Infancy
0
–1
1
ANCY • 0
–
INFANCY
T
he first year of life is marked by dramaticchanges in the amount and type of phys-ical activity displayed. Infants spend the first days of life sleeping and eating. However, 1 year later, when they become toddlers, they usually are crawling and probably have taken a few independent steps.
Motor skill development begins with the invol-untary reflexes that ensure the newborn infant’s survival. Over the next few months, these reflexes disappear as the infant slowly gains voluntary con-trol over body movements. With increasing concon-trol comes more physical activity. Sitting up, rolling over, crawling, standing, and eventually walking expand the infant’s level of physical activity.
Motor skill development, like other aspects of the infant’s development, is an individual process. Infants usually acquire motor skills in the same order, but the rate at which they acquire them is individual. For example, some infants walk as early as 9 months, whereas others do not walk until after their first birthday.
The way infants are held and handled, the toys they play with, and their environment all influence their motor skill development. Parents can influ-ence the quality of the infant’s movements by pro-viding a stimulating environment. Physical activity should be promoted from the time infants are born. Motor skills do not just appear. Motor skills, like cognitive skills, flourish when the infant is exposed to a stimulating environment. Physical activity opportunities and nurturing of motor skill develop-ment during the first year of life establish the foun-dation for physical activity behaviors.
Growth and Physical
Development
Immediately after birth, infants lose approxi-mately 6 percent of their body weight because of fluid loss and some breakdown of tissue. Infants usually regain their birthweight by 10 to 14 days after birth, and thereafter weight gain proceeds at a slower rate. Typically, infants’ birthweight doubles by 4 to 6 months and triples by age 1. On average, infants gain 5 to 7 oz per week in the first 4 to 6 months and 3 to 5 oz per week from 6 to 18 months. Infants usually increase in length by 50 percent in the first year, but the rate of increase slows down during the second half of the year. From birth to 6 months, infants gain approximately 1 inch per month, and from 6 to 12 months of age,
they gain about a 1/2inch per month.
These enormous changes make it difficult for infants to control their rapidly growing bodies. In addition, the head and trunk constitute about 70 percent of infants’ body length and most of its mass, making it difficult for them to achieve upright postures or any form of locomotion. How-ever, this large mass offers infants weight-training opportunities. As infants roll over, crawl to get a favorite toy, or walk along furniture, their head and trunk may be difficult to control, but they benefit from the physical challenge by increasing motor control and muscle development.
Muscles are not well developed at birth; there-fore, most of the first year of life involves building muscle mass. Infants need arm muscles to pick up objects. They need leg muscles to crawl, stand, and
–
eventually walk. They need their head and trunk muscles to control these two large body parts. And they need arm and leg muscles to move their trunks.
Neural development in infants involves the connection of 200 billion neurons, the conducting cells of the nervous system. Stimulation is critical to neural development. Without stimulation (e.g., visual, auditory, tactile), these cells die. With stimu-lation, these cells create elaborate networks that promote sensory and motor skill development. Stimulation can be provided in many ways (e.g., by hanging a mobile over the infant’s crib, which may motivate the infant to reach, or by placing a toy just out of reach, which may motivate the infant to roll over).
Healthy Lifestyles
Infants’ vitality and successful development depend on good nutrition during the first year of
life. Full-term infants who are fed on demand usual-ly consume the amount they need to grow well. But feeding infants is much more complex than simply offering food when they are hungry, and it serves purposes far beyond supporting their physical growth. Feeding provides opportunities for emo-tional bonding between the parent and infant. Infants improve their hand-eye coordination and fine motor skills as they begin to feed themselves.
In addition to interaction during feeding times, infants need play time to explore objects, engage in activities that stimulate their senses, and experience movement and action.
Building Partnerships
Partnerships among health professionals, fami-lies, and communities are essential for ensuring that families receive guidance on physical activity during infancy. Health professionals can have a tremendous
impact on decisions about physi-cal activity as they inform families about the importance of physical activity for motor skill develop-ment. They provide an opportuni-ty for families to discuss, reflect on, and decide which options best suit their circumstances. Health professionals also identify and contact community resources that help families.
The community may also need to help families by provid-ing programs that
• Encourage families to promote physical activity in infants.
INF
ANCY • 0
–
• Teach families about physical and motor skill development during infancy.
• Give infants the opportunity to be physically active.
