Sports Participation in Youth With Inflammatory Bowel Diseases:
The Role of Disease Activity and Subjective Physical Health
Symptoms
Rachel Neff Greenley, PhD,
*
Jessica P. Naftaly, MS,
*
Rachel J. Walker, MS,
*
Michael D. Kappelman, MD, MPH,
†Christopher F. Martin, MSPH,
†and Kristin L. Schneider, PhD
*
Background: Physical activity is important for youth with inflammatory bowel diseases (IBD), and sports participation is a common way in which youth are physically active. Yet, studies examining sports participation in youth with IBD and barriers to sports participation are lacking. This study examined the role of disease complications, body mass index (BMI), subjective physical health, and psychosocial functioning in influ-encing sports participation in a large sample of youth with IBD participating in the Crohn’s and Colitis Foundation of America Partners (CCFA Partners) Kids and Teens Registry.
Methods: CCFA Partners Kids and Teens is an internet-based cohort study in which participants and their parents self-report demographics, disease characteristics, anthropometrics, and validated assessments of physical health, psychosocial functioning, and perceived impairment in sports participation. We performed a cross-sectional analysis of 450 cohort participants, age 12–17 years.
Results: Nearly two-thirds of the sample reported that their IBD resulted in some impairment in sports participation. IBD disease activity was associated with perceived impairment in sports participation. In a forward regression analysis controlling for disease activity, fatigue, pain, and past IBD-related surgery emerged as the most salient correlates of impairment in sports participation.
Conclusions: Disease activity and subjective physical health symptoms were the most salient correlates of impairment in sports participation. Whether these barriers interfere with physical activity more generally deserves further study, as does replication of these findings longitudinally. Ultimately, a greater understanding of potential barriers to sports participation may be useful for generating targeted physical activity recom-mendations for youth with IBD.
Key Words: inflammatory bowel diseases, physical activity, sports participation
INTRODUCTION
Adequate physical activity is important for youth gen-erally,1 but particularly so for youth with inflammatory bowel disease (IBD) because those with IBD are at risk for develop-ing osteoporosis and because comorbid obesity increases the risk of IBD complications.2 Experts recommend that youth with IBD meet the physical activity recommendations for all youth, if possible,3 yet the few existing studies examining levels of physical activity in pediatric samples indicate that youth with IBD are less physically active than matched con-trols.4 Participation in sports is a particularly relevant area of
physical activity for youth. Nearly 60% of youth participate in organized sports,5 and the benefits of sports participation extend beyond just physical fitness. Youth who participate in sports report better psychosocial adjustment and higher life satisfaction, and participation in sports may protect youth from engagement in health-compromising behaviors (eg, substance use).6, 7 For youth with IBD, additional benefits of physical activity may include reduced disease activity.8 Yet, preliminary data suggest that roughly half of youth with IBD perceive their disease to cause at least occasional interference with participation in sports.9
Given the importance of physical activity for youth with IBD, the fact that their levels of physical activity are lower than healthy controls warrants further research attention. Specifically, an in-depth examination of the role of IBD dis-ease activity and complications (ie, presence of ostomy/pouch, past IBD-related surgeries), body mass index (BMI), subjec-tive physical health symptoms (ie, pain, fatigue), and psycho-social functioning (ie, anxiety and depressive symptoms) in a large patient group may identify youth at risk for suboptimal levels of physical activity. Research suggests that all of the aforementioned factors are associated with physical activity in either adult IBD samples4, 10, 11 or within the general population of adults.12 Additionally, in a small study of adolescents with
Received for publication July 6, 2017; Editorial Decision August 21, 2017 From the *Rosalind Franklin University of Medicine and Science, †University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
Conflicts of interest: Dr. Kappelman has been a consultant to the Crohn’s and Colitis Foundation.
Supported by: Crohn’s and Colitis Foundation.
Address correspondence to: Rachel Greenley, PhD, Department of Psychology, Rosalind Franklin University of Medicine and Science, 3333 Green Bay Road, North Chicago, IL 60064-3095 ([email protected]).
For permissions, please e-mail: [email protected].
