Racial Differences in Atrial Fibrillation-Related Cardiovascular
Disease and Mortality:
The Atherosclerosis Risk in Communities (ARIC) Study
Jared W. Magnani, MD, MSc, Faye L. Norby, MS, Sunil K. Agarwal, MD, PhD, Elsayed Z. Soliman, MD, MA, MS, Lin Y. Chen, MD, MS, Laura R. Loehr, PhD, and Alvaro Alonso, MD, PhD
Cardiology Section, Whitaker Cardiovascular Institute, Evans Department of Medicine, Boston University School of Medicine, Boston, Massachusetts (Magnani); currently with the Department of Medicine, Division of Cardiology, University of Pittsburgh Medical Center Heart and Vascular Institute, University of Pittsburgh, Pittsburgh, Pennsylvania (Magnani); Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis (Norby, Alonso); Department of Medicine, Johns Hopkins University, Baltimore, Maryland (Agarwal); Department of Epidemiology and Prevention, Epidemiological Cardiology Research Center, Wake Forest University School of Medicine, Winston- Salem, North Carolina (Soliman); Cardiovascular Division, Department of Medicine, University of Minnesota Medical School, Minneapolis (Chen); Department of Epidemiology, University of North Carolina, Chapel Hill (Loehr)
Abstract
IMPORTANCE—The adverse outcomes associated with atrial fibrillation (AF) have been studied in predominantly white cohorts. Racial differences in outcomes associated with AF merit
continued investigation.
OBJECTIVE—To evaluate the race-specific associations of AF with stroke, heart failure, coronary heart disease (CHD), and all-cause mortality in a community-based cohort.
Corresponding Author: Jared W. Magnani, MD, MSc, Division of Cardiology, Department of Medicine, UPMC Heart and Vascular Institute, University of Pittsburgh, Pittsburgh, PA 15213 ([email protected]).
Conflict of Interest Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of
Interest and none were reported.
Additional Contributions: We thank the staff and participants of the ARIC Study for their important contributions.
Author Contributions: Drs Magnani and Alonso had full access to all the data in the study and take responsibility for the integrity of
the data and the accuracy of the data analysis.
Study concept and design: Magnani, Norby, Soliman, Alonso. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Magnani.
Critical revision of the manuscript for important intellectual content: Norby, Agarwal, Soliman, Chen, Loehr, Alonso. Statistical analysis: Magnani, Norby.
Obtained funding: Magnani, Alonso.
Administrative, technical, or material support: Magnani, Agarwal, Alonso. Study supervision: Alonso.
HHS Public Access
Author manuscript
JAMA Cardiol
. Author manuscript; available in PMC 2017 March 13.Published in final edited form as:
JAMA Cardiol. 2016 July 01; 1(4): 433–441. doi:10.1001/jamacardio.2016.1025.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
DESIGN, SETTING, AND PARTICIPANTS—The Atherosclerosis Risk in Communities (ARIC) Study is a prospective, observational cohort. From 1987 through 1989, the ARIC Study enrolled 15 792 men and women and conducted 4 follow-up examinations (2011–2013) with active surveillance for vital status and hospitalizations. Race was determined by self-report and categorized as white, black, or other.
MAIN OUTCOMES AND MEASURES—Atrial fibrillation (adjudicated using
electrocardiograms, hospital discharge codes, and death certificates), stroke, heart failure, CHD, and mortality.
RESULTS—After exclusions, 15 080 participants (mean [SD] age, 54.2 [5.8] years; 8290 women [55.5%]; 3831 black individuals [25.4%]) were included in this analysis. During a mean (SD) follow-up of 20.6 (6.2) years, there were 2348 cases of incident AF. The incident rates of AF per 1000 person-years were 8.1 (95%CI, 7.7–8.5) in white individuals and 5.8 (95%CI, 5.2–6.3) in black individuals. The rates of stroke, heart failure, CHD, and mortality were higher in black individuals with AF than white individuals with AF. The association of AF with these outcomes, estimated with rate differences (rate of the end point in those with AF minus the rate in those without AF per 1000 person-years), also differed by race. The rate difference for stroke in individuals with AF was 10.2 (95%CI, 6.6–13.9) in white individuals and 21.4 (95%CI, 10.2– 32.6) in black individuals. For heart failure and CHD, the rate differences were 1.5- to 2.0-fold higher in black individuals than white individuals. White individuals with AF had a rate difference of 55.9 (95%CI, 48.1–63.7) for mortality compared with black individuals, who had a rate difference of 106.0 (95%CI, 86.0–125.9).
CONCLUSIONS AND RELEVANCE—In the prospective ARIC Study, the outcome of AF on the rates of stroke, heart failure, CHD, and mortality was considerably larger in black individuals than white individuals. These results indicate the vulnerability and increased risk in black individuals with AF. Continued investigation of racial differences in AF and its related adverse outcomes are essential to identify and mitigate racial disparities in the treatment of AF.
Atrial fibrillation (AF) is a common cardiac arrhythmia with significant adverse outcomes
and high social and medical costs.1 In the United States, AF affects approximately 1% of the
adult population and more than 5% of those 65 years and older.2,3 Atrial fibrillation has been
associated with increased risks of stroke by 5.0-fold, heart failure by 3.0-fold, and mortality
by 2.0-fold.4–7 The study of AF and its associated clinical adverse outcomes has been
conducted predominantly in cohorts with participants of mostly white race.
