Bicuspid aortic valve syndrome and
fibrillinopathies: potential impact on clinical
approach
Rosina De Cario
1,2,*, Elena Sticchi
1,2,*, Betti Giusti
1,2, Rosanna Abbate
1,2, Gian Franco Gensini
1,2,3,
Stefano Nistri
1,2,4, Guglielmina Pepe
1,21 Department of Experimental and Clinical Medicine, Section of Critical Medical Care and Medical Specialities; DENOTHE Center, University of Florence, Italy;
2 Department of Heart and Vessels, Marfan Syndrome and Related Disorders Regional Referral Center, Careggi Hospital, Florence, Italy;
3 S. Maria agli Ulivi Center, Fondazione Don Carlo Gnocchi, Onlus, IRCCS, Florence, Italy; 4 Cardiology Service, CMSR Veneto Medica, Altavilla Vicentina, Italy;
Introduction
Bicuspid aortic valve (BAV) is the most common congenital cardiac malformation with an estimated prevalence between 0.5% and 2% and a strong male predominance (M:F=3:1). BAV is a multifaceted, heterogeneous disorder (Figure 1). Its natural history is determined by hemodynamic valvular impairment (present at birth or, more commonly, acquired by aging), and/ or by increased prevalence of aortic abnormalities ranging from reduced aortic elasticity to aortic dilatation/aneurysm/ dissection1-10.
Each of the above features can be found in patients with isolated BAV or, in association with multiple congenital heart diseases (e.g. hypoplastic left heart syndrome, aortic coarctation, patent ductus arteriosus, ventricular septal defect), either in a syndromic (e.g. Turner’s syndrome, Williams syndrome) or in non-syndromic fashion. The familial clustering of BAV and/or its related aortopathy has been documented in up to 20-30% of patients with isolated BAV supporting the notion of a relevant genetic background in BAV. Moreover, BAV can be detected in relatives of individuals with congenital abnormalities of the left ventricular outflow tract. This evidence has highlighted the need for screening first-degree relatives of BAV patients for aortic valve abnormalities, anomalies of the left ventricular outflow tract, and thoracic aortic wall alterations. Nonetheless, while multiple studies have searched for gene mutations and association with different chromosomal loci, the genetic bases of BAV, to date, are poorly defined11-15.
Due to the high prevalence of isolated BAV, the perceived burden of thoracic aortic complications, namely aneurysm and dissection, has led many authors to an early indication to prophylactic aortic surgery in individuals with BAV in comparison with subjects with three-leaflet aortic valve16,17. This
position has been also supported by the presence of multiple reported similarities between BAV and Marfan syndrome (MFS)18. Recently, however, two large, long-term, retrospective
cohort studies of BAV patients 19,20, while confirming the
absolute increased risk of aortic dissection in BAV in
comparison with the general population, reported a low number of events. These findings have raised concerns 21,22 on the
application of surgical criteria adopted in Marfan (MF) patients to those with BAV and thoracic aortic aneurysm (TAA), resulting in more conservative and individualized recommendations for the repair of the aortic sinuses or replacement of the ascending aorta in BAV patients by the 2014 AHA/ACC valvular heart disease guidelines23.
Pathogenesis
Despite the high prevalence, the pathogenetic mechanisms underlying the development of BAV are yet to be entirely clarified.
Embryology
According to many studies, the major factor involved in BAV pathogenesis is represented by the fusion of the two cusps occurring in the earlier stages of valvulogenesis during fetal development. One of the first theories assumed that failure in
Abstract
Bicuspid aortic valve (BAV) is a common heterogeneous disorder whose natural history is determined by hemodynamic valvular impairment and/or increased prevalence of aortic abnormalities ranging from dilatation to aneurysm and dissection. BAV-related aortopathy is frequently associated with relevant aortic pathologic changes leading to structural alterations, characteristic degenerative lesions and histological changes of the aorta very similar to those identified and described in patients with Marfan syndrome (MFS), an inherited connective tissue disorder associated with mutations in fibrillin 1 (FBN1) gene in more than 90% of patients. Recently, a 4-fold increase in the prevalence of BAV in MFS patients has been reported. Subsequently, pathogenetic FBN1 mutations in patients with BAV and aortic dilatation/aneurysm in whom MFS and other more severe type 1 fibrillinopathies were clinically excluded have been identified. In this review we discuss how this evidence, together with that of the wide heterogeneity in pathogenetic mechanisms of BAV-related aortopathy, may impact the clinical management of BAV.
cusps separation is the result of an abnormal blood flow across the developing valves. More recently, it has been suggested that other mechanisms, such as cell migration, signalling pathways, and genetic susceptibility may be involved. These mechanisms, together with abnormal neural crest migration, might lead to isolated or combined defects of the ascending aorta and aortic valve 24-26. Aortic, cervicocephalic and
intracranial aneurysms all originate from the neural crest and are documented to have a higher incidence in BAV population27.
Furthermore, it has been shown that different embryological mechanisms are responsible for BAV with different spatial orientations of the cusps 28. Moreover, newer experimental
models have found alternative embryological pathways leading to BAV formation29. Other theories suggest that extracellular
matrix proteins, which are involved in cell differentiation and
cusp formation during the process of valvulogenesis, might play a pivotal role in BAV development. Endothelial nitric oxide is a key factor involved in the process of vascular and valve formation during embryogenesis. Lee and colleagues observed that knockout mice, lacking endothelial nitric oxide synthase, had a predisposition in developing BAV. This result supports the hypothesis that inadequate levels of this protein or its abnormalities may be involved in cell signalling alteration during valvulogenesis in mammalian heart30. However, all these
findings suggest that aortic valve dysfunction in BAV is the result of a combination of the altered biochemical, mechanical and morphological factors involved in late valve development by regulating the processes of valve tissue remodelling and leaflet architecture.
Clinical features associated with BAV
Aortic stenosis, a common complication of BAV (occurring in up to 50% of BAV patients), represents a result of premature fibrosis and calcification due to hemodynamic shear stress, an active process in which endothelium dysfunction takes place by involving inflammation, lipoprotein deposition, calcification, and ossification of the aortic side of the valve leaflets 31.
Aortic regurgitation has a lower prevalence in BAV than stenosis (7-20%) and represents the predominant functional complication in young age 32,33. The pathogenesis of aortic
regurgitation in BAV patients is complex: it can occur as an isolated functional abnormality due to fibrosis and retraction of the commissural margins of the leaflets or cusp prolapse.
Figure 3: Schematic representation of the spectrum of possible patterns of aortic dimensions in association with BAV and their classification according to three tested methods10,37,79,93-96. The
broken lines indicate the profile of a normal proximal aorta. Arrows emphasize the dimensional relations between diameters at the sinus, sinotubular and tubular levels96 (from Della Corte et al., Eur J
Cardiothorac Surg 2014 Jan 14)79.