IBD, disease complications and poorer psychological func-tioning were associated with greater perceived sports impair-ment.9 Identification of key risk factors for low levels of physical activity can inform the development of interventions to enhance physical activity in youth with IBD. Attention to increasing physical activity in youth is particularly important given that health promotion behaviors are still malleable during this period. Setting the stage for good habits related to physical activity during childhood can serve as the basis for the estab-lishment of healthy patterns of physical activity into young adulthood and beyond.13
The current study aimed to extend our understanding of risk factors for impairment in sports participation in a large, geographically diverse sample of pediatric patients with IBD from the Crohn’s and Colitis Foundation of America Partners (CCFA Partners) Study. Specific aims included: (1) to summa-rize levels of perceived impairment in sports participation; (2) to identify bivariate relationships between perceived impair-ment in sports participation and select variables, including disease complications (ie, presence of ostomy/pouch, past IBD-related surgeries), BMI, subjective physical health symptoms (ie, pain, fatigue), and psychosocial functioning (ie, anxiety symptoms, depression symptoms); and (3) to evaluate the most salient correlates of impairment in sports participation within and across the aforementioned domains, after accounting for relevant covariates. Selection of correlates for examination was informed by the existing IBD literature.4, 9–11
MATERIALS AND METHODS
Participants and Procedures
CCFA Partners Kids and Teens Registry is an inter-net-based cohort developed to study the natural history of pedi-atric IBD focusing on patient/family-reported exposures, health behaviors, and outcomes. Participants were recruited through the Crohn’s and Colitis Foundation (CCF) email roster, the foundation’s website, and social media outlets, at local educa-tion and fundraising events, at clinic visits, and through other dissemination channels.14 Parents/guardians provided online consent and youth provided online assent at study enrollment. Inclusion criteria for participation in the CCFA Partners Kids and Teens Registry were (1) age younger than 18 years at time of enrollment; (2) diagnosis of Crohn’s disease, ulcerative col-itis, or indeterminate colitis; and (3) a parent/guardian willing to participate. Study data were managed by the University of North Carolina (UNC) at Chapel Hill.
For this study, we performed a cross-sectional analysis of baseline data collected between August 2013 and April 2014. Additional inclusion criteria utilized for this analysis were (1) youth age 12–17 years at the time of completion of baseline survey and (2) no endorsement of another health condition unrelated to IBD that, based on parent report, greatly affected the youth’s “diet, exercise, digestion, lifestyle,
or mental health over the past month.” The latter criterion was implemented to reduce the likelihood that issues unre-lated to IBD could influence ratings of perceived impairment in sports participation.
Measures
Demographics
Parents/guardians provided answers to basic demo-graphic questions, including youth race, ethnicity, age at study enrollment, age at IBD diagnosis, and sex. The 2 ethnicity and race variables were recoded into a single dichotomized varia-ble of 0 (Non-Hispanic white) or 1 (Hispanic and/or nonwhite) because of the limited variability in participants who identified as Hispanic and/or nonwhite.
Disease activity
Disease activity was assessed via the youth completion of the Manitoba IBD Index (MIBDI).15 This measure of dis-ease activity was utilized to have a single measure applicable to all patients. The MIBDI is a single-item, self-report measure of disease activity in which the respondent endorses 1 of the following 6 responses to the statement: “In the past 6 months my disease activity has been”: 1 (constantly active, giving me symptoms every day); 2 (often active, giving my symptoms most days); 3 (sometimes active, giving me symptoms on some days, for instance, 1–2 days per week); 4 (occasionally active, giving me symptoms 1–2 days per month); 5 (rarely active, giv-ing me symptoms on a few days in the past 6 months); and 6 (I was well in the past 6 months, what I consider a remission or absence of symptoms).15 The MIBDI correlates highly with other disease activity measures including the Inflammatory Bowel Disease Questionnaire and the Harvey-Bradshaw Index, and it has been documented to have good test-retest reliability (r = 0.81).15
Presence of pouch or ostomy
Parents indicated whether the participating youth had an ostomy or a pouch via 2 separate questions. Given the low fre-quency of positive responses to either question, the questions were combined for analyses, and responses were coded as 0 (no ostomy or pouch) or 1 (ostomy or pouch present).
