ABSTRACT
AKSHAY, VENKITASUBRAMANIAN. Object-Oriented Framework for Healthcare Simulation. (Under the direction of Dr. Stephen D. Roberts and Dr. Jeffery A. Joines).
This thesis addresses the problem of modeling complexity of healthcare simulation projects. From an extensive literature review, three problems associated with healthcare simulation were elicited: lack of flexibility among healthcare simulation, lack of
implementation methodologies to support building of complex integrated multi-facility simulation models, and lack of stakeholder involvement in simulation projects.
The first problem was attributed to lack of flexibility in healthcare simulation
software. This can be deduced from sheer number of simulation projects resorting to develop their own simulation using general purpose languages. The root cause of the problem has been identified as the lack of conceptual framework in development of healthcare simulation libraries. In addition to this, we present four intuitive axioms to assist future simulation software developers and modelers in assessing the utility of simulation toolkit and models.
The second problem was attributed to lack of integrative framework for complex facilities simulations. Healthcare is a highly interconnected environment and multi-facility simulations will help in relaxing the fixed boundaries assumed in facility-specific simulation projects. In this thesis, we present a model development process that takes advantage of expertise of simulation community in facility-specific models and extend it to the development of complex integrated multi-facility systems.
Finally, we address the problem of stakeholder involvement and lack of
implementation in simulation projects in healthcare sector. We present a causal loop diagram to visualize the dynamics of four simulation success factors: Verification, Validation,
© Copyright 2012 by Venkitasubramanian Akshay
Object-Oriented Framework for Healthcare Simulation
by
Venkitasubramanian Akshay
A thesis submitted to the Graduate Faculty of North Carolina State University
in partial fulfillment of the requirements for the degree of
Master of Science
Industrial Engineering
Raleigh, North Carolina 2012
APPROVED BY:
_______________________________ ______________________________ Dr. Stephen D. Roberts Dr. Jeffery A. Joines
Committee Co-Chair Committee Co-Chair
_________________________________ Dr. Yunan Liu
ii
DEDICATION
iii
BIOGRAPHY
Akshay Venkitasubramanian was born on September 19th, 1988 in a quaint, little town of Neyveli, India to two bankers. Hence, he was brought up in a dynamic environment where they shifted places every 4 years. This change put him through 4 different school systems and helped him understand that his academic forte lied in mathematics and programming. In addition to this, growing up in diverse societies helped in cultivating his strong personal interests for social development. Combining his personal experiences with academic interest, he chose to study Electronics and Biomedical Engineering at Government Model Engineering College, Cochin where he graduated with FIRST class in June 2009.
During these four years, he actively became involved with the Young Indians (Yi) organization which provided a platform for students to work alongside leaders and
entrepreneurs designing and implementing initiatives to improve their local communities.For his contributions to the organization, he was awarded Most Valuable Member of the Year (All India) in 2009 and was given invited to give a talk on the topic of social development and youth involvement at the prestigious Indian School of Business, Hyderabad. This is where he came in touch with late management professor Dr. C.K.Prahalad (University of Michigan-Ross Business School) and the following interactions with Dr. C.K.Prahalad taught him that technology is only a part of the healthcare problem and that an equally-important focus should be on operations strategy.
After graduation, he decided to pursue a series of developmental internships in Nigeria and India to understand the role of healthcare systems while he pondered over the choice of graduate program. His uncle, Dr. Parasuram Balasubramanian (CEO, ThemeWorks Analytics), who holds a doctorate in Industrial Engineering from Purdue University was a huge help and he finally chose the graduate program in Industrial Engineering at North Carolina State University.
iv infection control practices. He is also an active member of Alpha Phi Mu, Institute for
Industrial Engineers, Society for Health Systems, System Dynamics Society, and INFORMS. He hopes to pursue doctoral studies in management science focusing on public health
v
ACKNOWLEDGEMENTS
The author wishes to express his sincere gratitude to his advisors: Dr. Stephen D Roberts and Dr. Jeffery A Joines for tirelessly working with him and instilling a culture of academic research. In addition to this, he is also grateful to them for supporting him through research and teaching assistantships. The author also expresses his thanks to Dr. Yunan Liu for his time and support in helping refine this work. Last but not the least, the author
vi
TABLE OF CONTENTS
LIST OF TABLES
...x
LIST OF FIGURES
...xi
READING STYLE GUIDE
...xvi
1. INTRODUCTION
... 1
1.1THE POWER TO SEE ...1
1.2HEALTHCARE AND SIMULATION ...2
1.2.1 Timeliness of Care ...2
1.2.2 Quality of Care ...3
1.2.3 Errors in care delivery ...4
1.2.4 Complexity in healthcare delivery ...4
1.2.5 Value of healthcare services ...5
1.3SIMULATION MODELING PARADIGMS ...6
1.3.1 Discrete Event Simulation (DES): ...7
1.3.2 System Dynamics (SD):...7
1.3.3 Agent-Based Modeling (ABM): ...7
1.4SIMULATION MODELING SOFTWARE ...8
1.4.1 Simulation software history- An overview ...8
1.4.2 Healthcare Simulation Packages ...10
1.4.2.1 MedmodelTM ...10
1.4.2.2 Flexsim HCTM ...11
1.5THESIS OUTLINE ...11
2. LITERATURE SURVEY
... 13
2.1OBJECT ORIENTED SIMULATION (OOS) ...13
2.2SYSTEMATIC REVIEW OF HEALTHCARE SIMULATION LITERATURE ...16
2.3PATIENT FLOW AND OPTIMIZATION ...18
vii
2.3.1 Inpatient Scheduling ...20
2.3.2 Emergency Department (ED) Simulations...21
2.3.3 Specialist Clinics ...23
2.3.4 Physician and Healthcare Staffing ...24
2.4HEALTHCARE ASSET ALLOCATION ...25
2.4.1 Bed Sizing and Planning ...25
2.4.2 Room Sizing and Planning ...25
2.4.3 Staff Sizing and Planning ...26
2.5HEALTH POLICY SIMULATIONS ...27
2.6MULTI-FACILITY SIMULATION MODELS ...31
2.7SIMULATION TUTORIALS ...32
2.7.1 Modeling Tutorials...32
2.7.2 Implementation Tutorials ...34