In addition, communities can provide (1) afford-able, skilled child care providers who promote physi-cal activity in infants, (2) safe environments for indoor and outdoor physical activity, and (3) sup-port for families of infants with special health care needs.
Strengths, and Issues and
Concerns
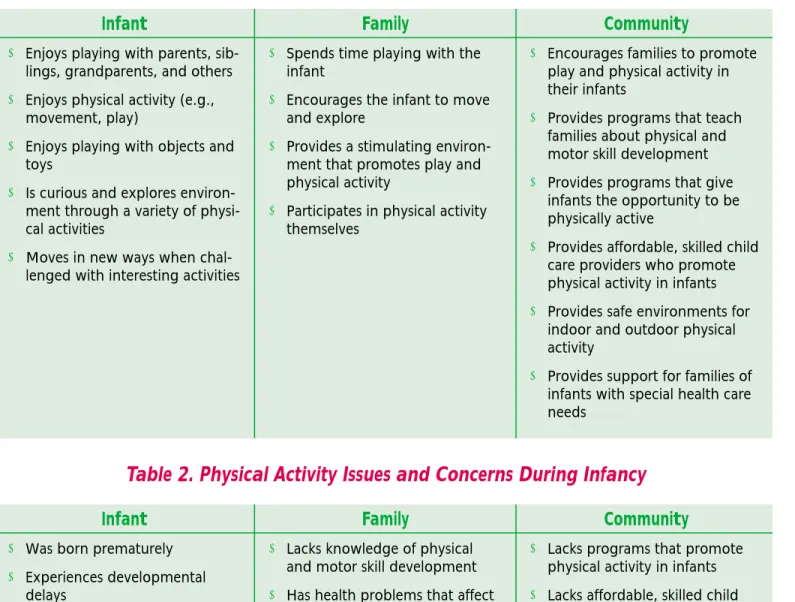
During health supervision visits, health profes-sionals should emphasize the physical activity strengths of the infant, family, and community (Table 1) and address any physical activity issues and concerns (Table 2).
–
INF
ANCY • 0
–
11 MONTHS
Infant
■ Enjoys playing with parents,
sib-lings, grandparents, and others
■ Enjoys physical activity (e.g.,
movement, play)
■ Enjoys playing with objects and
toys
■ Is curious and explores
environ-ment through a variety of physi-cal activities
■ Moves in new ways when
chal-lenged with interesting activities
Family
■ Spends time playing with the
infant
■ Encourages the infant to move
and explore
■ Provides a stimulating
environ-ment that promotes play and physical activity
■ Participates in physical activity
themselves
Community
■ Encourages families to promote
play and physical activity in their infants
■ Provides programs that teach
families about physical and motor skill development
■ Provides programs that give
infants the opportunity to be physically active
■ Provides affordable, skilled child
care providers who promote physical activity in infants
■ Provides safe environments for
indoor and outdoor physical activity
■ Provides support for families of
infants with special health care needs
Table 1. Physical Activity Strengths During Infancy
Table 2. Physical Activity Issues and Concerns During Infancy
Infant
■ Was born prematurely ■ Experiences developmental
delays
■ Experiences discomfort with
physical activity
■ Has health problems
Family
■ Lacks knowledge of physical
and motor skill development
■ Has health problems that affect
the amount of time spent with the infant
■ Has a work schedule or other
commitments that reduce the amount of time spent with the infant
Community
■ Lacks programs that promote
physical activity in infants
■ Lacks affordable, skilled child
care providers who promote physical activity in infants
■ Does not provide support for
families of infants with special health care needs
An infant’s level of physical activity should be assessed as part of health supervision visits. (For more information on health supervision, see Bright
Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents, listed under Suggested
Reading in this chapter.)
Health professionals can begin by gathering information about the infant’s level of physical activity. This can be accomplished by selectively asking key interview questions listed in this chap-ter, which provide a useful starting point for identi-fying physical activity issues and concerns.
Health professionals can then use this chapter’s screening and assessment guidelines, and counsel-ing guidelines, to provide families with anticipatory guidance. Interview questions, screening and assess-ment, and counseling should be used as appropriate and will vary from visit to visit, infant to infant, and family to family.
Desired outcomes for the infant, and the role of the family, are identified to assist health profession-als in promoting physical activity.
Interview Questions
The following questions are intended to be used selectively to gather information, to address the family’s issues and concerns, and to build partnerships.
Do you have any concerns about Julia’s development?