Several factors contribute to the more limited study of AF in racially or ethnically diverse cohorts compared with white cohorts. Multiple health care registries, databases, and
community-based studies8–14 have identified differences in the prevalence of AF by race,
such that reports8–14 have consistently identified AF as being less prevalent in racial and
ethnic minorities. In addition, it is well established that ethnic and racial minorities have less participation and recruitment in cardiovascular studies and trials compared with white
individuals.15 The deficit of minority participation in clinical studies extends to AF because
many landmark trials in AF have not reported or had limited enrollment of ethnic or racial
minorities.16 However, alongside the established racial differences in AF prevalence are
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
critical differences in the treatments to prevent outcomes associated with AF, particularly
stroke.11,17–19
Estimating the relations of AF to adverse outcomes in nonwhite cohorts has evident public health relevance. Observational cohorts may identify racial differences. Understanding such differences may guide interventions to address and mitigate disparities. To improve our understanding of the morbidity associated with AF in black individuals, we examined data
from the Atherosclerosis Risk in Communities (ARIC) Study,20 a large, mostly biracial,
community-based cohort. Specifically, we evaluated and compared the race-specific associations of AF with stroke, heart failure, coronary heart disease (CHD), and mortality between white and black individuals in this cohort.
Methods
Study Sample
The ARIC Study is a community-based cohort designed to investigate determinants of atherosclerosis and cardiovascular disease in the general population. Detailed methods have
been published elsewhere.20 Briefly, from 1987 through 1989, a total of 15 792 men and
women aged 45 to 64 years were recruited from 4 communities in the United States: Forsyth County, North Carolina; Jackson, Mississippi; northwest suburbs of Minneapolis,
Minnesota; and Washington County, Maryland. Participants were followed up prospectively through examination 4 (2011–2013). Participants in the Minneapolis and Washington County sites were mostly white individuals, whereas only black individuals were recruited in Jackson. In addition to the baseline examination, the ARIC Study has conducted 4 follow-up examinations (1990–1992, 1993–1995, 1996–1998, and 2011–2013) along with annual telephone calls to determine vital status and obtain information on hospitalizations during the previous year. Ongoing surveillance of local hospitals has simultaneously been used to identify hospitalizations of ARIC Study participants, and trained abstractors have collected information on discharge diagnoses.
Key Points
Question
What are the racial differences in the associations of atrial fibrillation (AF) and its adverse outcomes (stroke, heart failure, coronary heart disease, and mortality)?
Findings
In 15 080 participants in the Atherosclerosis Risk in Communities Study, the differences in adverse outcomes were greater for black individuals with AF than for white
individuals. Black individuals consistently had a 1.5- to 2-fold higher rate differences for the adverse outcomes than white individuals.
Meaning
The rate difference for adverse outcomes indicates the distinct vulnerability and increased risk of adverse outcomes in black individuals with AF.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
In the present analysis, we excluded the ARIC Study participants with prevalent AF at baseline (n = 37), those missing baseline electrocardiograms (ECGs) (n = 242), those lacking data on essential covariates (n = 330), and those of race other than white or black (n = 103). After exclusions, 15 080 participants were included in the present analysis. The ARIC Study has been approved by institutional review boards at participating institutions, and all participants provided written informed consent.
AF Ascertainment
Ascertainment of AF in the ARIC Study has been previously described12,21 and conducted
using 3 methods: study ECGs, hospital discharge codes, and death certificates. Standard, 10-second, 12-lead ECGs were obtained at baseline and at each of the subsequent follow-up examinations. Tracings were performed in the supine position using MAC PC Personal Cardiographs (Marquette Electronics Inc) and transmitted electronically to the ARIC ECG Reading Center (Epidemiological Cardiology Research Center, Wake Forest School of Medicine, Winston Salem, North Carolina), where they underwent automated reading and coding. Tracings with AF were reviewed by a cardiologist. Incident AF was identified from hospitalizations or death certificates using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 427.31 or 427.32. Incident AF in the setting of cardiothoracic surgery was not defined as AF in the ARIC Study. Use of discharge coding for AF identification has been reported as having a median positive predictive value
of 89% across multiple studies.22
Ascertainment of Cardiovascular Outcomes and Mortality
The outcomes of stroke, heart failure, and CHD were determined by physicians using validated adjudication protocols. Stroke was defined as sudden neurologic insult of 24-hour duration or longer or a neurologic insult associated with death without evidence of a
nonstroke cause of death.23 Stroke events were ascertained from surveillance of ARIC Study
participant hospitalization using ICD-9-CM codes 430 through 438 through 1997 and codes 430 through 436 thereafter. Strokes were classified by physician review and computer algorithm with standardized criteria and determined as hemorrhagic or ischemic. Heart failure was ascertained by review of hospitalization records and death certificates for a heart failure diagnosis. Specifically, incident cases with an ICD-9-CM code of 428 (428.0–428.9) or International Statistical Classification of Diseases, 10th Revision code I50 were classified
as heart failure.24 Coronary heart disease was determined using study surveillance and
adjudicated as previously described.25 Symptoms, biomarkers, and ECGs were incorporated
into a computerized algorithm.26 Disagreement between discharge coding and computer
algorithm was adjudicated by the ARIC Mortality and Morbidity Classification Committee. For the present analysis, CHD was defined as definite or probable myocardial infarction or definite fatal CHD. All-cause mortality was determined as identification of death by telephone contact with participant proxy, obituaries, hospital records, death certificates, or vital statistics from the National Death Index.