2.8RESEARCH SCOPE DEVELOPMENT ...36
2.9CHAPTER SUMMARY ...38
3. HEALTHCARE TOOLKIT DEVELOPMENT
... 39
3.1SIMIO–A BRIEF INTRODUCTION ...39
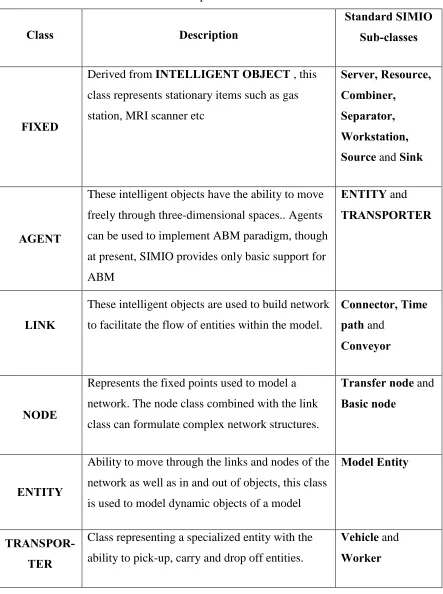
3.1.1 Base Classes...40
3.1.2 Building New Class ...42
3.2BASE CLASSES OF SIMIO-HC ...43
3.3FIXED GROUP ...46
3.3.1 Patient Care (PC) ...46
3.3.2 Patient Care with Lab Care Class (PC_Labcare) ...50
3.3.3 Hospital Workstation ...54
3.3.4 Hospital Workstation with Lab Care Class (HWS_Labcare) ...58
3.3.5 Redirect Object Class (RO) ...60
3.3.6 Waiting Room (WR) ...62
3.3.7 Registration Desk (RD) ...63
viii
3.4NODE ...67
3.4.1 Hospital Transfer node ...67
3.5TRANSPORTER CLASS ...68
3.5.1 Hospital Transporter Class (HT) ...69
3.5.2 Hospital Worker (HW) ...73
3.6ENTITY CLASS ...74
3.6.1 Patient Entity Class (PE) ...74
3.6.2 Specimen Entity (SE) ...77
3.7CHAPTER SUMMARY ...78
4. COMPLEX INTEGRATED MULTI-FACILITY SYSTEMS SIMULATION
... 79
4.1AN INTRODUCTION TO CIMS ...79
4.2BUILDING CIMSMODEL ...80
4.2.1 Emergency Department Model ...81
4.2.2 Oncology Clinic model ...84
4.2.3 Laboratory Services ...87
4.2.4 Radiology Services ...89
4.2.5 Facility Integration ...91
4.3MODEL DEPLOYMENT ...91
4.3.1 Experimentation Setup and Results ...93
4.4SIMULATION PROJECT LIFECYCLE ...97
4.5CHAPTER SUMMARY ...100
5. CONCLUSIONS AND FUTURE WORK
... 101
BIBLIOGRAPHY
... 104
APPENDICES
... 149
Appendix A SIMIO Framework: ...150
A.I Object-Oriented Programming Concepts ...150
ix
A.III Object Definitions ...153
A.IV SIMIO Standard Library ...158
A.V Additional Readings ...159
Appendix B : SIMIO-HC Toolkit ...161
B.I Base Class Overview ...161
B.II Patient Entity ...163
B.III Specimen Entity ...167
B.IV Hospital Transfer node ...168
B.V Redirect Object ...169
B.VI Waiting room Object ...173
B.VII Registration desk ...177
B.VIII Patient Care Object ...179
B.IX Patient Care with LabCare (PC_LabCare) ...185
B.X Hospital Workstation ...189
B.XI Hospital Workstation with Lab Care (HWS_Labcare) ...200
B.XII Statistics Collection Sink: ...207
B.XIII Hospital Transporter ...209
B.XIV Hospital Worker ...217
Appendix C : CIMS Model Development ...220
C.I Emergency Room Model ...220
C.II Oncology Clinic ...228
C.III Laboratory Services ...235
C.IV Radiology Services ...241
x
LIST OF TABLES
Table 3-1: Description of SIMIO Base Class ... 41
Table 3-2: Patient Care Object Label Definitions s ... 48
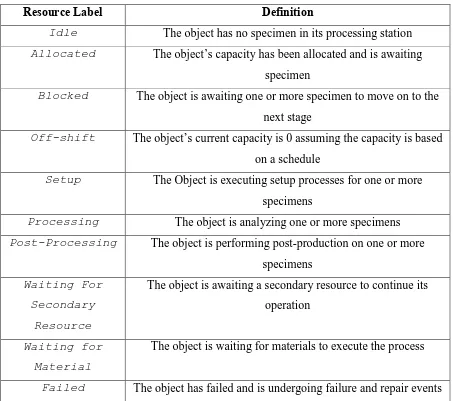
Table 3-3: Patient Care Object Resource State Definitions ... 49
Table 3-4: Hospital Workstation Resource States ... 57
Table 3-5: Agent Class Resource States ... 71
Table 3-6: Patient Entity Activity States... 77
Table 4-1: Patient Care Treating & Occupied Resource State Averages ... 95
Table 4-2: Laboratory utilization breakdown ... 95
Table 4-3: Radiology Department utilization breakdown ... 95
Table 4-4: Percent Time statistics breakdown for Patient’s activity ... 96
Table 4-5: Total Time statistics (in minutes) for patient’s activity ... 97
Table B-1: Patient Entity Lists………..163
Table B-2 : Patient Entity Function Table ... 163
Table B-3: Patient Entity States ... 165
Table B-4: Specimen Entity’s States ... 167
Table C-1: ED Patient Arrival Table (ED_ArrivalTable) ... 221
Table C-2: Data Table for Oncology Patients ... 230
Table C-3: Processed Specimen routing out expressions ... 240
xi
LIST OF FIGURES
Figure 1-1: Abstraction Levels For Dynamic Simulation Paradigms ...6
Figure 1-2: Block Diagram Of A DES Package [Adopted from Pidd and Carvalho(2006)] ..9
Figure 2-1 Breakdown of Literature Survey Papers ...37
Figure 3-1: Simio Base Classes ...40
Figure 3-2: Utility as function of Hierarchy and Class Count ...44
Figure 3-3: Class Hierarchy Tree of SIMIO-HC ...45
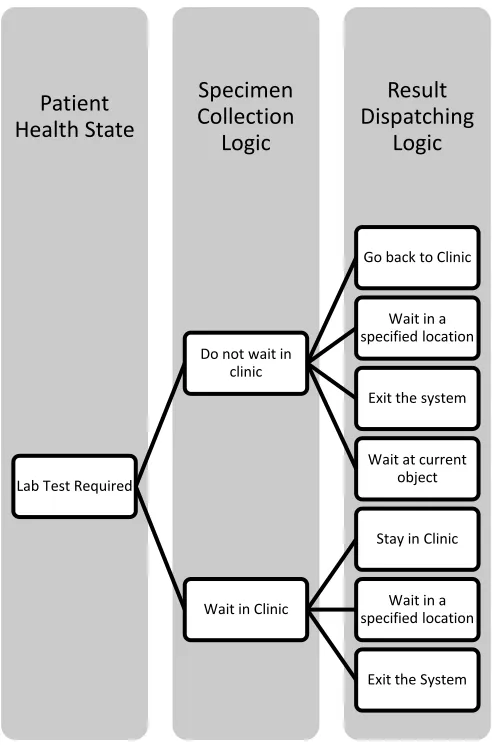
Figure 3-4: Decision Making Structure for Specimen Collection ...52
Figure 3-5: Utility Of a Class...54
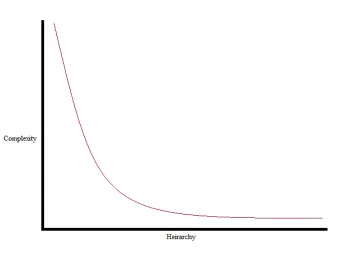
Figure 3-6: Relationship between Class Hierarchy and Its Complexity ...65
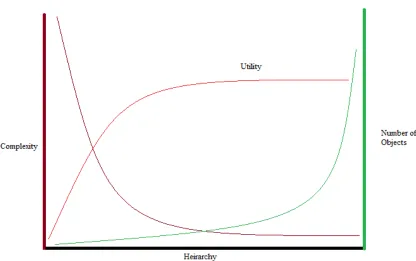
Figure 3-7: Utility of Class as a function of Complexity And Object Count ...66
Figure 3-8- Routing Logic Flowchart Of Hospital Transporter ...70
Figure 3-9 : Utility Function as a function of Run Speed and Complexity ...72
Figure 4-1: Hypothetical Hospital Model ...81
Figure 4-2: Emergency Department Conceptual Model ...82
Figure 4-3: Oncology Department Conceptual Model ...84
Figure 4-5- Treatment Patient Flow ...86
Figure 4-4- Check Up and Follow Up Patient Flow ...85
Figure 4-6: Treatment with Checkup Patient Flow...86
Figure 4-7: Laboratory Department Conceptual Model ...88
Figure 4-8: Radiology Department Conceptual Model ...90
Figure 4-9: Patient Time in System for 25 scenarios generated by OptQuest ...94
xii
Figure 4-11: Simulation Project Lifecycle ...99
Figure A-1: Standard Library of SIMIO………158
Figure B-1: Patient Related References Storage ...166
Figure B-2: Specimen Related Reference Storage ...168
Figure B-3: Modified Process for Hospital Transfer node ...169
Figure B-4: Process on Entering the Object ...171
Figure B-5: Redirect Object Processing Logic ...171
Figure B-6: Paperwork Batching Logic ...172
Figure B-7: Results Batching Process...172
Figure B-8: Entity Trying To Enter Waiting Room ...175
Figure B-9: Waiting Room Process-I ...175
Figure B-10: Waiting Room Process-II ...176
Figure B-11: When an Entity Balks ...176
Figure B-12: Renege Process to evaluate reneging conditions ...177
Figure B-13: When an entity enters Registration Desk...178
Figure B-14: Processing Entities In Registration Desk- I ...178
Figure B-15: Processing Entities in Registration Desk- II ...179
Figure B-16: Upon Initializing Run ...181
Figure B-17: When a seize request is evaluated ...182
Figure B-18: When capacity of the object is allocated ...182
Figure B-19: Upon Capacity Released ...183
Figure B-20: Patient Treatment Process -I ...183
Figure B-21: Patient Treatment Process -II ...184
xiii
Figure B-23: When a Patient Exits ...184
Figure B-24: When an Entity Enters pc_LabCare-I ...187
Figure B-25: When an Entity Enters pc_LabCare-II ...187
Figure B-26: Process for providing secondary care ...188
Figure B-27: Continue Treatment Process post visit to lab ...189
Figure B-28 Results Arrive and Batch Process...189
Figure B-29: Run Initialization Process ...191
Figure B-30: Seize Request Process ...192
Figure B-31: Capacity Changed Process ...192
Figure B-32: On Entering the Setup Buffer ...193
Figure B-33: Performing Setup Activity- I ...193
