linguistic qualities, such as the Communication subscale of the Social Skills Improvement
System Rating Scale (Lipscomb et al.) and the Verbal Comprehension subscale of the Wechsler Intelligence Scale for Children (Castorina et al.), the linguistic qualities measured by the MB-CDI are not identical to those obtained from previous assessments; for example, the measurements obtained from the MB-CDI may reflect more functional endpoints, and neither of the previous assessments have been obtained through parent-report (as opposed to teacher-report or self-report), which provides unique strengths and weaknesses. This is not to suggest that our
CHAPTER 4: APPROACH 4.1 Overview
The primary objective of our investigation was to examine associations between maternal exposure to OPEs during pregnancy and offspring’s development, including both cognitive and behavioral dimensions. We used data collected by the third phase of the PIN Study (PIN3) and subsequent follow-up studies (PIN Postpartum and PIN Kids; collectively “PIN Study” or “PIN Studies”), which constitute a prospective observational cohort study of mothers who delivered at the University of North Carolina Hospital between 2001 and 2006 and were followed-up post-pregnancy. Participating mothers were recruited in early pregnancy and provided demographic, health, and lifestyle information, as well as biological samples, including a urine specimen, which was used to measure concentrations of certain OPE metabolites. After the birth of the child, mother-child pairs completed multiple follow-up visits between 3 and 36 months postpartum. During these follow-up visits, which took place at participants’ homes, mothers provided additional demographic, health, and lifestyle information, and their children’s cognitive and behavioral development was assessed using a variety of psychological
Aim 1. Investigate the association between prenatal exposure to triphenyl phosphate (TPHP), isopropylated triarylphosphate isomers (ITPs), tris(1,3-dichloro-2-propyl) phosphate (TDCIPP), and tris(1-chloro-2-propyl) phosphate (TCIPP) and cognitive development.
Sub Aim 1a. Investigate effect measure modification of the above relationship by sex of the child.
Aim 2. Investigate the association between prenatal exposure to triphenyl phosphate (TPHP), isopropylated triarylphosphate isomers (ITPs), tris(1,3-dichloro-2-propyl) phosphate (TDCIPP), and tris(1-chloro-2-propyl) phosphate (TCIPP) and behavioral development.
Sub Aim 2a. Investigate effect measure modification of the above relationship by sex of the child.
4.2 Study Design and Study Population
Our analysis used data collected during the third phase of the Pregnancy, Infection, and Nutrition Study (PIN3) and subsequent follow-up studies, PIN Postpartum and PIN Kids
(collectively “PIN Study” or “PIN Studies”). The PIN Studies constitute an observational birth cohort study of prospective mothers living in central North Carolina recruited from prenatal care clinics at University of North Carolina hospitals between January 2001 and July 2005. Women were eligible to participate if they were older than 16 years of age, of 20 or fewer weeks
activity. During this telephone interview, participants were asked to schedule a visit to the UNC General Clinical Research Center to occur between 24 and 29 weeks gestation to provide certain biological samples, including a urine sample. Lastly, between 27 and 30 weeks gestation, women were contacted by phone to provide updated information regarding the qualities assessed in the first telephone interview, and to also solicit information pertaining to economic assistance, behaviors (e.g., sexual activity, drug use), vitamin and supplement use, experiences of discrimination, and residential information. Participating mothers gave birth between December 2002 and December 2005. Births were identified by daily screening of hospital delivery logs. Delivery information was abstracted from medical records and was available for 1942 mother-child pairs.