Surgical history
IBD-related surgical history was assessed via a single parent-reported question: “Have you ever had surgery for your IBD?” Responses were coded as 0 (negative history of IBD-related surgery) or 1 (positive history of IBD-IBD-related surgery).
BMI
accordance with Centers for Disease Control and Prevention guidelines.16.
Fatigue
Fatigue was measured via self-report using the following 4 items from the pediatric PROMIS item bank: “In the past 7 days”: “I got tired easily,” “Being tired made it hard for me to play or go out with my friends as much as I’d like,” “I felt weak,” and “I had trouble finishing things because I was too tired” on a scale of 0 (never) to 4 (almost always). Higher scores indicated greater fatigue. Internal consistency was high for the current sample (α = 0.92).
Pain
Pain was measured via self-report using the following 4 items from the pediatric PROMIS item bank: “In the past 7 days”: “I had trouble sleeping when I had pain,” “It was hard for me to pay attention when I had pain,” “It was hard for me to run when I had pain,” and “It was hard for me to have fun when I had pain” on a scale of 0 (never) to 4 (almost always). Higher scores reflected more pain. Internal consistency was high in the current sample (α = 0.94).
Depressive symptoms
Depressive symptoms were self-reported using the fol-lowing 4 items from the pediatric PROMIS item bank: “In the past 7 days”: “I thought that my life was bad,” “I felt lonely,” “I felt sad,” and “I felt like everything in my life went wrong” on a scale of 0 (never) to 4 (almost always). Higher scores reflected more depression symptoms. Internal consistency was high in the present sample (α = 0.92).
Anxiety symptoms
Anxiety symptoms were self-reported using the following 4 items from the pediatric PROMIS item bank: “In the past 7 days…” “I felt like something awful might happen,” “I was afraid that I would make mistakes,” “I felt worried,” and “I felt nervous” on a scale of 0 (never) to 4 (almost always). Higher scores reflected more anxiety symptoms. Internal consistency was high for the present sample (α = 0.91).
Perceived impairment in sports participation
Perceived impairment in sports participation was assessed via a single item from the IMPACT-35, which is an IBD-specific health-related quality of life measure.17 Youth responded to the following question: “Does your IBD get in the way of playing sports the way you would like to?” Scores ranged from 1 (always) to 5 (never), with higher scores indicating greater perceived impairment in sports participation. Internal consistency for the IMPACT-35 was high (α = 0.95) for the current sample, and this item evidenced adequate variability in assessing perceived impair-ment in sports participation in a previous pediatric IBD study.9
Data Analysis
Preliminary analyses were conducted to examine distribu-tional characteristics of independent and dependent variables and to summarize sample demographics. Data transformations were employed as needed to address non-normal distributions. Bivariate correlations of perceived impairment in sports par-ticipation with disease complications (ie, presence of ostomy/ pouch, past IBD-related surgeries), BMI z-score, subjective physical health symptoms (ie, self-reported pain, self-reported fatigue), and psychosocial functioning (ie, anxiety symptoms, depression symptoms) were conducted. In addition, multiple regression analysis was used to determine the most salient cor-relates of perceived impairment in sports participation from the group of aforementioned factors. Before conducting the multi-ple regression analysis, we examined correlations between per-ceived impairment in sports participation and 3 demographic or disease factors (race/ethnicity, age at IBD diagnosis, and dis-ease activity) to evaluate whether any of these variables should be included as covariates in regression analyses. Covariates sig-nificantly correlated with perceived impairment in sports par-ticipation at the bivariate level were included in the first step of the multiple regression. Forward selection was used on the second step of the analysis to examine which of the following variables were the most salient predictors of perceived impair-ment in sports participation: disease complications (ie, presence of ostomy/pouch, past IBD-related surgeries), BMI z-score, subjective physical health symptoms (ie, pain, fatigue), and psy-chosocial functioning (ie, anxiety symptoms, depression symp-toms). Analyses were performed using IBM SPSS version 24. Semipartial r2 were interpreted as indices of effect size, using
0.01 as a small effect size, 0.09 as a medium effect size, and 0.35 as a large effect size.18
Power analysis
We conducted a post hoc power analysis to ensure that our sample of 450 had adequate power to detect significant effects. We based our power analysis on findings from a small study of youth with IBD, which documented bivariate asso-ciations between perceived impairment in sports participa-tion, and sex, age, disease complications, subjective physical health symptoms, and psychosocial functioning ranging from
r = 0.45 to r = 0.72.9 We conservatively estimated an effect size of r = 0.45 for our study (ie, the smallest effect size found in the previous study). With a 2-tailed α = 0.05, a sample of 450 provided >90% power to detect bivariate associations between our variables of interest and perceived impairment in sports participation. For regression analyses, we estimated effect sizes based on the Plevinsky and colleagues study,9 in which semipar-tial correlations ranged from rsp2 = 0.09 to r
sp2 = 0.50. Using the
conservative effect size estimate of rsp2 = 0.09 (ie, the smallest
independent variables. Power analyses were conducted using GPower version 3.16.