Figure 1: Venn Diagram representing bicuspid aortic valve (BAV) syndrome. BAV can be isolated or associated with congenital heart diseases, can display hemodynamic valvular disorders (VD) which can be congenital or acquired (e.g.: post infective endocarditis, degenerative). The thoracic aorta can be dilated (TA dil), or aneurysmatic (TAA), and an increase incidence of thoracic aortic dissection (TAD) has been reported. These features can be associated in a syndromic or in a non-syndromic fashion.
Alternatively, it can also originate in combination with external factors such as aneurysmal enlargement of the root and valve annulus or valvular destruction secondary to endocarditis. Aortic regurgitation can also lead to an increased risk of heart failure, endocarditis and arrhythmia34. Recently, Benedik
and colleagues evaluated the histological and mechanical characteristics of the aortic wall in patients who underwent aortic stenosis or regurgitation surgery and showed that the latter group had a worse quality and a superior thickness of the ascending aorta than the former 35. Roberts and colleagues
observed, in histological sections of ascending aortas, only a minimal loss of medial elastic fibers in the aortic media of patients with aortic stenosis compared to severe elastic fibers damage reported in patients with aortic regurgitation36.
Aortic dilation (mainly involving the ascending aorta) is one of the most common non-valvular findings in BAV occurring in 35-80% of adult patients3,4,19,37,38. It is mainly asymptomatic and often
precedes aortic dissection or rupture. The considerable incidence of aortic dilation in BAV patients suggests a correlation between the aortic disease and the congenital malformation. Earlier studies, conducted by Larson and Edwards39, reported a 9-fold
increased risk of aortic dissection in BAV patients and an 18-fold higher risk in unicommissural aortic valve compared with controls. These findings suggested that the valve malformation may act as an independent risk factor for aortic dissection. However, the pathogenesis, as well as the cellular and molecular mechanisms underlying the development and progression of aortic dilation in BAV, is not clearly understood and remains controversial. Some mechanisms have been proposed so far that could take part in the pathogenesis of BAV-associated aortic aneurysms. According to the “Hemodynamic theory”, the altered hemodynamics in BAV, represented by a severe turbulence in blood flow, post-stenotic aortic dilation, and increased stroke volume, is the most common causative factor of root and ascending aorta segment dilation40.
Aortic dilation leads, as a consequence, to a greater expansion of the lumen, a reduction of wall thickness and a generalized increase of wall tension (Laplace law). These abnormalities may eventually result in aortic dissection or frank rupture. Vergara and colleagues41 have recently succeeded in supporting the
hemodynamic hypothesis according to which the critical blood flow dynamics in the ascending aorta of BAV patients were responsible for the development and progression of aneurysm. In this study, a surface model of ascending aorta was obtained from magnetic resonance imaging (MRI) and numerical simulations of ascending aorta hemodynamics with different configurations of orifice area and valve orientation were performed in order to investigate the resulting wall shear stress (WSS) distributions and the asymmetry of the blood flow. High WSS-based indices (introduced to evaluate quantitatively the influence of valve geometry on magnitude of WSS in the ascending aorta) were found at the mid-ascending aorta, at the sinus of Valsava and at the sinotubular junction. These data confirm that the higher risk of developing aneurysm in BAV patients is related to the peculiar geometry of BAV and, consequently, to the abnormality of the blood flow. Conti and colleagues found a 36% increase in voltage at the wall of the longitudinal curvature of the ascending aorta in patients with BAV compared with TAV in tricuspid aortic valve (TAV) patients42. In 2011, Girdauskas further confirmed the
role of altered hemodynamics as the main cause of aortopathy development in BAV despite the presence of a congenital defect43.
Common features underlying BAV and Marfan patients
The structural histological aortic pathology described above have been shown to be very similar to those identified and described in MF patients. MFS is an inherited connective tissue disorder associated with mutations in the fibrillin-1 (FBN1)
gene in more than 90% of patients, and in transforming growth factor beta receptor 2 and 1 (TGFBR2 and TGFBR1) genes in less than 5%44. The common degenerative lesions and
histological changes include degeneration of the aortic media with extracellular fragmentation and disorganization of elastic lamellae, high rate of vascular smooth muscle cell loss and accumulation of mucopolysaccharides 8,19,45. Several studies
demonstrated that vascular complications observed in MFS are a result of the impairment and weakness of the connective tissue due to the reduction of fibrillin-1. This glycoprotein represents the main component of the microfibril structures of the extracellular matrix, which has a crucial role in connecting vascular smooth muscle cells to elastin and collagen and, consequently, in maintaining tissue elasticity46-48. In 2003, Fedak
and colleagues hypothesized that the mechanism of vascular matrix reorganization and remodelling, that contributes to aortopathy associated with BAV, might be the result of fibrillin-1 deficiency49. Indeed, their data demonstrated a significant
reduction in fibrillin-1 glycoprotein content in the aortic media of a subset of patients with congenital BAV. They also observed that the abundance of fibrillin-1 was equivalent in patients with normal valves and in those with TAV disease, suggesting that the reduction of the protein was specific to the presence of the congenital BAV and it wasn’t the result of a valve dysfunction. Moreover, the deficiency of fibrillin-1 may result in an alteration of TGF-β signalling similar to that found in MFS7. Sakai and
colleagues observed that fibrillin-1 is homologous with the family of latent transforming growth factor β (TGF-β) binding proteins (LTBPs), which serve to hold TGF-β in an inactive complex in various tissues, including the extracellular matrix50.
The researchers showed that fibrillin-1 can bind TGF-β and LTBPs51,52. On the basis of these data, Dietz and co-workers
hypothesized that abnormal fibrillin-1 or reduced levels of fibrillin-1 in connective tissue, might result in an excess of active TGF-β. They managed to prove this hypothesis and to demonstrate that blocking TGF-β with neutralizing antibodies led to the normalization of lung development in affected mice53.
Data by Loeys and colleagues54, together with those from
studies involving mouse models of fibrillinopathies, showed that Marfan phenotype results mostly from perturbed TGF-β signalling53. Therefore, the aortic dilation in BAV may be the
result of an underlying congenital defect caused by a mutation in FBN1, TGFBR1 or TGFBR2 genes.