Figure B-34: Performing Setup Activity-II ...194
Figure B-35: Specimen Batching Process...195
Figure B-36: Creating and Batching Parent Specimen Entity Process...195
Figure B-37: Logic of Processing Activity-I ...196
Figure B-38: Logic of Processing Activity-II ...197
Figure B-39: Upon exiting processing buffer ...197
Figure B-40: On Entering Post-Production Buffer ...198
Figure B-41: Perform Post Production Activity Process ...199
Figure B-42: Post Production Buffer Exited ...199
Figure B-43: Initialization of the HWS_LabCare ...202
Figure B-44: Implementing Failure ...202
xiv
Figure B-46: On Repaired Process ...203
Figure B-47: On Entered Setup Buffer ...203
Figure B-48: Perform Setup Activity ...204
Figure B-49: Specimen Entity Create-I ...204
Figure B-50: Specimen Entity Create-II...205
Figure B-51: Processing Buffer Exited ...205
Figure B-52: Batching Addition to Perform Processing Activity Process ...206
Figure B-53: Results on Entering the Results Station ...207
Figure B-54: Waiting for Results Process ...207
Figure B-55: Collection of Statistics...209
Figure B-56: On creating the transporter ...211
Figure B-57: On Initializing the Simulation Run ...211
Figure B-58: Rider Loading Process...212
Figure B-59: Rider Loaded ...212
Figure B-60: Rider Unloading Process ...213
Figure B-61: Deciding if the Node is Destination Node-I ...213
Figure B-62: Pickup or Drop-off ...214
Figure B-63: Parking Decision Process ...215
Figure B-64: Seize Assistance Resources ...216
Figure B-65: Release Assistance Resources ...216
Figure B-66: Worker Capacity Changed Process ...217
Figure B-67: Upon Worker Capacity Released ...218
xv
Figure B-69: Implementing Fixed Routing...219
Figure C-1: Emergency Department Process Layout ...221
Figure C-2: Transferring patients to different entrances...223
Figure C-3: Diverting Ambulance if waiting room is full ...223
Figure C-4: Refusal of Service if Waiting Room is full at Registration Desk ...224
Figure C-5: Custom Treatment logic ...226
Figure C-6: Sample Warning for failing transfer from a node ...228
Figure C-7: Oncology Clinic Process Layout ...230
Figure C-8: Splitting entities between two transfer node ...231
Figure C-9: Modeling Nurse Triage ...233
Figure C-10: IV Setup Process ...234
Figure C-11: Post Treatment Process to remove IV line ...234
Figure C-12: Laboratory Patient Flow ...236
Figure C-13: Patient States Assignments for eliciting patient choices ...238
Figure C-14: Radiology Department Model Layout ...242
Figure C-15: Deciding random patient entity assignments for radiology service ...243
xvi
READING STYLE GUIDE
Certain formatting styles have been adopted in this paper to facilitate easy reading. All the fonts and their keys are explained below.
Legend Key
Processes Times new roman, 12 font, underlined represents SIMIO processes ELEMENTS Courier New, 12 font, ALL CAPS Italics represents elements EventNames Courier New, 12 font, First Letter Caps, represents elements
States Courier New, 12 font, Sentence Case, Italics represents state variables
Functions Cambria, 12, represents function definitions
Expressions Cambria 12, Italics represents expressions
Properties Times new roman, 12 , Italics represents properties as well as drop down selections
List Names Courier New, 12 font, Sentence Case, Underlined represents lists “ Output Node” Times new roman 12, Sentence case represents items of external view
“Concept” Times new roman 12, Sentence case, Italics represents concepts
BASE CLASS Times new roman 12, Bold, All Caps represents SIMIO Base Classes
Standard Library Times new roman 12, Bold Sentence case represents SIMIO Standard library
Hospital Worker Times new roman 12, Bold Italics represents SIMIO HC Base class HW_LC_Xray Times new roman 12, Italics, Underlined represents SIMIO-HC children
1
Chapter 1
Introduction
1.1 The Power to See
Just over a decade ago, the medical community was confronted by the Institute of Medicine (IOM) To err is human report (IOM, 2000) and Crossing the Quality Chasm Report (IOM, 2001). The reports attributed major shortcomings of the US healthcare system to the growing complexity of medical practice and technology amplified by a poor
organization healthcare delivery system. In a nutshell, these reports shifted the focus of medical community from just treating the disease to treating the entire person which ushered in the patient safety revolution. The core focus of this ongoing revolution is to improve the patient safety, quality, and effectiveness of the healthcare system.
A decade into the patient safety movement, the results are discouraging. A recent study carried out by the Institute of Healthcare Improvement (IHI) indicates the number of adverse events is maybe 10 times the reported value (Classen et al., 2011). Errors in healthcare has become the eighth leading cause of death in the USA (Dhillon, 2008). Moreover, current healthcare spending exceeds 17% of the GDP, which has further exacerbated the current healthcare systems condition creating a sense of urgency for developing efficient healthcare system models (Kaplan and Porter, 2011),.
2 Evidence based Medicine and what we today call “Modern Medicine” (Claridge and Fabian, 2005). In short, visualizing the system is critical in developing a systems perspective. The development of a systems perspective helps us understand the structure of the system which is responsible for the behavior of the system. Thus, in order to fix the behavior of the system, we need to fix the structure of the system and simulation modeling will help us just do that.
1.2 Healthcare and Simulation
McGlynn et al. (2003) carried out an empirical investigation of the quality of
healthcare delivered to adults in the USA and found out that only 54.9±0.6% adults received recommended care. Furthermore, their study also reported huge variation in the quality of care depending on patient’s condition. In fact, the literature on healthcare is laden with articles like these that emphasize on the importance of the systems view of healthcare problems (Barker et al., 2002; Berwick, 2002; Cook, 2001; Fordyce et al., 2003; Wears, 2000; Wears, 2003; Young et al., 2004). The dissatisfaction with healthcare service can be broadly classified in to five categories: Timeliness of Care, Quality of Care, Errors in Care Delivery, Complexity of healthcare system , and Cost effectiveness of care. These problems are briefly discussed in the next sections and we suggest how simulation and systems thinking can assist in fixing them.