Ethical Considerations
Institutional review board approval was gained through UNC at Chapel Hill and Rosalind Franklin University of Medicine and Science. Data were stored and managed by CCF and UNC School of Medicine. The parent/guardian provided online consent for their participation and for youth participa-tion. Youth provided online assent for their participaparticipa-tion.
RESULTS
Demographics of Study Population
The CCFA Partners Kids and Teens Registry sample con-sisted of 473 youth age 12–17 years. Participants were excluded from the analysis using list-wise deletion in SPSS to ensure that all participants had complete data on the variables of interest, which resulted in a sample size of 450 for the current analy-ses. Transformations were used to improve the normality of the following variables: anxiety (square root), pain (square root), depression (inverse), perceived impairment in sports participa-tion (reflected square root), BMI z-score (reflected square root), and age of IBD diagnosis (reflected square root). Correlation analyses to examine which variables should be included as covariates in multiple regression analyses revealed that disease activity was significantly correlated with perceived impairment in sports participation (r = –0.496, P < 0.001) and therefore was used as a covariate (Table 1). However, race/ethnicity and age of IBD diagnosis were not significantly associated with perceived impairment in sports participation and were not included as covariates.
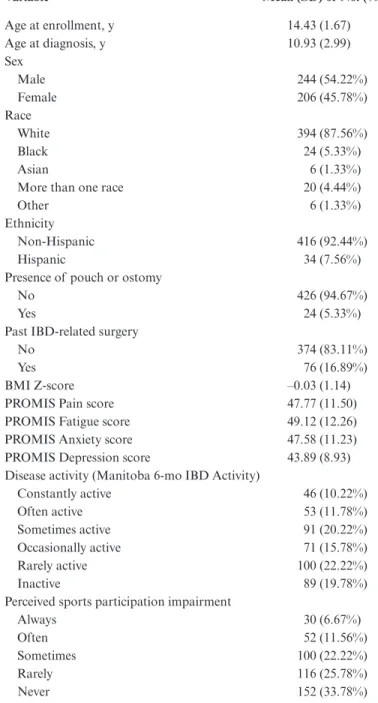
The average participant age was 14.4 (1.67) years, 45.8% of participating youth were female, and 84.0% identified as non-Hispanic white. More than half of participants reported at least occasional IBD disease activity within the past 6 months. See Table 2 for additional demographic information about the sample.
Perceived Impairment in Sports Participation
Nearly two-thirds of the sample (n = 298, 66.2%) reported that their IBD resulted in some perceived impairment in sportsparticipation, whereas a smaller subset (n = 82, 18.3%) reported that their IBD “often” or “almost always” interfered with their participation in sports (Table 2).
Bivariate Correlates of Impairment in
Sports Participation
Having a pouch or ostomy (r = .188, P < 0.001) or a past IBD-related surgery (r = .182, P < 0.001) were each associated with greater perceived impairment in sports participation, with small effect sizes (Table 2). Higher self-reported ratings of pain (r = 0.509, P < 0.001), fatigue (r = 0.563, P < 0.001), anxiety (r = 0.425, P < 0.001), and depression (r = –0.409, P < 0.001) were also associated with greater perceived impairment in sports participation. These effect sizes were medium or large in magnitude. BMI z-score was not associated with perceived impairment in sports participation (r = –0.056, P = 0.118).
