FINITE ELEMENT SIMULATION OF THREE SURGICAL TREATMENTS OF DISTAL RADIUS INTRA-ARTICULAR FRACTURE
ARASH NASROLLAHI SHIRAZI
A report submitted in partial fulfillment of the requirements for the award of the degree of
Master of Engineering (Mechanical)
Faculty of Mechanical Engineering Universiti Teknologi Malaysia
iii
To my beloved mother and father, Fakhrosadat Banaroei and Mohsen Nasrollahi Shirazi and my brother and sister, Pooyan and Sanaz for their never ending support.
iv
ACKNOWLEDGEMENT
To complete this Master Degree Project report, I learned many useful softwares and I had received a lot of information and valuable guidance from my supervisor, Assoc Prof. Eng. Dr. Rafiq Abdul Kadir. His knowledge and proficiency in Biomechanics supported and encouraged me to complete this project.
I respect and thank my beloved family Mrs. Fakhrosadat Banaroei and Mr. Mohsen Nasrollahi Shirazi, my sibeling, Mr. Amir and Mrs Fateme for their constantly love and support.
v
ABSTRACT
vi
ABSTRAKT
vii
TABLE OF CONTENT
CHAPTER TITLE PAGE
TITLE i
DECLARATION ii
DEDICATION iii
ACKNOWLEDGEMENTS iv
ABSTRACT v
ABSTRAK vi
TABLE OF CONTENTS vii
LIST OF TABLES xi
LIST OF FIGURES xii
LIST OF ABBREVIATIONS xiv
1 INTRODUCTION 1
1.1 Introduction 1
1.1.1 Wrist anatomy 1 1.1.1.1 Bones and joints 2
1.2 Wrist fracture 3
1.2.1 Distal radius fracture 3
1.3 Problem Statement 4
1.4 Objective of Study 5
viii
2 LITERATURE REVIEW 6
2.1 Introduction 6
2.1.1 Classification of intra-articular fracture 6 (1) Intra-articular fracture with displaced
dorsal fragment 7 (2) Dorsal split with dorsal dislocation 7 (3) palmar split with palmar dislocaton 8 (4) Complex distal radius fractures with
metaphyseal separation 9 (5) Destruction of the articular surface 9 2.2 Different studies on fixation methods 10 2.2.1 Clinical Method 10 2.2.1.1 Non-invasive Techniques 11 2.2.1.1.1 Conservative treatment 11 2.2.1.1.2 External Fixation 12 2.2.1.1.3 Pining 13 2.2.1.2 Open surgery 14 (a) Plates 14 (b) Fragment-specific Fixation 15 (c) Volar locking plates 16 2.2.2 Protocol for surgical treatment 17
2.3 Experimental Method 18
2.3.1 A novel non-bridging external fixator versus
volar angular stable plating 19 2.3.2 Comparing volar with dorsal fixation plates on
unstable extra-articular fractures 20 2.4 Computer Simulation Method 22
2.4.1 Biomechanical evaluation of three types of
implants 22
ix
3.1 Introduction 27
3.2 Mimics Software 27
Step 1: Imported the medical data 28 Step 2: Thresholding 29 Step 3: Segmentation density masks 29 Step 4: Region growing 30 Step 5: 3D Reconstruction 31 3.2.1 Constructed of fractured bone 32
3.3 Implant Design 35
3.3.1 Introduction of Solidworks Software 35 3.3.2 Designing the implants 36 3.4 Simulation of surgical fixation 37 3.5 Introduction to MSC.Marc Software 39 3.5.1 Analysing the three fixation methods 40 3.5.2 Applying the loads 41