Eligible mother-child pairs were invited to participate in postpartum follow-up visits (PIN Postpartum) at approximately 3 and 12 months; eligibility criteria included: agreed to be
contacted after delivery, singleton birth without major birth defects, and did not get pregnant in the year postpartum. Mothers who completed these follow-up visits were invited to also
participate in PIN Kids, which included additional follow-up visits at approximately 24 and 36 months. In total, 688 mothers participated in the 3-month follow-up, 550 mothers participated in the 12-month follow-up, 391 mothers participated in the 24-month follow-up, and 409 mothers participated in the 36 month-follow-up. During each of these follow-ups, which typically occurred at participants’ homes (or, rarely, by mail), mothers provided the following information: biometric measurements (e.g., height, weight), dietary information, breastfeeding status, behaviors, health status, occupational status, physical activity, and psychosocial measures. Additionally, during these at-home follow-up visits, children’s cognitive and behavioral development was assessed using a variety of psychological instruments. Specifically, trained staff administered the Mullen Scale of Early Learning (MSEL) to children at approximately 3 (n=315), 12 (n=358), and 36 (n=341) months postpartum; additionally, mothers completed the MacArthur-Bates
months (n=380), the Behavioral Assessment for Children, 2nd edition (BASC-2) at approximately 36 months (n=332), and the Infant-Toddler Social and Emotional Assessment (ITSEA) at
approximately 24 months (n=391).
Our analyses were limited to mothers who provided urine samples and whose urine samples were assessed for concentrations of OPE metabolites. Urine samples were analyzed for OPE metabolite concentrations if there was sufficient urine volume and if the child had growth measurements at birth, 3, 12, or 36 months [56]. Ultimately, the analysis of urine samples yielded useable OPE metabolite concentrations for 349 mothers.
Table 2 provides sample sizes and characteristics of the study population at key points during the study. In general, the baseline PIN3 Study population is primarily middle-aged (71% older than 25 years), white (69%), and well-educated (75% with at least some college). Mothers who participated in follow-ups were more likely than mothers in the overall baseline population to be older, white, better educated, and of lower Body Mass Index. Mothers for whom we have OPE metabolite concentrations are comparable to the population of mothers who participated in follow-ups.
Table 2. Relevant study population characteristics. Baseline
Cohort
Delivery
Information 3-Month
12-Month 36-Month OPE Metabolites
n=2006 n=1942 n=688 n=550 n=409 n=349
Maternal Age at Child's Birth