Covariates
Age, race (categorized as white, black, or other), smoking status, and highest level of education were provided by self-report. Body mass index was calculated as weight in
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
kilograms divided by height in meters squared. Hypertension was defined as a systolic blood pressure of 140mmHg or higher, a diastolic blood pressure higher than90mmHg, or use of medications to treat hypertension. Blood samples were obtained after individuals had fasted for 8 hours. Diabetes was determined by self-report of a physician diagnosis of diabetes, nonfasting blood glucose level of 200 mg/dL or higher, fasting blood glucose level of 126mg/dL or higher (to convert glucose to millimoles per liter, multiply by 0.0555), or use of insulin or other oral hypoglycemic medications. Measurement of serum creatinine in the
ARIC Study has been described previously.27 Estimated glomerular filtration rate at visits 1,
2, and 4 was calculated from serum creatinine as described by the Chronic Kidney Disease
Epidemiology Collaboration,28 and a value less than 60 mL/min/1.73m2 was used to define
baseline chronic kidney disease. Prevalent chronic obstructive pulmonary disease, stroke, and CHD at baseline were ascertained by self-report history of a diagnosis by a physician. Prevalent heart failure was identified as previously described using the Gothenburg criteria
and review of medications.24 Incident chronic kidney disease and chronic obstructive
pulmonary disease were defined using standardized methods articulated by the Centers for
Medicare & Medicaid Chronic Condition Data Warehouse.29
Statistical Analysis
We determined the distributions of continuous and categorical variables. The primary analysis was the relation of incident AF to the outcomes of stroke, heart failure, CHD, and all-cause mortality. We examined AF as a time-dependent exposure because we considered that increased duration of AF would contribute toward the risk of the outcome. To limit confounding by the covariates changing over time, we updated covariates across examinations. Covariates that could not be updated were used from the most immediate examination before the diagnosis of AF. We determined the age- and sex-standardized incidence of AF per 1000 person-years by race and examined the rates of the outcomes according to AF status and stratified by race. We calculated the rate ratio and rate difference of each outcome comparing participants with and without AF. We then examined the risk of the outcomes of stroke, heart failure, CHD, and mortality associated with incidence of AF in multivariable Cox proportional hazards models separately by race. For the analysis that examined stroke as an outcome, we additionally excluded participants with prevalent stroke (n = 269), yielding a sample size of 14 811. For heart failure, we excluded participants with prevalent heart failure (n = 686), yielding a sample size of 14 394. For CHD, we excluded participants with prevalent CHD (n = 722), yielding a sample size of 14 358. We examined the cumulative incidence of AF prospectively and constructed Kaplan-Meier curves for each outcome event stratifying by race. Study participants contributed observation time in the cohort without AF until the time of incident AF, when they began contributing toward the cohort with AF. All analyses were adjusted initially for age and sex (model 1); then for age, sex, educational level, body mass index, smoking status, hypertension, diabetes, chronic kidney disease, estimated glomerular filtration rate, chronic obstructive pulmonary disease, and cardiovascular disease, including prevalent CHD, stroke, and heart failure (model 2); and then adjusted for all covariates as time-dependent (model 3).
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
Results
After exclusions, at the baseline ARIC Study examination there were 15 080 participants (Table 1) with a mean (SD) age of 54.2 (5.8) years. Participants included 8290 women (55.5%) and 3831 black individuals (25.4%). Noteworthy racial differences in covariates at the baseline examination included body mass index (mean [SD], 27.0 [4.9] in white individuals and 29.6 [6.2] in black individuals) and the higher prevalence of hypertension and diabetes in black individuals.
Follow-up extended from the baseline examination (1987–1989) through the end of 2012. During a mean (SD) follow-up of 20.6 (6.2) years, there were 2348 cases of incident AF, 1914 in white individuals with an incidence rate of 8.1 (95% CI, 7.7–8.5) per 1000 person-years and 434 in black individuals with an incidence rate of 5.8 (95% CI, 5.2–6.3) per 1000 person-years.
The age- and sex-standardized event rates per 1000 person-years stratified by race and AF status are listed in Table 2. Event rates were greater in black individuals for all outcomes in ARIC Study participants with and without AF. Overall, the association of AF with
outcomes, as measured by the rate ratio, was similar in both racial groups. In both black and white individuals, stroke rates with AF were increased 5.0-fold compared with those without AF. The rate ratio for heart failure in individuals with AF was 13.7 (95% CI, 10.5–17.9) in white individuals and 9.7 (95% CI, 5.9–16.1) in black individuals compared with individuals without AF. White individuals with AF and black individuals with AF had a 6.0- to 7.0-fold increased rate of CHD than either race without AF and a 6.0-fold increased rate of all-cause mortality. The rate ratio for the association of AF with mortality was likewise 6.0-fold greater in white and black individuals with AF.