Genetics of BAV
BAV has an autosomal dominant pattern of inheritance with incomplete penetrance. Recent studies demonstrated that BAV may be due to mutations in different genes13. The transcriptional
regulator NOTCH1 gene (chr 9q34.3), encoding a single-pass transmembrane receptor and functioning in a highly conserved pathway, has been associated with the development and acceleration of calcium deposition in nonsyndromic BAV in humans55 (Table 1). The Notch signaling pathway plays a
critical role in cell fate determination and differentiation during organogenesis and it regulates osteogenesis56. However,
a consistent contribution of NOTCH1 gene variants to the development of BAV is yet to be clearly defined. Genome wide marker-based linkage analysis demonstrated a linkage of BAV to loci on chromosomes 18q, 5q and 13q in families with autosomal dominant inheritance of the disease57 (Table 1). These regions
are likely to contain genes whose mutations result in BAV and/ or associated cardiovascular manifestations, suggesting their potential role in valvulogenesis and cardiac development. Recently, the essential role of GATA5 (GATA-binding protein 5) in aortic valve morphogenesis and endocardial cell differentiation58
with a reduced UFD1L (ubiquitin fusion degradation 1-like) gene expression (Table 1). The UFD1L gene encodes a component of a multi-enzyme complex involved in the degradation of ubiquitin fusion proteins during embryogenesis and its down-regulation, probably due to an abnormal behavior of neural crest cells, may lead to reduced degradation activities. These results highlight the important role of the UFD1L gene in the development of ectoderm-derived structures, including neural crest cells in aortic leaflets formation, supporting the hypothesis of a genetic background in the pathogenesis of BAV59.Other genes have been
associated with BAV. Wooten and colleagues demonstrated an association between BAV and a locus containing AXIN1 and
PDIA2 genes in a cohort of 68 BAV probands and 830 control subjects60 (Table 1). AXIN1 (AXisINhibitor 1) is a critical member
of the Wnt pathway and acts as a crucial regulator of both heart valve formation61 and cardiac neural crest development62. It also
influences TGF-β signaling63. The potential role of PDIA2 (Protein
Disulfide Isomerase family A, member 2) in heart valve formation is unknown. Further genotyping is required to determine the relative contribution of AXIN1 and PDIA2 variants to BAV. About 12% of BAV/TAA patients carry mutations in ACTA2 (Actin, alpha 2, smooth muscle, aorta; chr. 10q), a distinct subgroup characterized by livedo reticularis on lower limbs, and iris flocculi64. Regarding TGFBR1 and TGFBR2 genes analyses, no
mutations were detected in BAVs with aortic dilation except for one incomplete clinically depicted patient carrying a TGFBR2
mutation65,66. Animal studies have also been performed to identify
genetic bases of BAV disease (Table 1). In mice, in particular, an association between BAV and the homozygous deletion of the endothelial nitric oxide synthase gene (Nos3) has been demonstrated, and haploinsufficiency in the cardiac homeobox gene Nk2-5, is linked to a higher incidence of BAV30,67.
Marfan Syndrome, BAV and FBN1 mutations
Recently, we demonstrated a 4-fold increase in the prevalence of BAV in a large cohort of unrelated MFS patients with respect to the general population screened by echocardiography68
(Figure 2). Indeed, out of the 257 unrelated MF patients [151 males (58%)], BAV was unequivocally identified in 12 (4.7%) MF patients [10 males (83%)]18. Only 3 patients accepted to
undergo mutation screening analysis18. Previously described
mutations were detected in 2 out of 3 patients69, they involved
conserved cysteine residues and are thought to be causative because they alter fibrillin-1 structure (Figure 2). These findings are consistent with data showing decreased FBN1 mRNA or protein content in a subgroup of BAV patients49, which suggest
that FBN1 may be one of the genes associated with BAV. Interestingly, most of MFS/BAV patients were males, a more common finding in BAV than in Marfan cohorts. Moreover, the association between the two disorders seems to cause a more severe involvement of the aorta with a higher percentage of TAA requiring surgery. Finally, our MFS/BAV did not present further congenital heart diseases, aortic valve calcification or livedo reticularis14,64. Interestingly, Z score was>2 in all our
adult patients44. Moreover, ectopia lentis, dural ectasia, myopia
and striae distense were common in our MFS/BAV, while they presented mostly minor skeleton criterion70.
Noteworthy, all 12 MFS/BAV patients satisfied the clinical diagnostic criteria for MFS also according to the newly revised Ghent criteria44. Although a reduced FBN1 content has been
reported in the aortic media of BAV patients49, it has been
stated that in multiple clinical disorders associated with FBN1 alterations there is no propensity for congenital aortic valve malformations71. Our data challenged this consideration,
prompting the need for the mutation screening analysis of BAV patients not fulfilling the clinical criteria for MFS. Moreover, from the practical point of view, the paper of Nistri et al.18
underscored the need to optimize the visualization of aortic valve morphology in MFS patients and the importance of comprehensive clinical evaluation of BAV patients to detect clinical features suggestive for inherited connective tissue disorders.
Subsequently, our group performed a study aimed to screen for FBN1 mutations in ten patients with BAV and thoracic aortic dilation, not fulfilling the clinical criteria for MFS11 (Figure
2). Mutation analysis was performed on 8 of the 10 patients and FBN1 mutations were detected in two. One patient had a c.1586G>A, p.Arg529Gln amino acid substitution which represents a basic to polar neutral charge change in exon 12 (cbEGF-like 03 domain). In the other patient, a double mutation was detected: a c.1906A > G change (p.Arg636Gly basic to apolar substitution) and a c.8176C > T mutation (p.Arg2726Trp causing a basic to apolar change); the first located in exon 15 (cbEGF-like 06 domain), the second in exon 64 (COOH unique region)11 (Figure 2).
This was the first study reporting pathogenetic FBN1 mutations in patients with BAV and aortic dilation/aneurysm in whom MFS and other more severe type 1 fibrillinopathies were clinically excluded44. The mutations detected in the two unrelated studied
patients are arginine substitutions11. The Arg529Gln mutation
detected in one patient was also reported at the UMD-FBN1 database in a male proband of France geographic origin with an incomplete MFS phenotype. Moreover, a single nucleotide substitution in the same codon, causing a preterminal stop codon, was previously described in a Norwegian patient displaying a classic MF phenotype with ectopia lentis, thoracic aorta dilation and systemic features72. The other patient
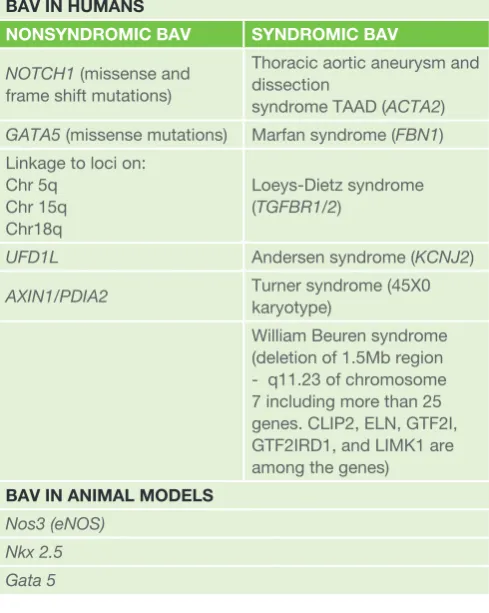
Table 1: Genes involved in BAV in human and animal models
BAV IN HUMANS
NONSYNDROMIC BAV SYNDROMIC BAV
NOTCH1 (missense and frame shift mutations)
Thoracic aortic aneurysm and dissection
syndrome TAAD (ACTA2)
GATA5 (missense mutations) Marfan syndrome (FBN1) Linkage to loci on:
Chr 5q Chr 15q Chr18q
Loeys-Dietz syndrome (TGFBR1/2)
UFD1L Andersen syndrome (KCNJ2)
AXIN1/PDIA2 Turner syndrome (45X0 karyotype)
William Beuren syndrome (deletion of 1.5Mb region - q11.23 of chromosome 7 including more than 25 genes. CLIP2, ELN, GTF2I, GTF2IRD1, and LIMK1 are among the genes)
BAV IN ANIMAL MODELS Nos3 (eNOS)
showed two mutations, one (Arg2726Trp) was previously associated with variable clinical phenotypes, including mitral valve prolapse (MVP) and myopia69, isolated skeletal features73,
combined skeletal and ocular manifestations74, mild skeletal
abnormalities75; and a family in which the mutation displayed
incomplete penetrance76. This mutation was reported in one
chromosome of the 1000Genomes and NHLBI Exome Variant Server databases as rs61746008 (http://www.1000genomes. org/ and http://evs.gs.washington. edu/EVS/). The second mutation (Arg636Gly) has never been reported in literature, although another single nucleotide substitution, responsible for a different amino acid change at the same codon (Arg636Ile) in a MF patient with aortic root dilation, ectopia lentis and minor involvement of skeleton, was previously described74.