1.2.1 Timeliness of Care
Invariably, one of the main causes of dissatisfaction among patients is the
unprecedented waiting times for patients, as highlighted in IOM (2001). This unpredictability in waiting time can be frustrating as well as affect the effectiveness of care for the patient and the care provider. For the patient, the waiting time may cause him/her to come in contact with other infections or various environmental factors may interact to further complicate the patient’s condition. As for the delay in treatment, this delay factor can reduce the
3 importance of achieving time-stable performance of workload (or utilization) to provide consistent quality of service (Feldman et al, 2008). Thus we can extend the same concept to healthcare service. Furthermore, empirical research results presented by Kuntz, Mennicken, and Scholtes (2012) show that the utilization of care providers should be moderate (i.e.86-87%) to minimize the chance of adverse event and indirectly, mortality rate.
Simulation modeling has been used for over 60 years in the service industries to appropriately staff as well predict customer flows in order to maximize utilization of clinics while providing best service. We intend to extend the very same methodology to healthcare systems in order to improve its timeliness of care factor.
1.2.2 Quality of Care
In the healthcare field, patient satisfaction should be the fundamental measure of quality of care (Berwick, 2002).Quality problems in healthcare services in both managed care and fee for service care systems can be divided in to three categories: underuse, overuse, or misuse. “Underuse” is defined as the failure to provide healthcare when it would have provided desirable outcome. “Overuse” is defined as the provision of service that can produce an undesirable outcome. “Misuse” is defined as choosing appropriate treatment but failure to avoid preventable complications. In short, the healthcare delivery process is not well understood which makes quality of healthcare also a systematic problem (NRHQ, 1998).
The first step in solving any problem is to understand it and represent it appropriately. Simulation modeling as a tool has been used in the Operations Research (or Management Science)1 field to do the very same task of representing the problem in a language that we can comprehend. Moreover, visualization of simulation model has helped in effective problem solving where there are diverse stakeholders such as in the healthcare field.
4
1.2.3 Errors in care delivery
In the United States, at least 44,000 people and maybe as many as 98,000 people die due to preventable medical errors (IOM, 2000). To put these numbers in perspective, the mortality in hospitals due to preventable medical errors exceeds mortality due to motor vehicle accidents, breast cancer, and AIDS. The most often cited reason for such errors is decentralized structure of healthcare service or the non-existence of systematic approach to delivery of healthcare. In layman terms, a patient does not die because one medical person made a mistake but because one person’s mistake sets off a chain reaction in the patient’s care chain compounding errors. Thus, the fatal errors are generated by faulty systems whose processes and conditions inhibit the system’s stakeholders from preventing it.
In order to fix errors, we should perform systematic analysis of the causes so that we fix the system. If this approach is not taken, fixing the errors will only further complicate the system. Simulation modeling can play a critical role in analyzing the system and eliciting errors. Moreover, with today’s computing power and advances in simulation languages, we can perform “what-if” analysis to yield valuable insights in to the system’s behavior.
1.2.4 Complexity in healthcare delivery
The Boeing 777 was considered to be too complicated to be flown by human pilot until a veteran US air force pilot extended the remarkable simple concept of a checklist to commercial aviation. Today this concept has been extended to the medical world and has been hailed in the medical community as a remarkable breakthrough as it has reduced the surgical errors by a third worldwide (Gawande, 2010) .The checklist provided surgeons a systematic way to deal with the complexities of surgical procedures by standardizing it. Moreover as complexity increases, latent errors also survive longer in the system and in the case of healthcare, this translates to fatalities (Wears, 2003).
5 the healthcare system for extended periods of time making simulation an attractive substitute. Furthermore, simulators have been used extensively in the aviation industries to formulate and test their checklists making an even stronger argument to use simulation models in the field of healthcare given both are high precision industries.
1.2.5 Value of healthcare services
The classical economics definition of value is the intersection of purchaser’s perception of goods or service and the cost which the purchaser is willing to pay for it. For example, if you paid $10 for a slice of pizza at a restaurant compared to spending the same money on chef’s special pasta at the restaurant, the latter would feel more satisfying. If we further try to extrapolate this concept to healthcare services, we can express the value of healthcare service as the cost effectiveness of care received.
𝑉𝑎𝑙𝑢𝑒 =𝑃𝑎𝑦𝑚𝑒𝑛𝑡𝑄𝑢𝑎𝑙𝑖𝑡𝑦
Given the fact that quality of healthcare services is at best ambiguous as it is heavily dependent on individual factors such as patient’s age, caregiver’s experience among multifarious factors, this equation can be considered as not well defined (HFMA, 2011).
6
1.3 Simulation Modeling Paradigms
Among the various simulation modeling paradigms, four modeling paradigms stand out in the healthcare literature (Fone et al., 2003; Katsaliaki and Mustafee, 2011): Discrete Event Simulation (DES), System Dynamics (SD), Monte Carlo Simulation (MCS), and more recently, Agent based model (ABM). With the exception of Monte Carlo Simulation, all other aforementioned paradigms are dynamic modeling paradigms and can therefore capture the dynamics of complex systems.
Among the dynamic modeling paradigms, discrete event and system dynamics take a top down approach where you define the rules of the physical world and the entities are modeled in the system. Agent based models take a bottom up approach where each agent (or entity) logic is defined and these intelligent agents interact with each other in the world based on these rules to develop system behavior. For a more detailed comparison of these paradigms, refer to Borshchev and Filippov (2004).
DISCRETE EVENT MODEL AGENT BASED MODEL SYSTEM DYNAMICS LOW MEDIUM HIGH LEV EL O F A B S TR A C TI O N
7 The choice of modeling paradigm is also based on the nature of the problem. If the problem requires a macro approach, then system dynamics will be the method of choice. On the other hand, if you have a problem that requires operational level detail with supporting process level data, discrete event modeling paradigm will be the most appropriate. If you have only individual level data (for example: person’s immunity, contact rate) and want to incorporate Artificial Intelligence (AI), then agent based modeling is ideally suited. Figure 1-1 correlates modeling paradigms with the level of abstraction.
1.3.1 Discrete Event Simulation (DES):
Discrete Event Simulation (DES) technique is the most popular among the simulation modeling techniques (Robinson, 2005). The roots of this modeling paradigm can be traced back to the 1950s and offers a “transaction-flow world view” of the system. In other words, we visualize the system as discrete units of traffic (or transaction) flow from point to point competing for system’s resources. The model’s state changes only at discrete points of time called event times. The event times can be randomly generated and it is possible for multiple units of traffic to be manipulated simultaneously. For a better understanding of DES, the reader may refer to Schriber and Brunner (2009).
1.3.2 System Dynamics (SD):
Developed by Jay.W.Forrester in the 1960s, this simulation paradigm helps us understand the behavior of complex systems. This simulation paradigm can capture the internal complexity of the system in order to represent them as feedback processes to explain the behavior of an entire system. The system dynamics models capture the nonlinearity using feedback (or causal) loops and stocks and flows. For a deeper understanding on the subject, the reader may refer to Sterman (2000) .
1.3.3 Agent-Based Modeling (ABM):
8 compared to computer science, social science, and economics fields (Siebers et al. 2010). Nonetheless, the problems tackled by this paradigm are unique compared to SD or DES and has a wide range of applications in real world problems.
ABM is a complex system composed of simple autonomous decision making agents who follow simple behavior rules defined by the modeler. The system properties emerge as a result of the interaction of these agents with each another and the environment which is of interest to the modeler. These agents mimic their counterparts in real world and thus make it an attractive method for modeling human behavior. For a more detailed tutorial on this methodology, refer to Bonabeau (2002).
1.4 Simulation Modeling Software
Among the OR/MS tools available today, Simulation has been acknowledged to be the most popular technique. (Fildes and Ranyard, 1997; Jeffrey and Seaton, 1995; O’Kane, Spenceley, and Taylor, 2000). Simulation has become an indispensable tool in addressing a wide range of problems posed by complex systems in a cost effective way. The growth in power and popularity of simulation methodology is highly correlated with developments in computing world.