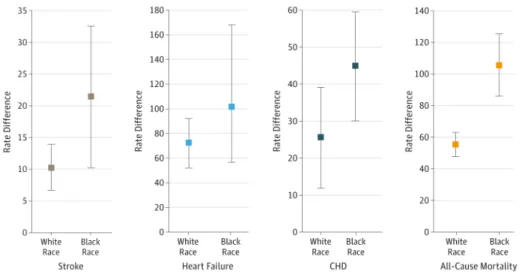
Marked racial differences were identified in examining the absolute (rather than relative) risk of outcomes associated with AF, as estimated using risk differences. The age- and sex-adjusted rate differences for stroke, heart failure, and CHD comparing black individuals with AF with those without AF were considerably greater than the estimates for white
individuals. The rate difference for stroke in black individuals with AF compared with black individuals without AF was twice that of white individuals with AF. Heart failure and CHD rate differences were 1.5- to 2.0-fold higher in black individuals than the estimates for white individuals. The rate difference in black individuals with AF (rate difference, 106.0; 95% CI, 86.0–125.9) was roughly twice that of white individuals (rate difference, 55.9; 95% CI, 48.1–63.7). Figure 1 presents the rate differences by race for the 4 outcomes.
The multivariable hazard ratios for association of AF with the outcomes by race are summarized in Table 3. Atrial fibrillation was associated with more than 3 times the risk of CHD in black individuals with AF compared with black individuals without AF. Atrial fibrillation in black individuals was associated with amore than 4.0-foldincreased risk of mortality compared with black individuals without AF. In contrast, AF in white individuals was associated with a 3.6-fold increased risk of all-cause mortality.
Figure 2 shows the Kaplan-Meier curve by AF status separately in white and black individuals. In all outcomes, black individuals without AF have lower event-free survival
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
rates compared with white individuals without AF. With AF, black individuals similarly have lower event-free survival rates than white individuals. The curves for stroke in those with AF (Figure 2A) diverge early and rapidly. In Figure 2B, black individuals with AF rapidly accumulate heart failure events, stabilizing after approximately 15years. There is a similarly steeper descent in black individuals with AF and CHD(Figure 2C) compared with white individuals. Black individuals with AF had a rapid accumulation of mortality events (Figure 2D). The log-rank tests for comparing events by race were all statistically significant (P < . 001 for all outcomes).
Discussion
We examined the associations of AF with adverse outcomes in the ARIC Study extending from the baseline examination to more than 20 years of follow-up. Consistent with a prior
report12 from the ARIC Study, we observed a higher incidence of AF in white individuals
compared with black individuals. Both white and black individuals with AF had markedly increased risks of the outcomes of stroke, heart failure, CHD, and all-cause mortality. We appreciated that the estimates of the associations with the outcomes had consistent overlap in black and white individuals. Importantly, the rate differences (the difference in incidence rates in those with and without AF) of the outcomes differed by race. We observed that black individuals with AF had an approximately 1.5- to 2.0-fold greater rate difference for each outcome than white individuals with AF. Our results indicate that black ARIC Study participants with AF are at considerably greater risk for associated adverse outcomes than white individuals with AF.
The distinction between the concepts of racial differences and disparities has been well
articulated.30 Racial differences are independent of social factors, whereas racial disparities
result from biases or practices with a systemic origin. Whether our findings may be described as racial differences or racial disparities merits attention. We have identified clear racial differences in adverse outcomes associated with AF but are not able to assert whether such findings are the result of racial disparities. The ARIC Study is a prospective,
observational cohort; hence, we are not able to dissect or identify the causes of our findings. We consider that our results contribute toward an increasing number of observations describing significant racial differences in AF outcomes and complement the extant
literature that suggests disparities in AF treatment.8,18,19,31
The racial differences in the outcomes examined in this study have been demonstrated
outside the study of AF. In the ARIC Study and other cohorts,32,33 blacks have been
previously found to have a greater incidence of the study outcomes. There has been limited study of racial differences in AF. Ina large, hospital-based registry (Get with the Guidelines– Heart Failure) of black and white patients with heart failure, racial differences in in-hospital
mortality were not observed.8 A large study11 of Medicare beneficiaries identified that black
individuals with AF have a 2.0-foldgreater incidence of strokes than white individuals and
along with community-based and registry studies8,11,18 identified that black individuals have
concomitant decreased treatment with anticoagulation. Other literature corroborates the
decreased use of anticoagulation in black individuals for stroke prevention in general.31,34
Our investigation indicates that racial differences in the outcome of AF on adverse outcomes
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
extend beyond stroke to other conditions associated previously with AF, specifically, heart failure, CHD, and all-cause mortality. These findings are derived from an established community-based cohort with carefully adjudicated cardiovascular end points and long follow-up.
Our findings have important public health implications. First and most immediate is the need to bolster prevention of adverse outcomes in black individuals with AF. Our results indicate the increased vulnerability of black individuals to the outcomes of stroke, CHD, heart failure, and mortality relative to white individuals. Racial disparities in outcomes associated with AF are not cited in professional statements and guidelines for treating AF and
preventing its complications.35,36 The inclusion of racial disparities in AF as part of such
documents may contribute toward improved treatment of AF in black individuals and other racial and ethnic minorities. It is further imperative that registries, such as the Get with the
Guidelines–AFIB,37 increase our understanding of racial differences in outcomes associated
with AF and optimize identifying the systemic causes for racial disparities.