How often do you play with her? Do both you and your spouse play with
Alexander?
What are some physical activities you do with him?
How often during the day is Julia in an open environment, such as on the living room floor? How do you carry her?
Is Alexander distressed when you gently bounce him or swing him around?
Is he interested in his environment? What are his favorite toys? Do toys motivate him to move?
INFANCY PHYSICAL ACTIVITY SUPERVISION
–
Is Julia interested in objects, toys, and people around her?
What are some of her achievements?
Are you comfortable with Alexander’s increasing independence? Do you encourage him to be independent?
Are you pleased he can stand by himself? Are you worried that he might hurt himself?
When Alexander is awake, how much time does he spend in an infant safety seat or swing, on the floor, on your lap, or in someone’s arms? How does Julia’s development compare to that of
your other children when they were this age? Do you have any questions?
Screening and Assessment
■ Measure the infant’s length, weight, and head
circumference, and plot these on a standard growth chart (see Tool H: CDC Growth Charts). Deviation from the expected growth pattern (e.g., a major change in growth percentiles on the chart) should be evaluated. This may be normal or may indicate a problem (e.g., difficulties with eating).
■ Examine the infant for other medical problems
that may interfere with motor skill development.
■ Determine whether the infant has a history of ear
infections.
■ Determine whether the infant has a heart
murmur.
■ Assess the symmetry of the infant’s arms and
legs.
■ Assess the infant’s muscle tone in the arms and
legs (i.e., resistance to joint extension).
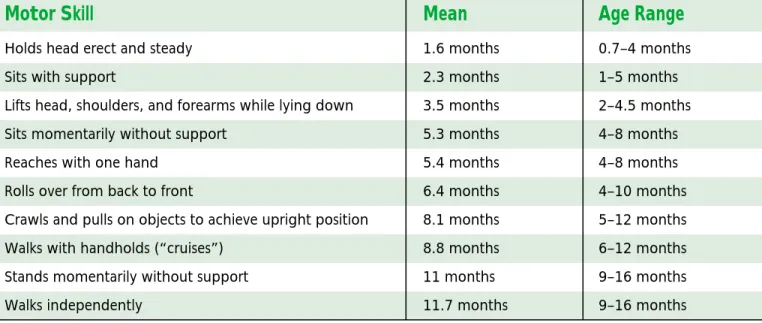
■ Assess the infant’s motor skill development. The
Bayley Scales of Infant Development are often
used for this purpose (Table 3).1
Counseling
Health professionals can use the following information to provide anticipatory guidance to families. Anticipatory guidance provides informa-tion on the infant’s physical status and on what to expect as the infant enters the next developmental period, and fosters the promotion of physical activity.
General
■ Encourage parents to attend classes to learn
about promoting physical activity during infan-cy. Suggest that they participate in parent-infant play groups.
■ Infants need the opportunity to move. Encourage
parents to provide objects and toys and to play games to encourage their infants to move and do things for themselves.
■ Gently turning, rolling, bouncing, and swaying
infants are excellent ways to increase their mus-cle strength and to help them develop important connections between the brain and muscles.
■ Tell parents that rough-and-tumble activities are
not appropriate for infants. Infants usually signal their distress (e.g., by crying) if the physical activ-ity is too vigorous, overwhelming, or disconcert-ing. Parents should pay attention to these signals and stop the physical activity if needed.
INF
ANCY • 0
–
■ Encourage parents to ask the child care provider how much time the infant spends moving around (i.e., not sitting in an infant safety seat or sleeping).
Physical Development
■ Infants need physical activity from the time they
are born. Encourage parents to nurture their infants’ motor skill development and to promote physical activity.
■ Infants need to develop head and trunk control.
When infants are 3 months old, parents can encourage this control by (1) placing the infant on their laps, facing them; (2) holding the infant’s hands and encouraging the infant to stand; and (3) pulling the infant up into a stand-ing position. When the infant is pulled up, the
infant should stand with the parent’s support. If the infant can hold the upright posture, the par-ent can gpar-ently sway the infant side to side.
Safety
■ Infants need a safe environment for physical
activity.