Most Salient Correlates of Impairment
in Sports Participation
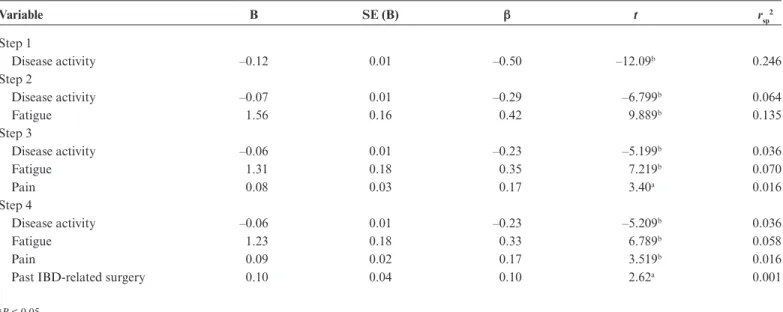
After controlling for disease activity, fatigue, pain, and ever having had an IBD-related surgery each emerged as signifi-cant correlates of perceived impairment in sports participation. The final regression model, which included disease activity as a covariate, explained a total of 40.6% of the variance in per-ceived impairment in sports participation (multiple R = .637;
R2 = .406; F (4,445) = 76.026; P < 0.001), the equivalent of a
large effect. Moreover, the unique impact of each independent variable was significant. In the final model, fatigue explained the most variance in perceived impairment in sports partici-pation, 5.8% (P < 0.001), whereas disease activity accounted for 3.6% of unique variance (P < 0.001) and pain explained 1.6% (P < 0.001) of the variance in perceived impairment in sports participation. Finally, ever having had surgery for IBD explained 0.1% of the total variance (P = 0.009), a small but statistically significant effect (Table 3).
DISCUSSION
In youth with IBD, fatigue, pain and past IBD-related surgery were the most salient correlates of perceived impair-ment in sports participation after accounting for IBD disease activity. Fatigue was the largest contributor to perceived impair-ment in sports. Fatigue was positively associated with perceived
TABLE 1.
Correlations of Perceived Impairment in Sports Participation With Variables of Interest (n = 450)
Measures Race
Age of Diagnosis
Disease
Activity Age Sex
Pouch or Ostomy
IBD Surgery
BMI
Z-Score Pain Fatigue Anxiety Depression
Impairment in
sports 0.00 –0.04 –0.50
b 0.03 0.04 0.19a 0.18b –0.06 0.51b 0.56b 0.43b –0.41b
aP < 0.05.
impairment in sports in a smaller cross-sectional study of youth with IBD,9 and it appears to interfere with sports par-ticipation specifically, and physical activity generally, in youth with other types of chronic illness.19, 20 Similarly, pain impedes physical activity in youth with chronic illnesses19, 21–23; however, this study is the first to replicate that finding in a pediatric IBD sample. Importantly, fatigue and pain were significant con-tributors to perceived impairment in sports participation even after accounting for the role of disease activity, suggesting the
importance of assessing these barriers specifically regardless of disease activity level. Though fatigue and pain are common barriers to physical activity, exercise is often recommended to address fatigue and pain in adults with chronic fatigue and chronic pain.24, 25 However, current recommendations for youth with other chronic conditions such as juvenile arthritis advo-cate for limiting physical activity until pain subsides.26 Whether physical activity could reduce fatigue and pain in youth with IBD, both acutely and long term, to alleviate sports impair-ment deserves further study.
Regarding the role of IBD disease complications, youth who reported at least 1 previous IBD-related surgery endorsed greater perceived impairment in sports participation than those who had not undergone an IBD surgery previously in multivar-iate analyses. In contrast, the presence of an ostomy or pouch was not as strongly associated with sports impairment in regres-sion analyses. However, it should be noted that few individuals (n = 24, 5%) had either an ostomy or a pouch. Moreover, the bivariate association of having a pouch or ostomy with per-ceived sports impairment was comparable in magnitude to the bivariate association between IBD-related surgery history and perceived impairment in sports participation, suggesting that shared variance between pouch/ostomy and other domains of functioning may have contributed to it being a less salient pre-dictor in regression analyses. Additionally, the length of time since surgery was not measured in the present study; certainly youth who had recently completed surgery would be expected to limit their activities, especially sports participation, until they have fully healed. Youth could potentially miss an entire sport season depending on the sport and when the child had surgery. Even after a child has healed from surgery, caution may be warranted with respect to engagement in vigorous physical activity. In support of this, 1 small study of adults with Crohn’s disease found that maximum exercise load was limited in adults with a bowel resection compared with adults without a bowel resection.27 More research is needed, particularly in youth with IBD who have an ostomy or pouch, to understand whether physical activity recommendations for youth with IBD should be tailored based on IBD treatment.