Second, our results underscore the necessity of improving AF prevention in black
individuals because the social and medical costs of the associated morbidity are high. Much has been made of the decreased incidence of AF in black individuals despite the increased prevalence of risk factors. The observation has been cited by the most recent professional
society guidelines on AF evaluation and management.36 A priority is now to address the
high public health costs of AF in black individuals. Efforts need to focus on detecting and addressing AF in black individuals to prevent its associated complications.
Third, black individuals and other racial and ethnic minorities have had markedly limited participation in clinical trials in AF. The AF Follow-up Investigation of Rhythm
Management (n = 4060) included only 263 black individuals (<7% of the study cohort).38
Black individuals comprise 1% to 4% of participants in AF registries.39,40 Pivotal
studies41–43 of AF rate and rhythm control have unknown generalizability to black
individuals. The sentinel clinical trials of novel oral anticoagulants included uniformly limited numbers of participants with nonwhite race or ethnicity. For example, less than 2%
of trial participants assessing the safety of rivaroxaban were of black race,44 and subgroup
analyses by race have not been uniformly reported in the novel oral anticoagulant trials.45
Increased enrollment of racial and ethnic minorities would strengthen statistical power and enhance generalizability of trial findings to vulnerable populations. Furthermore, improving minority recruitment and enrollment to such studies is central to understanding mechanisms for disparities in AF.
Fourth, it is recognized that AF identification in black individuals has been challenging and
may rely on the method of detection and ascertainment.46 Broader initiatives with
contemporary monitoring will improve AF identification and may challenge the notion of racial differences in AF prevalence. Increased surveillance of AF in black individuals may also enhance recruitment to clinical trials and registries.
Our analysis has several strengths, including the long-term, prospective follow-up conducted in the ARIC Study, along with consistent ascertainment and adjudication of AF and the
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
studied outcomes. The analysis is further strengthened by inclusion of more than 14 000 participants and the generalizability enhanced by the geographic diversity of ARIC Study participant sites.
There are important limitations to the analysis that also merit attention. First, AF misclassification was possible. Reliance on ICD coding may have resulted in incomplete identification of participants with AF. We would expect that misclassification of AF status by ICD codes would be nondifferential with respect to the outcomes examined in this study, biasing our results toward the null. Second, subclinical AF, not recognized as a clinical diagnosis and hence not recorded using ICD coding, may also have been present in ARIC Study participants. It is possible that such individuals would be healthier and less likely to experience hospitalization. Third, although the ARIC Study participants come from 4 distinct sites, the black participants included in this study are primarily recruited from Mississippi. The generalizability of our findings to black individuals living in other
geographic regions in the United States is limited. Fourth, we did not adjust for treatments of AF, such as anticoagulation, cardioversion, or medications, which may confound the relation of AF and the examined outcomes. Likewise, we are not able to exclude residual
confounding, particularly from exposures associated with adverse outcomes in AF (eg, left atrial volume and sleep-disordered breathing). Fifth, the ARIC Study is a predominantly biracial, community-based cohort, and as such generalizability to other races or ethnicities is also limited.
Conclusions
We observed markedly increased rates of stroke, heart failure, CHD, and mortality in black individuals with AF compared with white individuals in the prospective, community based ARIC Study. Our results contribute toward under standing the significant racial differences in black and white individuals with AF. Further study must now address the mechanisms for such differences to improve treatment of AF and prevent complications. Likewise, continued investigation of the causes and origins for such racial differences may identify racial
disparities and suggest approaches to address and mitigate them.
Acknowledgments
Funding/Support: The ARIC Study is performed as a collaborative study supported by contracts
HHSN268201100005C, HHSN268201100006C, HHSN 268201100007C, HHSN268201100008C,
HHSN268201100009C, HHSN268201100010C, HHSN268201100011C, and HHSN 268201100012C from the National Heart, Lung, and Blood Institute. This study was additionally funded by grant 16EIA26410001 from the American Heart Association and grant R01-HL122200 from the National Heart, Lung, and Blood Institute. This work was supported by grant 2015084 from the Doris Duke Charitable Foundation (Dr Magnani).