–
11 MONTHS
Table 3. Motor Skill Development During Infancy
Mean
1.6 months 2.3 months 3.5 months 5.3 months 5.4 months 6.4 months 8.1 months 8.8 months 11 months 11.7 monthsMotor Skill
Holds head erect and steady Sits with support
Lifts head, shoulders, and forearms while lying down Sits momentarily without support
Reaches with one hand Rolls over from back to front
Crawls and pulls on objects to achieve upright position Walks with handholds (“cruises”)
Stands momentarily without support Walks independently
Age Range
0.7–4 months 1–5 months 2–4.5 months 4–8 months 4–8 months 4–10 months 5–12 months 6–12 months 9–16 months 9–16 monthsEducational/Attitudinal
■ Enjoys moving
■ Enjoys playing with parents,
sib-lings, grandparents, and others
Behavioral
■ Achieves motor skills milestones
at an appropriate age
■ Plays with objects and toys and
explores the environment
Health/Physical Status
■ Develops the strength and
pos-tural control to walk
■ Develops the fine motor skills
needed to pick up objects, toys, and food and manipulate them with both hands
Educational/Attitudinal
■ Understands the importance of
physical activity (e.g., move-ment, play)
■ Recognizes developmentally
appropriate motor skills
Behavioral
■ Plays with the infant
■ Promotes physical activity in the
infant
Health/Physical Status
■ Recognizes delays in motor skill
development
Infant
Family
INF
ANCY • 0
–
–
11 MONTHS
References
1. Bayley N. 1969. Manual for the Bayley Scales of Infant
Development. New York, NY: The Psychological Corp.
Suggested Reading
American Academy of Pediatrics, Committee on Injury and Poison Prevention. 1995. Injuries associated with infant walkers. Pediatrics 95(5):778–780.
American Academy of Pediatrics, Committee on Sports Medicine and Fitness and Committee on Injury and Poison Prevention. 2000. Swimming programs for infants and toddlers. Pediatrics 105(4):868–870. Association of State and Territorial Directors of Health
Promotion and Public Health Education. 1997. How
to Promote Physical Activity in Your Community (2nd
ed.). Washington, DC: Association of State and Terri-torial Directors of Health Promotion and Public Health Education.
Bly L. 1994. Motor Skills Acquisition in the First Year. New York, NY: Academic Press.
Bornstein M, Lamb ME. 1992. Development in Infancy: An
Introduction. New York, NY: McGraw-Hill.
Clark JE. 1994. Motor development. In Ramachandran VS, ed., Encyclopedia of Human Behavior (pp. 245–255). San Diego, CA: Academic Press.
Field T. 1990. Infancy. Cambridge, MA: Harvard Universi-ty Press.
Green M, Palfrey JS, eds. 2000. Bright Futures: Guidelines
for Health Supervision of Infants, Children, and Adoles-cents (2nd ed.). Arlington, VA: National Center for
Education in Maternal and Child Health.
Haywood KM. 1993. Life Span Motor Development (2nd ed.). Champaign, IL: Human Kinetics.
Shumway-Cook A, Woollacott M. 1995. Motor Control:
Theory and Practical Applications. Baltimore, MD:
Williams and Wilkins.
U.S. Department of Health and Human Services; U.S. Department of Education. 2000. Promoting Better
Health for Young People Through Physical Activity and Sports: A Report to the President from the Secretary of Health and Human Services and the Secretary of Educa-tion. Atlanta, GA: U.S. Department of Health and
I’m Afraid Natalie Might Break!
N
atalie is Susan andJacob’s first baby. They are the first among their friends to have a baby. They have no family members living nearby. Susan brings Natalie in to see Dr. Fuentes for her 6-month health supervision visit, and the physi-cian notices that Susan handles Natalie like a china doll. Natalie exhibits very little head and trunk control. When placed on her stomach, she fusses and raises her head only to see what’s in front of her. When a toy is placed in front of her, Natalie looks at the toy but doesn’t reach for it. Dr. Fuentes determines that Natalie’s height and weight are normal. She is alert and happy. However, her motor skill devel-opment is lagging—most notice-ably in head and trunk control.
Dr. Fuentes asks Susan how she and Jacob interact with Natalie. Susan admits that she and Jacob are not very sure of themselves when it comes to holding and playing with Natalie. Susan discloses that she is afraid Natalie might “break” if she lets her move around too much. In
fact, Natalie spends most of the day in her infant seat or crib.
Dr. Fuentes asks Susan to show her how she carries, undresses, and bathes Natalie. The demonstrations confirm that Susan is gentle and extremely careful—so much so that Natalie remains passive. With as much gentleness as Susan exhibited, Dr. Fuentes picks up Natalie. Howev-er, Dr. Fuentes encourages Natalie to sit while he holds her firmly under the arms. Dr. Fuentes care-fully moves Natalie from side to side to show Susan how she can move Natalie without hurting her.