According to “Sorting Tolerant From Intolerant” (SIFT,http:// sift.jcvi.org) both the Arg2726Trp and Arg636Gly mutations act decreasing protein stability as evaluated in silicoby MuPro (http://www.igb.uci.edu/-baldig/mutation.html). It is unknown at present if the two FBN1 mutations of the second patient are in cis on the chromosome or in trans. The detection of FBN1
point mutations in patients with BAV/TAA without MFS, adds to the striking clinical heterogeneity of both BAV and type I fibrillinopathies showing that aortic dilation/aneurysm may develop in a subgroup of BAV patients as a manifestation of an inherited connective tissue disorder. Noteworthy, the two patients carrying the mutations were male, one displayed a family history of TAA, another had MVP, without systemic features which were otherwise prevalent in the remaining patients. Moreover, both had aortic aneurysm size attaining the threshold for surgery according to old American and current European Guidelines77,78, notwithstanding the young age, with
the largest diameter localized at the level of the sinuses of Valsalva, a pattern of aortic dilation, specifically addressed as “root phenotype” by Della Corte et al37, and considered to
be an independent predictor of fast progression79 (Figure 3).
Interestingly, 8 out of our 10 patients displayed this phenotype, in association with a certain degree of systemic features typical of connective tissue disorders11. Finally, the 2 patients
bearing FBN1 mutations had significant aortic regurgitation, which is a powerful predictor of loss of aortic medial elastic fibers in patients with ascending aortic aneurysms and aortic valve disease35,36. These findings call for greater focus on the
BAV-related cardiovascular abnormalities rather than on the MFS-like systemic features, which may well coexist and warrant investigation in BAV patients in general, but are not associated with the FBN1 mutations identified in the present study. On the other hand, these FBN1 mutations do not completely fulfil the definition of the major criterion for MFS according to the revised Ghent criteria since they have never been detected in Marfan patients with TAA44. Therefore, our two BAV/TAA patients did
not achieve the diagnosis of MFS.
FBN1 gene has been previously associated with various conditions11,80,81. The interfamilial clinical heterogeneity at the
FBN1 locus is further characterized by a striking intrafamilial variability (OMIM*134797). Contrasting data have been reported regarding the genetic background of BAV-related aortopathy. A
decrease in FBN1 mRNA and protein has been demonstrated
in some BAV patients suggesting a possible involvement of
FBN1 with BAV49. Moreover, single nucleotide polymorphisms
(SNPs) spread in the area of the FBN1 gene, which predispose to TAA, have been reported80. On the other hand, other
investigators have screened BAV patients for mutations in
FBN1, TGFBR2, and TGFBR1 genes and failed to detect any mutation, concluding that FBN1 gene is not, or only rarely, associated with BAV66. More recently, a mutation in TGFBR2
gene was reported in a patient classified as aortic dilation/
aneurysm but otherwise not well clinically defined43. Another
recent study, comparing gene expression in subjects with BAV and TAV, reported an increase of FBN1 mRNA only in the subjects with TAV81. Thus, it is conceivable that BAV represents
the phenotypic manifestation of many distinct clinical outliers underlined by genetic, molecular, and structural anomalies that do not follow a common path82. At present, we cannot exclude
a coincidence of a common trait such as BAV in males and a rare trait like MFS in our patients.
Conclusions
Recent improvements in knowledge regarding the natural history of the aortopathy in BAV19,20 have raised concerns
regarding the direct application of surgical criteria adopted in MFS patients to those with BAV and aortic dilation/ aneurysm21,22 although multiple similarities have been shown
between MFS and BAV patients. Due to the prevalence of BAV and of associated dilatation/aneurysm of the ascending aorta, the increase in relative risk for aortic dissection in BAV patients could result into a disproportionately high indication for prophylactic aortic surgery by implementing criteria adopted for MFS and related disorders. Despite the 7-10 fold-increase in risk of dissection, the incidence of aortic dissection/rupture remains low (3-4/10.000 patient-years)19-23. Moreover, data
regarding a threshold of aortic size portending an absolute increase in risk of dissection in BAV, such to warrant aortic surgery (when aortic valve replacement is not indicated based on the severity of aortic stenosis or regurgitation) are limited. On the other hand, cardiovascular events are considerable in patients with FBN1 mutations and remain so throughout life, with men appearing to be at higher risk for an aortic event than women83. Our findings may thus have potential clinical
implications, if confirmed by larger studies. Although sample size of our study and its retrospective design did not propose surgical implications, our data support the need of future studies aimed at characterizing BAV patients with aortic dilation/ aneurysm according both to valvular and aortic phenotype (including rate of increase in aortic size), family history of aortic dissection and systemic clinical stigmata of connective tissue disorders, eventually performing genetic testing when appropriate, in order to promote individualized approach to these patients23. Whether such an approach would result in
a different outcome, potentially affecting therapeutic choices in patients with BAV and aortic dilation/aneurysm, should be a pivotal target of such research23. A further implication for
the discovery of the presence of FBN1 mutations in BAVs with and without systemic manifestations of MFS, is the need of a multidisciplinary approach (including internal medicine, medical genetics, cardiology, ophthalmology, cardiovascular surgery, orthopaedic, and molecular biology experts) for a comprehensive global assessment and, possibly, management of patients with BAV. While a number of studies79,84 underscore
the relevance of a more detailed phenotyping of BAV and its related aortic aneurysm, our data address the potential role of a generalized phenotypic approach aimed at detecting and possibly graduating the systemic manifestations of connective tissue disorders. In this perspective, a clinically oriented utilization of genetic testing, may be useful for the recognition of a responsible gene mutation to identify syndromic features, to confirm a clinical diagnosis, and to evaluate relatives who are at risk for the condition. However, a cautionary word regarding use and interpretation of genetic tests is needed, and genetic counselling should be included with its use.