4 RESULTS AND DISCUSSION 43
4.1 Introduction 43
4.2 Axial-loads results 44
4.2.1 Displacement 44 4.2.2 Von-Mises Stress 46
4.3 Bending results 49
4.3.1 Displacement 49 4.3.2 Von-Mises Stress 51
4.4 Torsional results 53
x
5 DISCUSSION AND RECOMMENDATION 62
5.1 Discussion 62
5.2 Recommendations 63
xi
LIST OF TABLES
TABLE NO. TITLE PAGE
4.1 Maximum displacement (mm) and maximum von Mises stress (MPa) values of the bone around the screws of all three groups under the applied loads
47
4.2 Maximum displacement (mm) and maximum von Mises stress (MPa) values of the bone around the screws of all three groups under the bending loads
52
4.3 Maximum displacement (mm) and maximum von Mises stress (MPa) values of the bone around the screws of all three groups under the torsional loads
xii
TABLE OF FIGURES
FIGURE NO. TITLE PAGE
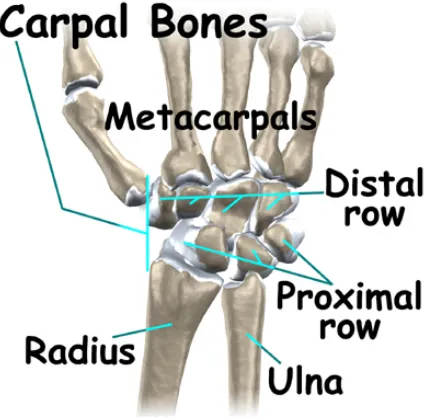
1.1 Distal and proximal rows of carpal bones 2
2.1 CT-based classification of comminuted intra-articular fractures of the distal radius. Type I: intra-articular
fracture with displaced dorso-ulnar fragment
7
2.2 Type II: dorsal split with dorsal dislocation 8
2.3 Type III: palmar split with palmar dislocation 8
2.4 Type IV: complex distal radius fractures with metaphyseal separation
9
2.5 Type V: destruction of the articular surface 10
2.6 Schematic drawing of a monolateral external fixator with double ball joints after application to the radial aspect of the second metacarpal and diaphysis of the radius: the distal ball joint is centred between the capitate (C) and lunate bone (L) (intraoperatively
by identification with a bone elevator under image intensification, lower part of the image) to allow for
mobilisation of the fixator.
xiii
2.7 Typical placement of two T-pins for fixation a distal radius fracture is shown in this posterior-anterior radiograph. The surgeon has inserted two T-pins from
the radio styloid to stable fracture fixation. The surgeon has inserted two T-pins from the radio styloid
to stable fracture fixation
14
2.8 A fragment-specific wrist fixation system 15
2.9 A 31-year-old woman with reverse Barton fracture fixed by volar locking plate
16
2.1O The southern Sweden treatment protocol for DRF when selecting different treatments the patient’s age
and demands
18
2.11 Experimental test with isolated radius placed of custom-made compensator to applied ratio (60-40%)
of the forces transferred to scaphoid and lunata fragments. (A) Non-bridging external fixation method.
(B) Volar locking fixation method
19
2.12 (A)The LDRS 2.4-mm intermediate and styloid plates. (B)The LDRS 2.4-mm volar plate.
(C)The LDRS 2.4-mm volar and styloid plates. (D) The 3.5-mm stainless steel T plate.