The secret, Dr. Fuentes says, is to encourage Natalie to move independently. “Natalie’s head and trunk are almost two-thirds of her weight, and she has to learn to control them. You and Jacob need to give Natalie oppor-tunities to strengthen her mus-cles and her brain’s connections to the muscles, while offering support if she needs it. Tonight, spend some time with Natalie sit-ting on your lap facing you; hold her gently but firmly, and let her
sway back and forth and side to side. Make it a game. Talk to her and encourage her. As long as you are gentle but hold her firm-ly, she won’t break.”
INF
ANCY • 0
–
FREQUENTLY ASKED QUESTIONS
ABOUT PHYSICAL ACTIVITY IN INFANCY
■ How can I encourage my baby to be
physi-cally active?
Babies need physical activity from the time they are born. Provide your baby with opportunities that encourage her to move. Offer her a chal-lenge (for example, a toy just out of reach) and see how she reacts. She will let you know if you push her too much. When babies move, their arms and legs often look jerky and uncoordinat-ed. Remember, your baby is learning a lot of new skills in her first year. When a baby’s brain and muscles learn how to work together, her move-ments will get smoother.
■ What’s the best way to carry my baby?
Carry your baby in a way that makes him feel secure and comfortable. Try to vary the position. For example, instead of always carrying your baby so that he faces backward, carry him so that he faces forward, to give him the opportunity to look in the direction you are going.
■ Should I use a walker to help my baby
learn to walk?
Babies should never be placed in an infant walker (baby walker) because of the considerable risk of injury and even death. The risk of injury from the use of walkers is even greater in homes with stairs. Make sure your child care provider does not use walkers.
■ My baby’s head flops over to the side
when she is upright. Should I support her head?
Yes, offer light but firm support. Try to offer less support each time, so that eventually she will be able control her head herself.
■ My friend’s baby, who is the same age as
mine, is sitting on his own, but my baby can’t do this yet. Should I be worried?
Babies develop at different rates. As long as your baby attains motor skills at an appropriate age, there is nothing to worry about.
■ What can I expect my baby to do as he
grows?
Newborn to 1 Month
Your baby will have rooting, sucking, and swal-lowing reflexes.
He will begin to develop the ability to start and stop sucking.
He will wake up and fall asleep easily.
3 to 4 Months
Your baby will raise her head when she is on her stomach.
She will follow objects and sounds with her eyes. She will put her hand in her mouth a lot.
She will sit with support.
–
INF
ANCY • 0
–
11 MONTHS
6 Months
Your baby’s torso will move in the direction of his head when he turns his head while lying on his back.
He will reach for objects and pick them up with one hand.
He will hold his hands together. He will sit with support.
7 to 9 Months
Your baby will reach for pieces of food and pick them up between her thumb and forefinger.
9 to 12 Months
Your baby will play games such as peek-a-boo. He will explore toys with his eyes and mouth, and will transfer a toy from one hand to the other.
He will sit and crawl, and may walk without support.
Resources for Families
See Tool F: Physical Activity Resources for con-tact information on national organizations that can provide information on physical activity. State and local departments of public health and education and local libraries are additional sources of information.
Bressler KW, Parker D. 2000. Yoga Baby: Exercises to Help
You Bond with Your Baby Physically, Emotionally, and Spiritually. New York, NY: Broadway Books.
Clements RL, Lee M. 1998. Parent’s Guide to Physical Play. New York, NY: American Association for the Child’s Right to Play.
Cooper KH. 1999. Fit Kids! The Complete Shape-Up Program
for Birth Through High School. Nashville, TN:
Broad-man and HolBroad-man Publishers.
Eliot L. 1999. What’s Going On in There? How the Brain and
Mind Develop in the First Five Years of Life. New York,
NY: Bantam Books.
Fox S. 1999. Baby Steps: Exercises for Baby’s First Year of
Life. New York, NY: Berkley Publishing Group.
Meltzoff AN, Gopnik AM, Kuhl PK. 1999. The Scientist in
the Crib: Minds, Brains and How Children Learn. New
York, NY: Morrow/Avon.
Segal M. 1998. Your Child at Play: Birth to One Year. New York, NY: New Market Press.