References
1. Magnani JW, Rienstra M, Lin H, et al. Atrial fibrillation: current knowledge and future directions in epidemiology and genomics. Circulation. 2011; 124(18):1982–1993. [PubMed: 22042927] 2. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national
implications for rhythm management and stroke prevention: the An Ticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001; 285(18):2370–2375. [PubMed: 11343485]
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
3. Piccini JP, Hammill BG, Sinner MF, et al. Incidence and prevalence of atrial fibrillation and associated mortality among Medicare beneficiaries, 1993–2007. Circ Cardiovasc Qual Outcomes. 2012; 5(1):85–93. [PubMed: 22235070]
4. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991; 22(8):983–988. [PubMed: 1866765]
5. Wang TJ, Larson MG, Levy D, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003; 107(23):2920–2925. [PubMed: 12771006]
6. Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998; 98(10):946–952. [PubMed: 9737513]
7. Conen D, Chae CU, Glynn RJ, et al. Risk of death and cardiovascular events in initially healthy women with new-onset atrial fibrillation. JAMA. 2011; 305(20):2080–2087. [PubMed: 21610240] 8. Thomas KL, Piccini JP, Liang L, et al. Get With the Guidelines Steering Committee and Hospitals. Racial differences in the prevalence and outcomes of atrial fibrillation among patients hospitalized with heart failure. J Am Heart Assoc. 2013; 2(5):e000200. [PubMed: 24072530]
9. Dewland TA, Olgin JE, Vittinghoff E, Marcus GM. Incident atrial fibrillation among Asians, Hispanics, blacks, and whites. Circulation. 2013; 128(23):2470–2477. [PubMed: 24103419] 10. Shen AY, Contreras R, Sobnosky S, et al. Racial/ethnic differences in the prevalence of atrial
fibrillation among older adults: a cross-sectional study. J Natl Med Assoc. 2010; 102(10):906–913. [PubMed: 21053705]
11. Birman-Deych E, Radford MJ, Nilasena DS, Gage BF. Use and effectiveness of warfarin in Medicare beneficiaries with atrial fibrillation. Stroke. 2006; 37(4):1070–1074. [PubMed: 16528001]
12. Alonso A, Agarwal SK, Soliman EZ, et al. Incidence of atrial fibrillation in whites and African-Americans: the Atherosclerosis Risk in Communities (ARIC) study. Am Heart J. 2009; 158(1): 111–117. [PubMed: 19540400]
13. Lipworth L, Okafor H, Mumma MT, et al. Race-specific impact of atrial fibrillation risk factors in blacks and whites in the southern community cohort study. Am J Cardiol. 2012; 110(11):1637– 1642. [PubMed: 22922000]
14. Rodriguez CJ, Soliman EZ, Alonso A, et al. Atrial fibrillation incidence and risk factors in relation to race-ethnicity and the population attributable fraction of atrial fibrillation risk factors: the Multi-Ethnic Study of Atherosclerosis. Ann Epidemiol. 2015; 25(2):71–76. 76.e1. [PubMed: 25523897] 15. Yancy CW, Benjamin EJ, Fabunmi RP, Bonow RO. Discovering the full spectrum of cardiovascular
disease: Minority Health Summit 2003: executive summary. Circulation. 2005; 111(10):1339– 1349. [PubMed: 15769779]
16. Amponsah MK, Benjamin EJ, Magnani JW. Atrial fibrillation and race: a contemporary review. Curr Cardiovasc Risk Rep. 2013; 7(5)
17. Shen AY, Yao JF, Brar SS, Jorgensen MB, Wang X, Chen W. Racial/Ethnic differences in ischemic stroke rates and the efficacy of warfarin among patients with atrial fibrillation. Stroke. 2008; 39(10):2736–2743. [PubMed: 18635860]
18. Meschia JF, Merrill P, Soliman EZ, et al. Racial disparities in awareness and treatment of atrial fibrillation: the REasons for Geographic and Racial Differences in Stroke (REGARDS) study. Stroke. 2010; 41(4):581–587. [PubMed: 20190000]
19. Bhave PD, Lu X, Girotra S, Kamel H, Vaughan Sarrazin MS. Race- and sex-related differences in care for patients newly diagnosed with atrial fibrillation. Heart Rhythm. 2015; 12(7):1406–1412. [PubMed: 25814418]
20. The ARIC Investigators. The Atherosclerosis Risk in Communities (ARIC) Study: design and objectives. Am J Epidemiol. 1989; 129(4):687–702. [PubMed: 2646917]
21. Chamberlain AM, Agarwal SK, Ambrose M, Folsom AR, Soliman EZ, Alonso A. Metabolic syndrome and incidence of atrial fibrillation among blacks and whites in the Atherosclerosis Risk in Communities (ARIC) Study. Am Heart J. 2010; 159(5):850–856. [PubMed: 20435195]
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
22. Jensen PN, Johnson K, Floyd J, Heckbert SR, Carnahan R, Dublin S. A systematic review of validated methods for identifying atrial fibrillation using administrative data. Pharmacoepidemiol Drug Saf. 2012; 21(suppl 1):141–147. [PubMed: 22262600]
23. Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke. 1999; 30(4):736–743. [PubMed: 10187871]
24. Loehr LR, Rosamond WD, Chang PP, Folsom AR, Chambless LE. Heart failure incidence and survival (from the Atherosclerosis Risk in Communities study). Am J Cardiol. 2008; 101(7):1016– 1022. [PubMed: 18359324]
25. Soliman EZ, Lopez F, O’Neal WT, et al. Atrial fibrillation and risk of ST-segment-elevation versus non-ST-segment-elevation myocardial infarction: the Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2015; 131(21):1843–1850. [PubMed: 25918127]
26. White AD, Folsom AR, Chambless LE, et al. Community surveillance of coronary heart disease in the Atherosclerosis Risk in Communities (ARIC) Study: methods and initial two years’
experience. J Clin Epidemiol. 1996; 49(2):223–233. [PubMed: 8606324]
27. Manjunath G, Tighiouart H, Ibrahim H, et al. Level of kidney function as a risk factor for
atherosclerotic cardiovascular outcomes in the community. J Am Coll Cardiol. 2003; 41(1):47–55. [PubMed: 12570944]
28. Levey AS, Stevens LA, Schmid CH, et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009; 150(9):604–612. [PubMed: 19414839]
29. Chronic Disease Warehouse. [Accessed February 18, 2016] Chronic Conditions. https:// www.ccwdata.org/web/guest/condition-categories