21
2.13 Finite element of different surgical methods. (A) T shape single volar plate meshing model. (B) Meshing
model of double-palates fixation method. (C) The modified double-plating (MDP) meshing model
xiv
2.14 Loading conditions for model. Axial loading bending and torsion are indicated with arrows. The axial loading was applied in the middle of the upper radius
surface. The bending force was applied on the volar side of radius. Torsion is applied on both sides of the
radius representing the external rotating force
24
2.15 (A) Average total displacement of the fracture site under 50 N axial compression, 2 N-m bending and 2 N-m torsion loads. (B) Maximum displacement of the
fracture site under 50 N axial compression, 2 N-m bending and 2 N-m torsion loads
25
2.16 (A) Maximum von Mises stress value for bone in single, DP, and MDP models under 50 N axial compression, 2 N-m bending and 2 N-m torsional loads. (B) Maximum von Mises stress value of T plate
in single, DP, and MDP models under 50 N axial compression, 2 N-m bending and 2 N-m torsional loads
26
3.1 CT scan image for using in mimic 28
3.2 The top and side views for radius bone that Thresholding by the white color triangular to separate
the radius bone
29
3.3 The side view of region growing that shown in pink color
30
3.4 The process of smoothing (A, B and C) to achieve radius bone
31
3.5 The measured guide lines for cutting (A) Approximately 10 mm(10.44 mm) from the from articular surface. (B) About 15° (14.81°) volar wedge
xv
3.6 The simulated three segments unstable intra-articular fracture (AO 23-C2.1 fracture). The circle shows the
cut with the curve tool
33
3.7 (A) The scaphoid segment cleaned meshes. (B) The lunate segment cleaned meshes. (C) The distal
part of the radius cleaned meshes (all segment related to the cortical parts only)
34
3.8 (A) Intermediate dorsal LDRS 2.4 mm plate. (B) Volar T-shape LDRS 2.4 mm plate. (C) I-shape Styloid
LDRS 2.4 mm plate
37
3.9 Fixed all the meshes around the screws on both cortical and cancellous parts of bone
38
3.1O Fixed all the interfaced meshing part between all cancellous and cortical and screws. (The red parts
show the interfaced parts)
39
3.11 Defined the young’s modulus, Poisson’s ratio and contact parts for each part (that showed in collared
parts)
40
3.12 Axial loading that applied on scaphoid and lunate regions base on each percentage and tilt angle, bending load that exerted on simulated bone on volar side of the radius and the torsion applied of the radius part of the
bone
42
4.1 Model rigidity under axial compressive load 45
4.2 Maximum displacement of the bone around the screws under the 10 N, 25 N, 50N, and 100 N loads
xvi
4.3 Maximum von-Mises stress under the 10 N, 25 N, 50N and 100 N loads
46
4.4 Maximum von-Mises stress of the bone around the screws under the 10 N, 25 N, 50N, and 100 N loads
47
4.5 The contour plots of displacement for three groups of fixations under applied 100 N axial load
48
4.6 The mean maximum displacement under bending loads (1 N-m, 1.5 N-m, 2 N-m)
50
4.7 The maximum displacement around the screws under applied bending loads (1 N-m, 1.5 N-m, 2 N-m)
50
4.8 The maximum von-Mises stress under applied bending loads (1 N-m, 1.5 N-m, 2 N-m)
51
4.9 The maximum von-Mises stress around the screws under applied bending loads (1 N-m, 1.5 N-m and
2 N-m)
51
4.1O The contour plots of displacement for three groups of fixations under applied 2 N bending load
53
4.11 The mean maximum displacement under torsion loads (1.5 N-m, 2 N-m, 2.5 N-m)
54
4.12 The maximum displacement around the screws under applied torsion loads (1.5 N-m, 2 N-m, 2.5 N-m)
55
4.13 The maximum von-Mises stress under applied bending loads (1.5 N-m, 2 N-m and 2.5 N-m)
56
4.14 The maximum von Mises stress around the screws under applied torsion loads (1.5 N-m, 2 N-m and
2.5 N-m)
xvii
4.15 The contour plots of displacement for three groups of fixations under applied 2 N torsional load
58
4.16 (A) Average total displacement of the fracture site under the 100 N axial compression, 2 N-m bending and 2.5 N-m torsional loads. The total displacement was averaged from the displacement of the nodes on the fracture site. (B) Maximum von Mises stress value
for bone in three groups of fixations under 100 N compression load, 2 N-m bending and 2.5 N-m
torsional loads
xviii
LIST OF ABBREVIATIONS
2D - Two Dimensional 3D - Three Dimensional CAD - Computer-Aided design CT - Computerized Tomography DRFs - Distal Radius Fractures DP - Double Plating
FEA - Finite Element Analysis HU - Hounsfield Scale
CHAPTER 1
INTRODUCTION
1.1 Wrist joint
Wrist joint is the most complex of all joints in the body. The wrist must be
extremely mobile to give our hands a full range of motion. At the same time, the wrist
must provide the strength for heavy gripping. The kinematics and kinetics of the wrist
hasn’t been completely understood yet. The wrist joint plays a significant role in
maintaining a normal daily life. Normal wrist motions involve with the ligaments as well
as the carpal, radius and ulna bones [1].