Psychosocial factors such as depression and anxiety were not associated with perceived impairment in sports par-ticipation in regression models, despite research suggesting that symptoms of depression and anxiety often impede phys-ical activity in youth28, 29 and despite support for the role of these variables in influencing perceived impairment in sports participation in our bivariate analyses. In the current sample, depression and anxiety were strongly correlated with pain and fatigue. Thus, when all 4 variables competed to enter the regres-sion model, fatigue and pain emerged as the more salient fac-tors. Given interrelationships among these variables, if physical activity can be used to reduce pain and fatigue in youth with IBD, symptoms of depression and anxiety may be similarly alleviated.
TABLE 2.
Demographic and Descriptive Data for the
Sample of Youth With IBD (n = 450)
Variable Mean (SD) or No. (%)
Age at enrollment, y 14.43 (1.67) Age at diagnosis, y 10.93 (2.99) Sex
Male 244 (54.22%)
Female 206 (45.78%)
Race
White 394 (87.56%)
Black 24 (5.33%)
Asian 6 (1.33%)
More than one race 20 (4.44%)
Other 6 (1.33%)
Ethnicity
Non-Hispanic 416 (92.44%)
Hispanic 34 (7.56%)
Presence of pouch or ostomy
No 426 (94.67%)
Yes 24 (5.33%)
Past IBD-related surgery
No 374 (83.11%)
Yes 76 (16.89%)
BMI Z-score –0.03 (1.14)
PROMIS Pain score 47.77 (11.50) PROMIS Fatigue score 49.12 (12.26) PROMIS Anxiety score 47.58 (11.23) PROMIS Depression score 43.89 (8.93) Disease activity (Manitoba 6-mo IBD Activity)
Constantly active 46 (10.22%)
Often active 53 (11.78%)
Sometimes active 91 (20.22%) Occasionally active 71 (15.78%)
Rarely active 100 (22.22%)
Inactive 89 (19.78%)
Perceived sports participation impairment
Always 30 (6.67%)
Often 52 (11.56%)
Sometimes 100 (22.22%)
Rarely 116 (25.78%)
The present study found that 66% of the sample reported some level of impairment in sports participation, which is con-sistent with findings from a smaller study of youth with IBD.9 Sports participation is associated with physical activity and exercise engagement in youth.5 Although sports participation may present unique barriers for youth with IBD, such as lack of flexibility for engaging in physical activity or peer-related concerns, pain and fatigue likely interfere with physical activity participation generally. Adults with IBD report that fatigue is a physical activity barrier,30 and they often experience more pain and fatigue compared with the healthy population.31 Future research is needed to examine whether pain, fatigue, and pre-vious IBD surgery interfere with physical activity generally for youth with IBD. Understanding sports participation and gen-eral physical activity participation, and the relevant facilitators and barriers for each, could provide insight into interventions for increasing physical activity in youth with IBD. If youth with IBD are concerned about whether disease flare-ups impact their sports participation, facilitating engagement in unstructured physical activity may be more efficacious for increasing phys-ical activity.
Strengths of the study included the large sample size, variability in the disease activity of the sample, and the exam-ination of multiple physical and mental health factors. The sample’s limited ethnic and racial diversity and exclusion of children under 12 years of age reduces generalizability, and the cross-sectional design impedes a discussion of causality. Most constructs were assessed with 1 or 2 items, which may limit the measures’ ability to adequately capture the construct
of interest. Perceived sports impairment may not reflect actual participation in sports. This study also did not include other variables often associated with physical activity, such as self- efficacy and social support. Future research could use a lon-gitudinal design to test a broad range of factors and examine whether IBD-specific factors or physical activity–related fac-tors play a stronger role in impeding physical activity engage-ment for youth.