Notwithstanding a great interest 85,86, there is no proven medical
aortic size in BAV patients23. Indeed, the classic pathophysiology
of aortopathy in MFS founded the basis for the use of β-blockers, whose effectiveness in preventing aortic dissection in a
great proportion of a large cohort of MFS patients has been recently shown87. Moreover, the novel interpretation of the
pathophysiology of MFS-related aortopathy based on TGF-β
signaling88, has resulted in researches evaluating the potential of
TGF-β –antagonism by ACE-inhibitors and angiotensin II receptor blockers (ARB)89-92. Prospective, randomized, controlled trial,
indicating a beneficial effect of losartan treatment on aortic root dilation rate in adults with MFS, have been reported93.
However, since specific therapeutic data in BAV patients are lacking, no recommendation can be withdrawn, beyond that of treatment of systemic arterial hypertension23. It is conceivable
that the identification of specific genetic backgrounds and signalling pathways might theoretically support the utilization of specific medical approaches, in the future, tailored on individual patients93. Finally, considering the specific natural history of
patients with FBN1 mutations in the general population83 the
finding of such genetic etiology in BAV patients might justify an aggressive surgical approach in a subgroup of BAV individuals, but also support the recent indication of more conservative thresholds for aortic surgery in patients in whom such mutations are not detected.
Correspondence to:
Guglielmina Pepe, MD
Department of Experimental and Clinical Medicine University of Florence
Marfan Syndrome and Related Disorders Regional Referral Center (Tuscany Region)
Department of Heart and Vessels, Careggi Hospital Largo Brambilla, 3
50134 Florence Italy
Tel/Fax +390557949646 Email: [email protected]
References
1. Nistri S, Sorbo MD, Marin M, Palisi M, Scognamiglio R, Thiene G. Aortic root dilatation in young men with normally functioning bicuspid aortic valves. Heart. 1999 Jul;82(1):19-22
2. Nistri S, Sorbo MD, Basso C, Thiene G. Bicuspid aortic valve: abnormal aortic elastic properties. J Heart Valve Dis. 2002 May;11(3):369-73; discussion 373-4
3. Nistri S, Basso C, Marzari C, Mormino P, Thiene G: Frequency of bicuspid aortic valve in young male conscripts by echocardiogram. Am J Cardiol 2005, 96:718–721
4. Cecconi M, Nistri S, Quarti A, Manfrin M, Colonna PL, Molini E, Perna GP. Aortic dilatation in patients with bicuspid aortic valve. J Cardiovasc Med (Hagerstown). 2006 Jan;7(1):11-20
5. Nistri S, Grande-Allen J, Noale M, Basso C, Siviero P, Maggi S, Crepaldi G, Thiene G: Aortic elasticity and size in bicuspid aortic valve syndrome. Eur Heart J 2008, 29:472–479.
6. Fedak PW. Bicuspid aortic valve syndrome: heterogeneous but predictable? EurHeart J. 2008 Feb;29(4):432-3
7. Tadros TM, Klein MD, Shapira OM. Ascending aortic dilatation associated with bicuspid aortic valve: pathophysiology, molecular biology, and clinical implications. Circulation 2009 Feb 17;119(6):880-90 8. Siu SC, Silversides CK: Bicuspid aortic valve disease. J Am Coll
Cardiol2010, 55:2789–2800
9. Braverman AC. Aortic involvement in patients with a bicuspid aortic valve. Heart. 2011 Mar;97(6):506-13
10. Della Corte A, Bancone C, Buonocore M, Dialetto G, Covino FE, Manduca S, Scognamiglio G, D’Oria V, De Feo M. Pattern of ascending aortic dimensions predicts the growth rate of the aorta in patients with bicuspid aortic valve. JACC Cardiovasc Imaging. 2013 Dec;6(12):1301-10 11. Pepe G, Nistri S, Giusti B, Sticchi E, Attanasio M, Porciani C, Abbate
R, Bonow RO, Yacoub M, Gensini GF. Identification of fibrillin 1 gene
mutations in patients with bicuspid aortic valve (BAV) without Marfan syndrome. BMC Med Genet.2014 Feb 24;15:23
12. Clementi M, Notari L, Borghi A, Tenconi R. Familial congenital bicuspid aortic valve: a disorder of uncertain inheritance. Am J Med Genet 1996;62:336-8
13. Cripe L, Andelfinger G, Martin LJ,Shooner K, Benson DW. Bicuspid aortic valve is heritable. J Am Coll Cardiol 2004;44:138-43
14. Loscalzo ML, Goh DL, Loeys B, Kent KC, Spevak PJ, Dietz HC. Familial thoracic aortic dilation and bicommissural aortic valve: a prospective analysis of natural history and inheritance. Am J Med Genet A 2007;143a:1960–7
15. Kerstjens-Frederikse WS, Du MarchieSarvaas GJ, Ruiter JS, Van Den Akker PC, Temmerman AM, Van Melle JP, Hofstra RM, Berger RM. Left ventricular outflow tract obstruction: should cardiac screening be offered to first-degree relatives? Heart 2011 Aug;97(15):1228-32
16. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr, Eagle KA, Hermann LK, Isselbacher EM, Kazerooni EA, Kouchoukos NT, Lytle BW, Milewicz DM, Reich DL, Sen S, Shinn JA, Svensson LG, Williams DM; American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American College of Radiology; American Stroke Association; Society of CardiovascularAnesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society of Thoracic Surgeons; Society for Vascular Medicine. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter CardiovascInterv. 2010 Aug 1;76(2):E43-86
17. Svensson LG, Kim KH, Blackstone EH, Rajeswaran J, Gillinov AM, MihaljevicT,GriffinBP, Grimm R, Stewart WJ, Hammer DF, Lytle BW. Bicuspid aortic valvesurgery with proactive ascending aorta repairJThoracCardiovascSurg 2011Sep;142(3)622-9, 629.e1-3 18. Nistri S, Porciani MC, Attanasio M, Abbate R, Gensini GF, Pepe G.
Association of Marfan syndrome and bicuspid aortic valve: frequency and outcome. Int J Cardiol 2012 Mar 8;155(2):324-5
19. Michelena HI, Khanna AD, Mahoney D, Margaryan E, Topilsky Y, Suri RM, Eidem B, Edwards WD, Sundt TM 3rd, Enriquez-Sarano M: Incidence of aortic complications in patients with bicuspid aortic valves. JAMA 2011, 306:1104–1112
20. Tzemos N, Therrien J, Yip J, Thanassoulis G, Tremblay S, Jamorski MT, Webb GD, Siu SC: Outcomes in adults with bicuspid aortic valves. JAMA 2008, 300:1317–1325.
21. Sundt TM 3rd: Replacement of the ascending aorta in bicuspid aortic valve disease: where do we draw the line? J Thorac Cardiovasc Surg 2010, 140(6 Suppl):S41–S44.