<=25 568 (28) 542 (28) 163 (24) 118 (21) 81 (20) 77 (22)
26-30 641 (32) 623 (32) 221 (33) 177 (32) 135 (33) 126 (36)
31-35 560 (28) 545 (28) 219 (33) 177 (32) 134 (33) 107 (31)
>35 237 (12) 232 (12) 85 (13) 78 (14) 59 (14) 39 (11)
Maternal Race
White 1382 (69) 1337 (69) 526 (76) 433 (79) 332 (81) 277 (79)
Black 434 (22) 423 (22) 102 (15) 69 (13) 42 (10) 43 (12)
Hispanic 102 (5) 99 (5) 36 (5) 25 (5) 19 (5) 18 (5)
Asian 63 (3) 62 (3) 20 (3) 19 (3) 14 (2) 8 (2)
Other 24 (1) 20 (1) 4 (1) 4 (1) 2 (0) 3 (1)
Maternal Education (years)
<12 166 (8) 156 (8) 36 (5) 18 (3) 12 (3) 12 (3)
12 328 (16) 311 (16) 82 (12) 64 (12) 35 (9) 34 (10)
13-16 916 (46) 892 (46) 322 (47) 266 (48) 208 (51) 178 (51)
>16 587 (29) 574 (30) 248 (36) 202 (37) 154 (48) 125 (34)
Body Mass Index
<18.5 86 (5) 86 (5) 33 (5) 27 (5) 18 (4) 16 (5)
18.5-24.9 1005 (53) 988 (53) 398 (58) 329 (60) 256 (63) 204 (58)
25.0-29.9 376 (20) 366 (20) 133 (19) 101 (18) 73 (18) 72 (21)
≥30.0 431 (23) 419 (23) 122 (17) 92 (17) 61 (15) 57 (16)
Parity
Nulliparous 901 (45) 880 (46) 334 (49) 265 (48) 202 (49) 166 (47)
Multiparous 1098 (55) 1056 (55) 354 (51) 285 (52) 207 (51) 183 (52)
Child's Sex
Male 1004 (52) 1004 (52) 370 (54) 288 (52) 221 (54) 193 (55)
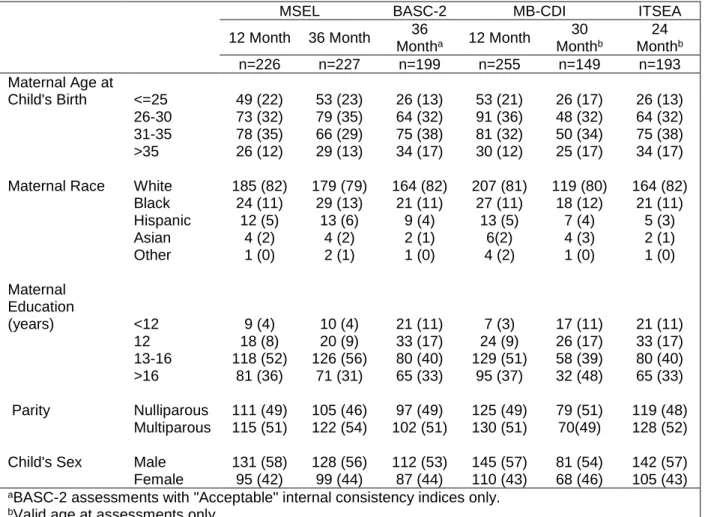
Table 3. Characteristics of participants for whom both OPE measurements and developmental assessments are available.
MSEL BASC-2 MB-CDI ITSEA
12 Month 36 Month
36
Montha 12 Month
30
Monthb
24
Monthb
n=226 n=227 n=199 n=255 n=149 n=193
Maternal Age at
Child's Birth <=25 49 (22) 53 (23) 26 (13) 53 (21) 26 (17) 26 (13)
26-30 73 (32) 79 (35) 64 (32) 91 (36) 48 (32) 64 (32)
31-35 78 (35) 66 (29) 75 (38) 81 (32) 50 (34) 75 (38)
>35 26 (12) 29 (13) 34 (17) 30 (12) 25 (17) 34 (17)
Maternal Race White 185 (82) 179 (79) 164 (82) 207 (81) 119 (80) 164 (82)
Black 24 (11) 29 (13) 21 (11) 27 (11) 18 (12) 21 (11)
Hispanic 12 (5) 13 (6) 9 (4) 13 (5) 7 (4) 5 (3)
Asian 4 (2) 4 (2) 2 (1) 6(2) 4 (3) 2 (1)
Other 1 (0) 2 (1) 1 (0) 4 (2) 1 (0) 1 (0)
Maternal Education
(years) <12 9 (4) 10 (4) 21 (11) 7 (3) 17 (11) 21 (11)
12 18 (8) 20 (9) 33 (17) 24 (9) 26 (17) 33 (17)
13-16 118 (52) 126 (56) 80 (40) 129 (51) 58 (39) 80 (40)
>16 81 (36) 71 (31) 65 (33) 95 (37) 32 (48) 65 (33)
Parity Nulliparous 111 (49) 105 (46) 97 (49) 125 (49) 79 (51) 119 (48)
Multiparous 115 (51) 122 (54) 102 (51) 130 (51) 70(49) 128 (52)
Child's Sex Male 131 (58) 128 (56) 112 (53) 145 (57) 81 (54) 142 (57)
Female 95 (42) 99 (44) 87 (44) 110 (43) 68 (46) 105 (43)
aBASC-2 assessments with "Acceptable" internal consistency indices only.
bValid age at assessments only.
Abbreviations: BASC, Behavioral Assessment System for Children; ITSEA, Infant-Toddler Social Emotional Assessment; MB-CDI, MacArthur-Bates Communicative Development Inventories; MSEL, Mullen Scales of Early Learning.