Physical symptoms of IBD, specifically pain and fatigue, may impede participation in sports among youth. Sports impairment in youth with IBD is concerning, especially if impairment results in overall physical inactivity, given the phys-ical and mental health benefits of regular physphys-ical activity.6–8 Over a 12-year period in Finland, the percentage of children with chronic conditions and physical disabilities who reported regular physical activity substantially increased (7% and 13% increases for girls and boys, respectively).32 Increased physical activity, particularly in girls, was attributed to participation in sports.32 Understanding whether targeted interventions involv-ing sport participation are required to address physical inactiv-ity in youth with IBD is an important next step.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the input of Ms. Jill Plevinsky, MA, patient representative, who provided valuable feedback on the research questions of interest. In addition, the authors appreciate the assistance of the following members of the CCFA Partners Research Team: Robert Sandler, Millie Long, Beth Jaeger, Amber Robb, Wenli Chen, and Kristen
TABLE 3.
Forward Multiple Regression Analysis Examining Correlates of Perceived Impairment in Sports Participation
Perceived Impairment in Sports Participation
Variable B SE (B) β t rsp2
Step 1
Disease activity –0.12 0.01 –0.50 –12.09b 0.246
Step 2
Disease activity –0.07 0.01 –0.29 –6.799b 0.064
Fatigue 1.56 0.16 0.42 9.889b 0.135
Step 3
Disease activity –0.06 0.01 –0.23 –5.199b 0.036
Fatigue 1.31 0.18 0.35 7.219b 0.070
Pain 0.08 0.03 0.17 3.40a 0.016
Step 4
Disease activity –0.06 0.01 –0.23 –5.209b 0.036
Fatigue 1.23 0.18 0.33 6.789b 0.058
Pain 0.09 0.02 0.17 3.519b 0.016
Past IBD-related surgery 0.10 0.04 0.10 2.62a 0.001
aP < 0.05
Anton. Finally, we are very appreciative of the contributions of patients and caregivers who completed the CCFA Partners Kids and Teens Surveys and the funding support provided by the Crohn’s and Colitis Foundation.
REFERENCES
1. Narula N, Fedorak RN. Exercise and inflammatory bowel disease. Can j Gastroenterol. 2008;22:497–504.
2. Janssen I, Leblanc AG. Systematic review of the health benefits of physical activ-ity and fitness in school-aged children and youth. Int j Behav Nutr Phys Act. 2010;7:40.
3. Crohn’s and Colitis Foundation of America. Crohn’s disease & ulcerative colitis: a guide for parents. http://www.ccfa.org/resources/guide-for-parents.html. Updated August 17, 2016. Accessed May 14, 2017.
4. Werkstetter KJ, Ullrich J, Schatz SB, et al. Lean body mass, physical activity and quality of life in paediatric patients with inflammatory bowel disease and in healthy controls. j Crohns Colitis. 2012;6:665–673.
5. The National Youth Risk Behavior Survey. Trends in the presence of physical activity and sedentary behaviors national: YRBS 1991–2015. http://www.cdc.gov/ healthyyouth/data/yrbs/pdf/trends/2015_us_physical_trend_yrbs.pdf. Published 2015. Accessed May 14, 2017.
6. Eime RM, Young JA, Harvey JT, et al. a systematic review of the psychological and social benefits of participation in sport for children and adolescents: inform-ing development of a conceptual model of health through sport. Int j Behav Nutr Phys Act. 2013;10:135.
7. Steiner H, McQuivey RW, Pavelski R, et al. Adolescents and sports: risk or bene-fit? Clin Pediatr (Phila). 2000;39:161–166.
8. Packer N, Hoffman-Goetz L, Ward G. Does physical activity affect quality of life, disease symptoms and immune measures in patients with inflammatory bowel disease? a systematic review. j Sports Med Phys Fitness. 2010;50:1–18.
9. Plevinsky JM, Wojtowicz AA, Poulopoulos N, et al. Perceived impairment in spots participation in adolescents with inflammatory bowel disease: a preliminary examination. J Pediatr Gastroenterol Nutr. In press.
10. Motl RW, Birnbaum AS, Kubik MY, Dishman RK. Naturally occurring changes in physical activity are inversely related to depressive symptoms during early ado-lescence. Psychosom Med. 2004;66:336–342.