1.4.1 Simulation software history- An overview
Although simulation did exist in pre- digital computing era, it was limited to academic circles. The applications of methodology were limited due to high level of complexity involved in analog computing machinery which proved to be cost ineffective. The onset of the digital computer revolution after World War II reshaped the prospects of computer simulation as the methodology. Gordon E Moore, co-founder of Intel predicted the computing power nearly doubled every 18 months which created an explosion of
9 standard for the forthcoming generation of simulation languages such as GASP, SLAM, SIMIAN/ARENA, SIMIO,etc. which made simulation a powerful, useful and cost effective OR/MS technique. Detailed accounts of aforementioned developments are presented in these papers if the reader wishes to explore this topic further; B.W. Hollocks (2006), Goldsman, Nance, and Wilson (2010), Ross (1967) and S. Robinson (2005).
Today, simulation has gained formal acceptance in every academic field. In fact, the field of climate science is entirely based on simulation models, even though some of them are difficult to validate. Furthermore, there is plethora of simulation languages and packages to address a wide spectrum of problems. In a recent issue OR/MS today magazine, Swain (2011) presented a survey of simulation software packages which boasted 55 simulation products from 29 vendors.
Figure 1-2: Block Diagram Of A DES Package [Adopted from Pidd and Carvalho(2006)]
10 tools which comprise of simulation objects with predefined methods and variables2, a
graphical library to visualize the system and integration capabilities in to corporate systems such as ERP systems, databases and spreadsheets. Secondly, a simulation package must be capable of executing simulation models with provisions for debugging, run control, and meaningful animations. Finally, the simulation package must have capabilities to perform analysis such as model experimentation and optimization, output analysis and interactive graphics to represent the results. The block diagram presented in Figure 1-2
accuratelyrepresents building blocks of a good simulation package.
1.4.2Healthcare Simulation Packages
Although any general simulation language can be used to model a healthcare system, it may be difficult for the modeler to model given the inherent complexity embedded in healthcare services. This concern probably spurred the development of specialized healthcare simulation packages to improve the cost effectiveness of employing simulation. In order to be precise, we define a healthcare simulation package as a simulation package consisting of object libraries and visualizations to model healthcare related situations with ease. Under this definition, MedmodelTM and Flexsim HCTM are the two popular software packages that can be categorized as healthcare simulation packages.
1.4.2.1 MedmodelTM
Developed in the late 1990s by Promodel Corporation, Medmodel package included functionality of ProModel (the general simulation package by Promodel) to match lab results to patients, preempting resources, staff schedules, subroutines and an extensive 2D healthcare symbol library. Moreover, this package had a drag and drop feature which made it easy to use. The package also has output analysis and optimization functionality along with
spreadsheet integration. A detailed tutorial on MedmodelTM is presented in Harrell and Lange (2001).
11 1.4.2.2 Flexsim HCTM
Flexsim HCTM is the healthcare extension of Flexsim, general simulation package. The Flexsim HCTM provides 3D custom objects to represent patient queuing, processing and resources with an in-depth focus on providing statistics in a graphically interactive way. Furthermore, Flexsim also has event triggers that allow the user to specify custom behavior from a drop down list when the corresponding system event is triggered. This construct can be used to develop preempt logic, among various other customized logic. It also provides a flow chart view to allow the modeler to represent the model logic without getting bogged down in the details of 3D figures. In terms of output analysis, Flexsim has a built-in
experimentation model as well as provides an add-in for Optimization and statistical output analysis. Flexsim has constructs to support Microsoft Excel integration, movie creation and interactive graphical presentations. For further information, refer to
http://www.flexsim.com/flexsim-healthcare/
1.5 Thesis Outline
Although, these healthcare simulation packages and paradigms have existed for some time, their application to real world healthcare problems has been only around 8% (Eldabi, 2009). In the same timeframe simulation has emerged as a popular decision support in the domains of manufacturing and services industries (Kuljis, Paul, and Stergioulas, 2007). This suggests that there are problems associated with current packages as well as paradigms which form the motivation behind this body of work.
Chapter 2 presents an extensive literature survey to study simulation software and healthcare industry. In order to understand problems associated with simulation packages, the literature survey spanning the domain of object-oriented simulation which covers the
evolution of simulation packages. To cover the healthcare aspect of this problem, we conduct a systematic review of healthcare simulation papers presented in Winter Simulation
12 The next phase of this thesis describes solutions to close the gaps in healthcare
simulation modeling elicited in previous chapters. In Chapter 3, we present the SIMIO-HC Toolkit along with the simulation development guidelines for developers and modelers. After the development of the tools, we address the issue of implementation of simulation projects in healthcare environment (Chapter 4). To demonstrate this, we apply the SIMIO-HC toolkit to build a Complex Integrated Multi-Facility System (CIMS) simulation model. We also explore the nature of simulation modeling engagements in this chapter. Finally, Chapter 5 presents the limitations of the framework and the work presented in this thesis. It also presents future directions for research in the domain of healthcare simulation.
13
Chapter 2
Literature Survey
The aim of this literature review is twofold: the first aim is to explore the domain of object oriented simulation and the second one is to perform a systematic review of the healthcare simulation domain. The ultimate goal of this review is to help the reader understand the scope of object-oriented frameworks for healthcare simulation.
2.1 Object Oriented Simulation (OOS)
Concepts of OOS first appeared in the Programming Languages journal in the paper SIMULA- an ALGOL based simulation language authored by Ole-Johan Dahl and Kristen
Nygaard (Dahl and Nygaard, 1966). The landmark paper introduced SIMULA’s basic concepts of classes, inheritance, polymorphism and run time (or dynamic) binding which are now considered as basics of Object oriented programming (OOP) and, by implication, OOS. The paper presents a very consistent framework and implementation of these concepts in ALGOL.
Roberts and Dessouky (1998) present a comprehensive review of the OOS field. They present a brief introduction to the concept of OOS and focus on polymorphism and dynamic binding concepts. They provide a detailed discussion on simulation libraries using C++, Self, Smalltalk, CLOS, Eiffel,Modula-3, objective-c and Java. The paper also provides a visual as well as textual comparison between procedural and OOS. Finally, the paper provides a list of future issues with OOS which includes OOS approaches to distributed and complex modeling, modeling and maintaining OOS systems, and validation of OOS models.
14 scalability and portability. A tutorial using Sim++ of all the above concepts is presented in this work.
For the reader to fully appreciate the elegance of OSS, an object-oriented view of the world is presented in Pegden (2010). This discussion presents the three views of simulation: Event, Process and Object. In the event orientation, the system is viewed as a serious of instantaneous events that alter the state of the system over time. Alternatively, in the process orientation view of the world, the entity flow is described in series of process step which change the state of the system over time. Finally, in the object-oriented view we see the world composed of objects that interact to alter the dynamics of the system. The object oriented view of the world is tandem with the way we view our world, which makes it easier to model complex problems.
On the topic of development of OOS languages, Bischak and Roberts (1991) present a comprehensive outlook on the central issues. The paper discusses world views and explains the OOS world view which is centered on an object. They also discuss scope, visibility and object creation and destruction and polymorphism in the context of OOS. In addition to this, they describe topics in object communication, problems and potential for OOS and
controversies surrounding OOS which refer to treatment of processes, control of simulation time, and statistics collection.
15 they modify objects which can be reused and in their own respect have developed a new object library.
J. A. Joines and Roberts (1998) is a one stop reference on OOS. The chapter covers topics from Object oriented thinking to implementation of these concepts using YANSL (Yet
ANother Simulation Language). In addition to all the basic concepts of OOS, it also discusses on the development of OOS languages which introduce the concept of frame and framework. A “frame” is a collection of classes that provide a level of abstraction for the
OOS language and “framework” is a collection of classes that provide the language a specific modeling ability.