30. Taylor AL. Racial differences and racial disparities: the distinction matters. Circulation. 2015; 131(10):848–850. [PubMed: 25673668]
31. Schwamm LH, Reeves MJ, Pan W, et al. Race/ethnicity, quality of care, and outcomes in ischemic stroke. Circulation. 2010; 121(13):1492–1501. [PubMed: 20308617]
32. Feinstein M, Ning H, Kang J, Bertoni A, Carnethon M, Lloyd-Jones DM. Racial differences in risks for first cardiovascular events and noncardiovascular death: the Atherosclerosis Risk in Communities study, the Cardiovascular Health Study, and the Multi-Ethnic Study of Atherosclerosis. Circulation. 2012; 126(1):50–59. [PubMed: 22693351]
33. Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics 2015 update: a report from the American Heart Association. Circulation. 2015; 131(4):e29–e322. [PubMed: 25520374] 34. Ibrahim SA, Kwoh CK, Harper DL, Baker DW. Racial differences in the utilization of oral
anticoagulant therapy in heart failure: a study of elderly hospitalized patients. J Gen Intern Med. 2000; 15(2):134–137. [PubMed: 10672118]
35. Van Wagoner DR, Piccini JP, Albert CM, et al. Progress toward the prevention and treatment of atrial fibrillation: a summary of the Heart Rhythm Society Research Forum on the Treatment and Prevention of Atrial Fibrillation, Washington, DC, December 9–10, 2013. Heart Rhythm. 2015; 12(1):e5–e29. [PubMed: 25460864]
36. January CT, Wann LS, Alpert JS, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014; 64(21):e1–e76. [PubMed: 24685669]
37. Lewis WR, Piccini JP, Turakhia MP, et al. Get With The Guidelines AFIB: novel quality improvement registry for hospitalized patients with atrial fibrillation. Circ Cardiovasc Qual Outcomes. 2014; 7(5):770–777. [PubMed: 25185244]
38. Bush D, Martin LW, Leman R, Chandler M, Haywood LJ. NHLBI AFFIRM Investigators. Atrial fibrillation among African Americans, Hispanics and Caucasians: clinical features and outcomes from the AFFIRM trial. J Natl Med Assoc. 2006; 98(3):330–339. [PubMed: 16573295] 39. Reiffel JA, Kowey PR, Myerburg R, et al. AFFECTS Scientific Advisory Committee and
Investigators. Practice patterns among United States cardiologists for managing adults with atrial
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
fibrillation (from the AFFECTS Registry). Am J Cardiol. 2010; 105(8):1122–1129. [PubMed: 20381664]
40. Le Heuzey JY, Breithardt G, Camm J, et al. The Record AF study: design, baseline data, and profile of patients according to chosen treatment strategy for atrial fibrillation. Am J Cardiol. 2010; 105(5):687–693. [PubMed: 20185018]
41. Rienstra M, Hagens VE, Van Veldhuisen DJ, et al. RAte Control versus Electrical Cardioversion for Persistent Atrial Fibrillation Study Group. Clinical characteristics of persistent lone atrial fibrillation in the RACE study. Am J Cardiol. 2004; 94(12):1486–1490. [PubMed: 15589001] 42. Groenveld HF, Crijns HJ, Van den Berg MP, et al. RACE II Investigators. The effect of rate control
on quality of life in patients with permanent atrial fibrillation: data from the RACE II (Rate Control Efficacy in Permanent Atrial Fibrillation II) study. J Am Coll Cardiol. 2011; 58(17):1795– 1803. [PubMed: 21996393]
43. Van Gelder IC, Groenveld HF, Crijns HJ, et al. RACE II Investigators. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010; 362(15):1363–1373. [PubMed: 20231232]
44. Patel MR, Mahaffey KW, Garg J, et al. ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011; 365(10):883–891. [PubMed: 21830957] 45. Akinboboye O. Use of oral anticoagulants in African-American and Caucasian patients with atrial
fibrillation: is there a treatment disparity? J Multidiscip Healthc. 2015; 8:217–228. [PubMed: 26056467]
46. Prineas RJ, Soliman EZ, Howard G, et al. The sensitivity of the method used to detect atrial fibrillation in population studies affects group-specific prevalence estimates: ethnic and regional distribution of atrial fibrillation in the REGARDS study. J Epidemiol. 2009; 19(4):177–181. [PubMed: 19561382]
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
Figure 1. Rate Differences for the Outcomes of Stroke, Heart Failure, Coronary Heart Disease (CHD), and Mortality Stratified by White and Black Race in the Atherosclerosis Risk in Communities Study
The rate difference for black individuals with atrial fibrillation exceeds that of white individuals across the 4 outcomes. Error bars indicate 95%CIs.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
Figure 2. Kaplan-Meier Curves of the Outcomes Stratified by Race (White or Black) and Atrial Fibrillation (AF) Status
The Atherosclerosis Risk in Communities Study participants contribute to the strata without the outcome until the incident event. Outcomes are not exclusive, and the Kaplan-Meier curve for each outcome is for the incident event. Log-rank test P < .001 for all. CHD indicates coronary heart disease.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Table 1
Baseline Characteristics of the Study Participants at Examination 1, Atherosclerosis Risk in Communities
(ARIC) Study, 1987–1989a
Characteristic Total Cohort (N = 15 080) White Individuals (n = 11 249) Black Individuals (n = 3831)
Age, y 54.2 (5.8) 54.4 (5.7) 53.6 (5.8) Women 8290 (55.0) 5932 (53) 2358 (62) Educational level less than high school 3510 (23) 1931 (17) 1579 (41) BMI 27.7 (5.3) 27.0 (4.9) 29.6 (6.2) Current smoker 3937 (26) 2786 (25) 1151 (30) Hypertension 5163 (34) 3044 (27) 2119 (55) Diabetes 1758 (12) 1021 (9) 737 (19) Prevalent
CHD 722 (5) 572 (5) 150 (4) Heart failure 686 (5) 423 (4) 263 (7) Stroke 269 (2) 189 (2) 80 (2) COPD 274 (2) 241 (2) 33 (1) eGFR, mL/min/1.73 m2 102.3 (15.8) 99.4 (12.6) 111.0 (20.4)
eGFR, <60 mL/min/1.73 m2 195 (1.3) 111 (0.99) 84 (2.2)
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate.