11. Martins J, Marques A, Sarmento H, Carreiro da Costa F. Adolescents’ perspec-tives on the barriers and facilitators of physical activity: a systematic review of qualitative studies. Health Educ Res. 2015;30:742–755.
12. Trost SG, Owen N, Bauman AE, et al. Correlates of adults’ participation in phys-ical activity: review and update. Med Sci Sports Exerc. 2002;34:1996–2001. 13. Telama R, Yang X, Viikari J, et al. Physical activity from childhood to adulthood:
a 21-year tracking study. Am j Prev Med. 2005;28:267–273.
14. Kappelman MD, Long MD, Martin C, et al. Evaluation of the patient-reported outcomes measurement information system in a large cohort of patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2014;12:1315–1323.e2.
15. Clara I, Lix LM, Walker JR, et al. The Manitoba ibd Index: evidence for a new and simple indicator of ibd activity. Am j Gastroenterol. 2009;104:1754–1763. 16. Center for Disease Control and Prevention growth charts: Z-score data files.
https://www.cdc.gov/growthcharts/zscore.htm. Updated August 4, 2009. Accessed May 14, 2017.
17. Perrin JM, Kuhlthau K, Chughtai A, et al. Measuring quality of life in pediatric patients with inflammatory bowel disease: psychometric and clinical characteris-tics. j Pediatr Gastroenterol Nutr. 2008;46:164–171.
18. Cohen J. Statistical Power Analyses for Behavioral Sciences. 2nd ed. Mahwah, NJ: Lawrence Erlbaum Associates; 1988.
19. Armbrust W, Lelieveld OH, Tuinstra J, et al. Fatigue in patients with juvenile idiopathic arthritis: relationship to perceived health, physical health, self-efficacy, and participation. Pediatr Rheumatol Online j. 2016;14:65.
20. Ameringer S, Elswick RK Jr, Smith W. Fatigue in adolescents and young adults with sickle cell disease: biological and behavioral correlates and health-related quality of life. j Pediatr Oncol Nurs. 2014;31:6–17.
21. Race DL, Sims-Gould J, Tucker LB, et al. ‘It might hurt, but you have to push through the pain’: perspectives on physical activity from children with juvenile idiopathic arthritis and their parents. J Child Health Care. 2016;20:428–436. 22. Tran ST, Salamon KS, Hainsworth KR, et al. Pain reports in children and
adoles-cents with type 1 diabetes mellitus. j Child Health Care. 2015;19:43–52. 23. Long AC, Palermo TM, Manees AM. Brief report: using actigraphy to compare
physical activity levels in adolescents with chronic pain and healthy adolescents. j Pediatr Psychol. 2008;33:660–665.
24. Geneen LJ, Moore RA, Clarke C, et al. Physical activity and exercise for chronic pain in adults: an overview of cochrane reviews. Cochrane Database Syst Rev. 2017;4:CD011279.
25. Afari N, Buchwald D. Chronic fatigue syndrome: a review. Am j Psychiatry. 2003;160:221–236.
26. Philpott J, Houghton K, Luke A. Physical activity recommendations for children with specific chronic health conditions: juvenile idiopathic arthritis, hemophilia, asthma and cystic fibrosis. Paediatr Child Health. 2010;15:213–225.
27. Brevinge H, Berglund B, Bosaeus I, et al. Exercise capacity in patients under-going proctocolectomy and small bowel resection for crohn’s disease. Br j Surg. 1995;82:1040–1045.
28. Sallis JF, Prochaska JJ, Taylor WC. a review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32:963–975.
29. Doré I, O’Loughlin JL, Beauchamp G, et al. Volume and social context of phys-ical activity in association with mental health, anxiety and depression among youth. Prev Med. 2016;91:344–350.
30. Tew GA, Jones K, Mikocka-Walus A. Physical activity habits, limitations, and predictors in people with inflammatory bowel disease: a large cross-sectional online survey. Inflamm Bowel Dis. 2016;22:2933–2942.
31. Jelsness-Jørgensen LP, Bernklev T, Henriksen M, et al. Chronic fatigue is more prevalent in patients with inflammatory bowel disease than in healthy controls.
Inflamm Bowel Dis. 2011;17:1564–1572.