Cubert and Fishwick (1998) explore the development of OOS in different simulation paradigms which include Finite State Machine (FSM), Functional Block Model (FBM), Equation Constraint Model (EQN) and System Dynamics (SD). The paper also explores the concept of multi-modeling and simulation application framework which is utilized in SIMIO. The paper also provides a detailed reference of object-oriented concepts to integrate model geometry and dynamics as well as the importance of visual elements to model building. The paper also discusses elements of OOS which include translator, simulation engine, and distributed model repository.
An earlier examples which is similar to this thesis is demonstrated in Malloy and Chen (1998) who extend SIMulation in Production, Logistics and Engineering (SIMPLE++) to model Personal Communication Service Network (PCS). The authors extended the
16 of the computer by reducing the scope of the simulation model which should be irrelevant given today's computing power.
The work presented in this thesis is a framework of healthcare objects; a collection of classes that can model healthcare operations. The classes were developed by extending classes from SIMIO’s bases classes. A special emphasis was placed on visualization given that simulation model’s credibility is derived from the engaging stakeholders. In addition to this, a framework’s utility was also factored in to the development which is influenced by the modeling capability and extensibility of the classes.
2.2 Systematic Review of Healthcare Simulation Literature
The field of healthcare simulation has exploded in the past decade to virtually include every segment of the healthcare industry. The simulation paradigms employed by these models have diversified from a handful to many different methodologies owing to a rise in computing power as well as the availability to user friendly software which has reduced the technical nature of modeling.
One of the earliest systematic reviews of the healthcare field was carried out by England and Roberts (1978) which reviewed ninety two simulation models and reported limited success of application of simulation models. Fone et al. (2003) performed a
subsequent literature review from the year 1980-1999 which assessed the value of computer simulation modeling in healthcare. The paper classified literature into five categories:
17 Building on the previous work, Jacobson, Hall, and Swisher (2006) presented a much more detail literature review of the DES packages in healthcare systems over the past forty years. The review divides published work in two main categories which are patient flow optimization and healthcare asset allocation. The review also has a section which deals with recent advances in modeling of healthcare systems. The main conclusion of their literature survey indicated there were few publications in the domain of complex integrated multi-facility systems or those that looked in to inter-departmental relationships. Their suggestions also included that the focus of DES packages should be on optimization add-ons, increased visualization, and object-oriented paradigm.
Günal and Pidd (2010) performed a systematic survey of DES literature and organized papers on the modeling detail required for accident and emergency units, outpatient and inpatient clinics. They also covered other types of hospital units and whole hospital simulations in their study. Their study also concluded that most studies are unit-specific and facility-unit-specific (i.e. customized for hospitals). They also report that literature is still vague on model implementation and use. A more general literature survey is presented by Katsaliaki and Mustafee (2011) where they extended the scope of modeling and
application areas. Their study also deals with the topics of funding, implementation, and model use in the healthcare domain.
Our literature review is survey of modeling techniques used in the healthcare domain. Since, the domain of healthcare simulation is expanding at a rapid rate, following a database search methodology will be flawed as we will miss landmark papers in simulation (Brailsford et al., 2009). Thus, we chose the Winter Simulation Conference which is a premier forum for simulation and chose to review the papers presented under the healthcare application section from the year 1997-2010 given their availability on the conference site.
18 and simulation tutorials. Thus, the areas specified below are explored in the rest of the
chapter.
1. Patient Flow and Optimization a. Outpatient Scheduling
b. Inpatient Scheduling and Admission c. Emergency Room Simulation Models d. Specialist Clinics
e. Physician and Healthcare Staff Scheduling 2. Healthcare Asset Allocation
a. Bed Sizing and Planning b. Room Sizing and Planning c. Staff Sizing and Planning 3. Health policy modeling
4. Multi-facility modeling 5. Tutorials
a. Modeling tutorial b. Implementation tutorial
2.3 Patient Flow and Optimization
A highly efficient hospital will be providing the a high quality of service for patients, as measured by patient related metrics such as patient waiting time, patient flow time, and patient service refusal rates. Patient Flow and optimization studies focus on improving the patient satisfaction by optimizing these patient related metrics by varying appointment scheduling systems, hospital resource allocation methodology, and reorganization of care processes to better serve the patient.
2.3.1Outpatient Scheduling
19 Guo, Wagner, and West (2004) presented a patient centric simulation approach to outpatient scheduling. They detail their development of the Patient Scheduling Simulation Model (PSSM) which can handle the four determinants of an outpatient department: External demand for appointments, Supply of provider slots, Patient flow logic (and accounts for internal generated demand) and a Scheduling algorithm. This paper also presents analysis strategies for scheduling algorithms which are extremely important.
Giachetti et al. (2005) present a discrete and continuous time simulation approach to analyze appointment scheduling at a dermatology clinic. The discrete event simulation model analyzed and created patient schedules, and the system dynamics model investigated
behavioral factors behind no show patients. This paper is a good example on how to combine and use discrete and system dynamics methodologies to analyze a system. This paper also provides an excellent summary on appointment scheduling policies. Giachetti (2008) investigates appointment scheduling policies for reducing patient wait time using a system dynamics model with queuing theory. This paper proves that when the no show rates are high, the system is operating below optimal capacity and suggests that pooling of
appointment types is a better alternative to overbooking.
20 the hospital is operating in steady state (or under normal condition) which might not be true always.
2.3.1Inpatient Scheduling
Operating Rooms (OR) or Surgical units are considered to be one of the most
expensive resources in a hospital. Thus, it must be allocated to the patients in a way that will increase its utilization rate while minimizing patient waiting times. Given the multifaceted nature of such problems, simulation has evolved to be a popular approach to solve them.
Lowery and Davis (1999) develop simple OR model using MEDMODEL software to evaluate block scheduling policies. Ferrin et al. (2004) develop incentives that can be
analyzed using a simulation model which are: Case Cart Completion, Pre Admission Testing and Room Turnaround time (includes setup and cleanup time). Denton et al. (2006) present a monte carlo simulation model and applied simulated annealing procedure to multi OR
surgical scheduling based on data collected from the Mayo Clinic. Huschka (2007) perform a bi-criteria evaluation OR scheduling problem where they analyzed the effects of competing objectives of mean patient waiting time versus overtime in the OR. The paper results suggest that the scheduling efficiency is highly sensitive to surgical mix. Ferrand, Magazine, and Rao (2010) study the allocation of OR room policies for elective versus emergency surgeries where they compare fixed and flexible policies.
Inpatient Scheduling heuristics are also a focus of research in the simulation
21 There are also other performance metrics on which efficient inpatient schedules can be generated. Reindl et al. (2009) develop a simulation model using SLX tool for a cataract surgical suite where they minimize the patient waiting time. The paper presents a
comprehensive analysis of performance metrics for OR scheduling. Stanciu, Vargas, and May (2010) present a revenue based approach to OR scheduling where the aim is to maximize revenue per unit time. The paper modifies the EMSRb algorithm to set near optimal protection level for each patient class. Pearce et al. (2010) develop a DES model to analyze the dynamics of preoperative room and its effect on OR. They also suggest a novel agent based modeling approach to improve the accuracy of the simulation model.
2.3.2Emergency Department (ED) Simulations
Emergency departments are on the frontline of healthcare service delivery. These services are critical to the public health infrastructure and a supply of patients for the
hospital. The demand for emergency services is unpredictable. Nonetheless, the services they provide are time critical where excessive waiting times could prove fatal. ED departments respond to these challenges by experimenting with their staffing levels and patient flow. This makes them excellent problems to be solved using simulation, different scenarios and
experiments can be examined without causing harm to anyone.