a
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
T ab le 2Age- and Se
x-Standardized Rates (per 1000 Person-years), Rate Ratios, and Rate Dif
ferences of Cardio
v
ascular Disease and All-Cause Mortality
Adv
erse Effect
Rate (95% CI) f
or White Indi
viduals
Rate (95% CI) f
or Black Indi
viduals
Standardized Rate for Those W
ith No
AF
Standardized Rate for Those W
ith AF
Rate Ratio
Rate Differ
ence
Standardized Rate for Those W
ith No
AF
Standardized Rate f
or Those W ith AF Rate Ratio Rate Differ ence Strok e 2.6 (2.4–2.8) 12.8 (9.1–16.4) 4.9 (3.7–6.6) 10.2 (6.6–13.9) 5.8 (5.2–6.4) 27.2 (15.6–38.4) 4.7 (3.1–7.1) 21.4 (10.2–32.6) Heart f ailure 5.6 (5.3–5.9) 77.4 (57.4–97.2) 13.7 (10.5–17.9) 71.8 (51.6–91.9) 11.6 (10.7–12.0) 112.8 (56.4–168.0) 9.7 (5.9–16.1) 101.4 (56.4–168.0) CHD 4.9 (4.6–5.2) 30.5 (16.8–44.2) 6.2 (3.9–9.8) 25.6 (11.9–39.2) 6.8 (6.2–7.5) 51.6 (37.0–66.3) 7.6 (5.6–10.2) 44.9 (30.1–59.5) All-cause mortality 12.0 (11.6–12.5) 68.0 (60.2–75.6) 5.6 (5.0–6.4) 55.9 (48.1–63.7) 20.4 (19.2–21.6) 126.7 (106.7–146.6) 6.1 (5.3–7.0) 106.0 (86.0–125.9) Abbre viations: AF
, atrial f
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Table 3
Summary of Events, Person-time, and Hazard Ratios for Cardiovascular Disease and Mortality, Atherosclerosis Risk in Communities (ARIC) Study, 1987–2009
Variable
White Individuals Black Individuals
No AF AF No AF AF
Total Stroke
No. of events 462 244 335 92 Person-time, y 219 805 8760 70 455 1060 Model 1a 1 [Reference] 2.20 (1.76–2.75) 1 [Reference] 3.03 (2.08–4.42) Model 2b 1 [Reference] 1.91 (1.52–2.39) 1 [Reference] 2.14 (1.46–3.13) Model 3c 1 [Reference] 1.81 (1.44–2.27) 1 [Reference] 2.05 (1.40–3.01)
Ischemic Stroke
No. of events 393 230 289 88 Person-time, y 220 108 8850 70 684 1075 Model 1a 1 [Reference] 2.49 (1.98–3.13) 1 [Reference] 3.19 (2.17–4.68) Model 2b 1 [Reference] 2.11 (1.68–2.66) 1 [Reference] 2.22 (1.51–3.27) Model 3c 1 [Reference] 1.99 (1.56–2.53) 1 [Reference] 2.15 (1.45–3.23)
Heart Failure
No. of events 870 879 584 239 Person-time, y 215 527 5327 67 295 446 Model 1a 1 [Reference] 4.30 (3.80–4.88) 1 [Reference] 3.57 (2.75–4.63) Model 2b 1 [Reference] 3.62 (3.19–4.10) 1 [Reference] 2.88 (2.22–3.74) Model 3c 1 [Reference] 2.96 (2.59–3.38) 1 [Reference] 2.52 (1.93–3.28)
Coronary Heart Disease
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Variable
White Individuals Black Individuals
No AF AF No AF AF
Model 3c 1 [Reference] 1.70 (1.41–2.05) 1 [Reference] 2.24 (1.63–3.09)
Overall Mortality
No. of deaths 2727 1007 1337 275 Person-time, y 22 5850 10 317 73 671 1632 Model 1a 1 [Reference] 4.14 (3.84–4.47) 1 [Reference] 5.13 (4.47–5.89) Model 2b 1 [Reference] 3.43 (3.17–3.71) 1 [Reference] 4.00 (3.48–4.61) Model 3c 1 [Reference] 2.18 (2.00–2.37) 1 [Reference] 2.40 (2.05–2.78) Abbreviation: AF, atrial fibrillation.
a
Model 1 adjusted for age and sex. b
Model 2 adjusted for baseline age, sex, educational level, body mass index, smoking status, hypertension, diabetes, prevalent coronary heart disease, heart failure, estimated glomerular filtration rate, chronic kidney disease, and chronic obstructive pulmonary disease.
c