1.1.1 Wrist anatomy
2
• bones and joints
• ligaments and tendons
• muscles
• nerves
• blood vessels
1.1.1.1 Bones and joints
The connections from the end of the forearm to the hand there are 15 bones. The
wrist itself contains 8 bones, called carpal bones, the ulna and the radius. The carpal
bones are separated into two rows, namely the proximal and distal that shown in Fig1.1.
3
The wrist joint comprises into three different parts, the radiocarpal joint,
intercarpal joint and the distal radioulnar joint. Most of the movements of the wrist
occurs at the radiocarpal joint, which is a synovial articulation composed by distal end of
the radius and the scaphoid, lunate and triquetrum bones [2].
1.2 Wrist fracture
Wrist fractures are kind of fractures that happen any of carpal bones and two
forearm bones (radius and ulna). The most commonly wrist fractures are distal radius
and scaphoid fractures.
1.2.1 Distal radius fracture
Comminuted fractures of distal end of the radius are caused by high-energy
trauma and present as shear and impacted fractures of the articular surface of the distal
radius with displacement of the fragments. The position of the hand and the carpal bone
and also the impact of the forces cause the articular fragmentation and the displacement.
Distal radius fractures are very common. In fact, the radius is the most commonly
broken bone in the arm. The break usually happens when a fall causes someone to land
on their outstretched hands. It can also happen in a car accident, a bike accident, a skiing
4
1.3 Problem Statement
Distal radius fractures are among the most common injuries, with an estimate
overall crude incidence of 36.6/10,000 years in women and 8.9/10,000
person-years in men. Assuming a continuous rise in the incidence of distal radial fractures with
age, and based on the fact that older population continues to grow, incidence of distal
radius fractures can be expected to increase. To allow for good functional outcome
following unstable distal radius fractures, restoration of both the radiocarpal and the
radioulnar relationship is essential, therefore surgical treatment should facilitate for
anatomic reduction and maintenance of the reduction. It means different surgical
methods can be used to fix the complicated, unstable and displaced distal radius
fractures.
The conventional volar plating for treated the dorsal displaced distal radius
fractures has been described with good results in young patients and with a mix of
fracture complexity. However, elderly patients with osteoporotic bone may have higher
risk of loss of reduction in conventional types of fixation because of screw loosening
and because of the toggle effect of the screws within the distal part of the plate.
Therefore the necessity of an optimum technique for restore not only the anatomical
alignment of the wrist but also its proper biomechanics such as preventing
re-displacement of the fragments and re-establishing the normal wrist load transmission
5
1.4 Objective of study
The objective summery of this study included:
1) Simulation of the distal part of the wrist and also simulation the
intra-articular distal radius fracture (AO 23-C2.1).
2) To develop 3D model of the fractured bone for all types of fixation
methods.
3) To simulate various surgical treatments for this type of intra-articular
fracture.
4) To compare between all different types of surgical treatments for fracture
fixation of the distal radius.
1.5 Scope of study
The scope the study, to simulate the 3D model of radius bone and also simulated
the unstable intra-articular fracture on bone. The next step to find the surgical methods
for this kind of distal radius fracture and simulated these surgical method as same as the
real plates of fixations. Then according to surgical open reduction and internal fixation
should find the optimum positioning for all types of fixations on fractured bone. To
provide the valid analysis should find the best positions for boundary condition and
exerting the loads. Should mention that the loads values should be choose base on the
daily motions that fractured wrist faces. Finally, should compare the results of all types