22. Roberts WC: Prophylactic replacement of a dilated ascending aorta at the time of aortic valve replacement of a dysfunctioning congenitally unicuspid or bicuspid aortic valve. Am J Cardiol 2011, 108:1371–1372 23. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton
RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014 Mar 3. pii: S0735-1097(14)01280-7 24. Sans-Coma V, Fernandez B, Duran AC, Thiene G, Arqué JM,
Muñoz-Chápuli R, Cardo M: Fusion of valve cushions as a key factor in the formation of congenital bicuspid aortic valves in Syrian hamsters. Anat Rec 1996;244:490–8
25. Duran AC, Frescura C, Sans-Coma V, Angelini A, Basso C, Thiene G. Bicuspid aortic valves in hearts with other congenital heart disease. J Heart Valve Dis 1995;4:581–90
26. Kappetein AP, Gittenberger-de Groot AC, Zwinderman AH, Rohmer J, Poelmann RE, Huysmans HA. The neural crest as a possible
pathogenetic factor in coarctation of the aorta and bicuspid aortic valve. J ThoracCardiovascSurg 1991;102:830–6
27. Schievink WI, Raissi SS, Maya MM, Velebir A. Screening for intracranial aneurysms in patients with bicuspid aortic valve. Neurology 2010 May 4;74(18):1430-3
28. Fernández B, Durán AC, Fernández-Gallego T, Fernández MC, Such M, Arqué JM, Sans-Coma V. Bicuspid aortic valves with different spatial orientations of the leaflets are distinct etiological entities. J Am Coll Cardiol2009 Dec 8;54(24):2312-8
29. Thomas PS, Sridurongrit S, Ruiz-Lozano P, Kaartinen V. Deficient signaling via Alk2 (Acvr1) leads to bicuspid aortic valve development. PLoS One 2012;7(4):e3553
31. Wallby L, Janerot-Sjoberg B, Steffensen T, Broqvist M. T lymphocyte infiltration in non-rheumatic aortic stenosis: a comparative descriptive study between tricuspid and bicuspid aortic valves. Heart 2002;88:348 –51
32. Roberts WC, Morrow AG, McIntosh CL, Jones M, Epstein SE. Congenitally bicuspid aortic valve causing severe, pure aortic
regurgitation without superimposed infective endocarditis. Analysis of 13 patients requiring aortic valve replacement. Am J Cardiol 1981;47(2):206– 9.
33. Lewin MB, Otto CM. The bicuspid aortic valve: adverse outcomes from infancy to old age. Circulation 2005;111(7):832–4
34. Fedak PW, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circula¬tion 2002;106:900–904
35. Benedik J, Pilarzcyk K, Wendt D, Price V, Tsagakis K, Perrey M, Baba HA, Jakob H. Is there any difference in aortic wall quality between patients with aortic stenosis and those with regurgitation? Eur J CardiothoracSurg 2013 Oct;44(4):754-9
36. Roberts WC, Vowels TJ, Ko JM, Filardo G, Hebeler RF Jr, Henry AC, Matter GJ, Hamman BL. Comparison of the structure of the aortic valve and ascending aorta in adults having aortic valve replacement for aortic stenosis versus for pure aortic regurgitation and resection of the ascending aorta for aneurysm. Circulation 2011 Mar 1;123(8):896-903 37. Della Corte A, Bancone C, Quarto C, Dialetto G, Covino FE, Scardone
M Caianiello G, Cotrufo M: Predictors of ascending aortic dilatation with bicuspid aortic valve: a wide spectrum of disease expression. Eur J CardiothoracSurg 2007;31: 397–405
38. Jackson V, Petrini J, Caidahl K, Eriksson MJ, Liska J, Eriksson P, Franco-Cereceda A: Bicuspid aortic valve leaflet morphology in relation to aortic root morphology: a study of 300 patients undergoing open-heart surgery. Eur J CardiothoracSurg 2011;40:118–24
39. Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsy study of161 cases. Am J Cardiol 1984 Mar 1;53(6):849-5
40. Thanassoulis G, Yip JWL, Filion K, Jamorski M, Webb G, Siu SC. Retrospective study to identify predictors of the presence and rapid progression of aortic dilatation in patients with bicuspid aortic valves. Nat ClinPractCardiovascMed 5: 821–8, 2008
41. Vergara C, Viscardi F, Antiga L, Luciani GB. Influence of bicuspid valve geometry on ascending aortic fluid dynamics: a parametric study. Artif Organs 2012 Apr;36(4):368-7
42. Conti CA, Della Corte A, Votta E, Del Viscovo L, Bancone C, De Santo LS, Redaelli A. Biomechanical implications of the congenital bicuspid aortic valve: a finite element study of aortic root function from in vivo data. J ThoracCardiovasc Surg2010 Oct;140(4):890-6, 896.e1-2
43. Girdauskas E, Borger MA, Secknus MA, Girdauskas G, Kuntze T. Is aortopathy in bicuspid aortic valve disease a congenital defect or a result of abnormal hemodynamics? A critical reappraisal of a one-sided argument. Eur J Cardiothorac Surg2011 Jun;39(6):809-14
44. Loeys BL, Dietz HC, Braverman AC, Callewaert BL, De Backer J, Devereux RB, Hilhorst-Hofstee Y, Jondeau G, Faivre L, Milewicz DM, Pyeritz RE, Sponseller PD, Wordsworth P, De Paepe AM: The revised Ghent nosology for the Marfan syndrome. J Med Genet 2010, 47:476–485 45. Nataatmadja M, West M, West J, Summers K, Walker P, Nagata M,
Watanabe T: Abnormal extracellular matrix protein transport associated with increased apoptosis of vascular smooth muscle cells in Marfan syndrome and bicuspid aortic valve thoracic aortic aneurysm. Circulation 2003, 108(Suppl 1):II329–II334
46. Milewicz DM, Pyeritz RE, Crawford ES, Byers PH. Marfan syndrome: defective synthesis, secretion, and extracellular matrix formation of fibrillin by cultured dermal fibroblasts. JClin Invest 1992;89(1):79-86
47. Pyeritz RE. The Marfan syndrome. In: Royce PM, Steinmann B, editors. Connective tissue and its heritable disorders: molecular, genetic and medical aspects. New York:Wiley-Liss;1993. p.437-68
48. de Sa M, Moshkovitz Y, Butany J, David TE. Histologic abnormalities of the ascending aorta and pulmonary trunk in patients with bicuspid aortic valve disease: clinical relevance to the ross procedure. J ThoracCardiovascSurg 1999 Oct;118(4):588-94
49. Fedak PW, de Sa MP, Verma S, Nili N, Kazemian P, Butany J, Strauss BH, Weisel RD, David TE. Vascular matrix remodeling in patients with bicuspid aortic valve malformations: implications for aortic dilatation. J ThoracCardiovascSurg 2003 Sep;126(3):797-806
50. Sakai LY, Keene DR. Fibrillin: monomers and microfibrils. Methods Enzymol1994;245:29-52
51. Maslen CL, Corson GM, Maddox BK, Glanville RW, Sakai LY. Partial sequence of a candidate gene for the Marfan syndrome. Nature 1991;352:334-7
52. Isogai Z, Ono RN, Ushiro S, Keene DR, Chen Y, Mazzieri R, Charbonneau NL, Reinhardt DP, Rifkin DB, Sakai LY: Latent transforming growth factor beta-binding protein 1 interacts with fibrillin and is a microfibril-associated protein. J BiolChem 2003;278:2750- 7
53. Gelb BD. Marfan’s syndrome and related disorders--more tightly connected than we thought. N Engl J Med 2006 Aug 24;355(8):841-4
54. Loeys BL, Schwarze U, Holm T, Callewaert BL, Thomas GH, Pannu H, De Backer JF, Oswald GL, Symoens S, Manouvrier S, Roberts AE, Faravelli F, Greco MA, Pyeritz RE, Milewicz DM, Coucke PJ, Cameron DE, Braverman AC, Byers PH, De Paepe AM, Dietz HC: Aneurysm syndromes caused by mutations in the TGF-β receptor. N Engl J Med 2006; 355:788-98 55. Mohamed SA, Aherrahrou Z, Liptau H, Erasmi AW, Hagemann C, Wrobel
S, Borzym K, Schunkert H, Sievers HH, Erdmann J: Novel missense mutations (p.T596M and p.P1797H) in NOTCH1 in patients with bicuspid aortic valve. BiochemBiophys Res Commun. 2006;345:1460–1465 56. Garg V. Molecular genetics of aortic valve disease. CurrOpinCardiol.