Rossetti, Trzcinski, and Syverud (1999) develop a staff scheduling simulation model in ARENA and is an excellent reference for verification and validation techniques for
22 Most of the ED simulations are planning tools whereby they are used for testing new and innovative policies before implemented in practice. Samaha, Armel, and Starks (2003) developed a simulation model in ARENA to test new ED policies to estimate the one that would reduce the length of stay (LOS). The paper developed a fast track policy to free beds for critically ill patients by expediting service for non-critical patient. Mahapatra et al. (2003) test a triage system for categorizing ED patients using a simulation model developed in ARENA in order to estimate patient waiting times in the ED. M. J. Miller, Ferrin, and Szymanski (2003) test six sigma policies using a simulation model of the ED employing the EXTEND simulation package. Davies (2007) tests the controversial “see and treat” policy versus “see” and “treat” policy using a SIMUL8 simulation package, where the former policy outperforms the latter one. The paper also discusses the problem of convincing the system’s stakeholders using simulation model. Ruohonen, Neittaanmaki, and Teittinen (2006) test the effect of triage team on the ED which according to their simulation model increases the ED efficiency by nearly 25%. Khurma, Bacioiu, and Pasek (2008) study the effect of new lean policies using a DES model and estimate savings in a future time horizon. Kolb et al. (2008) develop a simulation model in ARENA to test a five buffer concept which aims at reducing the overcrowding in the ER. Miller, Ferrin, and Shahi (2009) and Holm and Dahl (2010) estimate the impact of patient surge on ED operating efficiency.
ED simulation projects are the most common type of facility simulation projects which has given rise to a class of new class of simulation software, customized for its needs. M. J. Miller, Ferrin, and Messer (2004) present a study of the using EDSIM package in ER and the insights of using the tool. Sinreich and Marmor (2004) develop a simple and intuitive tool to analyze ED which flexible in design to account for difference in patient needs. Gunal and Pidd (2006) introduce DGHPsim simulation framework which can multitask and allocate doctor on the basis of experience. Holm and Dahl (2009) developed an ED model using FLEXSIM package where they simulate the effect of triage system.
23 are classified by the type of services required. Medeiros, Swenson, and DeFlitch (2008) present a Provider Directed Queuing system model for ED using ARENA which provides estimates of performance measures under various patient loads. Meng and Spedding (2008) model the ED using a combination of Fourier and autoregressive process which resulted in more realistic representation of the system. Beck, Balasubramanian, and Henneman (2009) present a simplified ED approach to model ED. Marmor et al. (2009) developed a real time decision support tool for ED using the offered load approach. Ismail, Abo-Hamad, and Arisha (2010) apply the balanced scorecard approach to optimize ED performance.
Chockalingam, Jayakumar, and Lawley (2010) model ED’s patients and resources flow using Petri nets. Using this model, they develop stochastic differential equations which are used for determining the time to divert ambulances to avoid ED overcrowding.
2.3.3Specialist Clinics
Specialist clinics are facilities that provide tertiary medical care such as
Chemotherapy centers, Laboratory, MRI imaging facility, etc. These clinics are highly
specialized in the services they provide, hence bringing in a new set of problems that can also be addressed by simulation. Most simulation studies that belong to the specialist clinic types focus on the facility design.
24 The models accounts for the cost for medicine shortages, medicine expirations, and the holding cost.
In addition to facility design, Specialist clinics simulation studies also deal with clinical quality management. Baesler and Sepulveda (2001) formulate a multi-objective optimization model for performance improvement in an oncology clinic. The objective was to minimize patient waiting time while maximizing resource and worker utilization. Martin, Gronhaug, and Haugene (2003) develop model to reduce overcrowding in geriatric clinic using PROMODEL by reducing patient waiting times. Centeno et al. (2010) develop a DES model to explore the factors affecting the performance of an endoscopy center. Interestingly, early arriving patients were causing the system to operate under capacity. Housseman et al. (2009) study the impact of RFID technologies in a cryo-conservation center and incorporate human error in to their simulation model. Ramis et al. (2008) model the imaging center as a pull system and minimize the patient waiting times. Yurtkuran and Emel (2008) develop a simulation based decision making tool to optimize pharmacy operations. Song, Bair, and Mingchang (2008) study the effect of physician starting time in a physical examination routine and patient arrival times using simulation with goal programming model.
2.3.4Physician and Healthcare Staffing
In resource constraint situations, physician and healthcare staffing becomes the focus of simulation problems that better serve the patient. These problems are usually
multi-objective problems where the simulation model minimizes provider idle times subject to patient constraints. Balasubramanian et al. (2007) convert a staffing problem in an
25 (2004) study the effectiveness of a tele-medicine program and conclude the poor scheduling of physicians and ineffective process flow is the root cause for poor system performance. Centeno et al. (2000) study the staffing policies using MEDMODEL in radiology
department.
2.4 Healthcare Asset Allocation
Healthcare is an ever changing field as it has to keep up with technological developments as well as demographic developments. In order to stay in line with these developments, hospital management teams rely heavily on planning and allocation of hospital assets. Simulation modeling is an attractive tool for these problems given the flexibility embedded in these tools and reduced assumptions required to model the scenarios.
2.4.1Bed Sizing and Planning
Bed availability is a major issue in hospitals as they must be available to treat patients. Moreover, bed availability in primary care facilities such as ICU and PACU will determine the efficiency of ED and OR respectively. On the other hand, having excess capacity will mean resource under-utilization and added maintenance costs which also is not acceptable solution. Cahill and Render (1999) develops a simulation model in ARENA for bed availability in the ICU unit. The further state that although they optimized the ICU bed utilization, it increased the backlog in downstream medical units highlighting the need for multi-facility approach to such problems.
2.4.2Room Sizing and Planning
26 Processing Time (LPT) schedule is the near-optimal schedule for operating rooms assuming longer operations have a longer recovery time. Ashby et al. (2008) use simulation as a tool for planning patient flow from the current hospital to replacement facility. Their work helps the administrators identify non-value added tasks which transforms this hospital in to a more efficient one. Alexopoulos et al. (2001) develop a simulation model to analyze a low cost vaccination clinic for the poor. The model is designed to incorporate other services in the future if they need to be offered.
Wiinamaki and Dronzek (2003) use simulation to validate an architectural design of an ED which would have impact on the downstream department. The model estimated future capacity requirements of the ED using length of stay of each patient. Miller et al. (2007) develop a simulation model to study the impact of merging six EDs in to a single one. This model identified potential bottlenecks in the ED simulation and was further used to test workarounds for the new facility.
Huschka et al. (2008) developed a DES model of relocation of interventional services for pain medicine at Mayo Clinic. This paper further states the importance of using
simulation in early stages of facility development as their model is critical for efficient facility design. de Mendonca et al. (2010) study the improvements to blood processing center using MEDMODEL package. The simulation model also accounts for human error in the order collection system which causes delays in the overall treatment of the patient.
2.4.3 Staff Sizing and Planning
27 improvement from the solution. Wong et al. (2003) study an electronic medical ordering system and its effect on pharmacy response time and correct medication delivery.
Weng and Houshmand (1999) present a case study on simulation application in a local clinic. They developed a model to estimate tradeoffs between patient performance measures and staffing cost to find the near-optimal staffing levels. Osidach and Fu (2003) also study the performance versus staffing cost tradeoffs in a mobile examination center. Spry and Lawley (2005) experiment with the staffing schedules in a pharmacy department as well as test the effect of a dispensing system to improve the facility’s effectiveness. Pirolo et al. (2009) studies the cardiovascular laboratory worker schedules which affects patient length of stay in ED. The simulation insights were considered in the redesign of the laboratory. Rohleder et al. (2010) developed a simulation model to test alternative care team design to improve the efficiency of the Mayo Clinic’s Outpatient department
Some studies in this category focus on the generalized staffing problems in whole system scenarios. Thorwarth, Arisha, and Harper (2009) derive a general analytic expression for staffing that leads stable queuing systems using simulation. Decision makers can use these expressions to design staffing policies that maximize service levels. See et al. (2009) study the staffing levels at an urgent care clinic during pandemic outbreaks and identify that clinical efficiency is sensitive to doctor staffing levels. Faller, Flynn, and Ferrin (2009) simulate the staffing levels for healthcare services in prison systems and provide a new process to improve the throughput of the system.