4.3 Assessment of Maternal Exposure to OPEs during Pregnancy
We used OPE metabolite concentrations measured in maternal urine during pregnancy to estimate fetal exposure to OPEs during gestation. Such measurements allow for estimation of maternal exposure, which functions as a measure for both potential indirect fetal exposure via maternal endocrine dysfunction (and possibly other pathways) and potential direct fetal
and metabolic mechanisms are also plausible [45, 184, 186-188]. For example, triphenyl phosphate is metabolized to diphenyl phosphate, tris(1,3-dicholoro-2-propyl) phosphate is metabolized to bis(1,3-dichloro-2-propyl) phosphate, and mono-substituted isopropyl-phenyl diphenyl phosphate is metabolized to isopropyl-phenyl phenyl phosphate (Figure 1). On the other hand, previous research suggests that BCIPP is not a major excreted metabolite of TCIPP [60], and recent research has demonstrated that BCIPHIPP is a significant metabolite of TCIPP [60, 184, 189]. This finding is reflected in our own study, where BCIPP was detected in only 49% of samples, whereas BCIPHIPP was detected in 98% of samples. Additionally, it is important to note that DPHP is a non-specific metabolite of TPHP, also being a metabolite of 2-ethylhexyldiphenyl phosphate [190], tert-butylphenyl diphenylphosphate [191], resorcinol bis(diphenylphosphate) [192], and potentially other compounds [60], and that DPHP may be used in industrial applications in its own right [193, 194]. Consequently, some studies that have examined relations between urinary DPHP concentrations and environmental TPHP
concentrations have reported only modest associations relative to other OPEs [24, 34],
suggesting that factors other than environmental TPHP may be responsible for excreted DPHP. Therefore, associations with DPHP must be interpreted with caution and may not be readily attributed to TPHP exposure.
example, Hoffman et al. [55] recruited 8 pregnant women and estimated variability over a single week (3 samples) and over pregnancy (18th week, 28th week, after birth); the investigators found that DPHP and BDCIPP concentrations were moderately to strongly consistent over one week (intraclass correlation coefficients (ICCs): 0.5 and 0.7, respectively), and over the course of pregnancy (ICCs: 0.5 and 0.6, respectively). Similarly, Romano et al. [126] measured urinary concentrations of DPHP and BDCIPP in 59 pregnant women at three points in pregnancy and observed ICCs of 0.51 and 0.61, respectively. In another study, Carignan et al. [127] measured OPE metabolite concentrations in 211 women undergoing in vitro fertilization and estimated ICCs for DPHP, BDCIPP, and ip-PPP; the investigators reported ICCs of 0.34, 0.36, and 0.37, respectively, between cycles (average: 178 days), and ICCS of 0.53, 0.48, and 0.44,
respectively, within cycles (average: 8 days). It is important to note that within these populations of pregnant women and women seeking to become pregnant, pregnancy-related changes in metabolism may increase variability in excreted OPE metabolite concentrations over time. Ultimately, despite the potential limitations of these metabolites as biomarkers of OPE exposure (e.g., potential non-specificity, relatively short half-lives), they provide useful estimates of OPE exposure and are the current gold-standard means to assess OPE exposure.
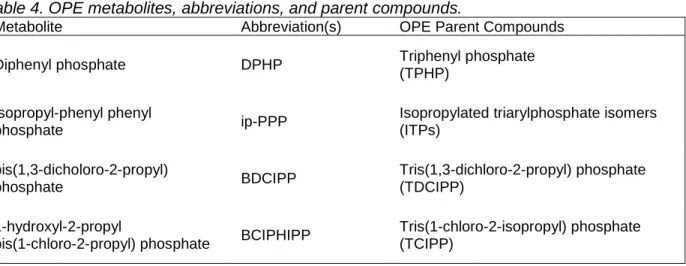
The metabolites of interest, their abbreviations, and their parent compounds are outlined in Table 4.