2006;21:180–184
57. Martin LJ, Ramachandran V, Cripe LH, Hinton RB, Andelfinger G, Taban¬gin M, Shooner K, Keddache M, Benson DW: Evidence in favor of linkage to human chromosomal regions 18q, 5q and 13q for bicuspid aortic valve and associated cardiovascular malformations. Hum Genet. 2007;121:275–284
58. Laforest B, Andelfinger G, Nemer M. Loss of Gata5 in mice leads to bi¬cuspid aortic valve. J Clin Invest. 2011;121:2876–2887
59. Mohamed SA, Hanke T, Schlueter C, Bullerdiek J, Sievers HH. Ubiquitin fusion degradation 1-like gene dysregulation in bicuspid aortic valve. J ThoracCardiovascSurg 2005 Dec;130(6):1531- 6
60. Wooten EC, Iyer LK, Montefusco MC, Hedgepeth AK, Payne DD, Kapur NK, HousmanDE, Mendelsohn ME, Huggins GS. Application of gene network analysis techniques identifies AXIN1/PDIA2 and endoglin haplotypes associated with bicuspid aortic valve. PLoS One 2010 Jan 21;5(1):e883
61. Armstrong EJ, Bischoff J: Heart Valve Development: Endothelial Cell Signaling and Differentiation. Circ Res 2004, 95: 459–470
62. Niessen K, Karsan A: Notch Signaling in Cardiac Development. Circ Res 2008, 102: 1169–1181
63. Wang J, Nagy A, Larsson J, Dudas M, Sucov HM, Kaartinen V. Defective ALK5 signaling in the neural crest leads to increased postmigratory neural crest cell apoptosis and severe outflow tract defects. BMC Dev Biol 2006 Nov 1;6:51
64. Guo DC, Pannu H, Tran-Fadulu V, Papke CL, Yu RK, Avidan N, Bourgeois S, Estrera AL, Safi HJ, Sparks E, Amor D, Ades L, McConnell V, Willoughby CE, Abuelo D, Willing M, Lewis RA, Kim DH, Scherer S, Tung PP, Ahn C, Buja LM, Raman CS, Shete SS, Milewicz DM: Mutations in smooth muscle alpha-actin (ACTA2) lead to thoracic aortic aneurysms and dissections. Nat Genet 2007, 39:1488–1493
65. Girdauskas E, Schulz S, Borger MA, Mierzwa M, Kuntze T. Transforming growth factor-beta receptor type II mutation in a patient with bicuspid aortic valve disease and intraoperative aortic dissection. Ann ThoracSurg2011;91:e70–1.
66. Arrington CB, Sower CT, Chuckwuk N, Stevens J, Leppert MF, Yetman AT, Bowles NE: Absence of TGFBR1 and TGFBR2 mutations in patients with bicuspid aortic valve and aortic dilation. Am J Cardiol 2008;102:629– 31
67. Biben C, Weber R, Kesteven S, Stanley E, McDonald L, Elliott DA, Barnett L, Köentgen F, Robb L, Feneley M, Harvey RP: Cardiac septal and valvulardysmorphogenesis in mice heterozygous for mutations in the homeobox gene Nkx2-5. Circ Res 2000;87:888–895
68. Basso C, Boschello M, Perrone C, Mecenero A, Cera A, Bicego D, Thiene G, De Dominicis E: An echocardiographic survey of primary school children for bicuspid aortic valve. Am J Cardiol 2004;93:661–3.
69. Attanasio M, Lapini I, Evangelisti L, Lucarini L, Giusti B, Porciani M, Fattori R, Anichini C, Abbate R, Gensini G, Pepe G: FBN1 mutation screening of patients with Marfansyndrome and relateddisorders: detection of 46 novel FBN1 mutations. Clin Genet 2008, 74:39–46
70. De Backer J, Loeys B, Devos D, Dietz H, De Sutter J, De Paepe A. A critical analysis of minor cardiovascular criteria in the diagnostic evaluation of patients with Marfan syndrome. Genet Med 2006;8:401–8 71. De Paepe A, Devereux RB, Dietz HC, Hennekam RC, Pyeritz RE.
Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet 1996;62:417–26
72. Rand-Hendriksen S, Tjeldhorn L, Lundby R, Semb SO, Offstad J, Andersen K, Geiran O, Paus B: Search for correlations between FBN1 genotype and complete Ghent phenotype in 44 unrelated Norwegian patients with Marfan syndrome. Am J Med Genet A 2007, 143A:1968– 1977
73. Milewicz DM, Grossfield J, Cao SN, Kielty C, Covitz W, Jewett T: A mutation in FBN1 disrupts profibrillin processing and results in isolated skeletal features of the Marfan syndrome. J Clin Invest 1995, 95:2373– 2378
74. Arbustini E, Grasso M, Ansaldi S, Malattia C, Pilotto A, Porcu E, Disabella E, Marziliano N, Pisani A, Lanzarini L, Mannarino S, Larizza D, Mosconi M, Antoniazzi E, Zoia MC, Meloni G, Magrassi L, Brega A, Bedeschi MF, Torrente I, Mari F, Tavazzi L: Identification of sixty-twonovel and twelveknown FBN1 mutations in eighty-oneunrelatedprobands with Marfansyndrome and otherfibrillinopathies. Hum Mutat 2005, 26:494 75. Van Dijk FS, Hamel BC, Hilhorst-Hofstee Y, Mulder BJ, Timmermans J,
76. Buoni S, Zannolli R, Macucci F, Ansaldi S, Grasso M, Arbustini E, Fois A: The FBN1 (R2726W) mutation is not fully penetrant.Ann Hum Genet 2004, 68:633–638
77. Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Jr FDP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B: ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to develop guidelines for the management of patients with valvular heart disease). J Am Coll Cardiol 2006, 48:e1–e148
78. Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A: Guidelines on the management of valvular heart disease: the task force on the management of valvular heart disease of the European society of cardiology. Eur Heart J 2007, 28:230–268
79. Della Corte A, Bancone C, Dialetto G, Covino FE, Manduca S, Montibello MV, De Feo M, Buonocore M, Nappi G. The ascending aorta with bicuspid aortic valve: aphenotypic classification with potential prognostic significance. Eur J CardiothoracSurg 2014 Jan 14
80. Lemaire SA, McDonald ML, Guo DC, Russell L, Miller CC 3rd, Johnson RJ, Bekheirnia MR, Franco LM, Nguyen M, Pyeritz RE, Bavaria JE, Devereux R, Maslen C, Holmes KW, Eagle K, Body SC, Seidman C, Seidman JG, Isselbacher EM, Bray M, Coselli JS, Estrera AL, Safi HJ, Belmont JW, Leal SM, Milewicz DM: Genome-wide association study identifies a susceptibility locus for thoracic aortic aneurysms and aortic dissections spanning FBN1 at 15q21.1. Nat Genet 2011, 43:996–1000 81. Folkersen L, Wågsäter D, Paloschi V, Jackson V, Petrini J, Kurtovic
S, Maleki S, Eriksson MJ, Caidahl K, Hamsten A, Michel JB, Liska J, Gabrielsen A, Franco-Cereceda A, Eriksson P: Unraveling divergent gene expression profiles in bicuspid and tricuspid aortic valve patients with thoracic aortic dilatation: the ASAP study. Mol Med 2011, 17:1365–1373 82. El-Hamamsy I, Yacoub MH: A measured approach to managing the aortic
root in patients with bicuspid aortic valve disease. CurrCardiol Rep 2009, 11:94–100
83. Détaint D, Faivre L, Collod-Beroud G, Child AH, Loeys BL, Binquet C, Gautier E,Arbustini E, Mayer K, Arslan-Kirchner M, Stheneur C, Halliday D, BeroudC,Bonithon-Kopp C, Claustres M, Plauchu H, Robinson PN, Kiotsekoglou A, DeBacker J, Adès L, Francke U, De Paepe A, Boileau C, Jondeau G: Cardiovascularmanifestations in men and women carrying a FBN1 mutation. Eur Heart J2010, 31:2223–2229
84. Fernández B, Durán AC, Fernández-Gallego T, Fernández MC, Such M, Arqué JM,Sans-Coma V. Bicuspid aortic valves with different spatial
orientations of the leaflets are distinct etiological entities. J Am Coll Cardiol 2009 Dec 8;54(24):2312-8
85. LadouceurMFermanian C, Lupoglazoff J-M, Edouard T, Dulac Y, Acar P, Magnier S, Jondeau G. Effect of beta-blockade on ascending aortic dilatation in Children with the Marfan syndrome. Am J Cardiol 2007;99:406-409
86. Vaidyanathan B. Role of beta-blockers in Marfan’s syndrome and bicuspid aortic valve: A time for re-appraisal. Ann Pediatr Card 2008;1:149-52 87. Jondeau G, Detaint D, Tubach F, Arnoult F, Milleron O, Raoux F, Delorme
G, Mimoun L, Krapf L, Hamroun D, Beroud C, Roy C, Vahanian A, Boileau C. Aortic event rate in the Marfan population: a cohort study. Circulation 2012 Jan 17;125(2):226-32
88. Habashi JP, Judge DP, Holm TM, Cohn RD, Loeys BL, Cooper TK, Myers L, Klein EC, Liu G, Calvi C, Podowski M, Neptune ER, Halushka MK, Bedja D, Gabrielson K, Rifkin DB, Carta L, Ramirez F, Huso DL, Dietz HC. Losartan, an AT1 antagonist, prevents aortic aneurysm in a mouse model of Marfan syndrome. Science 2006 Apr 7;312(5770):117-21
89. Ahimastos AA, Aggarwal A, D’Orsa KM, Formosa MF, White AJ, Savarirayan R, Dart AM, Kingwell BA. Effect of perindopril on large artery stiffness and aortic root diameter in patients with Marfan syndrome: a randomized controlled trial. JAMA 2007 Oct 3;298(13):1539-47 90. Brooke BS, Habashi JP, Judge DP, Patel N, Loeys B, Dietz HC 3rd.
Angiotensin II blockade and aortic-root dilation in Marfan’s syndrome. N Engl J Med. 2008 Jun 26;358(26):2787-95
91. Mueller GC, Stierle L, Stark V, Steiner K, von Kodolitsch Y, Weil J, Mir TS:Retrospective analysis of the effect of angiotensin II receptor blocker versus β-blocker on aortic root growth in paediatric patients with Marfan syndrome. Heart 2014;100:214-218
92. Groenink M, den Hartog AW, Franken R, Radonic T, de Waard V, Timmermans J, Scholte AJ, van den Berg MP, Spijkerboer AM, Marquering HA, Zwinderman AH, Mulder BJ. Losartan reduces aortic dilatation rate in adults with Marfan syndrome: a randomized controlled trial. Eur Heart J 2013 Dec;34(45):3491-500
93. Barrett PM, Topol EJ. The fibrillin-1 gene: unlocking new therapeutic pathways in cardiovascular disease. Heart 2013 Jan;99(2):83-90 94. Schaefer BM, Lewin MB, Stout KK, Gill E, Prueitt A, Byers PH, Otto CM.
The bicuspid aortic valve: an integrated phenotypic classification of leaflet morphology and aortic root shape. Heart 2008;94:1634–8
95. Park CB, Greason KL, Suri RM, Michelena HI, Schaff HV, Sundt TM III. Fate of nonreplaced sinuses of Valsalva in bicuspid aortic valve disease. J ThoracCardiovascSurg 2011;142:278–84
96. Della Corte A, Romano G, Tizzano F, Amarelli C, De Santo LS, De Feo, Scardone M, Dialetto G, Covino FE, Cotrufo M. Echocardiographic anatomy of ascending aorta dilatation: correlations with aortic valve morphology and function. Int J Cardiol 2006;113: 320–6
Ectopic calcification and bone: a comparison
of the effect of dietary carbohydrates, sugars
and protein
Rachel Nicoll BSc MA
1, John McLaren Howard PhD
2and Michael Y Henein MD PhD
11 Department of Public Health and Clinical Medicine and Heart Centre Umea University, Umea, Sweden
2 Acumen Lab, Tiverton, Devon, UK