2.5 Health Policy Simulations
“The thing [medicine] that still startles me is how fundamentally human an endeavor
it is”, a quote from Atul Gawande’s bestseller “Complications” (Gawande, 2002). Healthcare
28 that we seek to answer using the simulation can be aptly framed as: “Which is the best course of treatment?” Simulation models presented in this section are decision tools to influence physicians or policy makers and improve the healthcare field’s quality of treatment.
One of the most common applications of simulation modeling in decision support is cancer screening and treatment. Baldwin, Eldabi, and Paul (1999) present a flexible Markov chain model for designing adjuvant breast cancer treatment trial. Based on this model’s insights, health policy makers can collect the relevant data to study the interactions in breast cancer treatment trials. Tafazzoli et al. (2005) compare the screening methodologies for colorectal cancer. This paper provides a deterministic and probabilistic cost effectiveness analysis. Yaesoubi and Roberts (2008) develop a simulation model to analyze the
willingness to pay cost of health insurance providers for colorectal cancer, which is the cost of additional one life year gained from screening.
Organ transplant policies are another field where simulations are widely used to decide on equitable allocation of organs. Harper et al. (2000) develop a liver transplant simulation model for Unified network for Organ Sharing (UNOS) organization and incorporate general organ rejection rate into UNOS Liver allocation model. Baldwin et al. (2000) study the prioritization criteria for waiting list patients on UNOS Liver allocation model. Taranto et al. (2000) develop a national kidney allocation model and take in to account post-transplant events. Abellan et al. (2004) develop a discrete event simulation model of patient waiting behavior for renal transplantation. They use Bayesian inference to model inputs to the model. Davies (2006) study the equitable kidney allocation problem for different risk groups.
29 (2009) study HIV treatment in drug scarcity environment. The paper develops a simulation model to evaluate the current WHO policies.
Healthcare policy simulations are also used in public health preparedness problems which deal infectious disease outbreaks and public health response system preparation. Brandeau (2008) discusses the role of simulation in infectious disease control policy. The paper present simulation case studies on HIV, Contact tracing and hepatitis B infection progression. Hughes, Currie, and Corbett (2006) develop a compartment model to simulate TB disease spread in the presence of HIV where they assume the HIV disease progression to be static. Mellor et al. (2007) develop a model to test strategies to detect TB in high
prevalence of HIV environment and conclude that active contact tracing is the better method for these scenarios. Wynter and Ivy (2009) study the public health response to an E.coli outbreak in North Carolina State fair and identify that lab capacity to be a major bottleneck. Worth et al. (2010) develop a DES model in ARENA to model an outbreak of infectious disease and the response of public health department. The model also accounts for secondary infection spread by creating a submodel for contact tracing. Yarmand et al. (2010) study the cost effectiveness of isolation versus vaccination for an outbreak of H1N1 in a university campus. The study methodology involved development of a simulation model to model the disease progression, and an optimization model to minimize vaccination costs. The study results were analyzed using grid search methodology to identify feasible solutions.
Andradóttir et al. (2010) develop stochastic compartmental model to model pandemics in a mid-sized North American city and study the social and economic impact of vaccination at different levels. Lizon, Aleman, and Schwartz (2010) develop a SIR (Susceptible Infected and Recovered) model for SARS infection where they take in to account effectiveness of public healthcare system along with different thresholds of infections. Silva and Pinto (2010) study the effectiveness of emergency medical systems using simulation and optimize it to maximize the number of life saved by the services.
Apart from DES, Agent based modeling in combination to DES is gaining
30 agent based model to model individual behaviors during pandemic responses. Their model also accounts for close and casual contact which affects the way disease progresses in the society. Carr and Roberts (2010) develop an agent based model in C++ to model an infectious disease progression. They superimpose a facility allocation problem which
identifies the best spots to open clinics to effectively control infections. Barnes, Golden, and Wasil (2010) develop a dynamic patient network model for spread of hospital acquired infection taking the dynamic nature of hospital care worker in to consideration. Soorapanth and Chick (2010) present a differential equation model to study the behavior of behavioral interventions for HIV-infected persons. The compartment infection model includes HIV behaviors and compares intervention policies. Ekici, Keskinocak, and Swann (2008) study food distribution logistics response to pandemic avian flu using a dynamic update approach to build the food network.
Ambulance diversions are another class of problems investigated by healthcare simulation models. Maxwell, Henderson, and Topaloglu (2009) develop a markov decision process to model the decision to divert ambulance and solve it using a dynamic programming approach. Hagtvedt et al. (2009) apply game theory to study the ambulance diversion
problem which takes in to account the economic choices for each player. Ramirez, Fowler, and Wu (2009) go one step further and develop a DES model to study the financial impact of ambulance diversion on hospitals. Nafarrate, Fowler, and Wu (2010) develop a simulation model to perform a bi criteria evaluation of Ambulance diversion policies thereby evaluating the direct impact of ambulance diversion on the emergency department. The criteria under evaluation are mean waiting time and percentage of ambulances diverted.
Healthcare policy studies also span the domain of pharmaceutical industry.
31 competitive market and controlled advertising will only affect sales and not the cost of the drug.
2.6 Multi-facility Simulation Models
Until this point in this literature survey, we have presented the papers that only dealt with problems that are specific to a particular facility or for an operation type or function. In all of these models, our modeling insights are restricted to the operation under analysis and ignore the cascading effects of improvements on the connected parts of healthcare system. For example, improvement of ED throughput may increase the back log at inpatient units or may upset the scheduling of OR departments. Another good example is the experimentation of physician schedules. Physicians are shared between hospital departments and changing them in one department may have a pronounced effect in another department where the doctor’s works. These complex relationships that exist between facilities are investigated in the papers presented in this section.
Ballard and Kuhl (2006) develop a general method to estimate the maximum capacity of OR using simulation model while accounting for capacity constraints of PACU, Inpatient and outpatient departments. James Swisher et al. (1997) develop a simulation of physician network by taking in to account the staffing levels at each clinic which affects patient throughput. The patients use a call center for appointment scheduling which allocates patients based on their needs and clinical availability. This model was developed in a Visual simulation environment using an object-oriented approach. Multi-facility simulation systems are data intensive, which can be overcome using electronic medical records as presented in Takakuwa and Katagiri (2007). They develop a detailed simulation model of the whole hospital by harnessing the power of electronic medical records.
32 Ashby et al. (2008) simulate the complexities involved in transitioning of patients from the inpatient units of one hospital facility to another for the purposes of renovations. Kolb et al. (2007) study the effect on patient related metrics by coupling of ED and inpatient unit.
2.7 Simulation Tutorials
Every field needs practitioners that can advance the practice. Significant work presented in WSC belonged to the category of simulation theory. Simulation theory can be grouped in to two sections: Modeling and Implementation which will be discussed in the following sections.
2.7.1Modeling Tutorials
To propel the field of simulation forward, there needs to development in modeling techniques which can be brought around by development
• new modeling tools enhancing current modeling capabilities
• development of new software to address requirements of new domains • new modeling techniques to capture the dynamics of complex systems
These papers help simulation community stay abreast with latest advancements in the field of simulation modeling.
![Figure 1-2: Block Diagram Of A DES Package [Adopted from Pidd and Carvalho(2006)]](https://thumb-us.123doks.com/thumbv2/123dok_us/1614114.1200205/27.612.114.522.333.578/figure-block-diagram-des-package-adopted-pidd-carvalho.webp)