Table 4. OPE metabolites, abbreviations, and parent compounds.
Metabolite Abbreviation(s) OPE Parent Compounds
Diphenyl phosphate DPHP Triphenyl phosphate
(TPHP)
Isopropyl-phenyl phenyl
phosphate ip-PPP
Isopropylated triarylphosphate isomers (ITPs)
bis(1,3-dicholoro-2-propyl)
phosphate BDCIPP
Tris(1,3-dichloro-2-propyl) phosphate (TDCIPP)
1-hydroxyl-2-propyl
bis(1-chloro-2-propyl) phosphate BCIPHIPP
Tris(1-chloro-2-isopropyl) phosphate (TCIPP)
Concentrations of these OPE metabolites were measured in maternal urine obtained during pregnancy using methods designed and described by Van Den Eede et al. [198] and adapted for 5 ml of urine by Butt et al. [51]. The specific methods employed in this analysis are thoroughly detailed in Hoffman et al. [56]; below, we provide a direct citation detailing the
laboratory methods used to measure metabolites as previously described in Hoffman et al. [56]. During the late-second or early-third trimester, PIN women collected a spot urine
sample in a standard urine collection cup. The time and date of collection was recorded, and urine samples were aliquoted into polyethylene storage tubes and frozen at −80°C until analysis.
Urine samples were extracted using enzyme deconjugation and solid phase
extraction (SPE) techniques as previously described (Van den Eede et al., 2013) but adapted for 5ml of urine (Butt et al., 2016). In brief, samples were thawed, 5 ml of urine were aliquoted into a clean glass test tube, the internal standard mixture was spiked (10 ng of d10-BDCIPP, 8.8 ng of d10-DPHP; 25 ng of d12-TCEP) and samples vortexed. After pH adjustment with sodium acetate (1.75 ml of 1 M sodium acetate, pH 5), the enzyme solution was added (250 μl of 1000 units/ml μ-glucuronidase, 33 units/ml sulfatase in 0.2 M sodium acetate buffer), and the samples were vortexed and incubated overnight in a 37 °C water bath. Samples were extracted and cleaned using SPE with a StrataX-AW (60 mg, 3 ml) column, and were reconstituted in 500 μl of 1:1 water:methanol, as previously described (Butt et al., 2016). Internal standard recovery was quantified by spiking with 13C2-DPHP.
previously described (Butt et al., 2014 and Butt et al., 2016). Data were acquired under multiple reaction monitoring conditions using optimized parameters. Analyte responses were normalized to internal standard responses. BCIPP and BDCIPP were normalized using d10-BDCIPP, DPHP, ip-PPP and tb-PPP were normalized using d10-DPHP and BCIPHIPP was normalized using d12-TCEP. The mean recovery of the mass-labelled standards in the urine samples (n = 349) was 97% (standard error (SE) = 2.1%) for d10-DPHP, 98% (SE=3.0%) for d10-BDCIPP and 34% (SE=1.0%) for d12-TCEP. The low d12-TCEP recovery is partially due to
quantification inaccuracies resulting from matrix suppression since the d12-TCEP recovery was 55–73% in the blank samples (clean water only). Analyte values were blank corrected using the mean laboratory blank levels. Method detection limits (MDLs) were calculated as three times the standard deviation of the laboratory blanks, normalized to the average urine volume (3 ml). Sample were assessed in three batches and MDLs were calculated separately for each batch (MDLs: 136–333 pg/ ml for BCIPP, 127–243 pg/ml for DPHP, 60–197 pg/ml for BDCIPP, 37–177 pg/ml for ip-PPP, 213–846 pg/ml for tb-PPP and 3–33 pg/ml for BCIPHIPP. Specific gravity (SG) was measured in each urine sample prior to analysis using a digital handheld refractometer (Atago). Relative method accuracy was assessed by measuring PFR metabolites in SRM 3673 (n=3). Specific gravity-normalized